
Abstract
How has Sub-Sahara Africa (SSA) experienced the COVID-19 pandemic? This article seeks to examine the challenges faced by a region that was earlier expected to be the epicenter of the pandemic. The study identifies three critical stages that pose challenges for governments and development partners operating in SSA trying to avoid mass infections and the subsequent negative socioeconomic impacts of the pandemic. First, the article begins by examining the challenges experienced in restraining the spread of COVID-19 such as the lack of adequate resources and technology to effectively pursue contact tracing, the dilemma of implementing lockdowns, and the impact of fake news. Second, the article looks at the challenges arising from technical and capacity elements of testing, treatment, and the development and access to vaccines. Finally, the study examines the potential obstacles to a smooth post-COVID-19 recovery. The author argues that although some positive actions have been taken by governments in SSA during the pandemic, the challenges that are emerging as a result of the direct and indirect impacts of the disease cannot be overlooked. The authors therefore offer several recommendations that can guide policy responses against pandemics in the short and long-run.
Introduction
The novel coronavirus (COVID-19) pandemic has emerged as one of the most serious global health crises recorded in the recent history (UNDP, 2020). Since its outbreak in China (Wuhan) in December 2019, the virus spread to all the seven continents, leaving behind devastating social and economic impacts (Gondwe, 2020). By April 30, 2021, the World Health Organization (WHO) reported over 150 million COVID-19 confirmed cases, and 3.158 million deaths globally. Additionally, as of a similar date, America (61.9 million), Europe (51.6 million), and South East Asia (21.8 million) emerged as the three leading regions with the highest confirmed COVID-19 infections.
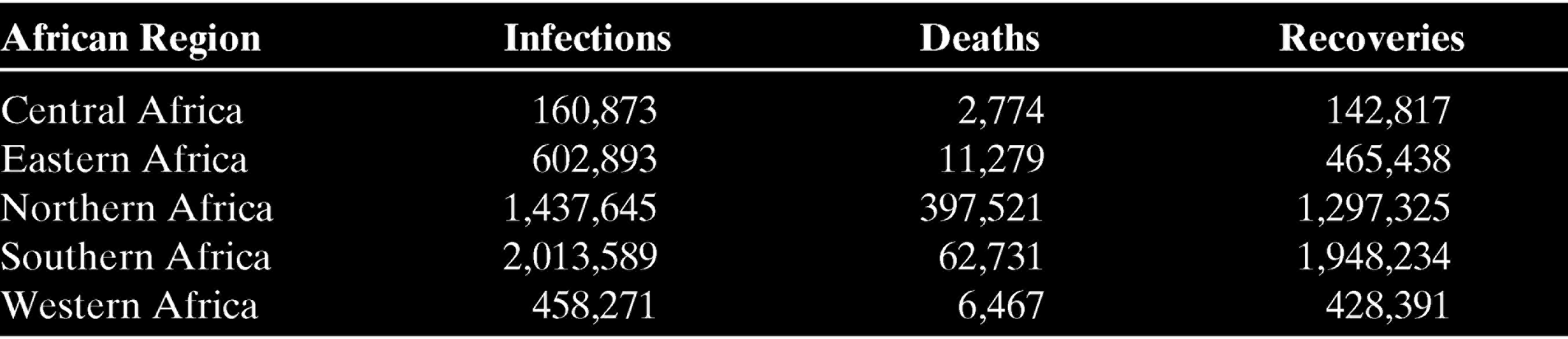
Comparatively, by the same period, Africa had recorded lower numbers of infections despite earlier statistical models projecting that the continent was likely to be the most ravaged by infections. The continent recorded its first case in Egypt in February 2020, and by April 30, 2021, infections had increased to over 4.5 million, over 121 thousand deaths, and approximately 4.1 million recoveries. In Sub-Saharan Africa (SSA), Nigeria was the first country to record the first positive test on February 27, 2020. However, South Africa emerged as the worst hit country in the SSA by April 2021 after recording more than 1.5 million infections, over 54 thousand deaths, and approximately 1.5 million recoveries. Other countries such as Ethiopia, Nigeria, and Kenya followed at distant, respectively. During the earlier phases of the pandemic, most of the confirmed cases of the virus were largely imported from Europe and the USA rather than China where it originated (Shabir & Aijaz, 2020). Henceforth, infections were largely a result of community transmissions. By the end of April 2021, the southern African region had the highest number of COVID-19 confirmed cases in Africa (Africa Centre for Disease Control [A-CDC]) (Table 1).
Regional Statistics of COVID-19 in SSA by April 30, 2021
Although governments were able to record some success in the management of COVID-19 after the first wave of infections, the relaxation of public health protocols subsequently led to the outbreak of second wave of infections across Europe, America, Asia, Middle East, and Africa by December 2020 (Salyer et al., 2021). In Africa, some studies such as Anjorin (2020) highlighted the fear of the continent undergoing a third wave of infections which could have been deadlier than what had been experienced during the first wave between February and June 2020. The commencement of COVID-19 vaccine manufacturing in December 2020 offered a great ray of hope that perhaps Africa could even pull through the pandemic without experiencing a severe outbreak of the virus as had been projected in earlier scientific models. But new problems that emerged around vaccine distribution in the form of vaccine nationalism raised questions whether the continent would be spared from the worst of the virus given the continent’s lack of adequate capacity to secure adequate vaccines for its citizens. As such, after 18 months since the outbreak, it is perhaps too early to assess the full impact of COVID-19 in terms of infections and deaths in SSA.
From an economic outlook, the pandemic hit the continent at a time when prospects of most SSA countries were high and promising. In early 2020, Africa was on course to continue its economic expansion, with the projected growth rate increase from 2.9% in 2019 to 3.2% in 2020 and 3.5% in 2021 (United Nations, 2020). Significant gains were also recorded in health indicators and poverty reduction. Technology and innovation were highly embraced across SSA, with African youth acting as early adopters of new technological platforms such as mobile money (Muragu et al., 2021). The entry into force of the African Continental Free Trade Area (AfCFTA) in May 2019 promised to boost intra-African trade by as much as 25% by 2040 (UNCTAD, 2019). A study by Odusola (2018) observed that the region enjoyed some of the highest global returns on foreign direct investment.
When COVID-19 emerged, these economic gains experienced significant reversals. But of more concern were the potential indirect political consequences of the virus. Although SSA has made great strides economically, the continent still has struggled with endemic problems of political instability, human rights violations, corruption, conflicts, humanitarian crises, unfair electoral processes, and weak governance. The public health measures and protocols that were needed to manage the further spread of the virus could be easily exploited by autocratic regimes to centralize political power.
It is against these dynamics that SSA states were faced with a unique position in managing the challenges posed by the COVID-19 pandemic. As a health problem, prolonged lack of investment in critical health systems, on the one hand, and decades of economic growth characterized by growing inequalities, the pandemic found several SSA states in very fragile conditions. As the pandemic unfolded, it became imperative that SSA take careful and sustainable measures to prevent and reduce the impact of the pandemic, and strengthen the foundations from which the region could recover and continue with its socio-political and economic development agendas. Failure to achieve this could throw many countries in the region into long-term and deep political, economic, social and humanitarian crises. It is in this context that this article seeks to uncover the challenges and recovery opportunities of the COVID-19 pandemic in SSA.
Challenges in managing the spread of COVID-19 in SSA
Dire predictions about the SSA region somewhat made sense in a way as most African governments did not appear to take the virus threat seriously. Most African countries continued to allow direct flights from China when most Western countries prohibited planes from certain cities in Asia during the initial stages of the pandemic (Stone et al., 2020). Nonetheless, the nearly three months that passed before the first positive test was confirmed in SSA could be considered as having granted African countries a window of opportunity to prepare for the outbreak. But could SSA states, even when given ample time to prepare for the pandemic, had been able to do so? As a developing region, SSA faced numerous structural challenges that undermined any sort of effective and efficient response mechanism required against an infectious virus pandemic such as COVID-19.
Most countries in SSA are ranked as low- or middle-income countries with resource-poor and fragile health systems in terms of health infrastructure (Gilson et al., 2020). As a consequence, countries are often woefully unprepared for any severe outbreak of infectious diseases such as COVID-19. The capacity of SSA states to provide critical intensive care was highlighted by the WHO as amongst the lowest in the world (Lucero-Prisno et al., 2020). For example, for over 12 months after the outbreak of COVID-19, Kenya had only 600 intensive-care unit (ICU) beds for its entire population of about 53 million, compared to the United States that had 34 ICU beds for every 100,000 people (Ouma et al., 2020). Similarly, most West African countries had less than two doctors per 10,000 people, compared to Italy, which had 41 doctors per 10,000 (Tinto et al., 2020). Severe infections of COVID-19 were diagnosed to lead to respiratory problems that require ventilation support. But in the absence of adequate ventilators, qualified health practitioners, reliable power supply, and oxygen, managing the virus became a huge challenge. Equally important, health centers in many urban centers in SSA tended to be overcrowded, whereas in rural communities, unmotorable roads and unreliable means of transport made it difficult for people to access health care (Dagba et al., 2021).
As a measure to manage the spread of the virus, health experts and institutions prescribed the adoption of several behavioral changes to supplement the gradual distribution of vaccines (Dagba et al., 2021). The behavioral practices included, but not limited to, proper hygienic sneezing and coughing techniques; avoiding overcrowded places or gatherings such as places of worship and open markets; frequent washing of hands with running water and soap; using hand sanitizers; wearing face masks in public places; not shaking hands; and maintaining a social distance of at least 1 m from the next person (Van Bavel et al., 2020). But in SSA, poverty rates remain high and many people live in overcrowded slums. According to a study by Ilesanmi et al. (2020), approximately 61.7% of African urban dwellers live in slums; thus, it was nearly impossible for individuals to observe social distance protocols (D’Alessandro et al., 2020). Moreover, these behavioral practices needed to manage COVID-19 clashed with African cultural norms and the daily ways of social life. Handshakes and frequent unplanned social visits characterize African social relations. Often, refusing to shake hands, for instance, is interpreted as a sign of disrespect for the other person, especially when the other person is elderly. Even though avoiding handshakes and maintaining social distance were difficult, staying at home was a much bigger problem for the many day laborers and self-employed individuals working in the informal sector. According to a study by Kraemer-Mbula and Wunsch-Vincent (2016), the informal sector was the main source of employment across SSA, accounting for more than 70% of employment. As such, for the majority of people, staying at home amounts to sentencing those in the informal sector and daily wage earners to eviction from their homes, malnutrition or even starvation.
A study by Dagba et al. (2021) observed that African governments implemented blanket policies that affected the less privileged members of society. Given the informal nature of African countries, many people who are mostly daily wage earners and laborers flouted the COVID-19 health protocols such as curfews, lockdown, and social distancing imposed by governments (Nyadera & Onditi, 2020). Also, corruption was reported regarding the management of COVID-19 funds in Africa. For example, Kenyan investigators recommended the prosecution of at least 15 top government officials and businesspeople over the alleged misuse of millions of dollars meant for buying COVID-19 medical supplies (Igunza, 2020). In Ghana, Anas Aremyaw Anas’ “Corona Quacks” exposé implicated quack doctors who sold fake COVID-19 cure to the public valued in thousands of dollars (Anas, 2020).
Van Bavel et al. (2020) also observed the global rise in fake news and misinformation. In their study, they discussed the disconnect between scientific information and public perceptions regarding curfews, lockdown, regular hygiene, and social distancing. Noncompliance with COVID-19 safety protocols in SSA was also due to social media misinformation, conspiracy theories, and the inaccessibility of government information in remote areas. This “infodemic” was more acute in countries such as Tanzania, Burundi, and Madagascar where the government publicly denied either the existence of COVID-19 itself, or that it was a dangerous virus (Orso et al., 2020). In Tanzania, for instance, on April 27, 2020, the late President John Pombe Magufuli declined to implement COVID-19 protocols and instead argued that Tanzania was protected against the virus through divine intervention, and that what the country needed to combat the virus was prayers (Munishi, 2020). This greatly eroded public perception of the virus and significantly minimized the likelihood of public adherence to COVID-19 protocols.
In 2020, several SSA countries were scheduled to hold elections. In many of these states, political processes such as campaigns continued in earnest. Overcrowding in rallies in total disregard of COVID-19 protocols characterized elections in Burundi, Burkina Faso, Côte d’Ivoire, Central African Republic, Malawi, Uganda, and Ghana (Asplund & Akinduro, 2020). The reputation of SSA states to not conduct free and fair elections in the past, as well as the tendency of African leaders to attempt overstaying their term, made it very difficult for any discussions to be held with regard to postponing an election. Many SSA regimes are treated with great suspicion in the court of public opinion, and any attempts made to discuss the postponement of elections could not be perceived as a genuine concern to manage the pandemic, rather, as just another attempt by an African leader to remain in position of power.
Perhaps the greatest challenge to the management of COVID-19 was the absence of domestic biotechnological production and scientific research expertise that could enable SSA governments to undertake adequate testing and research in virus transmission and vaccine development. Indeed, SSA countries were largely dependent on imported equipment and reagents needed for the testing of the virus. Although capacity to meet the demand for critical equipment such as personal protection equipment rapidly developed within the first few months after the outbreak of the virus, testing continued to be significantly hindered by the inability for states to achieve rapid technological expansion and financial limitations (Kavanagh et al., 2020).
Despite these deep and glaring challenges that Africa faced during the pandemic, from a perspective of public health, and comparatively to the experiences of other regions, SSA recorded lower cases. Perhaps Africa’s experience in dealing with several diseases and viruses such as HIV/AIDs, Ebola, malaria, and tuberculosis, proved to be an advantage (Mennechet & Dzomo, 2020) because African governments and communities had developed some sort of indigenous mechanisms to respond to infectious diseases (Ogunleye et al., 2020). Over time, several SSA countries had benefited from past global initiatives to strengthen health systems to combat malaria, HIV/AIDs, tuberculosis, and Ebola (Mwisongo & Nabyonga-Orem, 2016). The African Centre for Disease Control, on the other hand, had also accelerated efforts to strengthen surveillance and diagnostic capacity of the continent; thus, Africa, at the time of the outbreak, was less fragile and vulnerable as had been widely thought.
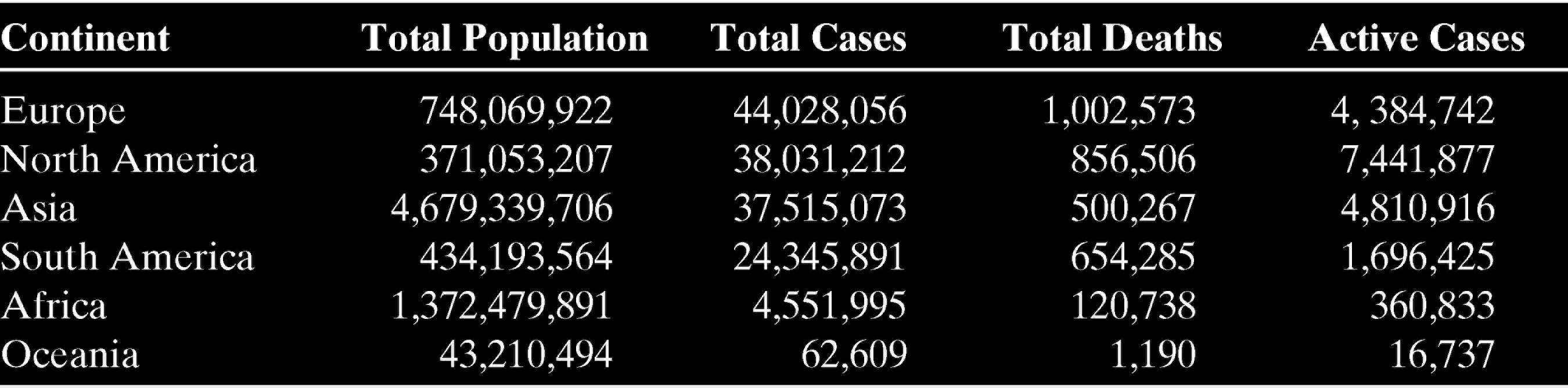
Additionally, heads of states and governments, Ministries of Health, hospitals, clinics, and community health centers took swift actions after the WHO declared COVID-19 a global health pandemic, and the continent begun recording positive tests (Onditi et al., 2020). SSA countries vigorously pursued containment measures such as identifying, assessing, and isolating people suspected to be infected or had been in close contact with an infected person. By March 2020, other radical mitigation measures such as closure of borders, suspension of internal flights, closure of public markets, and enacting bans on social gathering were adopted (Nyadera & Onditi, 2020). These measures significantly shaped Africa’s experience with COVID-19 by proving wrong previous predictions that the SSA would be overrun by infections within a few months after infections shifted from being imported to community transmission. Table 2 shows that Africa follows the Oceania region as the least continent affected by the pandemic. By April 27, 2021, the African continent had recorded less than five million coronavirus cases.
Coronavirus Cases by Regions of the World
The debate as to why the continent of Africa has not seen the worst of the COVID-19 pandemic and whether it is only a matter of time before high numbers of infections and death increase remains unanswered (Nyadera et al., 2021). One thing that the authors have observed is that unlike other outbreak of diseases in the continent, the response by the African government has been different. Most countries were quick to adopt WHO prevention measures such as closing their borders, setting up scientific committees, imposing cessation of movement between cities, as well as better publicity of the dangers of the disease. In addition, the authors argue that a low number of visitors from a high-risk regions during the initial outbreak, low mobility within the country, especially by those coming from abroad and who tend to stay within the capital cities, as well as previous experience dealing with other pandemics could explain why African countries, except for a few regions in the north and south, have recorded less numbers of cases. Indeed, the question of testing has been brought up as a justification for the low numbers with proponents arguing that low tests in the continent could explain the low number of infections being reported. However, from the experience in the USA, Europe, Latin America, and countries such as India and Brazil, the number of people seeking medical and hospitalization as well as the number of deaths in the mentioned regions and countries are much higher than the continent.
Despite the low cases of infections and deaths in Africa, at least in the context of earlier statistical models, the continent should not have the illusion that it has adequate capacity and experience to combat the virus. The experience of India’s second COVID-19 wave has offered a stark example of the dangers of falling prey to illusion, and why the region must continue to build its capacity. There is need for coordinated intra-African and global support and collaboration. The rise of nationalism that was experienced during the purchase of critical medical equipment and subsequently in the distribution of vaccines saw Africa confined to the peripheries of global supply chains (Kirby, 2020). Similar to past experiences, lifesaving equipment could only be accessed by SSA countries long after they were made available in Europe and North America (Musa et al., 2020). International coordination and support is therefore critical to strengthening SSA health systems.
Post COVID-19 Recovery Challenges
The exacerbation of the economic impacts of the pandemic decreased regional growth to –2% by the end of 2020, thereby pushing SSA into its first recession in 25 years (Toure, 2020; World Bank, 2021). South Africa and Angola, which are SSA’s second and third largest economies, respectively, experienced an economic contraction of 7% and 4%, respectively, in 2020. SSA’s largest economy in terms of nominal GDP, Nigeria, also experienced a contraction in its GDP by 6.1%, the worst in more than a decade. According to a study by Mennechet and Dzomo (2020), the economic impact of COVID-19 in SSA erased at least five years of progress in fighting poverty by driving approximately 40 million people into abject poverty by the end of 2020. A report by the World Bank estimated that SSA needed an emergency economic stimulus of USD 100 billion that included USD 44 billion for interest waiver. The Bank estimated that SSA lost between USD 37 billion and USD 79 billion in economic output in 2020 (Ataguba, 2020; Stiglitz & Rashid, 2020, 2020).
In light of these far-reaching economic impacts, some economists and policy analysts advocated for market-based policy arrangement response mechanisms that could initiate aggregate action clauses for one-to-two-year freezes on both principal and interest amounts of all external government debt repayments (Gelpern et al., 2020). Some members of the G20 responded to these policy suggestions and announced debt relief packages for the poorest countries, most of which are found in SSA. The World Bank and the International Monetary Fund (IMF) issued official statements that encouraged bilateral lenders to suspend debt payments (Gilbert et al., 2020). Importantly, these international development institutions reiterated their commitment to offer their ideas for policy advice and financial assistance to many SSA countries during and in post-COVID-19 recovery (World Bank, 2020). For instance, by June 2020, IMF postponed debt payment for 27 poorest countries from April 2020 to October 2021.
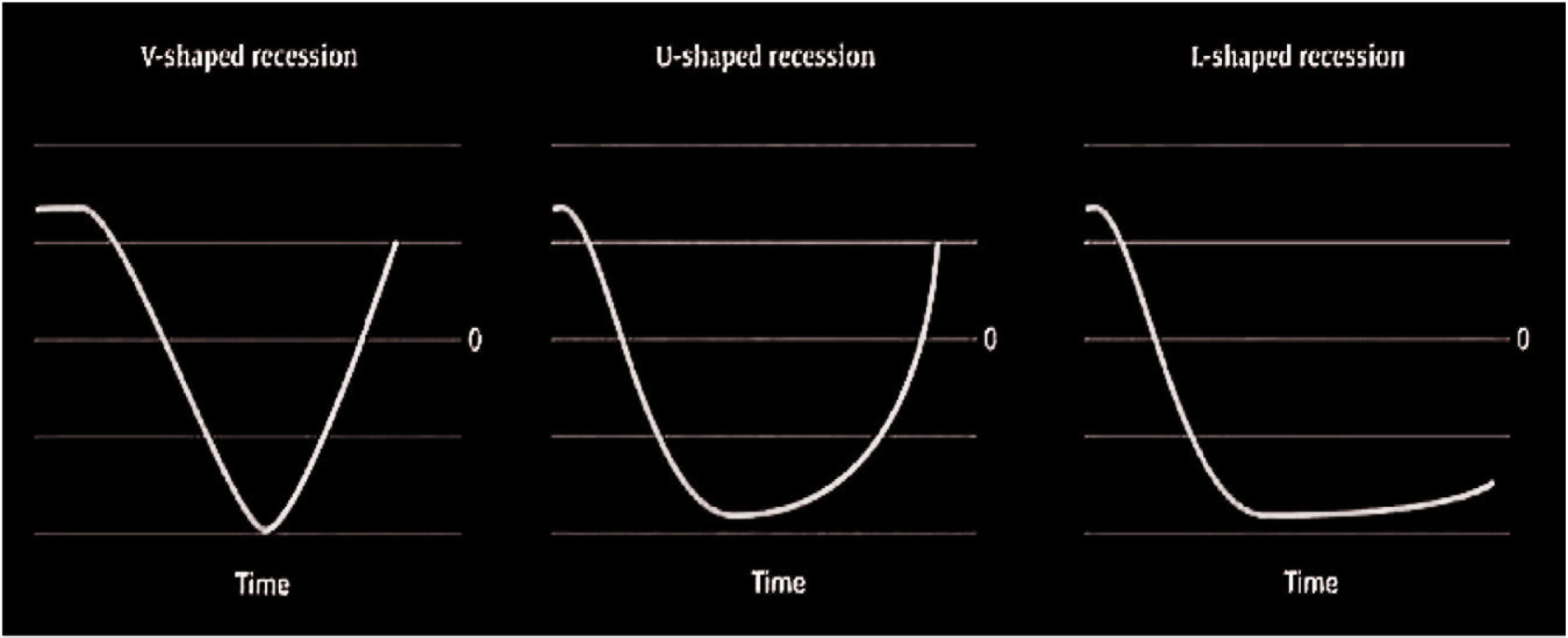
That said, some economists predicted that SSA would experience an L-shaped post-COVID-19 economic recovery (Dagba et al., 2021). This is the worst-case economic scenario in which economic growth declines and does not recover for years. Although growth may be recorded within a few financial quarters, recovery to the pre-recession levels may take longer. Yet, this prediction was made when the overarching perception was that SSA would be ravaged by COVID-19 and that the impact on employment, income, health, tourism, and economic growth would be unprecedented. Other models such as W-shaped were predicted if new waves of infections emerged after containing the first wave; V-shape as the best scenario could be experienced if economies would rebound as quick as it had declined after a successful campaign to manage the pandemic; and, a U-shape if a long period of time was recorded between the phases of economic decline and recovery. Figure 1 shows the post-COVID-19 recessionary recovery scenarios.
While developed countries were projected to have V- and U-shaped recovery in the short run, developing regions such as SSA were projected to have an L-shaped recovery in the long run. For instance, in Nigeria, the decline of global oil prices from an average of USD 70 per barrel at the beginning of the year to historic lows of USD 18 per barrel by March 2020 compelled the government to devalue the naira by 15% (Ataguba, 2020). Low oil prices were also projected to have a significant impact on Angola and Algeria, the region’s second and third largest oil producers, respectively. In Angola, where oil accounts for 90% of total export revenues, the value of oil exports fell by nearly 50% between April and May, while in Algeria, where oil accounts for 90% of total export revenue and funds 60% of the budget, the government announced in May that it would cut the 2020 national budget by 50% (Oxford Business Group, 2020).
The International Labour Organization (ILO) also reported that 22 million full-time employees would be unemployed by the end of 2020 in the continent (ILO, 2020). Forecasts for Nigeria suggested that the unemployment rate could rise to 33.6% (39.4 million) during a similar period. Small and medium enterprises risked complete collapse and could further undermine economic recovery. Democratic Republic of the Congo was also projected to have an unemployment rate of 36%, whereas South Africa recorded an unemployment rate of 28%. The unemployment rate in Kenya, Tanzania, Egypt, Ghana, and Niger were 10%, 8%, 7.3%, 2.1%, and 0.5%, respectively. These projections were predicted to affect SSA countries’ recovery plans (ILO, 2020).
The pandemic also affected the stock and financial markets. Major stocks such as KCB Group and Safaricom in Kenya declined by 7% and 5.4%, respectively, on the first day the country recorded its first case of COVID-19. The Nairobi Stock Exchange had to be suspended on the second day due to continuous plunge of stocks (Ozili, 2020). The tourism industry emerged as one of the most affected economic sectors. In South Africa, tourism fell by nearly 80%, whereas Kenya experienced a sharp decline in foreign tourists by about 55% due to the emergence of COVID-19. The pandemic shut down tourist attraction destinations (Rogerson & Baum, 2020), ranging from the safari lodges across southern and eastern Africa, the sensational castles and forts in Ghana, the motionless cable cars at Cape Town’s Table Mountain, among others.
The health sector cannot be left out in the discussion of post-COVID-19 recovery challenges. According to a study by Hogan et al. (2020), the pandemic caused considerable disturbances to the region’s health services because of several endemic and epidemiological problems. By focusing on the management of COVID-19, existing response mechanisms and gains made in combating other diseases such as malaria, tuberculosis, and HIV could be at risk of getting lesser attention, thereby limiting the usual programmatic activities. Hogan et al. (2020) contended that in a high-burden setting like the COVID-19 pandemic, deaths due to malaria, tuberculosis, and HIV could rise by up to 10%, 20%, and 36% over five years, respectively. For HIV, the most significant impact was assessed to be from interference in antiretroviral treatment, which could happen in times of high demand on health systems. For tuberculosis, the most significant impact was projected to be from the decline in treatment of new cases and timely diagnosis because of the prolonged period of post-COVID-19 recovery. Lastly, for malaria, the most significant impact could be an outcome of interference in the region’s planned net campaigns. As a consequence, these disturbances could result in loss of the gains made in the war against these disease epidemics in SSA.
An additional challenge that the region faced was the closure of schools particularly in the absence of alternative frameworks for learning such as robust access of online platforms that both teachers and students could use to limit the impact of the pandemic on education (Ozili, 2020). Governments of many countries in the SSA region temporarily shut down all institutions of learning. The governments of Kenya, South Africa, Ghana, Nigeria, Ethiopia, Rwanda, amongst others, announced the closure of all schools across the country and banned all public gatherings. As many countries continued to battle with the second and third waves of COVID-19, many institutions of learning remained completely closed or partially open by April 2021. The UN Educational, Scientific and Cultural Organization (UNESCO) recommended the use of online educational platforms for both students and teachers; yet, many countries in SSA lacked the necessary infrastructure and equipment to implement such programs.
Ways SSA Can Respond to the Impacts of the Pandemic
The COVID-19 pandemic had a great impact on societies across the continent; yet, despite the challenges, it also influenced the need for new discourses on how SSA governments can transform the challenges into new opportunities to drive the continent forward. Given the global and novel nature of the pandemic, no single government could be able to address its impacts without effective collaboration. Due to the weakened regional and global economic growth, SSA experienced a deep impact on trade with external partners and within the region. It is therefore imperative that the region seizes the opportunity to engage in collaboration and exploits its scale and potential capabilities to speed up the implementation of economic partnerships such as the AfCFTA. The harmonization of trade policies will have a great impact on strengthening intra-African commerce, increase the competitiveness of African goods and services, establish global export opportunities, and open up new market frontiers within the region. These processes will also facilitate the region in reconfiguring the pattern of global value chains. Indeed, the experience of the pandemic exposed the limitations that SSA faces by being overdependent on few global economic regions for the supply of certain goods and services. The region must therefore use post-COVID-19 recovery opportunity to pursue greater ambitions of more self-reliance such that the region becomes both a consumer and a producer of goods and services. This will not only support local economies, but also create significant employment opportunities.
SSA must also embrace digital technologies in its post-COVID-19 recovery agenda. The “Africa rising” narrative that had dominated the first two decades of the twenty-first century was also exposed during the pandemic as skewed. This is because the unprecedented economic growth experienced in the region was largely in relation to the GDP, which is in itself one dimensional. This economic growth had not generated social inclusion, and its benefits have largely failed to capture the demographic dynamics of the region such as its youthful population who continue to face high rates of unemployment and poverty. To address the myriad of challenges facing SSA, it is important that the region embraced digital technology by providing adequate investment on digital infrastructure. Digital technology emerged at the tip of the COVID-19 response both from a health perspective and also by managing the socioeconomic crisis by enabling the continuity of business, education, communication, and access to justice through digital courts. Despite the increasing relevance of technology, Africa continues to lag behind with only approximately 28% of the continent’s population able to access reliable internet.
Several health experts highlighted that the best defense against the COVID-19 virus was achieving herd immunity. In other words, that majority of the population will have to be vaccinated. This emphasizes the importance of acquisition of COVID-19 vaccines. Remarkable achievements were made in parts of the development of vaccines as a result of decisive investments, commitment of scientists from different parts of the world, and the sacrifices and risks of volunteers who were used as human test subjects for the vaccines. But challenges in the supply of vaccines created a new problem of vaccine nationalism. According to a study by Katz et al. (2021), the rate of global daily vaccination estimated at 6.7 million doses by April 2021 could translate to the achievement of the recommended heard immunity of 70%–80% of the global population in approximately 4.6 years, that is, by 2025. The concerns about access to vaccines influenced states to compete, and this created inequalities, especially for the developing and poor States who either lacked the necessary expertise to conduct effective vaccination programs or access to vaccines. Cognizant of these challenges, it is fundamental that Africa strengthens its response mechanisms through coordinated regional and continental collaboration. Critical institutions such as national public health institutes, leading private health research institutions, the A-CDC, ministries of health, African Union (AU) Commission, Africa Medical Supplies Platform, and the Africa Taskforce for COVID-19 Preparedness and Response need to operate in a well-coordinated framework to ensure that testing, supply of critical medical equipment, and access to vaccines can be achieved not only during the pandemic, but also develop capacity for future response to health pandemics.
It is critical for the continent to address the emerging debt crisis. Even before the outbreak of the pandemic, there were growing alarms over the rising public debts incurred by SSA governments. Governments of Kenya, Ethiopia, and Angola had, for instance, been involved in the implementation of debt-driven mega infrastructural development such as ports, highways, dams, railways, bridges, and airports. Many of these projects were funded by nonconcessional loans, that is, loans from commercial markets that attach higher interest rates than alternative funding from international multilateral institutions such as the World Bank and IMF. Perhaps this preference is due to attempts by SSA governments to avoid the conditionalities that are often attached to concessional funding by the World Bank and IMF. The need to avail emergency funding increased levels of public debts because of additional expenditure that was needed to mitigate economic fallout by offering financial support to households, businesses, and purchase of additional emergency medical equipment (Dickson & Yao, 2020). According to a report by the African Development Bank, by March 2021, the continent owed USD 546 billion in external debt—equivalent to 25% of its GDP and slightly above its annual revenue of USD 501 billion. In countries such as Kenya, out of the USD 15 billion that was projected as total revenue collection for the 2020/2021 financial year, USD 8.5 billion was to be channeled toward the repayment of public debts approximated at USD 58 billion (World Bank, 2020). Whereas countries such as South Sudan, Somalia, and Mozambique were already past the levels of debt distress by 2020, others such as Ethiopia, Ghana, Zambia, Malawi, Chad, Togo, and Cape Verde were categorized as exposed to debt distress because of shorter maturity of debts, depreciation in currency exchange rates, rising interests on public debt, and expanded budgetary deficits. Responding to these debt concerns therefore necessitate SSA governments to engage in collective debt repayment relief negotiations with international financial institutions such as the World Bank, IMF, and leading bilateral lenders such as China during the post-COVID-19 recovery phase. This would create the necessary fiscal space required to cushion states from the economic impacts of the pandemic and reposition the region back into sustainable economic recovery.
Increased funding for the public health sector should be taken up as a matter of priority. Even though SSA has been exposed to various disease pandemics such as Ebola and Zika viruses in the past, COVID-19 perhaps had the biggest impact on SSA’s fragile healthcare systems. This fragility was the outcome of the systematic failure of African governments to adequately invest in the healthcare system. In 2001, AU member states pledged in the Abuja Declaration to increase budgetary allocations by at least 15% of annual government budget on the health sector (Zimano, 2020). However, an appraisal report of the Declaration, a decade later, revealed that only one state achieved this target, whereas 11 states reduced the expenditure. The treatment and management costs associated with the COVID-19 offered important lessons on why governments need to significantly increase investments in the healthcare system. Not only was the cost outside the reach of many African households, but also accessing the health facilities with appropriate health equipment and staffing became a huge challenge. Although COVID-19 was the most immediate challenge, the region still grappled with other diseases such as HIV/AIDS, malaria, tuberculosis, episodes of Ebola outbreaks, and a huge challenge of water and sanitation. The experience of COVID-19 should mark a new step in solidifying the urgency in which SSA addresses its approach to the management of these diseases as well as sanitation. As population continues to expand and consumption of water increases in the midst of climate change induced droughts, more effort is needed to make clean water accessible to communities. In other words, ensuring and promoting continuous prevention and treatment of other diseases as well as more investments in water and sanitation is critical to the mitigation of COVID-19 and any other future outbreak of viruses.
Last but not least, there is an urgent need for the continent to have a radical economic transformation. The continent already has an existing mini-vision 2030 and AU’s Agenda 2063. To embark on this path in the post-COVID-19 era, African governments must come up with new programs and initiatives that can thrust the continent back into not only robust, but also inclusive economic growth (Maulani & Agwanda, 2020). As discussed previously, in addition to containing the ballooning public debt problem, there will be the need for governments to find other innovative ways to mobilize resources and establish ways that can facilitate employment intensive growth both in the public and private sectors. This will not only address the issue of rising unemployment rates, but also expand the government tax base (Black, 2016). Economic sectors such as agriculture will require more support in order to ensure food security. SSA governments must therefore begin thinking about developing agricultural friendly policies to increase production especially during pandemics. The existence of the AfCFTA creates a viable platform through which African governments can exploit further to strengthen the continent’s manufacturing capacity and easier technology transfer from one end of the continent to the other. But the pandemic has also created new multistakeholder platforms, linking business-to-businesses, governments, civil societies, and international development partners. These new stakeholder platforms should be cultivated into new avenues in post-COVID-19 era that will drive economic transformation across the continent.
Conclusion
The aim of this article was to contribute to the growing number of studies on the impact of COVID-19 in the world. Although several studies have focused on the direct impact of the pandemic on the health sectors of countries across the world, few have sought to examine the different constraints states are facing during and after the pandemic. This article looked at the experience of COVID-19 in Africa beyond the number of infections and discussed the challenges the continent has faced in dealing with the disease in three stages. In the first stage, the continent struggled to stop the disease from coming into the continent partly due to slow response in locking down its borders, an act that has proven very effective in territories such as Macau, but also the failure of contact tracing in the continent. Once local transmission overwhelmed the prevention strategy, most countries in the continent turned to containment efforts. These efforts exposed the existing socioeconomic inequalities as different segments of the societies faced different challenges amid the containment polices such lockdown, curfew, and cessation of movement to and from different parts of the countries. The most affected segments of the societies are those who have historically experienced marginalization and hail from low-income backgrounds. Challenges with the provision of healthcare services and support quickly became visible, though efforts adopted by most of the government are indeed commendable, and nearly 12 months into the pandemic, the continent has not experienced a big loss in lives compared to other continents. However, while the impact on health has been low, postpandemic recovery could have a devastating impact on the continent if adequate measures are not taken in advance. This article has therefore provided a number of policies for consideration by African governments.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author received no financial support for the research, authorship and/or publication of this article.