
Abstract
This qualitative study explores how a small group of young adult South Africans discursively construct health during in-depth semi-structured interviews, and the ways in which these discourses are used to construct subjectivity. Data was collected from 20 mostly white, university educated participants and were analysed using Foucauldian discourse analysis. One of the discourses identified, ‘health and work’, is discussed with a specific focus on the construction of subject positions and the possible implications these have. We explore the personal implications of how the use of ‘health and work’ discourses construct participants as in alignment with moral norms. However, we also argue that these discourses individualise the responsibility for (ill)health and deploy the association between good health and virtue to perpetuate capitalist notions of the work ethic and neoliberal ideologies which are implicated in the perpetuation of health inequities.
Introduction
To work is good, not to work is evil. (Bauman, 2005: 5)
Health and employment are two of the South African government's key focus areas. This national emphasis on health and work, as well as globalised norms which idealise both, play a significant role in shaping how young adult South Africans talk about health, and how they construct their identities. This article explores how discourses of work underpin constructions of health among 20 young South African adults living in urban areas. The implications of these discourses for subjectivity as well as the socio-economic structures which both facilitate and are reproduced through ‘health and work’ discourses are explored. Constructions of the hard worker are discussed and critiqued in relation to dominant discourses of health idealising productivity and individualism. These discourses function to reproduce an unjust and unequal status quo through the reinforcement of the virtue of work (Beder, 2000) and the moralisation of health.
Here, health, work and moralism become intricately intertwined as individuals negotiate their sense of self in an increasingly globalised context. This article argues that economic interests play a role in structuring health discourse and subjectivities which then function to reproduce capitalist systems which are responsible for many health inequities. By deconstructing this process, this analysis aims to reveal concealed ‘regimes of power and knowledge’ and highlight the ways in which discourses ‘at the micro level of language’ are intimately connected with ‘macro level institutions’ (Kramer, 2019: 236).
Background
In this section we will provide a broad overview of some of the historic, economic and contextual factors that shape the South African health context. More specifically we will explore how neoliberalism emerged in South Africa and how this relates to South Africa's complex health landscape. We then explore the key concepts of healthism and the work-ethic which emerge from a neoliberal context and shape and are reproduced within the discourses discussed in this analysis.
We begin with a brief discussion of the macroeconomic changes that occurred during South Africa's transition to democracy. Ornellas et al. (2017: 537) summarises these shifts, highlighting the pressure the IMF, the World Bank, and the media placed on South Africa to redirect their economic strategy towards: … one that would emphasize private sector growth, cutting down of state deficits, controlling inflation, imposing wage restraints, and recognizing the superiority of the market over state regulatory and redistributive interventions… [and further] policy changes based on neoliberal ideals, such as that of increasing privatization, thereby isolating the poor from necessary services.
Neoliberal economies tend to be characterized by cuts in welfare spending and the implementation of austerity measures. South African health care spending has stagnated since 2012 (Blecher et al., 2017) and this, in combination with the high levels of inequality, has meant that many of the health care problems associated with neoliberal austerity measures are faced here (Moult and Müller, 2017). These include issues like the under-resourced public health system, the increased reliance on privatized health care, a decrease in available services, and increased waiting times. In addition, ‘neoliberalism, as an ideology that holds market exchange and economic rationalism as ethics in themselves, and as being capable of acting as a guide for all human action, has seeped into public service provision in South Africa as much as elsewhere internationally’ (Harvey, 2000; Moult and Müller, 2017: 219).
In contrast, the South African government often emphasizes the importance of health care for all, pointing out that South Africa's constitution protects the right of all citizens to health care services and has proposed a plan for a National Health Insurance (NHI) system which aims to ensure Universal Health Care (Blecher et al., 2017). On the surface then, it appears that the South African government is committed to promoting a collectivist attitude to addressing health problems and improving citizens’ health status. However, a number of factors undermine this effort to acknowledge the social and structural determinants of health and complicate the context in which South Africans seek to make sense of health. These include extremely high levels of inequality in the country which have resulted in a ‘two-tier’ health care system where those who can afford it purchase private medical aid schemes and make use of private healthcare services. Those who cannot make use of the often understaffed and under resourced state health care system (Moult and Müller, 2017).
The rise of neoliberal capitalism in the West has increasingly shifted the responsibility for health from the state to individual citizens (Kennedy and Markula, 2011). This means that they are responsible for taking various preventative actions to avoid disease (Petersen and Lupton, 1996) but also for overcoming disease. This shift is particularly noticeable in the USA, however, individualistic forms of sense making are also present in South Africa (Zici et al., 2021). While there are also collectivist understandings of the self and strong ties between some social groups in South Africa, this is being undermined by the economic and social consequences of macroeconomic decisions, described above. In addition, individualising behaviour change interventions can be seen in public health approaches to addressing the HIV/AIDS pandemic in South Africa (Gilbert, 2012) as well as interventions addressing obesity and smoking which function to construct health as an individual problem. Individualising health discourses have also been observed within South African health media (Samaai, 2022) and within the personal understandings of health and the body among South African middle-class women (Campbell, 2017).
The following sections explore two important social constructs which have become dominant within individualistic neoliberal societies namely the work-ethic and healthism. Both of these constructs emphasise individual responsibility for one's success and choices but they also both idealise and moralise work and health respectively. Aligning oneself with these ideals enables individuals to demonstrate their desirability in accordance with neoliberal standards of self-sufficiency. A brief explanation of both constructs is presented followed by an exploration of how they are relevant within a South African context.
The work ethic
The work ethic refers to the value assigned to work as an end in itself and the understanding that working hard is a virtue, indicative of moral worth (Weber, 1967). The idealisation of the work ethic coincided with the rise of capitalism and provided a conducive environment for the promulgation of capitalism as a system of trade and commerce. It also provided moral legitimacy for the zealous pursuit of profit and growth (Beder, 2000). Lafargue (1907) and Beder (2000) have critiqued the unquestioned value placed on work as an end in itself and as the only way of achieving self-fulfilment. Beder (2000) argues that the work ethic is central to the power wielded over societies by corporations. The belief underlying the work ethic is the idea that society is fair and that inequalities are the result of individual differentials in discipline and commitment in relation to work. This means that attention is diverted from the structural privileges and disadvantages awarded to different groups (Beder, 2000). By constructing healthiness as linked up with the work ethic, inequalities in health status are also implicitly constructed as individually earned, rather than structurally maintained.
The work ethic in South Africa
There has also been some interesting discussion on the culture of work/ work ethic in South Africa. For example, Lawhon et al. (2018) describe the promulgation of the work ethic in a South African working-class context of mass unemployment and limited job opportunities where newer forms of the work ethic including ‘entrepreneurialism’ are perpetuated. Some studies which were identified, reproduce the discourses being critiqued in this article and idealise individualistic notions of hard work and economic growth as ends in themselves. For example, an article comparing the work ethic of South African and Chinese workers argues that a significant problem exists in the South African work force as they are deemed to be insufficiently motivated to work hard which has resulted in low productivity, largely related to labour strikes (Slabbert and Ukpere, 2011).
Other articles, however, present a critical perspective, outlining some of the problematic consequences of the perpetuation of the work ethic. Hirshberg and Ford (2001: 65) argue that the prevalence of belief in the work ethic can contribute to ‘tendencies to attribute poverty to the deficiencies of the poor and not society, which yield negative attitudes toward government assistance’. Similar findings which link beliefs in the Protestant work ethic to negative attitudes towards disadvantaged groups and a disapproval of social welfare programmes have been noted by many other researchers (Furnham, 1982; Rosenthal et al., 2011). This was also demonstrated within a South African context in Barchiesi's work which highlights the resistance to social protections and redistributive grants due to the feared threat of these measures to the work ethic of South African citizens. He also describes examples of management views where reduced employment security and regulation were believed to foster a strong work ethic which they felt to be lacking. As a result, as Beder (2000) argues, the work ethic functions to bolster and reproduce capitalist systems which, in their current forms, often underlie a number of health inequities.
Finally, Wale and Foster’s (2007: 52) discussion of wealthy white South Africans and privilege, focused on the notion of the work ethic, poverty, and morality. They identified that prominent discourses of poverty reinforced: the notion that the wealthy get jobs based on the fact that they are hard workers, and hard workers are morally good people; therefore, the wealthy are morally good people deserving of their wealth. In opposition the poor are poor because they are lazy sinners.
This moralisation of work, and how its linked to healthism will be discussed in the next section.
The moralisation of health
In 1980, Crawford coined the term ‘healthism’ which refers to the increasing moralisation of health that has occurred in some societies. It has been argued that health, which was previously confined to the area of biology and disease, has permeated into almost all aspects of life (Metzl, 2010). Crawford (2006) attributes this to the advancement of the ‘holism’ discourse of health and the increasing popularity of ideas relating to mind-over-matter health practices and effects. Crawford (2006: 411) argues that holistic versions of individual responsibility are, ‘among the most repugnant’ as the punishment for failing to achieve health, which in this case has become increasingly broad, encompassing most aspects of life, is even greater as not only do individuals deserve to be ill, but they are also understood as wanting to be ill. As a result, health comes to be viewed as a moral imperative and an essential aspect of both self-worth and social status (Metzl, 2010).
Research on health and morality in South Africa has mostly focused on the stigma attached to certain illnesses, the effects that this stigma can have on illness experiences and access and adherence to treatment. The stigma of illness in South Africa, particularly in relation to HIV but also more recently to obesity (Henry and Kollamparambil, 2017) and diabetes (Mendenhall and Norris, 2015) mean that being ill (in certain ways) can, in some situations, be constructed as an indication of individual moral failing. Moralising health plays a role in legitimating this stigma and obfuscating the social and structural determinants of health inequities (Crawford, 2006). Many other researchers have found similar associations between the construction of good health as deserved and neoliberal ideologies which legitimate inequality (Lebesco, 2011; Luna, 2019).
Here, it is important to highlight that individuals do not uncritically absorb and reproduce dominant discourses or neoliberal ways of being, in isolation. Instead, we acknowledge the multiple and contradictory discourses which participants use to make sense of their health and themselves. This article focuses on how some of these broader ideas appear within the speech of different participants and illustrates how these specific utterances form part of these broader structures (Willig, 2013).
Theoretical framework
This study drew on a social constructionist theoretical framework. This approach is based on the understanding that reality, knowledge and the self are all socially constructed through language and within social interactions (Burr, 2019). Foucault's (1972) work on discourse discusses how language and power constitute meaning. Discourses are seen to both facilitate and legitimate this use of power and can challenge the dominant power structures. The dominant discourses in our cultures are usually intertwined with the institutions of our societies and they serve to support and sustain one another (Foucault, 1972). Of particular relevance to the current article is Foucault's conceptualisation of subjectivity. Foucault's writing on the construction of the self, along with Rose's (1998) exploration of the subject based on Foucault's work, were drawn on to frame the study.
Foucault (1988) views the self as constructed through social, historical and discursive processes. In his later work, he becomes increasingly interested in, ‘the kind of relationship you ought to have with yourself… which determines how the individual is supposed to constitute himself as a moral subject of his own actions’ (Foucault, 1983: 340). He describes four aspects of this relationship, one of which focuses on what we do to work on and change ourselves to behave ethically- the ‘self-forming activity’ (Foucault, 1983: 355). Foucault's notion of ‘technologies of the self’ further explores the active elements of the process through which subjects are constituted. Foucault (1988: 18) defines technologies of the self as those which, permit individuals to effect by their own means or with the help of others a certain number of operations on their own bodies and souls, thoughts, conduct, and way of being, so as to transform themselves in order to attain a certain state of happiness, purity, wisdom, perfection, or immortality.
Foucault's ideas on the role of the relationship to oneself in the constitution of subjectivity has been taken up by Rose (1998) to explore the social construction of the individual, particularly within neoliberal contexts. Rose (1998) argues that the form of power at work within these practices are governed by a ‘reflexive hermeneutics’. Individuals are trained to develop a style of thinking about and reflecting on the adequacy of one's alignment to a set of moral norms. These reflections are then translated into actions of various kinds aimed towards self-improvement. Different discourses construct subjects which are viewed as ideal in certain societies at certain historical moments and are shaped by and shape the societies in which they come to be constituted. This understanding of the active (although not necessarily conscious) construction of the self through the taking up and resisting of different discourses underpins the analysis presented in this article.
Methodology
This research was based on a broader qualitative study which explored how a small group of young South Africans discursively constructed health. This study was an exploratory, discourse analytic study aiming to unpack the varied and multiple discourses participants use in relation to health and healthiness.
The study sample was comprised of 20 young South African adults. Participants were recruited using purposive and snowball sampling from the researcher's own professional and social networks. Participants ranged in age from 18- 35. All had at least a secondary level of education and many had advanced degrees or were pursuing tertiary studies. The characteristics of the participants including, gender, race, and occupation are depicted in Table 1.
Participant demographics.
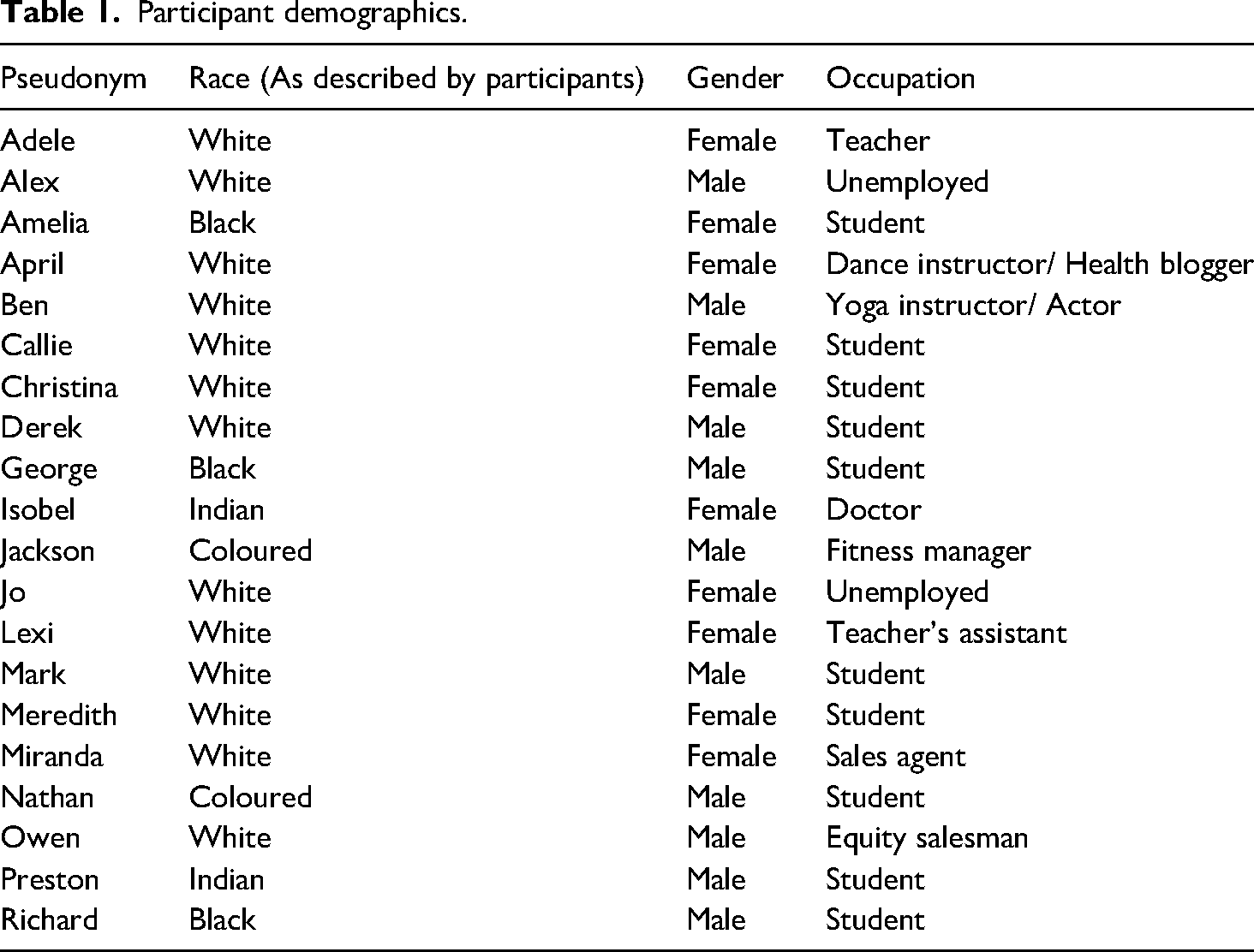
In addition, all participants described themselves as ‘healthy’ at the time of the interviews, which occurred pre-Covid. By studying how those who described themselves as being in good health make sense of the concept of health, we are able to unpack why some health discourses are appealing and how they take root and become pervasive. This then allows us to unravel some of the potential implications of these dominant discourses, not only for this group of participants, but also for society more broadly. It also allows for an exploration of how certain discourses may be reproducing systems of privilege and inequality and by making these links we can begin to imagine new ways of constructing health that build towards more equitable societies (Parker, 1992). This, however, means that the results discussed in this paper may not reflect how those located in other social categories or those who are ill construct the concept of health or take up health discourses to construct their identities.
Another limitation related to the sample is that the composition of the sample was not racially and economically homogenous. While specific information on household income was not collected, some participants (based on their descriptions of their lifestyles) appeared to come from the upper middle-class bracket, lived in suburban areas and had access to discretionary income. However, a few participants came from urban township areas which are generally categorised as low-income neighbourhoods. This means that the sample is not representative of a homogenous social context and the article, therefore, only presents some of the broad macro, but not meso or micro, level contextual factors which may be relevant to participants. In addition, the findings cannot be generalised but instead are indicative of some broad trends.
Individual, in-depth, semi-structured interviews were conducted and ranged in length from approximately 30 to 90 min. The intention of the interviews was to allow participants to talk about their experiences with, and understandings of, health. All interviews were transcribed verbatim and transcriptions were analysed using a Foucauldian method of discourse analysis based on Willig's (2013) steps. This approach provides clear guidelines on how to identify discourses and explore their personal and social implications. It was most appropriate for this study as it has a specific focus on subjectivity. The following section briefly outlines the six steps and how they were applied in this study.
During the first stage, Discursive Constructions, the discursive object was identified in all transcripts. In this case, all references to health were noted. During the second stage, Discourses, the different constructions of the discursive object are located within wider discourses (Willig, 2013). For example, in this study, the construction of ‘health as work’ can be situated within a wider discourse of individual responsibility. In stage 3, Action Orientation, the function of discussing the discursive object in certain ways was considered. Questions such as ‘To what extent do they fulfil functions such as assign responsibility or promote one version of events over another? How do they position the speaker within the moral order invoked by the construction?’ were explored (Willig, 2013: 120). In other words, in this step we considered what the participants gain by constructing health using different discourses at particular times. Stage 4, Positioning, involves looking at the subject positions offered up by different discourses (Willig, 2013). Here, we identified the responsible citizen and healthy hard-worker as subject positions available to participants. During stage 5, Practice, the actions that were made possible through the use of different discourses were explored. For example, behaviours such as smoking weed, exercising, eating chocolate etc. were made available (or not) through the use of the ‘health and work’ discourses. In stage 6, Subjectivity, the potential consequences, specifically in terms of emotions and experiences, of taking up certain subject positions were explored (Willig, 2013).
This stage in the analysis is, of necessity, the most speculative. This is because here we are attempting to make links between the discursive construction used by participants and their implications for subjective experience. Since there is no necessary direct relationship between language and various mental states… we can do no more than to delineate what can be felt, thought and experienced from within various subject positions. (Willig, 2013: 136, Emphasis in original)
In this analysis, implications for subjective experience included, for example, the protection of a positive self-image and maintaining a sense of control.
This paper focuses specifically on one (‘Health and work’) of seven discourses identified through the analysis and how participants used this discourse to construct what it means to be healthy. More specifically, the focus of the article is on understanding the implications of the discourses implicit within the participants speech.
Results and discussion
This section will discuss one of the discourses identified from the interviews with participants: ‘Health and work’. It is important to note, that while participants were not asked specifically about work in the interviews (which focused on their understandings and experiences of health and healthy lifestyles), all participants made various references to work in their discussions. Within this discourse health and work were inextricably linked and mutually reinforced as ideals. This discourse manifested in two ways: ‘Health enables hard work’ and ‘Health as hard work’. Firstly, health was seen as essential in order to facilitate work (most often discussed in the sense of formal, paid labour) and, secondly, being healthy was understood as requiring sustained effort- it was a type of work. Examples of how these discourses came through in participants’ speech will be presented, followed by an exploration of how these discourses functioned within our conversations, and the implications they had for subjectivity. Two subject positions: the healthy hard worker and the responsible citizen were made available through the use of these discourses, which will be explored further. Furthermore, how these discourses are linked to and reproduce broader discourses such as healthism and the work ethic is discussed.
Health enables hard work
The discussion below addresses the construction of health in relation to dominant ideals surrounding productivity. Participants emphasised the idea that being healthy was necessary in order to have the option to work, and work was implied to be essential to individual and social functioning and critical to overall well-being. Ill-health was constructed as restricting productivity while good health ensured that individuals were free to work efficiently and without hindrance. The quotes below explicitly mentioned the importance of health in allowing individuals the opportunity to work. Ben: I definitely feel slow and sluggish [when feeling a bit unhealthy] and I notice it specifically in my work then that starts to fade. Christina: When you are healthy with like your body and your mind and in everything… you go out and do things to work harder to go the extra mile…a lot of jobs are reliant on you being well and I think, so to provide for yourself and to provide for your family you actually need to be in optimal situation so you can retain your job. It sounds so depressing. But unfortunately, it's the way that the world works now.
Here, participants link health with energy and activity, and this was seen as essential for them to fully participate in the ‘working world’. The above quotes show how discourses framing health as important for productivity are internalised by different participants and reproduced in their constructions of health and illness. It is interesting to note the affective difference in the tone participants used when constructing health in this way, both between participants and by the same participant at different points in the interview. Christina, initially constructs an aspirational notion of healthiness which allows you to be and achieve more. However, later in the interview she describes healthiness as necessary in order to avoid the negative consequences of not being sufficiently productive i.e., not being able to ‘retain your job’ and ‘provide for your family’. She also describes this situation as ‘depressing’ but is resigned to trying to work within the system as best as she can. The contrast between these demonstrates how constructing health in this way can be experienced as motivating, but also restrictive and disheartening. In other words, from this framing, maintaining health can allow individuals to perceive a degree of control over their employment status but, simultaneously, the prospect of ill-health is constructed as a constant threat to one's employability.
This discourse, ‘health enables hard work’, can be linked to other discourses participants drew on during the interviews which constructed dependency on others as problematic and idealised independence. By emphasising the importance of maintaining their health as a means of ensuring that one could go to work, participants could take up the subject position of responsible citizen who contributes to society and is not dependent on others for financial security. This in turn also reinforces the idealisation of work itself. These ideas can be situated within broader national and global understandings of the intersections between health and productivity.
More specifically, health has come to be framed as key to economic prosperity (both nationally and personally), and ill-health has come to be constructed as a financial burden. Global health promotion discourses often draw on notions of productivity in relation to health (Petersen and Lupton, 1996). In addition, global efforts to increase health spending have increasingly turned to the ‘return on investment’ discourse where investing in health or ‘human capital’ has been framed as an effective way of improving the economic growth of countries (Sparke, 2016). On the other hand, ill-health is often framed as harmful to economic prosperity. Harvey (2000: 106) argues that within a capitalist society, illness is defined as the ‘inability to go to work’.
In a South African context, poor health is often pointed to as a significant barrier to economic growth and is a key consideration in thinking through ways to enhance international investment in the country (OECD, 2018). National discourse addressing the economy and the productivity of the workforce also often refer to health. One factor which, for many years, has often been presented as partly responsible for South Africa's so-called ‘productivity disaster’ (Jacobs, 2024) is ill-health. Specifically, the HIV/AIDS epidemic and TB are often talked about as negatively affecting businesses by compromising individuals’ ability to go to work regularly and, when there, to work quickly and effectively (Booysen et al., 2003; World Economic Forum, 2008). More broadly, employment in South Africa is highly insecure and large percentages of the population are unemployed (Statistics South Africa, 2019). In this uncertain context, the implications of constructing health as having a significant impact on an individuals’ success or employment status, may be even more pronounced.
A further way in which participants in this study drew on the ‘health enables hard work’ discourse was when justifying behaviours labelled ‘unhealthy’. They explained that if these behaviours are not impairing their productivity then they are not really bad for one's health. In addition, if these behaviours enhance productivity they could be considered healthy for that situation. Miranda: I have one friend who, you know, she smokes weed everyday whenever she can, but she is one of the most highly functional and productive people I’ve ever met! …she was just active all the time, and she says that she has got a lot of you know anxiety issues and if she doesn’t smoke weed um those you know those completely overwhelm her, and that's why she smokes so much weed, it helps keep her calm and less anxious. Whereas if I were to smoke weed all day every day, I would be the most lazy useless person, I would just sit in my room eating and watching series whereas she, that actually helps her handle the hectic pace at which she does things. So, you know something like that- it's hugely different according person to person um but also for some people helps them be more functional whereas with other people it makes them a lot less functional…
Miranda constructs healthiness as being active, calm and focused and having a sense of control over one's mental state and a resilience to respond to ‘the hectic pace’ that is required. By associating good health with these positive traits, healthiness is reproduced as a taken for granted ideal. In contrast, unhealthiness is constructed as undesirable through its associated with, ‘anxiety issues’, ‘overwhelm’ and people who are ‘lazy’ and ‘useless’. Miranda's quote conflates notions of healthiness and notions of functionality thereby reinforcing the idea that health is essential because of its role in supporting productivity as well as the construction of productivity as an ideal. The perceived health status of the friend that she describes is preserved because of her ability to maintain what she describes as an impressive level of productivity even though the behaviour ('smoke weed all day every day’) she engaged in to achieve this functionality could be labelled unhealthy. By introducing the importance of productivity in relation to health, Miranda effectively muddies the distinction between healthy and unhealthy behaviours and may therefore be able to sidestep some of the negative perceptions of certain behaviours as unhealthy, provided that they can be defended in terms of their ability to enhance productive output.
Interestingly, neither her friend's seeming dependence on marijuana nor the perceived excessiveness of the demands being placed on her were identified as problematic. While this discourse may enable individuals to defend against criticisms of certain behaviours, the construction of high levels of productivity as an unquestionable good means that health becomes secondary to productivity. In the quote above we see the two ideals placed in opposition to each other- ill-health (‘anxiety issues’ and ‘overwhelm’) on the one hand and productivity (‘active all the time’ and ‘handle the hectic pace at which she does things’) on the other. In order to resolve the conflict between the two, the health ideal is reconstructed in productivity's terms, further reinforcing the work ethic and prioritising individual adaption.
Beder (2000) argues, the promulgation of the work ethic functions to bolster capitalist systems which idealise individualism and are associated with reduced state spending on social welfare and health. Similarly, Wilson, (2017: 150) discusses how: instead of resisting and transforming the shared structures that condition our everyday lives and make us sick, we are encouraged to engage in individualised and privatised practices of self-care that shut down our critical capacities for social connection and political intervention.
While this discourse may serve participants by, in one sense, lowering the bar for what behaviours are considered healthy, in order to maintain their health status, they now need to prove their productivity which appears just as, if not even more, demanding. In addition, the moralism associated with health is effectively extended to and supports the existing moralisation of hard work which can have a number of stigmatising implications. Lastly, by reorienting the evidence for health towards the level of their work-ethic, the neoliberal discourses which contribute to the production of health inequities are reinforced.
Health as hard work
The second way in which participants linked health and work was through the use of the discourse ‘health as hard work’ where they constructed improving and maintaining an acceptable level of health as requiring the devotion of significant time and effort. Participants frequently described their diligent engagement in the hard work of health when talking about how they tried to stay healthy and the kinds of things it was necessary to do in order to achieve healthiness. Amelia: I do yoga, go to the gym and I try to eat the best and try to eat as healthy as I can. I take care of my health as much as I possibly can. Lexi: You’ve got to be quite disciplined or like persevere to see a change and that's where people often probably give up after a while. Like for me if - I don’t think I’m like massively paranoid about it- but if I notice if I’ve put on a bit of weight, I’d rather just deal with it there and then rather than leave it and then you have to spend like so much longer but ja, I think it's quite difficult for people to like really persevere with like eating healthy, exercising and then also maintain it and not just go- once you’ve lost the weight, not just go back. Richard: because I knew every time I push harder I’m closer to that dream where I’m gonna be in that physical shape. So, I’d be in the gym doing sit ups maybe and then my stomach would pull in a direction it's never pulled before, like it's going to come out, like something's going to come out of my stomach! And I would actually laugh ‘cause I enjoyed that, I enjoyed the pain and I actually understood what they meant by ‘no pain no gain’. So when you feel the pain, you know that something's happening, so when I felt that pain, I was like ‘yeah I’m doing something right’.
From these quotes, health is being constructed as requiring ongoing, sustained effort that relies on behavioural (‘do exercise’, ‘cook a meal’, ‘do yoga’, ‘eat as healthy as I can’, ‘push harder’) and psychological (‘not eat that chocolate’, ‘be quite disciplined’, ‘persevere’) work. Work in this context is constituted as involving pain, discipline, sacrifice and perseverance and demands individuals’ ongoing engagement in challenging activities and denying themselves ease. In their descriptions and explanations of their experiences of health, the participants drew on and reproduced the notion of the work ethic. As Laird (2001: 855) asserts: Throughout the evolution of the work ethic, hard work has been associated with good character and virtue. Work has become the central feature of most people's lives, the source of their self-identity, income, status, and social respectability. It gives them their purpose and provides them with social relations and a structure to their day. In a work-dominated society, happiness must be earned through hard work. The suffering and boredom associated with work is the price one has to pay in order to attain happiness.
The ‘health as hard work’ discourse and its emphasis on the work ethic, may serve individuals by highlighting the effort expended in pursuit of health and focusing less on any specific health outcomes, or physical or other signifiers of good health. The construction of ‘health as hard work’ positions subjects as both healthy and as hard workers in ways which allowed for positive self-perceptions in a context which could be relentlessly and unrealistically demanding. By drawing on ideals of healthiness and a strong work ethic, individuals may be able to protect themselves from criticism against their perceived insufficiencies in relation to both. For example, Lexi's proactive desire to manage her weight, seen above, foregrounds the common social stigma that an increase in weight is associated with laziness. The use of the ‘health as hard work’ discourse at this point, emphasizes her ability to address her weight gain timeously and with ‘discipline’ and ‘[perseverance]’, thereby allowing her to contradict the critical ideas mentioned above.
While the focus here is on effort and sacrifice, Richard also highlighted the benefits of the work he engaged in, ‘I enjoyed that’ and being ‘closer to the dream’. These ideas are also noted in Jo's quotes below. Jo: it's a lot of work doing exercise, it's a lot of work not eating that chocolate it's a lot of work not- having to cook a meal in a certain way to make sure that there's nutrients, but at the same time, once you’ve done all that and once you’ve put in all that work, you really feel the reward. There's a reward for your effort. Jo: people tend to, when they're healthy, they tend to be happier… they tend to be people who are confident in themselves. Probably because they know how much exercise they are putting in or how much work they putting in to their food and eating and things like that, so they tend to be more confident.
Jo constructs this extensive hard work as ‘worth the effort’. In these cases, the rewards seem to come from a sense of pride or satisfaction as a result of the hard work itself and not only from improved health/physical states or anticipated health improvements. Working hard on one's health is constructed as a virtuous pursuit which allows individuals to take up the desirable healthy hard worker subject position. This subject position allows individuals to see themselves as disciplined, restrained, conscientious and strong-willed leading to them being ‘happier’ and ‘more confident’. These findings are similar to those in Luna's (2019) research on American runners who emphasised the physical suffering they often endured as part of their quests for fitness. Wilson (2017) argues how fundamental the kind of self-care the participants in this study described is to the neoliberal social order. She explains that, ‘neoliberal governmentality hinges on biopolitical regimes of self-governmentality- on individual and privatised practices of self-care’ (Wilson, 2017: 151). Here we see how this discourse is producing the subjects necessary to reproduce the social order (Foucault, 1972).
While the use of this discourse may serve participants in various ways, we see some of the stigmatising implications of this discourse in Preston's quote below which describes his views on the causes of unhealthiness: Preston: I think most people know that maintaining good health is important in life. But I think some people are just inherently lazy, and I think we do live in an age where the internet has made so many things so much easier. I can see it from a fundamental point of view, that because of our inherent laziness in this generation, because of how instant everything is, people don’t have the motivation necessarily to do what's best for them, even though they know…
In Preston's quote, unhealthiness is attributed to ‘inherent laziness’ and a lack of ‘motivation’. In his quote, he initially refers to only ‘some people’ as being ‘inherently lazy’- suggesting that some people are inherently better than others. However, later in his quote he makes use of the pronoun ‘our’ when describing ‘inherent laziness’ in this way including himself in the group that he is discussing. As a result, he is able to present himself as not only naturally imbuing morally ideal characteristics in line with the work ethic such as discipline and diligence, he is also able to view himself as one of few who are able to overcome the obstacle of an inherent character flaw in order to improve himself and support his health. His moral superiority is not as a result of some innate characteristics that he has no control over, instead it is as a result of his agency and sovereignty over his personality. By changing his presentation of what he believes to be the cause of individual poor health from the criticism of a problematic group of people to a cultural problem that he too is afflicted with, he is also able to avoid the appearance of being judgmental.
The individualism implicit in all of the quotes which draw on this discourse is especially prominent in this quote. We see similarities here with Wale and Foster's (2007) work on the moralising constructions of wealth and poverty employed by wealthy white South Africans. In their work, it was poverty which was associated with laziness and sinfulness while wealth accumulation was constructed as resulting from moral superiority and a strong work ethic. In the present study, we see ill-health becoming associated with laziness and good health with a strength of character and a dedication to hard work. These constructions individualise the responsibility for health, ignoring the social and structural inequities which play a substantial role in determining health outcomes in South Africa. The ‘health work’ that individuals engage in is also constructed as evidence of a person's moral value. In other words, healthism discourses which associate health with morality are reproduced in a way that positions participants as meeting the demands of a society which values good health and productivity. However, healthism discourses can have a range of stigmatising consequences and when merged with discourses idealising the work ethic as we see in the ‘health and work’ discourses, they serve to further prop up neoliberal capitalist notions of individual responsibility, undermine communitarian ideals, and present a discursive logic where an abdication of the state's responsibility for health is justifiable. In a South African context where the majority of citizen's rely on state funded healthcare, these ideas are particularly concerning.
Conclusion
This article contributes to the literature by demonstrating the application of social constructionism and exploring how globalised capitalist discourses are (re)produced in relation to personal health and subjectivity. This paper shows how participants used ‘health and work’ discourses construct health in a way that reproduced the idealisation of the work ethic and the moralisation of health (healthism). We argue that this individualises the responsibility for (ill)health and perpetuates capitalist notions of the work ethic. The article critically reflects on some of the ways in which participants constructed health, may work to reproduce the neoliberal systems which produce health inequities in the first place. In a South African context of extremely high levels of inequality, the consequences of promoting individualising ideologies which sanction reduced state support are especially pernicious.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding received from the NRF Scholarship for 2013 Innovation Doctoral Scholarship (Grant No 83803) and the South African Research Chair in Health Systems, Complexity and Social Change supported by the South African Research Chair’s Initiative of the Department of Science and Technology and National Research Foundation of South Africa (Grant No. 82769) is hereby acknowledged. Any opinion, finding and conclusion or recommendation expressed in this material is that of the author and the NRF does not accept any liability in this regard.
Author biographies
Michelle De Jong is a social science researcher with a background in psychology and a PhD from Rhodes University Department of Journalism and Media Studies. She currently works as a Senior Lecturer at the School of Public Health at the University of the Western Cape. Research interests include: gender, health and identity, health and consumer culture and respectful care for women and children's health.
Simóne Plüg is a social science researcher with a background in critical social and community psychology. Her research interests include violence, trauma and neglect; health, gendered identities, and inequality; and transformative pedagogies and participatory methodologies.
Anthony Collins in an interdisciplinary social theorist whose work explores violence, trauma, and social justice from perspectives of the global South. They are Honorary Visiting Professor at Rhodes University, Honorary Research Professor at the International Centre of Nonviolence at Durban University of Technology, research fellow at AVReQ Stellenbosch University, and lecturer in Social Inquiry at La Trobe University.