
Abstract
Culturally and Linguistically Diverse (CALD) communities, including children, can face a multitude of barriers when accessing health services. With increased availability of paediatric allied health telehealth services in recent years, uptake of these services by children and their families from CALD communities is not well understood. The aim of this study was to describe the demographic characteristic of families from CALD and non-CALD backgrounds seeking speech pathology or occupational therapy services for their children, determine if telehealth uptake differs between families from CALD and non-CALD backgrounds and between families across different language groups, and identify factors influencing telehealth uptake. Although, rate of telehealth uptake was significantly lower for families of clients from CALD communities, neither CALD status nor language independently influenced uptake of telehealth when a broader range of factors were considered. Contrary to expectations, speech pathology clients were less likely to uptake telehealth services compared to occupational therapy clients. Additionally, where families of clients lived rather than CALD background per se impacted likelihood to uptake telehealth. To ensure equitable access to services for all children and their families, health services need to be mindful of the multiple factors influencing uptake of allied health telehealth services.
Introduction
Allied Health telehealth services have been reported to yield equally effective outcomes to face-to-face allied health services (Speyer et al., 2018; Sutherland et al., 2017). Prior to Coronavirus disease 2019 (COVID-19), much of the research on telehealth uptake and use focused on clients living in rural and remote communities – clients with a need and presumed willingness to access telehealth to avoid extensive travel time associated with face-to-face services (Hines et al., 2019; Speyer et al., 2018). However, drawing on the Framework for Digital Health Equity (Richardson et al., 2022), successful uptake and use of telehealth by clients of all ages, whether living in metropolitan areas or remote communities can be influenced by multiple factors across six domains: biological (e.g. type of health condition) (Carter et al., 2019), behavioural (e.g. willingness to communicate via a screen) (Fong et al., 2025), physical/built environment (e.g. ambience of telehealth space) (Duane et al., 2022), sociocultural environment (e.g. language/s spoken by clients and healthcare provider) (Adepoju et al., 2022; Tang et al., 2024), the health care system (e.g. type of therapies available via telehealth) (Malliaras et al., 2021), and digital environment (e.g. access and ability to use technology for telehealth) (Tang et al., 2024). If telehealth is to be embedded into a health service, it must be accessible and useful for all clients eligible for the service including children and their families.
Historically, people from culturally and linguistically diverse (CALD) communities have been reported to have difficulties accessing healthcare due to factors including language barriers, discrimination, and prejudice (Pham et al., 2021). It is unknown if children and families from CALD communities living in metropolitan areas would accept use of telehealth as a viable means of receiving commonly sought after allied health services, specifically for paediatric speech pathology (SP) and occupational therapy (OT) services (Ciccia et al., 2011; Hines et al., 2019; Ingersoll and Berger, 2015; Langbecker et al., 2019). Our paper explores this issue of the sociocultural environment and telehealth uptake.
Cultural and linguistic diversity: healthcare access, experience, and outcomes
Australia is a culturally diverse country with an estimated CALD population of greater than seven million (Pham et al., 2021). This paper adopts a commonly accepted broad or inclusive definition of CALD populations in Australia, in keeping with the Australian Institute of Health and Welfare (Australian Institute of Health and Welfare, 2025). Specifically, a person from a CALD community may have been born overseas, have a parent who was born overseas, or speak a language other than English at home.
Across literature on healthcare access, experience, and outcomes for people from CALD communities, it is apparent that barriers and challenges exist (Duong and Tran, 2025; Henderson and Kendall, 2011; Tang et al., 2024). For example, CALD communities have been reported to face discrimination, prejudice, and racism from society when accessing healthcare (Pham et al., 2021). Caregivers with limited English have also reported to be less satisfied with their experience of healthcare services for their children compared to caregivers who identify as English proficient (Duong and Tran, 2025). As a group, people from CALD communities have also been reported to be more likely to experience poorer health outcomes compared to individuals from non-CALD communities (Michael et al., 2013). Such experiences are thought to contribute to hesitancy and unwillingness to seek future healthcare services (Henderson and Kendall, 2011).
Telehealth had been embedded as a mode for delivery of health services prior to the COVID-19 pandemic, (e.g. Carter et al., 2019), however, emerging evidence suggests that barriers and challenges continue to exist, as CALD communities have been reported to be less likely to adopt or continue with using telehealth. For instance, adults who identified as African American, Asian, American Indian, Pacific Islander and Hispanic have been reported to be less likely to use telehealth across different healthcare contexts (Adepoju et al., 2022). However, in a study comparing access, readiness, and willingness to engage in allied health telehealth among adults from CALD and non-CALD communities, there was no difference between the groups (Tang et al. (2024). Rather, what mattered was age, as older adults had poorer access to telehealth (Tang et al., 2024).
Uptake of allied health telehealth among children and their parents/carers from CALD communities has received relatively less attention, and warrants research (Alfano et al., 2022). Moreover, unlike telehealth with older adults, successful implementation of telehealth with children and their families requires consideration of a broader range of unique issues such as parents’ preference, resources, digital literacy in addition to children’s characteristics such as age, ability to engage online, and type of developmental concerns (Mills et al., 2023).
Allied health telehealth services with children and their families
Allied health for children includes various services, with OT and SP being most common (Ciccia et al., 2011; Hines et al., 2019; Ingersoll and Berger, 2015; Langbecker et al., 2019). OT telehealth services for children have addressed a range of areas such as self-care, play and social skills, motor skills, sensory processing ability, and school readiness through play-based activities (e.g. handwriting, cutting, dressing, play) (Domínguez-Lucio et al., 2022; Mills et al., 2023; Tkach and Earwood, 2024). SP telehealth services for children have targeted areas such as speech accuracy, understanding and use of language, and fluency through play-based activities and conversation with children and/or via parent training (particularly for children 0-3 years) (Fong et al., 2025; Langbecker et al., 2019; Wales et al., 2017).
Within the evidence based on OT and SP telehealth services, issues on feasibility, effectiveness, and satisfaction with telehealth have been explored (Ciccia et al., 2011; Hines et al., 2019; Ingersoll and Berger, 2015; Langbecker et al., 2019; Tkach and Earwood., 2024), as well as parent, provider and referrer perceptions of services (Baker et al., 2025; Campbell et al., 2019). Research evaluating use of telehealth for paediatric populations suggests that this method of healthcare delivery is viable (Ciccia et al., 2011; Gözde et al., 2021; Hines et al., 2019; Hsu et al., 2021; Ingersoll and Berger, 2015; Langbecker et al., 2019; Sutherland et al., 2017; Wales et al., 2017). However, across this research, consideration of diversity of languages spoken and cultural background among participants has been understudied.
To date, only one study has reported on the cultural and linguistic characteristics of participants. Specifically, Stewart et al. (2017) assessed outcome of Cognitive-Behavioural-Therapy (CBT) when delivered via telehealth. Fifteen children aged 7–16-years were included in the study, with seven from Hispanic backgrounds, six from African American backgrounds and two from English-speaking backgrounds. Authors concluded positive outcomes post intervention, with reduction in symptoms. Although encouraging, various factors could influence uptake and success of telehealth with younger children, given that parents typically need to be present alongside their child.
What factors might influence telehealth uptake?
Across literature, a range of factors have been identified to influence access to healthcare. For instance, children who are developmentally vulnerable and their families have a high need for services yet ironically been reported to be less likely to access healthcare services (Woolfenden et al., 2020). Wait times and associated costs have also been reported to exacerbate inequities of access for those living in lower socio-economic or disadvantaged areas (Australian Institute of Health and Welfare, 2016). Given the importance of access to healthcare in the first 2000 days of life (New South Wales Health, 2019), a child’s priority for service coupled with area of residence needs consideration when exploring telehealth uptake.
Considering the Health Care Systems domain at the interpersonal level of the Framework for Digital Health Equity (Richardson et al., 2022), concerns over therapist-client rapport have also been reported to potentially influence uptake of paediatric allied health telehealth services (Campbell et al., 2019). It has been suggested that only once a therapeutic relationship has been established via face-to-face service, people may be more willing to use telehealth (Simpson and Reid, 2014). These findings suggest that influence of client’s status (i.e. being existing or new to the service) at the time telehealth is offered needs be explored. The nature of therapy could also impact uptake given findings that telehealth may pose challenges for hands-on therapies, such as OT, given lack of physical touch when compared to talking-focused therapies such as SP (Malliaras et al. (2021).
Research gap: uptake of allied health telehealth services for children from CALD and non-CALD communities
Given that children and their families in CALD communities can experience barriers to accessing healthcare (Pham et al., 2021), it is reasonable to suggest that this group may also experience barriers with telehealth uptake. Research is therefore needed to determine if uptake of paediatric SP and OT telehealth services differs between families of clients from CALD versus non-CALD communities. Such research will help determine if potential disparities related to cultural and linguistic differences exist in Australia. Additionally, research is needed to describe demographic characteristic of families of clients seeking SP and OT services, and identify potential factors influencing telehealth uptake, to contextualize and understand the potential role of CALD status on uptake.
Aim and research questions
The aims of this study were to describe the demographic characteristic of families from CALD and non-CALD backgrounds seeking OT or SP allied health services for their children, determine if telehealth uptake differs between families based on CALD background and between families across different language groups, and identify factors influencing telehealth uptake. Due to existing disparities in healthcare access of CALD populations, it could be hypothesised that telehealth uptake of OT and SP service by families of clients from CALD backgrounds would be less compared to families of clients from non-CALD backgrounds. Our study was designed to answer the following questions. 1. In CALD and non-CALD families seeking paediatric OT and/or SP services for their children, are there differences between the two groups in terms of overall uptake of telehealth, area residence, discipline of service (SP vs OT), priority category for service, whether they are existing or new clients to the service, and type of diagnosis (including waiting for diagnosis)? 2. Is likelihood of telehealth uptake associated with child’s category of priority for service based on age and risk status, allied health discipline (SP vs OT), whether they identify as CALD or non-CALD, language spoken, and area of residence (i.e. LGA)?
Materials and methods
Research design
A retrospective cross-sectional between groups review of clinical records was used to address the aims of this study. Ethical approval was obtained from the South-Western Sydney Local Health District Human Research Ethics Committee (2020/ETH01959).
Population
The population of interest were children referred to and/or receiving speech pathology and/or occupational therapy services at the time of the clinical records review. Clinical records for the children were divided into one of two groups according to CALD status – CALD or non-CALD. Children who were either born overseas or spoke a language other than English at home were classified as from the CALD group (Australian Institute of Health and Welfare, 2025).
Source of clients’ clinical records
Data were sourced from a review of clinical records for children referred to or receiving SP and OT services across seven community health centres within a public tertiary health provider. These centres service people, including children and their families residing in the Greater Western Sydney region, one of the most multicultural communities in Australia. The period of extracted data for the study was 30th March 2020 to 30th September 2020 during the COVID-19 pandemic as telehealth consultations were the primary mode of service delivery at this time.
Inclusion and exclusion criteria for client record review
In keeping with Gearing and colleagues’ (2006), a convenience sampling approach was chosen where all records for children referred to or currently using relevant community health OT and SP services were eligible to be included in the review. Convenience sampling as opposed to quota or systematic sampling (Gearing et al., 2006) ensured that the sample was as large as possible and representative of real-world practice. The broad inclusion criteria client records for children were as follows. (1) Referred to or receiving OT or SP services: Two disciplines (OT and SP) were selected as they are commonly accessed allied health services for children (Department of Health and Human Services, 2018) and align with two allied health disciplines typically reported in research on the topic of telehealth and allied health services. (2) Living in one of seven community health centres within a metropolitan Local Health District at any time during study period. Seven community health centres covered four Local Government Areas (i.e. LGAs). Regarding LGAs of residence, LGA#1 and LGA#4 had more CALD and lower SES clients than other LGAs, according to the SEIFA index (ABS, 2021). (3) Meeting one of four service priority categories: ≤3 years, 3;1-5;11 years, school-age- (i.e. age at time of school entry to Year 6, equivalent to approximately 12;11 years), or ‘at-risk’ (i.e. children with additional medical and/or social vulnerabilities).
Client records were excluded if more than 50% of required data to be extracted was missing from a client’s record, and/or there was no information about the client’s CALD background in the clinical record.
Clinical record review procedure
Procedures for data collection were based on recommendations for clinical record review by Sarkar and Seshadri (2014). First, demographic and clinical information were extracted. This included LGA of residence, allied health discipline, priority category for service, whether client was new or existing to the service, diagnoses, and decision to uptake telehealth, CALD background and language group. Second, appropriate electronic and paper file sources of routine data were identified by the health professionals (SPs and OTs managing a child’s case) with authority to extract relevant research data from those sources. Third, a suitable electronic instrument was identified, developed, and agreed upon by the third and last author for collating data – an excel spreadsheet with columns for each variable of interest. An identical copy of the spreadsheet format was shared with relevant OT and SPs at each community health centre. Senior OT and SPs across Centres collated all spreadsheets into one spreadsheet for each discipline, then checked and removed any potentially identifying information. They then shared de-identified spreadsheets with authors for data cleaning, combining, and analysis. Finally, the first author cleaned the data by identifying unclear, potentially incorrect, and missing data. Data were then formatted for analysis.
Planned data analysis
Demographic characteristics of clients a .
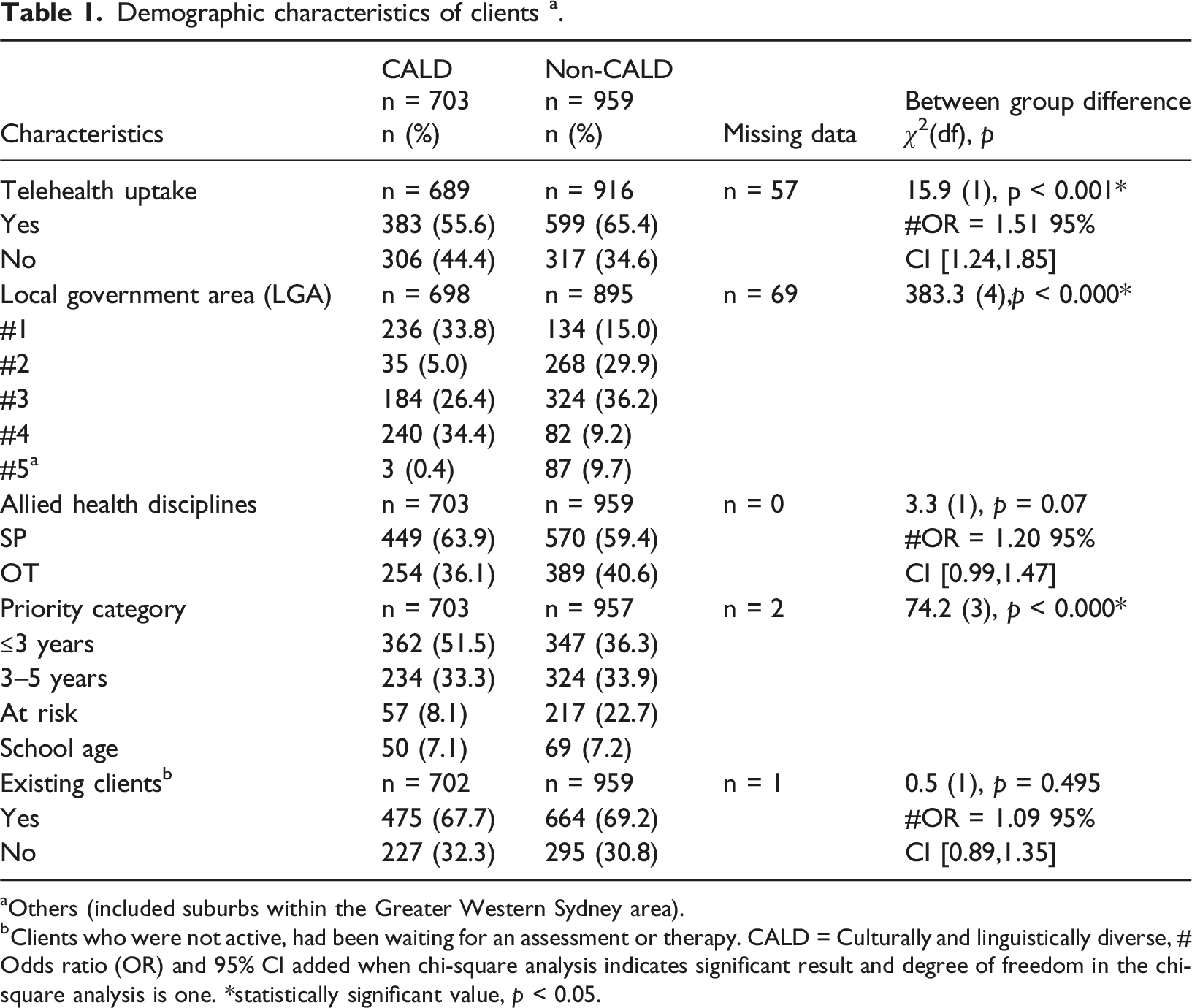
aOthers (included suburbs within the Greater Western Sydney area).
bClients who were not active, had been waiting for an assessment or therapy. CALD = Culturally and linguistically diverse, # Odds ratio (OR) and 95% CI added when chi-square analysis indicates significant result and degree of freedom in the chi-square analysis is one. *statistically significant value, p < 0.05.
Regression analysis of factors influencing uptake of telehealth for paediatric speech pathology and occupational therapy clients during the COVID-19 study period.
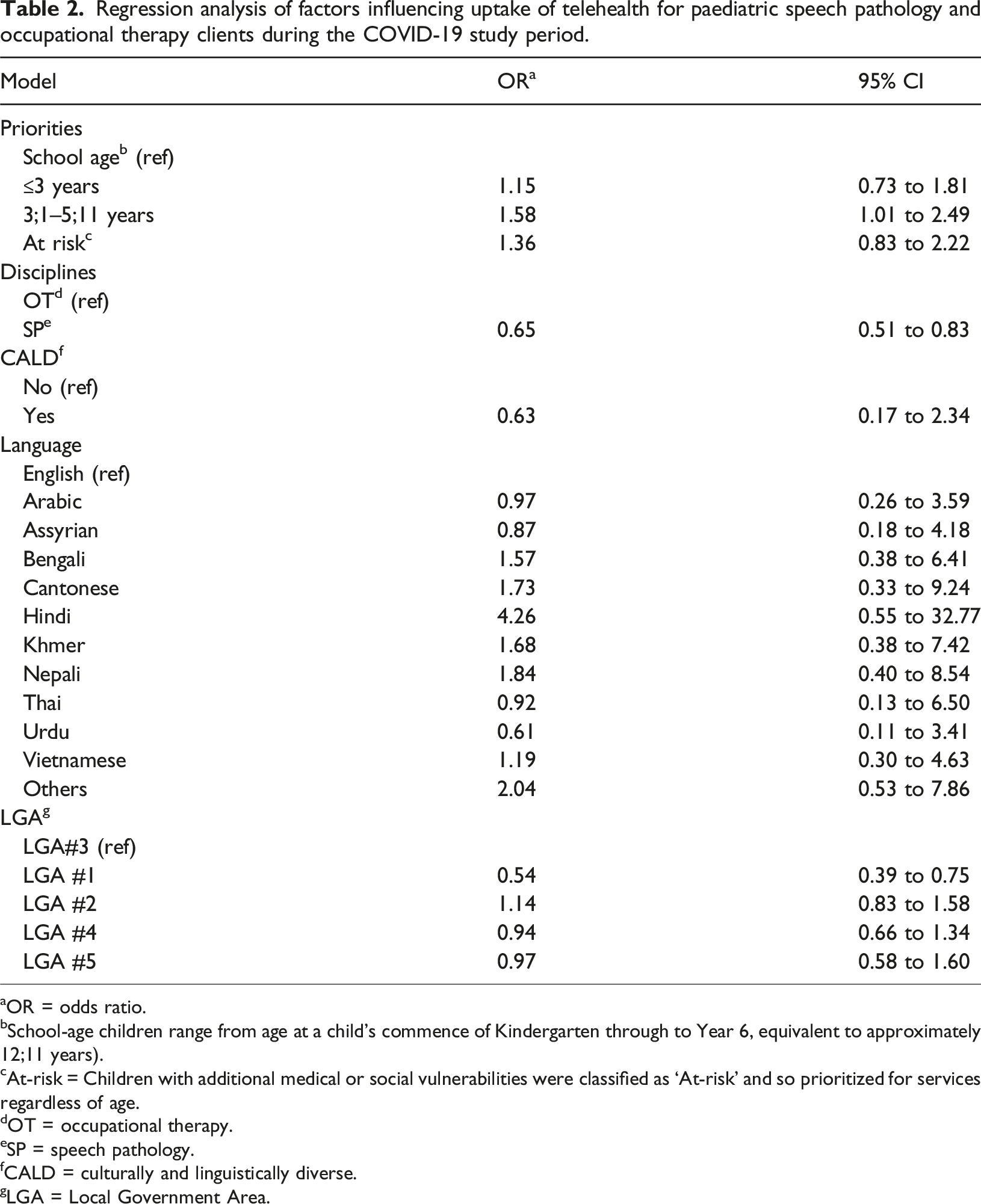
aOR = odds ratio.
bSchool-age children range from age at a child’s commence of Kindergarten through to Year 6, equivalent to approximately 12;11 years).
cAt-risk = Children with additional medical or social vulnerabilities were classified as ‘At-risk’ and so prioritized for services regardless of age.
dOT = occupational therapy.
eSP = speech pathology.
fCALD = culturally and linguistically diverse.
gLGA = Local Government Area.
Results
Clinical records for 1688 child clients seeking OT or SP services were identified for review. Out of these clients, 26 clients were excluded due to having more than 50% of data missing due to inability to extract information from clinical files. This left a total of 1662 client files meeting criteria: 703 clients (42.3%) from CALD backgrounds, 959 clients (57.7%) from non-CALD backgrounds. Fifty-eight languages were reported to be spoken across 1662 clients, with English spoken by 1011 clients (60.8%) (including 92 clients (5.5%) who reported speaking one other language in addition to English at home, and five clients speaking two other languages in addition to English). Across 58 languages spoken, 18 languages apart from English were reported to be spoken by more than five clients. Across 1662 clients, the three most common languages spoken apart from English included Arabic (n = 234, 14.1%), Vietnamese (n = 114, 6.9%), and Bengali (n = 64, 3.9%). Table 1 provides proportion of clients from CALD and non-CALD backgrounds across variables of interest including telehealth uptake, LGA of residence, discipline of services (SP and OT), priority category for service, whether clients were new or existing at the time when telehealth was introduced. Across 1662 client records, 982 (61.2%) accepted telehealth.
Regarding research question 1, telehealth uptake was significantly lower χ2 (df) = 16.1 (1), p < 0.001 for families from CALD backgrounds (n = 384) (55.6%) as compared to families from non-CALD backgrounds (n = 598) (65.4%). Of the total SP referrals, 449 clients (63.9%) were from CALD backgrounds; for OT, 254 clients (36.2%). There was a significant between group difference in categories of priority χ2 (df) = 70.6 (3), p < 0.000*. More than half of clients from CALD backgrounds were prioritised in the ≤3 years group (n = 362, 51.3%) in contrast to n = 347 (36.3%) for non-CALD group.
To further understand the heterogeneity across the client records, diagnoses are summarized in Supplemental Materials 1. There were 24 diagnostic categories. Of children seeking SP services, proportionally more children from CALD backgrounds had been diagnosed with a language disorder. By contrast, proportionally more children from non-CALD backgrounds had been diagnosed with a speech sound disorder. Regarding diagnoses for children seeking OT services, more children from non-CALD backgrounds were diagnosed with sensory disorders. Across two disciplines, there were 438 (26.8%) children waiting for a diagnosis. An odds ratio was calculated to further understand the likelihood of children from CALD backgrounds having no diagnosis as compared to children from non-CALD backgrounds. Children from CALD backgrounds were twice as likely yet to have a diagnosis (OR = 2.2 95% CI [1.8, 2.7]).
Regarding question 2, the binary logistic regression model was statistically significant, χ2 (20) = 80.09, p < 0.001 when the model was controlled by CALD, LGA, disciplines, language used, and priorities of service. Both disciplines and LGAs were found to be factors associated with telehealth uptake (Table 2). Priority for service and CALD status were not independent factors associated with telehealth uptake. Clients receiving SP services had significantly lower odd to take up telehealth as compared to clients receiving OT services (OR = 0.65 95% CI [0. 51, 0.82]). There was also a significant difference in likelihood between clients who were residing from LGA #1 to take up telehealth as compared to clients living in the LGA #3 (OR = 0.54 95% CI [0.4, 0.8]). While individual family’s socioeconomic status was not collected, results indicated that clients residing in an area with lower socioeconomic status (based on SEIFA index) were less likely to accept telehealth as compared to clients residing in an area with higher socioeconomic status.
Discussion
The main aim of our study was to determine if uptake of SP and OT telehealth services for children differed between families of clients from CALD versus non-CALD communities. To contextualize findings, a broader range of relevant factors were considered including whether uptake differed according to language group, area residence, discipline of service (SP vs OT), priority category for service, whether they are existing or new clients to the service, and type of diagnosis (including waiting for diagnosis). In summary, rate of telehealth uptake was significantly lower for families of clients from CALD backgrounds. However, contrary to expectations, being from CALD backgrounds or languages were not independent factors influencing uptake of telehealth when considered in a context with a broader range of factors. Rather, LGA of residence and allied health discipline were factors that influenced telehealth uptake by families of clients. Our discussion considers plausible reasons for these unexpected findings in the context of extant literature.
What factors might influence uptake of telehealth?
First, children and their families are unique. Although we divided clinical records based on CALD status, children and their families can differ in many ways. One factor reported to underly a decision to not use telehealth has been a child’s age with infants and toddlers (i.e. aged 0–2 years) considered too young to engage in telehealth sessions (Mills et al., 2023). In the current study, age was not a factor. It is possible that opportunities for parent training via telehealth, as opposed to provision of therapy directly with a toddler attenuated the potential contribution of age.
Second, it is possible that a child’s diagnosed condition and whether telehealth would meet a child’s needs and therapy goals contributes to parents’ decision to use telehealth irrespective of CALD status. In a qualitative study of families’ perceptions and attitudes towards telehealth in early intervention, parents of children with autism spectrum disorder (ASD) considered telehealth to be challenging, suggesting their children need in-person time to develop rapport before using telehealth (Yang et al., 2021). Again, in our study, type of condition was not a factor underlying telehealth uptake. It is possible that the wide diversity of conditions across SP and OT paediatric populations in the current study masked the role of specific conditions in the decision to use telehealth. It is also possible that provision of parent-training via telehealth for children with conditions such as ASD masked parents’ decisions, given that parent-training has previously been reported as a viable option for such families (Ingersoll and Berger, 2015).
Third, although SP interventions often focus on talking, SP clients were less likely to adopt telehealth compared to OT in our study. This was intriguing and contrasts with previous research suggesting that hands-on type therapies, such as OT, would be associated with being less likely to uptake telehealth given the need for physical prompts and tactile cues at times (Morris et al., 2014). It is possible that availability of interactive technology that can be utilised for rehabilitation in children may have encouraged families of clients to accept OT (Domínguez-Lucio et al., 2022). Why, however, would telehealth uptake be lower for families of clients referred to or receiving SP services? Fong et al., 2025 offer some insight. In their study exploring telehealth services for children who are medically complex, the parent of one child receiving SP services noted ‘speech and language especially was very difficult because she’s deaf/blind and so she’s absolutely not interested in screens of any kind’ (Fong et al., 2025: p. 345). This insight suggests that although talking is the audio and/or visual modality of communication when using telehealth, it may not be suitable for all SP clients. Research is needed to further understand factors underlying the difference between telehealth uptake between OT and SP services such as quality of the audio signal for listening to young children’s speech, and how young children engage or struggle to engage in the type of SP therapeutic activities during a telehealth session.
Fourth, clinicians’ assumptions about families of clients’ ability to use technology may play an inadvertent role in uptake of telehealth. Clinicians could have a view that telehealth is not a ‘hands-on’ therapy and may limit engagement with the client (Malliaras et al., 2021). It is also possible that level of experience and confidence to use telehealth varied across clinicians at time of the study, as they may not have used telehealth as part of routine practice prior to COVID-19 (Malliaras et al., 2021; Wade et al., 2014). Furthermore, clinicians’ inherent biases and assumption about a family’s suitability for telehealth may have contributed to lower uptake for clients from higher priority groups (Prahalad et al., 2022). Clinicians’ working in specific LGAs may have also had implicit biases that contributed to fewer clients from CALD backgrounds in those LGAs taking up telehealth. As demonstrated across similar studies, awareness of telehealth or allied health interventions tend to be poorer among people from CALD backgrounds (Tang et al., 2024, Prahalad et al., 2022). This potential for differences between clinicians and how they might inadvertently influence parents’ decisions to uptake telehealth warrants further research.
Finally, it is possible that a digital divide existed for families of clients living in LGA#1 and LGA#4, as those LGAs happened to have more CALD and lower SES clients – factors associated with inequity of access to telehealth (Australian Institute of Family Studies, 2024). Further research is required to deeply understand optimal service delivery pathways for children and their families to ensure equitable telehealth services (Thomas et al., 2024). Future research should also look at uptake of telehealth among Aboriginal communities through Aboriginal controlled services and lower SES families.
Strengths and limitations
This study explored telehealth uptake of children from CALD backgrounds seeking allied health services in comparison to children from non-CALD backgrounds. This study provides a deeper understanding of demographic characteristic of clients seeking the service, disparities in uptake and influencing factors impacting decisions to engage in telehealth. A strength of this study was the large sample size, providing a representative depiction of telehealth uptake of the local population. Use of pre-existing data collected for the purpose of an overarching clinical review is a limitation. This also meant that we were limited in our ability to collect information related to family characteristics such as self-perceived level of language proficiency, income and highest level of education in parents. Lack of data related to family characteristics meant that an adjusted model could not be conducted to evaluate if such family characteristics influenced uptake of telehealth. Possibility of bias present during data collection is acknowledged and cannot be disregarded. We also recognised that allied health is devised of disciplines beyond OT and SP. With this, it is acknowledged that these results may not be generalisable to allied health entirely. Nonetheless, considering that SP and OT are the two most common allied health services accessed by paediatric populations, findings provide important results to inform allied health clinicians on factors to consider before implementing telehealth services. Finally, the study was conducted during the height of the COVID-19 pandemic, which meant that community health services could only be delivered via telehealth and clients may have been forced to agree to telehealth. It is possible that acceptance post pandemic may differ and a repeated measure of uptake is warranted to evaluate if factors impacting uptake of telehealth remained similar.
Implications for practice
Our results highlight that allied health telehealth services for children need to be equitable. Based on Gallegos-Rejas et al. (2023) work, a multi-stakeholder approach could be helpful in designing equitable telehealth services through engaging consumers, advocacy groups, clinicians, health services and administrators, policy-makers, industry, and researchers. For instance, clinicians and administrators could learn how multiple domains of influence (Richardson et al., 2022) could coalesce to drive inequality in telehealth uptake for children in their local area. Through training, clinicians could become cognizant of their pre-conceived beliefs about children suitable for telehealth, and advocate for change when they identify barriers for children from CALD families in their area. Clinicians and administrators could also appreciate that simply providing access to technology for telehealth is not sufficient, and partner with consumers to design solutions for equitable uptake (Mistry et al., 2022). Stakeholders could also discern when and how telehealth best complements rather than replaces face-to-face services, to ensure all children get the help they need (Rocha et al., 2026).
Conclusion
Provision of allied health telehealth services for children can be challenging. In this study, it was anticipated that uptake OT and SP service by families of clients from CALD backgrounds would be less compared to families of clients from non-CALD backgrounds. Our findings revealed a more complex and nuanced picture. What matter was where families of clients lived, and type of allied health discipline. Results of this study should motivate clinicians and policy makers to further understand the complex interplay of factors contributing to telehealth uptake in their local service, to ensure all children have equitable access to services.
Supplemental material
Supplemental material – Telehealth uptake by families seeking allied health services for young children: Does culturally and linguistically diverse background matter?
Supplemental material for Telehealth uptake by families seeking allied health services for young children: Does culturally and linguistically diverse background matter? by Chloe Li, Clarice Y Tang, Katrina Tosi, Elise Baker in Journal of Child Health Care.
Footnotes
Acknowledgements
The authors acknowledge the contribution of the SP and OT clinicians, particularly Kirralee Hazeltine and Annette Zucco, in Primary and community health centres across South-Western Sydney Local Health District.
Ethical coniderations
Ethics approval for this study was obtained from the South-Western Sydney Local Health District Human Research Ethics Committee (2020/ETH01959).
Funding
The authors disclosed receipt of financial support for the publication of this article from the Council of Australian University Librarians (CAUL) to cover open access article processing charges (APCs).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.