
Abstract
Esophageal Atresia/Tracheoesophageal Atresia (EA/TEF) is a multisystem congenital anomaly. Historically, children with EA/TEF lack coordinated care. A multidisciplinary clinic was established in 2005 to provide coordinated care and improve access to outpatient care. This single-center retrospective cohort study was conducted to describe our cohort of patients with EA/TEF born between March 2005 and March 2011, assess coordination of care, and to compare outcomes of children in the multidisciplinary clinic to the previous cohort without a multi-disciplinary clinic. A chart review identified demographics, hospitalizations, emergency visits, clinic visits, and coordination of outpatient care. Twenty-seven patients were included; 75.9% had a C-type EA/TEF. Clinics provided multidisciplinary care and compliance with the visit schedule was high with a median of 100% (IQR 50). Compared to the earlier cohort, the new cohort (N = 27) had fewer hospital admissions and LOS was reduced significantly in the first 2 years of life. Multidisciplinary care clinics for medically complex children can improve coordination of visits with multiple health care providers and may contribute to reduced use of acute care services.
What is known on this subject
Children with TEF/EA have complex medical needs and coordination of care at our center was poor. Pediatric patients have benefited from multidisciplinary care. A multidisciplinary clinic was thus implemented for our patients and health care outcomes were assessed.
What this study adds
This study adds quantitative outcome data to the body of literature around Multidisciplinary care for children with complex medical conditions. We report improvements in admissions, length of stay, and procedures for children with TEF/EA after implementation of a multidisciplinary clinic.
Introduction
Esophageal Atresia/Tracheoesophageal Atresia (EA/TEF) is a multisystem congenital anomaly occurring in 1/4500 births, requiring prompt identification and complex treatment including surgery (Pinheiro et al., 2012). Children with EA/TEF have prolonged hospital stays, multiple surgeries, and care from a variety of health care professionals (Pinheiro et al., 2012; Little et al., 2003; Deboer et al., 2016; Friedmacher et al., 2017). The numerous complications associated with EA/TEF include esophageal dysfunction, chest and spine deformities, and pulmonary disease (Acher et al., 2016). Pulmonary and esophageal symptoms can impair the quality of life of the patients and challenge their families and health care providers (Little et al., 2003; Bal et al., 2016; Gibreel et al., 2017). Symptoms of cough and wheeze, as well as recurrent bronchitis and pneumonia are common. Esophageal dysmotility and gastroesophageal reflux often occur after surgical repair of esophageal atresia (Pereira et al., 2003; Friedmacher et al., 2017) and permanent respiratory damage may result from recurrent respiratory tract illness (Kovesi, 2013; Patria et al., 2017; Porcaro et al., 2017). Therefore, these children need to be followed long-term to evaluate and address these issues (Acher et al., 2016; Romeo et al., 2000; Deboer et al., 2016).
Lack of continuity within medical care results in additional stress for the parents of children with any chronic condition including EA/TEF (Miller et al., 2009). Some stressors on families may be reduced by care from a multidisciplinary team thus enhancing quality of life (Goldhagen et al., 2016) (Labree et al., 2010). When the multidisciplinary team is committed to coordination of care then further improvements are possible including integrated services, monitoring progress, surveillance for early signs of problems, and targeting at-risk patients with assessment of medical, functional, emotional, and social needs (Peter et al., 2011) (Van Dongen et al., 2020). Golden and Nageswaran (2012) found that access as well as coordination of services is the greater problem for parents with chronically ill children, including EA/TEF, than with the quality of the health care services.
In a study conducted at our institution, children with EA/TEF underwent multiple surgical procedures and extensive hospitalizations and care was poorly coordinated (Bjornson and Mitchell, 2006). The lack of a primary clinic meant an extra burden of multiple separate visits with many different specialists (Bjornson and Mitchell, 2006). Hence a multidisciplinary TEF Clinic was initiated at our center in 2005 with an overarching aim of improving coordination of services for both scheduled care and unanticipated issues.
This multidisciplinary clinic, recognizing the complex effects on many body systems for EA/TEF survivors, allows these patients to access multiple health care professionals in 1 day and provides a primary clinic from initial hospital discharge to adulthood based on age and anticipated service needs (Supplemental Table 1). Multi-disciplinary team members included: Pediatrician, Pediatric Respirologist, Registered Nurse, Registered Dietician, Occupational Therapist, Social Work, Pediatric General Surgeon, and Pediatric Gastroenterologist. The clinic aims to provide coordinated care, provide psychosocial support, minimize time spent in the hospital, and related parental financial burdens, with the goal of improving quality of life for patients and their families. Outcomes such as frequency of hospital admissions, critical care admissions, and length of stay may be improved by screening for common complications associated with EA/TEF, providing families with anticipatory guidance, and improving access to outpatient care in a central clinic setting. The role of multidisciplinary care clinics in improving patient outcomes has been studied in some specific chronic pediatric patient populations (Goldhagen et al., 2016; Zurynski et al., 2019) but has not been studied in EA/TEF.
Aim
To describe the cohort of patients with EA/TEF at our center, assess coordination of care provided to this population and to compare outcomes of children enrolled in the current multidisciplinary clinic to the previous cohort of children with EA/TEF before the clinic existed.
Methods
Study design
This was a single-center retrospective cohort study of children born between March 2005 and March 2011 with EA/TEF enrolled in the multi-disciplinary EA/TEF clinic at our center. Using chart review, the following variables were described: (1) patient demographics, (2) coordination of care, and (3) selected clinical outcomes (emergency room visits, hospital admissions, PICU length of stay, total length of stay, recurrent fistula repair, g-tube insertion, esophageal dilation, endoscopy, and bronchoscopy) as compared to a pre-clinic cohort from April 1994 to September 1999 (Bjornson and Mitchell, 2006).
Participants included children with EA/TEF born between March 2005 and March 2011 and who were cared for in the EA/TEF clinic. The time frame of birth to 6 years of age was chosen for data inclusion to ensure an adequate amount of time for the impact of outpatient care to be assessed. These patients were born after the initiation of the EA/TEF clinic and so were eligible to be followed from birth. Children with TEF alone, TEF and EA and EA alone were all included (Supplementary Figure 1). Patients who did not survive past 1 year of age were included in demographic data collection but were excluded from the study, as those patients had unusually marked medical complexity to confound their data contribution to the study. The pre-clinic cohort participants, as described in a previous study, included all patients with EA/TEF, TEF alone and EA alone from April 1994 to September 1999 who survived past 1 year of age. (Bjornson and Mitchell, 2006).
Demographics
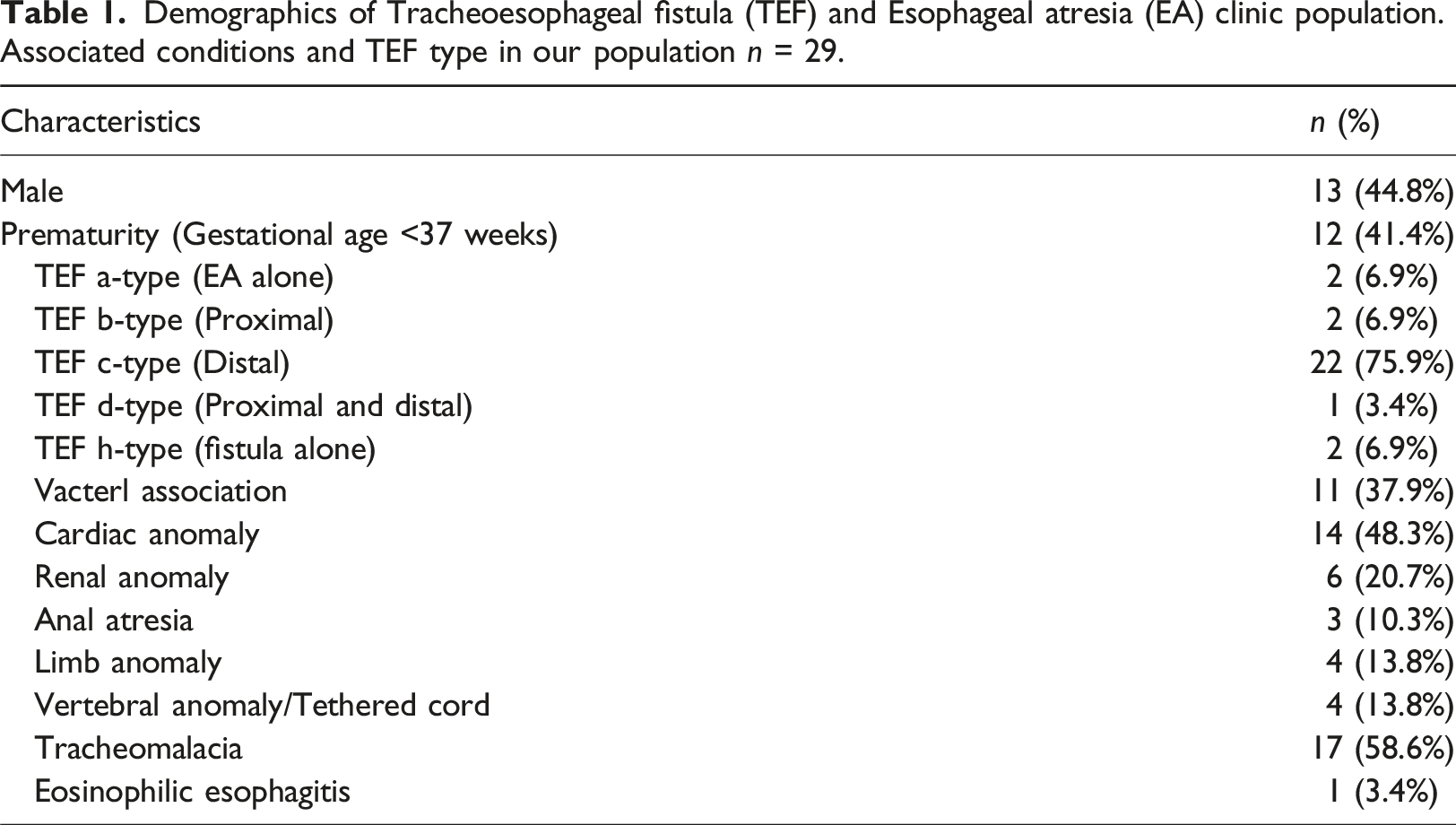
Demographics of Tracheoesophageal fistula (TEF) and Esophageal atresia (EA) clinic population. Associated conditions and TEF type in our population n = 29.
Coordination of care
The aim of the study was to assess coordination of care as this was the goal of the current clinic. Coordinated care was defined as attending scheduled visits in clinic from age zero to 6 years, care received from multiple providers at a single visit and no unanticipated visits to clinic or the ED. Attainment of this clinic goal was evaluated by examining: (a) proportion of patient visits to multiple health care providers were coordinated on the same calendar day; (b) proportion of scheduled visits occur within the projected schedules for different age groups; and (c) number and types of scheduled medical appointments occurring within 7 days, 30 days, or greater than 30 days apart from a scheduled EA/TEF clinic visit. (Supplementary Table 1).
Medical outcomes
The secondary objective was to compare outcomes of the two cohorts with differences in integration of services in the first 5 years of life. The results from the clinic cohort were compared to the 2006 study pre-clinic cohort of EA/TEF patients born from 1994 to 1999. This analysis compared the following outcome measures per year for each of the first 5 years of life: recurrent fistula repair, g-tube insertion, esophageal dilation, endoscopy, and bronchoscopy, rates of visits to the ED; rates of admissions to a tertiary care facility; average length of stay (ALOS) during admissions to a facility; and total days of stay in a hospital facility.
Statistical analysis
Descriptive statistics were used. Data are presented as either medians with IQR or means with standard deviation (SD) and comparisons were done using the t test. We recognize that for certain outcomes, the distribution may not be symmetric; however, since the only data we had from the previous study were the summaries themselves and not the data, this was the only way to attempt a comparison. The entire population for the years considered is being included in the study, and no specific effect size was expected a priori, hence a power-based sample size calculation is not provided. We present comparisons with 95% confidence intervals since our sample size is the full population at our center and our conclusions are for each variable separately.
Results
Twenty-nine children born between March 2005 and March 2011 were identified for review. Demographics of the population are shown in Table 1. There were 27 participants who had complete data to form the analysis cohort, as there were two children who passed away during initial admission.
The number of health care providers per clinic visit within the multidisciplinary clinic ranged from medians of 3.17 (IQR 1.19) to 4.60 (IQR 0.82) and physicians per visit ranged from medians of 1.5 (IQR 0.47) to 2.00 (IQR 0). The median of full adherence (100% of suggested visits) to the clinic schedule was high (Supplementary Table 3). Other than the planned visits, the EA/TEF clinic responded to patient needs by providing urgent or unplanned clinic visits with a mean of 0.44 (SD 0.64) per patient in the first year. There were also multiple telephone call assessments with advice provided to the patients and families by clinic nurses and dietitians. Not all telephone visits were consistently recorded. The timing of clinic visits outside of the EA/TEF clinic is shown in Supplementary Table 4. During the first year of life, there were more subspecialty visits on different days from the EA/TEF clinic and more of these additional clinic visits were closer in time to the EA/TEF clinic visits. Over subsequent years there were less additional visits close to the scheduled TEF/EA clinics.
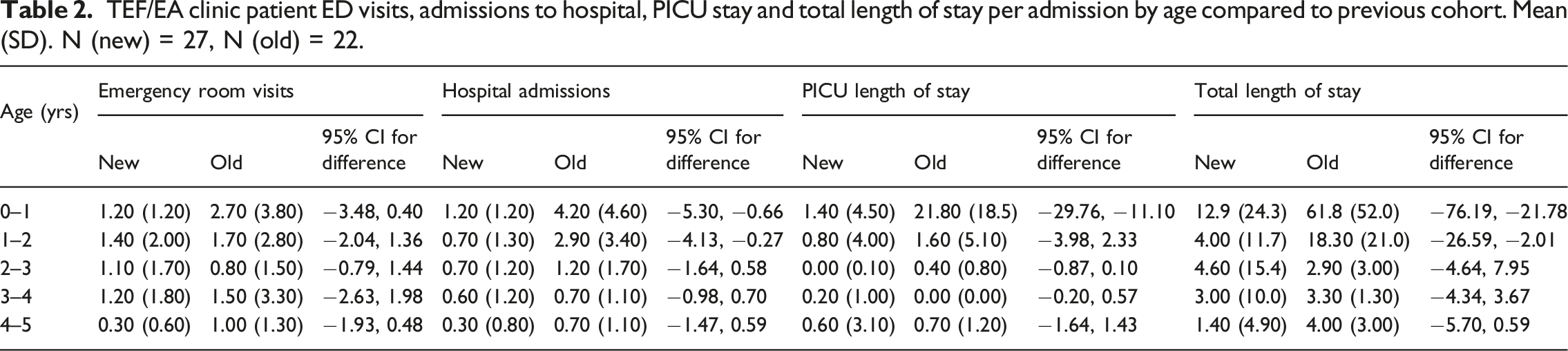
TEF/EA clinic patient ED visits, admissions to hospital, PICU stay and total length of stay per admission by age compared to previous cohort. Mean (SD). N (new) = 27, N (old) = 22.
TEF/EA clinic patient procedures by age compared to previous cohort. Mean (SD) N (new) = 27, N (old) = 22.

Subsequent admissions were statistically significantly reduced in number as well as reduced in LOS when compared to the pre-multidisciplinary clinic cohort. This was more notable in the first 2 years of life. In year zero to one, the mean number of admissions per patient was 1.20 (SD 1.20) with a difference of −2.98 95% CI [−5.30, −0.66] from the previous cohort and mean LOS per admission was 12.80 (SD 24.3) with a difference of −49.0 95% CI [−76.19, −21.78]. In year 1 to 2 the mean number of admissions per patient was 0.70 (SD 1.3) with a difference of −2.20 95% CI [−4.13, −0.27], and mean LOS per admission was 4.0 (SD 11.7) with a difference of −14.30 95% CI [−26.59, −2.01].
On review of procedures compared to the previous cohort (N = 22), we found a statistically significant reduction in procedures during the first 2 years of life (Table 2). From birth to one, the mean total procedures per patient in the new cohort was 2.4 (SD 2.8), with a difference of −4.39 95% CI [−7.77 to −1.02]. In years one to two, the mean total procedures per patient in the new cohort was 0.7 (SD 1.7), with a difference of −2.36 95% CI [−4.64 to −0.08].
Discussion
For children with EA/TEF at our center, we demonstrated improvement in coordination of care and clinical outcomes in the cohort of patients cared for in a multidisciplinary clinic when compared to a previous cohort. Published studies have not demonstrated the value of multidisciplinary and coordinated care on this population of children with medical complexity through quantitative evidence such as data on admissions, length of stay, and procedures (Acher et al., 2016; Syed et al., 2020). Data in this study provide quantitative evidence of improvement in patient care outcomes for children with EA/TEF cared for in a pediatric multidisciplinary clinic.
Populations in cohorts from separate time periods are similar in complexity, including type of EA/TEF, prematurity, and proportions of associated anomalies (Bjornson and Mitchell, 2006). Average length of stay (ALOS) for the initial stay was longer in the newer cohort, but not statistically significant. In the new cohort, the ALOS may have been impacted by inclusion of two children with isolated long gap esophageal atresia as these patients are known to have a more complex clinical and surgical course (Seguir et al., 2005). The length of the initial hospital stay is not unexpected and is reflective of the acuity and complexity of the perioperative, surgical, and medical care required for the stabilization, repair, and recovery of these infants prior to the first discharge from hospital (Syed et al., 2020). Overall, the new cohort possessed comparable or higher complexity compared to the historical cohort allowing for comparison of outcomes of the two cohorts.
Implementation of the EA/TEF clinic was crucial in achieving coordination of care which was its main priority (Supplementary Table 4). The high number of HCPs and MDs per patient per visit was impressive especially in comparison to traditional clinic visits in the previous cohort (Bjornson and Mitchell, 2006). High adherence to clinic schedules promotes effective use of healthcare resources as reported by Kheirkhah et al. (2016). Increased clinic visit adherence has been associated with fewer ED visits and admissions in other pediatric chronic care populations such as epilepsy (Bailey et al., 2021). Care coordination can also reduce overall costs for families and the health care system as shown in several studies of care coordination programs for children with complex health needs (Cunningham et al., 2008; Peter et al., 2011; Webber et al., 2018; Zurynski et al., 2019). The EA/TEF clinic worked to coordinate appointments on the same day, however, some of the other clinics the children needed to attend run only on certain dates and require their own multidisciplinary staff. As a result, some additional visits occurred close to a scheduled EA/TEF clinic, and this was most common in the first year of life when subspecialty and surgical visits were more numerous.
Fewer hospital admissions and LOS seen in the new cohort may be attributed to the multidisciplinary care provided, the availability of timely outpatient assessments and urgent clinic appointments for intercurrent illnesses and acute care issues, as well as anticipatory guidance during follow-up visits. Children in their first 2 years of life demonstrated more notable reduction in hospital admission and length of stay, perhaps due to increased frequency of EA/TEF related complications requiring acute care services in the earlier years of life. Reduced time in an acute care setting is an important clinical outcome. In other studies, reduced acute care use following care coordination has been associated with other outcomes such as lower cost and better quality of life. For example, several studies (Zurynski et al., 2019; Howard et al., 2017; Cohen et al., 2012) have demonstrated that care coordination programs for children with medical complexity have been shown to reduce acute care visits as well as reduced overall costs. Goldhagen et al. (2016) reported that a coordinated care program for palliative care led to reduced hospital days of stay and overall improvement in patient and family quality of life.
Reduction in total number of procedures in the first 2 years of life in the new cohort could have resulted from surgical and medical EA/TEF management changes such as a shift in surgical techniques toward an endoscopic approach and a transition to medical reflux management with proton pump inhibitors (PPI). Our clinic patients were followed frequently with optimization of reflux management including use of PPI for all patients in their early years which may help decrease total procedures in the first 2 years of life by reducing symptoms and improving weight gain (Krishnan et al., 2016). Medical evidence for PPI use improving outcomes in EA/TEF has been variable. One systematic review (Shawyer et al., 2014) showed that medical management of gastroesophageal reflux via acid suppression was successful in reducing respiratory and gastrointestinal symptoms, as well as improving weight gain. However, a 2018 systematic review by Miyake et al. (2018) demonstrated that PPI use did not directly correlate with a reduction in strictures, although the quality of the evidence was low. Coordinated clinic care may also have contributed to lower procedure numbers by facilitating multidisciplinary assessment of symptoms, comprehensive medical management plans including medications and feeding, ongoing follow up and adjustment based on the clinical course, and ongoing family supports for medication and treatment plan adherence.
Limitations
While this study demonstrates the importance of multidisciplinary care for children with EA/TEF, there are limitations. EA/TEF is a rare disorder, and most centers have a small population (Spitz 2011). This study was from a single center with a small sample size. However, it was inclusive of the entire outpatient population of these children surviving past 1 year of age in our center and allows for comparison to our previous same center cohort. Another limitation in comparing these groups is that surgical technology and hospital care have also changed over time and may result in changes to admission criteria, length of stay, time in ICU or other measures (Pinheiro et al., 2012). There is no plausible way to control for these factors. While we demonstrated an improvement in the number of admissions, length of stay, and procedures, this study did not complete a full economic analysis of this impact and quality of life could not be compared as such measures were not completed in the previous cohort. Determining causation is not possible given the many variables which may modify or confound the relationship; however, we demonstrated an association between the change in clinic care model and patient outcomes. This study is also limited to examining the effect of multidisciplinary care in children with EA/TEF later in childhood. More research is needed to assess long-term outcomes.
Implications for practice
Multidisciplinary clinics are one approach to providing coordination of care for patients with rare, multisystem conditions. As these clinics involve multiple physician specialties, nursing and allied health, they require an investment of resources by the health system. Demonstrating a reduction in acute care utilization as seen in this study can aid clinicians and families in advocating for multidisciplinary care clinics for EA/TEF and other similar multisystem conditions. The feasibility of this model of care coordination was also demonstrated in the study of our EA/TEF clinic as multiple providers attended per visit and families were able to adhere to the clinic schedule. The structure of this clinic can be replicated in other centers and for other conditions. At our center, a similar multidisciplinary clinic was successfully implemented for children with congenital diaphragmatic hernia.
Conclusion
Our EA/TEF multidisciplinary care clinic improved coordination of visits with multiple health care providers and was associated with reduced use of acute care services and invasive procedures. This study highlights the impact of multidisciplinary care on outcomes in EA/TEF in the first 5 years of life. Long-term outcomes for these patients would be an important area for further studies. This model of multi-disciplinary and coordinated care could be beneficial to other discrete populations of children with medical complexity.
Supplemental Material
Supplemental Material - Multidisciplinary coordination of care for children with esophageal atresia and tracheoesophageal fistula
Supplemental Material for Multidisciplinary coordination of care for children with esophageal atresia and tracheoesophageal fistula by Jody M. Platt, Alberto Nettel-Aguirre, Candice L. Bjornson, Ian Mitchell, Kathryn Davis, and Michelle Bailey in Journal of Child Health Care
Supplemental Material
Supplemental Material - Multidisciplinary coordination of care for children with esophageal atresia and tracheoesophageal fistula
Supplemental Material for Multidisciplinary coordination of care for children with esophageal atresia and tracheoesophageal fistula by Jody M. Platt, Alberto Nettel-Aguirre, Candice L. Bjornson, Ian Mitchell, Kathryn Davis, Michelle Bailey in Journal of Child Health Care
Abbreviations
Esophageal atresia
Tracheoesophageal fistula
Footnotes
Author’s Note
This article demonstrates improvements in health care outcomes for children with EA/TEF after implementation of a multidisciplinary clinic.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics approval
This study was approved by the research ethics board at our center.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.