
Abstract
Children living in disadvantaged communities have substantially increased risk for deleterious health and developmental outcomes. A considerable proportion of developmental delay is avoidable; however if children do not receive appropriate treatment within this critical period, damage can be irreparable. Community paediatric clinics provide medical and developmental assessment; deliver health promotion services, counselling, and advice to caregivers; and referral to services. The aim of this study was to systematically search, appraise, and synthesise the literature exploring the role of community paediatric clinics in supporting developmental outcomes and services for children living in disadvantaged communities. Electronic databases were searched using a carefully developed search strategy. Validated tools and appropriate guidelines assessed quality and confidence in evidence. Data analysis and mixed-methods synthesis was guided by the Segregated Framework for Mixed-Method Systematic Reviews. Eighteen studies were selected for inclusion. Areas of emphasis in the literature include the identification and monitoring of developmental delay; engagement of vulnerable families; relational working with children, families, and local services; referral to early intervention services; parental empowerment, practitioner capacity building; and tackling barriers to healthcare access. Through use of a child and family-centred model of care, community paediatric clinics can better meet the needs of vulnerable populations.
Keywords
Definitions
Community paediatric clinics are located in the community whose practice is focused on children and their families who visit the clinic and supporting their access to needed services (Ukep, 2009).
Child development refers to the sequence of physical, language, thought, and emotional changes that occur in a child from birth (CDC, 2021).
Developmental delay, identified in prenatal to 8 years, is described as a significant variation in a child’s achievement of expected milestones for their actual or adjusted age (Argall et al., 2022).
Disadvantaged communities refer to areas which suffer most from a combination of economic, health, and environmental burdens (Ukep, 2009).
Early intervention services are supports available to babies and young children with developmental delays and disabilities and their families (CDC, 2021).
The Human Development Index (HDI) was used to determine high-income and very high-income countries. We used predefined categories of the distribution of HDI by country: high (zero point seven–zero point seven nine) and very high (≥ zero point eight) (UNDP, 2020).
Introduction
The most critical period of human development is conception to age six when brain architecture foundations develop (Zero to Three, 2001). How well brain structures form determines child development, well-being, learning, and behaviours that follow (Shonkoff and Phillips, 2000). Developmental delays can impact children’s ability to participate in activities of daily living including play, independently dressing and toileting, social relationships, and academic performance (Smith and Gallego, 2021). Delays can also impact health and functioning requiring higher rates of healthcare, multidisciplinary appointments, and learning supports at school (Boulet et al., 2009; Davidson et al., 2004).
Children of low socio-economic status living in poverty are often at increased risk of developmental delay and poor physical or mental health, perform less well in school, and often enter an inter-generational cycle of reduced employment, higher fertility, and health inequalities (Heckman and Masterov, 2007; Komro et al., 2013; Levanthal and Brooks-Gunn, 2000; Nicholson et al., 2012). The ‘at-risk’ status for very young children with developmental disabilities is further exacerbated when living in poverty (Aber, Jones, & Cohen, 2000). A considerable proportion of developmental delay is avoidable (Levanthal and Brooks-Gunn, 2000); however if children do not receive appropriate treatment within this critical period, damage can be irreparable (Nicholson et al., 2012). Early detection and intervention can enhance developmental trajectories improving child, family, and community outcomes (Komro et al., 2013; Levanthal and Brooks-Gunn, 2000; Nicholson et al., 2012). Gains associated with early implementation of services can ease financial burdens on healthcare systems (Heckman and Masterov, 2007; Jacobson and Mulick, 2000; Järbrink & Knapp, 2001). The World Health Organisation (WHO) reports one of the most efficient ways of ‘closing the gap’ in health inequities is to address the needs of those who are most disadvantaged (WHO, 2013).
Families and children made vulnerable by multiple intersecting social determinants of health face both social and structural challenges in accessing health care (Ukpeh, 2009). Given the multiplicity of health risks associated with social disadvantage, strategies to promote child health and well-being go beyond traditional medical-based settings and involve community-wide policy strategies that change the broader environment in which children live (Shonkoff and Phillips, 2000). Community paediatric clinics treat unwell children, monitor developmental concerns and delay, deliver health promotion services, counselling and advice, and referral to other health professionals (Komro et al., 2013). Implemented in community settings, these clinics are usually delivered by a paediatrician and medical team (Ukep, 2009). These multi-disciplinary teams work across agencies with local therapists, nurses, schools, social services, the voluntary sector, and local authority (RCPCH, 2017). Often implemented in areas of social disadvantage where individuals are increasingly vulnerable, a substantial number of children attending paediatric clinics have developmental issues (Leventhal and Brooks-Gunn, 2000).
Bronfenbrenner’s Ecological Systems Theory assumes that humans encounter different environments throughout their life that influence development and behaviours (Bronfrenbrenner, 1992). This theory underscores the importance of community interventions and local services, the relationships between these systems, and the role local and national policies have on child health and development (Marshall, 2004). Approaches to implementation are also important (Shonkoff and Phillips, 2000). Traditional approaches to identifying child developmental delay, that is, screening techniques, can be difficult to implement, time consuming to administer, and often yield results which are difficult to interpret, leading clinicians to resort to a ‘wait and see’ approach when identifying and treating developmental delay (Williams and Holmes, 2004). Evidence shows early identification can be dramatically improved by the utilisation of local knowledge and experience, particularly parental knowledge when treating children with subtle developmental delay (Marshall, 2004; Williams and Holmes, 2004). In 1993, Spencer reported that a shift from hospital-based care towards community paediatric care was required (Spencer, 1993). In subsequent decades, several studies reported on community paediatric clinics implemented in disadvantaged areas. To date, a systematic review of the evidence on community paediatric clinics and their role in supporting developmental outcomes and services has not been conducted.
Aim
To systematically search, appraise, and synthesise available literature exploring community paediatric clinics and their role in supporting developmental outcomes and services for children living in disadvantaged communities in high-income countries.
Methods
We performed a mixed-method systematic review, guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) Statement (Page et al., 2021). The study protocol was registered with the International Prospective Register of Systematic Reviews (registration number: CRD42021243889), and overarching question and sub-questions were the following:
What role do community paediatric clinics play in supporting developmental outcomes and services for children living in disadvantaged communities? • How do community paediatric clinics aid early identification of developmental delay in vulnerable children? • How do community paediatric clinics engage vulnerable children and families? • How do community paediatric clinics enhance referrals of vulnerable children to early intervention services?
Study eligibility criteria
Eligibility criteria for studies
Search strategy
Figure 1 outlines study selection processes from identification, screening, eligibility, and inclusion. Medical Subject Heading (MESH) databases identified relevant concepts, terms, descriptors, and synonyms. A combination of pre-defined search terms agreed upon a priori by two reviewers was searched using Boolean logic. Search terms and strategy are provided in Supplementary File 1. PRISMA flow diagram of study selection process (Page et al., 2021)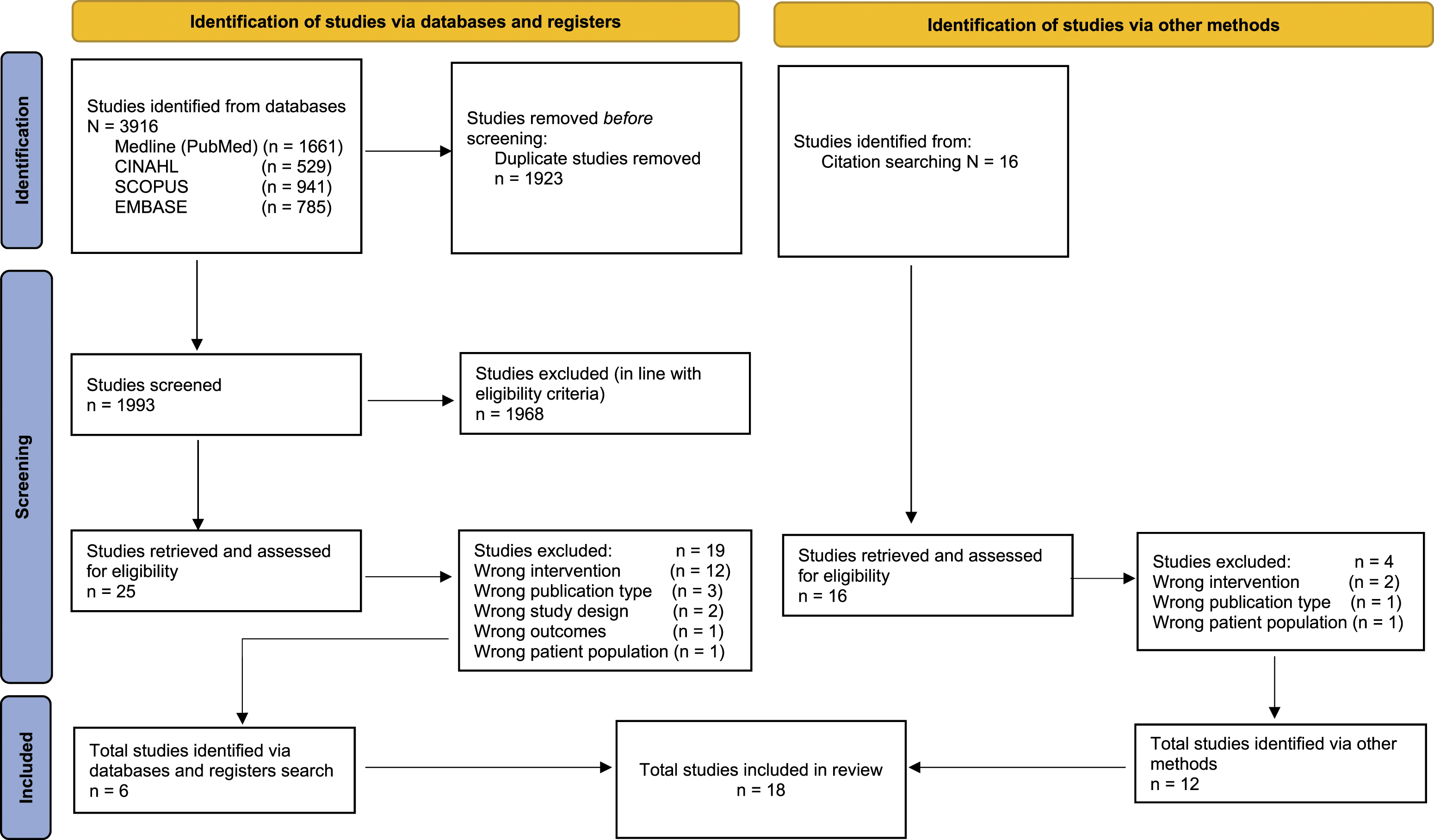
Two authors independently searched four electronic databases: Medical Literature Analysis and Retrieval System Online (MEDLINE), Excerpta Medica Database (Embase), Scopus, and Cumulative Index to Nursing and Allied Health Literature (CINAHL). An initial search was conducted on 1 January 2021 and repeated on 29 October 2021 to ensure newly published studies were reviewed for possible inclusion. Additional activities included reference list searches, hand-searching of key journals, and contacting key authors.
Two independent reviewers engaged in a three-stage study selection process. Results of respective analyses were compared following the completion of each phase. Conflicts were resolved through discussion. Where necessary, a third reviewer was consulted.
Data management
Mendeley Ltd. Desktop Application was used for importing and collating studies and bibliography development. Covidence 2020 guided importing saved papers from Mendeley, screening titles and abstracts, creating forms, assessing risk of bias, and data extraction.
Data extraction
Data on the characteristics of included studies were extracted and entered into a purpose-built datasheet by one reviewer and checked for accuracy by the second reviewer. Supplementary File 2 outlines specific data items extracted.
Review team members independently read and re-read all included studies in chronological order focussing initially on content and context. Data extraction was guided by the Segregated Framework for Mixed-Method Systematic Reviews (Sandelowski et al., 2006). This model assumes studies in a targeted domain are grouped for synthesis not by methods but by findings viewed as answering the same research questions or addressing the same aspects of a target phenomenon. Analytic emphasis is on transforming findings to enable them to be combined, in this case transforming all data to qualitative form.
Our lead author open-coded included studies extracting first-order interpretations (clinic data and views of participants) and second-order interpretations (views of authors). In quantitative studies, first-order interpretations were derived from questionnaire data, clinic descriptive statistics, and descriptive explanations of clinic data (where applicable). In qualitative studies, first-order interpretations were derived from attitudes and experiences of practitioners as presented in result sections. Second-order interpretations were derived from authors’ views contained within discussion and conclusion sections. To aid extraction, a text file was created by the first reviewer and checked for accuracy by the second reviewer. At this point, data collected from quantitative studies were transformed into qualitative data, enabling the synthesis of all data in qualitative form.
Data analysis and synthesis
The Segregated Framework for Mixed-Method Systematic Reviews (Sandelowski et al., 2006) guided data analysis and synthesis. Within this framework, the ‘Integrated Design’ model was used to synthesise transformed data. Data were thematically analysed in line with The Framework Method (Richie and Lewis, 2003), and NVivo 12 Pro (QSR International) was used to collate data for thematic analysis. Thematic analysis was performed by two reviewers and involved pooling codes, developing overarching themes and sub-themes, and further review and collapsing of themes which saw data synthesised to generate a set of overarching themes and interpretation of the findings. Results are reported to conform with the PRISMA Statement (Page et al., 2021).
Quality appraisal
Included studies were independently assessed by two reviewers for methodological validity. Diversity of methods across studies meant that a range of validated tools were used. The Critical Appraisal Skills Programme (CASP) Cohort Checklist (CASP, 2018a) assessed methodological quality of cohort studies; the CASP Qualitative Checklist (CASP, 2018b) was used for qualitative studies; the Joanna Briggs Institute Critical Appraisal Tools was used for case series studies (JBI, 2017), and the Mixed Methods Appraisal Tool (MMAT) was used for mixed-method studies (Hong et al., 2019).
Assessing confidence in evidence
Likewise, diversity of methods across studies meant that the use of an adapted tool was necessary to assess confidence in evidence in a standardised approach. An adaptation of the GRADE CERQual approach was used (Lewin et al., 2018). Outcomes of interest were as follows: (1) methodological limitations, (2) relevance of studies to research questions, (3) coherence of findings, and (4) adequacy of data supporting findings. Using quality appraisal results, two reviewers independently assessed each of the four components.
Results
Search results
Figure 1 provides an overview of the study selection process.
Overview of included studies
Study characteristics are outlined in Supplementary File 3. Studies were published between 1981 and 2021. All reported on paediatric clinics implemented in disadvantaged communities. Eight studies reported on clinics implemented in England, four in the United States of America, four in Australia, and two in Canada. Fourteen clinics were general child health clinics offering medical assessment and support to children in a particular age category living within the allocated catchment area. In addition, one community clinic focussed on the assessment and diagnosis of ASD, another specialised in children exposed to perinatal risks, and another was specifically a paediatric occupational therapy clinic. In terms of study design, five studies were quantitative cohort studies, seven were quantitative case series, two were qualitative case series, and four were mixed-method studies. All studies included children from birth to 18 years living in disadvantaged communities in high-income countries; seven studies focused on children from birth to 7 years, five studies included children from birth to 13 years, five studies included children from birth to 18 years, and one study focussed on practitioner’s perspectives of the impact of community paediatric clinics on child developmental outcomes.
Quality appraisal
Supplementary File 4 outlines the quality assessment process. We judged the overall quality of studies to be moderate. Strengths included clear reporting of methodological approaches and incorporation of reflexivity. Common weaknesses were lack of clarity regarding methods, lack of explicit research questions, and concerns with the interpretation of findings.
Translation of included studies
Data analysis identified four key outcome domains (themes), encompassing eleven sub-themes, reflecting community paediatric clinics and their role in supporting developmental services and outcomes for children living with disadvantage in high-income countries. Each sub-theme was supported by qualitative data and transformed quantitative data. Where relevant quantitative data were available for extraction, these were presented in tables.
Child-level outcomes
Identification of developmental delay
Ten studies reported on the identification of developmental delays as part of their primary outcomes (Blair et al., 1997; Didcock and Polnay, 2001; Edwards et al., 2020; Fox et al., 2007; Koushik et al., 2015; Mehta and Raman, 2014; Nicoll et al., 1986; Shulman et al., 2000; Sewell et al., 1986; Wong et al., 2012). Supplementary File 5 outlines developmental outcome categories and the percentage of children identified with a delay or concern. Behavioural, social, and emotional delays emerged as the most frequent areas of concern, followed by speech, language, and communication, and vision and hearing. Other areas included gross and fine motor delay, and learning and cognitive limitations. Studies found a significant number of children presented with multiple problems and disorders (Didcock and Polnay, 2001; Blair et al., 1997; Edwards et al., 2020; Fox et al., 2007; Koushik et al., 2015; Mehta and Raman, 2014; Shulman et al., 2000; Wong et al., 2012), particularly older children whose presentations reflected complex situations in which multiple interventions were required (Fox et al., 2007; Nicoll et al., 1986; Sewell et al., 1986; Wong et al., 2012).
Referrals to services
Seven studies recorded frequencies of children referred from clinics to other services (Brown et al., 2015; Edwards et al., 2020; Mehta and Raman, 2014; Nicoll et al., 1986; Shulman et al., 2000; Sewell et al., 1986; Wong et al., 2012). Supplementary File 6 provides an overview of service types and percentage of children referred. Children were most frequently referred to developmental services and medical specialists. Speech and language therapy, audiology, and ophthalmology were common developmental referrals (Edwards et al., 2020; Mehta and Raman, 2014). A significant number of referrals to family and child support services were noted.
Time to diagnosis
Two studies reported time to diagnoses of children attending community paediatric clinics (Koushik et al., 2015; Wong et al., 2012). Koushik et al. (2015) recorded a statistically significant difference between those who received a diagnosis prior to the clinic (M = 141.6, SD: 76.1) compared to those who attended the community clinic, (M = 87, SD = 36.6); t(36) = 2.7, p < .05. Prior to clinic development, patients received a diagnosis within approximately 5 months compared to less than 3 months after clinic implementation (Koushik et al., 2015).
Family-level outcomes
Attendance
Nine studies reported attendance rates at clinics (Smith and Gallego, 2021; Brown et al., 2015; McLeod et al., 2015; Maharaj et al., 2014; Didcock and Polnay, 2001; Blair et al., 1997; Spencer, 1993; Nicoll et al., 1986; Hart et al., 1981). Brown et al. (2015) found attendance at the 2-to-4-month routine visit increased from 68% to 79% and 35% to 59% since clinic implementation, as opposed to results from the control site where rates did not improve. Likewise, comparison studies reported a greater number of younger children, under the age of five years, attended a community clinic compared to a hospital clinic (Blair et al., 1997). Two comparison studies showed a marked difference in attendance rates of families living in more deprived areas than less deprived, highlighting the challenges vulnerable families face in accessing healthcare (McLeod et al., 2015; Maharaj et al., 2014). McLeod et al. (2015) found children living in the most deprived area within their study were 1.8 times more likely not to attend than those living in the least deprived area, and those living >7.5 km away from clinics were 1.2 times more likely not to attend than those living 4.8 km from clinics. Evidence highlighted how community paediatric clinics work towards increasing attendance of vulnerable families (Blair et al., 1997; Brown et al., 2015; Maharaj et al., 2014; Smith and Gallego, 2021). After the implementation of new processes for managing referrals into the community clinic, Maharaj et al. (2014) found non-attendance rates halved and the gap between the most deprived and least deprived areas closed.
Engaging vulnerable families
Six studies highlighted the importance of community clinician’s interpersonal skills and its value in terms of narrowing the gap in health inequalities by building trusting relationships with families (Blair et al., 1997; Edwards et al., 2020; Hart et al., 1981; Koushik et al., 2015; Lynam et al., 2010; Wong et al., 2012). Communication with families increased parental empowerment by providing them with knowledge of and how best to address children’s needs (Edwards et al., 2020; Koushik et al., 2015; Wong et al., 2012). Wong et al. (2012, p.9) found that interpersonal communication, particularly treating parents and caregivers with respect, was significantly associated with parental empowerment. Qualitative data emphasised the value parents and caregivers placed on communicating with community clinicians (Wong et al., 2012; Lynam et al., 2010). Parents reported feeling relief when issues were flagged in community clinics as a treatment plan to support their child could then be developed (Koushik et al., 2015; Hart et al., 1981). Community clinics were also found to be a source of advice for social issues, a service not always available within communities (Edwards et al., 2020; Hart et al., 1981; Koushik et al., 2015; Wong et al., 2012). Practitioners felt building trusting relationships with families was vital to supporting them to attend appointments (Edwards et al., 2020; Koushik et al., 2015; Wong et al., 2012). Finally, Blair et al. (1997) found that discharges occurred more frequently after the first visit to a hospital-based clinic compared to a community-based clinic, highlighting the emphasis community clinics place on building relationships with caregivers to ensure attendance at children’s health and developmental assessments.
Practitioner-level outcomes
Increasing community awareness of child developmental needs
Three studies reported on the benefits of community paediatric clinics on practitioner capacity building (Edwards et al., 2020; Heath et al., 2012; Sewell et al., 1986). Qualitative findings highlighted the confidence gained by early childhood practitioners who participated in training provided by the community paediatric clinic and how this newly acquired child health and development knowledge was incorporated within their professional practice (Edwards et al., 2020; Sewell et al., 1986). Referrals data emphasised how newly acquired knowledge and training influenced non-health workers in the community to increase their referrals of children at developmental risk to child specialists and other healthcare providers (Edwards et al., 2020). Findings also underscored the positive impacts of local practitioner capacity building on the quality of referrals to hospital consultants and health specialists (Heath et al., 2012).
Transferring specialist knowledge to the community
Three studies reported on expertise offered to communities by clinic paediatricians and multi-disciplinary teams (Heath et al., 2012; Lynam et al., 2010; Sewell et al., 1986). Qualitative data highlighted the importance of specialist knowledge on issues such as foetal alcohol syndrome, particularly relevant to the health needs of vulnerable communities (Lynam et al., 2010). Practitioners interviewed by Heath et al. (2012) felt a paediatric model of care that offered education and collaboration in the community was of significant value.
Child and family-centred model of care
Engagement and accessibility
Community paediatric clinics were found to employ a child and family-centred model of care which was accessible and encouraged engagement (Hart et al., 1981; McLeod et al., 2015; Smith and Gallego, 2021; Spencer, 1993; Wong et al., 2012). When comparing community- and hospital-based clinics, Spencer (1993) reported most caregivers favoured outreach clinics due to convenience (56%), better communication between community clinicians and other services (21%), and the advantage of familiar surroundings (21%). Likewise, parents and caregivers surveyed by McLeod et al. (2015) found community clinics to be less disruptive to daily life, and the comfortable setting was associated with more meaningful consultations. Two studies found barriers to healthcare access often include the rigid nature of traditional clinics requiring attendance during work or school hours, or that require families to wait for long periods (Smith and Gallego, 2021; Wong et al., 2012). Wong et al. (2012) examined the in-clinic wait times of families referred to a community clinic. Most families (87%) waited from 0 to 20 minutes to be seen, and caregivers emphasised the appeal of shorter wait times, particularly those who had children with high needs or sensory issues. Same-day appointments were arranged for families requiring urgent consultation (Wong et al., 2012).
Partnership working and shared goals
Both quantitative and qualitative data highlighted the importance of partnership working and shared goals among clinicians and local services (Brown et al., 2015; Heath et al., 2012; Lynam et al., 2010; Shulman et al., 2000). Collaboration with local child and family support services was frequently reported (Brown et al., 2015; Lynam et al., 2010; Shulman et al., 2000). Multi-disciplinary and multi-agency meetings to develop healthcare plans that most effectively meet children’s and families’ needs were commonplace in community clinics (Edwards et al., 2020; Lynam et al., 2010; Wong et al., 2012). Maharaj et al. (2014) found that deprived children were more than twice as likely to require multi-agency meetings as part of their medical care. Partnership working in disadvantaged communities was found to be essential for building relationships (Lynam et al., 2010). Local agencies were found to link with clinics to provide background information, allowing clinicians to support families with complex needs in a more sensitive manner. Quantitative data supported these findings as referrals from local services increased significantly following clinic implementation (Brown et al., 2015; Lynam et al., 2010). The benefits of partnership working were also reported through quantitative attendance data (Edwards et al., 2020; Hart et al., 1981; Koushik et al., 2015; Wong et al., 2012).
Management of non-attendance
Twelve studies reported on effective clinic structures and administration processes to manage non-attendance (Brown et al., 2015; Blair et al., 1997; Didcock and Polnay, 2001; Fox et al., 2007; Hart et al., 1981; Koushik et al., 2015; Lynam et al., 2010; McLeod et al., 2015; Nicoll et al., 1986; Smith and Gallego, 2021; Spencer, 1993; Wong et al., 2012). Two studies outlined interventions that used a standardised patient care path to track and identify children who missed follow-up appointments (Smith and Gallego, 2021; Koushik et al., 2015). Others described automated registries which prompted clinic staff based on children’s identified needs (Brown et al., 2015). One study examined the implementation of a hospital-based ‘drag and drop’ referrals model compared to a ‘choose and book’ system (McLeod et al., 2015). Findings showed a substantially higher rate of attendance associated with the ‘choose and book’ system which provided families with more choice regarding appointment dates and times. Lastly, Maharaj et al. (2014) enacted a system of ‘active management’ for non-attenders, facilitating multiple appointments to support engagement with families and to prevent loss to follow-up.
Tackling barriers to healthcare access
Several studies documented how the community clinic model tackles barriers to healthcare access (Brown et al., 2015; Blair et al., 1997; Didcock and Polnay, 2001; Fox et al., 2007; Hart et al., 1981; Koushik et al., 2015; Lynam et al., 2010; Maharaj et al., 2014; Nicoll et al., 1986; Shulman et al., 2000; Sewell et al., 1986; Smith and Gallego, 2021; Wong et al., 2012). Findings highlighted the challenges vulnerable families experience when trying to access prevention and early intervention services that require referral through formal community structures in a timely manner (Brown et al., 2015; Lynam et al., 2010; Sewell et al., 1981). Transport challenges and travel distances hindered families’ ability to access hospital-based health and developmental treatment (Smith and Gallego, 2021; McLeod et al., 2015; Lynam et al., 2010). Furthermore, vulnerable families were found to experience negative assumptions about their situations from health professionals (Lynam et al., 2010). Evidence underscores the value of community clinics to overcome the constraints structural and social barriers place on access to healthcare (Brown et al., 2015; Didcock and Polnay, 2001; Lynam et al., 2010; Wong et al., 2012).
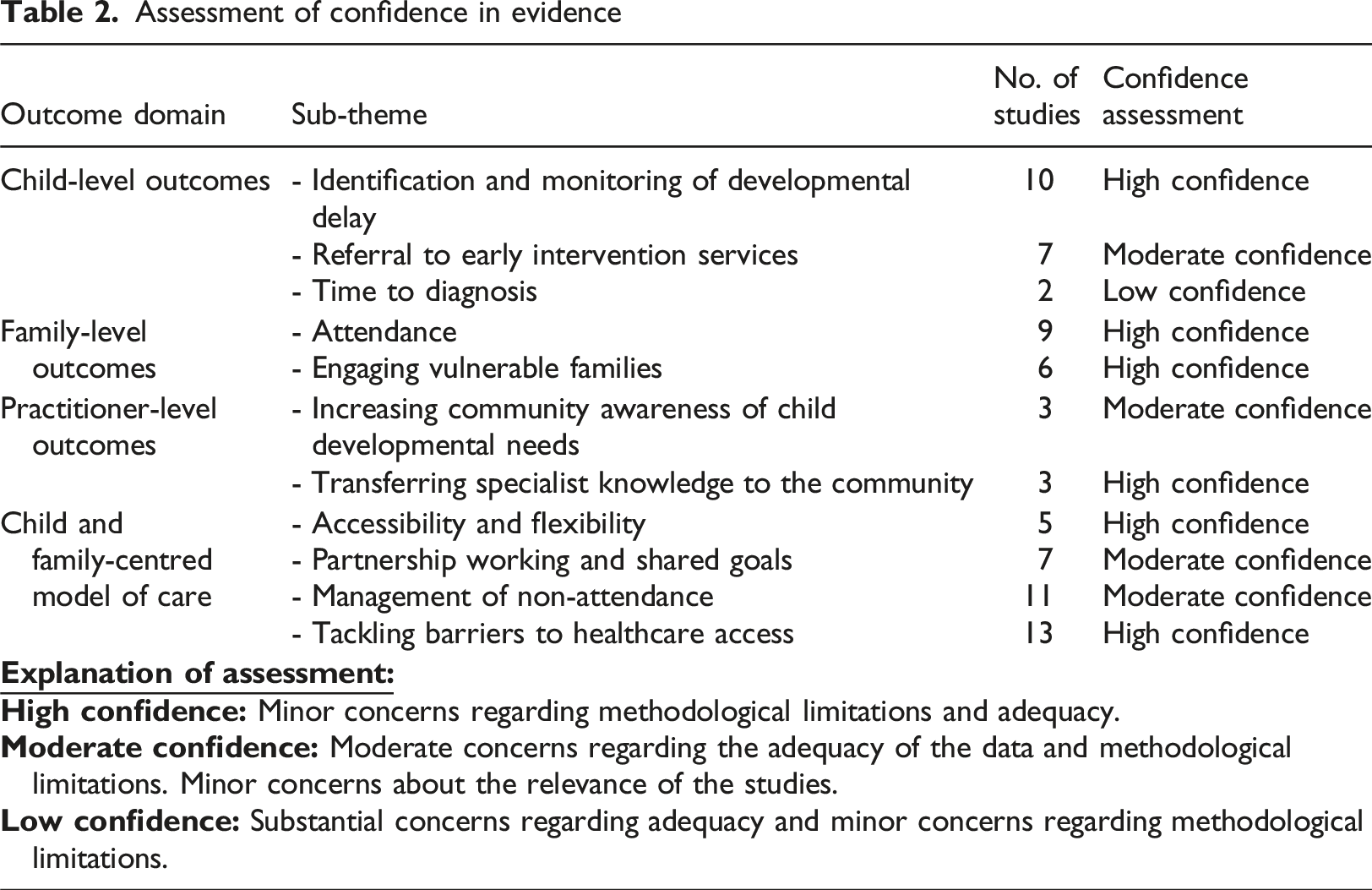
Confidence in evidence
Assessment of confidence in evidence
Discussion
We examined community paediatric clinics and their role in supporting developmental outcomes and services for children living in disadvantaged communities in high-income countries. Eighteen studies were identified, mainly observational primary research consisting of descriptive data. Methodological quality of studies was adequate, and confidence in evidence was deemed to be moderate. By systematically appraising and synthesising quantitative, qualitative, and mixed-method research on the topic, several key findings emerged. Community paediatric clinics play a significant role in (a) early identification and diagnosis of developmental delay, (b) engaging vulnerable children and families, (c) referring vulnerable children and families to early intervention and family support services, and (d) tackling barriers to healthcare access for vulnerable populations.
A key theme across clinics was the use of a child and family-centred model of care. This approach facilitated more responsive supports tailored to vulnerable children’s needs. Argal et al. (2022, p.6) argue that ‘family-centred models of care are mostly broad and/or conceptual, with less clarity on how to translate theory into practice’. Our study offers additional insights into effective child and family-centred models of practice. Of significance, the practice of relational working helped clinicians to build trusting relationships with families. Treating parents and caregivers with respect was found to encourage more active participation. In exploring the elements of family-centred care that are most meaningful to caregivers, Argal et al. (2022) found that families value communication and trust when working with health practitioners. Likewise, Pickering and Busse (2010) underscore the importance of increased communication and relational working when working with children with health needs.
Structures and administration processes within community paediatric clinics were found to effectively manage referrals and tackle non-attendance rates of traditionally harder to reach families. Caregivers and practitioners cited flexibility and accessibility of clinics as strong enablers to parental engagement and attendance. Findings underscore the importance of designing services that can meet families’ complex needs through a holistic approach and collaboration between local services at the point of delivery. Redder and Morris (2020, p.) conclude, ‘there is a gap in the literature which draws together the threads of knowledge that clearly explain the process/es by which parents and caregivers become empowered to work in partnership with health professionals’. Adopting an active management approach for non-attendance was found to be vital to ensure continued engagement by providing families with opportunities to attend additional appointments or to be followed up via the community clinic’s multidisciplinary network. Community paediatric clinics provide a comprehensive, accessible, and flexible service, while also being able to respond proportionately to children and families with higher levels of need.
Previous research on community paediatric clinics highlighted their benefits in terms of increasing collaboration among community practitioners, increasing patient satisfaction, adopting more efficient and guideline-consistent care, and less usage of in-patient services (Bowling et al., 1997; Bond et al., 2000; Bowling and Bond, 2001; Gruen et al., 2003; Komro et al., 2013; Powell, 2002). Calls have been made for further research on how health professionals can work with families to support and maximise children’s health and developmental potential in the early years (Kearney and Fulbrook, 2012). This systematic review offers valuable insights and contributes to the evidence on the significant role community paediatric clinics play in supporting developmental outcomes and services for the most vulnerable of children and their families.
Limitations
Although there is a wide geographical spread of clinics within included studies, our search yielded studies published in the English language only. Likewise, no time limitation was applied to database searches. Although this was useful to understand the true scope of available evidence, interpretation of some findings could be skewed due to changes in research methods over time and to cultural and societal shifts. We chose to explore community paediatric clinics located in disadvantaged areas in high-income countries only. While children across all countries would benefit from such comprehensive paediatric healthcare in their localities, primary healthcare services in low- and middle-income countries differ greatly to high-income countries. As our phenomenon of interest was the community paediatric clinic, we needed to ensure, as best as possible, parity of contexts across studies. A final limitation is the lack of control groups within the research, hindering the ability to measure the impact of community paediatric clinics. This review underscores the need for high-quality comparative studies which will add to the evidence base on the value of community clinics in disadvantaged settings where outreach may confer most benefit to access and health outcomes of vulnerable children.
Implications for practice and policy
This study offers strong evidence for an effective healthcare model which may encourage thoughtful examination of current service models within community paediatrics, particularly in disadvantaged areas. Findings support tackling health inequity via a child and family-centred model whereby clinicians adopt a relational approach to working with families, facilitating a service that is accessible to all but capable of responding proportionately according to levels of need. Community paediatric clinics have the potential to increase practitioners’ knowledge of child development across the spectrum of community health and family support services. This study generates important insights regarding healthcare supports valued by parents and caregivers which empower them to become active participants in their child’s health. Policy makers can utilise findings to tackle social and structural barriers to healthcare access for vulnerable children. Findings can also be used to address health inequities more broadly. In 2010 and more recently in 2020, Marmot concluded that sole focus on the most disadvantaged will not reduce inequalities sufficiently and action is needed across the social scale. This model of community paediatric care can facilitate improved access to specialist paediatric healthcare regardless of demographic, socio-economic, or geographical status.
Conclusion
This paper offers a comprehensive review and synthesis of the evidence available on community paediatric clinics and their role in supporting developmental outcomes and services for children living in disadvantaged communities. Findings indicate community paediatric clinics successfully engage vulnerable children and their families through a child and family-centred model of care, reducing health inequalities due to poor access. Clinics facilitate the strengthening of working relationships between medical practitioners and community agencies, aiding the detection, monitoring, and treatment of childhood developmental delay. Furthermore, parents and caregivers find ease of access, education on child behavioural and developmental problems, and liaison values as perceived advantages of attending clinics. Finally, community paediatric clinics provide disadvantaged areas with accessible specialist knowledge of child health and development, heighten community awareness of child development, and increase parent and professional choice. To reduce health disparities, Klein et al. (2011) underscore the importance of focussing on the broader dimensions of health to include factors which better address the needs of low-income and minority populations. This model of community paediatric healthcare can better meet the needs of vulnerable children and their families. Due to the greater prevalence of childhood developmental delay in disadvantaged communities, clinics must be prioritised and concentrated in these areas.
Supplemental Material
Supplemental Material – Community paediatric clinics and their role in supporting developmental outcomes and services for children living in disadvantaged communities
Supplemental Material for Community paediatric clinics and their role in supporting developmental outcomes and services for children living in disadvantaged communities by Lynn Buckley, Louise Gibson, Katherine Harford, Nicola Cornally, and Margaret Curtin in the Journal of Child Health Care.
Footnotes
Acknowledgements
We wish to acknowledge the main funders of the study, the Irish Research Council (Project ID: EBPPG/2019/197) and Let’s Grow Together Infant & Childhood Partnerships CLG Ireland. This work was part of a PhD project conducted through University College Cork Ireland in conjunction with the Structured Population and Health-services Research Education (SPHeRE) Programme Ireland.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Irish Research Council (Project ID: EBPPG/2019/197) and Let’s Grow Together Infant & Childhood Partnerships CLG Ireland.
Ethical approval
This review does not require ethical approval as persons were not involved directly in the study. This review is part of a wider PhD research project for which ethical approval has been granted by the Clinical Research Ethics Committee of the Cork Teaching Hospitals, University College Cork, Ireland.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.