
Abstract
Parents of children with non-malignant life-limiting conditions frequently accept roles that exceed the conventional activities of parenting in relation to the intensity, complexity and temporal nature of the family caregiver experience. This paper explores the prevalent and all-consuming experiences of parents caring for their children. A qualitative descriptive study design was used. Twenty-three parents (both mothers and fathers) were interviewed. Transcribed interview data were analyzed using thematic analysis. ‘Managing an unexpected life’ was the central concept when parents recounted ongoing efforts to address the emotional and practical effects of their child’s condition on their life and that of their family. Analysis revealed three main distinct but interrelated themes within the concept of ‘Managing an unexpected life’ helping us enhance our understanding of parents’ experiences: ‘Striving for normality’, ‘Becoming the expert’ and ‘Fighting for your child’. Findings suggest that the central concept of ‘Managing an unexpected life’ appeared to be in keeping with a caregiver’s career. Findings likewise suggest the need for improved and focused support and services to enhance parents’ career caregiving.
Introduction
The umbrella term ‘childhood life-limiting condition’ incorporates children with non-malignant as well as malignant conditions, with the range of conditions being extensive (Siden, 2018). Worldwide, there has been a marked increase in the number of children living with life-limiting conditions, and this trend is expected to continue (Bowers et al., 2020; Fraser et al., 2020).
The majority of children requiring palliative care are those with non-malignant life-limiting conditions (NMLLCs) (Siden, 2018). Advancements in both treatment and technology have led to prolonged life-spans for these children (Koch and Jones, 2018; Nageswaran et al., 2018). Consequently, more families will be embarking upon a trajectory of caring (Whiting, 2014).
When a child has a NMLLC, parental participation is heightened, as they have to respond to the extensive healthcare needs of the child, often over an extended period (Bailey-Pearce et al., 2017). Understanding the experience of parents is imperative given the gravity of a NMLLC and the child’s dependence on them (Bailey-Pearce et al., 2017; Courtney et al., 2018). While this importance is acknowledged, there is a paucity of studies which provide specific insights into parental experiences of caregiving (Collins et al., 2020).
Previous research has largely focused on parental stress and coping (Darlington et al., 2018; Oakley et al., 2021; Senger et al., 2016). Studies internationally have mainly focused on the perception of services (Noyes et al., 2018; Parravicini et al., 2018). Of the limited research, Courtney et al. (2018) explored mothers' experiences of caregiving when their child has a life-limiting neurodevelopmental disability and found that their overall experiences were characterized by a constant struggle. More research exists regarding the experience of caregiving among parents of children with cancer (Cox, 2018; Molinaro and Fletcher, 2018; Tang et al., 2020). While these studies are discerning, there is a need to specifically understand the experience of caregiving among parents of children with NMLLCs. On this premise, this paper aimed to explore the prevalent experiences of parents who are caring for a child with a NMLLC, together with their experience of support. This paper is part of a PhD thesis which explored the experience of caring for children with NMLLCs in Ireland and has not been published elsewhere (Hurley, 2020).
Aim
To explore the prevalent experiences of parents who are caring for a child with a NMLLC on the island of Ireland, together with their experience of support.
Methods
Research design
A qualitative descriptive study design was employed to attain a broad insight into parental experiences of caregiving.
Recruitment and sampling
A purposive sampling technique was adopted. An Advisory Group that included healthcare professionals and academics active in Children’s Palliative Care (CPC) practice and research on the island of Ireland oversaw the study’s execution, playing a key role in advising regarding recruitment. A children’s hospital, two children’s units within regional hospitals, a respite facility and a children’s hospice were among the five organizations that provided recruitment support. The organizations were all located in Ireland, with one in the north and two in urban and rural areas. Eligible parents (both mothers and fathers) were over eighteen years old and from a wide socio-demographic spread. English language proficiency was essential for study participation.
Ethics
Approval was gained from the Ethics Committee of the relevant University (DCUREC/2014/013) and from the five organizations involved in recruitment.
Data collection
Data were collected using single-occasion one-to-one semi-structured interviews. A topic guide was used. The guide was designed to examine parents’ experiences of parenting a child with a NMLLC. Kallio et al. (2016) suggest that rigorous development of a qualitative semi-structured interview guide contributes to the objectivity and trustworthiness of studies. An initial pilot interview was conducted with one parent to check the guide.
Data analysis
Thematic analysis was used to guide data analysis (Braun and Clarke, 2013). Verbatim transcriptions of the recorded interviews were made, verified for accuracy and then entered into QSR
International’s NVivo 10 software for data storage and management.
Each member of the research team undertook independent analysis and coding of two separate transcripts. The research team met to discuss the resultant set of codes and decide on future analytical direction. Subsequently, the research team undertook independent analysis of the same transcript and discussed similarities and differences in the resultant set of codes. This process resulted in the revision of codes and helped clarify and confirm the research findings. The research team then continued to check and came together on a number of occasions. One overall concept, ‘Managing an unexpected life’, comprising of three themes, emerged, helping us enhance our understanding of parents’ experiences of caregiving. Exemplars were selected.
To assure trustworthiness, the second author conducted all interviews and kept memos detailing interactions. Comprehensive observations concerning the child and family were recorded in the memos. The memos helped to systemize, relate and cross-reference data.
Findings
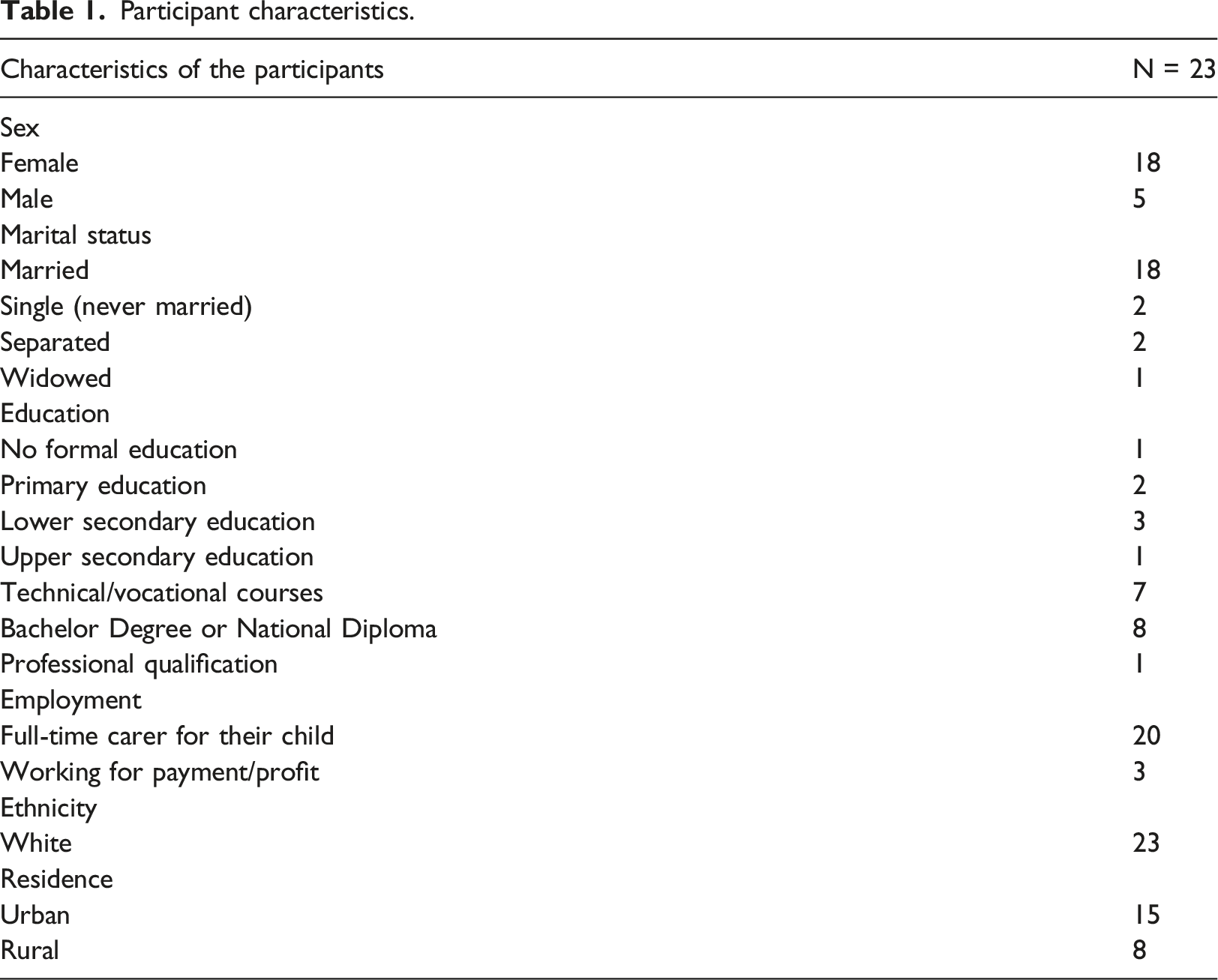
Sample size and participant characteristics
Participant characteristics.
The central concept: Managing an unexpected life
‘Managing an unexpected life’ was the central concept when parents’ recounted the ongoing process of care that was ever-changing depending on the child’s condition. Central to such management were attempts to respond to the resultant impact on their lives and that of their families. Analysis revealed three main distinct but interrelated themes within this concept, helping enhance our understanding of parents’ experiences, those being: ‘Striving for normality’, ‘Becoming the expert’ and ‘Fighting for your child’.
Parents talked about their realization that they had no alternative but to move forward and try to manage their new life. Nevertheless, they could only move forward and begin to manage when the powerful emotions felt at the time of diagnosis dissipated: ‘I was so upset when it happened first, I was crying and crying. But crying wasn’t going to change anything. I had to get up and get on and do the best that I could’. [Bridget]
What was evident was that while parental suffering had not entirely subsided, it had diminished from its peak intensity following the diagnosis. A few factors evident in parent accounts made the early management challenging.
First of all, accepting their situation required a protracted process of deliberation: ‘For the first few months I dwelled on, why us and why me?’ [Bridget]
Parents suggested that this was exhausting and that it practically paralyzed them from developing strategies that were now necessary for managing their new life. Secondly, parents considered how they had at first made a continual comparison between the child with the NMLLC and the healthy child they had anticipated having. With time, parents' aspirations were replaced by the reality of their child’s condition and the need to manage the new life they now faced. Undoubtedly, there were moments when parents were reminded of what they had lost as they watched others move through life’s milestones. Parents spoke of these occasions as being a time of renewed grief.
Parents' ability to cope with the situation appeared to be aided by having a practical focus: ‘I just focused on looking after her and playing with her and kissing her and cuddling her’. [Lisa].
The parents appeared to manage this new life out of a mixture of obligation and unrelenting love and devotion. ‘Managing’, however, was never a skill that was completely developed. Changes and deterioration in the child’s condition altered life again, which presented numerous new challenges and frequently rekindled grief reactions.
Parents, over time, seemed to realize that managing this new life was a never-ending task. Parental tenacity seemed to increase along with this insight: ‘when he got diagnosed as being blind, I thought, we've just got to find a way to cope’. [Deirdre]
Parents shared a communal goal for a ‘normal’ life. In an attempt to manage, parents strove to preserve normal routines and create a ‘new normal’. Thus, ‘Striving for normality’ emerged as a theme as it was a key component of ‘Managing an unexpected life’.
Striving for normality
A core element of the parents’ management strategies within their new life was unquestionably their determination relating to their shared goal for normality: ‘I wanted to be a normal mammy’. [Eleanor]
Achieving any semblance of ‘normality’ was essential and worthy of celebration. On the other hand, parents lamented the loss of normality as they continued their journey of caregiving, coming to realize that life would never be the same again. The diagnosis impacted every aspect of their lives. For the child, the parents and the family as a whole, it was crucial to recover control, equilibrium and stability.
Parents had to learn to juggle the numerous contending demands of family life together with caring for their children. Disruption to normal work life was inevitable, with many cutting back their hours or leaving altogether: ‘I would love to be able to go back to work’. [Karen]
The new normal created by parents was either partially or entirely devoid of the social possibilities they had previously experienced through work.
In the incessant strive for a ‘new normal’, relationships between parents evolved. Parents had to learn to adjust to the impact on their relationship, which for some, regrettably, meant disengagement: ‘It just kind of took its toll’. [Lisa]
Parents described how the child’s care demands frequently resulted in guilt over the effects on siblings. In the ‘strive for normality’, adaptation was necessary whereby one parent frequently attended to the needs of the child whilst the other met the siblings’ needs.
The isolation felt in the ‘unexpected world’ was intensified as support from friends often disappeared: ‘the longer you're on this journey the more people you lose along the way’. [Patricia]
Parents frequently defended this apparent desertion of their friends as a difficulty in appreciating the complexities of caring for their children while handling many competing demands in their family life. Parents often turned to other parents in comparable circumstances as a life-sustaining source of support. They felt that only parents in comparable situations could genuinely comprehend the daily challenges they encountered, so these parents became part of their ‘new life’ and part of the ‘new’ normal they strove to create.
Parents mainly discussed establishing and upholding normalcy in the home. However, the presence of equipment regularly encroached into the home, serving as a continual reminder that ‘normal’ life was undeniably altered. Nevertheless, parents thought that being at home was in the best interests of the child and family and represented a safer, more normal environment than the hospital. The ‘new normal’ was completely disrupted through periods of hospitalization: ‘it’s awful’. [Elizabeth]
Parents felt psychologically and physically exhausted as they strove to care for and protect their children in this setting, which was not the normality they had created for them.
As parents strove to maintain normal routines and create a ‘new normal’, they became proficient at organizing, including scheduling and fitting in appointments; formulating information for healthcare professionals (such as summarized medical histories); and being ready for emergencies. Care needed to be managed twenty-four hours a day and, for some, this involved significant disruption to sleep. Lack of sleep and continual strain made managing this new life extremely difficult: ‘we just make it work, but it’s really hard’. [Karen]
Parents gained expertise in managing their child’s care as well as responding to the needs of the whole family. So, managing this ‘unexpected life’ also had, at its core, developing the skills and expertise of parenting in a different way. It was truly a journey over time, henceforth ‘Becoming the expert’ arose as a theme given its centrality to ‘Managing an unexpected life’.
Becoming the ‘Expert’
Parents clearly articulated that their confidence and competence in their capacity to care for their children improved over time. Often correlated with a lack of trust in the ‘medical system’, they started to develop confidence in their own abilities, realizing that they could pay attention to their intuition, learn from their child and trust their own experience of caring for their child: ‘after his first smile I remember saying, I’m never going to trust any of those doctors again’. [Karen]
The emotional burden of providing the complex care also lessened, as a result of either a growing sense of acceptance and/or a belief that carrying out procedures had become simpler over time.
Parents wanted to view themselves first and foremost as parents and did not want their relationship with their child to be characterized by the nursing tasks they performed. They described dissatisfaction at the way in which their nursing role occasionally overshadowed their parenting experience: ‘sometimes I feel like his nurse and not his mammy and I hate it’. [Catherine]
Parents needed to identify their own boundaries. Setting boundaries was occasionally challenging. For instance, some parents had the option to assume responsibility for carrying out procedures, whereas others did not. Where parents did not have an option, this was occasionally due to limited service provision. However, the majority of parents lived in two-parent households, and among those, many shared responsibility for procedures with their spouse. Occasionally, fixed roles were assumed. In other situations, parents alternated between the many duties that were required. Where responsibility was shared with their partner, parents highly appreciated this.
In becoming the ‘expert’, parents gained a deep understanding of their child’s care requirements, which were seen as nuanced, unique and different. The need to become accustomed to fluctuating needs was at times daunting and, in the parents' opinion, could compromise their feeling of competence. Another matter for parents was the observation that healthcare professionals did not recognize them as ‘expert’. Occasionally, healthcare professionals positioned themselves as experts without considering the views of parents, which created frustration: ‘She doesn’t listen. It's frustrating, because it's hard enough’. [James]
Parents felt that genuine health concerns were regularly disregarded, and parents had to challenge healthcare professionals to take issues seriously. As a component of becoming an ‘expert’, parents gained self-assurance in their capacity to challenge the advice of healthcare professionals'.
Though parents unwittingly became the experts in their child’s care, they still needed education to acquire the new skills needed to meet the evolving needs of the child. In addition to education, parents reported a desire for ongoing assistance in managing their children’s ever-changing care needs. While parents noted times when their child’s condition was relatively stable, there were also periods of illness and decline when they needed ‘expert professional support’ in order to carry on in their parenting role. Parents spoke of the daily battles they had to wage for services and support in order to manage to care for their children and ultimately manage their unexpected lives. Hence, ‘Fighting for your child’ arose as a theme as it was an integral component to ‘Managing an unexpected life’ as parents saw it.
Fighting for your child
This theme relates to the parents’ resolve to fight on their child’s behalf, whether this meant obtaining a second opinion, looking into treatment possibilities or getting what the parents viewed as optimum levels of care for their child. Fathers and mothers fought intensely on their children’s behalf. Fighting was viewed as critical: ‘you have to fight’. [Anne]
However, parents described the physical and mental exhaustion they experienced as a result of fighting. They spoke of feeling resentful when fighting on behalf of their child dominated their parenting experience and characterized regular family life. Parents often felt isolated and unsupported in their fight: ‘Not one person has fought his corner for me….’ [Maria]
Parents expressed how they found this idea of fighting difficult because they could not afford to lose the support of influential healthcare professionals. As a result, parents appeared to be performing a balancing act. Withdrawal or the continual threat of withdrawal of services was an incessant source of worry: ‘every year they try to reduce his care, and that’s where my battle is, his condition hasn’t changed, nothing has changed’. [Elizabeth]
In fighting, parents described experiencing significant gaps in service delivery and the existence of a clear disconnect between what the child needed and what the services could offer: ‘her main need where physio is concerned is chest, the physio actually doesn't do chest physio’. [Patrick]
Parents claimed that there was not only a lack of funds for services but also a shortage of healthcare professionals who could provide those services, which reinforced the case for parental ‘fighting’.
The perception of a geographic imbalance in the distribution of services was another factor that affected parents' perceptions of the need to ‘fight’. Parents, in particular, spoke about out-of-home respite services. Additionally, some parents expressed discontent with the inappropriateness of the surroundings in which these services were offered: ‘There are no bright colours. There are no toys. Not one toy. I can't send him somewhere like that because it doesn't do us any good’. [Patricia]
When given the option to use out-of-home respite care, parents who had access to it said they simultaneously felt guilty and relieved. As in the situation mentioned above, parents' reluctance to use respite care was exacerbated if they were dissatisfied with the services offered. Even when the fight resulted in appropriate out-of-home respite, there were still issues. In some ways, it appeared to make parents feel that they had failed their child, but in reality, they needed it to refresh themselves with the strength to continue caring.
Obtaining in-home respite also posed many challenges, instigating battles for parents. The complex care required by the child made finding an appropriate healthcare professional difficult. As a result, in-home respite was typically scheduled around the requirements of the professional caregiver rather than those of the parents: ‘you are curtailed with their availability, but at the same time they are my saving grace’. [Karen]
In-home respite was perceived positively by all parents since it gave them the ability to manage their own circumstances. Such outcomes gave incentive and validated the fights that parents engaged in.
Many parents described their ‘battle’ to secure equipment they believed their children needed. Some parents declared defeat, finding and procuring their own equipment. Parents also mentioned how a lack of information contributed to prolonged fighting that was often needless. Information from other parents was determined as a significant source of information, serving as vital ammunition in their ongoing battles for their children.
‘Managing an unexpected life’ was a difficult and never-ending task for parents. Considering that these children had progressive conditions, this was unsurprising. However, parents used crucial action strategies to allow them to manage as effectively as imaginable.
Discussion
The central concept of ‘Managing an unexpected life’ has highlighted the prevalent and all-consuming experiences of caregiving amongst parents. Pearlin’s (1992) concept of the ‘caregiver’s career’ appeared to be a fitting way to understand parents’ experiences as they responded to the often sudden, always unwanted call into ‘an unexpected life’.
Many aspects, including the importance of background variables and characteristics of the caregiver, are considered within this framework (Pearlin, 1992). Identified originally by the role undertaken by spouses of individuals with dementia, the role undertaken as a carer was regarded as a fatalistic career with identifiable stages. In the first stage, known as the Encounter stage, caregivers confront the diagnosis and loss of their former life and acquire necessary skills. In the middle, or Enduring stage, caregivers manage extensive care routines while attempting to deal with social isolation. In the final, or Exit stage, the career is relinquished to some degree, either due to institutionalization or the death of the ill spouse. During the period of caregiving, the demands of the role change and, accordingly, the effects on the well-being of the caregiver are not constant.
Within this study, the ‘Encounter stage’ of this new life plunged parents into a world of learning new skills and parenting in a very unexpected way. Thus, parents seemed to have similar experiences to spouses of those with dementia in terms of emotional responses when they were catapulted into this world they did not know existed, a world they never wanted to be in. Parents experienced a panoply of changes, and they longed for their previous life. Parents' perception of the need to fight, particularly in terms of fighting for services, was central to the ‘Encounter stage’. Challenges encountered as parents embarked upon their caregiver’s career resonated with previous CPC research, including attempts to preserve aspects of normality (Courtney et al., 2018; Nicholl and Begley, 2012; Price et al., 2011; Steele, 2000), the requirement to become an expert (Mitchell et al., 2019), the tantamount battle with both the child’s condition and the battle for services and, most touchingly, the numerous evolving losses (Verberne et al., 2017).
Our findings provide evidence to support how, over time, parents take control of their child’s care through a combination of bonding, parental knowledge, empowerment and acquired expertise. This stage is similar to Pearlin’s (1992) second stage, that being the ‘Enduring stage’. During the ‘Enduring stage’, parental adjustment seemed to be a dynamic process as a result of changes in their child’s condition combined with fluctuating family needs. The growth of parental expertise in caring alongside coping with social isolation was apparent in this stage and is also described in studies incorporating parents of children with long-term conditions (Nightingale et al., 2014; Smith et al., 2015). Parents of children with complex chronic conditions reported diverse feelings concerning healthcare professionals’ acknowledgement of their expertise (Rafferty and Sullivan, 2017). Equally, parents in this study expressed similar feelings. Parents suggested contradictory expectations in that they felt they were prophesied to become experts while still deferring to the advice of healthcare professionals.
Entering the ‘caregiver’s career’ of parents requires compassion and skills from healthcare professionals in both the ‘Encounter’ and ‘Enduring’ stage. Appropriately assessing parental values, acknowledging felt losses and respecting individual managing strategies appear necessary to establish a therapeutic relationship. Recognizing and validating the role of ‘expert caregiver’ must be fundamental to care provision. Gibson’s (1999) pioneering study established a link between the notion of an expert mother and the empowering process. The challenge for healthcare professionals is to combine parents' knowledge with their clinical expertise in order to enhance care.
Though many parents obtain assistance from their partner and/or significant other, the support system of parents becomes significantly reduced, compounding the isolation they feel within the space they now find themselves. Evidence suggests that there is a substantial disparity in how parents adapt to the situation (Nicholas et al., 2016; Verberne et al., 2017). Connecting with parents in similar situations appeared to be particularly valuable. Social support has been identified as one of the best methods for managing and maintaining psychological well-being for parents of children with life-limiting conditions as they navigate the often protracted and always painful caregiving career (Coad et al., 2015; Collins et al., 2016; Nicholas et al., 2016).
Professionals' roles in determining the ever-changing requirements of the child with a NMLLC and their family as they navigate the staged process rely on regular assessment. Parents strive to create normality whilst focussing on complex caregiving. However, they are acutely aware of the certainty of their child’s death at an unknown time. At that time, the final or ‘Exit stage’ is when the child will die and the career is relinquished (Pearlin, 1992).
Strengths and limitations
The sample consisted primarily of mothers, given that few fathers volunteered to participate. Therefore, when interpreting the findings, it is worth noting the disproportionate representation of mothers, which may have concealed gender viewpoint disparities. This is, nonetheless, in line with earlier research in the field. Research indicates that the role of caregiver is often assumed by mothers (Smith et al., 2015). Henceforth, mothers’ perspectives often dominate research (Sabzevari et al., 2016). The study was carried out in Ireland, where the structure of the health care system may differ from other countries. However, the strength is that it encompassed the whole island of Ireland. Notwithstanding endeavours to include a diverse range of respondents, this sample lacked cultural diversity. The sample’s ethnic makeup was uniform, with all parents being White and of Irish descent. The requirement for English language proficiency may have influenced this. Future researchers should take a more active approach in terms of seeking opinions from parents of all ethnic backgrounds, particularly in light of Ireland’s rapid transformation into a multicultural society. A limitation often cited with qualitative research is difficulties in generalizing the findings. However, the findings do convey a depth of understanding of what it is like for parents caring for their children with NMLLCs. Nonetheless, it’s still simply a qualitative descriptive study. It is likely that we may have obtained greater richness by considering other qualitative designs. For example, adopting a phenomenological design may have facilitated greater insight into lived experience and meaning-making. Despite its limitations, our study contributes to knowledge in the revelation that numerous challenges are linked with becoming a caregiver. These challenges seem responsive to interventions. This could be a focus for further research to test this assumption in practice. As mentioned by Pearlin (1992), whose theoretical framework for role transition was adopted to conduct our study, knowing what to anticipate is inextricably linked to the transition process.
Practice implications
Reflecting back on the early stages, parents stressed the importance of receiving care that would have helped their acceptance process. They also alluded to the importance of timely advice catered to their particular circumstances as an intervention that would have facilitated them to manage. Henceforth, it is important to adopt a proactive intervention strategy from the beginning of the caregiver career to promote adaptation. Therefore, it is vital that healthcare professionals determine the support needs of caregivers promptly so that services provided closely match their requirements and expectations. It is essential to acknowledge that as parents continue on their caregiver’s career trajectory, their needs may change, alongside the changing needs of their child. Consequently, ongoing assessment is necessary. Realizing the nature of expert parents in respect of the characteristics that constitute becoming an expert would seem pivotal in facilitating a better parent-professional partnership.
Conclusion
This study reveals that parental experiences of caregiving can be conceptualized as a ‘caregiver’s career’. Like a professional career, the concept of a ‘caregiver’s career’ connotes a dynamic process where an individual moves through a series of stages, needing significant adjustments and restructuring of responsibility over time. For a caregiver, these stages include preparation for and acquisition of the caregiver role and carrying out related duties. Numerous patterns of change exist within these stages, such as the requirement for augmented support. It is imperative to note that the ‘caregiver career’ differs from a professional career in a number of ways (Ducharme et al., 2011). Parents in our study clearly articulated that becoming a caregiver is not characteristically chosen. As a result, preparation for this role will often occur once it has already been acquired (Koch and Jones, 2018). The role also contrasts with occupational careers in that advancement along its pathway is driven not by determination, but rather by progression of the conditions and dependencies generated. To conclude, unlike an occupational career, a caregiver career cannot be entered into or exited voluntarily. It appears to be a calling fuelled by unconditional love and sheer determination.
Copyright
The authors can confirm that the repository does not hold any copyright claims to the PhD thesis.
Footnotes
Acknowledgements
The authors would like to thank the parents who participated in this study and who gave so generously of their precious time. The authors would also like to thank the Gatekeepers at each organization for their assistance with regard to recruitment of participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the All-Ireland Institute of Hospice and Palliative Care (AIIHPC) and the Health Research Board (HRB).