
Abstract
Advancements in life-sustaining technologies have extended the lives of children with medical complexities, increasing demand for substantial healthcare services. Caring for these children requires significant caregiver time and energy, affecting their well-being. These experiences highlight a critical need for psychosocial interventions—like legacy-building—to foster adaptive coping, facilitate meaning making, and optimize outcomes for this population. This study explores how parents/caregivers of medically complex children perceive and experience the concept of legacy. Thirty-one parents/caregivers participated in semi-structured interviews, which were analyzed using inductive coding. Three themes emerged: (1) legacy is both what you leave behind and what you live right now, (2) legacy inspires change, and (3) legacy is shaped by healthcare experiences. Findings highlight the need for inclusive, adaptable legacy-building practices that address families’ unique needs and enhance psychosocial support for this population.
Introduction
The concept of “legacy” has gained attention in healthcare but remains underexplored in the care of children with medical complexity and their families (Keller et al., 2024). Between 0.7% and 11.4% of U.S. children are considered medically complex, a population characterized by multiorgan system involvement, chronic health conditions, and high healthcare needs (Cohen et al., 2011; Leyenaar et al., 2022; Teicher et al., 2023). Advances in medical technologies have improved survival rates, yet these children and their families face significant emotional, logistical, financial, and physiological challenges (Cohn et al., 2020; De Souza et al., 2025; Gallo et al., 2021; Holmes et al., 2024; Sidra et al., 2022). Caregivers often report disrupted family routines, emotional distress, and insufficient support systems (Holmes et al., 2024; Teicher et al., 2023; Willis et al., 2024; Yu et al., 2020), with contributing factors including chronic stress, lack of respite, and social isolation. Despite these challenges, psychosocial interventions remain limited. Legacy building offers a promising approach to foster coping and strengthen familial bonds through meaningful activities like handprint art or intentional shared experiences (Akard et al., 2021; Boles, 2014; Jones et al., 2022; Love et al., 2022). While widely studied in end-of-life contexts (Allen et al., 2008; Foster et al., 2012), legacy building as a lifelong process for families navigating medical experiences has only recently been explored (Boles et al., 2020; Boles and Jones, 2021; Cahalan et al., 2022; Daniels et al., 2024; Hirt et al., 2023; Jones et al., 2022; Keller et al., 2024).
Legacy building may take on unique forms depending on a child's abilities, influencing how it is understood and implemented. Critics argue that legacy interventions impose emotional labor on families or fail to balance perspectives of children and caregivers (Deng et al., 2025). Caregivers may struggle with societal expectations of legacy or reconciling their child’s individuality with their own memories. Research often overlooks potential negative emotions or unintended burdens associated with legacy building (Cahalan et al., 2022). Legacy may also involve reversing negative patterns, not just fostering positive traits (Edgoose et al., 2022; Franklin and Cheung, 2017). More research is needed to explore how legacy functions and how it can be effectively applied in pediatric healthcare settings.
Aim
The aim of this study was to address a critical gap in legacy research and explore how parents/caregivers of children with medical complexity understand and engage with legacy.
Methods
Study design
Given known geographic dispersion and varied experiences of families of medically complex children (Cohen et al., 2011; Leyenaar et al., 2022), this multi-site qualitative study was informed by Moustakas' (1994) psychological phenomenology because of the abstract social-emotional nature of its central focus: the concept of legacy. This approach utilized semi-structured interviews to capture rich, in-depth narratives while remaining flexible enough to explore the populations’ unique experiences (Boles et al., 2017).
Sites
Participants were recruited from two U.S. sites. Site 1, Monroe Carell Jr. Children’s Hospital at Vanderbilt, includes a 400-patient pediatric complex care service housed within a freestanding children’s hospital. Expedited Institutional Review Board (IRB) approval was obtained (protocol 220669). Site 2, LeBonheur Children’s Hospital, includes a 400+-patient multidisciplinary cerebral palsy clinic at a private orthopedic practice in Memphis, Tennessee. IRB approval was also obtained for this site (protocol 22-08836-XP). All participants provided written informed consent.
Population
Eligible participants were (1) primary caregivers of pediatric patients with complex healthcare needs treated at Site 1 or Site 2, who (2) spoke English, (3) were 18 years or older, and (4) volunteered to participate. Exclusion criteria included non-English speakers or those unwilling to provide consent. No additional criteria were applied to ensure diverse experiences.
Procedures
Care teams at both sites distributed recruitment flyers inviting parents/caregivers to schedule 30-min interviews in person, by phone, or via Zoom (version 5.14.0 manufactured by Zoom Communications Inc.). After providing consent, participants completed a demographic survey and a semi-structured interview guided by six questions adapted from prior legacy research (Boles et al., 2020; Dunbar et al., 2023; Goldberg et al., 2022; Jones et al., 2022, 2023). All interviews were audio recorded.
Analysis
Descriptive statistics summarized participant demographics. Interview transcripts underwent qualitative thematic analysis guided by Moustakas’ (1994) framework to mirror the team’s prior legacy research with other parent/caregiver, patient, and provider populations (Boles et al., 2020; Dunbar et al., 2023; Goldberg et al., 2022; Jones et al., 2022, 2023). Two researchers independently coded transcripts line-by-line before synthesizing codes into categories through iterative discussions. Themes were finalized by re-reviewing transcripts to ensure alignment with participant responses (Boles et al., 2017). Participants are referred to in the results section using pseudonyms to protect confidentiality (e.g., “Monique” for Participant 21).
Findings
General and clinical characteristics of the participants
Participant demographics and clinical characteristics.
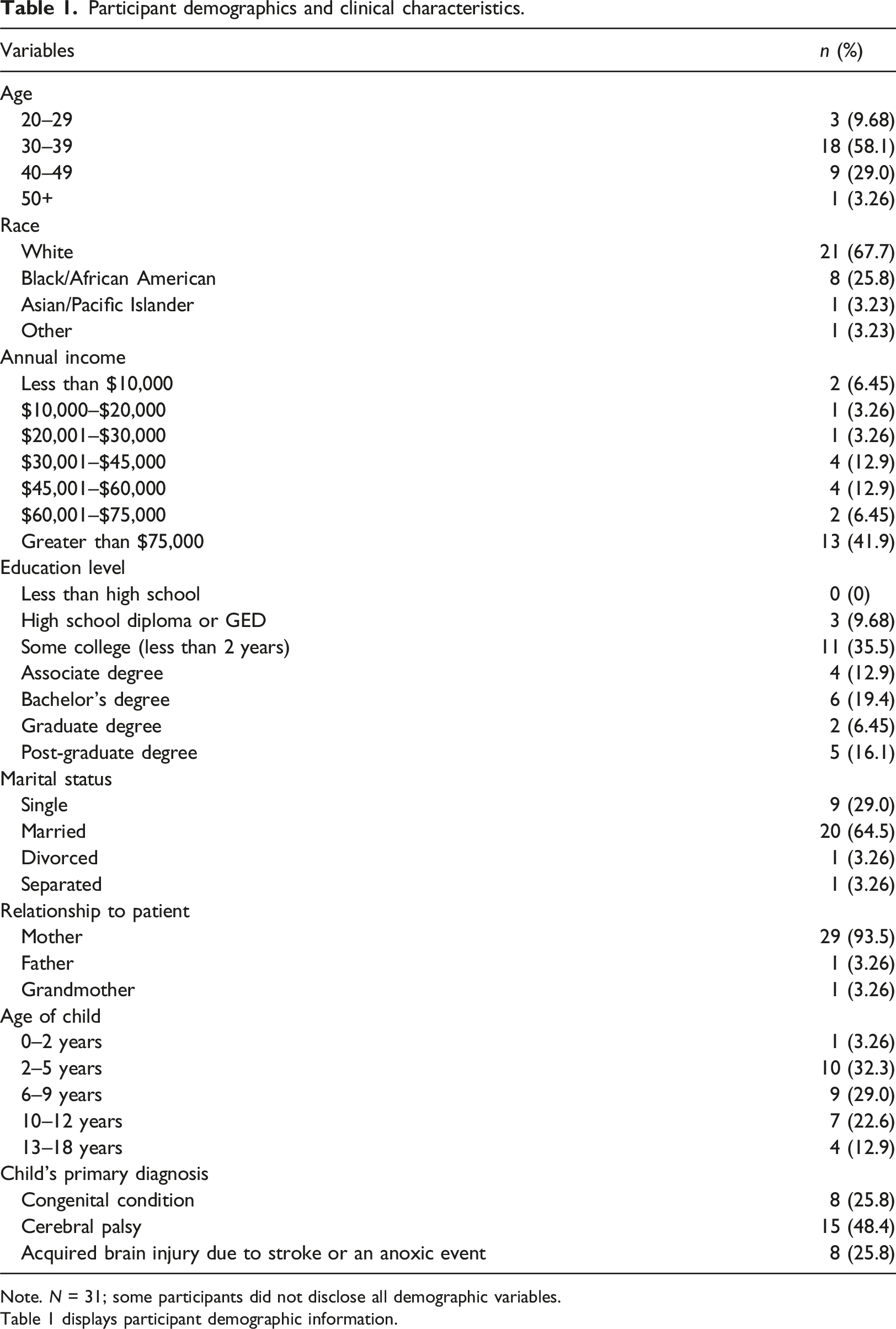
Note. N = 31; some participants did not disclose all demographic variables.
Table 1 displays participant demographic information.
Thematic results
Analysis identified three central themes: (1) legacy is both what you leave behind and what you live right now, (2) legacy inspires change, and (3) legacy is shaped by healthcare experiences. These themes collectively illustrate how participants interpreted legacy as an intersection of their current lives, lived experiences, and ways they hoped to be remembered posthumously. This notion of legacy also evolved to encompass their child’s unique contributions and personhood, reflecting ongoing efforts to preserve and amplify their significance within family and societal narratives.
Legacy is both what you leave behind and what you live right now
Participants defined legacy as the connection between their present lives, lived experiences, and hopes for how their children might be remembered after death. This concept was explored through three subthemes: (1) personhood, persistence, and progress; (2) history across generations; and (3) lasting memories of shared experiences.
“an extra chromosome of only love and joy” (Monique). “a fighter” (Brielle). “determined” (Tanisha). “the best and funniest person” (Lauren). “sassy” (Rochelle). “love that they can give and the spirit that they bring to the house” (Kiara).
This focus on personhood underscored a profound need for children with chronic illness or disability to be seen, recognized, and valued as individuals. Winona captured this sentiment while describing her son:
“He’s kind of magnetic and people kind of radiate to him and his smile kind of draws people in. Then when he talks with his eye gaze app it really draws people in and you see his personality and his sass and all the things that people would not even realize
–
that so many people just don't give him credit for.”
Despite societal stigma and limited understanding of these children’s abilities, participants highlighted their children’s personhood and rejected reductive assumptions. This strength-based approach demonstrated how participants appeared to actively resist the isolation and stigma their children often face due to chronic illness or disability. Participants also frequently emphasized legacy as persistence to overcome challenges and exceed expectations. For example, Mariah shared:
“His legacy will always be the thought of beating the odds because he has shocked and surprised every doctor and every medical staff member that comes across us by doing things that they never thought would be possible.”
Similarly, Rochelle recalled being told her son wouldn’t live to see his first birthday, sharing:
“I had a pediatrician tell me that I might as well get used to how it was, that he probably wouldn't even make it to his first birthday, and just in March we celebrated his tenth.”
It appeared evident that children’s resilience and achievements formed an essential part of their legacy, particularly in contexts where low expectations or stigma prevail.
“We represent the legacy our parents, grandparents, and great-grandparents left behind.... we have a duty being a product of that legacy” (Monique). “Your legacy is like to me like what you leave behind—the impression you made on the world and the people around you. I mean, I still talk about my grandparents and the influence they had on my upbringing and everything” (Ebony). “Being the unwanted child in the foster system with a disability has made me who I am today, taking the special needs children that are technically unwanted and caring for them because everybody deserves somebody to love them” (Amara). “Leaving something behind for my child” (Latrice). “Money, security, memories” (Vanessa). “Decisions we make” (Monique). “Traditions” (Taylor). “The things that matter that carry on through generations” (Winona).
“Legacy to me is any fun activities, especially the simple ones, like if it’s just her having a good day where she’s able to go to the park or when she makes new friends, that makes me happy. And I feel like all those little experiences are it.”
Participants described how shared memories with their children carried deep emotional significance, particularly in the context of grief and loss. For Winona, legacy was inseparable from memories of love and connection she had experienced:
“For me it's all about love and memories. Memories are huge for me. I have lost another child with special needs, so legacy is very huge for me.”
By ensuring their children were included in family activities and creating opportunities for connection, participants saw shared experiences as central to legacy. These memories embodied the love and care they sought to preserve and pass on.
Legacy inspires change
Participants described legacy as a means of educating and inspiring others but that the process of creating and preserving legacy was often constrained by social and systemic barriers. These included experiences of stigma, exclusion from community networks, and feelings of isolation resulting from the burden of care. Despite these challenges, participants demonstrated how legacy could be a tool for positive change, particularly in countering misconceptions and advocating for inclusion. This theme highlights two primary avenues through which legacy informs beliefs and inspires action: (1) teaching others and changing perspectives through advocacy, and (2) learning, growing, and creating connections through the community.
“There’s a lot of things that [my child’s] legacy could change if people would actually listen...bad experiences can impact legacy.”
For these families, creating and preserving legacy became intertwined with their broader fight for social inclusion. Overcoming stigma and advocating for greater understanding and acceptance was essential, not only to ensure their child’s legacy, but also to foster a more inclusive environment for all children with disabilities.
Participants also described their child’s legacy as a powerful vehicle for changing perceptions about children with disabilities. Through advocacy, they sought to challenge societal misconceptions and redefine what it means to live a meaningful life. For example, Kiana shared:
“The typical things that we think about... for success that was a successful life and legacy. I feel like he’s changed what that looks like for me. His mark on the world might look a little different, but it can be so great to help so many people.”
Parents often used everyday interactions as opportunities to educate others, as Maya explained:
“When people meet us and ask about her, we explain her situation and her diagnosis, and we try to educate people on her situation and allow them to be more aware because most people don’t realize that that’s something that does occur.”
Many participants described the emotional toll of advocating for their child in spaces where they encountered misunderstanding or dismissal. These frustrations highlight the dual nature of advocacy—while it serves as a means of preserving and amplifying their child’s legacy, it can also be an emotionally taxing endeavor.
“Empower each other with knowledge” (Simone). “Creating maybe more answers to somebody else later on” (Nia). “Some good to help somebody else in the same situation” (Destiny).
For some, these connections were deeply personal and rooted in their desire to support others navigating similar challenges. Hannah reflected:
“I’m
proud to be able to help someone with encouragement and let them know like it might sound sad right now especially to be diagnosed, it can be very dark... you can see a light in the darkness so if I could just be some kind of encouragement and send encouraging words to someone when they go through their life’s journey it means a lot to me because unfortunately I didn't have that support.”
Social media also emerged as a vital tool for creating connections and sustaining legacy. Many participants highlighted the practical and emotional benefits of using social media to share updates, gather information, and build relationships. As Zoe shared: “I was getting overwhelmed having to answer a bunch of phone calls and text messages. I wanted a place where I could just go and give an update and everybody that I wanted could see it.”
It also provided a way to access valuable medical information and support for participants, with Deja describing her use of online communities to research medical procedures, share insights, and prepare other families: “[We] research every procedure that we go through, and we talk to lots of parents that's been maybe been through it and just get everyone's opinion before we do each procedure. So, after each procedure, we go back to the other parents that are waiting and just explain the procedure. I think it just helps parents and children if they know what's going to happen and you're able to talk them through it... it just really helps calm them” (Deja).
Connections formed either in person or online reflected the deeply communal nature of legacy-building among families navigating the challenges of raising children with medical complexities.
Ultimately, participants viewed legacy as a means of advocating for inclusion, fostering connection, and countering stigma. Whether changing perspectives, educating others, or building supportive communities, legacy was seen as a deeply personal and profound social endeavor. In navigating barriers presented by disability stigma, families demonstrated the transformative power of legacy in creating a more inclusive and compassionate society.
Legacy is shaped by healthcare experiences
Participants in this study described healthcare experiences as an integral component of legacy, especially through encounters that either honored or challenged their child’s legacy.
“Feel heard, understood, and empowered” (Monique). “Providing a sense of comfort” (Aaliyah). “Having excellent bedside manners” (Alana). “Offering encouragement” (Vanessa). “Taking time to ask questions and listen” (Brooke).
Similarly, Winona described how a provider’s belief in her son’s abilities opened new doors:
“[His]
doctor at [study site] said there’s so much more inside this little boy if we can find a way to get it out. And if that doctor believed in him and
believed-
and
seeing that what we’ve seen in him and she’s the one that sent him for the trials for the eye gaze and because of her my son can speak.”
Such moments of provider-shared hope and encouragement were particularly impactful. Providers who took time to listen, collaborate, and respect parents’ expertise led to a shared partnership that honored their child’s legacy. For example, Alana shared: “He’s the best doctor we’ve ever had because he listened to us and he cared about what we said and he’s always said, ‘if you’re concerned, I’m concerned because you know your child best” (Alana).
Moreover, providers who demonstrated personal connection and compassion fostered a sense of belonging and inclusion, particularly for children who frequently interacted with the healthcare system. Brooke reflected:
“…when we come into the doctor’s office, it’s always a great experience. They make him comfortable by just talking to him, asking him questions, and he enjoys talking to any and everybody.”
Ayana and Mariah shared similar sentiments as they felt their child’s legacy was honored when staff took care of their child beyond just their clinical diagnosis and demonstrated empathy, patience, and compassion. Patrice reminisced: “…everybody knows [my daughter] because she has been there so long. Every time she comes, they (are) happy to see her. Everybody mostly gave her nicknames, where they call her by different names. So, their support with her is more understanding on my end because it shows they care.”
These positive interactions contributed to a narrative of empowerment and trust that helped families feel seen and valued. Participants also reflected on the broader role of healthcare providers in upholding children’s rights by ensuring that their voices and experiences are acknowledged and respected.
“The smallest role has an impact; one negative experience can make the overall visit/stay a bad one or vice versa” (Ayanna). “There have been times when doctors and nurses have not celebrated the milestones he has made because they were too focused on the milestones he has not made” (Mariah). “Some provider interactions felt dismissive, rushed, and condescending without getting to know [my child] on a more individual level” (Lauren). “Sometimes the team doesn’t know your child, and that team changes often, and oftentimes they don’t listen to you as a parent. And as a result, they make things harder for their child because they just want to be right. And want to do things their way” (Amara).
Finally, systemic challenges—including difficulties navigating insurance, accessing financial or material resources, or advocating for necessary care—were described as particularly exhausting and disheartening. Mariah explained:
“Fighting with insurance and the hospital to get care for [our child] it got to the point where we were both having panic attacks like the middle of phone calls and just daily panic attacks trying to navigate the healthcare system. Which is not [our child’s] legacy, just the legacy of the healthcare system.”
Discussion
Drawing from limited literature on legacy perceptions and interventions among children and families navigating illness and hospitalization, this study explored how parents of medically complex children understood and described the concept of legacy. Accomplishing this empirical aim expands and enriches the current legacy definitions and practices offered in healthcare settings, while helping to identify intervention priorities and adaptations best suited for the unique needs of this population. Participant responses were clustered around three themes: (1) legacy is both what you leave behind and what you live right now, (2) legacy inspires change, and (3) legacy is shaped by healthcare experiences.
Despite many limitations or challenges children with medical complexity and their families may face in medical and social contexts, findings from this study appear to align with recent research on the legacy perceptions of hospitalized children (Dunbar et al., 2023), parents/caregivers of hospitalized children (Jones et al., 2022), healthcare providers (Boles et al., 2020), bereaved parents (Jones et al., 2023), parents who have experienced infant or perinatal loss (Goldberg et al., 2022), and even adults living with psychological and substance-use disorders (Franklin and Cheung, 2017). Akin to these previous investigations, participants in this study regarded legacy as something that can be left behind, transmitted across generations, and represented through one’s personhood (Boles and Jones, 2021). Distinctively, however, participants in this study primarily reflected on the unique needs of children with medical complexity and how their medical experiences contributed to their legacy.
Like prior work with other populations (Allen et al., 2008; Boles et al., 2020; Cahalan et al., 2022; Daniels et al., 2024; Dunbar et al., 2023; Goldberg et al., 2022; Hirt et al., 2023; Jones et al., 2022, 2023), participants in this study spoke to legacy as something intergenerational, left behind through memories and shared experiences. Intangible values and memories passed down from grandparents, parents, or current family experiences all played a significant role in shaping participants’ understanding of legacy. Like conceptions of legacy reported in previous studies with pediatric patients (Dunbar et al., 2023), parents/caregivers (Jones et al., 2022), bereaved parents (Jones et al., 2023), and adult patients nearing end of life (Boles and Jones, 2021), participants in this study primarily described legacy as an accumulation of personality traits, characteristics, and qualities that they exhibit each day.
Despite the evident developmental or physical limitations of their child, participants in this study emphasized and described their child’s unique presence—and joy they bring to each interaction—as defining features of their legacy, rather than specific accomplishments or accumulations seen in earlier work as described by healthcare providers (Boles et al., 2020). This finding also closely aligns with bereaved parents/caregivers’ emphasis on how individual attributes of their child can translate into memory-making interventions (Love et al., 2022). Additionally, participants noted how their child’s persistence through adversity and progress throughout life stood as hallmark features of their child’s legacy, despite the often-conservative expectations others held for them.
Thus, it appears from this study that legacy manifests through someone’s traits and characteristics, especially as they evolve and grow throughout shared experiences. Likewise, participant responses emphasized legacy as a process that unfolded over time, challenging the idea of legacy as time-limited, intentional, tangible mementos created and reserved for intentional use at or near end of life (Akard et al., 2021; Allen et al., 2008; Foster et al., 2012). Considering this alongside recent work on legacy as a continuous process throughout life and illness (Boles and Jones, 2021; Cahalan et al., 2022; Daniels et al., 2024; Sisk et al., 2012), healthcare and psychosocial providers should conduct individualized assessments and strive to honor and support each child’s legacy throughout their medical journey—regardless of presumed abilities or prognosis. Such a shift challenges providers to dedicate genuine time and energy to each child and family to recognize strengths over deficits, celebrate accomplishments, and see beyond the child’s diagnoses, enhancing the child’s legacy in the present moment as they’re living through it.
Creating connections within the community and advocating to inspire change emerged as additional key elements of legacy for participants in this study. Advocating for their child and other children and families like them was a driving force of legacy in their lives. Like sentiments expressed by parents/caregivers (Jones et al., 2022), bereaved parents (Jones et al., 2023), and adults with co-occurring disorders (Franklin and Cheung, 2017), participants in this study saw legacy as a tool for education and change. Given the significant distress that parents/caregivers and children with complex medical needs experience (Cohn et al., 2020; Holmes et al., 2024; Teicher et al., 2023; Yu et al., 2020), individualized and collaborative care is vital in supporting and honoring one’s legacy. However, for legacy interventions to be effective, providers must take the time to listen to families, address concerns, provide resources, and facilitate opportunities to connect with other medically complex families. These opportunities can provide families with essential social and emotional support, helping them feel less isolated (Holmes et al., 2024). Additionally, providers must prioritize individualized assessment of legacy needs in an effort to optimize the quality of healthcare experiences, bolster community support, and strengthen familial bonds.
Finally, participants described the lasting impacts of healthcare experiences on the development and evolution of one’s legacy. Every interaction, according to participants, has the power to transform relationships and influence their child’s developmental progress or illness trajectory. While some caregivers shared positive memories of providers nicknames for their child and celebrations of their successes as legacy expressions, others relayed instances in which some providers challenged their child’s legacy by underestimating abilities or failing to provide resources and information. Given the increased healthcare service needs of this population (Gallo et al., 2021; Leyenaar et al., 2022), staff should make every effort to provide effective communication, comfort, encouragement, empathetic bedside manners, active listening, and family-centered collaboration from diagnosis onward. Shifting away from deficit-based care frameworks towards more strength-based approaches can help disrupt potentially stigmatizing narratives, create space for honoring diverse developmental journeys, and sustain long-term positive relationships between healthcare providers and families.
While earlier studies have explored the legacy experiences of patients and family members across inpatient settings, researchers to date have not explicitly addressed these in outpatient environments. This was the first study to recruit across multiple sites to understand legacy perceptions and needs of caregivers of medically complex children. Themes that emerged from this study translate into specific ways clinical staff and providers can adapt current yet outdated legacy interventions in a way that is inclusive and expansive to meet the needs of this population.
Limitations
Findings are limited by a primarily English-speaking sample from a specific U.S. region, leaving much less known about legacy needs and practices in other areas of the world. Future research should expand recruitment efforts nationally and internationally to ensure broader representation and explore cultural differences in legacy perceptions. Additionally, using a broader definition of “medically complex” captured varied experiences but may limit transferability to other populations and settings.
Implications for practice
Results of this study demonstrate that healthcare providers play a key role in shaping legacy through every interaction for this population. Employing practices that promote strength-based care, effective communication, and therapeutic relationships is essential to honoring a child’s legacy and providing high-quality healthcare. Furthermore, flexible and inclusive legacy-oriented interventions should be integrated into care protocols across the illness trajectory, highlighting caregivers’ perceptions and children’s individuality while prioritizing community-based networks and addressing systemic barriers such as stigma These can include things like allowing time and space for families to share stories, convey their child’s unique traits and interests (in or outside of their medical record), or even connect with other patients and families to swap insights and information. It is also essential to support families in sharing and celebrating milestones—whether expected or unanticipated, big or small—and offer ways for families to honor their child’s memory when death occurs. Further research is needed to evaluate psychosocial outcomes and refine these interventions for diverse populations.
Conclusion
This study provides novel insights into the legacy perceptions of parents/caregivers of children with medical complexity, adding to the existing literature that to date has only concerned typically developing or bereaved children and families. Findings highlighted the importance of family-centered care, celebrating individuality, fostering connections, and emphasizing empathy as each child lives their legacy in and beyond the hospital or clinic walls. Legacy, for this population, was not reserved for concrete moments, items, or activities created intentionally at or after death, but rather an ongoing process connected to every healthcare encounter and life experience, anchored in the past, present, and future all at once. By reframing legacy in this way, healthcare teams can intentionally recognize, support, and preserve every child’s legacy—especially those of children with medical complexity—throughout their healthcare journey.
Footnotes
Acknowledgments
The authors would like to thank the parents/caregivers who participated in the study. Authors would also like to thank Liz Peacock, China Tully, Briana Keller, and members of the CHILL lab at Vanderbilt University for their help and support.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical considerations
Our study was approved by the Vanderbilt University Medical Center Institutional Review Board (approval no.: 220669) and The University of Tennessee Health Science Center Institutional Review Board (approval no.: 22-08836-XP).
Consent to participate
All participants provided written informed consent at both sites prior to enrollment in the study.
Data Availability Statement
Data can be made available upon request.