
Abstract
Existing research suggests that children who experience poverty and hospitalization in early childhood are at risk of developing behavior problems. We examined whether the association between early childhood hospitalization and children’s internalizing and externalizing behaviors were moderated by family poverty status and child sex. Participants included 224 children from the National Institute of Child Health and Human Development Study of Early Child Care and Youth Development. There was no direct association between hospitalization and problematic behaviors. Poverty status during early childhood, but not child sex, significantly moderated the association between hospitalization and externalizing problems. Findings support the need for community programs that promote an integrative approach to healthcare for families experiencing poverty.
Keywords
Between 8 and 17% of preschool aged children are identified with clinically significant behavioral problems (Cree et al., 2018; Holtz et al., 2015). Children who display such internalizing behaviors as abnormal dependence on adults, headaches, or nail-biting might experience internal states such as anxiety, depression, social isolation, and/or withdrawal (Madigan et al., 2013; Stacks and Goff, 2006). Children who display such externalizing behaviors as arguing, fighting, having trouble sitting still, or impulsivity might struggle with aggression, impulsivity, and/or hyperactivity (Achenbach, 1991; Stacks and Goff, 2006). Internalizing and externalizing behaviors in early childhood have become the focus of recent study, as these problematic behaviors can have detrimental effects on children’s development and lifelong success (Brennan et al., 2012; Sasser et al., 2016). Several child characteristics and experiences have been found to influence the development of behavioral problems. For example, there are sex differences in children’s presentation of behavior problems, with females more likely to exhibit internalizing behaviors and males more likely to present externalizing behaviors, comparatively (Achenbach, 1991; Ormel et al., 2005). Further, research has shown that children exposed to poverty are at greater risk of developing behavioral problems in early childhood and of experiencing hospitalization (Huaqing Qi and Kaiser, 2003; Stormont, 2002).
Compounding the issue, hospitalization in childhood has been shown to increase problem behaviors (Levy et al., 2008; Rennick et al., 2004; Small, 2002). Most studies examining the effects of hospitalization on children’s development are limited by their designs (McCartney et al., 2006; Rennick and Rashotte, 2009). For example, research testing the association between hospitalization and behavior problems primarily have used nonexperimental or correlational designs (Rennick and Rashotte, 2009). These research designs limit the causal associations that can be drawn between exposure (e.g., hospitalization) and outcome variables (e.g., behavioral outcomes; McCartney et al., 2006). Few studies have compared children who have been hospitalized to children who have not experienced hospitalization (Rees et al., 2004; Small, 2002), particularly on problematic behaviors. Thus, it is unclear if behaviors observed in hospitalized children would have developed even if they had not experienced hospitalization.
Hospitalization in childhood
According to the fundamental cause theory of disease, differential access to socioeconomic resources can impact health through multiple mechanisms (e.g., access to health services, health literacy, and social networks) and contribute to health disparities (Link and Phelan, 1995). In support of the theory, researchers have found that children from impoverished families are more likely than their affluent peers to be hospitalized due to risk factors including poor health, low child birthweight, and poor preventative health practices (Kersten et al., 2018; Larson and Halfon, 2010) and that family income is a primary predictor of healthcare outcomes (Levy et al., 2008).
Children who experience poverty are in worse health than more affluent children (Levy et al., 2008) and are at risk of asthma, obesity, acute illness, and injury (Chen et al., 2002, 2006a, 2006b). Families living in poverty are more likely to utilize acute care clinics and emergency departments, and are less likely to attend primary care visits compared to families not living in poverty (Kersten et al., 2018; Larson and Halfon, 2010), resulting in greater levels of hospitalization for children from poor families (Brooks-Gunn et al., 1998). Given the prevalence of hospitalization during childhood, especially for children who experience poverty, understanding the effects of hospitalization on child development is of critical importance.
Hospitalization and child development
In general, 10–15% of preschoolers display mild to moderate behavioral problems (i.e., internalizing and externalizing; Campbell, 1995), but hospitalized children might be more likely to display internalizing and externalizing behaviors, given the stress associated with hospitalization. Previous research, primarily focused on the degree to which children exhibited internalizing or externalizing behaviors prior to and after hospitalization (Small et al., 2009; Small and Melnyk, 2006), has found that children between 2 and 7 years old who exhibited high levels of problem behaviors prior to hospitalization experienced a greater increase in these behaviors after discharge compared to children with lower levels of problem behaviors prior to hospitalization (Small and Melnyk, 2006).
Although children in early childhood are likely to display internalizing and externalizing behaviors as a result of their developmental age, environmental, and child-level risk factors can increase the likelihood of exhibiting problematic behaviors (Cree et al., 2018; DeCarlo Santiago, 2011). Family income is a risk factor that might influence children’s problem behaviors through multiple mechanisms. For example, children and adolescents living in poverty are more likely to exhibit internalizing and externalizing behaviors compared to more affluent children (DeCarlo Santiago et al., 2011). Research has identified sex differences in the effect of hospitalization on internalizing and externalizing behaviors, with males more likely to exhibit problem behaviors than females (Tiedeman and Clatworthy, 1990). As early as age 5–11, males exhibit more anxiety than females at admission, discharge, and after hospitalization (Tiedeman and Clatworthy, 1990). Furthermore, males are more likely to display and maintain internalizing and externalizing behaviors than females after hospitalization (Tiedeman and Clatworthy, 1990). These findings highlight the need to examine exposure to poverty and sex when considering the effects of hospitalization on the development of behavior problems in early childhood.
Aims
The present study had two aims: (1) to investigate the association between ever being hospitalized in early childhood and the development of internalizing and externalizing behaviors prior to kindergarten, and (2) to examine if family poverty status and/or sex moderate this association. Based on previous literature, the following hypotheses were explored: (1) hospitalized children would exhibit higher levels of internalizing and externalizing behaviors than children who have not been hospitalized; (2) the association between hospitalization and internalizing and externalizing behaviors would be stronger for children from poor families than for children who did not experience poverty; and (3) the association between hospitalization and internalizing and externalizing behaviors would be stronger for males than females.
Method
Population
Child and parent observations were drawn from the National Institute of Child Health and Human Development Study of Early Child Care and Youth Development (NICHD SECCYD). The NICHD SECCYD collected data through at-home interviews, questionnaires, observations, and telephone contact at various time points in early childhood. Telephone contact that included family updates were conducted at 18, 21, 27, 30, 33, 42, 46, and 50 months. Home interviews were conducted at 1, 15, 24, 36, and 54 months. Observations and questionnaires were completed in the home or lab at 6 and 54 months. See supplementary material for description of each variable’s collection time point and collection method. Further information regarding data collection procedures is included in the Manuals of Operation of the NICHD SECCYD (NICHD Early Child Care Research Network, 1993).
Measures
Hospitalization
Questions asked during data collection interviews and telephone calls were similar although not the same at every wave, including questions on the child’s health, hospitalization, check-ups, and reasons for illness or injury. The questions about hospitalization typically included “Has (child) seen a doctor or other medical professional or visited a clinic or emergency room since (X month call)?”. The mother was then asked, “Was child hospitalized?”. To measure hospitalization, a binary variable was created at each time point to represent if a mother reported a child to be hospitalized at 15, 18, 21, 24, 27, 30, 33, 36, 42, 46, 50, or 54 months for prior conditions, illness, injury, or other reason. Next, a binary variable “ever hospitalized” was created in which a child received a 1 if the child was ever hospitalized between 15 and 54 months.
Internalizing and externalizing behaviors
As a measure of their child’s current social competence and behavior problems, mothers completed the Child Behavior Checklist (CBCL; Achenbach, 1991) when the child was 54 months old. The CBCL is valid, reliable, and internally consistent and represents both broadband and narrowband measures of children’s adjustment and problem behavior (Achenbach, 1991). Items measure a series of behaviors (100 items) rated on a 3-point scale from 0 (not true of the child) to 2 (very true of the child). Empirically derived syndromes are scored with standard computer programs to generate narrow band syndrome scores (e.g., social problems, depression, delinquency, aggression, and attention problems) and broad band syndrome scores (externalizing behavior problems, internalizing behavior problems, total problems). Internalizing Behavior Problems combines the Social Withdrawal, Somatic Complaints, and Anxiety/Depression scales, while Externalizing Behavior Problems combines the Delinquent Behavior and Aggressive Behavior scales (Achenbach, 1991). Raw scores from the CBCL are converted to standardized T scores based on age and sex. T scores less than 60 are considered in the normal range, 60–63 represent borderline scores, and scores greater than 63 are in the clinical range (Achenbach, 1991).
Moderator variables
Child sex (male, female) was recorded during recruitment at the hospital. Family poverty status was also reported during home visits throughout early childhood. A binary “poor/not poor” variable was created at each time point (1, 6, 15, 24, 36, and 54 months) by calculating poverty thresholds based on household size and income-to-needs ratio. The ratio was computed by dividing family income by the poverty threshold for each household (U.S. Department of Labor, 1994). Next, a binary “ever poor” variable was created to assess if children were ever below the poverty line during early childhood.
Selecting covariates for propensity score analysis
Measures reported by mothers at the 1-month interview were used to estimate the propensity score. Maternal age was measured in years. Maternal, paternal, and child race were chosen from the following options: American Indian, Asian or Pacific Islander, African American, White, or Other. Mother, father, and child Hispanic ethnicity were collected as binary questions (no, yes). Race/ethnicity was coded as a binary variable of White non-Hispanic or other race/ethnicity because of the predominance of White non-Hispanic participants in the study and the small number of participants identifying as other racial/ethnic groups (Ross et al., 2020). Marital status was used to create a binary variable of “living together/not living together”. Maternal and paternal education were separately dummy coded to indicate having at least a high school diploma or GED (0: < high school degree or GED, 1: >= high school degree or GED).
During recruitment, mothers reported on the child’s birth weight (grams) and gestational age (weeks). At 1-month interview, the mother reported on health measures related to the baby. Type of delivery included three choices of vaginal delivery, planned c-section, or emergency c-section. A binary variable for type of delivery was created for “vaginal/not vaginal” birth. Two variables were combined to measure length of stay for the child. Mothers reported on how many days the baby stayed in the hospital. Complications after delivery was a binary variable of yes or no. Child’s health was rated as poor, fair, good, or excellent, then health of the baby was coded as a binary variable rated as “poor/fair” and “good/excellent”. Respiratory problems (including runny nose, cough, or cold) and intestinal problems (including vomiting, diarrhea, and not eating) were assessed with two yes/no questions. Preventative care for the baby such as attending routine check-up was reported by mothers through a yes/no question.
Child temperament was collected in-home when the child was 6 months old through the Revised Infant Temperament Questionnaire (McDevitt and Carey, 1978) with reliability and validity previously demonstrated (Slabach et al., 1991). Maternal sensitivity was assessed through the Mother-Child Interaction Semi-Structured Procedure based on previous findings on qualities of parenting and development of secure attachments for children (Egeland and Farber, 1984). Maternal sensitivity was rated by objective observers using 15-minute videos of mother’s interacting with their children during free play, collected at the 6-month home visit (no previous studies evaluate psychometric properties). Maternal social support was collected in-home at 1-month using the Relationships with Other People instrument (Marshall and Barnett, 1993). Reliability was high (α = .91) and maternal sensitivity was significantly correlated with depression (r = −.38, p < .001), anxiety (r = −.23, p < .001), and physical health as measured by physical symptoms (r = −.20, p < .001). Although the distribution of maternal social support was skewed, previous research has not transformed the data (Bono et al., 2016). Maternal mental health was collected using the Center of Epidemiological Studies Depression Scale (CES-D) during the 6-month home visit (Orme et al., 1986) and was log transformed due to skewness. Internal consistency was high in the general population (α =.85) and in the clinical sample (α =.90), and high correlations between the CES-D and other measures of depressive symptoms have been demonstrated (Orme et al., 1986). Maternal substance abuse and environmental smoke exposure was determined by mothers reporting on a two-item binary questionnaire (Overpeck and Moss, 1991; Sexton et al., 1990; Tager, 1991).
Analytic approach
Utilizing propensity score matching, the present study compared children’s behavior problems (i.e., internalizing and externalizing) at 54 months in a sample of children who were hospitalized in early childhood (between 15 and 54 months) to a matched control sample of children who were not hospitalized in early childhood. We also examined poverty and child sex as potential moderators of the association between hospitalization and behavior problems.
Descriptive statistics for childhood hospitalization, problematic behaviors, and propensity score matching covariates.
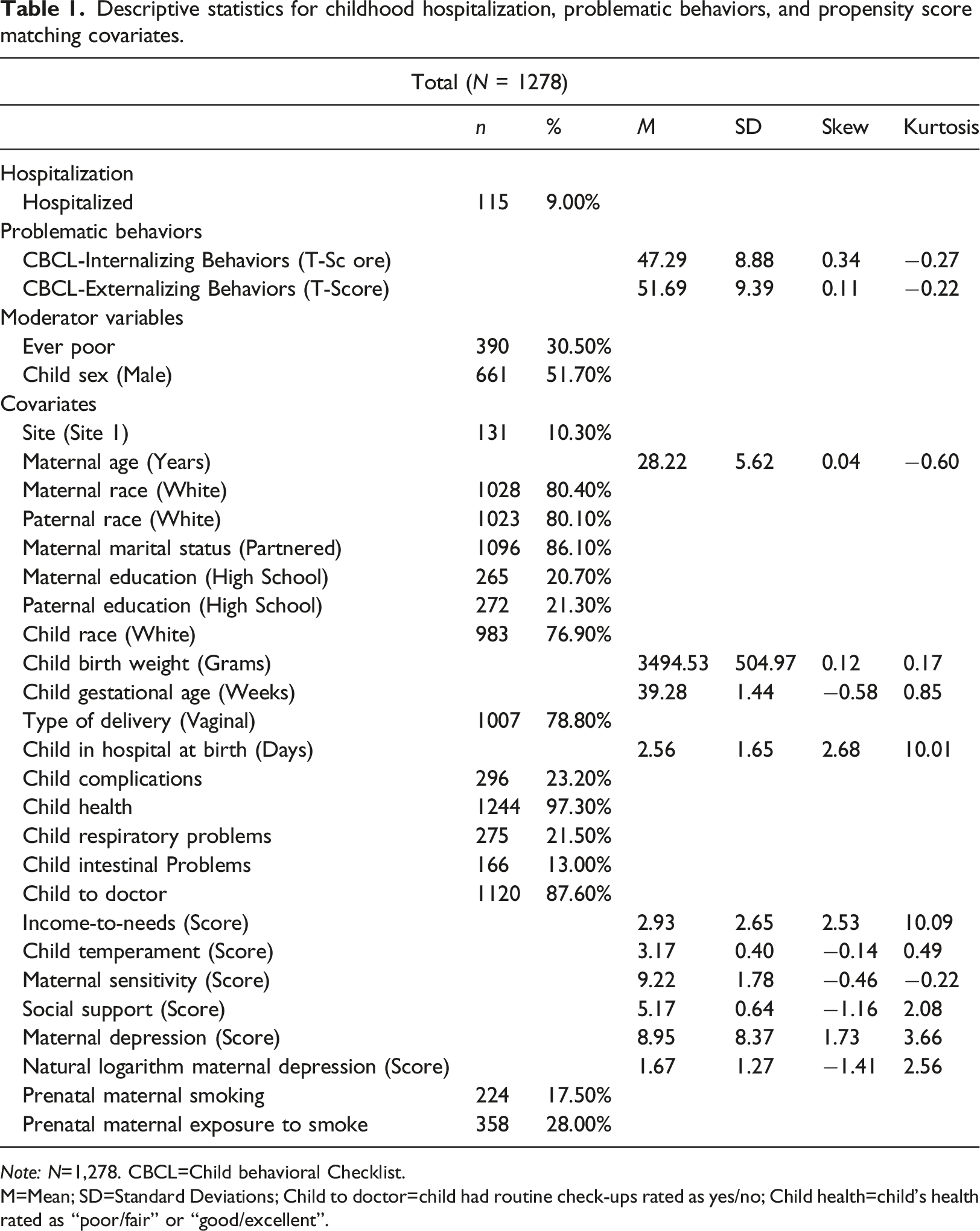
Note: N=1,278. CBCL=Child behavioral Checklist.
M=Mean; SD=Standard Deviations; Child to doctor=child had routine check-ups rated as yes/no; Child health=child’s health rated as “poor/fair” or “good/excellent”.
Missing data
Of 1364 children in the original study, 1278 children were considered for inclusion based on complete outcome data. Multiple imputation was used on the sample of 1278 participants using Blimp 3.0 (Keller and Enders, 2021). The imputation model included all observed variables and the hypothesized moderator interactions of hospitalization and sex and hospitalization and exposure to poverty (Von Hippel, 2009). After creating 20 imputed datasets, analyses generate parameter estimates and standard errors that are combined in a pooling phase (Graham et al., 2007; Enders, 2010). SPSS 28 does not allow data to be pooled when estimating propensity scores, thus, pooling for this phase was handled manually. Pooling the propensity score analyses consisted of averaging parameter estimates and standard errors.
Estimating the propensity score and outcome models
Balancing of the matched sample covariates and propensity score averages.
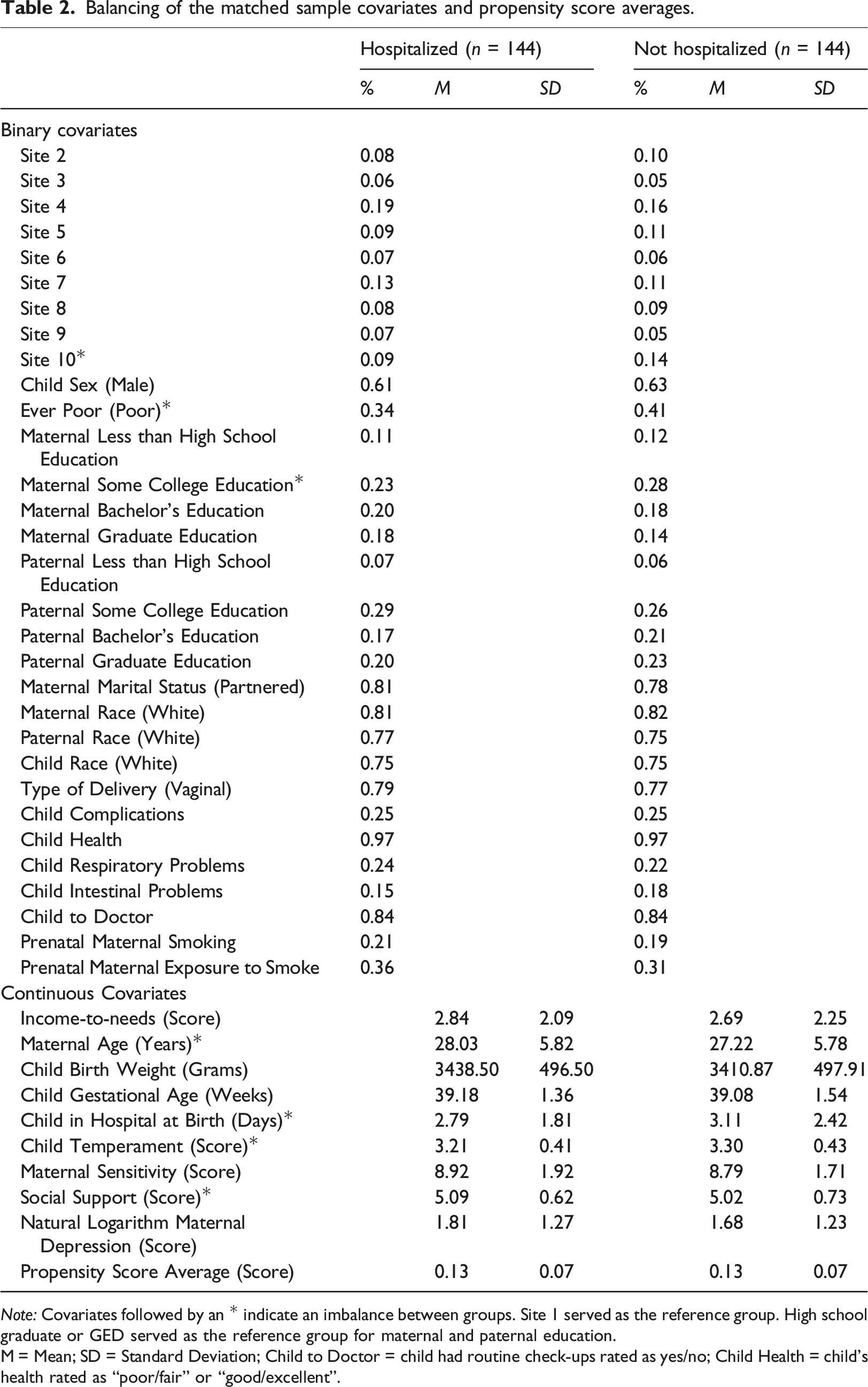
Note: Covariates followed by an * indicate an imbalance between groups. Site 1 served as the reference group. High school graduate or GED served as the reference group for maternal and paternal education.
M = Mean; SD = Standard Deviation; Child to Doctor = child had routine check-ups rated as yes/no; Child Health = child's health rated as “poor/fair” or “good/excellent”.
Using the sample of hospitalized and non-hospitalized children matched on propensity scores, hypotheses were tested using a multivariate multiple regression approach in SPSS 28 (IBM Corp., 2021). Multiple regression was appropriate because internalizing and externalizing behaviors are continuous outcomes that are normally distributed. In the first model, the main effect of hospitalization on problematic behaviors was examined. Next, two separate models examined main effects for hospitalization and poverty status and sex on problematic behaviors. Third, two additional models examined the moderating effect of poverty status and sex on the association between hospitalization and problematic behaviors. These two models included measures of hospitalization, poverty status, or sex, and a variable capturing the multiplicative interaction between hospitalization and poverty status or sex. For example, to test whether the association between hospitalization and externalizing behavior differed for children who did and did not experience poverty, a categorical variable capturing each combination of hospitalization and childhood poverty was included in the regression model, with children who were hospitalized and did not experience poverty as the reference category. Similarly, children who were hospitalized and female served as the reference group when examining the interaction between hospitalization and sex.
A fourth set of models were used to examine the robustness of moderated effects when including covariates that were unbalanced in the propensity score matching process (Nguyen et al., 2017). False Discovery Rate was calculated for the hypothesized effects (i.e., hospitalization, poverty status, sex, and moderated effects) to reduce the potential for Type I error due to multiple testing (Benjamini and Hochberg, 1995).
Results
Prior to conducting analyses, the sample was reduced from 1364 participants to 1278 participants to exclude individuals without complete data on hospitalization. This inclusion criterion was established to avoid the possibility that hospitalization would be imputed for children who dropped out of the study prior to 54 months. See Table 1 for description of characteristics of the total sample. Of the 1278 participants, 228 children were included in the matched sample. Demographic characteristics were compared for the matched (n = 228, 17.80%) and unmatched groups (n = 1,050, 82.80%), with two significant differences identified. There was a significant difference for sex (X 2 = 11.38, p < .001) and mothers’ Ethnicity/race (X 2 = 4.19, p =.041) between the children included in the matched and unmatched samples, with a higher percentage of males in the matched sample and a higher percentage of mothers who were a race/ethnicity other than White non-Hispanic in the unmatched sample.
Main effects and moderation of hospitalization and problematic behaviors on poverty, status, and sex.
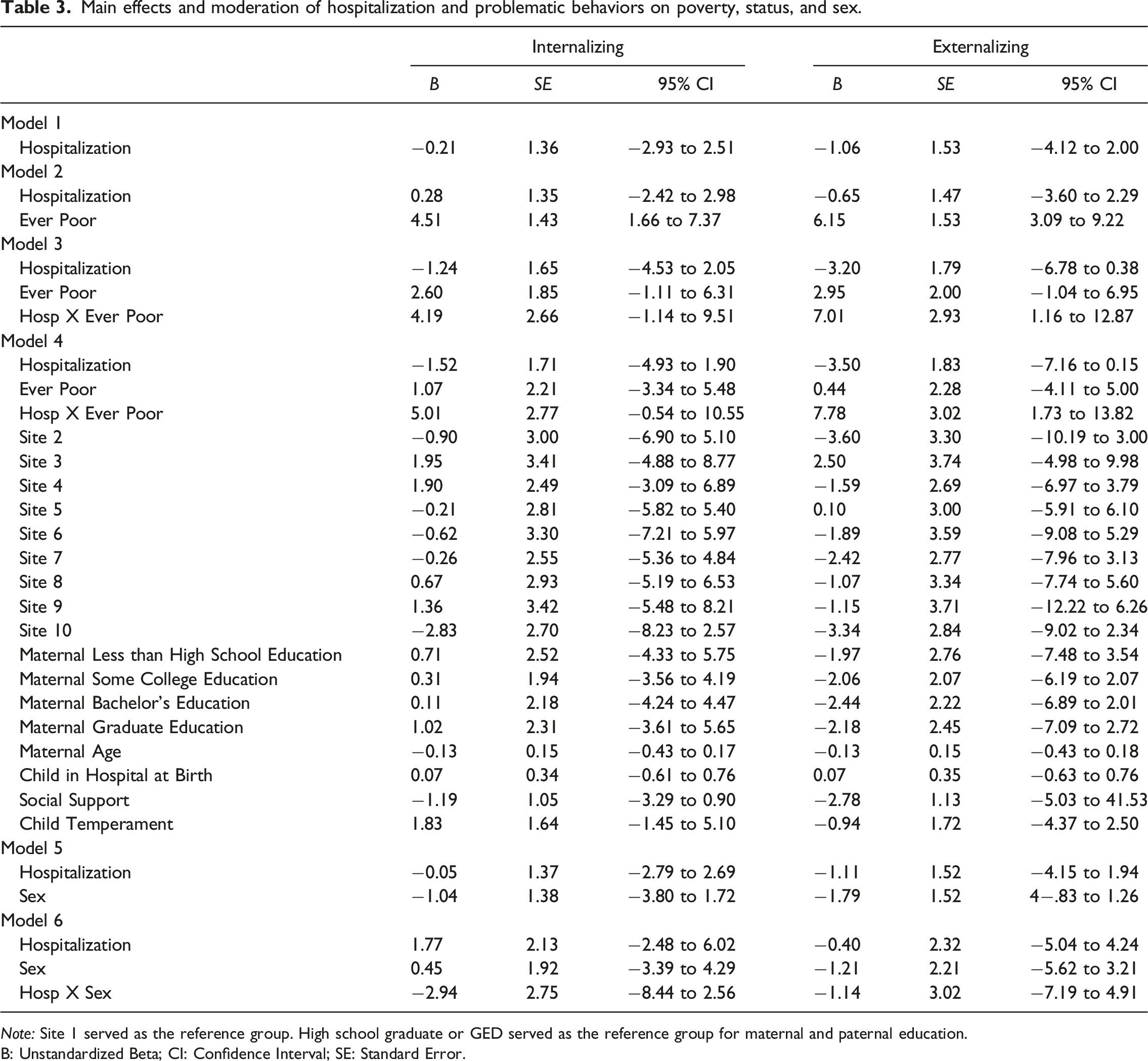
Note: Site 1 served as the reference group. High school graduate or GED served as the reference group for maternal and paternal education.
B: Unstandardized Beta; CI: Confidence Interval; SE: Standard Error.
Matched sample descriptive statistics for hospitalization and outcome variables by hospitalization and sex.
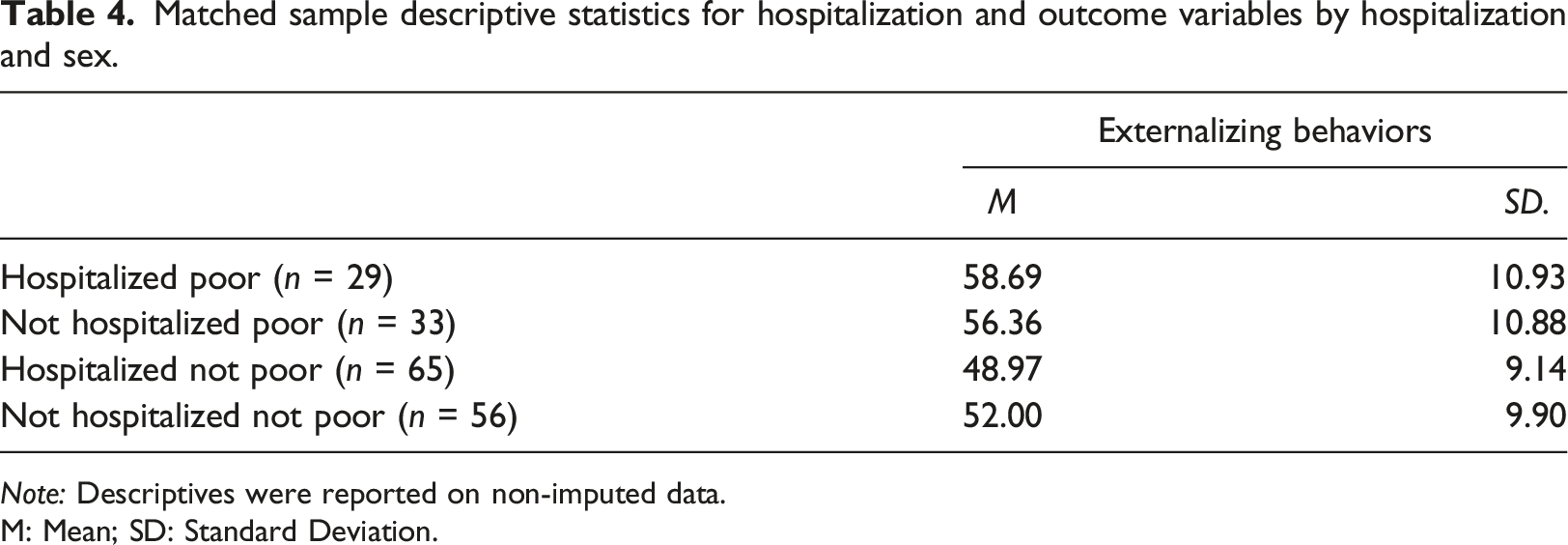
Note: Descriptives were reported on non-imputed data.
M: Mean; SD: Standard Deviation.
For the primary analyses, we present unstandardized regression coefficients and 95% confidence intervals (CI) for statically significant results with potential clinical implications. Contrary to hypothesis one, there was no direct association between hospitalization and problematic behaviors (see Model 1 in Table 3; Internalizing: B = −0.21, 95% CI [−2.93, 2.51]; Externalizing: B = −1.0695% CI [−4.12, 2.00]). Income-to-needs was directly associated with both outcomes when added to the model (see Model 2 in Table 3; Internalizing: B = 4.51, 95% CI [1.66,7.37]; Externalizing: B = 6.15, 95% CI [3.09, 9.22]). In partial support of hypothesis two, poverty significantly moderated the association between hospitalization and externalizing behaviors (see Model 3 in Table 3; Internalizing: B = 4.19, 95% CI [−1.14, 9.51]; Externalizing: B = 7.01, 95% CI [1.16, 12.87]). The significant moderated effect was still present for externalizing behaviors after including unbalanced covariates and adjustment for False Discovery Rate (see Model 4 in Table 3; Externalizing: B = −7.66, 95% CI [1.73, 13.82]). Sex was also not directly associated with hospitalization and problematic behaviors (see Model 5 in Table 2; Internalizing: B = −1.04, 95% CI [−3.80, 1.72]; Externalizing: B = −1.79, 95% CI [−4.83, 1.26]). Analyses examining sex revealed that children’s sex did not moderate the association between hospitalization and problematic behaviors (see Model 6 in Table 3; Internalizing: B = −2.94, 95% CI [−8.44, 2.56]; Externalizing: B = −1.14, 95% CI [−7.19, 4.91]).
Follow-up analyses further examined how childhood exposure to poverty moderated the association between hospitalization and externalizing behaviors. Means and standard deviations for externalizing behaviors are presented by hospitalization and poverty status in Table 4. Children who were both hospitalized and experienced poverty had estimated externalizing scores 7.62 units higher than children who experienced hospitalization but were never poor (B = 7.62, 95% CI [−2.83, 12.41]).
Discussion
We investigated if being hospitalized in early childhood was associated with the development of internalizing and externalizing behaviors and whether family poverty status and/or sex moderated this association. Using a rigorous quasi-experimental design, we found evidence of the direct impact of poverty on socioemotional development during early childhood. Contrary to previous research on hospitalization, our results did not reveal a significant association between hospitalization and internalizing or externalizing behaviors (Small et al., 2009; Small and Melnyk, 2006). Instead, poverty status appeared to moderate the impact of childhood hospitalization on externalizing behaviors. Children who were hospitalized and experienced poverty at some point during early childhood displayed greater externalizing behaviors than children who were hospitalized but did not experience poverty. These results strengthen findings that adequate socioeconomic resources are directly associated with fewer problematic behaviors in childhood, as well as suggest that exposure to poverty might amplify the negative impact of stressful events (e.g., hospitalization) on externalizing behavior.
We identified a novel yet intuitive finding that the association between hospitalization and externalizing behaviors was modified by experiences of childhood poverty. Children living in poverty are more likely to be hospitalized and exhibit more behavior problems compared to those from more affluent families (DeCarlo Santiago et al., 2011). These results suggest that the effects of hospitalization for children’s externalizing problems in early childhood differ depending on whether the child had experienced poverty in early childhood. As expected, children who experienced both poverty and hospitalization had higher externalizing problems than children who experienced hospitalization but not poverty. This is the first study to examine poverty status as a factor driving the association between general hospitalization and behavior problems, as others have focused only on children who are in ICUs during early childhood (Rees et al., 2004; Small, 2002). Our findings highlight the need to reduce exposure to poverty in all children, but especially emphasize the need to develop interventions that can reduce the harmful impact of hospitalization on children exposed to poverty.
Reducing the risk of hospitalization for children that experience poverty might also help address their heightened risk for externalizing behaviors. Although improving the health of children in poverty is a complex and challenging issue, programs in communities that promote an integrative approach to healthcare for families that have experienced poverty that combine physical, cognitive, emotional, and social support have shown promise (Brown et al., 2021; Carroll et al., 2020; Halfon et al., 2007; High et al., 2000; Page and Golden, 2009). Such programs could reduce the cost of medical bills that occur after hospitalization by preventing hospitalization in the first place, which is particularly important for families that experience poverty.
Contrary to previous research focused on samples of older children, we found no differences between kindergarten-age males and females after hospitalization on behavioral outcomes (Small et al., 2009). Further, previous research that has found sex to be significantly related to children’s behavior problems has focused only on hospitalized children (Tiedeman and Clatworthy, 1990), without a comparison sample.
Study limitations
An important limitation in the current study is that children’s underlying reason for hospitalization, hospital length of stay, frequency, or ICU status were not explored. Previous research has found that children who experience critical and intensive hospital stays are likely to have severe chronic illnesses and those individuals show higher levels of problematic behaviors compared to hospitalized peers with less severe illness (Pinquart and Teubert, 2012). Another limitation of the current study is that we utilized a static measure of poverty (i.e., income-to-needs ratio) collected when the child was one month old. It is possible that families moved in and out of poverty throughout the study (i.e., birth to 54 months) and it is important to acknowledge that duration, timing, and stability of circumstances throughout children’s development have differential effects on childhood outcomes (Ben-Shlomo and Kuh, 2002). Another limitation was that our sample was not nationally representative and included mainly White non-Hispanic participants. This leaves questions, given that racial and ethnic characteristics are highly related to poverty status (Chen et al., 2002) and underrepresented populations, including Black and Hispanic individuals, are more likely to be hospitalized compared to White individuals (Mayberry et al., 2000). Further, individuals from less affluent Black and Hispanic families are likely to show more behavior problems than White children (Keiley et al., 2000). Thus, future research should strive to use diverse and representative samples to examine behavioral outcomes related to poverty and external stressors in childhood.
Future directions
Future research should include children who have been hospitalized for different reasons and different durations/frequency throughout early childhood. Work that incorporates current poverty status at the time of hospitalization would provide a more sensitive test of the moderation effects examined in the present study. Also, future studies should explore race/ethnicity as moderating factors in the relation between hospitalization, poverty exposure, and problematic behaviors.
Implications for practice
As previously stated, reducing the risk of hospitalization for children that experience poverty could help decrease their compounding risk for problematic behaviors. The primary method through which the medical field attempts to improve children’s health outcomes is through parental education about healthy and preventative behaviors for children (Glascoe et al., 1998). Parents receiving health related education, particularly those living in poverty, experience better health outcomes for their children (Glascoe et al., 1998). One factor related to preventative health care is having health insurance (Chen et al., 2002); families with health insurance are more likely to engage in preventative practices such as and are less likely to use emergency rooms and urgent care clinics (Mayberry et al., 2000). During those preventative practices, like check-ups, parents are often provided with information that support the promotion of children’s health and behavior (Glascoe et al., 1998). However, families living in poverty are less likely to have health insurance compared to more affluent families and children without consistent health insurance could be at risk for multiple hospitalizations and behavior problems because of the lack of preventative care and educational services provided by hospitals.
If children are hospitalized, auxiliary services provided by hospitals are an integrative health care approach that could reduce problematic behaviors for hospitalized children who have experienced poverty. For example, certified child life specialists can provide emotional support and teach coping strategies that children and families might need after hospitalization which can help improve coping mechanisms for these individuals (Romito et al., 2021). Hospitalized children from families that experience poverty might not have the financial and educational resources at home compared to children from more affluent families to help promote healthy coping mechanisms. Improving coping mechanisms could help hospitalized children that have experienced poverty improve their problematic behaviors.
Conclusions
The current study extends prior research in three important ways. First, our findings suggest that problematic behaviors seen after hospitalization are not above and beyond what would typically be observed during early childhood. Second, we found that of children who were hospitalized, children who experience moderate to high levels of poverty during early childhood exhibited higher rates of externalizing behaviors than those who did not experience poverty. Lastly, our use of a quasi-experimental method to estimate the impact of hospitalization and poverty exposure on behavioral outcomes produced results with greater internal validity than other comparable studies.
Supplemental Material
Supplemental Material - Early childhood hospitalization and problematic behaviors: A propensity score analysis
Supplemental Material for Early childhood hospitalization and problematic behaviors: A propensity score analysis by Toria B Flynn, Priscilla M Goble, Nicholas J Bishop, and Amy A Weimer in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.