
Abstract
Health anxiety by proxy is a newly described phenomenon where parents worry excessively that their child suffers from a serious illness. In a former study, six parents with distressing worries about their child’s health were interviewed to develop the Health Anxiety by Proxy Scale. The present study is a secondary analysis of these semi-structured interview data using interpretative phenomenological analysis aiming to explore for the first time the lived experience of parents with health anxiety by proxy. Analysis revealed three main themes: ‘Faces of distress’ describing various aspects of parents' experienced distress; ‘Invasive insecurity and mistrust’ portraying how anxiety affects parents' relationship with their children, health professionals and family; and ‘Making sense of own worries’ covering parents' ambivalence regarding their anxiety and rationalization of their worries. Knowledge about perspectives of parents who suffer from health anxiety by proxy can inform communication in clinical encounters where validation of parents' experiences may be key to forging an alliance for further treatment; and to recognising and potentially lowering barriers to receiving help that lies in parents’ potential mistrust in professional help.
Introduction
Health anxiety (HA) is characterised by fear of and worries about suffering from a serious illness accompanied by misinterpretation of normal bodily symptoms, leading to a pathological illness conviction (hypochondriasis (World Health Organization, 2018)/illness anxiety disorder (American Psychiatric Association, 2016)). Health anxiety by proxy is a newly described clinical phenomenon characterised by obsessive parental worries about their child’s health, leading to preoccupation with symptoms and fear that health professionals overlook serious illness in the child (Lockhart, 2016). Health anxiety by proxy was first empirically confirmed in a study of mothers suffering from HA (Thorgaard et al., 2017b). The results showed more profound HA by proxy worries in mothers diagnosed with HA than in mothers with rheumatoid arthritis and healthy mothers (Thorgaard et al., 2017b).
Health anxiety by proxy may have direct, specific and serious consequences for children subjected to unnecessary and potentially unpleasant medical examinations (Lockhart, 2016). Furthermore, due to social learning (Bandura, 1977) via parental reinforcement and modelling, children could possibly be at risk of developing maladaptive illness perceptions and behaviours (Jamison and Walker, 1992; Köteles et al., 2015; Levy, 2011; Marshall et al., 2007; Thorgaard et al., 2017a; Wright et al., 2017).
Current research with parents with other types of mental health problems has also focussed on the child’s risk of developing mental health problems (Ellersgaard et al., 2018; Mattejat and Remschmidt, 2008; Rasic et al., 2014; Santvoort et al., 2015; Stapp et al., 2020; Thanhäuser et al., 2017; Thorgaard, 2017) which may be increased due to a combination of genetic vulnerability and intergenerational transmission through social learning. In contrast, parents' perspectives and experiences have been explored only in a few studies, for example, studies on bipolar disorder (Tjoflåt and Ramvi, 2013), borderline personality disorder (Lumsden et al., 2018) and parents with different psychiatric diagnoses (Boursnell, 2007; Jones et al., 2016; Van der Ende et al., 2016). Consistent themes described across these studies are worries about future mental illness in their child, how to balance taking care of oneself and of one’s child, fear of being stigmatised as a bad parent and how children motivate their parents to manage their illness (Boursnell, 2007; Jones et al., 2016; Lumsden et al., 2018; Tjoflåt and Ramvi, 2013; Van der Ende et al., 2016).
Parental worrying about their child’s health has been somewhat investigated in qualitative studies on parents of children and adolescents with functional somatic symptoms and chronic pain (Brodwall et al., 2018; Hulgaard et al., 2020; Jordan et al., 2007; Maciver et al., 2010; McWilliams et al., 2016). Parents in these studies are not described with own mental health problems, and their profound worries about their children’s health seem to be linked to perceived absence of a clear diagnosis explaining their children’s symptoms (Hulgaard et al., 2020; Jordan et al., 2007). The parents are described as highly involved in caretaking and decision-making concerning their child’s health, and their illness behaviours may reinforce their child’s symptoms (Hulgaard et al., 2020; Jordan et al., 2007). Further, as a result of parental worrying and preoccupation with symptoms, the child may become more worried and interpret symptoms more negatively which may, in turn, affect the child’s coping strategies (Levy, 2011; Marshall et al., 2007; Walker et al., 2006).
Given these findings, it is likely that improved knowledge about thoughts and motives of parents with HA by proxy may be important in reducing intergenerational transmission of health worries. However, to the best of our knowledge, HA by proxy has not previously been described in detail based on interviews. Such unique information may be important for clinicians and researchers to better understand this specific anxiety phenomenon and how to help affected parents and families.
In a recent study, qualitative interviews were used to explore symptoms of HA by proxy as part of developing a new questionnaire: The Health Anxiety by ProxY Scale (HAPYS) (Ingeman et al., 2021). HAPYS addresses topics such as worries about the child’s symptoms, control and avoidance behaviour, and impact of worries on parents' lives, but several other aspects of parents' lived experiences of their anxiety were also apparent in these interviews.
Aim
This study aimed to perform a secondary analysis of interview data from the previous study of HAPYS (Ingeman et al., 2021) by using in-depth qualitative methods to obtain more detailed knowledge on how parents with HA by proxy perceive being anxious for their child’s health and living with this anxiety.
Methods
The present study is part of a research project investigating HA by proxy in terms of assessment and treatment. Specifically, this study is a secondary analysis of interviews used to develop the HAPYS.
Setting
The study was conducted at (Aarhus) University Hospital, (Denmark) as a collaborative effort between the Department of Child and Adolescent Psychiatry and The Research Clinic for Functional Disorders and Psychosomatics (The Research Clinic).
Recruitment
Recruitment took place in two ways: (1) after diagnostic assessment for HA at The Research Clinic if clinical impression indicated HA by proxy; or (2) by self-recruitment, that is, parents contacted the main author after finding questions on the clinic’s webpage concerning HA by proxy applicable to them. The selection process aimed to provide access to various particular perspectives on HA by proxy, thus variation in referral (self-referral and clinician approach), variation in parental gender and variation in children’s age. A small sample size is appropriate as it allows detailed accounts of individual experiences with attention to subtle meanings and nuances, which may be endangered in large sample sizes (Brocki and Wearden, 2006).
Assessment questions.

Ethics
The study was conducted according to guidelines from the (Danish) Research Ethics Committee (55/2018) and approved by the Data (Danish) Protection Agency (approval number). All participants received written and oral information and signed a written consent form prior to interviews, giving permission to use the data for research purposes.
Data collection
Semi-structured individual interviews (see Supplemenary materials) were conducted by the main author. The main author had no prior relation with the participants other than the assessment phone call. Interviews were recorded and subsequently transcribed verbatim.
Data analysis
The interviews were analysed using interpretative phenomenological analysis (IPA). IPA offers an opportunity for exploration of phenomena about which only little knowledge exists and is suitable for small sample sizes focusing on in-depth descriptions over generalisations (Smith and Osborn, 2015). Interpretative phenomenological analysis seeks to understand participant experiences, while recognizing the researcher’s subjective role in the interpretative process. Interpretative phenomenological analysis is useful for understanding each participant’s lived experience in an open manner unrestrained by predefined concepts (Smith and Osborn, 2015).
Transcripts were analysed in their original language (Danish), but quotations were translated for publication, and participants were provided with pseudonyms. Stepwise analysis was performed by the first and second authors assisted by NVivo 12 (QSR International Pty Ltd, 2018). During step one, interviews were read, and ideas for themes were discussed. In step two, interviews were coded individually and then across interviews in several rounds. In step three, main themes and sub-themes were determined in several discussion rounds. The main author is a female psychologist with clinical experience with HA. The two co-authors are child and adolescent psychiatrists with research and clinical expertise in HA and functional disorders. Furthermore, the second author is experienced in IPA and independently coded four randomly chosen interviews during step two. Two interviews were read by the last author for step three. All authors took part in discussion and definition of themes.
Findings
Participants
Participant characteristics (N = 6).
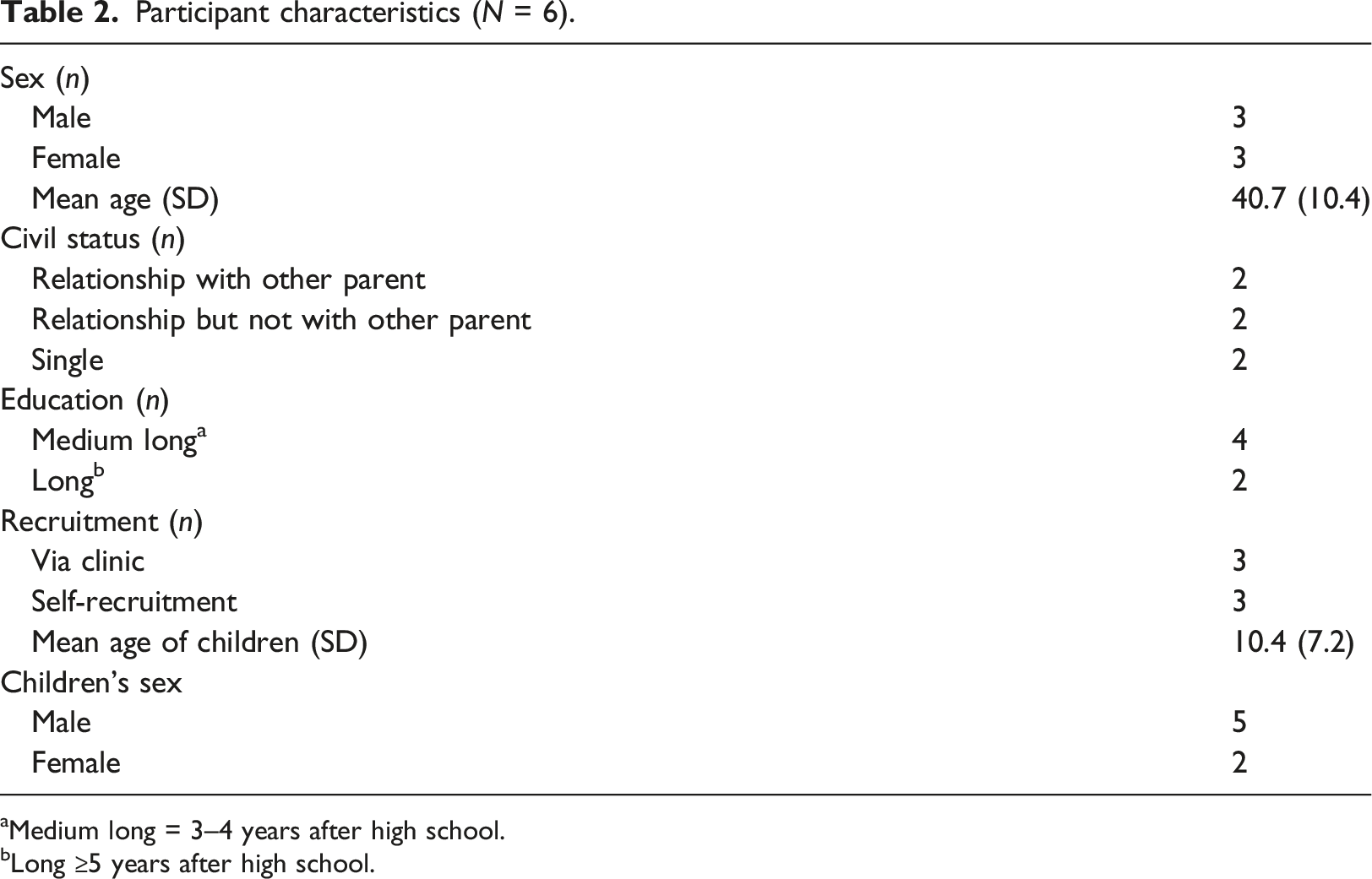
aMedium long = 3–4 years after high school.
bLong ≥5 years after high school.
Interviews
The interviews were conducted between June 2018 and March 2019 at a location chosen by the participant: four interviews at The Research Clinic, one by video conferencing, and one in a private room at a public library (61–94 min (mean: 74 min)).
Themes
Three main themes were identified reflecting parental experiences of living with HA by proxy (Figure 1). The first theme, ‘Faces of distress’, described how the parents experienced distress in relation to various aspects of dealing with their child’s symptoms and their own worries for their child (Subthemes: ‘Fearing for the child’, ‘Effects on daily living’, and ‘Feeling guilty and ashamed’). The second theme, ‘Invasive insecurity and mistrust’, portrayed the parents' feelings of anxiety-derived mistrust invading their relationships with their children, family members and meetings with healthcare professionals (Subthemes: ‘Mistrust in child to report and evaluate own symptoms’, ‘Difficulties trusting healthcare professionals’ and ‘Family conflicts’). The last theme, ‘Making sense of own worries’, covered the parents' various understandings and explanations of their own anxiety (Subthemes: ‘Ambivalence in relation to worrying’ and ‘Rationalising worry’). Identified themes (white boxes) and subthemes (gray boxes).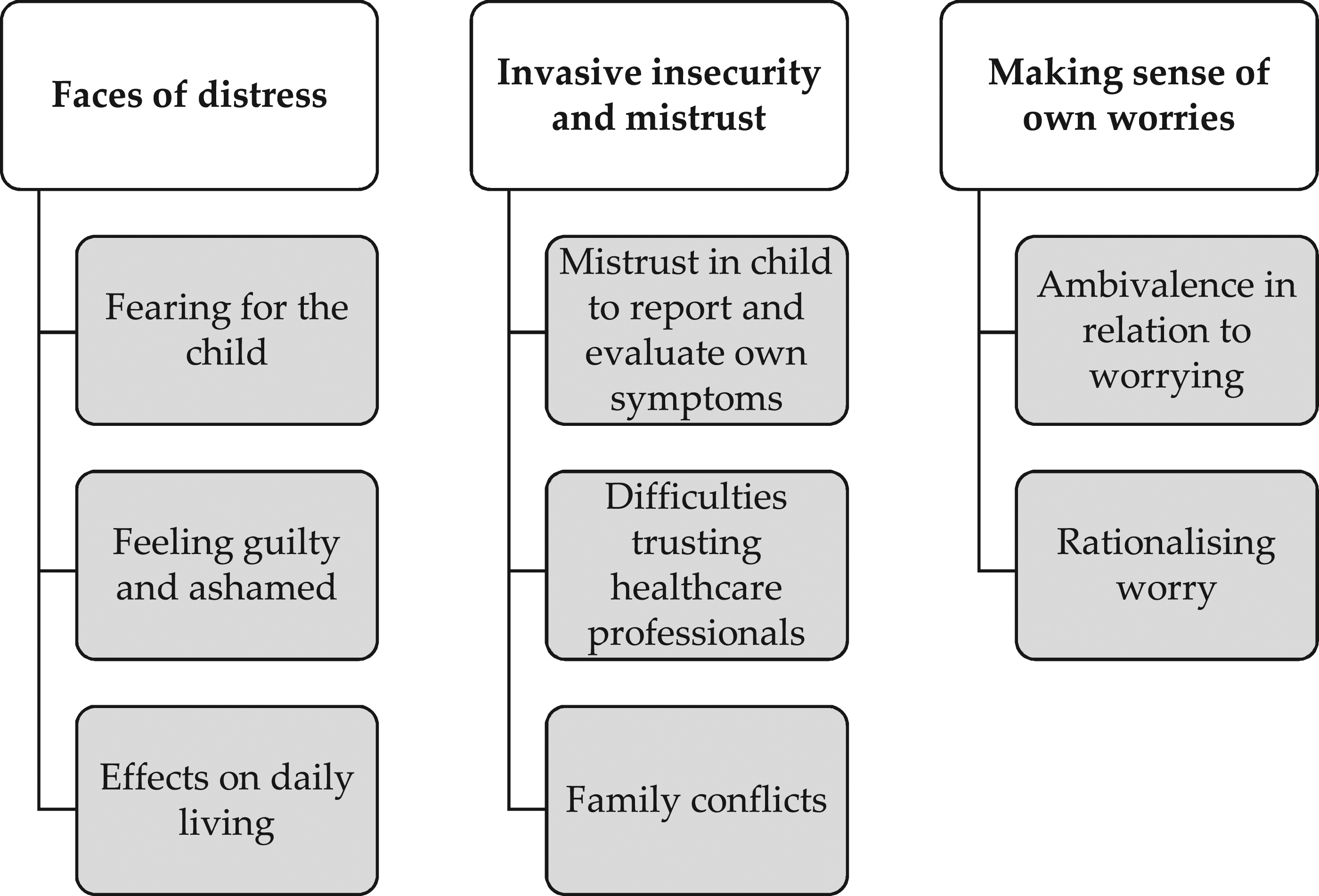
Faces of distress
Fearing for the child
Parents described profound worries that their child would become severely ill. Marian who had two almost grown-up sons, whom she had raised alone since her youngest was 5 months old, described her fears of losing her children due to serious illness. An episode with her youngest son’s admission to a hospital and her brother’s death from late detected colon cancer triggered and aggravated her worries. ‘I simply think that, fundamentally, I am so scared that they will get ill and die without me finding out’. (Marian)
Her anxiety revolved around her children dying from illness. This fear was central for several parents. But her distress was also evident in fearing that she would not find out in time to prevent it, thus reinforcing feelings of a parental responsibility to prevent serious illness in her children.
Effects on daily living
Parents experienced effects of their anxiety on daily life and activities. Kirsten described a positive relationship with her content and happy nine-year-old daughter. Even so, she was very aware of potential influences of her anxiety on her child and their family life. ‘Well, I think I am nervous that it will delay her development, because somehow, in this worry … or if you are scared of living or scared of taking chances that means that you limit yourself. It is very limiting to be scared and worried like this. It overshadows many of the exciting things that are also part of life’. (Kirsten)
Kirsten described her personal experiences of being restrained by anxiety in her own life, intertwined with fear that she might transfer this restraint to her daughter. Thus, for Kirsten, the distress of having HA by proxy was not limited to worries related to her daughter’s health. Rather, she described concerns for her daughter’s overall development as she was worried that her own fearful and overprotective behaviour would restrain her daughter.
Feeling guilty and ashamed
For some, distress was related to awareness that anxiety-related behaviours could harm the child combined with feelings of being unable to change these behaviours or find help to do so. In some cases, this predicament resulted in feelings of guilt and shame. Below is a quote from Susan who lived alone with her 17-year-old son and was very consumed with monitoring his possible symptoms and taking him to a doctor: she described her own childhood experiences of HA among adult family members. ‘Well, also letting the shame and guilt I feel in relation to this out into the open. It is hard to show others, also because I think … in my family, I grew up with… my aunt who I may resemble … that I should not become like my aunt. But also in society in general. The word, when I first heard hypochondriac, it was like I felt I was wrong. The feeling of being wrong and I felt like I inconvenienced the doctor. You don't do this because you want to – you do it because I don't know how to do anything else. If I could have done anything else, I would have’. (Susan)
Susan described an awareness of her anxiety and related behaviours as potentially excessive and unpleasant for her child. These feelings were likely tied to her family history and perception that hypochondriasis carries negative and stigmatized social interpretations. Further, negative experiences with the healthcare system exacerbated her feelings of shame and guilt.
Invasive insecurity and mistrust
Mistrust in the child to report and evaluate own symptoms
Parents with younger children described behaviours to control their anxiety, such as examining the child or consulting a doctor. Parents of older children described their struggle to accept the child’s personal boundaries about their body and health as these could be in the way of control behaviours. For some parents, trusting their child to evaluate own symptoms was a challenge. Peter’s daughter of 11 years had become reluctant to see doctors after an episode where she had become ‘hysterical’ during a scan of her lymph node. ‘But then I am also afraid that she doesn't … that she sometimes doesn't tell us. It is like she doesn't always tell everything. If she says she feels sick. “Well, what is wrong!?""I don't know," she says. “Well is it because you are not telling … that you are afraid to tell me that there is something wrong" right?’.
He elaborates: ‘She doesn't like to go to the doctor’. (Peter)
Peter worried that his daughter was withholding information from him when she was sick as a way of avoiding going to the doctor. His need to check his daughter’s health may in this way be exacerbated and at the same time challenge their mutual trust.
Difficulties trusting healthcare professionals
The healthcare system was a setting in which some parents sought confirmation and reassurance as a way of dealing with their anxiety. But it was also a setting associated with fear and mistrust. ‘In my experience, you have to be on your toes in today's [country]. Just because a doctor said something, I don't necessarily take it as gospel truth. It [the child's symptom] needs to be examined properly. Because I have experienced – and that is probably my own bad experience with the hospital system – that you get shelved or the doctors have overlooked something, I am very alert, you know. I want us to be taken seriously and the things to be examined’. (Kirsten)
Kirsten was sceptical towards the healthcare system and did not trust healthcare professionals to be sufficiently thorough. Therefore, she was extra observant, made demands about examinations and did not believe the doctor’s word unconditionally. She rationalised this scepticism by reference to previous experiences of insufficient treatment and a general perception that persistence is necessary in order to be taken seriously. As such, use of the healthcare system as a way of seeking reassurance was both dissatisfactory and mistrustful.
Family conflicts
Parents described involvement of family members as a way of coping with their anxiety. Some parents described how reassurance from their family was helpful, and some parents experienced conflicts with family members. William, a father of a 15-month-old boy, dealt with his anxiety by examining his son or by taking him to the doctor. Often, he also talked to his girlfriend about his worries. ‘Well, she does not feel the same way at all, so that’s … She says: "Don't worry about it". […] So in order to avoid conflicts, we try to leave it there, but then I go around being extra observant of it [the child's symptom] for a while after I have seen something [a possible symptom]’. (William)
William describes his attempts to curb worries and control behaviour in order to avoid conflicts with his girlfriend. Still, even when his girlfriend reassured him about the benign nature of their son’s symptoms, he continued to keep an extra eye on him. Making decisions about their child may pose special challenges when one parent suffers from HA by proxy as conflict may arise when the other parent does not agree with the need to worry or does not participate in control behaviours, either by not providing enough reassurance or by making the parent with HA by proxy stop performing unfavourable coping strategies.
Making sense of own worries
Ambivalence in relation to worrying
All parents had some insight into the excessive nature of their worries for their child’s health as they had agreed to participate in this study. Nonetheless, during interviews, it became evident that the parents felt ambivalent about their worries and argued how their worries and related behaviours might be necessary. William described his reasons for reacting when he detected a symptom in his son: ‘Like, if I don't react on this, do I risk that he will become seriously ill? It is also like: I feel like I am not taking proper care of my child by saying "oh this is probably nothing." So, there is a conflict there because I sort of …’. (William)
He felt like he was taking a risk that his son might develop serious illness by not reacting to his son’s symptoms. Thus, worrying was a way of protecting his son and being a responsible parent.
However, William also conveyed his awareness that his checking behaviours had a negative effect on his son. His worries would sometimes lead him to examine him, even if he would complain. William was asked how he felt when his son complained about examinations. ‘Well, I get sad, because after all I know that ... […] of course I don't want to be one of those … well, he begins to … if I … well, if he detects that I am worried, when he gets older. If he begins to wonder: "Well, is there something wrong with me? Why are they checking all time if there is something wrong with me?" Then that is of course not something I want to put on him’. (William)
The interrupted sentences may indicate that it was difficult for William to talk about his behaviour possibly having negative consequences for his son. Overall, he expressed an ambivalent position in which he was aware of these consequences but still felt a need to react to his child’s symptoms in order to protect him. This exemplifies the uncertainty about ‘normal’ parental worries described by several parents, which contributed to ambivalence and uncertainty in judging the relevance of worries and deciding when a reaction was necessary.
Rationalising worry
For some parents, rationalisations were based on negative personal experiences with the healthcare system or on stories about people who had received inadequate treatment; for others, rationalisations were based on a conviction that only they could take proper care of their child.
Marian had had a brother who died only five weeks after a late discovered cancer illness. She explained this as possibly exacerbating her worries that illness may be overlooked in her children. Explaining what she was worried about, she said: ‘… that I overlook something. And of course it definitely gets ... worse in relation to my brother’s illness. He falls ill in 2014 and the doctors do not detect it. They say he is stressed and has a depression, but he hasn't. He has colon cancer which they don't detect until just five weeks before he dies. So, I have a very good example of how doctors can actually overlook something’. (Marian)
This example of doctors overlooking symptoms of serious illness were overgeneralised and applied to all doctors. As such, this experience became an explanation for her worries about overlooking a serious illness in her children and a rationalisation of her worry.
Discussion
The aim of this study was to investigate how parents with HA by proxy perceive being anxious for their child’s health and living with this anxiety. Three main themes emerged from our analysis: 1) ‘Faces of Distress’: Parents described feelings of distress because they felt anxious about their child’s health, feelings of shame and guilt, and fear of pervasive consequences of their anxiety for their everyday lives and close relationships. 2) ‘Invasive insecurity and mistrust’: Parents were affected by anxiety-induced mistrust in others (their child, partner, and healthcare professionals) to evaluate the child’s symptoms. 3) ‘Making sense of own worries’: Parents were ambivalent about their worries wavering between justifying them with previous poor experiences with the healthcare system, and realising their excessiveness and potentially harmful effects on the child.
Parental feelings of shame and guilt were exacerbated during encounters with family members or doctors. Other studies have described how parents with mental illness worry about not being a sufficiently good parent and describe how this causes feelings of shame and guilt aggravated by social stigma making it challenging to share their mental health problems (Boursnell, 2007; Jones et al., 2016; Lumsden et al., 2018; Tjoflåt and Ramvi, 2013; Van der Ende et al., 2016). This may pose a barrier to seeking help (Corrigan, 2004; Rüsch et al., 2005; Struch et al., 2008).
Another barrier for help-seeking may be parents’ description of mistrust in the healthcare system, which was often rooted in previous experiences with diseases overlooked by doctors. Similar explanations for mistrust have been reported in studies on parents of children with functional somatic disorders (FSD) (Brodwall et al., 2018; Hulgaard et al., 2020). Parents of children with FSD also describe how they feel left alone with the responsibility of caring, have many healthcare contacts, and how they fear not being taken seriously by doctors. A lack of trust in healthcare professionals may become an important barrier to receiving help (McWilliams et al., 2016). Difficulty trusting doctors is also a clinical characteristic of HA (Kellner et al., 1987; Salkovskis et al., 2002; Speckens et al., 2000). All parents in the present study were diagnosed with HA which may indicate that mistrust in healthcare professionals can spill over into HA by proxy.
The specific mistrust and suspicion between parent and child outlined has not been reported in other qualitative studies of parents with mental illness (Boursnell, 2007; Jones et al., 2016; Lumsden et al., 2018; Tjoflåt and Ramvi, 2013; Van der Ende et al., 2016). It could be a distinct theme in HA by proxy. However, more research is needed to investigate the extent and impact of this.
When rationalising own behaviours, parents were caught between a conviction that they had to protect their child from serious diseases and concerns about possible negative consequences of their anxious behaviour, including putting the child at risk of developing HA. Being worried about transferring mental illness to one’s child is not unique for parents with HA by proxy (Jones et al., 2016; Lumsden et al., 2018; Tjoflåt and Ramvi, 2013; Van der Ende et al., 2016). However, whereas parents in these studies were mostly worried that their child would inherit their disorder, parents with HA by proxy were very aware that their anxiety-coping behaviour may directly affect their child. This awareness of social learning patterns may be an important factor in addressing HA by proxy.
Studies on social learning patterns have shown that parents' reaction to their child’s symptoms affects the child’s perception of and worries about symptoms and reporting of pain (Levy, 2011). Furthermore, parental dysfunctional coping (Albiani et al., 2019), over-involvement, protective behaviour (Möller et al., 2015; Woodruff-Borden et al., 2002), worries about the child (Fisak et al., 2012) and less parental emotional flexibility (Van der Giessen and Bögels, 2018) seem to be associated with parental anxiety and to enhance their child’s anxiety.
It has been suggested that anxious parents overestimate potential threats to their child. This bias may be transferred from parent to child through the above-mentioned behaviours (Fisak et al., 2012). Lack of emotional flexibility in parents with anxiety has been suggested to make it difficult for them to regulate anxiety and flexibly switch between emotions when interacting with their child (Van der Giessen and Bögels, 2018). Further, children may not learn how to cope effectively with distress (Woodruff-Borden et al., 2002). It seems likely that similar issues may be present in parents with HA by proxy, adding to potential intergenerational transmission. Through knowledge about the experience of having HA by proxy, intergenerational transmission may be targeted more efficiently. Moving forward, experiences from prevention interventions in other anxiety disorders focusing on social learning may also be extended to parents with HA by proxy (Cartwright-Hatton et al., 2018; Ginsburg et al., 2015; Yap et al., 2016).
Overall, the identified themes offer insight into experiences and behavioural motives of parents with HA by proxy. Specifically, wishing to protect their child from illness should be recognised as very different from underlying motives of parental behaviour seen in factitious disorder imposed by another (FDIA) (American Psychiatric Association, 2016) (Munchhausen syndrome by proxy (Meadow, 1977)), although the pathological picture of frequent healthcare contacts may appear similar. In HA by proxy, frequent contacts are based on excessive parental worries about the child’s health, whereas parents with FDIA fabricate illness symptoms in their child to achieve personal attention.
Strengths and limitations
The consolidated criteria for reporting qualitative research statement were widely met (Tong et al., 2007). However, participant feedback, data saturation, re-interviews and adjustment of interview guide were not performed. These shortcomings are largely explained by the study being a secondary analysis of interviews originally conducted with another aim.
Other limitations concern the study population. The informants were a selected group of parents who were aware of the excessiveness of their worries, which influenced their perspectives. Further, HA by proxy is not yet a diagnosis defined by clear-cut criteria. However, recruitment procedures and thorough inclusion criteria ensured a representative selection of parents. First, it was important that the parents experienced distress in daily life due to their worries about their child’s health. Second, these worries must not be caused by a diagnosed illness in their child. Though we did not directly assess the children’s health status, parental statements gave no indications of severe illness.
Several strengths were also identified. The research team consisting of a psychologist and two child and adolescent psychiatrists working with HA secured expert knowledge. Further, the second author was not involved in data collection or study design and was thus blinded to the interview guide, which enhanced analytic breadth. Finally, the analysis was conducted stepwise with several rounds of individual coding and discussion meetings. This process strengthened selection of the final themes. Under the premise of IPA where subjectivity of the researcher is a contributing factor to data collection and analyses, other themes may have emerged had the study been conducted by different researchers. This does not mean that the reported themes are incorrect; it means that they are a product of a unique interaction between researchers and participants.
Implications for practice
An enhanced understanding of HA by proxy as a phenomenon can improve clinicians’ work with affected families, including how to target potential transmission of undesirable patterns of parental illness behaviours and perceptions to the child. Specifically, in paediatric clinical settings it may challenge collaboration between families and healthcare professionals and treatment-course of the child, if potential HA by proxy is not addressed. As such, clinicians may be better able to communicate about parental health-related worries and anxious behaviour if they know more about the parents' own perspectives. Especially, it may be important to recognise these parents' possible mistrust in healthcare professionals and ambivalence towards own worries as barriers for accepting and receiving help.
Conclusions
This study is the first to explore lived experiences of parents with HA by proxy. The parents reported great distress due to their anxiety, not only directly in relation to a fear of losing their child but also in daily life as a consequence of their anxiety-driven behaviours. Further, parents experienced mistrust in others' evaluation of their child’s symptoms, which in some cases affected the relationship with their child, family, and healthcare professionals. Parents used previous negative experiences with the healthcare system to rationalise their worries, although they also described an awareness of potentially negative consequences of these behaviours for their children. This ambivalence could cause further distress for affected parents.
Supplemental Material
Supplemental Material - Health anxiety by proxy – through the eyes of the parents
Supplemental Material for Health anxiety by proxy – through the eyes of the parents by Katrine Ingeman, Ditte Roth Hulgaard and Charlotte U Rask in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the Central Denmark Region and Aarhus University, Denmark.
Ethical approval
The study was conducted according to the guidelines of the Danish Research Ethics Committee (55/2018) and approved by the Data Protection Agency (1-16-02-921-17).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.