
Abstract
Developmental hip dysplasia is an abnormality of the hip joint which is associated with an unstable or dislocatable hip. During infancy, hips should be screened to determine whether they are stable, unstable or dislocated. In Australia, this screening is often performed by nurses using physical assessment. Physical examination includes a number of assessments which seek to identify underlying abnormalities in hip joint anatomy and function. This scoping review outlines the physical assessments used by nurses in the screening and surveillance of developmental hip dysplasia. A review of the literature identified 15 (N = 15; 100%) sources of evidence, which included original research articles (n = 6; 40%), expert opinion pieces (n = 2; 13.3%) and practice guidelines (n = 7; 46.7%). There were 18 physical assessments identified as being used by nurses in the screening process for developmental hip dysplasia. However, it is apparent that high quality research is required to examine the timing, specificity and sensitivity of the physical assessments identified.
Introduction
Developmental dysplasia of the hip (DDH) describes a spectrum of abnormalities in which the femoral head and acetabulum are not in alignment, grow abnormally or a combination of both (Committee on Quality Improvement, 2000; Shipman et al., 2006). These abnormalities can occur in utero, in the perinatal period, or during infancy and early childhood as a result of both genetic and environmental factors (Committee on Quality Improvement, 2000). The use of physical assessment to detect DDH in infancy and early childhood is a long standing practice used by health professionals internationally (Barlow, 1962; Ortolani, 1937).
Routine screening of newborns for DDH began in Sweden in 1948 (Barlow, 1962). The importance of this initial screening assessment is well-documented in literature and is reflected in international guidelines and recommendations for DDH screening (Canadian Task Force on Preventitive Health Care, 2001; Committee on Quality Improvement, 2000; International Hip Dysplasia Institute, 2015; Public Health England, 2021). Early screening, and therefore early diagnosis, in most circumstances leads to less invasive treatment over a shorter duration (Williams, 2018). Long term prognosis for treated DDH is good, without diagnosis and treatment the long-term impacts can include pain, decreased function and eventually arthritis (Williams, 2018).
There is no international agreement on the appropriate physical examination, or timing and frequency of screening for DDH throughout early infancy and childhood (Sewell et al., 2009; Shorter et al., 2011). Internationally, recommendations for DDH screening ranges from physical examination to universal ultrasonography of the hip joint (Williams, 2018). Physical examination includes a number of assessments which seek to identify underlying abnormalities in hip joint anatomy and function (Williams, 2018). These abnormalities manifest as differences in movements, appearance of the limb and provocative tests (Williams, 2018). Universal ultrasonography is recommended for DDH screening in European countries, while targeted ultrasonography of infants with a positive physical examination is used in Australia, America and Canada (Canadian Task Force on Preventitive Health Care, 2001; Committee on Quality Improvement, 2000; International Hip Dysplasia Institute, 2015; Public Health England, 2021; Williams, 2018).
In Australia, recommendations for DDH screening are that infants receive a newborn DDH screening assessment and additional assessments at universal child health checks; timing of hip assessment at these universal health checks varies between states (Government of South Australia, 2017; New South Wales Health, 2011). In Australia, universal child health checks are most frequently completed by Child Health Nurses at home visits, in child centres and clinic environments. Thus, in Australia, nurses are often the first clinician to assess an infant’s hip for DDH.
Through undertaking a preliminary search of the literature, it was identified that there are inconsistencies in recommended assessments used in the screening process for DDH (Wright et al., 2018). There appears to be a paucity of information on the approaches to physical assessment that are used by nurses in the ongoing screening and surveillance of all children and infants. This provided the rationale for a detailed search of current literature to determine the types of assessments that are used and recommended for nurses when screening for DDH.
Aim
To gain a thorough understanding of the research area by identifying and appraising all available peer-reviewed literature, policy documents, expert opinions, case studies and commentaries in order to capture all physical assessment techniques used by nurses when screening for DDH.
The objectives of this scoping review are to document and thematically collate the physical assessments used by nurses who screen for DDH; understand the recommendations associated with these physical assessments; and clarify what gaps exist in the literature and policy in regard to the recommended physical assessments, accuracy of physical assessments and recommended timing of physical assessment when nurses and midwives screen for DDH.
The research questions posed for the scoping review were two-fold; (1) What physical assessments do nurses use to screen for DDH in children and infants? and (2) What physical assessments for the practice guidelines, if any, recommend when screening for DDH in children and infants?
Materials and methods
Approach
This scoping review follows the methodologically rigorous six-stage framework outlined by Arksey and O’Malley (2005). A scoping review approach was determined the best approach to this review as it enabled the rapid mapping of literature and key concepts underpinning this area of research, and to identify the main sources and types of evidence available (Arksey and O’Malley, 2005). Arksey and O’Malley’s (2005) framework supports identification of primary and secondary sources of literature related to the research questions, including quantitative and qualitative research, opinion articles and international policies and guidelines. This six-stage framework supports a rigorous scoping review process that is transparent and replicable, therefore, increasing the reliability of the review findings. However, the sixth stage which focusses on consultation is rarely used and is not included in this review. The five stages used include: identifying the research question, identifying relevant studies, study selection, charting the data, and collating, summarising and reporting the results (Arksey and O’Malley, 2005). Whilst Arksey and O’Malley’s (2005) framework will be the predominant methodology, the findings of the review including study selection, charting of the data and reporting of results will use considerations from the recently published PRISMA-ScR framework (Tricco et al., 2018). There was no protocol registered for this scoping review.
Inclusion criteria
Clinicians identified in the scoping review were any health professional who identifies as a: nurse, child health nurse, midwife, maternal and child health nurse, health visitor or any other term that identifies a 'nurse' who conducts physical screening assessments on infants/children. Explored concepts included an assessment, screening or examination for DDH in children and infants. The context of the scoping review was any setting where nurses performed the assessments. Only publications in English were considered for inclusion. Primary research was only included if it was identified that the research had an explicit ethics statement. Qualitative, quantitative and mixed-methods primary research, policy documents, expert opinion, case studies and commentaries were all considered in order to capture all assessment techniques used by nurses when screening for DDH. No restrictions were places on time range for included publications.
Search strategy and study selection
To ensure a rigorous and replicable search of the databases, a university academic librarian was consulted to advise on the search strategy including; identifying key search terms and phrases and the chosen databases appropriate to the research question. Using the predefined types of participants, concept and context of the study, the key terms were developed with the application of medical subject headings (MeSH) (U.S. National Library of Medicine, 2019).
To identify potentially relevant sources the following databases were searched: Medline, EMBASE, Scopus, Informit, Joanna Briggs Institute, The Cochrane Library and Web of Science. The databases searched were selected to identify relevant sources including policy documents and primary research from nursing, paediatric and child health perspectives with the aim of searching multiple peer-reviewed sources. Arksey and O’Malley (2005) recommend the routine checking of all bibliographies of studies found through electronic database searching to ensure all relevant evidence is included in the ‘scoping’. This step was followed during study selection stage to ensure again rigour and replication of the scoping review. The final point in identifying relevant sources suggested by Arksey and O’Malley (2005) is to search existing networks, relevant organisations and conferences. A Google Scholar search was conducted at this stage to identify relevant policy documents. The search of the databases was conducted by the first author (LS) in March 2019. The identified articles were then imported into Covidence® to be screened and reviewed by two additional authors (LP and JC) for inclusion in the final review. Any difference of opinion between the authors was resolved by the fourth author (AE). The PRISMA flow diagram showing the flow of material through the different stages of the review is shown in Figure 1. PRISMA flow diagram for article selection.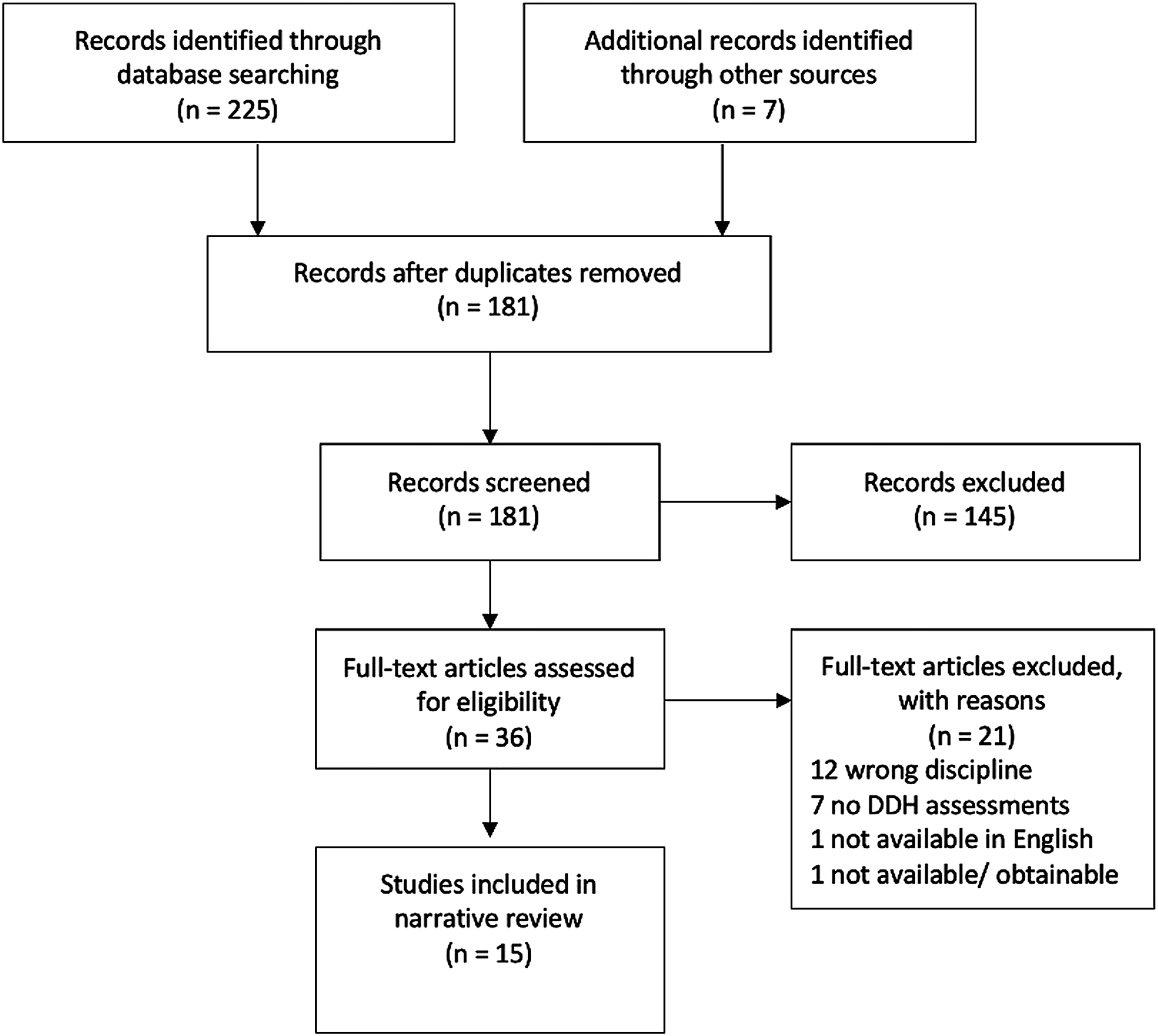
Data charting and collation
Summary of included articles.
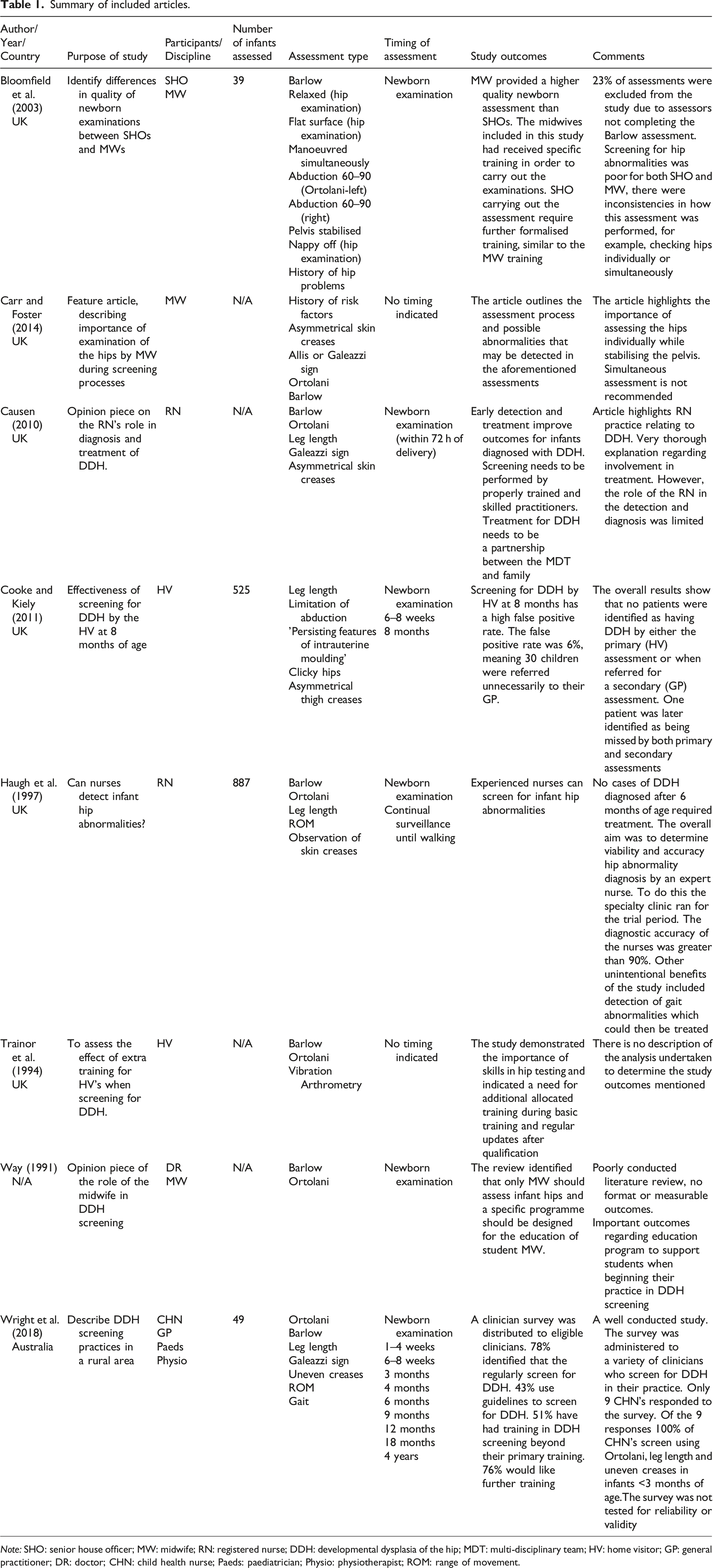
Note: SHO: senior house officer; MW: midwife; RN: registered nurse; DDH: developmental dysplasia of the hip; MDT: multi-disciplinary team; HV: home visitor; GP: general practitioner; DR: doctor; CHN: child health nurse; Paeds: paediatrician; Physio: physiotherapist; ROM: range of movement.
Summary of included practice guidelines.
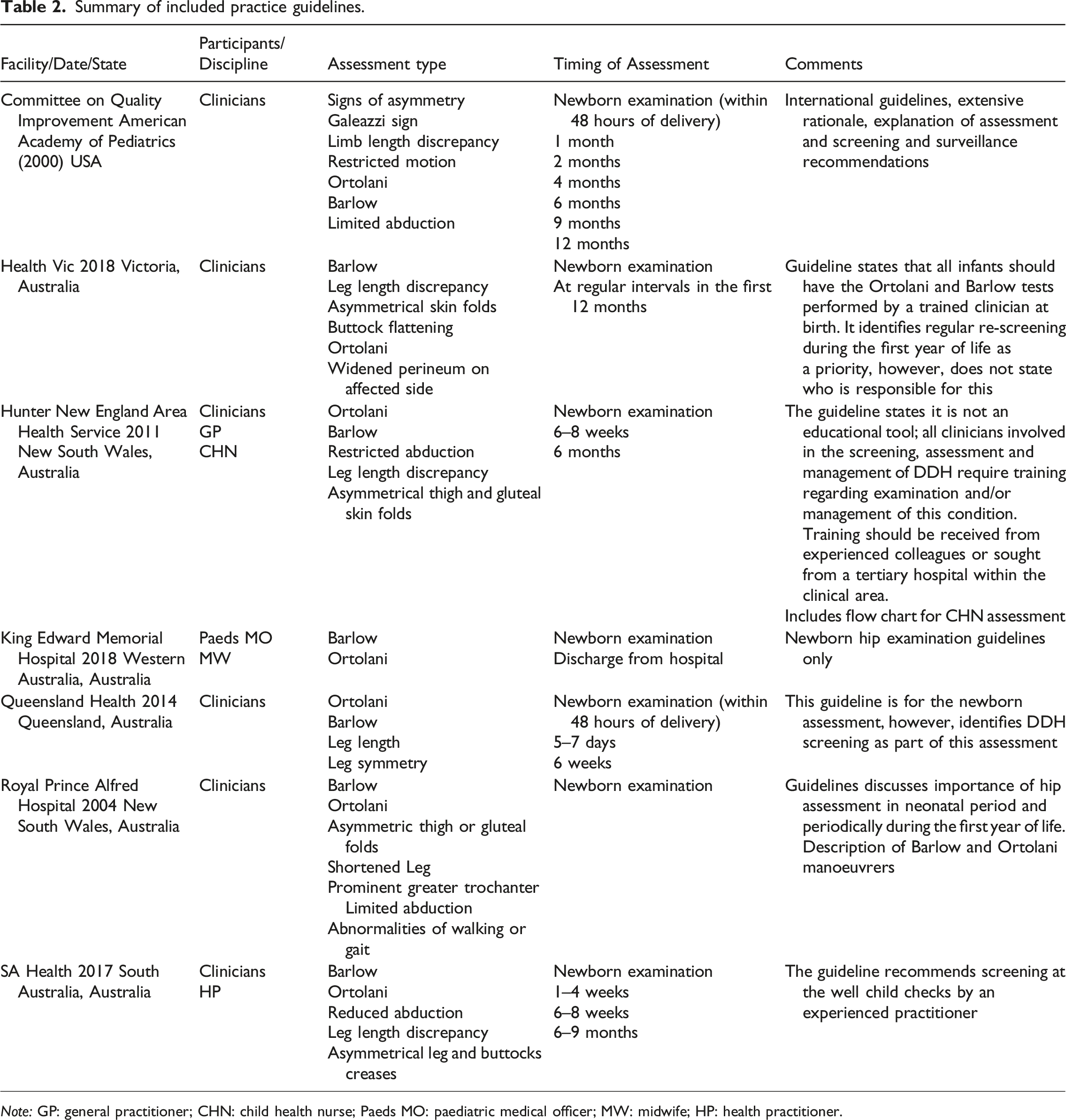
Note: GP: general practitioner; CHN: child health nurse; Paeds MO: paediatric medical officer; MW: midwife; HP: health practitioner.
Results
The fifth stage of the scoping review framework outlined by Arksey and O’Malley (2005) is to summarise and report the findings. A total of 15 (N = 15; 100%) sources of evidence met the inclusion criteria (Table 1 and 2). The sources included original research articles (n = 6; 40%), expert opinion pieces (n = 2; 13.3%) and practice guidelines (n = 7; 46.7%). There were 18 physical assessments to detect DDH identified, detail of these assessments is provided in Figure 2. All (N = 15; 100%) included sources identified assessments in three key areas; Barlow manoeuvre, Ortolani manoeuvre and assessment of legs (Bloomfield et al., 2003; Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Government of Western Australia, 2016; Haugh et al., 1997; New South Wales Health, 2004; New South Wales Health, 2011; Trainor et al., 1994; Queensland Government, 2014; Victoria State Government, 2018; Way 1991; Wright et al., 2018). A majority (n = 14; 93.3%) of the sources, identified the Barlow manoeuvre as a key assessment (Bloomfield et al., 2003; Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Government of South Australia, 2017; Government of Western Australia, 2016; Haugh et al., 1997; New South Wales Health, 2011, 2004; Trainor et al., 1994; Queensland Government, 2014; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). Although 13 (n = 13; 86.7%) of the included sources, identified the Ortolani manoeuvre as an additional screening assessment (Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Government of South Australia, 2017; Government of Western Australia North Metropolitan Health Service, 2016; Gross and Hitch, 1979; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Trainor et al., 1994; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). Finally, assessment of legs was identified in 11 (n = 11; 73.3%) included sources (Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Victoria State Government, 2018; Wright et al., 2018), assessments of legs included asymmetric skin folds, leg length discrepancy, Galeazzi sign, range of movement, limitation of abduction, leg symmetry and short femur sign. Summary of assessments identified through scoping review.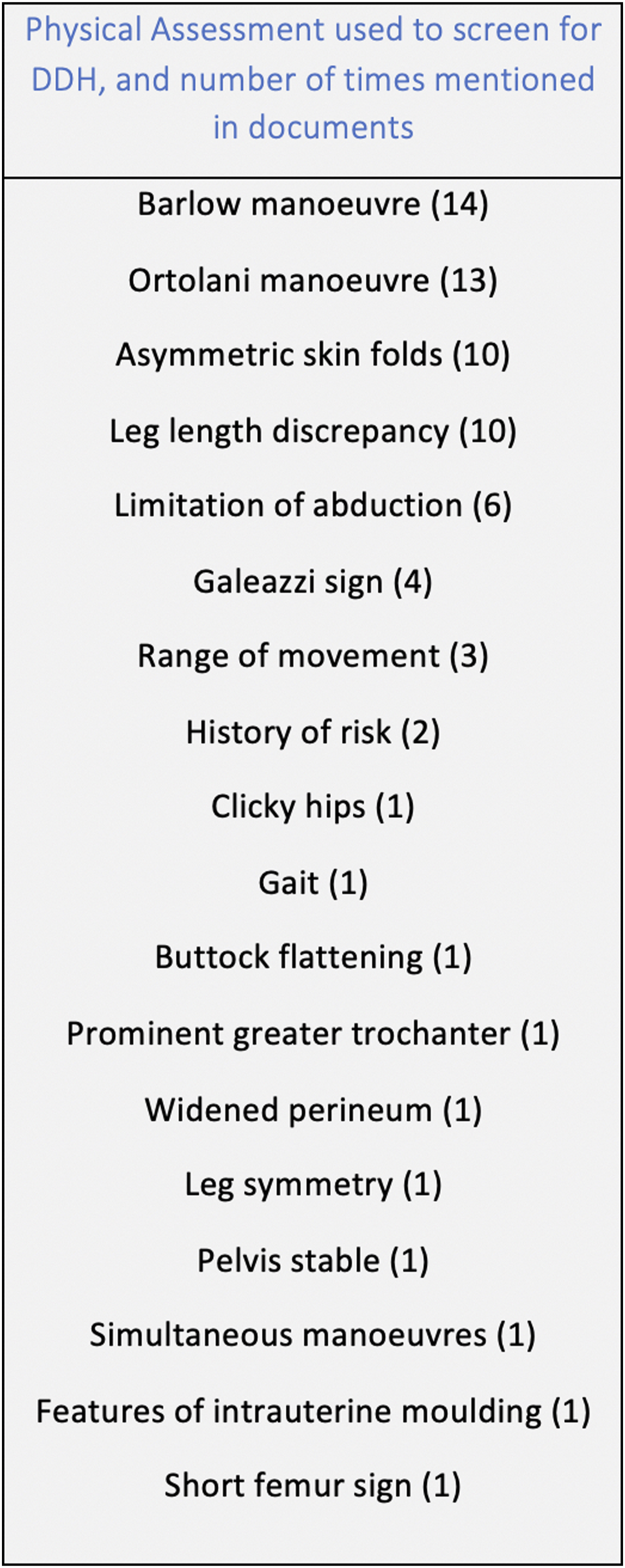
Discussion
The aim of this literature review was to identify and understand the physical assessments that nurses use when assessing for DDH, specifically as they relate to practice in Australia. This review identified three key assessments used in practice; Barlow manoeuvre, Ortolani manoeuvre and assessment of legs. Use of these physical assessments to screen for DDH is recommended in children from birth until four years of age and is commonly done by nurses at home visits and in clinical environments.
Barlow manoeuvre
The Barlow manoeuvre was first described by Dr Thomas Barlow, in Salford, England 1962 (Barlow, 1962). The manoeuvre involves adducting the infant’s hip and exertion of forward pressure applied behind the greater trochanter, each hip should be examined individually (Barlow, 1962). If the hip is dislocatable this gentle force will cause the head of the femur to slip out of the acetabulum (Barlow, 1962; Williams, 2018). The Barlow test is considered positive if the infant’s hip can be manually dislocated as described (Barlow, 1962; Williams, 2018). Due to the complexity of this assessment nearly all the included sources discussed the need for extensive experience and additional training to adequately complete the manoeuvre (Bloomfield et al., 2003; Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Government of South Australia, 2017; Trainor et al., 1994; Wright et al., 2018). Bloomfield et al. (2003) found both nurses and doctors inadequately performed the Barlow manoeuvre when rated by a specialist observer. An additional study supported this finding, showing that specific training and extensive experience was essential to detect hip abnormalities using the Barlow manoeuvre (Trainor et al., 1994). The complexity of this assessment means that one third to one half of positive findings will be missed when not conducted by a trained expert (Cooke and Kiely, 2011). No sources included information on the sensitivity or specificity of the Barlow manoeuvre when performed by nurses. Additionally, beyond the initial newborn examination it was not clear as to the timing of the Barlow manoeuvre when performed by nurses.
Ortolani manoeuvre
The Ortolani manoeuvre was first described by Dr Marino Ortolani in 1936 (Ortolani, 1937). The manoeuvre involves flexing and adducting the hip, then abducting the hip while applying gentle traction and pressure on the greater trochanter (Barlow, 1962; Williams, 2018). If the hip is dislocated the head of the femur will relocate into the acetabulum with a ‘clunk’ (Barlow, 1962; Williams, 2018). The Ortolani test is considered positive if the dislocated hip is able to be manually reduced as described (Barlow, 1962; Williams, 2018). The included sources which explained the Ortolani manoeuvre, identified either a ‘click’ or a ‘clunk’ when an assessment was positive (Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Government of South Australia, 2017; Government of Western Australia North Metropolitan Health Service, 2016; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Trainor et al., 1994; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). Additional studies have found that a ‘click’, however, is not a positive finding or an indicator of hip abnormality (Bolander, 2016; Committee on Quality Improvement, 2000). This inconsistency means that there is no agreement in the literature as to how the Ortolani manoeuvre should be performed. As with the Barlow manoeuvre there is no information as to the timing beyond the newborn period, sensitivity and specificity of the Ortolani manoeuvre in nurses screening practices.
Assessments of legs
Assessments of the legs included visual inspection for asymmetrical skin folds, testing for Galeazzi’s sign and assessment of leg length. To assess for asymmetrical skin folds, symmetry of the folds was observed bilaterally in the thigh buttocks and leg (Carr and Foster, 2014; Committee on Quality Improvement, 2000). Although the included sources stated that asymmetry of skin folds was a positive finding for DDH, a 2019 study has determined that this is not an accurate assessment for DDH (Kang et al., 2019). Four (n = 4; 26.7%) sources identified a positive Galeazzi sign as an indicator of DDH (Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Wright et al., 2018). Galeazzi sign is assessed when the infant is placed in the supine position with their knees and hips flexed, uneven knee height is considered positive for DDH (Committee on Quality Improvement, 2000; Williams, 2018). Similarly, to asymmetrical skin folds, 10 (n = 10; 66.7%) studies identified that a discrepancy in leg length was a positive indicator of DDH. This assessment was not described in any of the sources, and as with the Barlow and Ortolani manoeuvre no information was provided regarding the accuracy of this assessment. Overall, assessment of legs was the most common physical assessment performed by nurses in conjunction with the Barlow and Ortolani manoeuvre (Carr and Foster, 2014; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Victoria State Government, 2018; Wright et al., 2018).
Timing of assessment
In addition to the assessments performed, an area of interest was the timing of these physical assessments. Similarly to the assessments used, there is limited agreement in the literature as to when these assessments should occur and the appropriateness of these assessments in the ongoing screening process. Thirteen (n = 13; 86.7%) of the included sources identified specific times that the physical assessments should be used to screen for DDH (Bloomfield et al., 2003; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Government of Western Australia North Metropolitan Health Service, 2016; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). All of these 13 (n = 13; 86.7%) sources identified the newborn examination as the appropriate time to assess for DDH using physical assessment (Bloomfield et al., 2003; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Government of Western Australia North Metropolitan Health Service, 2016; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). There were though discrepancies in the timing of the newborn examination, with two (n = 2; 13.3%) sources stating the newborn examination should occur with 48 h post birth (Committee on Quality Improvement, 2000; Queensland Government, 2014) and another (n = 1; 6.7%) stating within 72 h post birth (Causon, 2010). Although the newborn examination is cited in the literature as a critical point for DDH assessment, the ongoing surveillance throughout early childhood is equally important (Committee on Quality Improvement, 2000). Despite the recognised international importance of screening into early childhood (Committee on Quality Improvement, 2000), only 8 (n = 8; 53.3%) of the included sources made recommendations that included forms of ongoing surveillance from birth until the age of four (Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Haugh et al., 1997; New South Wales Health, 2011; Victoria State Government, 2018; Wright et al., 2018). The included studies did not provide information on when particular assessments should be conducted with respect to the age of the infant and the accuracy of the physical assessment (Bloomfield et al., 2003; Causon, 2010; Committee on Quality Improvement, 2000; Cooke and Kiely, 2011; Government of South Australia, 2017; Government of Western Australia North Metropolitan Health Service, 2016; Haugh et al., 1997; New South Wales Health, 2011; New South Wales Health, 2004; Queensland Government, 2014; Victoria State Government, 2018; Way, 1991; Wright et al., 2018). The two predominant physical assessments identified in this review, the Barlow and Ortolani manoeuvres are reliant on the infant being relaxed and lying supine without its nappy, with a trained expert performing the assessments (Sewell et al., 2009). The Barlow attempts to dislocate an articulated femoral head; while the Ortolani aims to relocate a dislocated femoral head (Committee on Quality Improvement, 2000; Sewell et al., 2009). In a newborn muscle tone and soft tissues are lax; therefore, a dislocated hip may be easily manipulated using physical assessment (Sewell et al., 2009). As an infant develops muscle tone and changes in soft tissue occur, these physical assessments become less useful (Sewell et al., 2009; Paton, 2017). Therefore, to conduct an accurate physical assessment the Barlow and Ortolani manoeuvres may only be reliable in early infancy, in the first 2–3 months of life (Sewell et al., 2009).
Implications for practice
The primary aim of this scoping review was to identify the physical assessments used by nurses in the screening process for DDH. The review identified three key methods of assessment; Barlow manoeuvre, Ortolani manoeuvre and assessment of legs. All included sources emphasised the need for clinical expertise and additional training in physical assessment when performing these tests. Although both the Barlow and Ortolani manoeuvres will detect an unstable hip, they will not detect a dislocated irreducible hip or a stable hip with abnormal anatomy (Sewell et al., 2009). An assessment of leg length and hip abduction will assist clinicians in detecting a dislocated irreducible hip (Sewell et al., 2009). It has further been suggested that only an ultrasound will identify a stable hip with abnormal anatomy (Sewell et al., 2009). The complexities in understanding the pathology of DDH, performing the physical assessments, identifying the timing of the assessments and interpreting the screening results may mean that DDH is being under or over-identified, and subsequently under or over-treated.
Although this review specifically looked at the role of nurses, it is relevant for any health professional that is responsible for the initial and ongoing screening and surveillance of DDH.
Strengths and limitations
This literature review was undertaken in a systematic and rigorous way with advice from an Academic Librarian with respect to the search strategy. A limitation of this review is that only sources published in English were included. Therefore, relevant published sources in other languages may have been missed. Included practice guidelines were predominantly from Australian health facilities, reflective of the research teams’ location of practice. Additionally, while three key methods of assessment were identified, there was no information concerning the effectiveness of these physical assessments when performed by nurses.
This scoping review was constrained by the small number of sources that identified nurses as a clinician who screens for DDH. This limitation may have overlooked additional information regarding DDH assessment conducted by other clinicians.
Conclusion
This scoping review identified that there are 18 assessments that nurses use in practice to assess for DDH and many of these should only be performed by a trained expert. Despite recommendations for these assessments there is no reported evidence of diagnostic accuracy related to either the physical assessments used or the timing of these physical assessments.
It is recommended that future research examines nursing practice related to the assessment of DDH, including, nursing knowledge, attitude and practice relating to DDH, timing of assessment, and specificity and sensitivity of the physical assessments used. Further research in this area would potentially benefit all nurses and other health professionals who screen infants for DDH and increase associated detection and treatment rates for infants with DDH.
Supplemental Material
Supplemental Material for Nurses assessment of development hip dysplasia: A scoping review
Supplemental Material for Nurses assessment of development hip dysplasia: A scoping review by Larissa Smart, Lemuel Pelentsov, Jessie Childs, Nicole Williams and Adrian Esterman in Journal of Child Health Care
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.