
Abstract
This study compares the impact of children’s cardiac rhythm devices and health status on their parents with that of healthy controls. Furthermore, it aims to ascertain whether sociodemographic characteristics and medical data are associated with parent-reported impacts. This cross-sectional study is part of a comprehensive single-center study of long-term psychosocial outcomes in pediatric patients with pacemakers and implantable cardioverter defibrillators. The study includes 69 patients with their parents: 69 mothers and 57 fathers. Parents responded to the Pediatric Quality of Life Inventory Family Impact Module and to open-ended questions assessing impact on family life and treatment satisfaction. Parents reported more negative impact on family life than healthy controls in all three summary scores. Among fathers, presence of a child’s congenital heart disease and female sex is associated with lower family function. No group differences emerged regarding device type. Positive and negative cognitive aspects predominated for patients’ mothers and fathers. However, one substantial difference is that mothers reported more positive and negative emotional impact than fathers. We conclude that parents’ well-being should be addressed in clinical contexts, especially through emotional and practical support and open communication focused on parents’ worries and concerns.
Keywords
Introduction
Pediatric patients with heart diseases often require electrophysiological therapy (Saksena and Camm, 2012). For instance, congenital and acquired complete heart block is treated with pacemakers (PMs), and predisposition to ventricular tachycardia is treated with implantable cardioverter defibrillators (ICDs) (Koenig et al., 2004). Most of these patients suffer negative consequences that influence their health-related quality of life (HRQoL) (Czosek et al., 2015; Pyngottu et al., 2019; Werner et al., 2019a). For example, they are dependent throughout their lives on pacing therapy, including device-related revisions and complications (Allam et al., 2018). Moreover, patients’ lifestyle modifications such as activity restrictions and visible scarring can raise significant concerns like social withdrawal or depression (Allam et al., 2018).
There is strong evidence that child health status influences parents’ well-being (Bemister et al., 2014; Kaugars et al., 2018; Khanna et al., 2015; Kunz et al., 2011; Lazow et al., 2019; Muscara et al., 2015, 2017; Sischo et al., 2017; Wei et al., 2015; Werner et al., 2019a). For example, parents of pediatric patients with cardiac rhythm devices (CRDs) report post-traumatic stress symptoms even over long term (Werner et al., 2019a). It has been also reported that parents of children with more complex heart disease have poorer psychological health than healthy controls, including more stress, depression, and anxiety (Wray et al., 2018).
The impact of pediatric chronic health conditions on parents and families can be measured with the Pediatric Quality of Life Inventory
Only a few studies have examined the burden on parents of children with CRD. Knowledge about this may help to better support these parents in clinical practice. To capture their experiences and needs as precisely as possible, we chose an approach that combines quantitative and qualitative methods.
Our hypothesis was that parents whose children have CRDs would report more negative impact than parents of healthy controls. Furthermore, we were interested in knowing whether parent-reported impact levels were associated with sociodemographic and medical characteristics: child sex, age, socioeconomic status (SES), age at implantation, presence or absence of congenital heart disease (CHD), number of hospitalizations, device type, parent age, and marital status.
More qualitative information was gathered about the impact on patients and their families through one open-ended question. We were interested in knowing how satisfied parents were with consultations and treatment at the hospital. Thus, we asked the parents three structured-response questions and one open-ended question to evaluate parents’ satisfaction and their suggestions for improving treatment. Our hypothesis was that parents were satisfied with the treatment overall but would like more support and to receive more information about their children’s treatment and new developments in treatment options.
Aim
This study aims to compare the impact of children’s CRDs and health status on family functioning and parents’ well-being with that of healthy controls. Our study also aims to analyze associations between parents’ impact levels and sociodemographic and medical characteristics. Through qualitative analysis, it was aimed to identify additional parental concerns and suggestions for improving current forms of treatment, as well as gauging overall parental satisfaction.
Methods
Population and procedure
This cross-sectional case-control study was approved by the local ethical review board (Swiss ethics, Req-2015-0322) and conducted at the University Children’s Hospital of Zurich. All pediatric patients with CRDs between the ages 3 and 18 years, who were scheduled for regular follow-up visits at the cardiology outpatient clinic between September 2015 and September 2016, were asked to participate in this study. Patients were excluded if they had undergone PM or ICD implantation within the 3 months prior to study enrollment; this was to minimize the influence of acute medical interventions on impact. Further exclusion criteria were permanent residence outside Switzerland, lack of German language fluency, refusal to sign informed consent, and severe intellectual disability (Cummings, 2011). Healthy controls were matched in age and sex and recruited among friends of patients (40%) and from advertisements placed at university and community day care centers (60%). Interviews and standardized questionnaires were used to ensure that control participants had no chronic medical or cognitive impairments.
This investigation is part of a comprehensive single-center study of long-term psychosocial outcomes in pediatric CRD patients (Werner et al., 2019a, 2019b). All parents and adolescents >14 years provided written consent after study procedure and aims had been explained in detail and all children provided verbal consent.
The child’s medical data were collected retrospectively from medical records. All questionnaires were sent by post and completed at home. After deadline, reminders were dispatched. The completed questionnaires were returned by post.
Measures
Family functioning and parent HRQoL
The validated German version of the PedsQLTM 3.0 FIM (Muscara et al., 2017; Varni et al., 2004) measured the impact of a chronic pediatric health condition on parents’ self-reported family functioning and HRQoL in the previous 4 weeks. The questionnaire contains 36 items, which respondents answer on a five-point Likert scale ranging from never a problem (0) to almost always a problem (4). It comprises of eight subscale scores: physical functioning (six items), emotional functioning (five items), social functioning (four items), cognitive functioning (five items), communication (three items), worry (five items), daily activities (three items), and family relationships (five items). Three summary scores are calculated: (1) Parent HRQoL Summary score, calculated from mean values for physical, emotional, social, and cognitive functioning; (2) Family Functioning Summary score, calculated from mean values for daily activities and family relationships; and (3) Total Impact score, computed from mean values for all eight subscales. The items are reverse-scored and linearly transformed to a 0–100 scale so that higher score represents better functioning.
Parents’ feelings, opinions, and concerns regarding the influence of their children’s disease on their lives
To gather more information on the subjective impact on parents’ lives, mothers and fathers separately answered one open-ended question: “How did the PM or ICD of your child affect your own life as a mother or father?”. No answer categories were provided, and parents were free to record their written responses as they chose. Their answers were analyzed as described below.
Parental satisfaction with treatment
Parents’ satisfaction with treatment at the hospital was rated by both parents on a five-point -Likert scale. Parents were asked to indicate the extent to which these three statements applied: 1) “I am very satisfied (5) to not satisfied (1) with medical treatment of my child”, 2) “The consultation that my child and we as parents have received was very competent (5) to not at all competent (1)”, and 3) “The opportunity to discuss concerns and questions’ rated from ‘completely acceptable’ (5) to ‘not at all acceptable’ (1)”. Additionally, one open-ended question was asked: “What should be changed in the future and/or added regarding treatment and consulting of families with similar problems?”. Their answers were analyzed as described below.
Parents and children’s sociodemographic data and children’s medical data
Children’s ages, sex, device type, ages at device implantation, presence of CHD, and number of hospitalization days were taken from medical records. SES was assessed from maternal education and paternal occupation on a scale ranging from 2 to 12 points, with 2 being the lowest and 12 being the highest. The scores were then divided into three SES categories: low SES score (2–5), mid-range SES score (6–9), and high SES score (10–12). This classification has proven reliability and validity as an indicator of SES in Switzerland (Largo et al., 1989).
Parents’ ages and marital status were gathered in a short demographic questionnaire answered by the parents.
Content analysis
To form answer categories, answers for each question were first entered into an Excel file (Microsoft Excel for Mac 2019, Version 16.30). Each entry was double-checked to ensure that answers were completely and correctly copied. Mayring’s procedure was used to inductively form categories from all the material provided by parents in these steps (Mayring, 2015; Kuckartz, 2016). First, the material was summarized so that answers only included their key content. Second, answers were transformed to a uniform language level. These remained as close as possible to the original text, and interpretation was avoided. Third, the paraphrases were generalized, those with identical meanings were bundled, and those with similar meaning were deleted after agreement between two raters was reached. MAXQDA software Version 12 (MAXQDA, Version 12, 1995–2018, VERBI Software-Consult-Sozialforschung GmbH, Berlin, Germany) was used to assign all the paraphrases to categories.
The answers about “parents’ feelings, opinions, and concerns regarding the influence of their child’s disease on their lives” were categorized as follows: In the first round, categories were formulated with positive, negative, and neutral/no effect. Then, the World Health Organization’s (WHO) definition of health was used to provide four subcategories: motor, physical, cognitive, and emotional functioning (Nobile, 2014). After the first round, three more categories were added: time, job, with negative responses only, and other. The category for other was formed for miscellaneous answers.
Example items for motor behavior include “Thanks to the device, we were able to be more active during leisure time than before” (positive) and “We always needed a lot of time to plan family holidays and activities, and especially to check how near hospitals were” (negative). Example items for cognitive behavior include “We thought the PM/ICD made child’s heart and life safer” (positive) and “We always worried about our child’s future” (negative). Example items for emotional behavior include “We were very thankful for the PM”; “We were less worried about child’s life” (positive) and “We were very fearful and anxious” (negative). Example items for time include “More time spent as a family doing physical activities like hiking” (positive) and “All the doctors’ appointments are a big- and stressful-time commitment” (negative). An example item for the job category is “It was no longer possible to do a job”. All answers describing no change were categorized under neutral/no effect. Example items include “Our daily routine was not restricted at all” and “We’ve had no change since PM implantation”.
The responses for “parental satisfaction with treatment” were grouped in nine categories: (a) “more transparent and open communication between the medical team and patients’ family”, (b) “support with administrative affairs”, (c) “freely accessible psychiatric and psychological counseling”, (d) “increased competence and individual medical care”, (e) “inclusion and more responsibilities in medical routine process”, (f) “providing up-to-date scientific information on CRD development and procedures”, (g) “more offers for networking with other parents”, (h) “no change”, and (i) “unclassifiable”.
Statistical analysis
Data were analyzed using SPSS 23 for MAC (IBM Corp., Armonk, NY). All tests with a p-value of p ≤ 0.05 were considered statistically significant. Variables with non-normal distributions (Kolmogorov-Smirnov test) are presented with median and interquartile range (IQR), others with mean and standard deviation (SD). Chi square and Mann–Whitney U-tests were used to conduct the dropout analysis between participants and non-participants and compare child’s sex, age at study beginning, device type, age at implantation, pre-existing CHD, total days of hospitalization and intake of medication. Wilcoxon signed-rank tests were performed to compare the PedsQL FIM scores between patients’ parents, parents of healthy controls, and patient mothers and fathers. Mann–Whitney U-tests were used to compare the impact level between subgroups (females/males, PM/ICD, and CHD/no CHD). Kendall Tau correlations were estimated for associations between PedsQL FIM scores and sociodemographic and medical data. Wilcoxon signed-rank tests were performed to compare mothers and fathers’ satisfaction with treatment. The strength of the relationship is based on Cohen’s d; suggested interpretations of values are <0.2 small, 0.5 (>0.2 and <0.8) medium, and >0.8 large effects (Cohen, 1992).
Results
Participants
The study included 69 participants from 89 eligible patients with a PM or an ICD (80% response rate). Overall, 20 patients did not participate, for these reasons: lack of time (n = 15), lost to follow-up (n = 4) and one family with two affected children (n = 1). Study participants did not differ significantly from the 20 non-participants in their sex, age at study beginning, device type, age at initial device implantation, presence of structural CHD, use of any medication, or total length of cardiac hospitalization.
Sample characteristics
The average age of patients at assessment was 11.2 years (SD = 4.6, n = 27, 39% females, n = 55, 80% had a Swiss nationality). The median age at device implantation was 4.2 years (IQR = 6.9). In all, 56 patients (81%) had a PM and 13 (19%) had an ICD. Some 38 of the 69 (55%) suffered from a CHD. The median duration of hospital stays for cardiac monitoring and treatment was 32 days (IQR = 58). The mean age of the mothers was 41.7 years (SD = 5.9) and of the fathers 44.4 years (SD = 7.4). Nearly all parents were married or lived together (n = 54, 84%) while 8 parents (12%) were divorced or lived separately, and 3 parents (4%) had missing values. Concerning SES, 17 patients (25%) had a high, 49 (71%) a mid-range, and 3 (4%) a low SES score.
Family functioning and parent HRQoL
Descriptive statistics for PedsQL FIM scores of mothers and fathers of children with PM and ICD device: comparison with control group and between mothers and fathers.
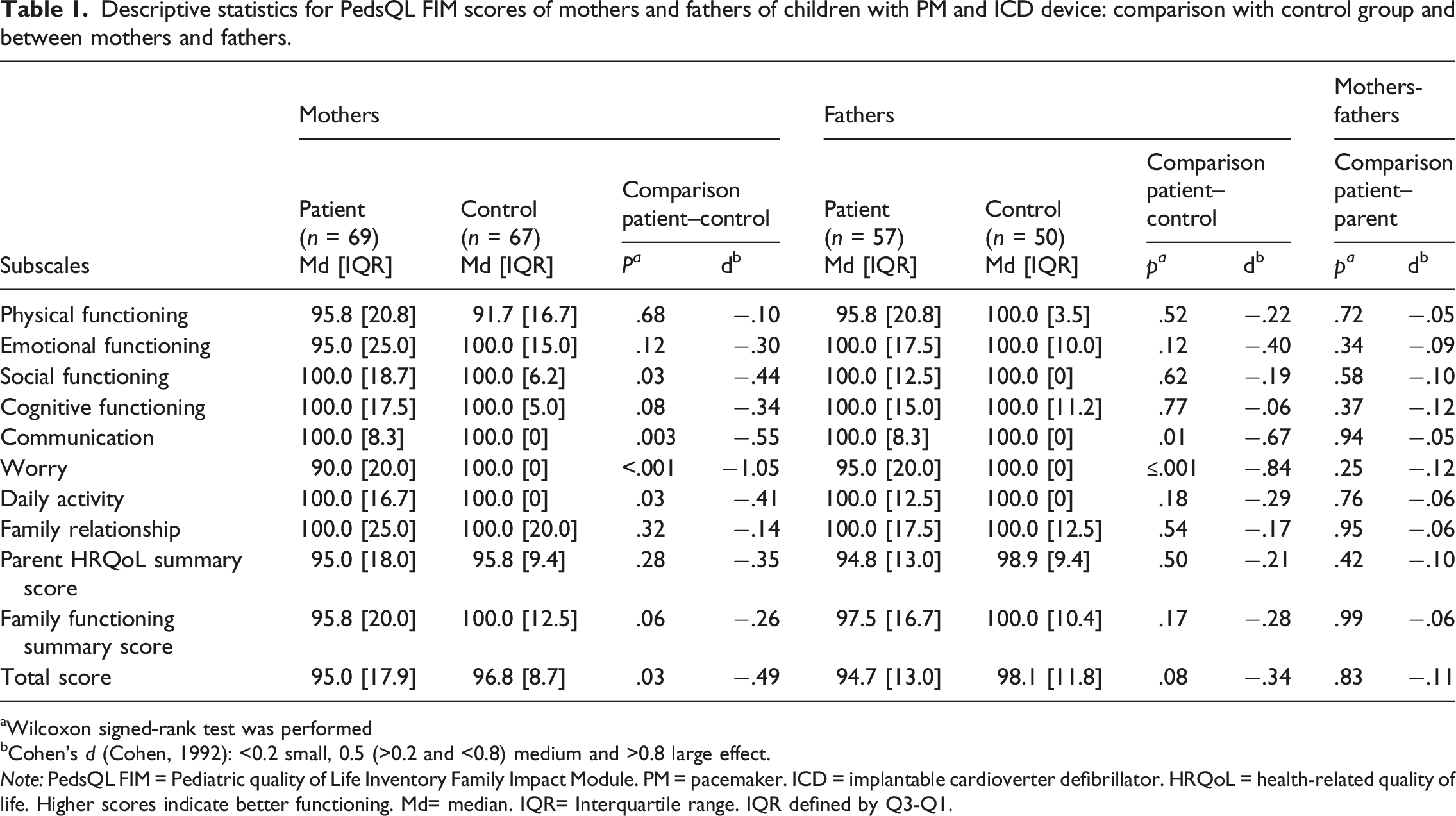
Wilcoxon signed-rank test was performed
Cohen’s d (Cohen, 1992): <0.2 small, 0.5 (>0.2 and <0.8) medium and >0.8 large effect.
Note: PedsQL FIM = Pediatric quality of Life Inventory Family Impact Module. PM = pacemaker. ICD = implantable cardioverter defibrillator. HRQoL = health-related quality of life. Higher scores indicate better functioning. Md= median. IQR= Interquartile range. IQR defined by Q3-Q1.
Patients’ mothers and fathers showed lower PedsQL FIM scores with medium effect sizes than healthy controls in all three summary scores, but with exception of lower total scores for patients’ mothers, no statistically significant differences emerged. Patients’ mothers and fathers showed no statistically significant differences on any of the subscales or the three summary scores.
Family functioning and parent HRQoL by parents’ and children’s sociodemographic data and children’s medical data
No associations were found between child age, age at implantation, number of hospitalizations, SES, parent age, marital status and PedsQL FIM scores. Statistically significant associations were found between fathers’ family functioning summary score and child’s sex r = −.28, 95%CI [-.49,-.04] and CHD r = −.24, 95%CI [−.47, −.001].
Mothers’ and fathers’ PedsQL FIM summary scores and total score compared separately for patients’ sex, device type, and CHD.
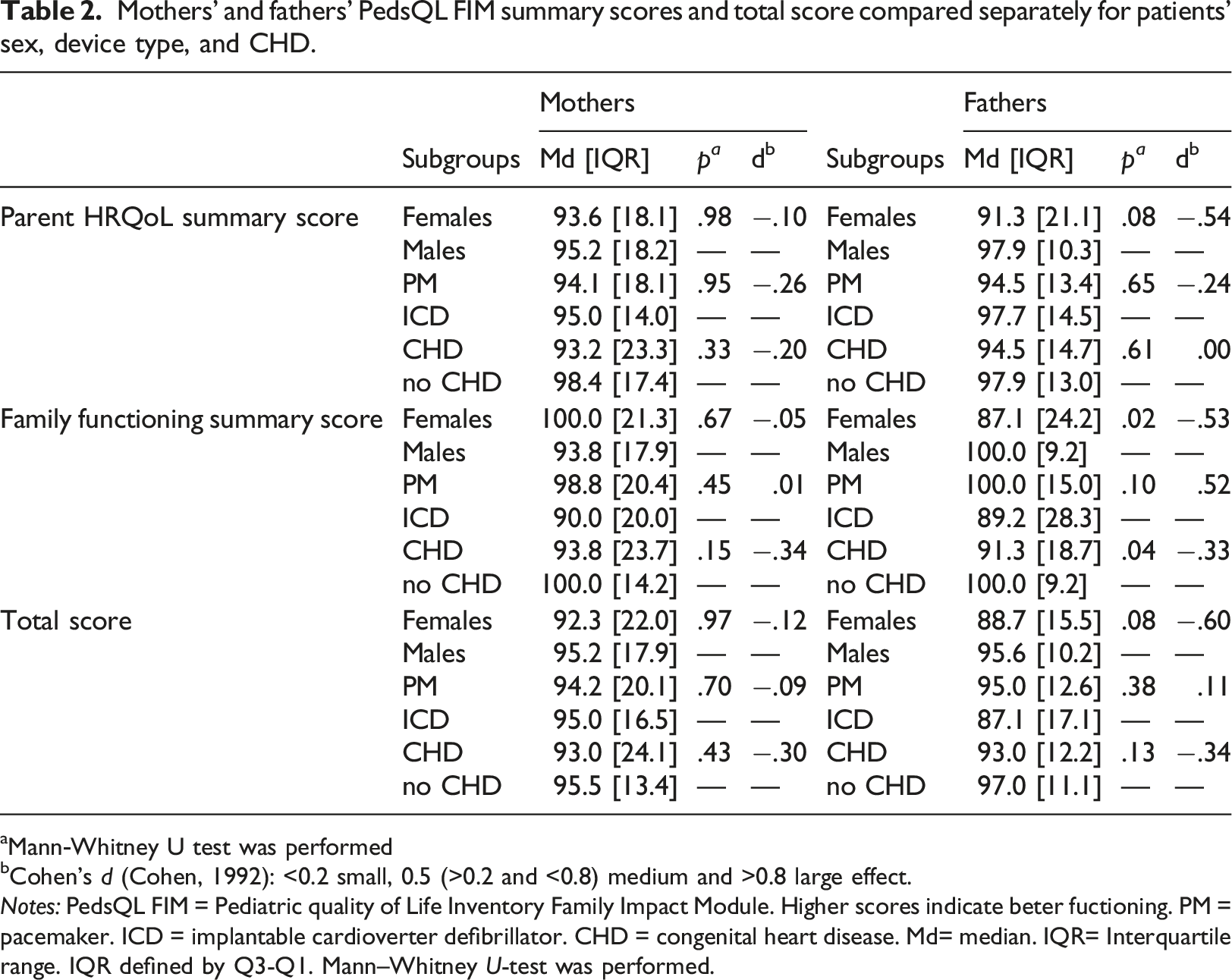
Mann-Whitney U test was performed
Cohen’s d (Cohen, 1992): <0.2 small, 0.5 (>0.2 and <0.8) medium and >0.8 large effect.
Notes: PedsQL FIM = Pediatric quality of Life Inventory Family Impact Module. Higher scores indicate beter fuctioning. PM = pacemaker. ICD = implantable cardioverter defibrillator. CHD = congenital heart disease. Md= median. IQR= Interquartile range. IQR defined by Q3-Q1. Mann–Whitney U-test was performed.
Parents’ feelings, opinions, and concerns regarding the influence of their child’s disease on their lives
Mothers provided 110 statements and the fathers 66 statements about the influence of their child’s CRD on their lives. Overall, 35 statements (32%) by mothers and 25 (38%) by fathers were classified as positive, 67 (61%) by mothers and 34 (51%) by fathers as negative, and 3 (3%) by mothers and 5 (8%) by fathers as neutral; 5 (4%) by mothers and 2 (3%) by fathers remained unclassified (Figure 1). (a)–(d) Parents subjective involvement: Frequencies and detailed classifications of parental statements concerning the influence of the child’s cardiac rhythm device on the parents’ lives evaluated by content analysis.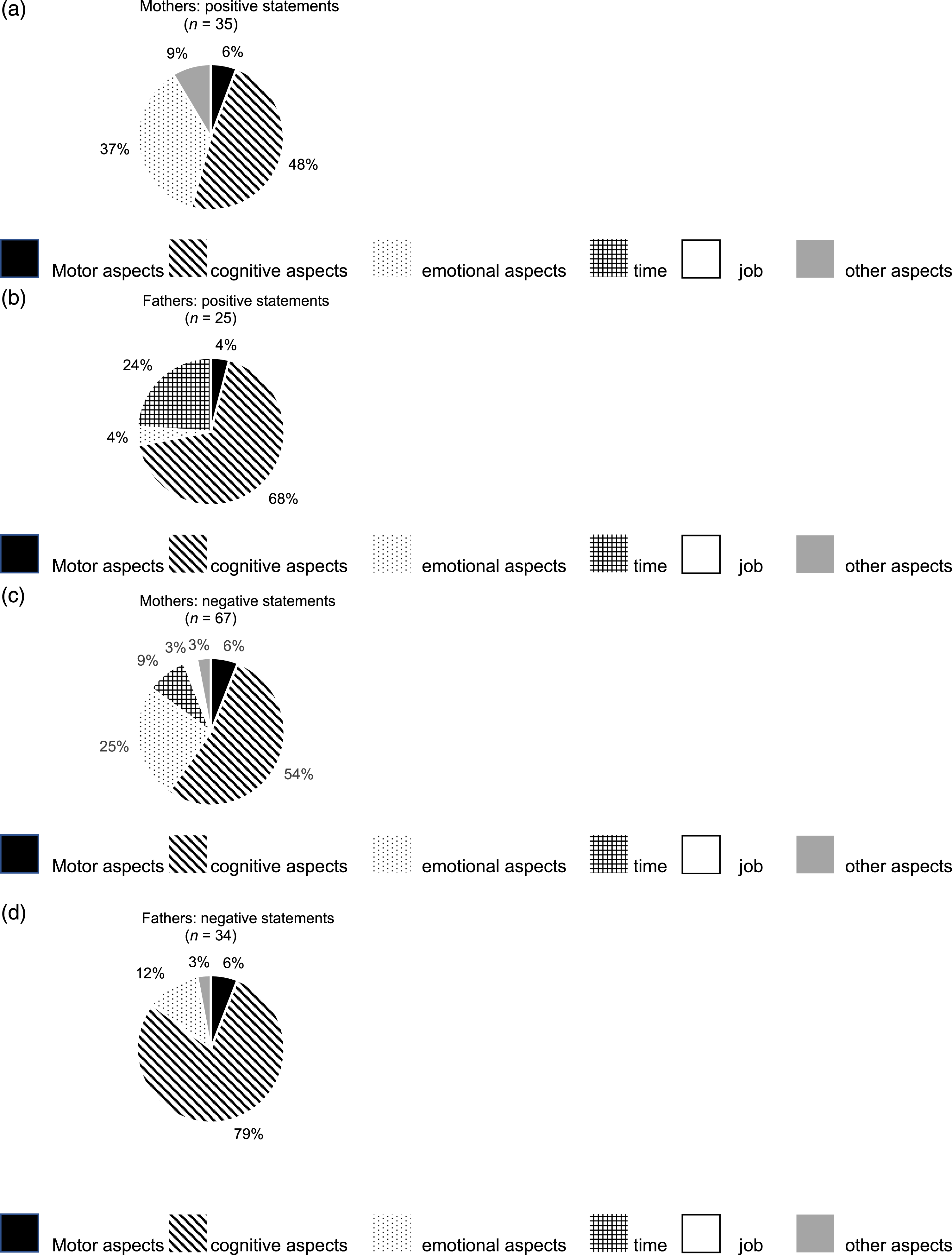
Among positive statements, cognitive aspects were most frequently mentioned by both parents, but few parents mentioned motor aspects. The greatest difference between mothers and fathers was for emotional aspects, which predominated among mothers (n = 13, 37%), but not among fathers (n = 1, 4%). Furthermore, 6 of the fathers (24%) mentioned positive aspects of time, which no mother reported.
Among negative statements, the dominant answer category for both parents was that for cognitive aspects. Again, one substantial difference was that mothers reported more emotional impact than fathers (n = 17, 25% vs. n = 4, 12%). Moreover, only mothers mentioned negative issues about time and job, but no such negative impact was reported by fathers.
Parental satisfaction with treatment
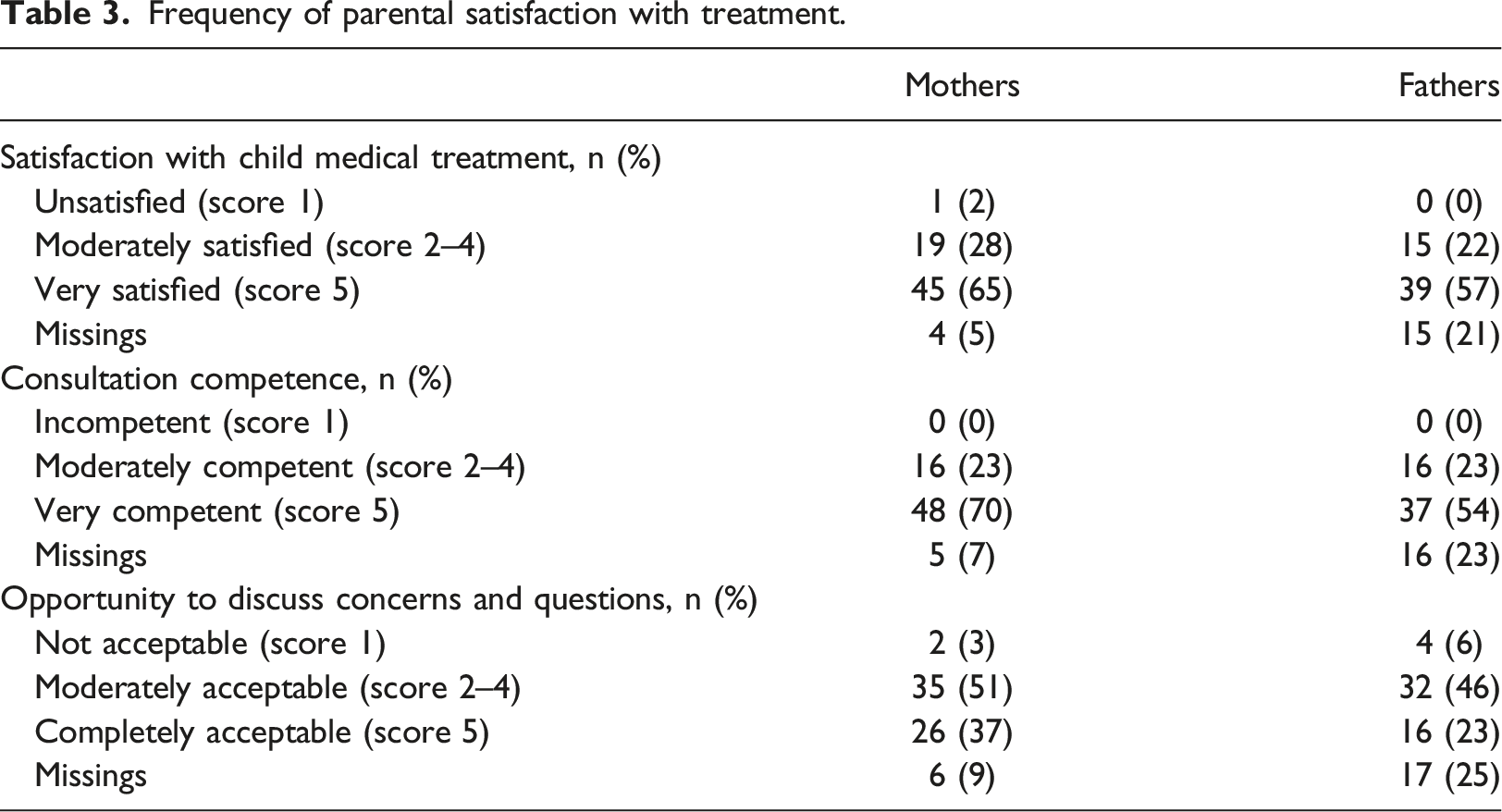
Frequency of parental satisfaction with treatment.
Suggestions
More “transparent and open communication between the medical team and patient’s family” was suggested by most parents (mothers n = 10, 25%; fathers n = 10, 25%). This was followed by “freely accessible psychiatric and psychological counseling” (mothers n = 6, 15%; fathers n = 1, 3%), “inclusion and more responsibilities in medical routine processes” (mothers n = 5, 13%; fathers n = 2, 5%), “increased competence and individual medical care” (mothers n = 4, 10%; fathers n = 5, 13%), “providing up-to-date scientific information on CRD development and procedures” (mothers n = 4, 10%; fathers n = 3, 8%), “more offers for networking with other parents” (mothers n = 4, 10%; fathers n = 0), and “more support with administrative affairs” (mothers n = 1, 3%; fathers n = 10, 25%), no change (mothers n = 1, 3%; fathers n = 3, 8%), and unclassifiable (mothers n = 4, 10%; fathers n = 4, 10%).
Discussion
Our study showed that both mothers and fathers of children with CRDs reported more negative impact on family life than healthy controls. Whether a child had a PM or an ICD implanted was not statistically different in this regard, but the presence of a child’s CHD was associated with lower family functioning. Especially fathers of children with CHD reported greater impact than fathers of children without CHD. Also, fathers of female children reported lower family functioning than fathers of male children, while no such effect was found for the mothers. Our qualitative approach showed some more details about the impact of children’s CRDs on families. Both mothers and fathers reported most frequently positive and negative cognitive aspects such as hopes or worries, whereas mothers reported more positive and negative emotional impact than fathers. Although most parents were very satisfied with their child’s medical treatment, they wished to get more “transparent and open communication between the medical team and patient’s family”.
Family functioning and parent HRQoL
This study, with a high response rate, is the first to compare family functioning and parent HRQoL in parents of children with CRDs with parents of healthy controls. Family functioning and parent HRQoL (summary scores) were not significantly lower in the control group. Regarding subscales, our results show that parents of children with CRDs have more worries than parents of healthy controls which is in line with our hypothesis. These are worries about possible effects of the disease on other family members, about their child’s medication and its possible side effects, and about their child’s future.
In addition, they reported more communication problems. This includes hesitation in talking to people outside the family about their child’s health status, feeling misunderstood in conversations with people who do not know their child’s medical history, and inhibition when talking to health care professionals about their own feelings.
Patients’ mothers reported lower social functioning and more problems with daily activities, resulting in greater overall impact on family functioning than mothers of healthy controls. This is in line with previous studies (Caicedo, 2014; Jelenova et al., 2015).
Family functioning and parent HRQoL by patients’ sex, device type, and CHD
Fathers reported greater impact, especially reduced family functioning, when their child was a girl. This might indicate that fathers have more difficulties in communicating with girls when they are sick.
Our study included 55% CHD patients, and our results confirmed our hypothesis, which was that mothers and fathers of children with CHD reported lower family functioning than controls. This could be because children affected by CHD have more complex health problems, entailing more medical treatment, longer hospital stays, and more physical limitations (Ruggiero et al., 2018).
No differences were found regarding parental family functioning and HRQoL between the PM and ICD groups. This might be due to our sample size, which included only 13 ICD patients.
Parents’ feelings, opinions, and concerns regarding the influence of their child’s disease on their lives
Our qualitative analysis showed that most negative statements reported by patients’ parents involved both cognitive and emotional aspects. Parents frequently described worries about such aspects of their child’s future as schooling, job opportunities, and health conditions.
Parents described limitations to their child’s free time activities and constant worries about physical threats such as magnets in their child’s surroundings and about the functioning of the device. Moreover, parents mentioned fear and anxiety concerning their child’s health status, such as dependency on the CRD.
The answers to the open-ended question found some disparities between mothers and fathers. Cognitive aspects predominated the positive and negative statements of both mothers and fathers, but the mothers’ responses to both positive and negative statements had more emotional content than fathers’. This might indicate that mothers carry more of the emotional burden than fathers, or that they generally talk more easily about their feelings (Goldshmidt and Weller, 2000).
The fathers’ positive statements included time aspects (e.g., spending more time with their children), which none of the mothers mentioned. This might be because fathers might attach a higher value to activities such as sports and spending time outside with their children. In contrast, mothers only mentioned time aspects in negative statements. This might be because mothers are the primary caregivers and thus take the patients to all their medical appointments and stay with them at the hospital, Also other studies with parents of children with a chronic health condition show more negative impact on mothers than fathers (Carmassi et al., 2018; Jönsson et al., 2015; Nieuwesteeg et al., 2017).
The open-ended questions were predominantly answered by mothers (63% of all answers), rather than by fathers (35% of all answers). Thus, we can only speculate about why fewer fathers responded to these questions. Open-ended questions might have required more time than the structured questionnaire and thus might have seemed less manageable and attractive. In addition, they might have believed they lacked the ability to express their worries and concerns adequately through this format.
Parental satisfaction with treatment and suggested improvements
The finding that most parents were satisfied with the treatment their child received, is itself very satisfactory. However, parents also suggested some improvements. Recommendations most frequently offered were for “transparent and open communication between the medical team and the patient’s family”, “increased competence and individual medical care”, and “providing up-to-date scientific information on CRD development and procedures”. Of course, every hospital and medical team works every day to provide the best treatment, but these suggestions imply that more work is needed to enhance treatment. This may include extending consultation time to allow parents to raise their personal concerns, ask about the latest scientific information and discuss ways to tailor the therapy more closely to each patient’s medical needs and personality.
Another improvement the parents suggested was a “parent networking group”. Such a group could be formed quite simply, by providing all parents information about such groups and options on how to join. It could benefit overall satisfaction with the pediatric healthcare service, as there is evidence for a positive impact of social network and support groups on coping with worries about children’s diseases (Sigurdardottir et al., 2017; Tak and McCubbin, 2002). Some parents mentioned the need for “more support with administrative affairs”. This aspect has been mentioned previously by parents of chronically ill children including diabetes mellitus, asthma, epilepsy, chronic renal failure, and cancer (Fawcett et al., 2005). A networking group would also enable parents to help each other out by exchanging information about such problems.
In addition, parents suggested “freely accessible psychiatric/psychological counseling”. In fact, psychiatric and psychological counseling is already available and good evidence has demonstrated the importance of counseling in parents of children with chronic disease (Eccleston et al., 2015). To this end, perhaps counseling should be offered routinely during hospital visits and at follow-up appointments.
Study limitations
Our study entails some limitations that merit note. First, the qualitative approach is a form of research in which room for interpretation remains, even if we have strictly followed all suggestions provided (Mayring, 2015). Second, not all parents answered the open-ended question, and therefore these answers do not represent our cohort completely. Third, we had only 13 ICD patients, which limits the statistical power of any subgroup analyses. Also, a type II error might be more likely because of our sample size. Moreover, generalizing from our data to any population of parents of children with CRDs might be problematic. However, the catchment area of the University Children’s Hospital of Zurich is extensive, because only a few hospitals in Switzerland treat pediatric patients with CRDs. Multicenter international studies could be conducted to increase the power in future studies. Fourth, although our two study groups were matched in terms of age and sex and about 80% of the participants in both groups had a Swiss nationality, more participants of the control group (46%) had a high SES score than of the patient group (24%). Furthermore, there may be other differences that may have influenced the study results. Also the possibility that some cross-contamination occurred between patients and controls cannot be excluded, since 40% of the controls were recruited via patients’ best friends which is a convenient but not ideal source of controls (Bunin et al., 2011; Wacholder et al., 1992)). Fifth, as most of our parents presented a mid-range (71%) and high (25%) SES score, our results are not representative for the whole population. The SES of patient group differed from the general population, in which 40% presents a high, 38% a mid-range and 42% a low SES score (Huwiler, 2002). The reason for this bias could be either that non-German-speaking parents were excluded from participation in the study or that among eligible families, those with a low SES score might have declined participation because they had fewer resources to cope with their child’s disease.
Implication for practice
The impact of CRDs of pediatric patients on family functioning and parents’ HRQoL could be positively influenced by providing more up-to-date medical information on new developments and procedures concerning CRDs and by offering a parenting networking group. Moreover, additional appointments may need to be scheduled if some questions remain unanswered. Furthermore, psychiatric and psychological support could be broadened as could counseling for parents, concerning educational issues, parenting sick children, and help dealing with broader health related stress issues (such as learning relaxation techniques and managing anxiety).
Conclusions
Our study illustrates some long-term impacts of pediatric PMs and ICDs on parents. Future focus in clinical context should be on the parents’ well-being, especially on emotional and practical aspects and open communication to reduce parents’ worries and concerns. The difference between the answers given by mothers and fathers leads us to suggest addressing them individually.
Footnotes
Acknowledgements
We thank Silvia Hilfiker, Karin Steinmann, and Alina Rüegg for patient recruitment and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: We thank the Stiftung for “Herzschrittmacher und Elektrophysiologie” for their support.
Ethical approval
The study was approved by the ethical review board of the Canton of Zurich, Switzerland, and was performed in full accordance with the Declaration of Helsinki.