
Abstract
While race and ethnicity have been acknowledged as determinants of health, there remain gaps regarding their effects on experiences of paediatric care. This scoping review examines empirical literature regarding the state and experience of paediatric care provided to racially and ethnically diverse families in North America. We seek to clarify the needs of care administrators and recipients, as well as to conceptualize what paediatric care must look like to enable equitable practices and optimal health outcomes. Utilizing Arksey and O’Malley’s framework, we reviewed literature published between 2005 and 2020, most of which was written within an American context. The literature reviewed featured quantitative, qualitative and mixed methods studies. Paediatric care administrators and recipients collectively identified the following as domains requiring an increased focus: (1) knowledge (awareness or training), (2) alignment of views and values, (3) resources and (4) communication. Findings suggest overall that despite there being merit in the cultural competency efforts underway, more patient-centric approaches are vital. This review concludes by encouraging the sustained development of cultural safety initiatives in paediatric care to ultimately promote patient comfort and provider-patient collaboration.
Keywords
Introduction
Although the healthcare system plays a central role in ensuring a child’s safety, health and well-being (Seid et al., 2003), the ways in which parents and children are able to interact with the healthcare system vary drastically on the basis of race and ethnicity (Cheng and Goodman, 2014; Kelly et al., 2012; Pachter and Coll, 2009; Riera and Walker, 2010; Seid et al., 2003; Wright et al., 2019). Despite cultural variations in how parent–child relationships are conceptualized and managed, they are often marked by an inherent tendency toward nurturance and protection (Seid et al., 2003). Paediatric health care providers enter this dynamic as co-facilitators, assisting parents in ensuring that their children are on a life path conducive to their overall health and well-being. However, the predisposition of racialized families to having negative experiences in seeking and receiving paediatric care consequentially sets their children on a trajectory for negative health outcomes in the future (Cheng and Goodman, 2014; George and Bassani, 2018; Pachter and Coll, 2009; Priest et al., 2018; Seid et al., 2003; Wright et al., 2019).
Membership in a racialized group is imposed by social structures and beliefs which regard race as a socially assigned classification (Jones et al., 2008). In this article, the term ‘racialized’ refers to those who have experienced discrimination, whether implicitly or explicitly, as a result of their race, ethnicity or skin colour. Interactions between racialized families and the healthcare system have been described in academic literature as promotive of risky health behaviours and discouraging of help-seeking behaviours (Hyman, 2009; Powell et al., 2016; Williams et al., 2003, 2019).
While many health inequities stem from institutionalized forms of structural racism, both directly through access to healthcare, and indirectly, through variations in psychosocial stress load (Brondolo et al., 2009), some variance in the experiences of racialized and ethnic minorities can be explained by cultural differences. Culture is conceptualized as the latent construct which underlies analysis of race and ethnicity – otherwise described as a categorical variable that enables the dissection of groups (Murry et al., 2001). Further, its unifying nature can be utilized as a means of explaining the manifestation of racial and ethnic differences, as well as to broaden understanding of human development (Murry et al., 2001). Primary care, when provided appropriately, can assist in mediating racial and ethnic inequities (Wright et al., 2019). While favourable provider–patient interactions and positive experiences of care are important in any medical practice, this topic is particularly important for paediatrics, as paediatric health care providers are expected to not only manage communication with their patients, but with the parents or caregivers of these patients as well. Addressing the cultural needs of racialized patients, their families and health care providers may simultaneously be a means of prevention for negative health outcomes of racialized children, as well as a solution to mitigating the effects of racially and ethnically rooted disparities. This scoping review examines what is known in existing peer-reviewed, empirical literature regarding the paediatric care provided to racially and ethnically diverse families in North America.
The prospect of equitable standards of paediatric care has been associated with culturally competent practices since their emergence (Stanley, 2006). Cultural competency, although lacking a single agreed-upon definition, is based on the assumption that health care providers should be expected to possess a certain amount of cultural knowledge in providing care to patients of various cultural backgrounds (Stanley, 2006). Cultural competency does have its merits as one of the first concepts utilized in healthcare practice which considers the cultural needs of the patients, but it has recently been criticized for its portrayal as a skill that can be ‘acquired’ by health care providers through training (Stanley, 2006). This perception contributes to a hindrance in the advancement of equitable care measures seeing as the true necessity is in actively enabling such practice as opposed to a static acquisition of knowledge.
There is a duality in the patient–provider relationship whereby cultural discrepancies are felt on both ends (Patel et al., 2018; Sakai et al., 2019; Wald et al., 2014), and ‘cultural safety’ may be a potential solution in addressing these discrepancies. Cultural safety has recently emerged as an approach that holistically considers the role of social and historical contexts, as well as structural and interpersonal power imbalances, in influencing the healthcare experiences of patients (Anishnawbe Health Toronto, 2011; National Aboriginal Health Organization, 2009). The key difference between cultural competency and cultural safety is the conceptualization of power (Curtis et al., 2019). Whereas cultural competency tends to maintain that power is in the hands of the health care provider, cultural safety confronts interpersonal power differences in the provider–patient relationship and considers how power can be renegotiated to facilitate appropriate care. As a newly emerging avenue of practice, particularly in Indigenous contexts, the concept of cultural safety is still in its early stages of development and more analysis is needed to understand how it can be applied in clinical practice.
Provision of equitable care requires a thorough understanding of patients’ needs and an acknowledgement of the vast differences between – and within – various racial and ethnic groups. Paediatric health care practitioners are currently employing their own, individually crafted strategies to foster positive provider–patient relations and facilitate favourable patient experiences (Grandpierre et al., 2019; Kim-Godwin and McMurry, 2012). While these individual-level efforts are commendable, there is a gap in research regarding their effectiveness, as well as in the acknowledgement of the structures in place within the healthcare system which, to date, have not been the most conducive to addressing the cultural needs of all parties involved with paediatric care.
Aim
This scoping review examines what academic literature reveals about the needs of racially and ethnically diverse paediatric patients, their families and health care providers in North American paediatric care. We seek to better understand previous and current efforts in providing paediatric care to racially and ethnically diverse patients, as well as to identify what care must look like to sufficiently satisfy the needs of families and health care providers. This study also explores what are commonly unacknowledged needs of patients, in order to inform a quality of care that does not waver on the basis of one’s race or ethnicity.
Methods
This scoping review was conducted utilizing Arksey and O’Malley’s framework, which considers scoping reviews as a useful approach for examining the extent, range and nature of research, as well as for identifying gaps in the existing literature (Arksey and O’Malley, 2005). Consequently, conducting this review, we sought to summarize the state of knowledge regarding the cultural needs of racially and ethnically diverse paediatric patients and their responding health care practitioners in North America. A scoping review methodology was selected in particular to map the available body of evidence by exploring what is known and what is missing from available literature. In alignment with Arksey and O’Malley’s (2005) framework, we followed the procedure below: Formulating the research question Identifying relevant literature Selecting literature based on inclusion and exclusion criteria Charting the data Collating, summarizing and reporting the results
In order to define and establish the parameters of this scoping review, we developed a broad research question which asked, ‘What does academic literature reveal about the needs of racially and ethnically diverse paediatric patients, their families and health care providers in North American paediatric care?’ As per the Arksey and O’Malley framework, our research question was framed more openly to allow for the retrieval of all relevant literature. The process of conducting scoping reviews is understood to be ‘not linear but iterative’, with writers often being compelled to engage with research reflexively (Arksey and O’Malley, 2005). In this sense, strict limitations were not placed on research terms and an upstream approach was taken in considering research demographics. When examining the provision of paediatric care, paediatric residents and faculty were included in addition to the paediatric health care professionals themselves. With regards to experience of paediatric care, examined literature included the views of parents, caregivers and patients on the care they have received within the healthcare setting.
Literature search strategy.

The articles retrieved from the search were imported into ProQuest RefWorks, an online reference manager, and screened for eligibility. A literature extraction tool was created in Microsoft Excel (v14.0). Recorded data from each article included authors, date of publication, publication information, region of research, demographics of research participants, research purpose, methods and key findings.
Scoping reviews do not seek to evaluate research; they strive to produce results which can be presented in an accessible format so that policy makers, practitioners and consumers can all make effective use of its findings (Arksey and O’Malley, 2005). Data were coded inductively whereby both authors read a selection of papers to generate key themes and discussed their findings to reach a consensus on the final coding scheme, which was then applied to the rest of the selected articles. Each article was inductively coded for the following themes: (1) perspectives of paediatric health care providers, (2) considerations of paediatric faculty and residents and (3) needs of paediatric patients and their families. The data were primarily summarized according to the demographics of research participants, research objectives and emerging topics. Ultimately, we retrospectively and concurrently explored the state of paediatric care in racially and ethnically diverse North America to identify the needs of paediatric patients and barriers for health care providers in present day, which are yet to be resolved.
Results and findings
Summary of literature search and selection
In total, 1519 articles were retrieved, of which 45% (n = 679) were duplicates and consequentially removed, leaving 840 papers for screening. The initial round of abstract screening identified 679 articles (81%) to be out of scope. The articles that were removed did not meet the inclusion criteria, mainly because they were either non-empirical studies or because they did not have sufficient analytical focus on the topic of interest, even if they mentioned it in some regard. After the initial screening, we identified 161 eligible articles (19%) that were left for the full-text screening. Among these articles, 82% (n = 132) were outside of the scope of interest on the basis of geographic location, participant demographics (i.e. samples were not racially or ethnically diverse), and the extent to which experiences within paediatric care were explored. The final pool of papers consisted of 29 articles, which were included in the scoping review. Figure 1 summarizes the literature search and selection process. PRISMA Flow Diagram.a The figure above provides a summary of the literature search and selection process that was undertaken for this scoping review.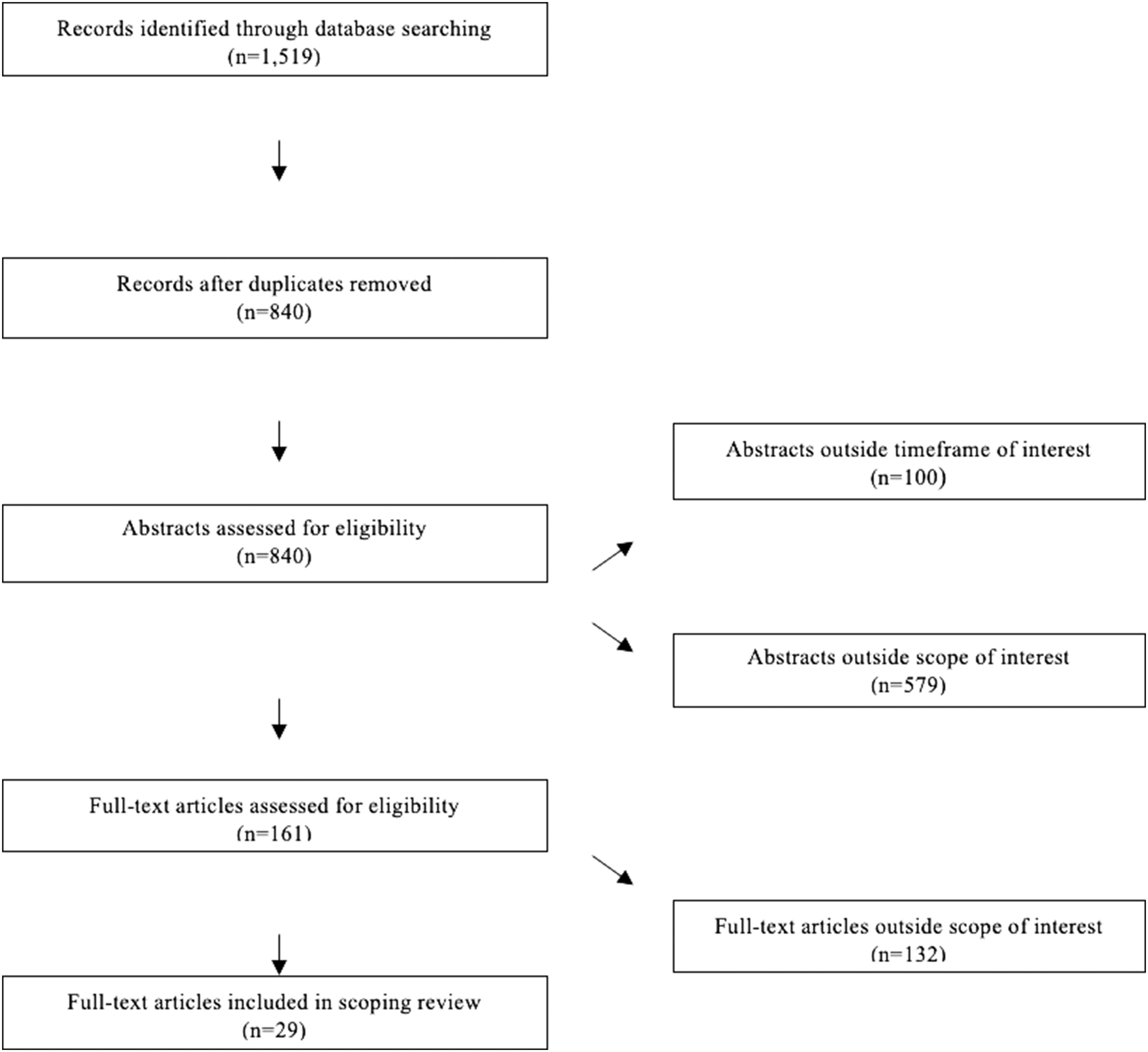
Characteristics of included literature
Summary of the reviewed papers. Organized by author, country, key sample characteristics, study format and key findings.
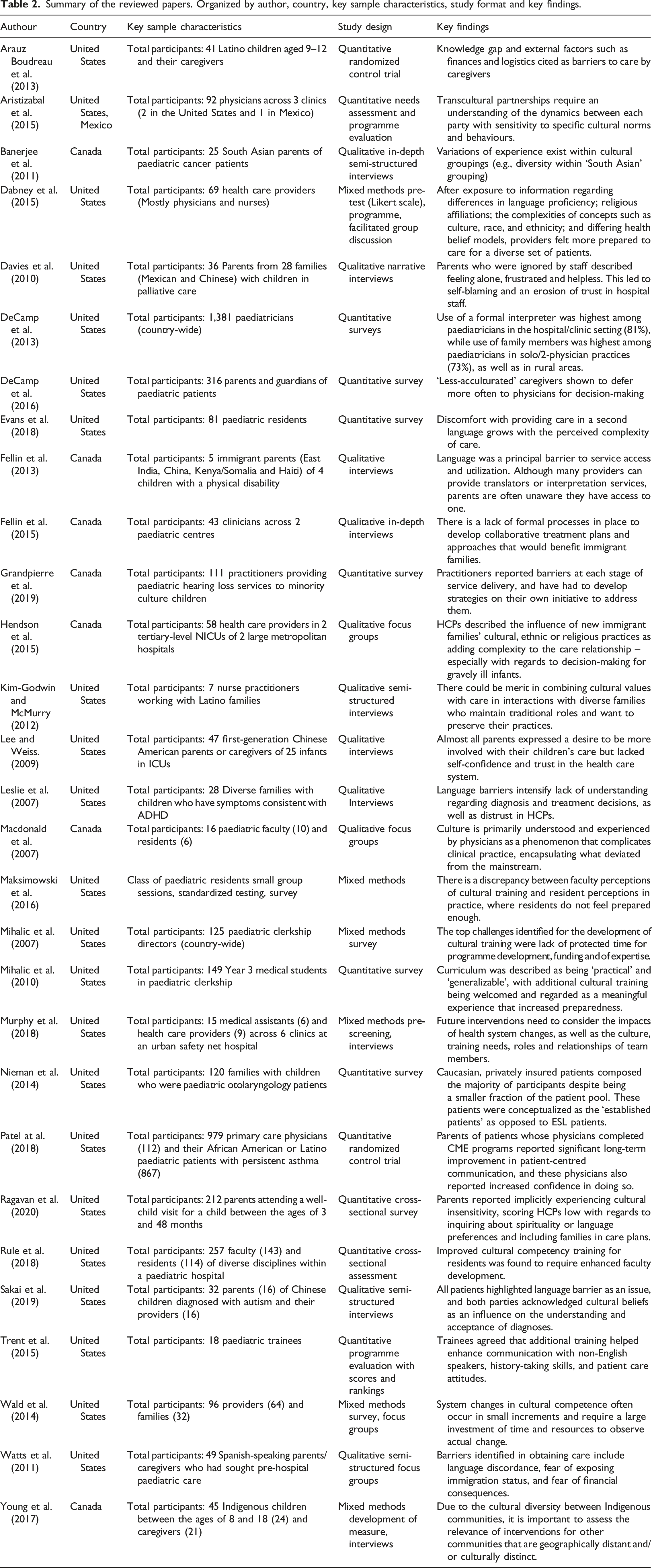
Almost half (n = 14) of the reviewed papers involved parents and caregivers as the primary research participants. Of these studies, only two (7%) also included paediatric patients as research participants. Paediatric health care practitioners were a population of interest in 11 studies (38%), while another 7 (24%) examined the experiences of paediatric residents and faculty. Paediatric health care providers whose needs were examined include primary care physicians, paediatricians, registered nurses, neonatal specialists, registered social workers, registered respiratory therapists and registered dieticians.
The articles reviewed were coded for three themes: perspectives of paediatric health care providers, considerations of paediatric faculty and residents, and needs of paediatric patients and their families. Within each theme, the sub-themes that emerged which were subsequently analyzed include (1) knowledge and awareness of health care providers and recipients on topics related to cultural competence, (2) alignment of cultural views and values between different parties participating in paediatric health care encounters, (3) lack of resources needed to support the provision of culturally appropriate care and (4) communication barriers related to the provision and receipt of culturally appropriate care (see Figure 2). Summary of the prevalence of sub-themes within each major thematic grouping.b The figure above illustrates the results of our scoping review with relation to the key themes and thematic categories identified. It highlights how many articles fell within each grouping, as well as which topics were most prominent within each examined group.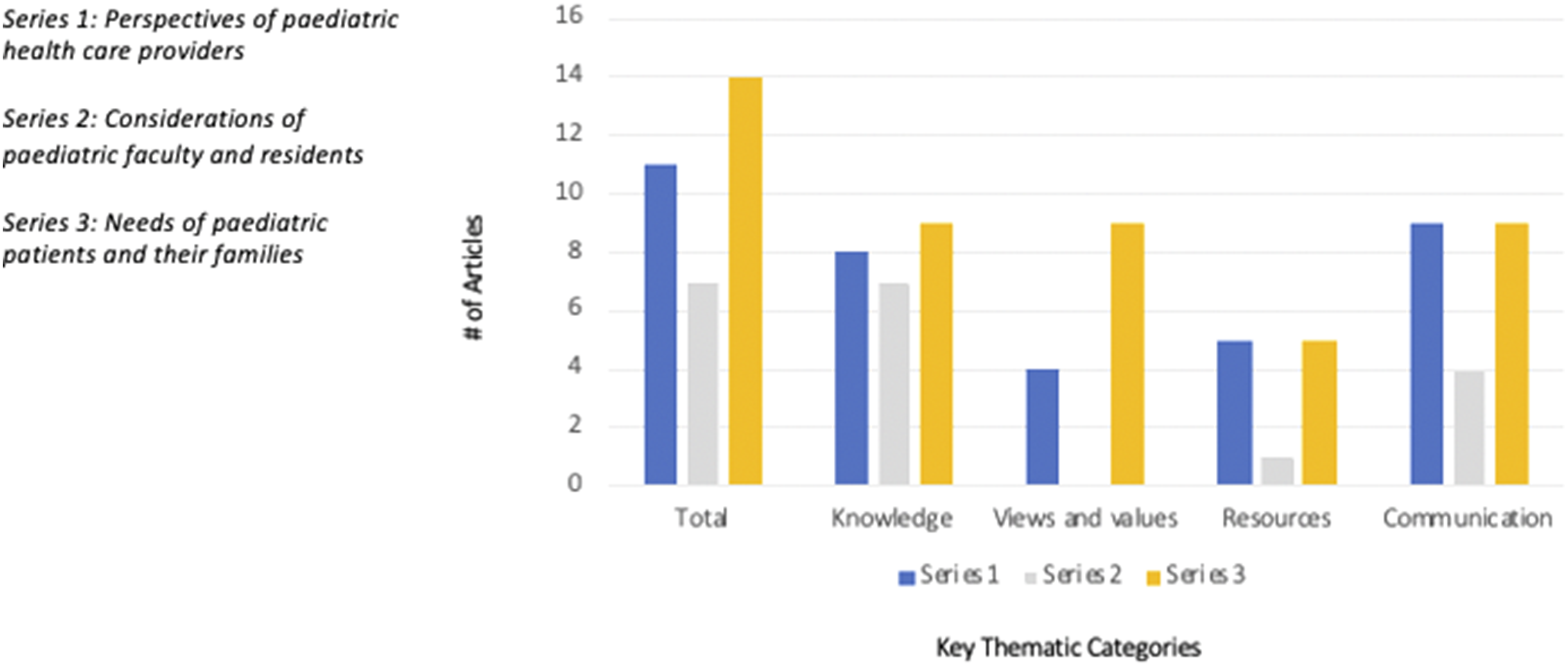
Theme 1: Perspectives of paediatric health care providers
In this thematic category, we coded 38% of the reviewed studies (n = 11), which focused on the barriers identified by paediatric health care providers in offering care that addresses the cultural needs of patients and their families. Health care practitioners saw their lack of training as a reason for feeling ill-equipped to address these needs (Maksimowski et al., 2016). Providers commonly attributed this to insufficient knowledge and training in areas such as decision-making processes for families, prevention of unintentional stereotyping, intuitive identification of families’ needs, and the presentation of medical information to audiences with limited English proficiency (Dabney et al., 2015; Fellin et al., 2013, 2015; Grandpierre et al., 2019; Hendson et al., 2015; Murphy et al., 2018).
Collaborative care was identified as a helpful coping mechanism when dealing with racialized families. However, it was simultaneously conceptualized as a band-aid solution (Fellin et al., 2013). For instance, a doctor may seek the help of a Muslim colleague in delivering care to a Muslim family, but this was perceived to lead to generalizations as opposed to facilitating individual relations with patients (Fellin et al., 2013). Discrepancies in the access and availability of resources were attributed to geographic location (Aristizabal et al., 2015; DeCamp et al., 2013), where resources in low-income and rural areas were more costly and sparser in availability (DeCamp et al., 2013). Cross-clinical collaboration was proposed as a means to mitigate the severity of these discrepancies (Aristizabal et al., 2015).
Communication barriers were found to result in an ‘intensified lack of understanding’ of diagnosis and treatment decisions (Leslie et al., 2007), which could directly predispose paediatric patients to negative health outcomes. However, communication was also framed as a solution. Strategies proposed in the literature to facilitate provider–patient communication included using simple language, providing interpreters, utilizing visual aids, and learning a few words or key phrases in the languages of the parents or caregivers (Grandpierre et al., 2019; Trent et al., 2015). Demonstrating the positive impact of responsive measures on patient outcomes has been deemed as difficult, so future research might focus on evaluating the long-term impact of cultural competency training on appropriate language services use, as this has not yet been evaluated (DeCamp et al., 2013).
Theme 2: Considerations of paediatric faculty and residents
Of the reviewed articles, 24% (n = 7) suggested that it is necessary to understand the existing needs of paediatric faculty and residents. These needs must be addressed prior to entrance into the workforce, as not taking action during training hinders quality care provision. A discrepancy between the perceptions of paediatric faculty and residents was noted in that faculty commonly perceived the training to be sufficient, yet those putting the training in practice with different patient populations perceived it to be inadequate (Maksimowski et al., 2016).
The views and values emphasized in the training of paediatric residents tend to be Eurocentric by default, primarily as a result of the historical formation of curricula. Training material has additionally been designed to be ‘practical’ and ‘generalizable’ (Mihalic et al., 2007), which may not always be entirely applicable in rapidly diversifying North American society. Modules on care provision which address cultural needs of patients have not been prioritized largely due to time constraints and lack of funding (Mihalic et al., 2007; Rule et al., 2018). Residents have notably wanted more mentorship by faculty as well on how to address the cultural needs of patients, but faculty have felt uncertain about their ability to do so (Macdonald et al., 2007). In this regard, paediatric faculty members acknowledged that comprehensive training to address these concerns should also include faculty development (Rule et al., 2018).
Theme 3: Needs of paediatric patients and their families
As most paediatric patients are young, their needs were commonly communicated by parents and caregivers. Overall, cultural views and values of patients and families that came into play when interacting with paediatric health care providers included initial distrust in providers, fear of the Western medical system, strong value in consulting social networks, interest in complementary and alternative medicine (CAM) and traditional remedies, stigma of disease or disability, as well as self-blame by parents for their child’s condition (Arauz Boudreau et al., 2013; Banerjee et al., 2011; Fellin et al., 2015; Lee and Weiss, 2009; Leslie et al., 2007; Ragavan et al., 2020).
Another major barrier regarding cultural needs was lack of communication due to language proficiency and lower levels of Western health literacy (DeCamp et al., 2016; Fellin et al., 2013, 2015; Leslie et al., 2007). Parents and caregivers often expressed confusion about the complexity of terminologies utilized by health care professionals, citing that they were unable to sufficiently grasp what it was their children were experiencing, or what their parental responsibility entailed (Davies et al., 2010; Fellin et al., 2015; Lee and Weiss, 2009; Leslie et al., 2007; Stanley, 2006; Watts et al., 2011). Parents and caregivers additionally detailed how a lack of resources inhibits their ability to follow recommendations of their health care providers. These challenges stemmed from financial difficulty, family dynamics, resident status, cultural community, reduced access to transportation and minimal access to safe spaces (Arauz Boudreau et al., 2013; Banerjee et al., 2011; Lee and Weiss, 2009; Sakai et al., 2019; Watts et al., 2011).
Ideally, paediatric care must help identify the needs of paediatric patients and their families as well as enable the provision of techniques and services to satisfy them. Equitable paediatric care may therefore promote an increased awareness and understanding of the circumstances of racialized families outside the appointment room. This would enable paediatric health care providers to be more adaptive in their recommendations to ensure appropriateness and feasibility for each patient’s family.
Discussion
This scoping review examined findings from empirical literature regarding the experiences of paediatric care provided to racially and ethnically diverse patients. In doing so, it explored the values, needs and barriers of various stakeholders: paediatric patients, their families, paediatric faculty and residents, as well as paediatric health care providers. Thematic analysis allowed us to clarify the needs of care stakeholders in four key areas: (1) knowledge, (2) views and values, (3) resources and (4) communication.
Our scoping review found that patient experiences of paediatric care are most often recounted by their parents. Parents serve as ‘important helpers’ or advocates who possess valuable knowledge about their children, which can ultimately influence the care that they receive (Aarthun et al., 2018). The dynamic that exists between these parties can impose unique tensions and challenges such as disagreement about diagnoses or the proposed courses of care on the basis of parental intuition or cultural beliefs (Banerjee et al., 2011; Hendson et al., 2015; Kim-Godwin and McMurry, 2012; Lee and Weiss, 2009; Leslie et al., 2007; Macdonald et al., 2007; Sakai et al., 2019). These sorts of challenges in healthcare are compounded when we factor in race and ethnicity (Cheng and Goodman, 2014; Kelly et al., 2012; Pachter and Coll, 2009; Riera and Walker, 2010; Seid et al., 2003; Wright et al., 2019). Therefore, we must shift from more paternalistic models of practice and conceptualize paediatric care as participatory. The identification of the needs of paediatric care administrators, as well as racially and ethnically diverse recipients, provide necessary insight into what sorts of considerations must be made to produce equitable standards and experiences of paediatric care.
It must be acknowledged that racially and ethnically diverse families can experience a multitude of barriers affecting their health status and outcomes, which extend far beyond the scope of healthcare, such as in education, housing and employment. In addition to systemic racism being a potential cause for health inequities experienced by racially and ethnically diverse groups, some of these barriers also stem from the lack of cultural training for health care providers (Brondolo et al., 2009; Maksimowski et al., 2016; Mihalic et al., 2007). Paediatric patients, their families, residents, faculty and health care providers considered in this scoping review collectively identified increased knowledge sharing and translation, the alignment of cultural views and values, access to resources, and clearer communication as necessary in the provision or acquisition of paediatric care. In lieu of identified constraints, such as time and financial means (Hendson et al., 2015), these may be key areas of focus to successfully address the cultural needs of paediatric patients and their families.
An upstream approach must be taken in addressing needs rooted in systemic barriers, such as the lack of prioritization of cultural competency modules in training (Brondolo et al., 2009), the scarcity of resources available to paediatric clinics in rural or low-income areas (DeCamp et al., 2013), and the reduced financial or logistical means for families to engage in healthy behaviours (Arauz Boudreau et al., 2013; Banerjee et al., 2011; Lee and Weiss, 2009; Sakai et al., 2019; Watts et al., 2011). Additionally, increased health literacy levels among families by way of sustained exposure to health information through community-based channels can enable a stronger understanding of the healthcare system and models of care practiced within North American contexts.
Our scoping review found that the marginalization of racially and ethnically diverse groups is often overlooked under the predominantly Eurocentric lens which is applied to paediatric training and practice (Mihalic et al., 2007; Rule et al., 2018). The observed need for increased knowledge sharing and translation was ultimately related to the training that health care providers apply in their interactions with patients (Brondolo et al., 2009; Maksimowski et al., 2016; Mihalic et al., 2007; Rule et al., 2018) and the beliefs that patients and their families bring to their interactions with providers (Davies et al., 2010; DeCamp et al., 2016; Fellin et al., 2013, 2015; Lee and Weiss, 2009; Leslie et al., 2007; Stanley, 2006; Watts et al., 2011).
Although minor effects of cultural competency efforts are beginning to be observed, further research is needed to determine their lasting impacts on clinical practice and patient experiences in paediatric care. Moreover, cultural competency efforts, the common means of addressing the cultural needs of patients (Stanley, 2006), are predominantly focused on the health care practitioner. The findings of our scoping review emphasize power imbalances between patients and providers, as feelings of powerlessness were only self-identified by recipients of care and not observed by those responsible for the administration of paediatric care (Banerjee et al., 2011; Fellin et al., 2013; Watts et al., 2011). This scoping review ultimately calls for more equitable and patient-centric approaches, such as through the application of a cultural safety lens. Training and interventions rooted in cultural safety are of utmost importance, as this lens helps facilitate self-awareness and self-reflection on the part of the health care practitioner (Anishnawbe Health Toronto, 2011; National Aboriginal Health Organization, 2009), and conceptualizes ‘safety’ as being determined by those who are experiencing healthcare as opposed to those who provide it.
This review has several limitations. While our scoping review was conducted to better understand how paediatric care is experienced in rapidly diversifying populations across North America, some of the studies that were analyzed already cited lack of representation of racialized communities in their clientele as a barrier for evaluating the efficacy of initiatives intended to serve them (Arauz Boudreau et al., 2013; DeCamp et al., 2013, 2016; Lee and Weiss, 2009; Nieman et al., 2014; Ragavan et al., 2020). Future studies may benefit from inter-clinic collaboration within geographical regions to increase recruitment whilst controlling for other important factors, such as socioeconomic status, which can play a role in health care experiences and outcomes (Lee and Weiss, 2009). Lastly, only two studies we reviewed incorporated the experiences of children, with all others which examined the receipt of paediatric care focussing on parents and caregivers. This is understandable, given the intensity of ethics protocol and the fact that some children may have neither clear understanding of their health circumstances nor sufficient levels of health literacy. However, research studies tailored to amplifying the voices of children may be beneficial since it is the children who directly receive the care and who can thus share more authentic accounts of the patient experience.
Notwithstanding these limitations, this review identified several implications for practice, as detailed above. Evidently, there is a necessity for more training and education centering on the provision of culturally safe care. This training must start early, during residency, and be developed in consultation with those who provide services to racially and ethnically diverse patients, as well as these patients themselves and their communities. Improved funding and access to resources are imperative to address the needs of these stakeholders, as well as to help facilitate the shift from Eurocentric, paternalistic models of care to more culturally safe and collaborative care.
Conclusion
Acknowledged as determinants of health and predictors of quality of care and health outcomes, race and ethnicity are variables which affect experiences of paediatric care for families in North America (Cheng and Goodman, 2014; George and Bassani, 2018; Pachter and Coll, 2009; Priest et al., 2018; Seid et al., 2003; Wright et al., 2019). This scoping review contributes to the existing literature on cultural needs in paediatric care whilst examining how the multi-faceted experiences of paediatric educators, residents, health care providers, patients and their families intersect to ascertain the quality and sustainability of clinical practice. Further, it reveals the systemic barriers in place which affect the ability of paediatric care providers to address the cultural needs of their patients and draws attention to the needs of racially and ethnically diverse families obtaining paediatric care.
This scoping review highlights the potential for cultural safety to pave the way for clinical practice within North American paediatric care contexts, focusing more on patient comfort and empowerment to ultimately foster provider–patient collaboration. Paediatric care extends beyond the four walls of the examination room whereby the impacts of the care received by families are felt beyond just the point of access. Paediatric health care providers have an enormous influence on the health outcomes and consequential trajectory of a child’s life, and it is through culturally safe and collaborative care that each child, no matter their race or ethnicity, will be able to obtain the paediatric care they rightfully deserve.
Footnotes
Author contributions
RL initially developed various combinations of keywords to be utilized for the search. In efforts to ensure sufficient coverage and an adequate scope of articles were being obtained, RL and EN collaborated to alter the search phrase. Microsoft Excel was used to develop the coding tool with which data was extracted. RL and EN both employed inductive reasoning to independently code five articles. Following, themes were compared to generate the coding scheme with which all other articles were analyzed. RL produced the manuscript, and made revisions as specified by EN. The manuscript was approved by both RL and EN.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.