
Abstract
Immigrant mothers who have immigrated during the last ten years and do not speak the language of the new country are found to be at particular risk of being affected by postpartum depression (PPD). Still they choose to participate to a lesser extent in screening for PPD and are not screened out as frequently as can be expected. In this study, non-native-speaking immigrant mothers’ experiences of participating in screening for PPD in the Swedish Child Health Services were elucidated. Thirteen qualitative interviews were performed with the help of an interpreter and analysed using latent content analysis. The possibility to participate in screening was appreciated by the mothers even though the concept of PPD in general was unclear. Cultural beliefs about mental ill health, negative expectations connected to their perceived value as a woman, shame at not being grateful enough for their new life and negative experience of the interaction during the screening challenged them in speaking about their mood. To facilitate the screening procedure for this vulnerable group of mothers, it is important to be aware of possible challenges when speaking about their mood and to strive for a trusting clinical interview with the assistance of a female interpreter on-site.
Keywords
Introduction
Maternal postpartum depression (PPD) is a global public health problem in which immigrant mothers are found to be at particular risk of being affected by. The prevalence of PPD in immigrant women is estimated to be as high as 20%, which is almost twice as high as in nonimmigrant women living in Western societies (Falah-Hassani et al., 2015). Vulnerable groups of immigrant mothers such as asylum seekers and refugees, especially those who recently migrated, may be at even higher risk of being affected (Dennis et al., 2017). The same applies to those who do not speak the language of the new country of residence (Bandyopadhyay et al., 2010). Important risk factors especially associated with PPD in immigrant mothers are lack of social support, poorer marital adjustment, and a perceived insufficient household income (Falah-Hassani et al., 2015). Other known risk factors are worrying about family members left behind, food insecurity, and reduced access to health care. Experiences of abuse before or during the pregnancy and physical complications post-birth also increase the risk of being affected (Dennis et al., 2017).
Given the well-documented negative consequences of PPD not only for the mother’s health, but also for her partner’s and primarily the infant’s health and development, early identification and treatment of PPD is essential (Goodman et al., 2011). In Sweden, a country in Northern Europe with of high rate of asylum applicants, the nurses in the Child Health Services (CHS), from the authorities’ perspective, bear the main responsibility for identifying mothers with signs of PPD. According to guidelines, all mothers should be invited to participate in screening for PPD six–eight weeks after giving birth (Swedish National Board of Health and Welfare, 2010). The screening is performed using the Edinburgh Postnatal Depression Scale (EPDS) method, which includes a self-report questionnaire with 10 items especially developed for screening for symptoms of PPD in connection with a clinical interview (Cox et al., 1987). When screening a non-Swedish-speaking immigrant woman, the CHS nurse is instructed to use a translated, validated scale, and be aware that the cut-off point may vary between different languages (Wickberg, 2016). Other circumstances, to take into consideration that may influence the screening, are the mother’s literacy level and the quality of the interpreter’s work, and also how different cultural interpretations of the questions can result in scores that do not reflect the mother’s mood (Department of Health Government of Western Australia, 2006).
Despite the fact that all mothers should be invited to participate in screening for PPD (Swedish National Board of Health and Welfare, 2010), research shows that immigrant mothers are not invited to participate to the same extent as native-born mothers (Massoudi et al., 2007). Health-care professionals experience screening of immigrant mothers as a challenging task (Teng et al, 2007). It is considered demanding to adapt the EPDS method when having to use an interpreter and a translated validated scale without deviating too much from the method’s original approach (Skoog et al., 2017). Interpreting culture-specific signs and symptoms of PPD is another challenge for the professionals (Onozawa et al., 2003). Statistics also reveal that immigrant mothers chose to participate in screening for PPD to a lesser extent than the domestic population and they are not screened out as frequently as can be expected in relation to the high prevalence (Centre of Excellence Child Health Services, 2017). The aim of the study was to elucidate non-native-speaking immigrant mothers’ experiences of participating in screening for PPD in the Swedish CHS.
Methods
Design
Since earlier knowledge of the phenomenon is fragmented, a qualitative interview study with an inductive approach was chosen as the study design (Elo and Kyngäs, 2008). Latent content analysis was used to describe variations of the participants’ experiences (Patton, 2002) in order to provide a rich understanding of the phenomenon. By performing a latent content analysis, the intention was that the underlying meaning of the text could be interpreted (Downe-Wamboldt, 1992).
Setting and participants
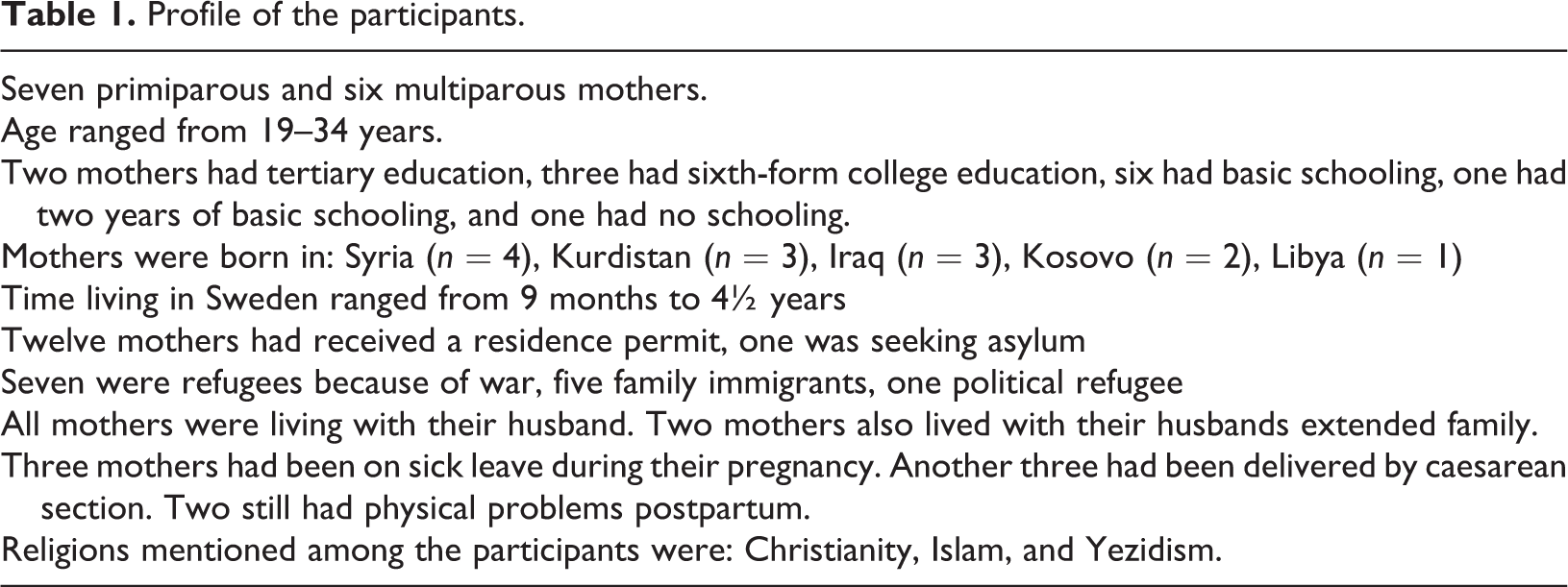
This study was conducted in the CHS in a county in the south of Sweden where 40% of the children (zero to six years old) were either born abroad or have one or both parents born abroad (Statistics Sweden, 2016). Immigrant mothers speaking the four languages most commonly using an interpreter, Albanian, Arabic, Badinani, or Turkish, without showing any signs of PPD according to the CHS nurses’ (henceforth described as nurses) clinical assessment after screening for PPD, were eligible to participate in the study. Mothers who were assessed to show signs of PPD were excluded. Twenty-five nurses in seven different Child Healthcare Centres (CHCs), among the 15 centres that performed most screening for PPD with the help of an interpreter, acted as intermediaries and informed suitable mothers about the study in connection with their infant’s three-month check-up. Translated information in each mother’s first language was used in addition to verbal information with the help of interpreters. When a mother expressed interest in participating in the study, the first author was notified and contacted the mother with help of an interpreter to give further information and to offer participation and arrange the interview. Four authorized female health-care interpreters were used in the interviews. Before the research interviews started, the mother was given individual information about qualitative research interviews and the nature of the study. Eighteen mothers expressed interest in the study, but three of them declined participation after being given further information. One mother withdrew her participation after she had been interviewed. One mother was previously acquainted with the first author and was excluded. In total, thirteen non-Swedish-speaking immigrant mothers were interviewed approximately one to two months after being screened for PPD. Profiles of the participants are presented in Table 1.
Profile of the participants.
Ethical considerations
The study was carried out in accordance with the WMA Declaration of Helsinki (World Medical Association, 2013). The participants received customized information about the nature of the study, freedom of participating, and measures to preserve their confidentiality in their own language and with the use of an authorized female health-care interpreter. They all gave their written informed consent. Ethical approval for the study was obtained from the Regional Ethics Committee in Lund, Sweden (case no. 2015/96).
Data collection
The interviews were performed in person by the first author, with the help of authorized female health-care interpreters, from November 2015 until November 2016. They lasted an average of 54 minutes (range 37–94 minutes) and were performed at a location chosen by the participant, which meant at her local CHC or in her home. A semi-structured interview guide covering four question areas was used (Table 2). To deepen the understanding of the participants, probing questions were asked to elaborate on their thoughts in more detail. Two pilot interviews were conducted to test the semi-structured interview guide. These did not result in any changes to the interview guide and were therefore also included in the research material. After the eleventh interview, no new data were found to emerge, but for confirmation, another two interviews were performed to make sure the data were saturated. The interviews were transcribed verbatim by the first author. Authorized interpreters other than the ones used in the interviews verified seven of the interviews by listening to the recording and comparing it to the transcription.
Question areas in the semi-structured interview guide.

Data analysis
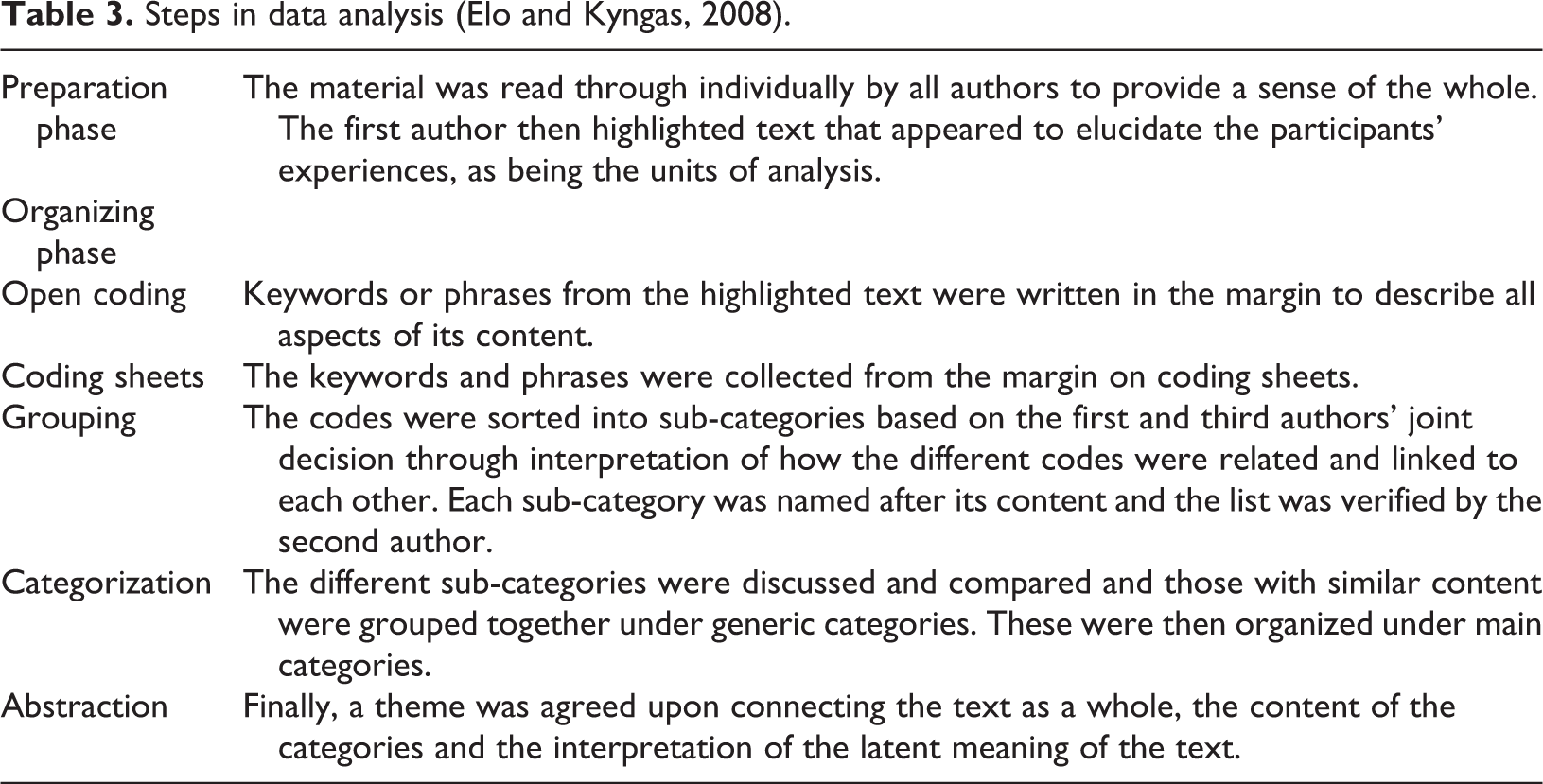
The data analysis was performed in six steps according to Elo and Kyngas (Table 3) (Elo and Kyngas, 2008).
Steps in data analysis (Elo and Kyngas, 2008).
Ethical approval
Ethical approval for the study was obtained from the Regional Ethics Committee in Lund Sweden (case no. 2015/96).
Results
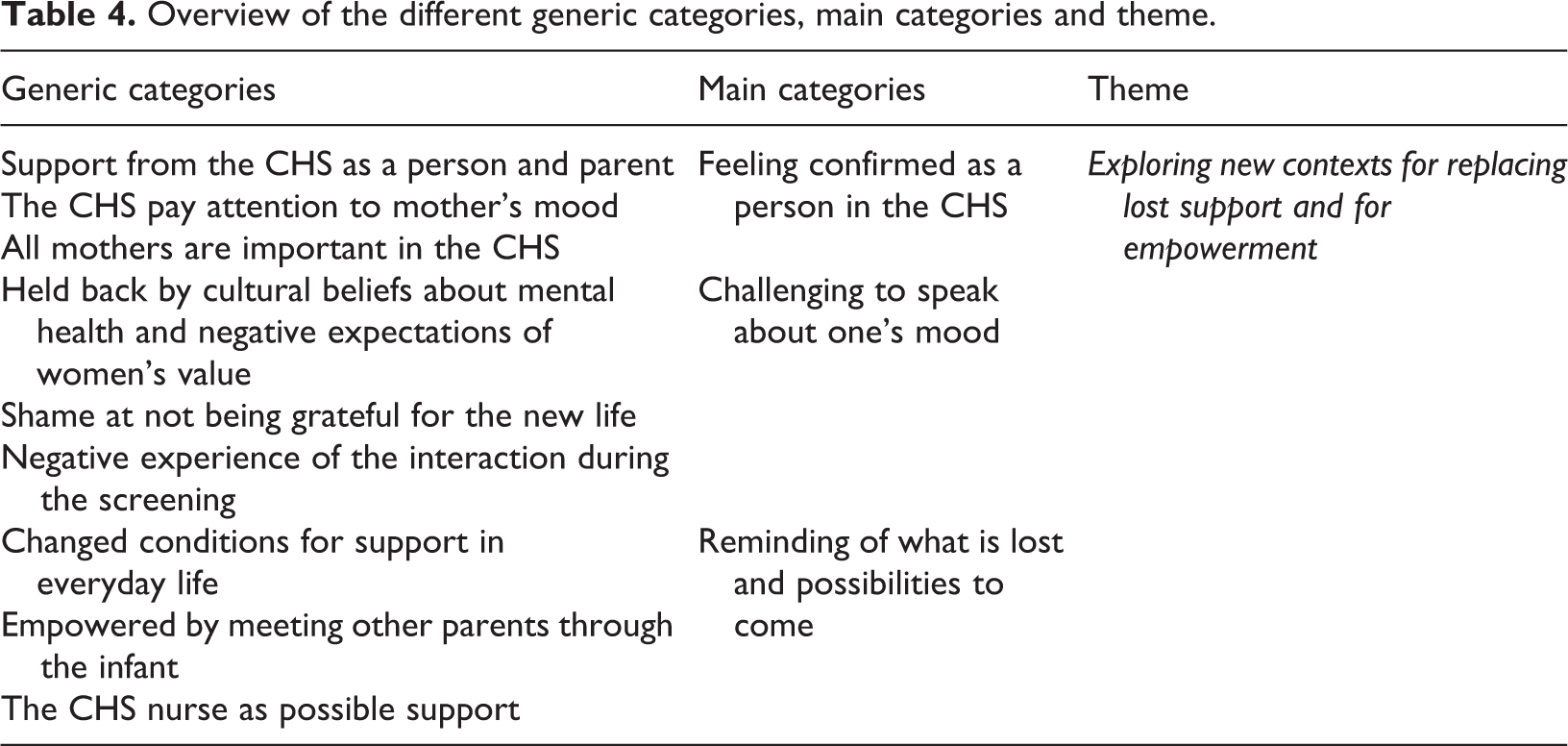
An overarching theme Exploring new contexts for replacing lost support and for empowerment illustrated the non-native-speaking immigrant mothers’ experiences of participating in screening for PPD in the Swedish CHS. The theme refers to how participating in the screening reminded the non-Swedish-speaking immigrant mothers (henceforth described as mothers) of their lack of support in their current life situation but were also seen as an opportunity to tentatively experience new ways of thinking about mental ill health and exploring new sources for support. Three main categories were identified and described as Feeling confirmed as a person in the CHS, Challenging to speak about one’s mood, and Reminding of what is lost and possibilities to come. The different generic and main categories are described in Table 4.
Overview of the different generic categories, main categories and theme.
Feeling confirmed as a person in the CHS
The mothers described how the visits to the CHS made them feel supported both as a person and as a parent. They felt confirmed as a person when being asked to participate in the screening for PPD just as all other mothers were.
The mothers appreciated coming to the CHC for the infant’s regular check-ups. They felt secure and grew in their role as a parent when the nurse answered their questions. The mothers experienced that the nurse did not just care for their infant but were also interested in them and their feelings. This was surprising for them as they had the impression that the CHS was mainly directed to the child’s health.
The reason for offering the screening was somewhat unclear to most mothers, but nevertheless mostly a positive experience. The relationship and the quality of the contact with the nurse were of importance for them when they decided to participate in the screening and if they found it meaningful. Oh, I was actually very happy that someone cared. It’s the first time that someone outside, a stranger, has asked me these questions. It was actually great and special. I’ve never experienced in a new country that a stranger with another language, there are many differences, but despite that when I was asked those questions, I was actually very happy. (No. 2) It felt like it was nothing wrong. Like it was completely normal. (No. 12)'
Challenging to speak about one’s mood
The mothers were challenged in speaking about their mood by cultural beliefs about mental ill health and negative expectations connected to their perceived value as a woman. Shame at not being grateful enough for their new life and the experience of the interaction during the screening also challenged them.
The concept of PPD was in general unknown to the mothers. Some had knowledge from their country of origin through information on the Internet, but none of them had experienced general discussions about PPD in their society, as speaking about mental ill health was not common and not accepted in their country of origin. Well, I can say that in a country that’s more developed it often works better than in our home countries. If you wanted to say that you’re not feeling mentally well it’s nothing that you can talk openly about then they’ll think you’re crazy. You can’t say that, but here in Sweden you can say that you’re not feeling well or it’s too much then there is the possibility that you can speak about it or calm down in some way to feel better again. (No. 6)
Their ability to speak about their mood was also negatively influenced by earlier negative encounters in health care and stories about the way women had been treated by health-care professionals in their country of origin. Well, I can say that it’s really hard down there. I’m telling you that you shouldn’t scream. They can become insane if you scream or are tense. You shouldn’t do that, then they get really angry. I have not given birth to children there, but my sister and my brother’s wife have had their deliveries there and they tell you that in [names a location] they can even beat the woman if she screams. (No. 13)
Another hindrance for bringing up negative emotions was feelings of guilt and shame and not being grateful enough for the comfortable life they now were living in Sweden.
Despite experiencing a good relationship with the nurse, some mothers were sensitive to the nurse’s availability, and if they perceived her as stressed or in other ways absent in the screening situation, they did not want to burden her further. Not all mothers had been given the opportunity to speak about their answers to the questionnaire but merely to fill out the EPDS by themselves or with the help of an interpreter. It felt like I wanted to open my heart and just talk but there wasn’t the opportunity. You just had the questions on paper and answered the question itself. (No. 1)
Reminding of what is lost and possibilities to come
When participating in the screening, the mothers were reminded of their changed conditions for support in everyday life and how they tried to orient themselves to find new ways of support. Two of the mothers had experienced PPD in connection with earlier pregnancies. Four of them spoke of having sleeping disorders; feeling sadness and crying for no reason; loss of interest in their daily life; suffering from fatigue, anxiety, anger, or irritability; self-loathing; and unexplained aches and pain in their legs and back. One of them also told about having delusions and thoughts of harming herself. Sometimes you get bored with life. Sometimes I can say that I wish I never even came into the world or oh I hope I just die. Such a feeling. But I’m afraid of dying. But I just say so because…I’m just saying so. Sometimes when I get very upset, I feel it in reality. (No. 7) Well, it’s like this if I don’t talk to my Mum every day, I just can't…I need to speak to her every day. (No. 10)
The infant was described as important company in daily life. The infant gave meaning in their life and a reason to start learning the language and to make new acquaintances. Some visited the open preschool at the local family centre and started to build a network for support and company. Others found support among their neighbors. The mothers also expressed that they found strength in their own ability to care for their infant.
In their current life situation, the mothers tried to orient themselves toward accepting other forms of available psychological support if needed. The relationship with the nurse was experienced as valuable and the home visit was highly appreciated. All mothers emphasized the value of regular support during the first weeks after giving birth, preferably in their home, to promote mental health. Therefore, I think that these new immigrants who have given birth here and then become depressed, by getting this help you can relieve these mothers with knowledge and tell them about different things so that they can understand what’s happening. And then you can come and see the mother in her home and see how the baby is doing. (No. 11)
Discussion
This study elucidated non-native-speaking immigrant mothers’ experience of participating in screening for PPD in the Swedish Child Health Services. The concepts of PPD and the purpose of the screening were in general unclear for the mothers but still they appreciated being asked to participate, since it was important for them to be treated just like everybody else. It appeared when deciding to participate in screening that the relationship and the quality of the contact with the nurse were of importance. Previous research found trust, rapport, and faith to be essential components for immigrant mothers to have a positive perception of a relationship with a health-care provider; likewise, that the mother felt the health-care provider’s genuine commitment and interested in her and awareness of her background (Donnelly et al., 2011). Awareness of the importance of establishing a supportive relationship for being able to interpret mothers’ mood was brought forward by CHS nurses in previous research (Skoog et al., 2017). The result of the present study draws attention to how information about PPD and the screening is given. Earlier research has shown that immigrant mothers were less likely to recall being asked about depressive symptoms and relationship problems by General Practitioner (GPs) and CHS nurses compared to domestic mothers (Lansakara et al., 2010. This may be related to the fact that mental illness is connected to social stigma in some cultures, which prevents mothers from seeking help (Collins et al., 2011). It might also be the reason why one of the participants in this study withdrew her interview. Knowledge of social stigma might also affect the nurses when presenting the screening and make her hesitate for fear of jeopardizing the relationship with the mother. As a first step to overcome difficulties in working effectively with immigrant mothers, health-care professionals must recognize and understand their own barriers and challenges (Donnelly et al., 2011). Research focusing on CHS nurses’ concerns during health check-ups suggested the need for training and guidance to improve their competence in discussing sensitive topics (Poutiainen et al., 2015). In the theory of human caring, it is emphasized how the nurse must be aware of herself to be able to use herself in the transpersonal caring relationship (Willis and Leone-Sheehan, 2018).
Social stigma about mental ill health was also found to challenge the mothers in speaking about their mood, as were negative expectations connected to their perceived value as a woman and shame of not being grateful enough for their new life. These challenges have previously been found to be barriers for immigrant mothers accessing mental health-care services (Donnelly et al., 2011). Another challenge was negative experience of the interaction during the screening. One criterion for being eligible to participate in the present study was to be screened without showing any signs of PPD according to the nurses’ assessment. Still almost one-third of the participants expressed symptoms of PPD in connection with the research interview. It appeared that some of the mothers had not been given the opportunity to speak about their answers in the EPDS. The questions in the EPDS were perceived as normal by the mothers, but the use of Likert-type scales is known to be problematic for migrants with poor educational attainment (Flaskerud, 2012). Health-care providers also need to be aware of how differently symptoms of PPD can be expressed in the EPDS. Recently, published research found that the level of education and the continent where they live influenced the expression of PPD in the EPDS much more than ethnicity and race. Women with lower levels of education were less likely to report crying and thoughts of self-harm and more likely to report anhedonia. This highlights the need to be careful and not stereotype mothers on the basis of their ethnic/racial background but rather explore the mothers’ cultural milieu (including education) beyond ethnicity and race (Di Florio et al., 2017). Furthermore, it emerged that some of the participants in the present study experienced physical symptoms such as back pain and aches during pregnancy and postpartum. Immigrant mothers are shown to report a significantly higher proportion of some physical symptoms such as severe headaches during the first three months postpartum. Such physical symptoms may be an expression of distress and can be missed when using single-time psychological screening instruments to identify mothers at risk of depression (Lansakara et al., 2009). Altogether this illuminates the complexity in using the EPDS with this group of mothers and emphasizes the importance of creating a trusting dialogue within the clinical interview for capturing signs of PPD. A great challenge in accomplishing this is the lack of a common language and having to rely on an interpreter. The participants in the study were in general content with the interpreter who assisted them during the screening, but if they had the possibility to choose, they would prefer a female interpreter on-site. This confirms earlier research findings within the same context (Barnes et al., 2011). Providing the assistance of a female interpreter on-site is an important step for creating better circumstances for the mother during the screening. Training in how to use interpreters might help the CHS nurses to be more confident in the screening procedure and likewise the interpreters would benefit from information beforehand about the screening procedure.
Most of the mothers in the present study were lacking conceptions of PPD and the purpose of the screening. By participating in the screening, the mothers felt reassured that the nurse would identify signs of PPD in case they did not recognize suffering from it by themselves. This raises the question of health literacy and the importance of providing educational services to immigrant mothers since they are at high risk of contracting PPD. In earlier research, immigrant mothers articulated the need for written resources in their own languages and making them available on the Internet and in public places (Riggs et al., 2012). Likewise, it has been shown that when immigrant mothers were made aware of services and had more knowledge about PPD, their access to help was facilitated (O’Mahony et al., 2012). We recommend that information about PPD is offered several times throughout pregnancy and the postpartum period, so that all mothers have the opportunity to gain information about PPD, recognize symptoms of depression, and learn about available support. In clinical guidelines for the United Kingdom, an early introduction of a general discussion about the mother’s mental health is suggested. A two-question screening tool for depression, relating to feelings of hopelessness or feeling down and lack of interest or pleasure, is recommended to be used already during the early postnatal period as a complement to a more comprehensive assessment using the EPDS (National Institute for Clinical Excellence, 2017). The U.S. Agency for Healthcare Research and Quality extends its recommendations even further and suggests serial testing with the use of the two-question screening tool (Myers et al., 2013). In the light of these recommendations, we believe further research on the impact of serial screening with the two-question screening tool in combination with a single-time screening with the EPDS would be interesting. Especially in terms of evaluating whether the mothers’ knowledge and awareness of mental health as well as ability to speak about their mood is improved compared to participating in a single-time screening with the EPDS.
Methodological considerations
The study was carried out in Sweden where the structure of the health-care system might differ from other countries, but the mothers’ experiences may be transferable as the EPDS screening for PPD is commonly used worldwide. Transferability of the results is also facilitated by describing the context and participants in as much detail as possible. To increase the dependability of the data, seven of thirteen research interviews were verified by a certified interpreter other than the one used in the interview. Likewise, where the data analysis described in detail in text and quotations used to make the interpretation transparent for the reader (Kvale and Brinkmann, 2009).
All authors had experience of working in different health-care contexts but only the first author was from the specific context. Having a pre-understanding of the context might be an advantage but could also constitute a bias if it influences the study in a subjective way. In an attempt to avoid letting pre-understanding influence the study and to strengthen the study’s confirmability, all three authors collaborated closely during the analysis. To increase the trustworthiness of the results, the analysis was partly conducted in parallel using researcher triangulation, which enhances a study’s credibility since it enables a consistency check of the results and reduces potential bias that might come from a single researcher analyzing the material (Polit and Beck, 2011).
Since the participants only represent a small group of mothers with three different languages, originating from five different countries, it can be argued that a larger sample would have strengthened the credibility of the results as additional variations could have been revealed. Still, despite the relatively small sample of participants, one cannot be certain that a larger sample would have revealed much additional variation since it is claimed that data saturation might occur already at 12 interviews provided that the participants are a relatively homogeneous group, the objective is fairly narrow and an interview guide is used (Guest et al., 2006). However, choosing the sample of participants differently might contribute to more variation in the results, but for ethical reasons, mothers assessed as showing signs of PPD were excluded.
Conclusions and clinical implications
Most PPD research focuses on mainstream populations. The perspectives of immigrant mothers, specifically those who are non-native speaking, receive little attention. Interviewing these vulnerable mothers was important and gave valuable information for future clinical practice. Based on our findings, we recommend the following: (i) strive to establish a trusting relationship with the mother and emphasize that supporting parental mental health is an important part of the work the CHS; (ii) offer customized information about PPD several times verbally with help of interpreter and in writing using translated information; (iii) provide a female interpreter on-site during the screening, who previously assisted the mother; and (iiii) strive for attentiveness to the mothers’ challenges for speaking about her mood like cultural beliefs about mental ill health, negative expectations connected to her perceived value as a woman, shame of not being grateful enough for her new life and negative experience of the interaction during the screening. These recommendations may contribute to decreasing the powerful stigma attached to this condition and subsequently also to promote mental health in these mothers and indirectly also their babies.
Footnotes
Acknowledgements
We thank the interviewed non-Swedish-speaking immigrant mothers for their invaluable contributions to the study. We also thank the participating interpreters for their expertise when performing the interviews.
Author contributions
MS designed the study, collected and analysed the data, and drafted the manuscript. VB designed the study, analysed the data, and drafted the manuscript. IH designed the study, analysed the data, and drafted the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors received financial support from the National Society for Paediatric Nurses, Region Skåne, Challenges of Migration and the Swedish Research Council for Health, Working Life and Welfare (FORTE).