
Abstract
Aims and Objectives:
Cognitive abilities between monolingual and bilingual individuals may differ, making it an important factor to consider during the administration of cognitive screening tools. Otherwise, assessments could be subject to misinterpretation, leading to possible inaccurate diagnoses. The current project aimed to compare cognitive performance of healthy older monolingual and bilingual anglophones on the English version of a new cognitive screening test designed for better recognition of atypical dementia: the Dépistage Cognitif de Québec (DCQ; www.dcqtest.org).
Design:
The DCQ was administered by qualified psychometricians to 85 native English-speaking participants aged 50 years and over, in various sites across Canada. Language proficiency was established using the Language Experience and Proficiency Questionnaire (LEAP-Q). The Montreal Cognitive Assessment (MoCA) was used to exclude individuals with cognitive impairments.
Data and Analysis:
Amid the anglophone participants recruited, 30 monolingual anglophones and 29 bilingual anglophones (English and French) met inclusion criteria. Groups had similar age, education, and MoCA scores. Monolinguals and bilinguals were compared on their total DCQ scores and each of the five DCQ indexes: Memory, Visuospatial, Executive, Language, and Behavioural.
Findings:
The bilingual participants performed better on the Language Index, which contributed to the significant bilingual advantage for the overall DCQ scores. When applying a Bonferroni correction, the differences between groups were, however, not maintained. No differences were found on any of the other indexes.
Originality:
This study is the first to explore psychometric properties of the DCQ in older monolingual and bilingual participants tested in their native language.
Implications:
Results highlight the importance of identifying and characterizing linguistic diversity before using new screening tools in clinical settings. The potential cognitive advantages of bilingualism should be considered when interpreting test data and explicitly discussed in neuropsychological reports.
Introduction
With an increasingly aging population, the World Health Organization (2019) has estimated that worldwide, 50 million people currently live with a major neurocognitive disorder, which is more commonly known as ‘dementia’. These include typical dementias (e.g., Alzheimer’s disease in its amnesic variant, or vascular cognitive disorder), as well as the atypical variants (e.g., language, visual or frontal/dysexecutive variants of Alzheimer’s disease, primary progressive aphasia, Lewy body disorders and the spectrum of frontotemporal dementia). As the number of new cases is expected to increase by nearly 10 million every year, it is estimated that by the year 2030, the number of individuals living with dementia will reach 82 million (World Health Organization, 2019). One of the great challenges facing our society today is thus preserving healthy brain function in our aging population. To this end, the timely detection of cognitive issues which may lead to a dementia diagnosis is crucial so that modifiable dementia risk factors, such as cardiovascular risk factors, can be modified and patients may be given strategies that promote healthy aging.
Early diagnosis and therapeutic interventions begin with an accurate clinical assessment. However, early identification of atypical syndromes remains challenging. Factors contributing to the delay between care seeking and accurate diagnosis include the lack of screening instruments specifically tailored towards early identification of atypical dementias (Cheng & Lam, 2018). Even among the most commonly used cognitive screening tools such as the Mini-Mental State Examination (MMSE; Folstein et al., 1975) and the Montreal Cognitive Assessment (MoCA; Nasreddine et al., 2005), behavioural measures are not taken into account, and none have been updated for recent diagnostic criteria (Sellami et al., 2018). Due to these limitations, the Dépistage Cognitif de Québec (DCQ; www.dcqtest.org) was recently developed in French by Laforce et al. (2018) at the Clinique Interdisciplinaire de Mémoire (CIME) of the Centre Hospitalier Universitaire de Québec and has been designed precisely for atypical dementias. It tests patients on five cognitive domains: memory, visuospatial abilities, executive functions, language, and behaviour (Laforce et al., 2018). Compared with the MoCA, the DCQ has been found to be superior in detecting atypical dementias, such as posterior cortical atrophy, the sub-types of primary progressive aphasia, the behavioural and dysexecutive variants of Alzheimer’s disease, and the Parkinson-plus syndromes (Sellami et al., 2018). The DCQ also has excellent internal consistency, test–retest reliability, and interrater reliability (Laforce et al., 2018). It was also studied in a prospective community-based sample of 53 healthy French-speaking Canadian volunteers aged between 80 and 94 years old with no history of cognitive difficulties and a MoCA score ≥ 24 (Gravel et al., 2020). The DCQ has recently been translated and adapted into English. Its validation in this second language is currently underway among an older population-base sample so that it may be used more widely.
As older demographics are becoming both more culturally and linguistically diverse with increases in immigration, it is essential for the validation of DCQ in English to include individuals with various linguistic backgrounds. In fact, authors like Mindt et al. (2019) have emphasized the need for neuropsychologists to engage in empirically supported, culturally responsive neuropsychological evaluation of linguistically diverse and underrepresented older populations. Considering that in Canada, the English–French bilingualism rate in 2016 reached its highest proportion ever at 17.9% (Statistics Canada, 2017), authors like Sousa and Rojjanasrirat (2011) have also recommended that when a bilingual population is accessible, such as in Canada, new instruments should be pre-field-tested not just among monolingual but also among bilingual individuals.
The pre-field testing of new cognitive screening tests among linguistically diverse older individuals is also crucial, as factors such as bilingualism may play a role in patient self-report, informant report, and expression of neuropsychiatric and cognitive symptoms during psychometric evaluations (Mindt et al., 2019). Without the proper specifications to guide the evaluation of bilingual populations, test results can be prone to misinterpretations that may lead to inaccurate diagnoses once instruments are validated and used in clinical settings (Léon, 2017). In addition, preliminary psychometric testing of instruments like the DCQ in both monolingual and bilingual populations is essential as the current literature indicates that cognitive differences may exist between these groups. Researchers have found significant differences between these two groups regarding their performance on tests measuring working and episodic memory, attention/executive functioning, particularly cognitive control, as well as on verbal measures such as expressive vocabulary, receptive vocabulary and verbal fluency. As these cognitive functions are all evaluated by the DCQ, it is important to consider possible cognitive differences between monolinguals and bilinguals on this tool. This importance is further emphasized by the fact that not all researchers have found the same results when comparing both groups on these various cognitive domains. More precisely, a large proportion of authors claim that there exists a bilingual advantage in older adults on various tasks measuring memory (Ljungberg et al., 2013; Schroeder & Marian, 2012), executive functions (Abutalebi et al., 2015; Bialystok et al., 2004, 2008a, 2008b; Cox et al., 2016; Friesen et a1., 2015; Ljungberg et al., 2013; Salvatierra & Rosselli, 2011; Schroeder & Marian, 2012), and language (Obler et al., 1986), while others assert that no significant differences exist between groups on these same cognitive domains: memory (Bialystok et al., 2008a; Cox et al., 2016; Fernandes et al., 2007; Kousaie et al., 2014), executive functions (Kousaie et al., 2014; Kousaie & Phillips, 2012; Obler et al., 1986; Rosselli et al., 2000; Salvatierra & Rosselli, 2011), and language (Friesen et al., 2015; Ljungberg et al., 2013; Schroeder & Marian, 2012). A third, but less abundant body of research has also supported the presence of a monolingual advantage in older adults for tests assessing memory (Clare et al., 2016; Obler et al., 1986) and language (Bialystok et al., 2008a; Clare et al., 2016; Fernandes et al., 2007).
Numerous potential reasons can explain the inconsistencies found in the current literature, which include concerns of publication bias, statistical flaws, and failure to match groups on potentially confounding variables (Lehtonen et al., 2018). Past studies have also not always agreed on how to define ‘bilingualism’, as bilingual language skills vary widely according to age of acquisition, exposure, and immersion. Apart from the absence of a standard operational definition of bilingualism, many researchers have not properly explained how they classified their participants into a monolingual or a bilingual group. Others, contrary to recommendation (Mindt et al., 2019), have often compared monolingual and bilingual groups that have different first languages.
Resolving the inconsistencies in the current literature by using demographically balanced groups, divided using a clear and consistent method to assess bilingualism, and tested in their primary language, is necessary to better compare cognitive functions between older monolingual and bilingual adults when validating new cognitive screening tests. Unfortunately, preliminary psychometric testing of new instruments in both these populations has rarely been conducted. To date, we are aware of only one cognitive screening test has been specifically standardized and validated for the use of linguistically diverse older adults. This was done with the MMSE, by Milman et al. (2018) who showed that neurologically healthy, highly proficient bilingual speakers performed differently than monolingual speakers and were more likely to be classified in the borderline/impaired range than matched monolingual individuals. These results further suggest that substantial differences may influence the psychometric evaluations of bilingual populations compared with monolingual ones, which poses a challenge to clinicians.
Having highlighted the need to conduct preliminary testing of new tools in diverse linguistic groups, the current study aimed to compare older monolingual and bilingual anglophones on the English version of the DCQ, in a sample of healthy Canadians aged 50 years and over. This sample was representative of the DCQ’s targeted population in a clinical setting. The main objective of this exploratory study was to compare the groups on their total DCQ scores and on the DCQ’s five index scores (Memory, Visuospatial, Executive, Language, and Behaviour). Adaptations and considerations are to be suggested for the future clinical use of the English DCQ in the event that significant differences are found between the two groups.
Methods
Participants
A total of 85 cognitively normal native English-speaking Canadians aged between 53 and 80 years were recruited. This was done via public announcements, advertisements, and through partnerships with other institutions (e.g., the Clinique Interdisciplinaire de la Mémoire in Quebec City, the Douglas Hospital Research Center in Montreal, the Research Center on Aging in Sherbrooke, the Sunnybrook Research Institute in Toronto, the University of Calgary and the Hotchkiss Brain Institute in Calgary, the St. Joseph’s Hospital in Saint John, New Brunswick and the University of British Columbia Hospital in Vancouver).
Participants were recruited if English was their first language and if they did not report a history of traumatic brain injury, delirium, brain surgery, neurological disease, encephalitis or meningitis, untreated metabolic condition, psychiatric illness, brain oncological therapy, alcohol/drug abuse, disabling visual/hearing disorders, experimental therapy, and illiteracy.
Materials
Montreal cognitive assessment (MoCA)
Global cognition was assessed using the MoCA (Nasreddine et al., 2005), a 12-minute cognitive screening tool to detect mild cognitive impairment and dementia. The MoCA is scored out of 30 points and assesses visuospatial and executive function, naming ability, memory, attention, language, abstraction, and orientation.
Language experience and proficiency questionnaire (LEAP-Q)
To determine their linguistic profiles and to place them in either the monolingual or bilingual group for the current study, all participants completed the LEAP-Q (Marian et al., 2007). This questionnaire measures an individual’s level of bilingualism based on their self-reported second language proficiency for reading, writing, and oral comprehension. The participants were asked to rate themselves using a Likert-type scale from 0 (i.e., extremely low) to 10 (i.e., perfect, native level). Age of second language acquisition, current language dominance, and current second language exposure are also information gathered by the questionnaire.
The internal and criterion-based validity of the LEAP-Q have been established (Marian et al., 2007) and have proven to be reliable indicators of language ability. The questionnaire has been translated into 16 languages and is valid among a healthy adult population with high school levels of literacy. As bilingualism is a concept difficult to measure, the LEAP-Q aims to capture factors that have previously been identified as important contributors to bilingual status such as language competence (including proficiency, dominance, and preference ratings across speaking, understanding, reading, and writing), age of language acquisition, modes of language acquisition, prior language exposure, and current language use.
Anglophones who reported no second language knowledge on the LEAP-Q were placed in the monolingual group. Those who self-reported a level of proficiency of 7 or higher (good to perfect) on their speaking, understanding, and reading skills in their second language, and who also reported using two languages regularly, were placed in the bilingual group. This strict cutoff for the bilingual group was used to focus on highly proficient bilinguals, who have been shown to differ on screening tasks compared with monolingual individuals (Milman et al., 2018). All participants reporting scores lower than 7 were excluded for the purpose of the current study.
Dépistage Cognitif de Québec (DCQ; www.dcqtest.org)
The DCQ (Laforce et al., 2018; Sellami et al., 2018) is a cognitive screening test administered in an average time of 25 minutes. It is scored on 100 points and targets five relevant domains: Memory, Visuospatial, Executive, Language, and Behaviour. The Memory Index (out of 24) assesses basic attention using the forward digit span, a short-term recall task of eight words with delayed recall after 15 minutes, and a recognition task. The Visuospatial Index (out of 14) tests visual recognition of overlapping figures and spatial rotation (the subject is asked to recognize an image from a scene with varied viewing angles). This index also includes a geometric figure drawing test. The Executive Functions Index (out of 10) includes a backward digit span, naming the months of the year backwards, an alternating graphic sequence test, a two-item verbal abstraction task, a phonemic fluency (of the letter A), and a modified Stroop test. The Language Index (out of 28) comprises a scene description task to assess spontaneous speech, a naming and single-word writing task, a multi-sentence writing test, assessment of comprehension through a sentence-picture matching test, a semantic verbal fluency task (animals), and a task requiring the participant to repeat short as well as long and complex sentences. Finally, the Behavioural Index (out of 24) explores 10 domains (depression, anxiety, delusions, hallucinations, irritability and aggression, apathy, disinhibition and impaired judgement, perseverations and compulsions, loss of empathy/sympathy and self-criticism) as reported by a significant other.
Procedure
Participants were first contacted by phone. To make sure they were healthy, an initial screening was conducted to gather information on current and past medical history. Participants were then either assessed individually at one of our testing sites or visited in their homes by a trained research assistant. They were informed about the nature of the study and the types of tasks that would be administered. Informed written consent was obtained from all participants. Testing occurred in a single session lasting approximately 1 hour. Participants first completed the LEAP-Q to assess their linguistic profiles. The MoCA and the DCQ were then administered in a randomized order to account for any carryover effect between the tests. Finally, to complete the DCQ’s caregiver questionnaire for the behavioural index, participants were asked to provide the phone number of a family member, friend, spouse, or caregiver. These individuals were then contacted within the following 2 months of the testing session to complete a 5-minute interview over the phone. This study was approved by the Ethics Committee of Laval University, Québec City, and the local ethics board of the participating sites.
Statistical analysis
Basic descriptive analyses included means and standard deviations. As Levene’s test was significant (p < .05), suggesting a violation of the assumption of equal variances, groups were compared using Welch’s unequal variances t test. Monolinguals and bilinguals were compared on their education levels, age, MoCA total score, DCQ total score, and for each DCQ index: Memory, Visuospatial, Executive Function, Language, and Behavioural. This was followed by a Bonferroni correction for multiple comparisons. Box plots charted for the findings did not suggest that the data were normally distributed, and as a result, the groups were once again compared on their MoCA total scores, DCQ total scores, and for all the DCQ’s indexes using a Mann–Whitney U test. This was followed by a second Bonferroni correction. Statistical analysis was performed using SPSS software (version 24.0) with the alpha level set at .05.
Results
Demographics
Following the testing session, five participants were excluded because they scored below 26 on the MoCA. This normative threshold has been set for healthy adults in the age group studied (Malek-Ahmadi et al., 2015; Nasreddine et al., 2005). For the purpose of our analysis and to ensure that monolinguals were compared with highly proficient bilinguals, 21 participants were also excluded as they did not meet the inclusion criteria for high proficiency in their second language. As a result, the final sample of participants included a total of 59 anglophones: 30 monolinguals and 29 bilinguals. Among monolinguals, age ranged between 53 and 80 years. In bilinguals, age varied between 51 and 79 years. Demographic variables for both monolingual and bilingual groups are presented in Table 1.
Descriptive data for the monolingual and bilingual groups.
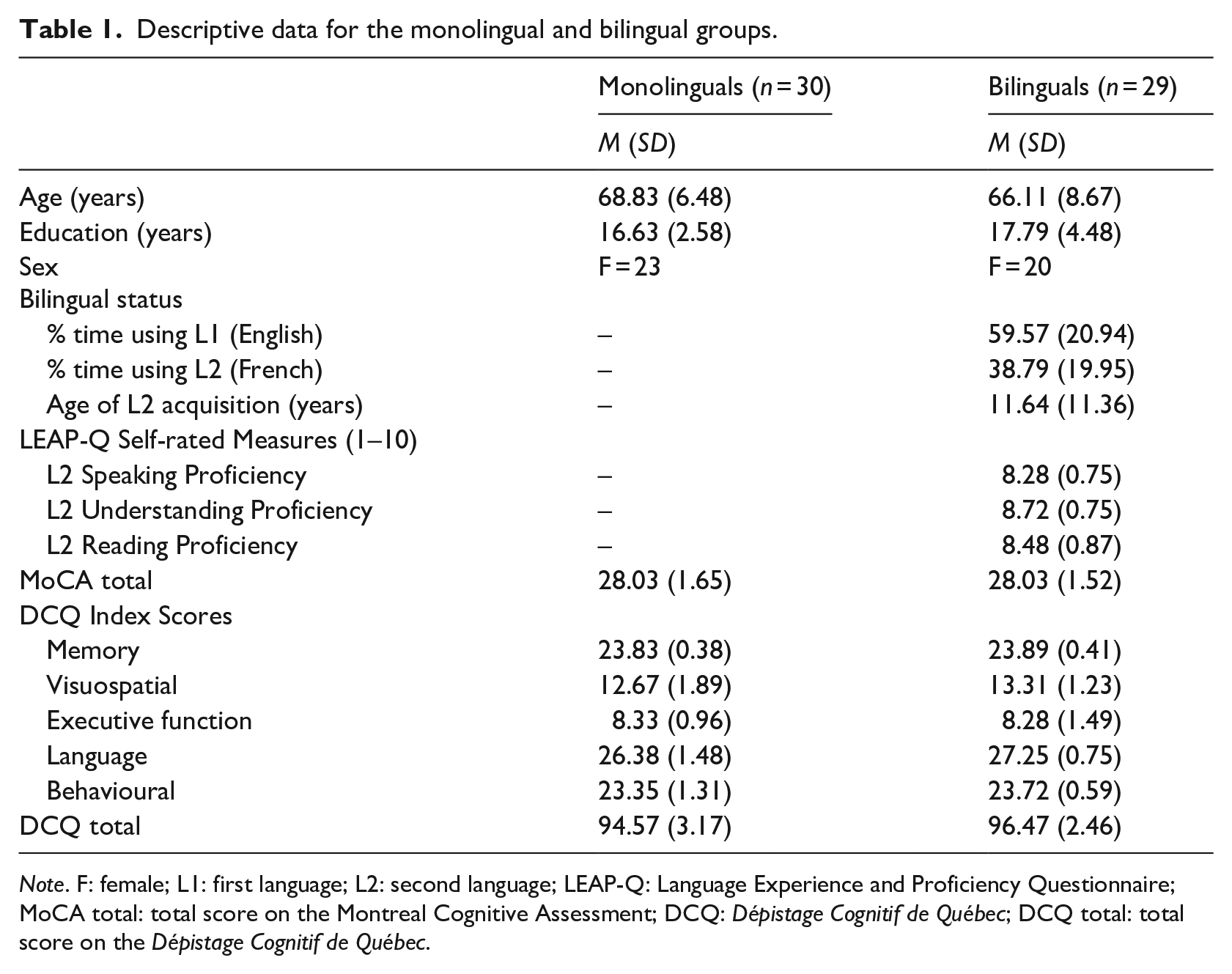
Note. F: female; L1: first language; L2: second language; LEAP-Q: Language Experience and Proficiency Questionnaire; MoCA total: total score on the Montreal Cognitive Assessment; DCQ: Dépistage Cognitif de Québec; DCQ total: total score on the Dépistage Cognitif de Québec.
There were no significant differences in age and education between the monolingual and bilingual groups (Table 2). There were also no significant differences between the groups on their MoCA test scores. The group of monolingual participants was composed of more women than men (76.66% female), as was the bilingual group (68.97% female). However, there were no differences between the proportion of women and men between groups (p = .51), nor was there a significant sex difference on the MoCA and the DCQ total test scores (p = .91 and p = .13, respectively). Furthermore, correlations between age, years of education, and total DCQ scores were not statistically significant (r = −.13, p = .34 and r = .19, p = .15, respectively).
Comparisons between monolingual and bilingual groups.
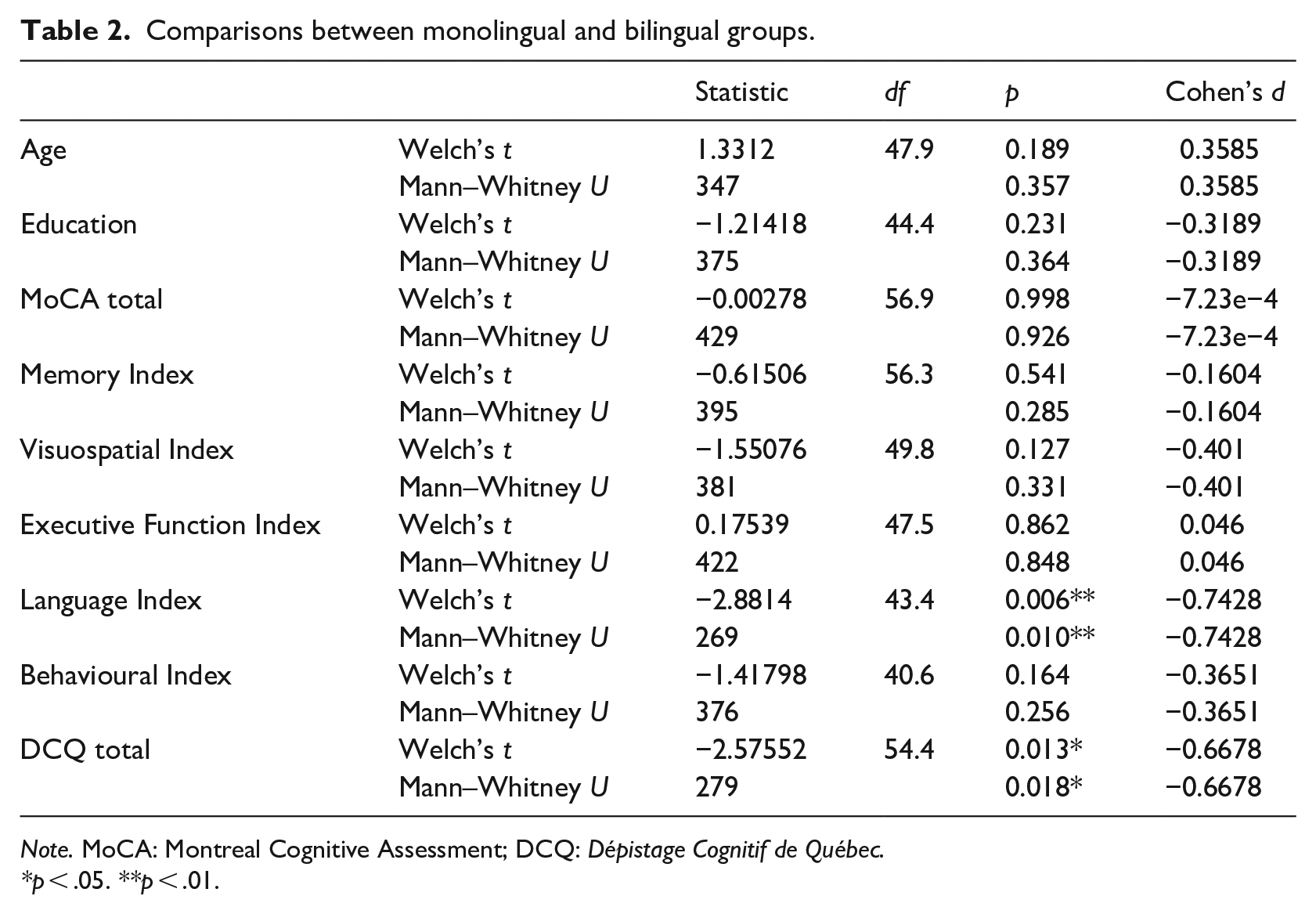
Note. MoCA: Montreal Cognitive Assessment; DCQ: Dépistage Cognitif de Québec.
*p < .05. **p < .01.
Within the bilingual group of participants, mean age of second language acquisition was 11.64 years (SD = 11.4). Their second language oral proficiency (M = 8.28, SD = 0.75), comprehension proficiency (M = 8.72, SD = 0.75), and reading proficiency (M = 8.42, SD = 0.87) on the LEAP-Q were all above the initial requirement of 7/10. All participants reported using both languages regularly and their exposure to English was greater than their exposure to the non-English language. Out of the 29 bilingual participants, 28 had French as their second language and only one reported having both French and Spanish as her second languages, being equally fluent in both. In total, six of the 29 bilingual participants were also proficient in a third language.
Comparisons between the monolingual and bilingual group
No significant group effects were found on the Memory Index (F = 1.12, p = .54), on the Visuospatial Index (F = 13.04, p = .13), on the Executive Function Index (F = 11.48, p = .86), or on the Behavioural Index (F = 5.52, p = .16). A significant difference was found between groups on the Language Index (F = 3.47, p ≤ .01) and on the DCQ total score (F = 2.90, p ≤ .05), indicating a higher average score for the bilingual group. When applying a Bonferroni correction for multiple comparisons (0.05 ÷ 6 = .0083), the difference between groups on the Language Index was maintained, but the significant effect between DCQ scores did not persist. Cohen’s d was used to calculate the effect size between the group means on the Language Index (d = −0.74) and on their total DCQ scores (d = −0.67).
A box plot for both the Language Index (Figure 1) and the DCQ total score (Figure 2) between groups was used to identify two monolingual outliers on the Language Index and one bilingual outlier among the total DCQ scores. The analyses were rerun without these outliers and remained significant for both the Language Index (F = 0.43, p ≤ .05, d = −0.66) and the total DCQ score (F = 5.81, p ≤ .005, d = −0.81).
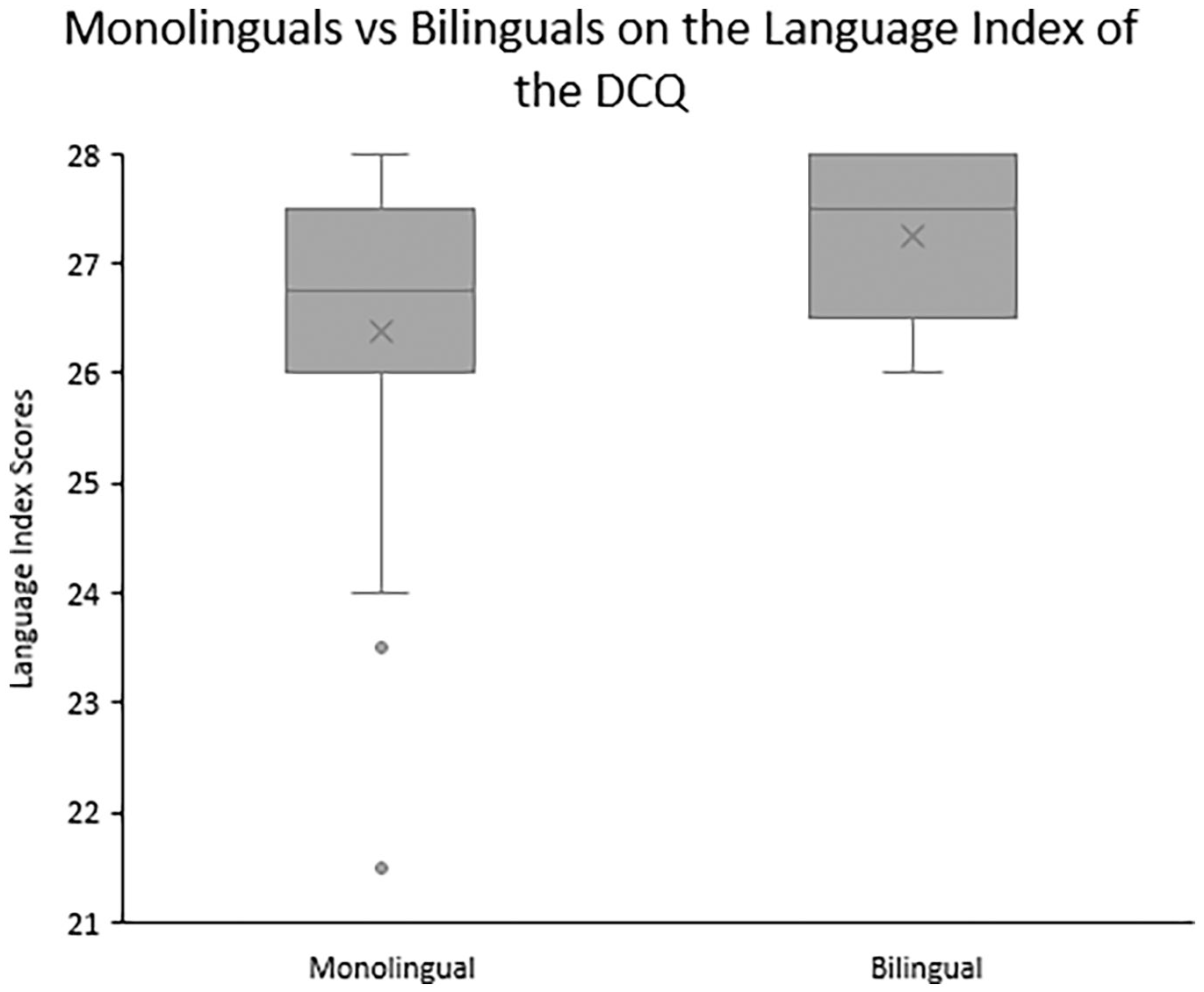
Box plot of monolingual and bilingual group scores (out of 28 points) on the Language Index of the Dépistage Cognitif de Québec (DCQ).
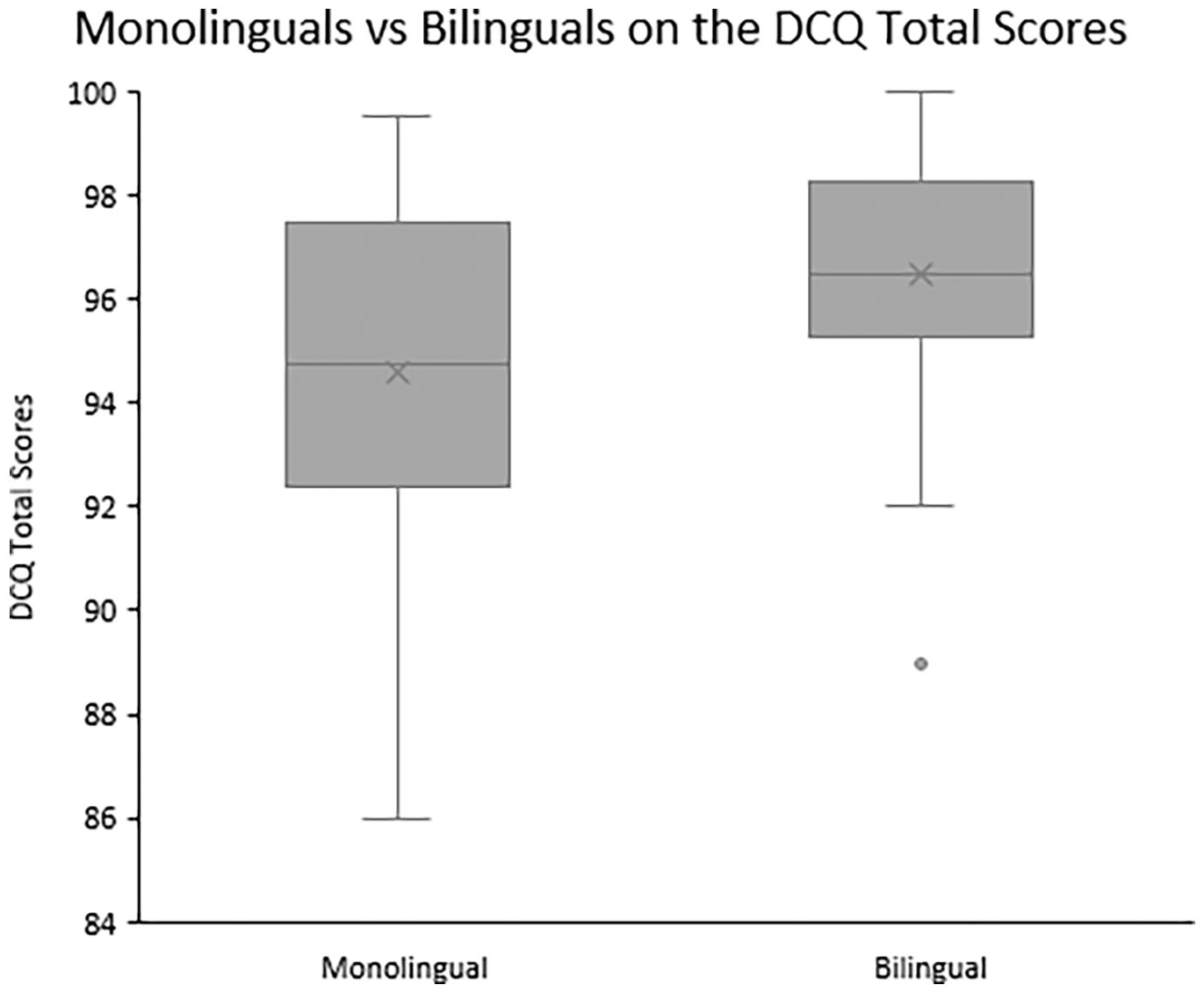
Box plot of monolingual and bilingual group scores (out of 100 points) on the Dépistage Cognitif de Québec (DCQ) total scores.
In addition, as the box plots charted (Figures 1 and 2) did not suggest that the data were normally distributed on the Language Index and for the total DCQ scores, a nonparametric test was also used to further compare the monolingual and bilingual groups on all variables, to confirm our previous findings. The Mann–Whitney U test supported the absence of significant effects between groups on the Memory Index (U = 395, p = .29), the Visuospatial Index (U = 381, p = .33), the Executive function Index (U = 422, p = .84), and the Behavioural Index (U = 376, p = .26). Again, a significant effect was established between groups on the Language Index (U = 269, p = .01) and on the DCQ total scores (U = 279, p ≤ .05) in favour of the bilingual group, but these effects were no longer significant after the Bonferroni correction. Interestingly, the highest possible sub-score of the six sub-scores composing the Language Index, the semantic sub-score (which has a total of 6 possible points as opposed to other sub-scores which range from 1 to 5 points), was higher for bilinguals (5.6) than for monolinguals (4.2), hence likely contributing to this difference between the groups.
Discussion
The present study explored the psychometric properties of the English DCQ in a sample of healthy monolingual and bilingual English-speaking Canadians aged 50 years and over. The main objectives were to compare the groups on their total DCQ scores and on their five-index scores. Our results indicated that bilinguals outperformed monolinguals on the DCQ total score, which was driven by a bilingual advantage on the Language Index. Following a Bonferroni correction, the bilingual advantage on the overall DCQ scores did not persist but the advantage on the Language Index remained. Overall, the effect sizes ranged between medium and large. We found no significant differences between groups on any of the other DCQ indexes: visuospatial, executive, memory, and behavioural.
A bilingual advantage for the overall DCQ
This study is the first to explore the psychometric properties of the DCQ in older monolingual and bilingual participants, both tested in their native language (English) and with bilingual participants who were all proficient in the same second language (French). The overall advantage found for bilinguals on the total DCQ score (before correcting for multiple comparisons) is consistent with a growing body of research suggesting that bilinguals may have a global advantage on cognitive tasks, presumably due to their greater cognitive reserve. Over recent years, the term ‘cognitive reserve’ has been used inconsistently, but most recent works aiming to clarify and propose a consensual definition of the concept agree that it refers to one’s cumulative improvement of neural resources that mitigates the effects of neural decline caused by ageing or age-related diseases (Cabeza et al., 2018). Cognitive reserve is not fixed or immutable and is influenced by relevant lifetime exposures which include early-life general cognitive ability (e.g., intelligence), education, occupation, physical exercise, leisure activities, social engagement (Stern et al., 2020), as well as language learning (Cheng et al., 2015). In fact, recent studies have suggested that language learning may lead to changes in the structure of the brain, which may consequently contribute to the promotion of an individual’s cognitive reserve (Cheng et al., 2015). Bilingualism enhances cognitive functions among healthy older individuals (Klimova, 2018; Kousaie & Phillips, 2017) and could also protect against future age-related losses. This said, as the bilingual advantage on the total DCQ score did not survive multiple comparisons, perhaps due to our sample of highly educated older adults, further research on bilingualism as a contributing factor to cognitive reserve, and its impact on cognitive screening tools, still needs to be conducted.
A bilingual advantage for the DCQ’s language index
In terms of the bilingual advantage on the Language Index of the DCQ, our findings are consistent with previous research. More precisely, the bilingual group in a study by Obler et al. (1986) did not perform better than monolinguals on all language-related tasks, but they did have an advantage on the category fluency task (animals), which is also present on the Language Index of the DCQ. This bilingual advantage on category fluency tasks has also been reproduced in Mathison’s (2017) study, where it was found that high-level bilinguals were able to retrieve more words than monolinguals on category fluency trials (animals, fruits, and clothes). Just like our study, Mathison’s study included a highly proficient group of bilinguals, who were all tested in their dominant language, and for whom second language acquisition varied between early and late life. As many people across the globe do not always acquire their second language early on, this group of bilinguals more closely resembles that of the population which will be tested by the DCQ.
Various hypotheses can be theorized to explain why our bilingual group may have performed better on the Language Index of the DCQ compared with our monolingual group. One of these explanations lies within the notion that bilinguals tend to have a combined vocabulary from both their languages that can sometimes be larger than in monolinguals (Mathison, 2017). This could be especially true if the acquisition of a second vocabulary is done in a foreign but related language to one’s first language (Keuleers et al., 2015). As Schepens et al. (2012) estimate that about 16% of English and French words have the same cognate, meaning that they have the same linguistic derivation, it is possible that the bilingual anglophones in our study shared or indirectly acquired a larger vocabulary through their knowledge of French than did the monolinguals. This could have advantaged them on tasks such as word naming and writing, all present on the Language Index of the DCQ. Moreover, the bilingual and monolingual participants in the study lived in the same cultural environment and therefore have a largely similar semantic memory store. The representations in this semantic memory store are retrieved in every linguistic task of the DCQ.
As also suggested by Mathison (2017), a second explanation as to why we found a bilingual advantage on the Language Index in older adults may result from the fact that our study solely included highly proficient bilinguals. In fact, Costa and colleagues (2006) proposed a differential language control mechanism for low- versus high-proficiency bilinguals. Irrespective of age of acquisition, Costa and colleagues theorize that low proficiency bilinguals rely on inhibitory mechanisms when using one of their languages to avoid interference from their second language. In contrast, higher proficiency bilinguals have a language-specific selection mechanism, which allows them to avoid this interference and maintain a dual-language activation. As a result, when completing a language-related task, such as during a naming, writing, or semantic task, highly proficient bilinguals exclude the non-target language from their selection process, which thus facilitates language retrieval (Costa et al., 1999; Costa & Santesteban, 2004; Costa et al., 2006).
The absence of a monolingual or bilingual advantage on all other indexes
Similarly to some of the current literature, our study did not find a monolingual nor a bilingual advantage on the memory or the executive function indexes of the DCQ (Bialystok et al., 2008a; Clare et al., 2016; Cox et al., 2016; Fernandes et al., 2007; Incera & McLennan, 2018; Kousaie et al., 2014; Kousaie & Phillips, 2012; Obler et al., 1986; Rosselli et al., 2000; Salvatierra & Rosselli, 2011). This absence of an advantage may again lie within the fact that the current study only included highly proficient bilinguals, who not only had a strong proficiency in their second language but also for whom the acquisition of a second language varied across their life. In fact, a study by Tao et al. (2011), comparing early bilingualism (around the age of 4) and later acquisition (after the age of 12), found that only early bilinguals outperformed monolinguals on the Lateralized Attention Network Test (Greene et al., 2008) which measures an individual’s vigilance, orienting and executive control networks. As the bilingual participant group in our study acquired on average their additional language after 11 years of age, this could explain why we did not find a significant difference between our groups on some of the DCQ’s indexes, such as on the executive or visuospatial index.
Another potential reason as to why the current study did not find a monolingual or bilingual advantage on the memory, executive, visuospatial, and behaviour index of the DCQ might be explained by the fact that all our participants were neurologically healthy adults (screened with the MoCA) and had high levels of education. This may have caused a ‘ceiling’ effect in our sample, as in such high-functioning older adults, differences between monolinguals and bilinguals may not have been detectable.
Finally, as our sample of bilingual participants was solely composed of native-English speakers, we can hypothesize that our participants were most likely non-immigrant North American-born individuals. This factor may partly explain why our groups had a similar performance on many of the DCQ’s indexes since previous research has attested that immigrant status is an important factor that can enhance bilingual performance (Fuller-Thomson & Kuh, 2014). Recent evidence also suggests that immigrants have slower rates of cognitive decline as they have a lower prevalence of chronic health conditions associated with dementia (e.g., high blood pressure, high cholesterol, or diabetes). They may also have a higher intelligence quotient (Milne et al., 2001), which is additionally highly protective against cognitive decline and dementia (Stern, 2006). Studies having controlled for immigration status found no group advantage between monolinguals and bilinguals on cognitive tasks measuring working memory and executive functions (Kousaie et al., 2014; Kousaie & Phillips, 2012). Although the current study did not actively control for immigrant status, past research shows that the absence or rather the small probability of having immigrants among our bilinguals could have contributed to the absence of differences between our groups.
Limitations
As the current study did not control for immigration status and was limited to neurologically healthy and highly educated older individuals, our findings cannot be generalized to all monolingual and bilingual healthy persons, nor to those with cognitive impairments. In addition, it is important to consider that bilingualism in the current study was measured with a questionnaire (LEAP-Q) and not with a complete language assessment. Nonetheless, the questionnaire used helped us distinctly classify the participants into either the ‘monolingual’ or the ‘bilingual’ group. Furthermore, with the LEAP-Q, we were able to make sure that individuals were using both their first and second language on a regular basis. This is important as bilingualism-induced subcortical effects have been shown to be directly related to active, continuous, and extensive immersion in a bilingual environment (Pliatsikas et al., 2017).
Finally, the bilingual group in the current study was also solely composed of anglophones who had French as their second language. Naturally, we are aware that this will not be the case for all bilinguals in a more diverse clinical setting. Nevertheless, testing participants who all had the same second language helped bolster our conclusions by controlling for any potential confounding variables linked to different second language knowledge. Moreover, as all participants shared the same first language (English), everyone was assessed in their strongest language thereby eliminating common confounding factors such as vocabulary size (Ljungberg et al., 2013). Testing participants in their first language is also a strength for the current study, as the DCQ will be administered to patients in their dominant language/first language when used in a clinical setting. This is crucial to obtain accurate results, as bilingual older adults who start to show mild cognitive impairments generally experience loss of their second language before the loss of their first language (Mindt et al., 2019).
The future clinical use of the DCQ
Despite these limitations, the results of the current study highlight the importance of identifying and characterizing linguistic diversity before using new screening tools in clinical settings. This is important as even healthy bilingual individuals, with high-education levels, may have noteworthy cognitive advantages that may affect their performance on language-related tasks, which may in turn affect their overall cognitive scores. This said, the results found on the DCQ should be interpreted in terms of cognitive epidemiology and not as an obligatory clinical adaptation for the future use of the tool. Although we observed differences between groups, there was less than a 2-point difference on their overall DCQ scores and less than a 1-point difference on their Language Index scores: the clinical or the functional significance of these differences remains unclear and should be interpreted with caution (Peterson, 2008).
Nonetheless, we believe that the potential cognitive advantages of bilingualism as shown on the DCQ should be considered when interpreting test data. This is especially important, as a higher performance on language-related tasks may have an impact on overall test scores. In addition, the effect that may have bilingualism on test results should be explicitly discussed in neuropsychological reports. More precisely, neuropsychologists should be sensitive to linguistic differences, and similar studies should be conducted for future cognitive screening measures in healthy and clinical populations. Future studies should also be conducted to further examine the differences between monolingual and bilingual participant or patient groups on language-related tasks.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.C.C. has consulted for or received travel honoraria or test products from Nestlé Health Science, Cargill, and Abbott. All other authors declare that there is no conflict of interest.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Canadian Institutes of Health Research (CIHR), the Fondation du CHU de Québec, the Alzheimer Society – Quebec Division, and La Chaire de recherche sur les Aphasies Primaires Progressives – Fondation de la famille Lemaire (app-ffl.ulaval.ca).
Author biographies
Recently retired,