
Abstract
Posttraumatic stress disorder (PTSD) in refugees has been linked to poor social outcomes. Self-stigma appears to be a potential barrier to social engagement in refugees with PTSD, however research into this relationship is scarce. As such, the study aimed to 1) investigate whether self-stigma of PTSD (SSPTSD) and self-stigma of seeking help (SSOSH) underlie the association between PTSD and reduced social engagement in refugees, and 2) identify psychological mechanisms underpinning the association between PTSD and both types of self-stigma. In this online study, 262 Arabic-speaking refugees who had resettled in Australia completed measures indexing PTSD, two types of self-stigma (SSPTSD and SSOSH), social engagement outcomes (help-seeking behaviour, perceived social support), and potential mechanisms (self-esteem, hope, and negative help-seeking beliefs). Path analyses revealed that greater PTSD symptom severity was associated with reduced help-seeking behaviour via greater SSOSH and lower perceived social support via greater SSPTSD. Path analyses also revealed that greater PTSD symptom severity had an indirect effect on both types of self-stigma via greater negative help-seeking beliefs and an indirect effect on SSPTSD via lower hope. Findings demonstrate the deleterious effect of self-stigma on refugee mental health, yet also indicate potential intervention targets to reduce the negative impact of self-stigma.
Keywords
Introduction
There are currently over 117 million forcibly displaced persons worldwide, including more than 40 million refugees and asylum-seekers (UNHCR, 2024). The refugee experience is characterized by exposure to war, violence, conflict, and persecution (UNHCR, 1951). As such, posttraumatic stress disorder (PTSD) is prevalent and elevated amongst refugees compared to the general population (Blackmore et al., 2020). PTSD has significant negative consequences for daily functioning, with research indicates that PTSD is linked to poor social outcomes in refugees and trauma-exposed populations (Bryant et al., 2023; Jellestad et al., 2021). More specifically, research with refugees has demonstrated that PTSD is associated with decreased social engagement with formal support (such as mental health professionals) and lower perceived social support from informal support (such as social network) in the post-migration environment (Ahmad et al., 2020; Fuhr et al., 2019; Slewa-Younan et al., 2015; Sundvall et al., 2021). This is problematic as access to both formal and informal support is important for recovery from the psychological consequences of traumatic experiences (Charuvastra & Cloitre, 2008; Wang et al., 2021).
One potential barrier to social engagement for refugees with PTSD is self-stigma relating to mental health and help-seeking. Stigma is an inherently social concept as it encompasses negative stereotypes existing in the community resulting in prejudice and discrimination (Corrigan & Watson, 2002). Self-stigma occurs when these negative stereotypes either about mental health (self-stigma of mental illness) or help-seeking (self-stigma of seeking help) are internalized and applied to the self, resulting in feelings of shame (Rüsch et al., 2005; Vogel et al., 2007). Additionally, self-stigma is associated with higher PTSD symptoms and has been demonstrated to underlie the relationship between PTSD severity and lower help-seeking intentions across both formal and informal sources in refugees (Byrow et al., 2019; Kira et al., 2014). While existing evidence points to self-stigma as a potential barrier to social engagement in refugees with PTSD symptoms, this relationship remains under-researched.
If self-stigma is indeed a key barrier to social engagement, it needs to be addressed to facilitate engagement with formal and informal support. In order to reduce self-stigma, it is first necessary to understand the psychological mechanisms underpinning the relationship between PTSD and self-stigma. Psychological factors that arise from PTSD symptoms (such as negative beliefs about the self, others, and the future) represent potentially malleable targets that could inform interventions designed to reduce self-stigma and increase social engagement amongst individuals with PTSD. We have identified three potential candidate mechanisms that may contribute to this relationship, namely self-esteem, hope, and negative help-seeking beliefs which have been implicated in various models of self-stigma (Corrigan et al., 2009; Yanos et al., 2008). Self-esteem can be defined as one's regard for oneself and one's abilities. Low self-esteem has been associated with elevated psychopathology and elevated self-stigma and has been identified as a mediator between stigma and various outcomes including depression (Lannin et al., 2015; Livingston & Boyd, 2010; Wood et al., 2017; Zeigler-Hill, 2011). Similar relationships are observed between self-stigma and hope, which can be defined as a positive appraisal about the future, specifically an individual's ability and motivation to achieve life goals (Snyder, 2002). Hope has demonstrated a well-established negative relationship with both self-stigma and PTSD (Cullen et al., 2017; Gallagher et al., 2020; Lysaker et al., 2007). The final proposed mechanism is negative help-seeking beliefs, which can be conceptualized as negative perceptions of help-seeking and the help-seeking process. This is particularly relevant in refugee communities, where such beliefs are well-documented, and can include fears that confidentiality will be breached, discomfort associated with speaking to a stranger even if they are a professional, and perceived lack of cultural competency in the practitioner (Byrow et al., 2020). Negative help-seeking beliefs have been shown to be positively correlated with self-stigma of mental illness and self-stigma of seeking help in a refugee sample (Mastrogiovanni et al., 2024). Given that stigma arises from beliefs, negative help-seeking beliefs may be an underlying mechanism contributing to self-stigma in refugees with PTSD (Clement et al., 2015; Krendl & Freeman, 2019).
Aims and hypotheses
The aims of the current study were two-fold. The first aim was to empirically test whether two types of self-stigma (related to PTSD and seeking help) account for the relationship between PTSD symptom severity and reduced social engagement (perceived social support and help-seeking behaviour) in refugees.
It is hypothesized that PTSD symptom severity will be associated with reduced help-seeking behaviour from formal support via by both types of self-stigma. Specifically, we hypothesize that greater PTSD symptom severity will be associated with greater self-stigma of PTSD (SSPTSD) and self-stigma of seeking help (SSOSH) which, and in turn, will be associated with reduced help-seeking behaviour.
A similar pattern is hypothesized for the association between PTSD symptom severity and perceived social support. Specifically, we hypothesize that greater PTSD symptom severity will be associated with greater self-stigma of PTSD, and in turn, will be associated with lower perceived social support. We do not anticipate a relationship between SSOSH and perceived social support, since the former pertains to stigma associated with speaking to a professional and therefore is not relevant to social support.
The second aim of the current study was to identify potentially malleable mechanisms underlying the association between PTSD and both types of self-stigma. To our knowledge, there has been no research to date investigating this in refugees. Given the well-established link of self-esteem and hope with self-stigma and PTSD in broader populations, as well as the relevance of help-seeking beliefs in refugee communities, it was hypothesized that these would act as potential mechanisms underlying the relationship between PTSD and both types of self-stigma. Specifically, it is hypothesized that greater PTSD symptom severity will be associated with lower self-esteem, lower hope, and greater negative help-seeking beliefs which, in turn, will be associated with greater SSPTSD and greater SSOSH.
Materials and methods
Participants
Participants were 262 refugees recruited from advertising at refugee centres and services, social media platforms (i.e., Facebook), and snowball-sampling where participants were asked to indicate if someone they knew would be interested in participating in the study. Snowball-sampling has been found to be an effective recruitment method to reach vulnerable populations (Sadler et al., 2010). Participants were required to meet the following criteria to participate: a) refugee or asylum-seeker background, b) literate (i.e., able to read and write) in Arabic, and c) over 18 years of age.
Measures
All measures were translated into Arabic, and then blind back-translated into English by accredited translators, with minor discrepancies reconciled in collaboration with Arabic translators experienced in working with mental health-related material.
Exposure to potentially traumatic events
The 16-item Harvard Trauma Questionnaire (Mollica et al., 1992) was used to assess potentially traumatic events (PTEs) commonly experienced by refugees. This is a widely used measure amongst populations that have experienced mass conflict and displacement (Mollica et al., 1998; Sigvardsdotter et al., 2016; Steel et al., 2009). An additional four items were added to capture other common traumatic events experienced by refugees, namely “Family Violence,” “Serious accident at work, home, or during recreational activity,” “Physical assault,” and “Assault with a weapon,” Participants indicated whether they have either experienced, witnessed, or learnt about each event or none of the above. In this study, endorsing “experienced,” “witnessed,” or “learnt about” was considered to constitute an affirmative response. Positive responses were summed to create a count indexing exposure to PTEs ranging from 0 to 20.
Posttraumatic stress symptoms
The 20-item Posttraumatic Diagnostic Scale-5 (PDS-5) (Foa et al., 2016) was used to measure PTSD symptoms. The Arabic version of the PDS has been validated and used in refugee samples (Alghamdi & Hunt, 2019; Selmo et al., 2019). Items comprise PTSD symptoms included in the DSM-5 mapping onto each symptom cluster. Participants indicated how much each symptom had bothered them in the past month using a 5-point rating scale (0 = not at all to 4 = 6 or more times a week / severe). A mean across all items was used to index PTSD symptom severity. Internal consistency for this scale in the study was ɑ = 0.97.
Hope
The 12-item Hope Scale (Abler et al., 2017) was used to measure hope in this study. Items measured anticipation of a positive future, personal motivation, and belief in one's ability to achieve goals. This scale has been previously used with participants living in a low-resource, high HIV-prevalence setting (Abler et al., 2017). Participants indicated the extent to which they agreed or disagreed with each item on a 4-point Likert scale (1 = totally disagree to 4 = totally agree). Internal consistency for this scale in the study was ɑ = 0.96.
Help-seeking beliefs
The Help-Seeking Beliefs Scale was developed to assess beliefs about help-seeking in refugees (Mastrogiovanni et al., 2024). The scale consists of 24 items and three subscales capturing fears about seeking help, beliefs about the appropriateness of seeking help, and the perceived necessity of help-seeking. Participants indicated the extent to which they agreed or disagreed with each item (1 = Strongly disagree to 4 = Strongly Agree). Greater scores indicate greater negative help-seeking beliefs. In a sample of Arabic-speaking refugees, the scale demonstrated excellent internal consistency (ɑ = 0.96).
Self-esteem
Self-esteem-focussed items from the self-esteem/self-efficacy subscale of the Empowerment Scale were used to measure self-esteem in this study (Rogers et al., 1997). The original subscale contained nine items, however items capturing self-efficacy were removed as this construct is already captured in the Hope Scale. The remaining four items measured self-esteem specifically. Participants indicated how much they agreed or disagreed with each statement on a 4-point scale (1 = strongly disagree to 4 = strongly agree). Internal consistency for this scale in the study was ɑ = 0.88.
Self-stigma of PTSD
A 24-item version of the Internalized Stigma of Mental Illness Scale was used to measure SSPTSD (Ritsher et al., 2003). The scale was selected as it is well-established, widely used, and validated in Arabic (Boyd et al., 2014; Kira et al., 2015; Mittal et al., 2012). The scale has four subscales capturing different aspects of self-stigma, namely alienation, stereotype endorsement, discrimination experience, and social withdrawal. The original scale includes a stigma-resistance subscale, however this subscale has shown poor internal consistency in previous studies and so was not included in the present study (Ritsher et al., 2003; Wastler et al., 2020). Participants indicated the extent to which they agreed with items assessing self-stigma in relation to symptoms of posttraumatic stress. Participants responded to each self-stigma belief on a 4-point scale (1 = strongly disagree to 4 = strongly agree). A mean across all items was calculated where higher total scores indicated greater SSPTSD. Internal consistency for this scale in the study was ɑ = 0.98.
Self-stigma of seeking help
A 5-item version of the Self-Stigma of Seeking Help scale was used to assess SSOSH (Vogel et al., 2006). The scale has strong psychometric properties (Vogel et al., 2006). Participants indicated the extent to which they agreed with items assessing feelings towards seeking professional help using a 5-point scale (1 = strongly disagree to 5 = strongly agree). The full 10-item version of this scale includes five items measured in the negative direction (e.g., “I would feel inadequate if I went to a therapist for psychological help”) and five items measured in the opposite direction (e.g., “My view of myself would not change just because I made the choice to see a therapist”). In the current study, we found that negative items showed strong internal consistency (ɑ = 0.85), as did positive items (ɑ = 0.85), but the two sets of items did not correlate strongly with one another (r = 0.36). Given this, and other evidence that items that are reverse-scored demonstrate poor internal consistency with the other items in cross-cultural research (Nickerson et al., 2015; Schlechter et al., 2021), we retained only the negative items for analyses in this study. Internal consistency for this 5-item version of the scale was ɑ = 0.85.
Perceived social support
Perceived social support was measured with eight items used by Araya et al. (2007) based on the Social Provisions Scale (Cutrona & Russell, 1987). Items assess the extent to which participants feel their relationships provide varying dimensions of social support, including attachment, guidance, recognition of worth, and reliable alliance. Participants indicated the extent to which they agree or disagree using a 5-point scale (1 = strongly disagree, to 5 = strongly agree). A mean across all items was calculated where higher total scores indicated greater perceived social support. Internal consistency for this scale in the study was ɑ = 0.94.
Help-seeking behaviour
An adapted version of the Actual Help-Seeking Questionnaire was used to measure help-seeking behaviour with six items (Rickwood et al., 2005). In this scale, participants indicated with a “yes” or “no” whether they had sought help in the past two weeks from a variety of formal sources (e.g., mental health professionals such as a psychologist, health professionals such as a doctor, or other professionals such as a caseworker). A count of the number of types of sources participants sought help from over the past two weeks was calculated, ranging from 0 to 6.
Procedure
Data collection was undertaken from November to December 2020. Potential participants who previously indicated interest in future Refugee Trauma and Recovery Program research studies were emailed an invitation to participate via a Qualtrics link. Of the potential participants invited, 39% completed the survey. Interested participants took part by clicking on the Qualtrics link and completing the informed consent procedures prior to completing the online survey consisting of the battery of questionnaires above along with questions indexing demographic information. The survey took approximately one hour to complete. Upon completion, participants were reimbursed with a AU$20 online voucher to compensate for costs associated with completing the study. All participant procedures were approved by the UNSW Human Research Ethics Committee, HC200709.
Data analysis
Analyses were conducted in two stages using MPLUS Version 8.4 (Muthén & Muthén, 2019). Using path analysis, Model 1 investigated the first aim of the study: examining the effect of PTSD symptom severity on social engagement outcomes (perceived social support and help-seeking behaviour) via self-stigma (related to PTSD and help-seeking). The second path model (Model 2) investigated the second aim of the study by estimating the same paths as Model 1, with the addition of hypothesized mechanisms underlying the association between PTSD and self-stigma (hope, self-esteem, and negative help-seeking beliefs). Both models estimated the direct and indirect effects pertaining to our hypotheses. Specifically, in Model 1, we studied the association between PTSD and help-seeking via both types of self-stigma and the association between PTSD and perceived social support via SSPTSD. In Model 2, we added potential mechanisms to the model to test the association between PTSD and both types of self-stigma via the mechanisms of interest (hope, self-esteem, and negative help-seeking beliefs). We initially included age, sex, years in Australia, and visa security as covariates influencing PTSD symptom severity but, as the association between these variables and PTSD did not reach significance, these were omitted from subsequent analyses. To account for missing data, a maximum likelihood estimator was implemented to adjust model parameters based on available information (Allison, 2012).
Model fit was assessed using the following criteria: the root mean square error of approximation (RMSEA) < 0.06, the Comparative Fit Index (CFI) > 0.95, the Tucker–Lewis Index (TLI) > 0.95, and the standardized root mean square residual (SRMR) < 0.05 (Hu & Bentler, 1999).
Results
Participant characteristics
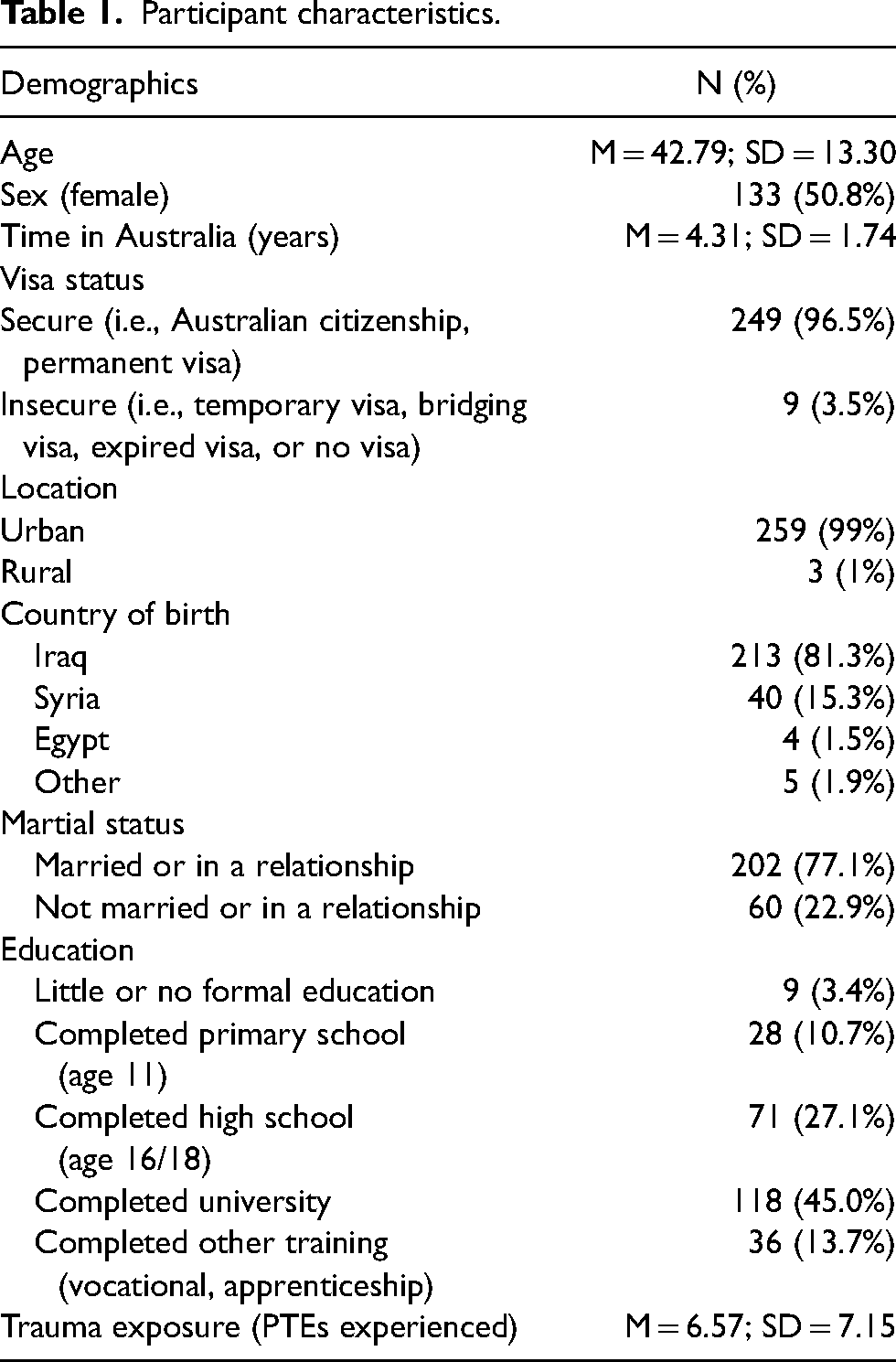
Participants were 42.79 years (SD = 13.30) on average, and just over half of the sample were female (n = 133, 50.8%). The majority of participants (n = 249, 96.5%) held a secure visa, resided in urban areas (n = 259, 99%), and had been in Australia for 4.31 years (SD = 1.74) on average. See Table 1 for more detailed participant characteristics.
Participant characteristics.
Path analysis
Missing data on the exogenous variable (PTSD) was below the 5% threshold.
Model 1: PTSD and social engagement outcomes via self-stigma
As all parameters were estimated, the model was saturated: CFI = 1.00, TLI = 1.00, RMSEA ≤ 0.001, SRMR = 0.006. In the supplementary materials, Table 2a presents the direct effects of Model 1 (also depicted in Figure 1) and Table 2b presents the indirect effects of Model 1.
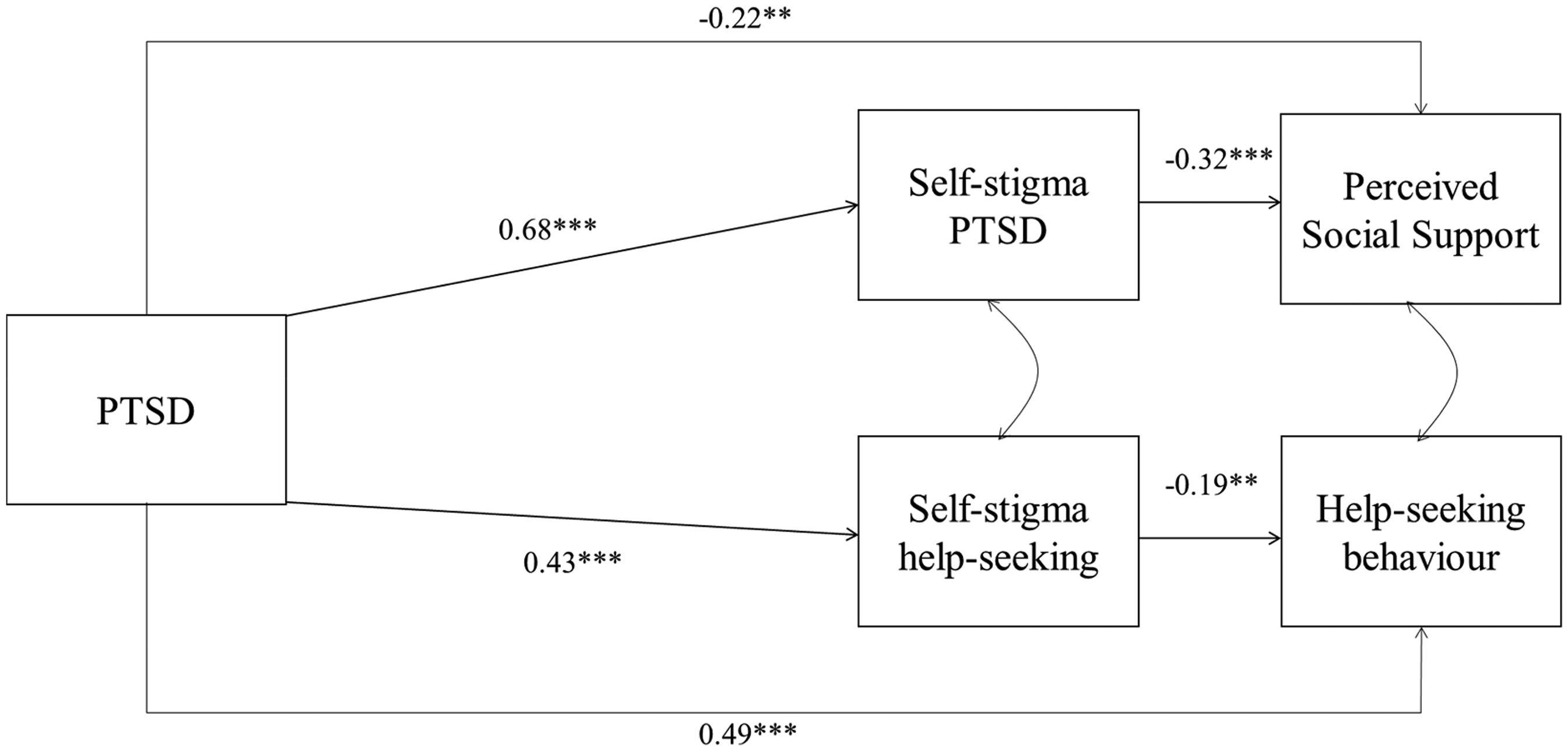
Schematic representing standardized coefficients of Model 1. For parsimony, only direct effects are displayed. See Table 2a and 2b for effect sizes of all paths. **p ≤ .01, ***p ≤ .001.
PTSD symptom severity and help-seeking behaviour
There was a significant indirect effect of PTSD on actual help-seeking behaviour via SSOSH, such that greater PTSD symptom severity was associated with greater SSOSH which, in turn, was associated with lower help-seeking behaviour (B = −0.05, SE = 0.02, ß = −0.08). Contrary to our hypothesis, there was no indirect effect of PTSD on help-seeking behaviour via SSPTSD.
PTSD symptom severity and perceived social support
There was a significant indirect effect of PTSD on perceived social support via SSPTSD (B = −0.23, SE = 0.06, ß = −0.21), whereby greater PTSD symptom severity was associated with greater SSPTSD which, in turn, was associated with lower perceived social support.
Model 2: PTSD and self-stigma via mechanisms
The initial model demonstrated a suboptimal fit: CFI = 0.951, TLI = 0.805, RMSEA = 0.153, SRMR = 0.056. As such, we considered modification indices to improve model fit. Modification indices suggested that estimating a path from hope to perceived social support would improve model fit. This path was added to the model which substantially improved model fit: CFI = 1.00, TLI = 1.00, RMSEA ≤ 0.001, SRMR = 0.015. In the supplementary materials, Table 3a presents the direct effects of Model 2 (also depicted in Figure 2) and Table 3b presents the indirect effects of Model 2.
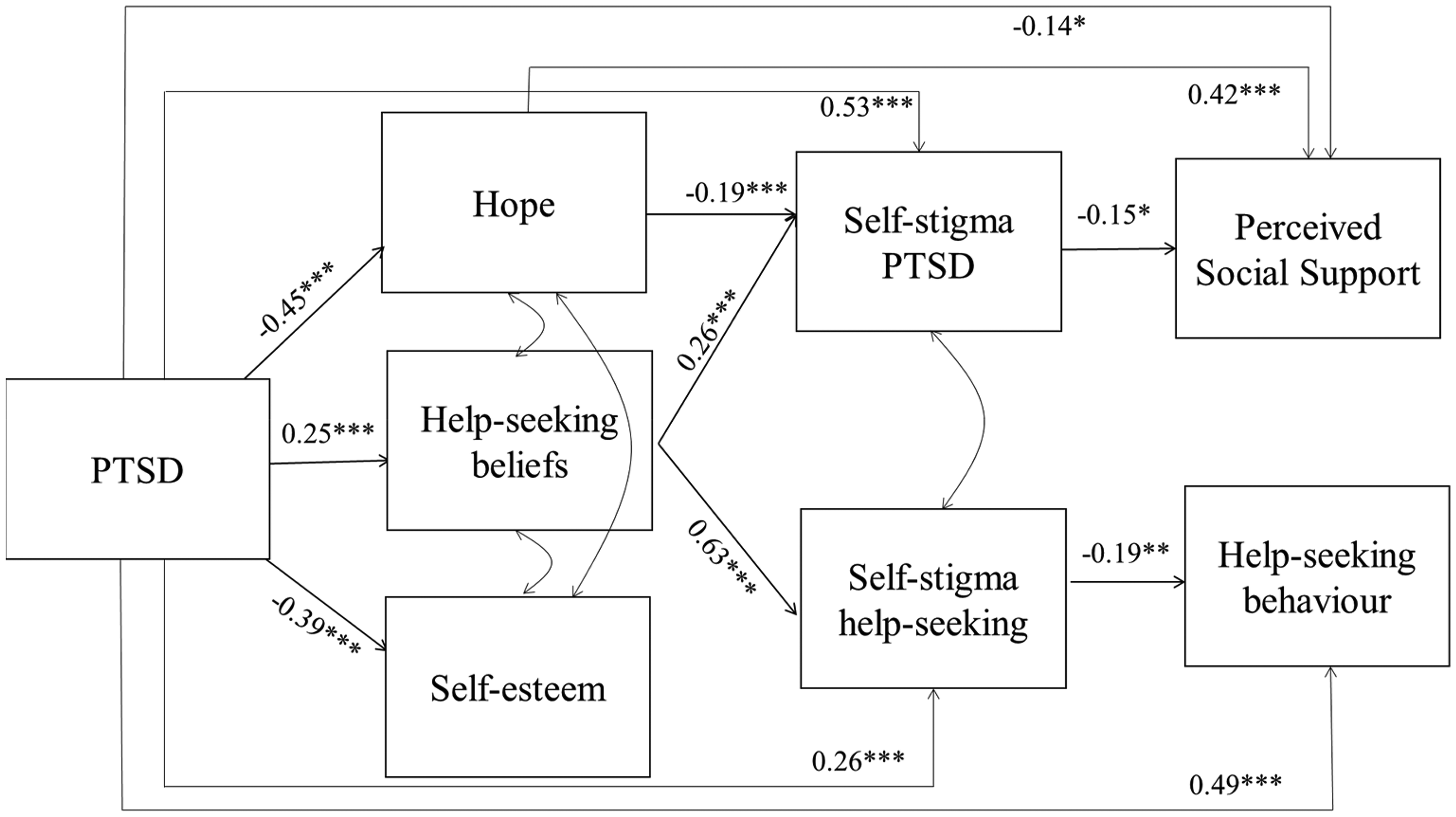
Schematic representing standardized coefficients of Model 2. For parsimony, only direct effects are displayed. See Table 3a and 3b for effect sizes of all paths. *p ≤ .05, **p ≤ .01, ***p ≤ .001.
PTSD symptom severity and SSPTSD
There was a significant indirect effect of PTSD on SSPTSD via hope whereby greater PTSD symptom severity was associated with lower levels of hope and, in turn, greater SSPTSD (B = 0.07, SE = 0.02, ß=0.09). There was also an indirect effect of PTSD on SSPTSD via help-seeking beliefs whereby PTSD symptom severity was associated with more negative help-seeking beliefs which in turn was associated with greater levels of SSPTSD (B = 0.05, SE = 0.02, ß = 0.06). Contrary to hypotheses, we did not observe an indirect effect of PTSD on SSPTSD via self-esteem.
PTSD symptom severity and SSOSH
There was a significant indirect effect of PTSD on SSOSH via help-seeking beliefs whereby greater PTSD symptom severity was associated with more negative help-seeking beliefs, which in turn was associated with greater levels of SSOSH (B = 0.16, SE = 0.04, ß = 0.16). Unexpectedly, we did not observe an indirect effect of PTSD on SSOSH via hope or self-esteem.
Discussion
The aims of the current study were to test whether 1) self-stigma underlies the relationship between PTSD and reduced social engagement and 2) negative help-seeking beliefs, self-esteem, and hope underlie the relationship between PTSD and self-stigma. To our knowledge, this is the first study to investigate psychological mechanisms underpinning the association between self-stigma and PTSD in refugees.
PTSD and social engagement outcomes via self-stigma
Investigation of the indirect effects of PTSD on social engagement via self-stigma revealed that different types of self-stigma had unique associations with different types of social engagement. Firstly, greater PTSD symptom severity, via SSOSH, was associated with participants seeking help from fewer mental health professionals (help-seeking behaviour). Secondly, PTSD symptom severity was associated with lower perceived social support from one's social network via greater SSPTSD.
The finding that greater PTSD symptom severity was associated with greater SSOSH, which in turn was associated with reduced help-seeking behaviour, suggests that SSOSH may be a barrier for refugees accessing support from mental health professionals. Past research with refugees has demonstrated an association between greater PTSD symptom severity and lower help-seeking intentions via SSOSH (Byrow et al., 2019). This study extends these findings beyond intentions to demonstrate that this effect is also present for behavioural responses. These findings are in accordance with research conducted with other populations, which demonstrates that SSOSH is consistently and negatively associated with reduced help-seeking (Clement et al., 2015). It is notable that, in this study, greater PTSD symptom severity had a positive direct effect on help-seeking behaviour such that greater PTSD symptom severity was associated with greater help-seeking behaviour. Thus, while refugees typically have lower help-seeking rates compared to the general population, those with higher symptoms were still more likely to seek support from mental health professionals relative to those with lower symptoms (Mazumdar et al., 2022). This is consistent with other research conducted with a refugee sample which indicated that greater psychosocial distress was associated with increased likelihood of professional help-seeking (Tomasi et al., 2022). In the context of a positive association between PTSD symptom severity and help-seeking, our finding that the negative indirect effect from PTSD symptoms to help-seeking via SSOSH suggests that SSOSH may interfere with the natural help-seeking process, thus representing an important barrier to address to reduce the treatment gap in refugees.
Consistent with our hypothesis, we found that SSPTSD played a role in the association between PTSD and lower perceived social support. This aligns with research demonstrating that self-stigma related to symptoms was associated with lower help-seeking intentions from informal sources (e.g., family members) in a refugee sample, and associated with weakened social support in a sample with serious mental health difficulties (Byrow et al., 2019; Livingston & Boyd, 2010). This finding suggests that shame about psychological symptoms (a key component of self-stigma) may hinder perceived social support from others, thereby reducing the likelihood of utilizing one's social network as a source of support. This may be particularly problematic in refugee communities from collectivist backgrounds where informal sources of support may be preferred and where connection to others is considered integral to identity (Grupp et al., 2019; Renner et al., 2020).
Contrary to our hypotheses, we did not observe an indirect effect of PTSD symptom severity on formal help-seeking behaviour via SSPTSD. This differs from previous studies that have observed that self-stigma related to mental illness is a barrier to help-seeking in refugees and other populations (Byrow et al., 2020; Clement et al., 2015). One possible explanation for this discrepancy in findings is that, in this study, we examined the effects of SSPTSD and SSOSH on formal help-seeking concurrently, thus investigating their independent associations with help-seeking over and above one another. This is in contrast to previous studies which have demonstrated these associations when investigating self-stigma related to mental illness independent of SSOSH. Given that these two types of self-stigma are correlated, past studies which investigated these variables in isolation may have obscured the unique relationship between SSPTSD and help-seeking behaviour in the current study. This explanation is supported by studies which have demonstrated that SSOSH emerges as the only significant predictor of help-seeking intentions when both types of self-stigma are considered concurrently (Lannin et al., 2015; Tucker et al., 2013).
In summary, the current study provides evidence for the specificity of particular types of self-stigma in influencing social engagement with formal and informal sources. Specifically, SSPTSD appears to underlie the association between PTSD symptom severity and perceived social support but not help-seeking behaviour, while SSOSH underlies the association between PTSD symptom severity and help-seeking behaviour but not perceived social support. While future longitudinal research is required to elucidate the extent to which different types of self-stigma are temporally related to different social engagement outcomes, the differential impact of various types of self-stigma observed in the current study can inform intervention approaches, depending on the focus and desired outcomes (increasing either formal or informal support). For example, utilizing effective mental health stigma reduction strategies such as psychoeducation and cognitive reappraisal to normalize symptoms may encourage individuals to utilize existing social support. In contrast, if the focus is on increasing engagement with mental health professionals, it may be more effective to normalize help-seeking and challenge misconceptions about the therapeutic process (Denkinger et al., 2022; Nickerson et al., 2019; Thornicroft et al., 2016).
PTSD and self-stigma via psychological mechanisms
In this study, we tested hypothesized psychological mechanisms underlying the association between PTSD symptom severity and self-stigma. Consistent with hypotheses, we found that greater PTSD symptom severity was associated with more negative help-seeking beliefs, which in turn was associated with increases in both types of self-stigma. Additionally, as anticipated, greater PTSD symptom severity was associated with reduced hope which in turn was associated with increased SSPTSD. However, there was no association between greater PTSD symptom severity and SSOSH via hope which was contrary to hypotheses. Finally, while PTSD symptom severity was associated with reduced self-esteem, there was no indirect effect observed from PTSD to SSPTSD or SSOSH via self-esteem.
Negative help-seeking beliefs was the only psychological mechanism that was associated with both types of self-stigma in this study. While longitudinal research is necessary to determine the temporal ordering of help-seeking beliefs and self-stigma, these findings highlight the potential role of perceptions of the help-seeking process (such as feared outcomes of help-seeking) in the development of self-stigma in refugees (Hammer et al., 2019; Mastrogiovanni et al., 2024). These findings replicate previous research demonstrating that negative perceptions of help-seeking and the help-seeking process contribute to reduced engagement with formal support amongst refugees and other groups (Byrow et al., 2020; Gulliver et al., 2010; Mojtabai et al., 2011; Schlechter et al., 2021; Vogt, 2011). These results suggest that addressing negative help-seeking beliefs regarding available services may represent an important intervention avenue to reduce self-stigma and in turn increase engagement with formal sources. This is supported by the significant indirect effect we observed of PTSD symptom severity on help-seeking behaviour via SSOSH and negative help-seeking beliefs in this study.
The finding that greater PTSD symptom severity was associated with reduced hope, which in turn was associated with greater SSPTSD (but not SSOSH), extends general population research to the refugee context, highlighting the association between hope and self-stigma (Corrigan et al., 2011; Yanos et al., 2020). Hope is defined as the individual's perceived ability to achieve their goals in the future (Snyder, 2002). It may be the case that experiencing PTSD symptoms depletes hope for the future via maladaptive coping strategies inhibiting recovery, thereby increasing shame and distress about persistent symptoms (Gallagher et al., 2020; Long, 2022). In contrast, contrary to our hypothesis, hope was not associated with increased SSOSH. One possible explanation for these divergent findings may lie in the conceptualization of hope as an intra-personal construct, which may make it more relevant for self-stigma relating to symptoms rather than SSOSH (which is related to shame about contact with a mental health professional). It is also notable that there was a significant path between hope and perceived social support in this study, indicating that the belief that one is likely to attain their goals in the future may be supported by one's interpersonal or informal network. This aligns with the broader literature that social support may promote hope amongst trauma survivors and military personnel with PTSD symptoms as well as research which has demonstrated a reciprocal and longitudinal association between hope and social support (Irving et al., 1997; Long, 2022; Xiang et al., 2020). This explanation is highly speculative, however, and further research is required to disentangle the complex associations between psychological mechanisms, self-stigma, and help-seeking.
Finally, contrary to hypotheses, there was no indirect effect observed between PTSD and either type of self-stigma via self-esteem. This is in contrast to research with participants with serious mental illness where there is a well-documented association between self-stigma and self-esteem (Lannin et al., 2015; Yanos et al., 2020). One potential methodological explanation for this discrepancy lies in the measure we used to index self-esteem. Items on this measure are focused on the individual (e.g., “I have a positive attitude about myself”), and thus may not have appropriately captured the construct in this sample of Arabic-speaking refugees who may be more likely to hold collectivist values (Ayyash-Abdo, 2001). Consistent with this, research indicates that self-esteem in collectivist cultures is often influenced by relationships with others and connection to the group, whereas self-esteem in individualistic cultures is more strongly determined by personal achievement and autonomy (Tafarodi & Swann, 1996). Accordingly, it may be important to adopt a more culturally relevant conceptualization of self-esteem in future investigations of self-stigma in individuals from collectivist cultures. Relatedly, alongside validated PTSD measures, it would be worthwhile to include measures which include culturally specific trauma-related symptoms, to capture contextual nuances that a PTSD diagnosis might not fully encompass (Good & Hinton, 2015; Legha, 2016).
Study findings should also be interpreted in the context of several limitations. Firstly, the nature of the sample limits ecological validity and therefore the extent to which findings can be generalized to refugees in a couple of ways. Recruitment in this study was restricted to one language group with a predominantly secure visa status. While it is important to note that a large proportion of the world's refugees are displaced from Arabic-speaking countries (Vogel et al., 2024), and Arabic-speakers are generally collectivist, as is the case of most cultures of refugee populations (Minkov & Kaasa, 2022), the highly specific sample does limit the extent to which findings can be generalized to the refugee population in general, given the diversity of cultural backgrounds and given that the majority of refugees are not resettled (UNHCR, 2024). It is also the case that participants in the present study may have some propensity towards help-seeking given that they volunteered to participate in a research study regarding mental health. This represents an important challenge of the field more broadly whereby the effects of stigma (such as reduced help-seeking) are likely to affect engagement with research investigating stigma. Therefore, the very people who the studies were designed for (i.e., those with high stigma preventing help-seeking) are unlikely to be captured. Future research could reconcile this by embedding stigma and outcome measures in mandatory service provision surveys to measure these associations in a more ecologically valid sample. This could additionally serve the purpose of alerting mental health practitioners if a consumer is at risk of drop-out. Secondly, the cross-sectional study design precludes conclusions about temporal order and causation. This provides an avenue for future research, as studies may benefit from using longitudinal data to explore the nature of these relationships across time. Finally, the current study focusses on PTSD given that traumatic events are often encountered in the context of war and persecution, as experienced by refugees. However, cumulative trauma and forced displacement can result in mental health difficulties beyond PTSD causing high comorbidity with depression, anxiety, and psychosis (Fazel et al., 2005). The present study did not include an analysis investigating the influence of other mental health symptoms on the association between self-stigma, mechanisms, and outcomes. Since it is likely the case that various symptom profiles would impact the associations observed, future research would benefit from replicating results using broad measures of distress—while this may be less specific than a disorder-based approach, it would likely be more representative given the prevalence of comorbidity.
Conclusion
The current research represents the first study to investigate the potential mechanisms underlying self-stigma, a prominent barrier to social engagement, in a refugee sample. Findings underscore the importance of targeting self-stigma to increase social engagement, specifically, to help refugees feel connected to informal support and facilitate engagement with formal support. The findings also suggest that hope and negative help-seeking beliefs may be viable intervention targets to reduce self-stigma and facilitate increased social engagement to support recovery in refugees.
Supplemental Material
sj-docx-1-tps-10.1177_13634615251348300 - Supplemental material for Mechanisms underlying the impact of self-stigma on social engagement in Arabic-speaking refugees: A path analysis
Supplemental material, sj-docx-1-tps-10.1177_13634615251348300 for Mechanisms underlying the impact of self-stigma on social engagement in Arabic-speaking refugees: A path analysis by Natalie Mastrogiovanni and Angela Nickerson in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors would like to thank all participants for their contributions to this study.
Author contributions
Data availability statement
The dataset generated and analysed in the present study is available from the corresponding author on reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The AN was supported by an Australian Health and Medical Research Council Leadership Fellowship.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.