
Abstract
Implementation of community mental health in Indonesia has been limited and under-resourced. Pasung (physical restraint and confinement) is still commonly used and many people do not receive formal mental health care. While pluralistic use of traditional and faith healing and psychiatric services is common, the relationship between the two systems is ambiguous and overlooked in mental health policy. Meanwhile, examples of collaboration between health professionals and traditional and faith-based healers (TFHs) for mental health exist in various settings, including Indonesia. However, there is limited research on the lived experiences and everyday practices of those engaged in such partnerships, including mental health workers, healers, and families, and what makes them successful. This paper presents findings from the visual research project ‘Together for Mental Health’ to illustrate the facilitators and barriers to pluralistic collaborations in the Indonesian context. Our focus was on partnerships that were already established, rather than those implemented as part of research projects or interventions. Using visual ethnography, we observed eight case studies in locations representative of the three main religions in the country: Java (predominantly Muslim), Bali (Hindu), and Flores (Roman Catholic). We conducted filmed ethnographic observations of collaborative practices and in-depth interviews with 20 mental health professionals, 12 TFHs, 28 people living with mental health conditions, and 16 caregivers. The study found converging themes related to facilitating factors and barriers in practices of pluralistic collaboration for mental health care in Indonesia. Facilitating factors included actors’ role perception and motive, openness to collaboration, and negotiations of care. Barriers included negative role perceptions, inadequate infrastructure, and unfavourable social environments. Findings suggest potential for successful collaboration between TFHs and formal mental health practitioners, drawing on lessons from existing good practices. To support future pluralistic collaboration for mental health care, incorporating these lessons into professional education and policies and stronger mental health care governance are needed.
Keywords
Introduction
Indonesia is in a long-term intertwined crisis of mental health and human rights. According to the World Bank Global Burden of Disease, the years of life lost to disability due to mental disorders in Indonesia are greater than the total of those lost to ischemic heart disease, cerebrovascular disease, diabetes, and tuberculosis (Mboi et al., 2018). Pasung, the local terminology for physical restraint and/or seclusion of people with mental illness, is still a frequent practice (Colucci, 2023; Hidayat et al., 2020; Yunita et al., 2020). Based on the 2018 Indonesian Basic Health Survey, approximately 280,000 households (7%) have at least one family member living with psychosis. Of these, 14% have practised pasung (Badan Penelitian dan Pengembangan Kesehatan, 2019). Many people subjected to pasung suffer from long-lasting muscular deterioration from immobility, as well as psychological consequences and further mental health decline (Anto & Colucci, 2015; Colucci, 2023).
‘Bebas Pasung’ (the ‘Free from pasung’ campaign) was a powerful driver for a new Mental Health Law ratified in 2014 (Hunt et al., 2023). In 2023 this law was replaced by the Omnibus Health Law No. 17, which covers both mental and physical health. The Omnibus Health Law introduces fines and imprisonment for those using pasung (UU no 17 2023). However, enforcing criminal sanctions is difficult because frequently pasung is a communal decision to restrain someone considered a danger to themselves or others (Anto & Colucci, 2015; Colucci, 2023; Minas & Diatri, 2008) and occurs in the context of an under-resourced mental health system, which is unaffordable, ineffective, and inaccessible to many (Colucci, 2016; Read & Colucci, 2023). It is also complicated by the widespread use of traditional and faith-based healing in lieu of, or in combination with, the formal health system. As well as families and community members, pasung is practised by many healers and also by some health workers (Human Rights Watch, 2016; Hunt et al., 2023).
The mental health system in Indonesia
Indonesia's formal mental health system has evolved from centralised, racialized, and class-based institutional care (Porath, 2008) to community-based mental health care integrated into primary care (Good et al., 2019). The 2014 Mental Health Law stated that mental health services should be de-centralized and provided through community health centres (Puskesmas). This policy is further emphasized in the new Omnibus Health Law 17 (UU 17, 2023). However, despite these policy commitments, implementation of the mental health programme continues to be under-resourced. There are 3,605 registered clinical psychologists (Indonesian Clinical Psychologists Association, 2023), 1,221 psychiatrists (Sitohang, 2022), and 14,760 mental health nurses (Sitohang, 2022) in Indonesia serving a population of 270 million people. Less than 1.5% of the 2019 Ministry of Health budget was allocated for mental health, most of which was spent on hospital-based services (Maramis et al., 2011). Less than half (46.18%) of all puskesmas run mental health programmes (Sitohang, 2022). Treatment for most mental illnesses is covered by the National Health Insurance (JKN), however this is primarily through medication. More recently, there has been recognition of the potential of allied health and social care professionals, such as psychologists and social workers, to provide more holistic community mental health care, with psychologists posted to work at puskesmas in some areas (Anjara et al., 2019; Setiyawati et al., 2014). However, progress is slow, and provision varies depending on each district's budget.
Medical pluralism in Indonesia
Globally, research shows widespread co-utilization of formal mental health services and traditional and faith healers (TFHs) (Cant, 2020; Green & Colucci, 2020; Hunt et al., 2023; Liem, 2020; Suryani et al., 2011). Healing pluralism refers to “situations where people may choose – or, particularly in mental health (where mental capacity to make decisions may be called into question), may have choices made for them – from a range of coexisting therapeutic options” (Orr & Bindi, 2017, pp. 307–308). In Indonesia, studies have shown that up to 70% of the population make use of TFHs (Febriyanti et al., 2024). However, there are differences between urban and rural populations, reflecting differences in availability and access to health services (Mulyanto et al., 2019). Where formal mental health services are available, these may be used either sequentially or alongside religious or spiritual treatments (Good et al., 2019; Marchira et al., 2016). In addition, perceptions of mental illness are shown to have changed over time. While spiritual understandings remain important, mental illness is also commonly associated with psychological factors, such as stress and trauma (Subandi et al., 2021). For many Muslims in Indonesia, particularly among those with more formal education, shamanistic healing may be avoided as conflicting with Islamic teaching, but prayers and Islamic treatments such as ruqyah are valued (Anjara et al., 2021; Subandi et al., 2021). Studies often fail to differentiate between these diverse forms of traditional or faith-based treatment. The Indonesia Family Life Survey 2014–2015 reported that among respondents with emotional, nervous, or psychiatric problems, 20.9% accessed biomedical mental health services, and 5.6% sought help from ‘traditional medicine,’ including shamans or those locally known as ‘wise men’ Chinese herbalists, masseurs, and acupuncturists. However, there was no specific reference to faith-based forms of healing, such as Islamic, Hindu, or Christian practitioners, so it is unclear if these were included (Pengpid & Peltzer, 2018). A more recent survey showed that 35.2% of participants chose formal mental health services to address mental health problems, while 3.1% preferred non-medical traditional therapies (Into the Light Indonesia, 2021).
Partnerships between mental health workers and TFHs have received renewed interest in global mental health in recent years (Green & Colucci, 2020; Gureje et al., 2015; Read et al., 2023; Solera-Deuchar et al., 2020). Research suggests that such collaborations may prevent harmful practices, improve access to care, and address spiritual and social needs (Gureje et al., 2020; Yaro et al., 2020). However, Green and Colucci (2020) highlight that a collaborative approach is often deemed to be contingent upon traditional healers’ ability to adhere to principles of “scientific rigour” and “evidence-based practices” (p. 10). Professionalization, training, and regulation of traditional and faith healers have been proposed to prevent harm (Yaro et al., 2020) but can reinforce hierarchies between biomedical and healing practitioners (Pham et al., 2021). Power dynamics, conflicting epistemologies, and lack of resources may all impact the success of collaborative practices (Gureje et al., 2020; Kpobi & Swartz, 2018; Read et al., 2023). Overall, despite the growing research in this field, there remains limited evidence on how such collaborations are practised in diverse contexts.
In contrast to other parts of the world, such as Ghana (Kpobi et al., 2023; Kpobi & Swartz, 2018; Read, 2019), action to support collaboration between healers and health workers in Indonesia is limited. For instance, while Viora (2019) outlines the rich variety of traditional, faith-based, spiritual, and indigenous healers in Indonesia, they are absent from her discussion on the way forward for community-based mental health care. The 2014 Indonesian Mental Health Law acknowledged the presence of non-biomedical care providers (Article 55) and suggested that they should collaborate with formal health services (Article 56). The Omnibus Health Law No. 17 explains that traditional medicine is provided by herbalists and/or skilled traditional medicine practitioners. The 2018 Health Minister Regulation on the Implementation of Complementary Traditional Medicine defines traditional medicine as “medicine and/or care using means and medications which refer to experience and inherited skills which are empirically accountable and according to the applicable norms in the society” (Menteri Kesehatan Republik Indonesia, 2018, p. 3). Under this legislation, local regency and city governments are tasked with registering and issuing permits for traditional healing facilities. However, traditional medicine is narrowly defined in the legislation as an approach that “makes use of biomedical and biocultural knowledge in its explanation, and its benefits and safety are proven scientifically” (Menteri Kesehatan Republik Indonesia, 2018, p. 2).
Implicit in this statement is the supremacy of biomedical knowledge and scientific evidence as the benchmark for other healing practices. While such policies claim to value the contributions of indigenous and spiritual knowledge and practices, too often regulation reinforces hierarchies between healers and health workers, which can increase distrust (Read et al., 2023). Spiritual experiences are devalued as ‘unscientific’ and the diversity of healing approaches discounted. As Pigg (1995) observed in Nepal, the incorporation of healers into health policy can often efface the valued spiritual, cultural, and social aspects which make them effective. More recently, Thomas Csordas (2023) has pointed to the ongoing tensions in global mental health between rights-based arguments for improved access to mental health services and those who believe that the expansion of such services may undermine indigenous approaches to healing and recovery. These arguments ironically tend to reinforce a dichotomizing view of spiritual and psychiatric approaches as fundamentally incommensurable. As argued by Kong et al. (2023), “the performance of identity and power dynamics in a competitive healing economy can lead to the emphasis on, or even exaggeration of, difference between practitioners of psychiatry and faith-based healing” (p. 2). To bridge the polarity between concerns with ‘efficacy,’ often narrowly defined, and lived experience, Csordas (2023) calls for an “elaboration of the empirical ethnographic knowledge base on what actually transpires in indigenous healing” (p. 444). Dialogue across different approaches to healing may lead not only to successful collaboration but to a richer and more inclusive understanding of mental illness and recovery (Baheretibeb et al., 2022; Kong et al., 2023; Read, 2019).
‘Together for Mental Health’ was devised as an interdisciplinary visual research project to explore attempts at developing collaborations for mental health care in Ghana and Indonesia, taking account of the diversity of healing practices and health systems both within and across the two countries, and the lived experiences of those engaged in such collaborations, as mental health workers, healers, and people receiving treatment for mental illness and their families (see https://movie-ment.org/together4mh). This paper, which complements the article reporting on research in Ghana (Kpobi et al., 2023) and the accompanying ethnographic film (Colucci, 2021a), explores how relationships between diverse healers, health workers, and families were developed in different locations in Indonesia in the context of epistemological tensions and resource constraints, and how they sought to address these and other barriers to collaboration. In contrast to studies that show how such collaborations were implemented within specific time-limited research interventions (Gureje et al., 2020; Ofori-Atta et al., 2018), we employed visual ethnography to follow pre-existing, locally established collaborations between healers, health workers, and families to understand the values, practices, debates, and compromises that made such collaborations possible in different contexts. Our research is thus focused on what Abimbola (2019) has termed ‘organic’ change, driven by internal processes over time, rather than on ‘surgical’ change, often implemented by external agents.
Methodology
Visual ethnography
Indonesia is a diverse archipelagic nation of over 270 million people, with more than 700 languages (Cant, 2020; Ministry of Education and Culture, 2019) and marked variance in political and economic conditions and cultural traditions. The ethnographic documentary approach implemented built on the methodology developed for the visual research project ‘Breaking the Chains’ (Colucci, 2016, 2023; https://movie-ment.org/breakingthechains/). Filmed field observations and interviews with persons with experience of mental illness and coercion or restraint, family carers, healers, mental health workers, and other key stakeholders were conducted in five geographically and culturally diverse locations in Indonesia. These were edited into an ethnographic documentary, Harmoni: Healing Together (Colucci, 2021a), accompanied by other case studies-based short films and a screening guide. 1
Data collection
Study sites and cases were purposefully selected to capture a wide range of collaborative partnerships drawing on different epistemological approaches and healing traditions. In identifying the case studies, the researchers consulted with mental health experts in Indonesia. In addition to receiving recommendations from existing networks, the study team also organized two consultative meetings with a National Advisory Committee composed of 16 policymakers, advocacy groups, and practitioners. Based on these suggestions, between October 2019 and January 2020 the research team in Indonesia (EC and AWP in all sites, with DS and WNJ in Yogyakarta) explored collaborative practices in communities where the three major organized religions are dominant: Islam in Java (Cianjur and Yogyakarta), Roman Catholicism in Flores (Manggarai and Sikka), and Balinese Hinduism in Bali (Denpasar). As described in our study in Ghana (Kpobi et al., 2023), we conducted filmed observations of interactions between mental health professionals, families, and caregivers, people with lived experience of mental health issues, and TFHs. We also filmed healing sessions and rituals within places of worship and community settings, interactions between mental health professionals and families, and daily routines of mental health professionals, healers, people with lived experience, and caregivers (including an NGO run by carers and people with lived experience). We also conducted filmed interviews with 20 mental health workers, 12 healers, 16 family caregivers, and 28 people receiving treatment for mental health conditions from healers and health workers. In addition to the filmed activities and interviews, notes were kept to record field observations. These three sets of data form the basis of this article.
The healers in the study came from varied Islamic, Hindu, and Roman Catholic traditions. Various terms are used to describe Islamic teachers or leaders. Kyai is used specifically to refer to the head of an Islamic boarding school (pesantren). In Balinese Hinduism, healers are referred to as Balian. In Flores, participants were Roman Catholic priests involved in Charismatic healing and faith-based rehabilitation and support services. Dukun are healers who use methods such as written Qur’anic passages as amulets, but many Indonesian Muslims consider this incongruent with Islamic principles. None of the participants identified as dukun, but dukun were mentioned many times in the interviews by participants. For more detailed information on the case studies for the filmed observations and interviews, see Supplementary File 1.
Ethics
The study received ethical clearance from Universitas Gadjah Mada (Ref: 4055/SD/PL.03.01/X/2018) and Middlesex University Psychology Research Ethics Committee (Ref: 5153). The study employed a staged consent process whereby the participants’ approval was acquired before data collection commenced and rechecked before each period of filming, detailing the level of anonymity they required, for example whether or not they wished to disclose their name, show their face, use their voice, etc.
Data analysis
The data was analysed using reflexive thematic analysis (Braun & Clarke, 2022) and informed by consistent reflection on our political, ideological, religious, and philosophical perspectives to take into account how these might influence our interpretation of the findings. All the researchers in the project are women. The researchers who conducted data collection in Indonesia come from health professional backgrounds (EC, DS, and WNJ from psychology and AWP from medicine). DS, WNJ, and AWP are Indonesian and belong to the dominant Islamic community. EC, who led the Indonesian data collection, is Italian, was brought up in the Catholic religion, and has almost two decades of research experience in Indonesia. UMR devised the research project with EC and analysed the data with EC and the Indonesian team. She is White British, was brought up within a Protestant religious group in the UK, and worked in UK mental health services as an occupational therapist before training in anthropology.
Video recordings of conversations and interviews were transcribed verbatim in the original languages (Bahasa Indonesia, Balinese, Sundanese, and Manggarai) and translated into English. Initial data analysis of the transcripts, visual footage, and fieldnotes occurred immediately after the visual data was collected to develop a thematic framework to guide the research film editorial process. Following this, systematic coding of the interview transcripts was conducted by the researchers (EC, DS, and AWP) using NVivo 12. The initial themes were refined and additional themes developed through an iterative and comparative process, triangulating findings from the fieldnotes, film footage, photographs, and observations. Findings were discussed and compared with the wider research team across Indonesia and Ghana, and the themes were further refined. Major themes were developed around the facilitators and barriers to collaboration, informed by the research questions. Subthemes were developed inductively from the data, illustrating various ideological and pragmatic motivations for collaboration (see Figure 1).
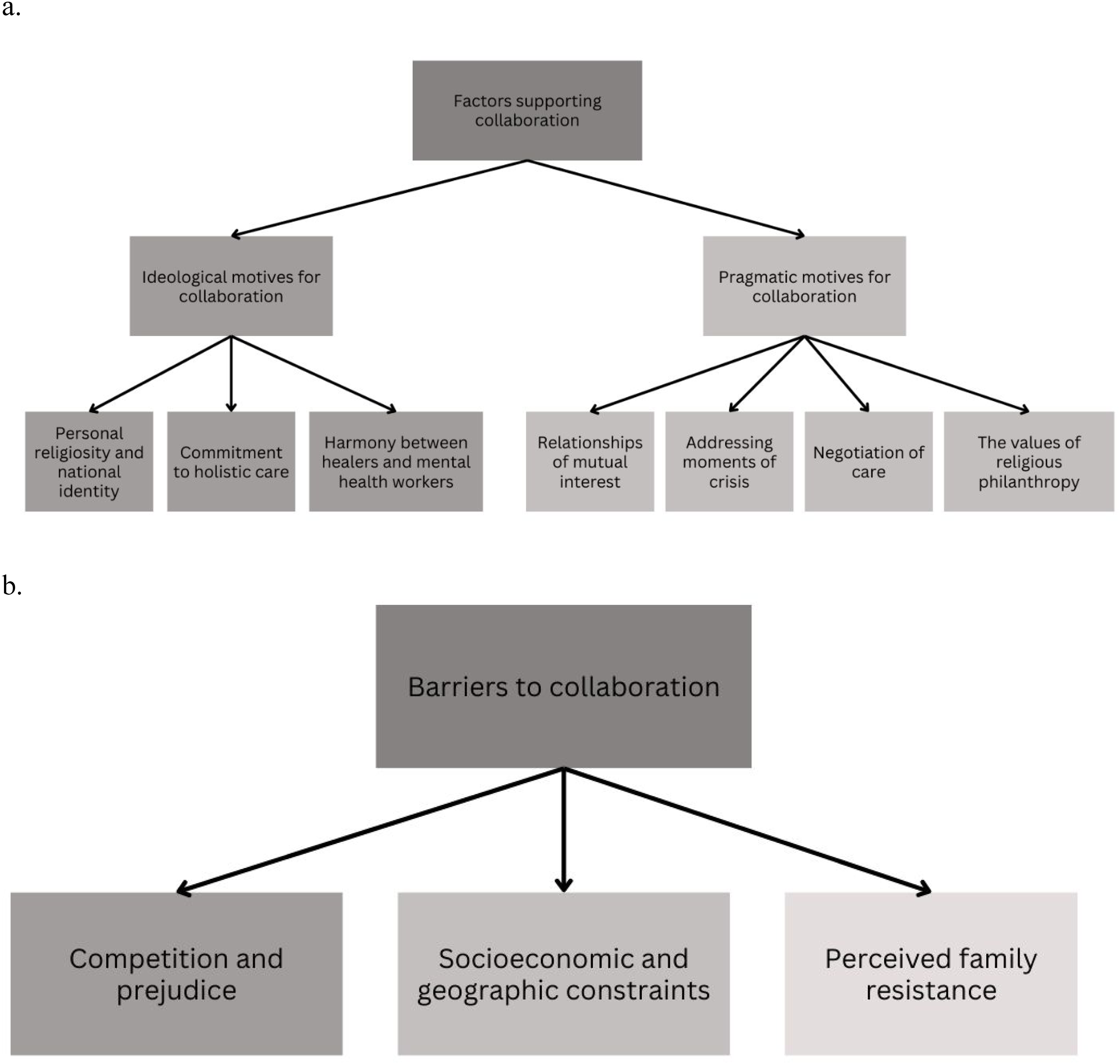
Theme mapping of a) facilitating factors and b) barriers of pluralistic collaboration in mental health care.
Results
Factors supporting collaboration
Ideological motives for collaboration
Personal religiosity and national identity
Despite the clear policy distinction between evidence-based mental health treatment and traditional or faith-based approaches, religion and spirituality were infused into the practices of mental health workers, influencing their values and worldviews as well as their approach to collaboration with healers. In this sense, spirituality was not seen as incommensurable with biomedically or psychologically informed mental health care, but rather as foundational to national and personal identity and values.
Nurhamid is the founder of a peer-led mental health rehabilitation shelter and NGO, Istana KSJ, in Cianjur (West Java) and caregiver to a family member living with mental illness. Nurhamid grew up as a devout Muslim and was active in a local religious study group. He declared that the values of his Muslim faith inspired his decision to dedicate himself to providing care and protection to people with mental health conditions: “We have religion as our principle. At the end of prayers, we recite Salam (greetings/peace), Rahmat (mercy), and Barokah (blessing). The consequence for people who pray is a loving way of life, which starts from protecting each other.”
2
The concept of ‘Pancasila’ is the ideological foundation within the national constitution of Indonesia, consisting of five principles referred to as ‘sila.’ Under Pancasila's first principle of theism, ‘belief in the one and only God,’ Indonesian national identity is deeply rooted in a spiritual-religious worldview. This shared commitment serves as the foundation for collaboration between health professionals and faith-based healers, regardless of their specific religious affiliation. Brother Honorius, a psychiatric nurse and priest in the Catholic Church in Manggarai (Flores) who works in Renceng Mose, a rehabilitation centre for people with mental illness and substance abuse, reflected this orientation when he stated (Figure 2): Indonesia counts as one of the religious countries, right? Religious … where the society is not alien from the world of faith. There is ‘Belief in the one and only God,’ and so on. So, [the perspective] that we try to build in [Renceng Mose] is still the general [perspective] in the general society. [My fellow doctors] will agree [with] collaborating with dukun, the traditional healers, the prayer groups, in managing cases of mental illness. Why? Because we—the doctors, paramedics, nurses, midwives—are also the product of, or were born in, Indonesia, in a culture with very high levels of mysticism and spiritual belief. It would be a lie if they did not feel that there should be a collaboration between the medical and spiritual fields! It would be a lie if they rejected that! Because we are born and raised in a world or in an environment like this.

The Catholic congregation attending a mass led by Father Ompy, after which he performs charismatic blessings of members of the congregation with items such as water, salt, religious trinkets, and herbal ingredients (Colucci, 2021a).
Prof. Suryani, a Hindu psychiatrist in Bali, who integrated spiritual practices such as yoga and meditation into her clinical practice, stated that almost everyone she has encountered in her long career, including herself, “believes we have a soul” that controls the mind and body. This informed her commitment to healing for the “mind-body-spirit” as congruent with “Balinese culture”: What I have seen in my patients is that they are Balinese with Hindu faith with their Balinese culture. Therefore, I will use the concept ‘mind-body-spirit.’ Because in Bali, the faith is that everybody has a spirit, roh [soul], atma, or whatever the name is. These spirits rule our mind, and our bodies. It is not the mind that is the highest, in the Balinese concept! It is the spirit, soul [roh], atma, or whatever the name is.
Commitment to holistic care
This approach to ‘mind-body-spirit’ in healing aligns with the bio-psycho-socio-spiritual approach to mental health, also termed the integrative mental health (IMH) care paradigm (Lake et al., 2012). This holistic paradigm was specifically alluded to by some mental health care professionals. For example, Dr. Warih, a Muslim psychiatrist practising in Yogyakarta, Java, stated: I personally think, aren’t humans holistic? So, the bio-psycho-socio-spiritual approach is certainly [what] every patient needs. So, when a patient asks, “Can we go to ruqyah, can we go to healers, other alternative healers?,” of course we view that—for instance they go to the kyai or to ruqyah—of course! Usually I motivate them this way: “Even [for] people with physical illness, [when] they get support, spiritually, they get better.”
Furthermore, this holistic approach is formalized within both the 2014 Mental Health Law and its successor the 2023 Omnibus Health Law, as well as in mental health policy. In the Omnibus Health Law, for example, health sectors are tasked to follow the principle of balance between individual and public needs, physical and mental health, as well as material and spiritual aspects. Alongside the principle of Pancasila, this further legitimizes mental health practitioners’ openness to integrating spirituality into their practice and working in collaboration with faith-based healers.
Harmony between healers and mental health workers
Consistent with this openness to a holistic approach, mental health practitioners who were engaged in collaboration with healers deliberately minimized any differences and instead emphasized points of similarity. Dr. Rai, a psychiatrist in Bali who collaborated with Hindu leaders and traditional healers in Bali, including Komang Gases, a Hindu healer, artist, and scholar, stated: I think the key to the success of collaboration is, firstly, we started to move from the same side. We looked for similarities in what we want to do. Whether it is me from a psychiatric approach, or Komang Gases from a cultural [approach], or Mpu Acharyananda [Hindu high priest / sulinggih] and Jero Mangku Dodi [a Hindu priest] from a religious [approach], but we started from the similarities. We did not seek differences. We look for similarities. Even if there is any difference, we don’t talk much about it.
Dr. Rai described how he sought to achieve ‘harmony’ by uniting seemingly opposing Balinese-Hindu concepts of the visible and invisible: I would use the phrase ‘sekala-niskala’ [the visible-the invisible]. Actually, in Balinese Hinduism, the key is harmony. We don’t negate each other. Not all religious figures, not all pemangku [Hindu priests] and Balians understand the collaboration that we do. [They think we are] trying to change tradition, trying to combine knowledges that they think actually cannot be combined or that we try to turn everything that is ‘niskala’ [invisible] into ‘sekala’ [visible], whereas we are trying to harmonize them.
In this approach the aim is not to ‘scientize’ niskala (the invisible/metaphysical realm) and incorporate it into the biomedical approach (as for example in the common reduction of traditional healing to psychological or social effects), but rather to ‘harmonize’ these different ontologies on their own terms, using one to enrich the other. The primacy of harmoni (harmony) as a cultural value in Indonesia is created and sustained through emphasizing togetherness and avoiding conflict.
Pragmatic motives for collaboration
We found two main forms of collaborative relationships: referral (health professionals and TFHs refering to each other's facility) and space sharing (health professionals and TFHs sharing their practices in one facility). For example, the referral relationship was implemented in Yogyakarta between Ustadz Fadhlan (an Islamic healer) and Dr. Warih (a Muslim psychiatrist), while the space sharing was observed in Al-Islamiy Rehabilitation Centre in Yogyakarta where the medical doctor and the religious healer worked together in the same building.
With the foundation of positive personal and religious motivations and openness described above, the formation of these collaborations was predominantly built on relationships of mutual interest between religious practitioners and mental health practitioners, exploiting moments of crisis, and negotiation of care and philanthropism.
Relationships of mutual interest
Some collaborations arose through relationships that were established in the course of clinical practice. For example, in Bali Dr. Rai, a motivated psychiatrist, developed a friendship with one of his patients, Dodi. Dodi is a young Balinese priest who runs training workshops for the local association of religious leaders in Denpasar. Their rapport grew beyond the initial patient–doctor relationship into a collegiate relationship, where Dodi involved Dr. Rai in his workshops, introducing him to Balinese faith-based healing practitioners such as Komang Gases. Komang Gases reminisced fondly about the start of his personal relationship with Dr. Rai which he described as a meeting of minds: When I met Dr. Rai, it was because we were holding a seminar. When I kept meeting him—I held a seminar once, twice, three times, until several times—“This is good! We match …” In the Balinese term, Menyama Beraya [we are family]. There is exchange of minds or sharing.
Similarly, Dr. Ronald, a medical doctor, and Father Ompy, a Catholic priest in Manggarai, Flores island, initially had a patient–doctor relationship when Father Ompy consulted Dr. Ronald for his physical illness. Dr. Ronald was very keen to engage faith-based practitioners who interact on the frontline with people living with mental illness. Meanwhile, Father Ompy's reputation in the local community as a charismatic Catholic priest was well known. From their relationship, Father Ompy became more familiar with Dr. Ronald and the Brothers of Charity's (Bruder Karitas) work in Renceng Mose Mental Rehabilitation Centre. During the weekly mass, where Father Ompy performed charismatic healing, he became more aware of his congregants who needed professional mental health care and provided recommendations to seek treatment from Renceng Mose clinic. The reciprocal openness to working together for a shared goal made it possible for these personal relationships to become the basis for broader organizational or institutional networks (Figure 3).

Multidisciplinary panellists at a seminar on the topic of kerauhan (trance). From left to right: Mahendra, a former hypnotherapy practitioner, Dr. Rai, a local psychiatrist and founder of the community mental health centre Rumah Berdaya, Dr. Komang, a Balinese culture scholar, performing artist, and community religious leader and healing practitioner, and dr. Fridari, a transpersonal psychology practitioner, scholar, and lecturer at Udayana University (Colucci, 2021a).
Addressing moments of crisis
Collaborations were also established at moments of crisis. Faith-based healing practitioners often encounter crises when patients are endangering themselves or others or have communication difficulties (Colucci et al. 2022; Prastyani et al., 2020). In these incidents, faith-based healing practitioners were faced with their own limitations and were motivated to seek assistance. Health professionals and their allies who welcomed such requests for assistance in a respectful manner effectively transformed moments of crisis into opportunities to build collaboration.
In parallel, health professionals may also find crises in their practice when patients stop their treatment. Dr. Warih supported her patients’ decision to receive Islamic healing services, however she was concerned that some Islamic healers might not permit their patients to receive medical treatment whilst undergoing ruqyah. She explained her concerns: The hope was for [the patients] to receive spiritual therapy to strengthen our therapy, with an awareness that the biological condition [of the patient] was still [treated] using pharmacotherapy. But [treatment] was stopped, because of the ruqyah practitioner's lack of understanding about mental illnesses and about pharmacotherapy.
However, she saw an opportunity for collaboration when an Islamic healer her patient used, Ustadz Fadhlan, was open to having a dialogue with her. This was the beginning of a relationship between them. Dr. Warih described how she sought to educate Ustadz Fadhlan on the need to continue patients on medication to ‘stabilize the neurotransmitters’ whilst also receiving Islamic treatment: Now, eventually, there was a chance to communicate with the ruqyah practitioner. I explained that, in mental illness, the medication is not just to put [the patient] to sleep but to restore the chemicals in the central nervous system—the neurotransmitters. If they were not stable yet, they would still need the medication to stabilize the neurotransmitters, and the medication should not be stopped just yet.
Negotiation of care
Dr. Warih's approach also illustrates the ways in which mental health practitioners negotiate with healers on different approaches to treatment. The research team observed negotiations in the delivery of psychiatric treatment to take into account potentially harmful interactions with faith-based healing approaches.
As with Dr. Warih and Ustadz Fadhlan, the most frequently negotiated practice in collaboration was around the use of psychiatric medication. Healers expressed concerns about the effects of medication and its impact on the patient's ability to undertake religious rituals. Meanwhile, psychiatrists were concerned that if patients discontinued medication to undertake religious treatment, they could relapse. As we observed Ustadz Fadhlan conducting a ruqyah therapy with a client at home, he expressed his concern about her inability to respond and concentrate during the ruqyah session due to the effect of the medication on her ‘consciousness’: I have performed ruqyah [for her] once [before], I met her at her house. And then, her condition had not changed, and she was taken to a mental hospital. After four months of care there, she stayed there. [When] she came home, no change yet. It turns out, when the ruqyah was performed yesterday, she was still taking medications from the psychiatrist. So, her consciousness was impaired.
Many psychiatrists would react defensively against healers who persuade patients to stop their medication. Instead, Dr. Warih was able to negotiate for the patient to be off medication for one day before ruqyah therapy: “Perhaps, when ruqyah is to be performed, the medication can be ceased, so they could focus during the ruqyah. After that, take the medication with adjustment, so they do not become counterproductive by stopping the medication.”
This flexibility to negotiate and compromise on the timing of medication addressed the concerns of ruqyah practitioners while also enabling patients to receive medical and spiritual treatment in parallel without any undesired interactions. Importantly, despite her ‘education’ for the healer on the effects of psychotropic medication, Dr. Warih's approach also took the Islamic healer's practice seriously, recognizing the conditions needed for it to succeed on its own terms, that is for the patient to not be sedated and to be consciously present.
Over time, some faith-based practitioners grew familiar with the medications given to their clients by psychiatrists and gained experience and formed opinions about them. For example, we observed a conversation between Father Andi, a Catholic priest, and Dr. Fatimah, the only practising psychiatrist in Flores, during a rural outreach service to visit families at home. Father Andi observed that, despite the patient taking medication for over a year, he had seen little effect and so queried whether it should be changed (Figure 4): This patient is the patient that we have released. He has been under medication for so long, but it seems the medicine doesn’t work. (…) After five times we approached him – we [kept giving] the medicine—he agreed. But until now, [the medicine] seemingly doesn’t work so well. It's [been] more than a year already. Now we are going to assist, what happens [next]? Do we need to change the medicine, or do we need to take [an]other approach?

Father Andi and Dr. Fatimah were visiting a patient in rural Sikka, Flores Island, who was living in a Rumah Aman, a house made of iron bars and bamboo walls, specifically built for people living with mental illness, particularly those who were in pasung (Colucci, 2021a).
Just like community-based mental health workers or community health cadres (volunteers coordinated by Primary Health Care clinics), many of the faith-based practitioners become close to the community they serve. Because they have followed their clients’ treatment over time, faith-based practitioners felt confident to raise concerns with health professionals about psychiatric medications and provide feedback on the effects they observed firsthand. This practice-based evidence gained from grassroots experience with families in the community helped to break down the hierarchies between medical and religious practitioners and create a more equitable relationship of mutual learning and respect.
The value of religious philanthropy
In the context of limited resources for mental health care, religious groups are also valued, not only in terms of their spiritual contribution but also for their readiness to provide practical support, ranging from manpower to providing housing and financial donations. These philanthropic activities are grounded within religious teaching as an act of worship and as a means of acquiring blessings or virtue. In Cianjur (West Java), support from a local Islamic charity was instrumental to the survival and operation of Istana KSJ, as described by a donor: When I [first] visited [Istana KSJ], it was extraordinary to witness Pak Nur's [Nurhamid's] determination to care for people with mental illness, with such a meagre setting. His house was small, a rented [property]. How many people were there then? Fifty to 60 people, at the time. (…) I had the initiative to talk to Bu Tika [social worker and member of an Islamic charity], also with Pak Nurhamid. I said, “Pray for me, hopefully there will be a better, more decent place.” We humanize them, we help them, we medicate them.
This bringing together of religious philanthropy and mental health practice strengthened both sides’ perception of uniting in a joint endeavour inspired by shared values and brought in much-needed resources, particularly to address psychosocial needs such as housing and social support.
Such religious charity was also prominent in Flores, where Catholic Camillian priests raised funds to build over 30 houses specifically for people living with mental illnesses who were previously in pasung. They also paid for health insurance for people with mental illness. As one of the priests, Pater Andi, explained: We decided that we will give everything we can. We work also to [provide patients with] a national ID card and a social [health] insurance card to rely on when they get sick again. Most of our patients, when they get sick, they cannot pay, because most of them are not registered.
Local health professionals also rely on the priests’ contribution to supply medication, given the scarce supply within the formal health system.
Barriers to collaboration
Although we identified several facilitating factors as described above, there were also barriers that limited collaboration. We identified three key barriers: competition and prejudice between and within healers and mental health practitioners, resource constraints, and perceived family resistance to psychiatric treatment (Figure 5).
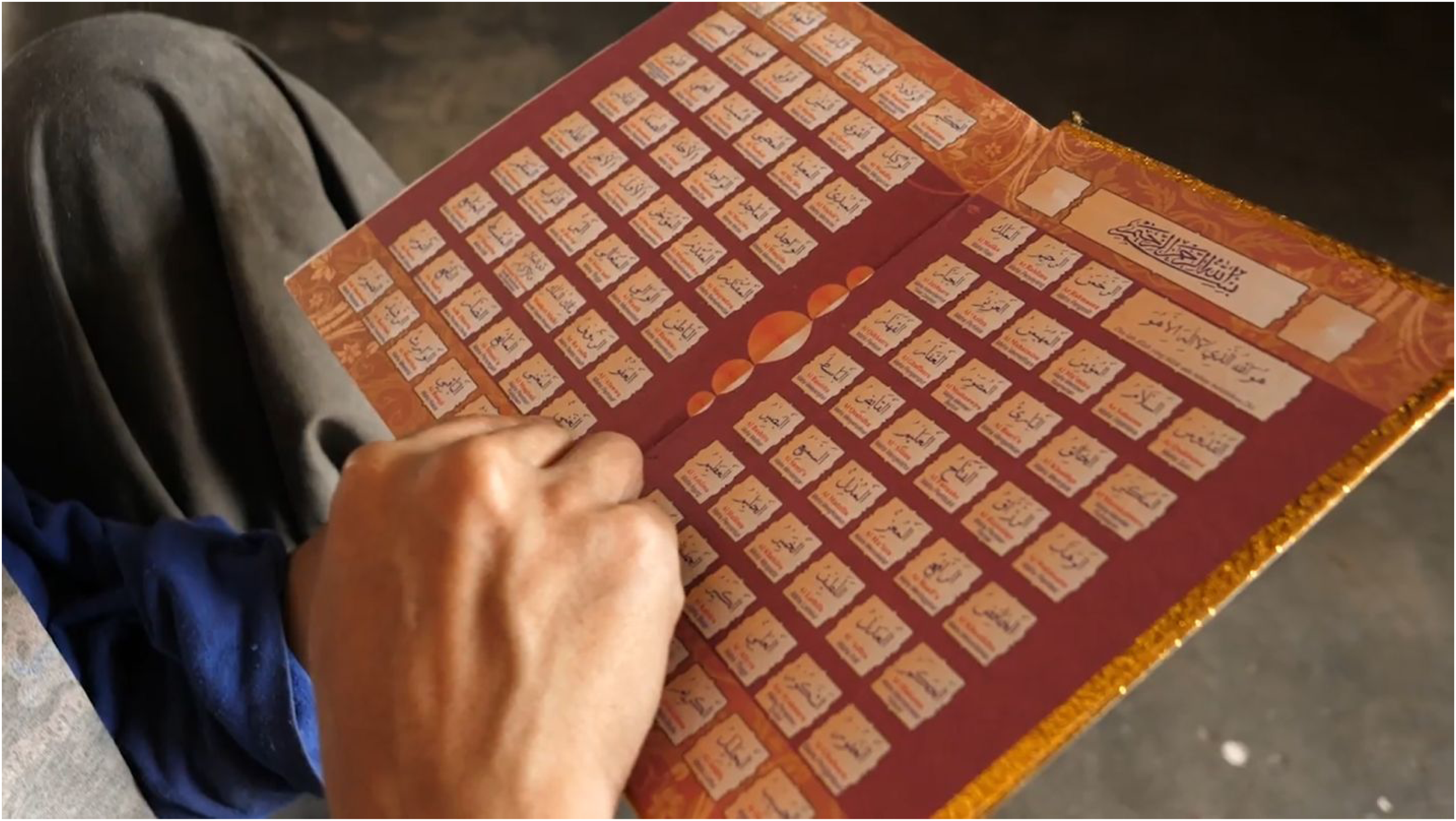
A resident of the mental rehabilitation wing of pesantren Nurul Haromain reading the Al Asma ul Husna, or the 99 Names and Attributes of Allah. Apart from reading the Qur’an or watching television, there is little to no other activity available to fill the residents’ leisure time (Colucci, 2021a).
Competition and prejudice
Remarks that reflected a view of the superiority of a particular healing epistemology and competition and scepticism between different healers were common, consistently with other reports (Green & Colucci, 2020; Kpobi & Swartz, 2018; Read, 2017). For example, one Islamic healer from Yogyakarta declared that the impact of medical treatment was temporary, whereas religious therapy could bring a lasting cure: “For medical [treatment], it's also good, actually, but it's only temporary. Meaning, healing only [occurs] for several hours but after several hours, they would relapse again.” Other study participants commented on the competitive atmosphere between practitioners. As Komang Gases mentioned: “There are also [practitioners] that become oppositional! The ones who refuse [to collaborate]. Why? Well, it goes back to ego, feeling ‘I am the greatest’ … and so on.”
There is also prejudice towards other practitioners’ motivations. This prejudice is not found exclusively between medical and faith-based practitioners but also between different faith-based healers. Some Islamic healers refused to be associated with ‘commercialized’ ruqyah practitioners, who they viewed as acting against Islamic practice. Such conflicts also existed between fellow health professionals. Psychiatrists with an unconventional approach, including those collaborating with faith-based healers, sometimes faced subtle or even overt criticism from their colleagues. Prof. Suryani reported that colleagues questioned her at a conference: “You are not a psychiatrist, you are not a scientist, you are only a dukun [traditional healer]. And all the participants laughed at me.”
Socioeconomic and geographic constraints
Participants also described difficulties in accessing formal mental health care, which impeded possibilities for successful collaboration. This included the cost of treatment. During a healing ritual we observed, Komang Gases intended to refer a young female client to mental health professionals after he had completed his treatment. However, he was concerned that her family could not afford it: For Iluh, I do plan to introduce her to a psychological doctor [psychiatrist]. So, I cleansed Iluh first. … I performed ruwat [healing ritual] on her first. I talked with her, communicated well and properly. Afterward, I feel comfortable, and then we will bring her to a psychological doctor. However, that is also upon her parents’ consent. Because if we are to meet a doctor, it would require cost.
Moreover, collaborative healing can be impossible if access to professional health workers is too difficult due to the unequal provision of services and poor road infrastructure, particularly in rural areas (Good et al., 2019). This can result in TFHs being the only accessible option, as Dr. Ronald observed: Actually, community access to primary health care, especially mental health, is very difficult. We know that, geographically, Manggarai is not only big, but [also] … the road access is very difficult. From the village, [one] must go to the capital of the regency to obtain psychiatric medication and receive an explanation about mental illness. It's very difficult.
Even if healers in these locations are predisposed towards collaboration, referring their clients to mental health professionals is difficult.
Perceived family resistance
In Indonesian society, where family members make most decisions, the family's acceptance of collaborative care is crucial. Mental health workers expressed concerns about families’ lack of knowledge about psychiatric treatment and fears of using psychiatric medication. Dr. Haqiqi, a psychiatrist in Yogyakarta, Java, stated: The challenge to collaborate between religious and medical [practitioners], usually it's the family's lack of knowledge about medical [treatment]. They expect only [treatment] from the religious side. They don’t want to be treated by the doctor, or they don’t want the patient to be given medication. They think that medications are like poison. So, the challenge comes from the family. Essentially [they want] to just read the Qur’an, not medication.
Due to stigma and discrimination, there is still hesitance to accept psychiatric treatment for a family member. For many families, religious healing is more acceptable and less stigmatizing. Using such healers may therefore be preferable to save the family's social image and promote social inclusion. Kyai Sirodjan, head of a pesantren in Yogyakarta, Java, expressed his view that there was less stigma if someone was treated in the pesantren than in a psychiatric hospital: At home, nobody wants to marry [someone with mental illness]. But, because they were in a pesantren not as a crazy [person] but in a boarding house, not from a mental hospital, after they go home they can marry. The image in the community is [they are] not someone who was in rehabilitation, not from a care centre, not from a mental hospital, but from a boarding school.
Discussion
It is well acknowledged in Indonesia and elsewhere that families have a large influence in shaping the path to care (Anto & Colucci, 2015; Hunt et al., 2023). This includes the decision to seek care from healing practitioners of various “epistemic communities” (Kirmayer, 2012, p. 115), including faith-based healing. As we and others have shown, religious identity and values have a powerful influence on help seeking for mental illness in Indonesia, despite the increase in community mental health services and changes in understanding of mental illness over time. Given the unequal distribution of mental health services and infrastructural challenges, this is unlikely to change. As we describe in this paper (and in our film), practitioners from both medical and faith-based approaches are therefore engaged in a creative variety of approaches to work together to provide care for people with mental health needs. These approaches have developed organically, motivated by both ideological and pragmatic factors. Ideological motives included shared religious values and national identity, a commitment to holistic care that addresses spiritual as well as medical needs, and a desire to maintain harmony. This phenomenon can be understood firstly by the epistemological pluralism embraced by health professionals who do not view their religious faith as incommensurate with scientific expertise. This was found throughout all the case studies, regardless of religion, and in our parallel research in Ghana (Colucci, 2021b; Kpobi et al., 2023). In Indonesia, this holistic integrative approach is supported by a strongly internalized and socially validated national identity, where religious faith is enshrined in the constitutional principles of Pancasila. Liem (2020) reached a similar conclusion in his study of clinical psychologists in Indonesia.
This epistemological openness enabled practitioners to adopt an integrative approach which aimed to support the preferences of families for religious and spiritual treatments, whilst also preventing harm. According to Park and Canaway (2019), the continuum of integration ranges from tolerant, to inclusive to integrative. Achieving integration depends on historical and cultural use of TFHs, political will, attitude and acceptance by providers, and resource availability. However, others caution that integration may result in a dilution of the healing potential of spiritual practices or subsume healers into biomedical practice (Pham et al., 2021). As demonstrated by participants in this study, collaboration must leave space for healing effects that go beyond what can be easily measured or understood within scientific paradigms and value phenomenological experience of the sacred (Csordas, 2023).
As we have shown in Ghana (Colucci 2021b; Kpobi et al., 2023; Read, 2019), successful collaboration is also built on the strength and sustainability of interpersonal relationships between health practitioners and healers. Mutual respect and trust between medical and faith-based healing practitioners was guided by the primary value of ‘harmony’ in Indonesian social relationships (Lestari et al., 2013; Panggabean et al., 2013). Harmony in Indonesian society is not only achieved through changes in the structure of relationships, but also maintained through “being considerate” (Lestari et al., 2013, p. 31) and having an accepting attitude towards each other. The ‘maintenance of harmony’ through active negotiation and compromise is thus key to successful collaboration. For this reason, we chose Harmoni: Healing Together as the title for the documentary film (Colucci, 2021a).
The second group of factors influencing collaboration in this context is the pragmatic motives, particularly in the face of resource scarcity and limited access to formal mental health services. In this situation, philanthropic support from religious groups or different practitioners pooling resources enabled mental health practitioners to make their services more widely available, and TFHs to diversify, extend their practice, and respond to crises. Despite calls for integration of TFHs within the mental health system (Soori et al., 2024), training, regulation, and professionalization of faith-based healers or other models of institutionalized collaboration were rarely mentioned by participants in this research. Rather, perspectives on collaboration were orientated towards personal motivations and values and employing informal rather than institutional platforms as the foundation for collaborative relationships. Most collaborative relationships we observed were formed serendipitously through personal relationships without formalized institutional support. Even in Ghana, where mental health policy officially mandates collaboration with faith-based healing practitioners, a lack of resources in practice rendered interpersonal relationships and motivation central to the success of partnerships with healers (Kpobi et al., 2023). As in Ghana, the current Omnibus Health Law in Indonesia includes traditional healers as part of the health workforce. However, also in common with Ghana, the law mandates health practitioners to monitor and regulate the activities of faith-based healers to prevent human rights abuses. This maintains and reinforces a hierarchical relationship that may perpetuate divisions, both in terms of identity and competition for resources. Neither country has sufficient programmatic, budgetary support for health workers to engage in sustainable partnerships with TFHs, leaving this mainly to the motivation, interest, and goodwill of individuals such as those highlighted in our research. Furthermore, inequities in access to mental health services across Indonesia, particularly in more remote rural communities, mean that options to combine medical, psychological, and traditional or faith-based forms of treatment are unavailable to many.
Limitations
The language barrier is one of the limitations of this study, as the local researchers, DS, AWP, and WJ, speak Indonesian and Javanese while the participants also spoke Sundanese, Balinese, or Manggarai. In these settings, we conducted interviews accompanied by local interpreters and hired translators to transcribe the interviews.
The relatively short time frame for this research meant that we could not observe participants, including people with lived experience, over a long period. Research has shown that help seeking by people with lived experience and caregivers fluctuates over time (Good et al., 2019). Furthermore, in this research we focus on particular instances where TFHs collaborated successfully with mental health professionals. Research with other healers or health workers would likely identify other facilitators and barriers.
Conclusion
As we have shown in this paper and the accompanying documentary research films, collaboration between traditional and faith-based healers and mental health professionals can develop through shared personal values and identity and openness to building relationships and dialogue. At the same time, collaboration can be limited by competition and conflict between practitioners of different epistemologies and by internal criticism from professional peers. In addition, weaknesses in the mental health system infrastructure and misunderstanding of formal mental health care by families and healers can present challenges for successful collaboration, possibilities for care, and protection of human rights.
Our findings suggest that harmonious and mutually respectful collaborations between mental health professionals and TFHs can arise organically out of shared relationships, values, and motivations, rather than through prescriptive institutional approaches. Nonetheless, without policy-level support, such partnerships may only be available to a few and may not be sustained in the long term. Too often, initiatives driven by charismatic, motivated individuals do not survive when those individuals are no longer around. Consequently, education for mental health professionals should include opportunities to reflexively engage with the spiritual and cultural values of the communities they serve to enable the formation of trusting, open-minded, respectful interactions with healers and families. In Ethiopia, for example, Baheretibeb and colleagues conducted consultative workshops employing a model of ‘transformative learning,’ bringing together psychiatrists and religious leaders for non-hierarchical ‘horizontal’ dialogue and critical reflection (Baheretibeb et al., 2022). Importantly, the workshops actively incorporated shared Ethiopian cultural and religious values to facilitate the learning process and build trust (Baheretibeb et al., 2022). Similar dialogue events have been held in Indonesia, one of which was captured in our documentary film (Colucci, 2021a).
Alongside this, to provide comprehensive mental health care that addresses socio-cultural and spiritual needs, the mental health system must allocate adequate resources to support efforts to engage with faith-based healing practitioners to build genuine and sustainable relationships. Suggestions for financing community mental health services include shifting funding from institutional services, diversifying health insurance to include social interventions, not only medication, and partnerships with NGOs (WHO, 2021), all of which could be used to support collaborations between healers and health workers as part of a holistic approach to community mental health care. The collaborative practices we have outlined provide lessons that could inform future partnerships in Indonesia and elsewhere.
Supplemental Material
sj-docx-1-tps-10.1177_13634615251338906 - Supplemental material for “They think we are trying to combine knowledges, whereas we are trying to harmonize them”: A visual exploration of what promotes successful collaboration between mental health workers and healers in Indonesia
Supplemental material, sj-docx-1-tps-10.1177_13634615251338906 for “They think we are trying to combine knowledges, whereas we are trying to harmonize them”: A visual exploration of what promotes successful collaboration between mental health workers and healers in Indonesia by Diana Setiyawati, Wulan Nur Jatmika, Ursula M Read, and Erminia Colucci in Transcultural Psychiatry
Footnotes
Acknowledgements
We gratefully acknowledge the support of the United Kingdom Research and Innovation Economic and Social Research Council (UKRI ESRC) and the Global Challenges Research Fund (GCRF) in funding the research and film production (ES/S00114X/1). This article builds on an earlier draft by Ade Widyati Prastyani, a postdoctoral researcher for the ‘Together for Mental Health’ project. The authors wish to also acknowledge the contribution of Lily Kpobi and Roberta Selormey for the fruitful discussions and collaboration, as well as the contribution and support from members of the project's Steering Committee, the Indonesian Advisory Committee, the Center for Public Mental Health Faculty of Psychology Universitas Gadjah Mada team, and all the individuals and organizations who participated in the research.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council (grant number ES/S00114X/1).
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.