
Abstract
Personal recovery, a western conceptualisation that focuses on hope and living meaningful lives of choice rather than focusing on symptom reduction, is a more recent concept in many Asian countries including Thailand. One way to promote recovery-oriented service delivery is to use outcome measures that capture self-reported personal recovery. This study aimed to evaluate a Thai translation of a self-report measure of mental health recovery, the Recovery Assessment Scale – Domains and Stages (RAS-DS). The study also explored the cultural similarities and differences between Thai (n = 190) and Australian (n = 301) recovery experiences by comparing Thai and Australian participant responses to RAS-DS items. Data were analysed using Rasch analysis. Analyses revealed that the Thai version of the RAS-DS had adequate measurement properties. Cultural comparisons suggested that most aspects contained within the RAS-DS appear to be applicable across both Thai and Australian contexts. Three findings suggest linguistic or cultural differences in Thai and Australian recovery experiences: (i) a ceiling effect for Thai participants, (ii) some items were “harder” or “easier” for one cultural group to endorse than the other, and (iii) a few items were “misfitting” for Thai participants.
Keywords
Introduction
Recovery-oriented practice is gaining prominence around the world (Le Boutillier et al., 2011; Lorien et al., 2020). Recovery-oriented practice draws on the concepts of personal mental health recovery and involves a movement from away a purely medical orientation in which absence of symptoms is the primary outcome measured and medication is the focus of treatment. Rather, recovery-oriented practice strives to support people to take an active role in their recovery and enable them to reclaim and develop new meaning in their lives (Le Boutillier et al., 2015). Shifting practice towards a more recovery-oriented approach is complex. One approach that can be helpful in this process is the adoption of self-report outcome measures focused on personal recovery (Le Boutillier et al., 2015; Leamy et al., 2011) rather than those focused on symptom amelioration (Slade, 2010; Thornicroft & Slade, 2014).
The vast majority of research into personal recovery and recovery-oriented practice has come from western, English-speaking countries (Kuek et al., 2020). In more recent times, interest in recovery has expanded across Asian countries (Kuek et al., 2020), including Thailand (Injui et al., 2019). In an attempt to support recovery-oriented practice in Thailand, the Recovery Assessment Scale – Domains and Stages (RAS-DS) (Hancock et al., 2015), a self-report measure of recovery, was translated from English into Thai.
The RAS-DS was developed in Australia (Hancock et al., 2015, 2019; Scanlan et al., 2018) from the original Recovery Assessment Scale (Corrigan et al., 2004; Giffort et al., 1995) which was developed in the United States. Previous research has demonstrated strong measurement properties of the original RAS-DS within the Australian context. However, given the history of development in western countries, it is possible that some aspects of recovery may not suit the Thai context.
In Thailand, it is estimated that the lifetime prevalence of mental or substance use disorders is 30.8% (Kittirattanapaiboon et al., 2017) and the prevalence of schizophrenia is 8.8 per 10,000 people (Phanthunane et al., 2010). Despite these high figures, only a relatively small proportion of people access formal mental health treatment (Kittirattanapaiboon et al., 2017; Pitakchinnapong & Rhein, 2019). In recent years, mental health services in Thailand have expanded and community-based services are available through public health systems (Kaewprom, 2011; Mongkol, 2017; Pavasuthipaisit et al., 2016; Pitakchinnapong & Rhein, 2019). Despite growing interest in recovery-oriented services in Thailand (Injui et al., 2019), previous studies have suggested that Thai mental health professionals’ perspectives have tended to come from a biomedical rather than a recovery-oriented perspective (Kaewprom, 2011; Kaewprom et al., 2011).
Approximately 95% of the Thai population is Buddhist (Wong-Anuchit et al., 2016). In line with Buddhist teachings, many Thai people believe mental illness is caused by Karma (i.e., payback for bad deeds [babb] in a previous life) or as a consequence of ghosts, spirits or supernatural powers (Burnard et al., 2006; Dangdomyouth et al., 2008; Rungreangkulkij & Chesla, 2001; Sanseeha et al., 2009; Sethabouppha & Kane, 2005). One of the central practices that stems from Buddhist teaching is thum-jai. Thum-jai is commonly translated to mean “acceptance”. Thum-jai is a culturally embedded coping strategy that Thai people adopt. It involves accepting fate or the reality of adversity rather than fighting against it and continuing to be in distress (Mills et al., 2019). These Buddhist derived beliefs and practices may influence individuals’ recovery. For example, the Buddhist practice of mindful meditation (which has been integrated into many western mental health programs; Phoenix, 2014) may promote better mental health recovery, but other beliefs related to the causes of mental illness may result in stigma which may hinder social support and recovery.
The context in Australia is quite different. First, there is a longer history of community mental health service availability (Allison et al., 2021; Rosen, 2006) and there is “a fairly good record comparatively for community tolerance of people with mental illness” (Rosen, 2006, p. 87). Community mental health literacy is improving and perceptions of the causes of mental illness include both genetic and social factors and are becoming more aligned with professional understandings (Jorm et al., 2005; Reavley & Jorm, 2012). More stigmatised views of causes of mental illness (e.g., illness is caused by a “weakness of character”) have been generally held by only a minority of the community and are decreasing over time (Jorm et al., 2005).
Authors comparing the broader cultural contexts of Thailand and Australia identified that the most pronounced difference was that Thailand was a highly collectivist country while Australia was a highly individualist country (Hofstede et al., 2010). Other differences included “power distance” which is related to hierarchy, with Australia rated as less hierarchical than Thailand, and the dimension of “Indulgence”, or gratification of personal needs or desires, with Australia being rated as more indulgent than Thailand (Hofstede et al., 2010).
These cultural and contextual differences between Australia where the RAS-DS was developed and Thailand where the translation will be used might mean that some of the concepts included in the RAS-DS may be experienced differently, or not be relevant, in the Thai context. Therefore, this study was established to explore the following research questions: (a) does RAS-DS (Thai) demonstrate acceptable measurement properties?; and (b) are there systematic differences in responses to RAS-DS items in Thai and Australian respondents that might suggest cultural differences in individuals’ experiences of recovery? Exploring these research questions will allow for the consideration of the usefulness of the RAS-DS (Thai) as a measure of mental health recovery in Thailand and to shed light on the cultural similarities and differences in terms of the conceptualisation of personal recovery.
Method
Data collection for Thai participants was approved by the Institute for the Development Human Research Protections (IHRP) Committee, Ministry of Public Health. All Thai participants gave written, informed consent. Data collection for the Australian participants was approved by the Human Research Ethics Committee at the University of Sydney.
Data collection
Thai participants were recruited from an occupational therapy unit within an inpatient institute of psychiatry department located in Bangkok, Thailand. Third year occupational therapy students presented RAS-DS (Thai) to participants after being trained in its use by the first author. Basic demographic information (age, gender and primary diagnosis) was also recorded. Australian participants (previously reported in Hancock et al., 2015) were participating in a range of programs delivered by non-government organisations in the states of New South Wales and Queensland.
Instrumentation
The RAS-DS (Thai) is a translation of the original, English-language RAS-DS developed in Australia (Hancock et al., 2015). The original RAS-DS (completed by the Australian participants in this study) has demonstrated good measurement properties, sensitivity to change and acceptability to consumers and clinicians in adult and youth mental health services (Hancock et al., 2015, 2020; Scanlan et al., 2018). The original RAS-DS and translated versions in 16 additional languages are currently used in 26 countries, including the United States (Gutierrez et al., 2020; Hughes & Moni, 2019), Canada (Sniatala & Herath, 2019), Hong Kong (Fung et al., 2020a, 2020b) and Egypt (El-Monshed & Amr, 2020).
RAS-DS includes 38 items categorised into four “domains” of recovery: “Doing things I value” (functional recovery: 6 items); “Looking forward” (personal recovery: 18 items), “Mastering my illness” (clinical recovery: 7 items) and “Connecting and belonging” (social recovery: 7 items). Each item is rated on a 4-point scale from 1 (untrue) to 4 (completely true). Item scores are totalled and then divided by the number of rated items for each domain to calculate an average domain score. To gain a percentage score, the average score is divided by 4 and multiplied by 100 to determine a “score” out of 100 (Hancock et al., 2019).
The RAS-DS (Thai) was developed by a rigorous process of forward and backward translation. Two bilingual mental health occupational therapists independently translated the RAS-DS into Thai. Differences were resolved by discussion to meet consensus. An independent backwards translation (Thai to English) was then conducted by a bilingual non-health professional. The back-translated version was then compared to the original English RAS-DS and again, consensus reached through discussions.
Finally, the Thai version was then presented to a group of individuals with mental illness (N = 64; schizophrenia 50%, depression 25% and bipolar disorder 25%) at the Family Link Center. These individuals completed the RAS-DS and provided comments. While some items on the back-translation were slightly different from the original wording (items 2, 22, 23, 26, and 32), feedback confirmed that the meaning was unchanged. Final approval was granted by the original developer, Nicola Hancock and The University of Sydney.
Overall, the aim of the translation process was to ensure that the concepts and ideas included in the original RAS-DS were accurately translated into the RAS-DS (Thai). For this part of the translation process, the relevance of these concepts to the recovery journeys of Thai people was not evaluated.
Analyses
Analyses presented in this article were completed using the Rasch analysis program, Winsteps (Version 4.5.3; Linacre, 2020). A detailed overview of the specific analyses are presented in Supplemental File 1 in the online Supplemental Material.
To answer the first research question, it was necessary to explore various aspects of the measurement properties of the RAS-DS (Thai). These analyses followed the process as undertaken in the original RAS-DS validation study (Hancock et al., 2015) and only included data from Thai participants.
The first aspect evaluated was the structure of the rating scale and the way people respond to each category. This is important because if the rating scale has too many categories, then differences between categories will be meaningless and may lead to inappropriate interpretations of scores. On the other hand, if the rating scale does not have enough categories, then measurement precision will be lost (Khadka et al., 2012; Linacre, 1999).
The second aspect evaluated was the alignment between each item and the overall construct measured by the RAS-DS (Thai) (i.e., mental health recovery for Thai people). If items don’t “fit” with the overall construct, then this might suggest the item is not related to recovery in the Thai context or it might be that the way the item is worded is confusing or interpreted differently by different respondents (Linacre, 1999; Wright & Linacre, 1994).
The next aspect explored was how well individual items work together to form a single construct. This is referred to as “dimensionality”. If the items don’t all work together, or there are several different dimensions present in the data, then this might suggest that total scores may not be meaningful and that items may need to be removed or subscale totals used instead of overall total scores (Bond & Fox, 2015).
Finally, overall measurement precision was evaluated. Winteps outputs provide statistics about how precise (reliable) measurements are in terms of both items and people. Additionally, these statistics indicate how many different “levels of ability” are distinguishable within the data (Bond & Fox, 2015; Linacre, 1999).
To answer the second research question, a Differential Item Functioning (DIF) analysis was completed. This analysis used both data from the Thai participants as well as data from the original Australian-based validation study (Hancock et al., 2015). DIF analyses allow the comparison of data from two (or more) groups of participants to look at systematic differences in response between those groups (Bond & Fox, 2015; Linacre, 2020). As applied to the context of this study, the DIF analysis allowed for exploration as to whether participants from Thailand were more (or less) likely to endorse particular items when compared to participants from Australia. If a DIF was present for a particular item, then it would suggest that participants from Thailand and Australia who are at the same level of “recovery” (as measured by the RAS-DS) are likely to score the item differently (e.g., Thai respondents might, on average, score the item as a “4”, but Australian respondents would on average score the item as a “3”).
Results
Participants
A total of 190 participants completed RAS-DS (Thai). Mean participant age was 37.9 years (SD = 12.2 years). Participants’ gender was evenly split between males (95; 50%) and females (95; 50%) and primary diagnoses were schizophrenia (101; 53%) and substance abuse (89; 47%). A total of 301 Australian participants were included in the original study. Some participants completed the RAS-DS on more than one occasion, so a total of 324 RAS-DS completions were included in the analysis. In the Australian group, the average age was 41.8 (SD = 11.9 years), and gender was fairly evenly split (females: 156, 52%; males: 140, 47%; not recorded: 5, 2%). The most common diagnoses included schizophrenia and other psychoses (124; 41.2%) and mood disorders (102; 33.9%).
Measurement properties of the RAS-DS (Thai)
Overall, the analysis suggests that the RAS-DS (Thai) has reasonable measurement properties. Full details of the analysis are included in the Supplemental File and are summarised below.
The structure of the rating scale met most of the expected requirements. Analysis suggested that some of the categories might be too close together to show meaningful distinctions between ratings (especially the lower ratings of “1” and “2”). However, overall, the categories were properly ordered and supported reliable measurement.
Most items showed good alignment with the overall construct being measured. While no items were overly misaligned with the overall construct, four items did fall slightly outside the usual expectations (referred to as “misfit”). These items were: Item 36 (I have friends without mental illness); Item 38 (I feel OK about my family situation); Item 35 (I have friends who have also experienced mental illness); and Item 7 (I can handle it if I get unwell again).
In terms of how well the items worked together to form a single construct (dimensionality), the analysis suggested that the items generally worked well together and there wasn’t a specific secondary dimension (additional construct) present. There was a “ceiling effect” in the data, whereby about half of the participants (102; 54%) had an overall measure that was above the level of the hardest item on the RAS-DS (Thai).
Finally, overall statistics for measurement precision were generally good. Results suggested that the measurement of people and the measurement properties of items were reliable and that the RAS-DS (Thai) could separate people into about four statistically distinguishable levels.
Systematic differences in responses to items between Thai respondents and Australian respondents
Table 1 summarises the results from the DIF analyses. Overall, there was no significant DIF for 27 items. Eleven items showed the presence of a DIF with six items being more likely to be affirmed and five items being less likely to be affirmed by Thai respondents compared with Australian respondents.
Results from the DIF analyses.
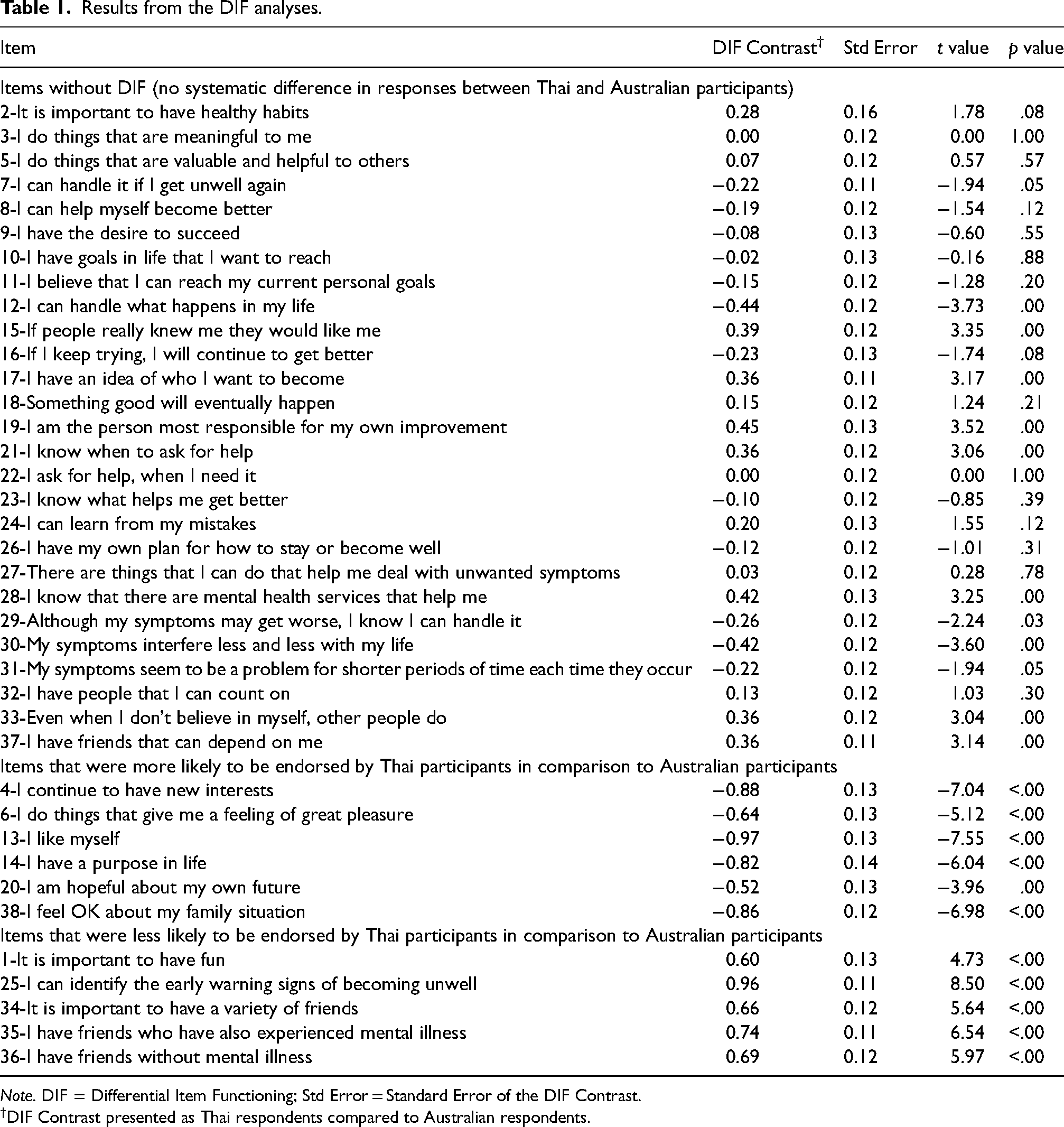
Note. DIF = Differential Item Functioning; Std Error = Standard Error of the DIF Contrast.
DIF Contrast presented as Thai respondents compared to Australian respondents.
Discussion
This project was established to explore two research questions: (a) does RAS-DS (Thai) demonstrate acceptable measurement properties; and (b) are there systematic differences in responses to RAS-DS items in Thai and Australian respondents that might suggest cultural differences in individuals’ experiences of recovery.
In terms of the first research question, overall results suggested that the RAS-DS (Thai) has reasonable measurement properties and would be an acceptable tool for use in Thailand. In terms of the second research question, responses were predominantly similar between Australian and Thai participants. This suggests that most of the constructs contained within the RAS-DS are relevant recovery constructs for both cultures. These include the 27 items in Table 1 where there was no significance in responses between Thai and Australian participants. There are, however, important differences between the way that Thai and Australian participants responded to particular items within the RAS-DS. These differences provide insights and raise questions about recovery constructs that might be more culturally dependent.
First, while the scale structure was sound, the lower categories (i.e., “untrue” and “a bit true”) were used more infrequently by Thai than Australian participants. For Thai participants, this resulted in a moderate “ceiling effect”. This greater “ceiling effect” within the Thai data may simply suggest that many participants in this sample were “more recovered” than could be accurately captured by the items listed in the RAS-DS. This may be related to the sampling procedure, as the occupational therapy students may have invited participants who were more advanced in their recovery journeys. Alternatively, participants might have responded in a way to “please” students or from a desire to demonstrate that they are recovered enough for hospital discharge. However, this difference might also reflect cultural differences. Thai cultural practice of thum-jai and Buddhist belief in Karma might both result in higher overall recovery scores. Previous authors (e.g., Wong-Anuchit et al., 2016) identified lower Thai scores compared to western participant scores on a scale measuring internalised stigma of mental illness, a construct closely aligned to recovery (in that lower internalised stigma is associated with more advanced recovery). These authors suggested that the Thai cultural practice of thum-jai, or being patient, reasonable and accepting of things that cannot be changed (Rungreangkulkij & Chesla, 2001; Wong-Anuchit et al., 2016), might result in “higher” scores on recovery-related scales. Thum-jai or acceptance is a Thai culturally embedded coping strategy (Mills et al., 2019), where people come to accept the reality of their situation rather than battle against it in distress. Further, for Thai people who understand their mental illness as a consequence of Karma, such as payback for bad deeds (babb) in a previous life, a sense of inevitability might add to or support thum-jai (Cheng & Tse, 2015; Kraus & Sears, 2009; Sethabouppha & Kane, 2005). Skills in mindfulness meditation, a Buddhist practice that has been incorporated into many western mental health interventions (Phoenix, 2014), might also support more advanced recovery for Thai participants.
It is also important to consider the items that demonstrated fit statistics outside of the recommended range. Three of these items (Item 35 – I have friends who have also experienced mental illness, Item 36 – I have friends without mental illness, and Item 38 – I feel OK about my family situation) have also been identified as having fit statistics outside of the recommended range with Australian participants (Hancock et al., 2015). Items 35 and 36 are related to friendship networks. Social connections with friends may be maintained by some individuals, even when they are at their earlier stages of their recovery journeys, whereas for others, re-establishing a friendship network may be something achieved in later stages of recovery. Additionally, it might be that some individuals only have friends without mental illness, rather than a diverse friendship group. In relation to Item 38, misfit was largely driven by individuals who were generally well-progressed in other areas of recovery but rated this item at the lowest category (“untrue”). This pattern is similar to results reported in previous studies (Hancock et al., 2015). For many individuals, families represented a powerful source of support, however for others, family relationships were a source of great difficulty or distress. In Thai culture the family unit is highly valued, however families face the stigma of mental illness and a patient's discharge is dependent on family acceptance of them going home (Poonnotok et al., 2019; Rungreangkulkij & Chesla, 2001; Sethabouppha & Kane, 2005). While the misfit for these three items might be explained by these reasons, it should also be considered that the misfit may be related to the wording of these items being confusing, interpreted differently by different participants or these concepts may have a poor alignment with the experience of recovery for Thai people.
However, one other item was misfitting for the Thai participant group and not for Australian participants and therefore suggests that this either reflects a cultural difference or a need for further exploration of the appropriateness of the Thai translation. This item was Item 7 – I can handle it if I get unwell again. Item 7, appears to strongly align with Thai practice of thum-jai or acceptance. Perhaps the somewhat unpredictable response patterns for Thai people responding to this item reflects a diversity in terms of people's strength in the Buddhist belief in Karma. It might also reflect that people are at differing stages of thum-jai with some still at a place of distress and non-acceptance while others have found and embraced the process of thum-jai and have reached a point where they are “letting it go… so life goes on” (Mills et al., 2019). Alternatively, rather than this unpredictability being culturally located, it is possible that the translation of this item may have created confusion or misinterpretation and needs further exploration and refinement. It may also reflect that this concept is not relevant to Thai participants’ journeys of recovery. This requires further examination.
The DIF analysis between Thai participants and Australian participants, suggests that the recovery experience is quite similar across both contexts with over 70% of items showing no systematic differences. This suggests that most aspects of recovery explored within the RAS-DS are universally relevant, or at least relevant within both Australian and Thai cultures rather than being culture-dependent. Previous authors recently found much alignment between western and Japanese constructs of recovery (Kanehara et al., 2022). However, while many similarities exist, it is valuable to examine items that were scored differently between Thai and Australian groups.
First, six items were more likely to be endorsed by (i.e., were “easier” for) Thai participants in comparison to Australian participants. Two items were from the “Doing things I value” domain (I continue to have new interests and I do things that give me a feeling of great pleasure); three were from the “Looking forward” domain (I like myself; I have a purpose in life; and I am hopeful about my own future); and one was from the “Connecting and belonging” domain (I feel OK about my family situation). The difference in the scoring on these items might well reflect cultural differences and subsequently, differences in the approach to and experience of recovery. Higher Thai scoring on these items might reflect the influence of Buddhist teachings and practices. Buddhism incorporates the law of Karma (Sethabouppha & Kane, 2005): good actions (boon) cause positive outcomes whereas bad actions (babb) lead to negative consequences. Buddhism teaches individuals to find pleasure in learning and establishing new interests. A meaningful life is aligned to supporting and caring for others (Rujkorakarn et al., 2018). Caring (metta) and helping the others (karuna) are key elements of compassion within Buddhist philosophy (Sethabouppha & Kane, 2005). Additionally, the concepts of self-compassion and thum-jai or acceptance, even in the face of suffering (Kraus & Sears, 2009; Poonnotok et al., 2019), may mean the items I like myself and I am hopeful about the future are easier for Thai participants to agree with, thus rate higher. The final item, I feel okay about my family situation, might be rated higher within the more “collective” culture of Thailand in comparison to Australia (Hofstede et al., 2010), placing more importance on caring for family members (Dangdomyouth et al., 2008; Kertchok et al., 2011; Poonnotok et al., 2019; Rungreangkulkij & Chesla, 2001; Sethabouppha & Kane, 2005), as well as individuals’ sense of personal commitment to do good things to compensate for the consequences of their mental disorder on the family (Burnard et al., 2006).
In contrast, five items were less likely to be endorsed (i.e., were “harder” for) Thai participants in comparison to Australian participants. Three were related to friendships from the “Connecting and belonging” domain (It is important to have a variety of friends, I have friends who have also experienced mental illness and I have friends without mental illness), one item was from the “Doing things I value” domain (It is important to have fun), one was from the “Mastering my illness” domain (I can identify the early warning signs of becoming unwell). Again, these differences in scoring may shed light upon cultural differences that have a flow-on impact upon people's experiences and approaches to recovery.
The “harder” nature of items related to friendships might relate to issues of stigma around mental illness (Kudva et al., 2020; Pitakchinnapong & Rhein, 2019; Sanseeha et al., 2009). Several authors have suggested that collectivist cultures expect a higher level of social conformity and are less tolerant of those who behave differently (Han & Pong, 2015; Papadopoulos et al., 2013; Pitakchinnapong & Rhein, 2019). These authors suggest that families within collectivist cultures are more likely to encourage their family member with mental illness to avoid contacts outside of the family in order to conceal the problem. Stigma may also be present for individuals who view mental illness as the result of bad Karma or ghosts, spirits or supernatural powers (Sanseeha et al., 2009; Sethabouppha & Kane, 2005). This would result in reduced opportunities for people to connect with and make friends outside of the family through activities such as employment (Kingsaiyhod, 2016; Kittirattanapaiboon et al., 2013). However, these results might also reflect that friendships outside of the family are considered less important for Thai participants. Previous studies found that both younger and older Thai people place far greater value on family relationships than other friendships (Gotzenbrucker & Kohl, 2014; Thanakwang et al., 2012). Results in relation to It is important to have fun are likely to reflect the greater importance that Thai culture places on caring for others above the more individually-focused indulgence (Hofstede et al., 2010) or engagement in pleasurable activities (Kraus & Sears, 2009; Rujkorakarn et al., 2018; Sethabouppha & Kane, 2005). Thai culture also has a greater expectation that younger generations should care for and respect older generations and places lower importance on individual freedoms such as seeking fun with friends (Pitakchinnapong & Rhein, 2019; Wongsawang et al., 2013). The final “harder” item (I can identify the early warning signs of becoming unwell) may demonstrate a lack of focus on mental health literacy, psychoeducation and self-management strategies as important components of mental health treatments in Thailand (Pavasuthipaisit et al., 2016; Pitakchinnapong & Rhein, 2019) and limited movement beyond the dominant biomedical approach toward more empowering recovery-oriented approaches (Kaewprom et al., 2011; Kingsaiyhod, 2016). In contrast, it might again reflect a greater Thai focus on acceptance (thum- jai) than on striving to understand and “battle” with the illness.
Limitations
This study has some limitations that should be highlighted. First, Australia and Thailand are both multicultural countries, so it may not be possible to generalise the findings from this study to all different cultural groups in each country. Additionally, exploration of items that demonstrate DIF between Thai and Australian participants is only one way of exploring potential cultural differences. More detailed, qualitative exploration of people's experiences of mental health recovery in Thailand and how this aligns with items on the RAS-DS should be undertaken in the future to strengthen knowledge in this area.
Conclusion
Overall, this study has demonstrated that RAS-DS (Thai) has sound measurement properties and may be a useful measure of mental health recovery in the Thai context. This study has also compared the way Thais and Australians scored the RAS-DS. While most items appear to be used in similar ways by both Australians and Thais, which lends support to the cross-cultural relevance of most of the constructs contained within the RAS-DS, some aspects appear to be quite different. These differences need further exploration, but some differences in item response that might reflect culturally different experiences of mental health recovery were discussed. Using the RAS-DS in routine practice in Thailand may be helpful in continuing to support a move toward more recovery-oriented approaches (Injui et al., 2019) and may also allow mental health workers to better understand the needs, ambitions and perspectives of the people they work with. Results highlight that further exploration of four items is needed to understand if these aspects are not meaningful within Thai culture or whether something has been lost in translation. Additionally, future projects should also explore whether there are additional elements important to the recovery journeys of individuals in Thailand. A synthesis of initial research in a range of Asian countries (Kuek et al., 2020) has suggested that there may be unique elements of the recovery journey in these contexts, but highlighted that further research is necessary.
Supplemental Material
sj-docx-1-tps-10.1177_13634615241250220 - Supplemental material for Measurement properties of the Thai translation of the Recovery Assessment Scale – Domains and Stages (RAS-DS) and comparison of recovery experiences between Thai and Australian consumers living with serious mental illness
Supplemental material, sj-docx-1-tps-10.1177_13634615241250220 for Measurement properties of the Thai translation of the Recovery Assessment Scale – Domains and Stages (RAS-DS) and comparison of recovery experiences between Thai and Australian consumers living with serious mental illness by Supalak Khemthong, Justin Newton Scanlan, and Nicola Hancock in Transcultural Psychiatry
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.