
Abstract
This article discusses the opportunities, dilemmas, and challenges involved in the cross-cultural adaptation (CCA) of psychological scales for use with refugee populations. It draws on insights derived from an attempt to adapt the 12-item General Health Questionnaire (GHQ-12) to the particular culture and context of Eritrean refugees residing in Israel. Multiple techniques including expert translations, a focus-group discussion, a survey, and piloting, were employed to attain a cross-cultural and conceptually equivalent measure. During the CCA process, the research team encountered issues pertaining to conceptual non-equivalence, the structure of the measure's responses and scoring system, and acceptability. These issues required the team to move beyond semantic translation by adapting certain items. This study demonstrates the compromises which need to be made in the adaptation process and indicates the potential bias which each of these compromises introduces. Despite its limitations, CCA does appear to significantly improve detection of mental health symptoms in refugee populations. Overall, the results of the present study provide support for the notion that the sensitive and appropriate assessment of individuals from refugee backgrounds requires adopting a rigorous, systematic, and contextual approach to instrument adaptation, with an emphasis on the integration of idioms of distress as well as the adaptation of Likert-type scales.
Introduction
Globally, the number of refugees and asylum seekers is the highest ever recorded. At the close of 2020, armed conflict, persecution, human rights violations, and violence have driven more than 80 million people across borders in search of safety (United Nations High Commissioner for Refugees, 2020b). Among the most profound disruptive consequences of conflict and global forced displacement are mental health issues, in particular, mild and moderate forms of depression, anxiety, and post-traumatic stress disorder (Blackmore et al., 2020; Charlson et al., 2019). Moreover, accurate measurement of these issues is crucial for establishing the burden of mental disorders in refugee populations, for conducting cross-cultural comparisons of symptoms, and for understanding “what works” in public health interventions and services (Tol et al., 2013). Indeed, the World Health Organization (WHO) Draft Global Action Plan “Promoting the health of refugees and migrants” (2019–2023) emphasizes the urgent need for reliable data to strengthen the evidence base of policies and programs focused on promoting the health of refugees and migrants (WHO, 2019).
Despite the importance of collecting robust scientific evidence, concerns have been raised over the cultural appropriateness of the traditional approach to measuring trauma and psychological distress in refugee populations. Currently, assessments conducted in refugee mental health research rely heavily on standardized psychological scales that were initially developed and validated in Western contexts and subsequently translated into local languages (Gadeberg et al., 2017; Gagnon & Tuck, 2004; Davidson et al., 2010; Hollifield et al., 2002). Yet, dramatic inconsistencies in the prevalence rates of mental health disorders in conflict-affected populations were observed. These have been attributed to methodological errors in measurement, calling into question the common practice of simply translating Western assessment tools to non-Western cultures (Charlson et al., 2019; Steel et al., 2009).
Indeed, there is a growing consensus that the single forward-and-back-translation procedure, common in both research and practice, can result in poor translations when used on its own, and thus may not be an adequate method for conducting and assessing quality in translated measures (Kaiser et al., 2019; Van Widenfelt et al., 2005). The gathering of data via poorly translated measures can, in turn, generate misleading generalizations and conclusions, including under-recognition or misidentification of psychiatric morbidity, which may result in the development and implementation of inapt, or even harmful, programs and policies (Allden et al., 2009). Recognizing the drawbacks of mere translation, researchers have since demonstrated the value of employing an alternate, cross-cultural adaptation (CCA) approach which explicitly incorporates the local or “emic” perspectives of a particular refugee community into established assessment measures (Bolton et al., 2009). This approach rests on the assumption that cultural knowledge and practices shape the ways people perceive and express distress, and, as such, must be taken into account for measures to achieve local validity (Kirmayer & Ban, 2013).
However, the procedures for adaptation of psychometric scales are still nascent: no guidelines are available, and much of the adaptation process is constrained by the time and funding at the research team's disposal (Mendenhall & Kim, 2019). Moreover, few empirical studies have detailed the specificities of the CCA process, such as the steps taken by the research team to achieve equivalence between the original and the adapted questionnaires, or the changes made to items and response categories (Charlson et al., 2019). The dearth of empirical research on the adaptation process is an important gap: by studying these accounts, researchers would be better able to prepare for the complexities of cross-cultural research with refugee populations.
This article aims to critically explore and reflect upon the challenges, dilemmas, and inevitable compromises involved in the cross-cultural adaptation of psychological scales for use with refugee participants. It draws on insights derived from the research team's attempt to adapt the General Health Questionnaire (GHQ-12) to the particular culture and context of Eritrean refugees residing in Israel. After describing the underlying theoretical perspectives and debates, the article reports results from one such adaptation process (which is part of a larger study exploring the on-the-ground lived experiences of psychological distress and well-being from the perspectives of Eritrean refugee adults residing in Israel). To critically assess validity, these results are then compared with interview findings derived from the second phase of the study.
Our overall argument is that translation is not a technical problem—as it is often characterized in medical and psychological scholarship—but rather a highly nuanced and complex task that greatly influences the validity of cross-cultural findings. By pulling back the curtain on cross-cultural research with refugees, and providing a transparent, forthright, and critical account of the realities of cross-cultural adaptation, the paper calls for a broader conversation about the complexities involved in translating individuals’ emotional worlds across languages and cultures.
Theoretical background and debates: Assessing mental health in refugee populations
Drawing on narrative theory and interpretive approaches, cross-cultural mental health researchers hold that cultural contexts shape how individuals and groups experience and express psychological distress (Kleinman, 1987; Mendenhall et al., 2016). Correspondingly, for measures to achieve local validity, they must take account of local conceptualizations of mental health, particularly idioms of distress (Cork et al., 2019). Idiom of distress is a concept originally developed by Nichter (1981) to draw attention to the distinctive manners in which different cultural groups communicate or manifest distress, both verbally and non-verbally (Lewis-Fernández & Kirmayer, 2019). Since idioms of distress are salient to members of a specific community, they can be used to develop and adapt measures which will make sense to research participants and which will be consistent with local priorities (Jayawickreme et al., 2012).
Yet, there remains disagreement among cross-cultural mental health scholars as to the role of local conceptualizations of mental health in instrument development. On the one hand, those in favor of developing and using new local measures argue that refugees’ local understandings of mental health should serve as the point of departure for instrument development. They insist that new measures can better capture the complexity and variance of local expressions of distress and resilience (Hinton et al., 2013). The development of these measures is often accomplished by employing a sequential mixed-methods approach (Allden et al., 2009; De Jong & Van Ommeren, 2002). For example, Miller et al. (2006) collected narrative data from the war-affected population in Kabul to construct the Afghan Symptom Checklist, a measure which was then administered to the local population.
On the other hand, critics point out that creating new instruments can be time-consuming and expensive, particularly in conflict-affected contexts in which resources often are limited and immediate results are needed (Ellis et al., 2007; Hollifield et al., 2002). Accordingly, it may not be feasible for cross-cultural researchers to develop a new instrument for each cultural community. Moreover, relying solely on local instruments and indicators may limit opportunities for aggregating findings in meta-analyses.
In the alternative cross-cultural adaptation (CCA) approach, local idioms of distress are incorporated into established assessment measures. Whereas mere translation solely focuses on achieving linguistic/literal equivalence, CCA takes both linguistic and cultural particularities into consideration, with the goal of producing cross-cultural and conceptually equivalent measures (Bolton et al., 2009). To date, CCA has been employed in numerous countries and populations including Syrian refugees in Jordan (Panter-Brick et al., 2018), Iraqi refugees in the United States (Shoeb et al., 2007), and conflict-affected adolescents in Nigeria (Kaiser et al., 2019). Scholars supporting CCA highlight the need for “rapid action and results” in refugee contexts, deeming this approach more efficient and pragmatic than developing entirely new measures. Moreover, adapting standardized instruments can be advantageous when conducting studies involving the comparison of symptoms, disorders, and risk/protective factors across cultures and settings (Rasmussen et al., 2014; Tol et al., 2013). Furthermore, transculturally adapting existing measures can facilitate communication of research findings to actors beyond the academy who may support funding for mental health service development (Kaiser et al., 2013).
Nonetheless, CCA is a complex endeavor, requiring multiple steps and considerations (Epstein et al., 2015). This complexity stems, in part, from the difficulty of faithfully translating words denoting emotional states and mental health concepts across languages and cultures. Researchers have demonstrated that some Western psychiatric categories are culturally determined and, as such, may not always fit with local cultural understandings and expressions of distress (Rasmussen et al., 2014). For example, Kohrt and Hruschka (2010) discovered that, in Nepal, there is no equivalent term for “post-traumatic stress disorder (PTSD)” as defined in Western cultures. Rather, psychological sequelae of torture, armed-conflict, and other negative life events are expressed through a wide range of idioms of distress. In such a scenario, simply translating items of a measure developed to capture the DSM-5 model of PTSD may not be enough to capture the diversity of trauma-related experiences in this population. Instead, local idioms or new items need to be incorporated into the measure to capture how Nepalis make sense of psychological trauma.
In addition, there remains a lack of consensus regarding best practices for CCA (Epstein et al., 2015), particularly with regard to the desired degree of deviation from an original scale (Mumford et al., 1991). This continuing discussion relates to the conflicting objectives of CCA: on the one hand, the new measure should remain as close as possible to the original in content, format, and rationale; on the other hand, adaptations are necessary for the measure to perform, in the new context, the same tasks for which it was originally designed (Mumford et al., 1991). As Canino et al. (1997) asked in their now seminal paper: “How much local cultural diversity can be incorporated into an established diagnostic instrument before the degree of alteration renders the instrument incapable of measuring the original constructs for which it was designed?” (p. 163). These factors, combined with the lengthy time and significant cost of local adaptation and testing, make CCA a daunting task. Consequently, many researchers shy away from this critical element of cross-cultural research, which may impede the rigor of research and the validity of the final findings. It is against this backdrop that the present study was implemented.
Methods
Setting
The cultural adaptation process presented in this article is part of a larger research project that was launched to address the unique plight of Eritrean refugees in Israel. The study was conducted over a 6-month period, between November 2019 and May 2020. It was a partnership between the author, a researcher at McGill University, and an Aid Organization for Refugees and Asylum Seekers in Israel (ASSAF), an Israeli non-governmental organization with a long-term presence in the country. ASSAF provides psychosocial support services to the asylum-seeking community in Israel, including individual treatment, advocacy, support groups, and humanitarian aid.
Due to the Eritrean government's repressive dictatorship, there are nearly 0.6 million Eritreans living in exile (United Nations High Commissioner for Refugees, 2020a), with approximately 21,890 seeking asylum in Israel (Population and Immigration Border Authority, 2020). Many Eritrean refugees have experienced profound losses and have undergone multiple traumatic experiences, such as torture, imprisonment, extreme deprivation, sexual and physical abuse, forced labor, human trafficking, and witnessing violence or death (Gebreyesus et al., 2019; Nakash et al., 2015). In Israel, Eritreans have been living in a state of liminal legality for a decade. While they are recognized under Israeli law as non-removable persons, they are nonetheless denied access or rights to the labor market, education, organized healthcare or social services (Ziegler, 2015). They live in isolation at the margins of Israeli society, prevented from attaining meaningful integration by a series of deliberate laws and policies.
Among the Eritreans who have entered Israel, the vast majority come from Senafe and its surroundings; the capital, Asmara; and the Gash-Barka region in the west (Terdiman, 2009). Most of the Eritreans in Israel belong to the largest Eritrean ethno-linguistic group, Tigrinya, which accounts for about half of Eritrea's population, while others belong to the Tigre, Afar, Bilen, Saho, and Rashaida groups (Terdiman, 2009). Each of the nine different ethnic groups in Eritrea has its own language, customs, and traditions. Nevertheless, over time, profound intermingling between the various ethno-linguistic groups has taken place and as a result, some traditions are shared among groups (Bereketeab, 2010).
Tigrinya is spoken fluently by almost all Eritrean refugees residing in Israel, and is the primary language for most. It is presumed to have been derived from Ge’ez, a Semitic language, and is written using the Ge’ez script (Fidel), which is also used for Amharic in Ethiopia (Bereketeab, 2010). Slight differences exist between the different dialects of Tigrinya, and native speakers can generally tell whether a Tigrinya speaker comes from a certain region in Eritrea. The vast majority of Eritreans in Israel are Christian, almost all of whom belong to the Orthodox church. A minority of the community belong to the Catholic or Pentecostal churches, while a small percentage are Muslim (Sabar & Rotbard, 2015). Informal estimates indicate that 80% of Eritrean refugees are men (Gebreyesus et al., 2018). Approximately half of the Eritrean community reside in Tel Aviv and its neighboring cities (Tel-Aviv Yafo Municipality, 2021).
Although a significant portion of Eritrean refugees residing in Israel successfully adapt—despite the traumatic experiences they faced in Eritrea and en route to Israel—empirical evidence indicates extraordinarily high levels of mental health problems (Mayer et al., 2020). Moreover, the prolonged nature of displacement in Israel, with its associated uncertainty about the future and persistent anxiety, is regarded as a major contributing factor to the mental health deterioration in some members of the Eritrean refugee community (Fennig & Denov, 2022).
Procedure
Data was collected by the author, an Israeli researcher at McGill University, who spoke Hebrew and English, alongside two Eritrean research assistants (RAs), one male and one female, who spoke Tigrinya, Hebrew, and English. The present study began in 2019. Prior to starting the study the author had led a year-long training program with ASSAF for interpreters working in mental health settings in the refugee community in Israel, from December 2017 to December 2018. Relationships of trust and rapport were thus established with many refugees from the Eritrean community during this period, facilitating recruitment into the current study. Moreover, the author has over 10 years of research and work experience among African migrants in Israel, facilitating entry into the field and equipping her with valuable contextual knowledge.
Prior to the study's conception, research assistants were recruited from the interpreter training mentioned above. RAs were chosen for their extensive experience with interpreting in the mental health and psychosocial (MHPSS) field and for their familiarity with the Eritrean community. Both RAs came to Israel as refugees, belonged to the Tigrinya ethno-linguistic group, and, at the time of the study, had been residing in the country for approximately 9 years. They were trained for four days in the project's aims, methods, and techniques for recruitment, procedures, and issues of ethics and confidentiality.
The CCA process was part of the initial screening phase of the study, in which an adapted version of the General Health Questionnaire-12 (GHQ-12; Goldberg, 1978) and an adapted sociodemographic questionnaire were administered. The objective of this phase was to determine participants’ eligibility to participate in the second phase of the study, which involved in-depth interviews. To be included in the latter, refugee respondents had to self-identify as having been exposed to trauma and as either currently suffering from mild to moderate psychological distress or having suffered in the past from psychological distress. In the initial research protocol, distress was to be determined qualitatively, relying on refugee respondents’ self-disclosure; however, the Research Ethics Board (REB) of McGill University requested that the research team either administer a screening instrument or have participants pre-interviewed by a qualified mental health professional. The REB wanted to ensure that respondents suffering from severe psychological distress be excluded from the study. In response, the lead researcher ultimately decided to determine the level of distress by administrating an adapted version of the GHQ-12.
With the assistance of ASSAF, participants were recruited using maximum variation sampling procedure. Participants were recruited largely through face-to-face solicitation and flyer distribution, conducted by the author and the RAs. A total of 39 participants took part in the screening phase of the study, of whom 34 proceeded to the interview portion of the study, while five individuals were excluded since they did not meet eligibility criteria. The in-depth interview portion of the study was conducted via a conceptually driven semi-structured interview guide with open-ended questions developed for the study and modelled after the DSM-5 Cultural Formulation Interview (CFI) (American Psychiatric Association, 2013). Interviews elicited information on participants’ definition of their mental health issues and their perceptions of cause, manifestation, and possible treatment or support.
Data analysis was inspired by a grounded theory approach to develop emergent themes (Glaser & Strauss, 1967). Two main data analysis “feedback loops” (Whitley & Crawford, 2005) were used: one following 15 interviews, and the other following 25 interviews. We then identified in vivo codes—codes that participants use themselves to divide the world. More conceptual codes were then added. Finally, we generated themes by engaging in constant comparative analysis (Glaser & Strauss, 1967), looking across the whole data set to compare cases.
The sample of the screening phase consisted of 14 men and 16 women. Participants were aged 26 to 45 (M = 33). Age at departure from Eritrea ranged from 15 to 30, with a mean of 18 years. Participants had been living in Israel for an average of 9 years, with a range of 7 to 14 years. Sixty per cent of participants were married with at least one child, 35% were single, and 5% were divorced, with children. Thirty-two participants self-identified as Christian, one as Muslim, and one as Pentecostal. Participants’ formal education varied, from 14 years to no education, with a mean of 10 years. All of the participants, except for three, were employed.
Participants were paid 20 shekel (approximately 7 Canadian dollars) for participating in the screening and an additional hourly rate of 45 shekel (approximately 18 Canadian dollars) for participating in the interview.
Ethical considerations
All study procedures were approved by the Research Ethics Board of McGill University. Research participants completed two consent forms: one for the screening phase, and another for the in-depth interview. This iterative consent approach explained the procedures for each phase and reminded refugees that their participation was voluntary, confidential and anonymous, and that they were free to withdraw their participation at any time.
All participants were provided with a list of referrals for receiving psychiatric or psychological services, free of charge. Participants who were identified in the screening or interview as particularly vulnerable received further assistance and support from the research team, who connected them with appropriate care services (e.g., social workers, shelters for domestic violence, community police).
Instruments
Translation and adaptation were completed for the General Health Questionnaire-12 (GHQ-12; Goldberg, 1978) as well as for a sociodemographic measure used in previous studies on refugee mental health in Israel, which included demographic questions relating to gender, date of birth, religion, family status, employment status, income, years of formal education, years living in Israel (Nakash et al., 2017).
The GHQ-12 is a self-administered 12-item screening instrument for general (non-psychotic) mental health issues. Its application in research settings as a screening tool for psychological distress is well documented, with results demonstrating reliability and validity in community samples in different cultural contexts (Anjara et al., 2020; Hystad & Johnsen, 2020). It consists of 12 questions assessing feelings of worry, stress, and inability over the past few weeks. Questions include: “Have you recently been able to manage your problems?” and “Have you recently lost much sleep over worry?” Items are rated on a 4-point Likert scale.
Our study used the original scoring by Goldberg, with response categories scored “not at all” and “no more than usual” as 0, “rather more than usual” and “much more than usual” as 1 (or the reverse depending on the question's phrasing), giving a possible range from 0 to 12, with higher scores indicating more severe distress symptoms. To differentiate between individuals with and without psychological distress, we used a cut-off score of 3. Accordingly, people who scored 2 or under were considered to have good mental wellbeing; if they did not self-identify as having suffered in the past from psychological distress, they were excluded from the study. Respondents who scored 9 or higher were considered to be suffering from severe psychological distress and were also excluded from the study. This cut-off score is in line with reports from previous studies that employed the GHQ-12 to examine psychological distress in resettled adult refugees living in the community (Jordans et al., 2012; Mölsä et al., 2014).
Adapting the GHQ-12: Rationale and process
Rationale
To overcome certain methodological challenges, both study instruments underwent a rigorous cultural adaptation process. The lead researcher's decision to employ this strategy was based on a number of considerations.
First, prior to this study, no effective, culturally appropriate psychological assessment measures existed for Eritrean refugee adults. To be sure, important efforts have been made to assess the validity of a number of translated instruments for Eritrean populations (Almedom et al., 2007; Amahazion, 2021; Getnet & Alem, 2019; Netsereab et al., 2018). However, the majority of mental health studies with Eritrean refugees rely on translation/back-translation of instruments that have not been rigorously adapted for Eritreans (Heeren et al., 2012; Kiat et al., 2017; Leiler et al., 2019; Mayer et al., 2020; Nakash et al., 2017).
Second, in order to enhance the study's feasibility given the limited timeframe and available resources, it was decided to adapt the GHQ-12 rather than to develop an entirely new instrument. Although one of the main objectives was to use the final qualitative findings on local idioms of distress to develop a new screening instrument, the research team needed a reliable measure to determine if refugee respondents met inclusion criteria before commencing the interviews; as a result, the research team could not wait for the completion of the study to measure distress.
Third, while cross-cultural studies often rely on simple translation and back-translation of instruments, the rigor of the final product mostly depends on the translators’ ability to identify and correct items which are incomprehensible, unacceptable, incomplete, or irrelevant (Van Ommeren et al., 1999). Although the research team valued the translators’ professionalism, the lead researcher wished to put in place additional measures to avoid inadvertent mistakes in translation. Finally, while there existed a previous Tigrinya translation of the GHQ-12 (Kiat et al., 2017), doubts had been expressed about the accuracy of certain items in this version (S. Gebremariam, personal communication, November 10, 2019).
The CCA process
CCA was executed by following Van Ommeren et al.’s (1999) five-step adaptation process, which has been widely used in cross-cultural mental health studies (Kaiser et al., 2019) (see Figure 1). The goal was to achieve equivalence along four dimensions: (1) Comprehensibility (linguistic equivalence) – the meaning of each item remains the same after translation; (2) Acceptability (technical equivalence) – the meaning and method of assessment is comparable in each culture with respect to the data that it yields; (3) Relevance (content equivalence) – the content of each item of the instrument is relevant to the phenomena of each culture being studied; (4) Completeness – the extent to which the item assesses the same concepts and ideas as the original (Flaherty et al., 1988; Van Ommeren et al., 1999).
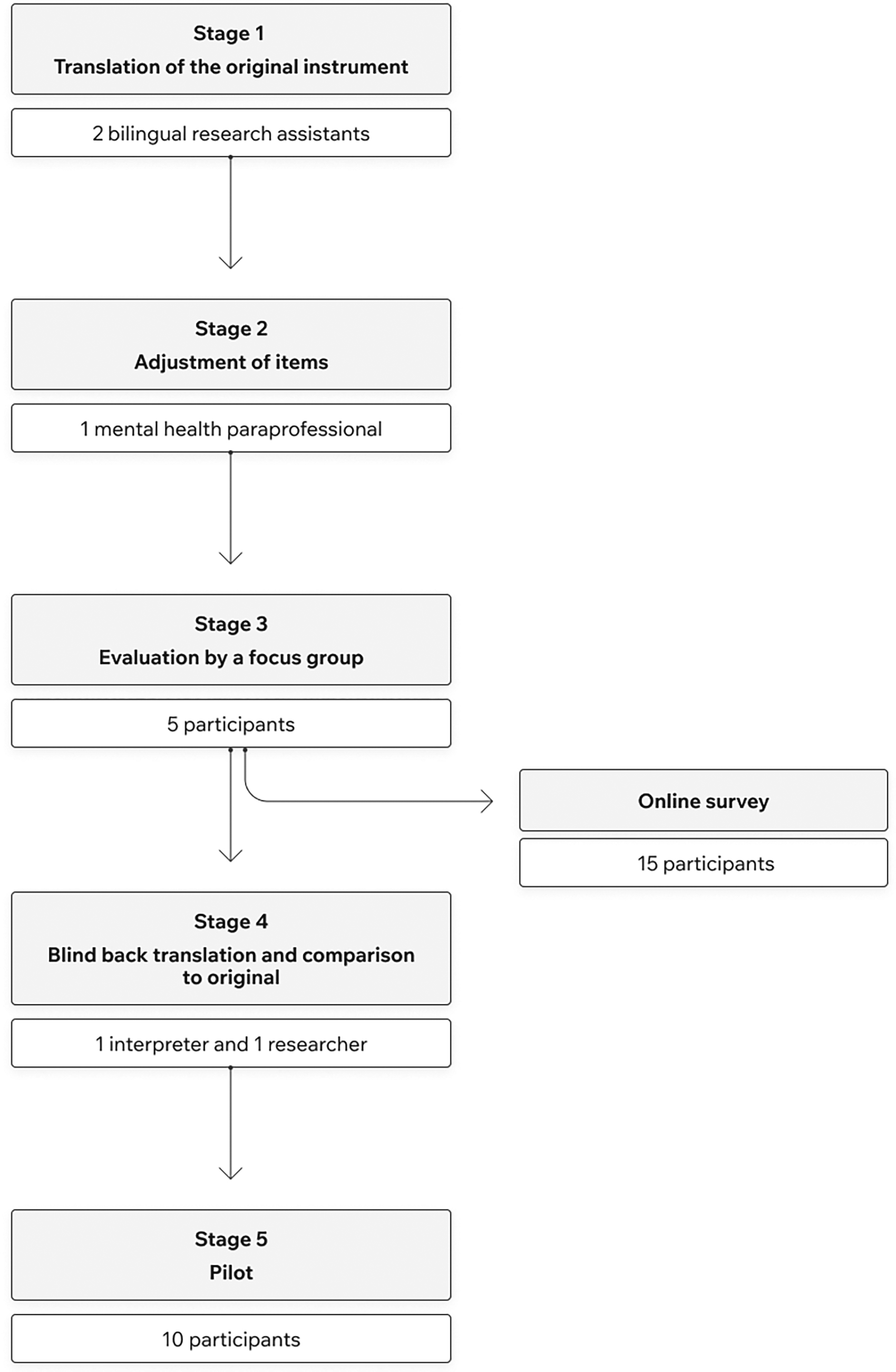
Cross-cultural adaptation process for the adapted GHQ-12.
First, each item was translated to Tigrinya by the study's bilingual RAs. Second, because Israel lacks mental health professionals proficient in Tigrinya, items were adjusted by a bilingual Eritrean student with a Bachelor's degree in psychology and experience with Western and Eritrean mental health concepts. Calling on trained mental health paraprofessionals—as opposed to clinical psychologists or psychiatrists—for the adaptation and validation of instruments is based on a procedure in previous studies in the context of limited availability of mental health experts (Bolton, 2001; Kohrt et al., 2011).
Afterwards, to make sure that the GHQ-12 included lay terminology that would be understood by all the participants (i.e., villagers speaking simple Tigrinya as well as more educated individuals coming from the city), the questionnaire items were evaluated by a focus group. The group was comprised of five young adults (M age = 27), all of whom had limited formal education. Next, the scale underwent back translation by a bilingual Eritrean interpreter who was not part of the research team and who was unfamiliar with the original items. The adjusted English version was then compared to the original English scale by the lead researcher to determine the completeness of the adjusted items. Finally, the modified scale was piloted on a small convenience sample of Eritrean participants who had no prior familiarity with the scale (n = 10). Participants were individually asked to fill out the scale and report on any challenges they experienced.
At each step of the adaptation process, issues pertaining to the acceptability, relevance, and comprehensibility of each item in the GHQ-12 were assessed and recorded. Items that performed poorly on any of these equivalence measures were adapted. All adaptation procedures were conducted in English and Tigrinya. Hebrew, although used at times in informal conversations, did not factor into the CCA process.
Results
In the following section we report the changes that were made to the tools to address problems with conceptual non-equivalence, the structure of the measure's responses and scoring system, and acceptability (the Tigrinya version of the GHQ-12 is available upon request). To further interrogate these changes and their appropriateness, findings from the interviews pertaining to Eritrean refugees’ expression of distress are presented below.
The problem of conceptual non-equivalence
Participants in the focus group reported difficulty with understanding the GHQ-12 item referring to the experience of depression (“Have you recently been feeling unhappy or depressed?”). The study's RAs and the bilingual mental health paraprofessional stated that Tigrinya does not have an equivalent for the Western idiom of “feeling depressed.” While in the first stage of the adaptation process the word Chincket (roughly translated as “distress”) was used, in the second stage this term was replaced by the bilingual mental health paraprofessional to Kzane, the formal Tigrinya term for depression. However, focus group participants were not familiar with the term Kzane and did not understand what it meant, later explaining that this term is rarely used and only employed by the educated elite or by health personnel.
The problem of non-equivalence (i.e., culture-specific terms, concepts, and expressions lacking equivalents in another culture) was overcome, in this case, by incorporating all possible phrases and terms that may be used by lay Eritrean refugees to describe depression-like problems and symptoms. To identify possible terms, the research team conducted a small-scale online survey among Eritreans (n = 15) that inquired about the translation of the term depression (“How do you translate depression in Tigrinya?”). The survey produced nine different terms. The research team then checked and discussed the findings, removing any terms that did not share features with depression. The final terms included in the tool were Zeyhgus (roughly translated as “unpleasant”), Kzane (roughly translated as “depression”) and Chincket (roughly translated as “distress”). The diverse answers generated in the survey demonstrate the lack of precise terminology in Tigrinya for “depression,” which was interpreted by lay individuals in a multitude of ways. In the comparison of the adjusted English version to the original English scale, the fourth stage of the adaptation process, the researcher noted that although the Tigrinya idioms did not constitute a complete semantic or conceptual equivalent, the item retained the same ideas as the original and therefore determined it to be complete.
Interview findings both complement and complicate findings from the adaptation process. A pervasive theme throughout the interviews was the prominent role of local idioms in the expression of suffering. Participants reported rarely speaking about issues pertaining to mental health directly. Instead, they often expressed psychological suffering indirectly, through verbal and non-verbal idioms. Many of the verbal idioms were related to the mind, describing over-usage or exhaustions of its capacity such as: “Bzuh mhasab” (thinking a lot) and “Ab aemroy selam ysen” (I don’t feel peace in my head). In addition, non-verbal somatic presentation of distress was common among participants. In particular, various symptoms related to the head were often mentioned. These included both mental symptoms (forgetfulness) and somatic symptoms (dizziness, poor sleep, and severe headaches).
The few Tigrinya idioms that were used by participants to express emotion directly took on different meanings which varied according to how these were expressed, along with the corresponding context. The same idiom was often employed to communicate diverse experiences—from mild distress to severe psychopathology. As S, an Eritrean interpreter working in a mental health clinic in Israel and one of the study's participants, explains: Chincket, for example, includes everything. People can use chincket for depression, for anxiety, also for stress. There is also the word tsekti but chincket they can also use it for fear, for panic, for worry. So it's really important that we pay attention. Because there are not a lot of words and the patients are used to using this word, chincket, for everything. But what makes it different is the tone and body language like [makes noise with mouth]. We have gestures that we use, not in all the cases but in a lot, to distinguish between this case and that. So it depends how the patient is expressing this to you, and then you can associate it to what he means if it's depression, anxiety or stress or fear or maybe he is preoccupied with something.
It is important to note, that throughout the adaptation process, the research team emphasized the need to maintain linguistic accuracy, while keeping the translations simple and clear enough to be easily understood by Eritreans from all educational backgrounds. In the first stage of the adaptation process there were several instances where one of the RAs used more formal language than was used by local people to express the same concept. In these instances, the local term was ultimately selected. For example, in Question 7 (“Have you been able to enjoy your day-to-day activities?”), the word “enjoy”—first translated as “Tzane,” a formal term—was eventually replaced with “Des,” a more common, simpler term.
Structure of responses and scoring system
The instrument's use of severity levels on a Likert scale generated confusion for participants in the pilot. The response options in the English GHQ-12 are “not at all,” “no more than usual,” “rather more than usual,” and “much more than usual.” During the pilot test, participants reported that these response categories sounded strange and abstract
Therefore, to ensure understanding of the instrument, the lead researcher decided to prepare it for administration by the study's RAs while retaining its original format (the Likert scale). A similar strategy has been used in other cross-cultural mental health studies (Ali et al., 2016). The GHQ-12 was originally designed for self-administration; however, due to the unforeseen difficulty regarding the Likert scale format as well as participants’ varying education and literacy levels, it was decided that, when necessary, the bilingual Eritrean RAs would read the scale items to respondents in their own language and then record their responses. When requested, the RAs would also provide short explanations regarding the instructions.
While this decision helped to ensure understanding of the instruments, it is possible that the RAs’ sociocultural identities may have influenced participants’ responses. There were three incidents, for example, in which participants, all male, received a low score (0–2) after having completed the scale with the assistance of an RA. Although participants rarely received a low score in the GHQ-12, this experience led the research team to pay greater attention to the influence of the RA's presence on participants’ responses.
The research team's intuitive suspicion regarding the RAs’ potential influence is reinforced by empirical findings derived from the interviews. Participants’ narratives revealed that issues pertaining to mental health were rarely shared with others. Participants often made a conscious effort to conceal their emotions, even from close friends and their own family members. This included actively refraining from talking about traumatic events, strong emotions, and symptoms. As expressed by one of the participants: “From a young age we learn to be afraid and we keep it locked inside” (Male, age 35). In light of these findings, it is quite possible that some participants tailored their responses according to their perception of the kinds of feelings they believed would be culturally appropriate for them to share in the presence of the RAs who came from the same refugee community.
Another element related to technical equivalence was the Likert scoring system of the measure, which was also found to be problematic. During the administration of the final scale, several participants expressed confusion and anxiety related to the scoring of the GHQ-12. Although participants signed a consent form explaining the purpose of screening activities prior to enrolment, several perceived the measure as a test in which there was a right or wrong answer. Those who scored either too high or too low to be considered for the study were visibly upset and confused when told that they could not be interviewed. Many of them were offended by their exclusion from the study and requested a chance to retake the psychological measure promising that “they will get the correct score this time.” It was only after a lengthy explanation relating to the risks of participation that respondents seemed to comprehend the purpose and implications of the measure and of the screening procedure.
Acceptability
On the demographic questionnaire, the item inquiring about participants’ income level raised acceptability concerns in the pretest, due to the context of extreme poverty and lack of services. The RAs reported that the question may have made the participants feel uncomfortable or embarrassed. They explained that participants may also have assumed that a question about income implied that they might receive benefits or services in return for interviewing, possibly leading them to report a lower income in order to become eligible for such services. Consequently, to avoid offending respondents or engendering false expectations, the question relating to income was excluded.
Lastly, Question 3 (“In the past 30 days have you felt that you are playing a useful part in things?”) was found to be a weak item in the pretest. Five out of the 10 participants did not understand the question, and requested explanations. Our adaptation team experienced difficulty with translating the phrase “in things” into Tigrinya. While it was decided not to omit the question entirely for fear of compromising the validity of the original instrument, further piloting is needed to determine the best way to phrase this item.
Discussion
Our findings illustrate the possibilities and pitfalls of the CCA approach, by describing how it was used to adapt the GHQ-12 to the culture and context of Eritrean refugees residing in Israel. They provide support for the notion that sensitive, appropriate assessment of individuals from refugee backgrounds requires adopting a rigorous, systematic, and contextual approach to instrument adaptation, with an emphasis on integrating idioms of distress while adapting Likert-type questions.
Integrating idioms of distress
The difficulties we encountered in identifying Tigrinya equivalents to the term “depression” resonate with previous studies that have adapted psychological scales for use with Eritrean refugees (Almedom et al., 2007; Getnet & Alem, 2019). These studies ran into similar difficulties when transferring concepts cross-culturally. For example, when administering an adapted “sense of coherence” scale (SOC-13) to measure resilience in Eritrea, Almedom et al. (2007) note that many of the participants “questioned the content of the SOC-13 scale during the process of its administration” (p. 96). They had particular difficulty with the SOC-13 assumption that well-being is an individualistic phenomenon. For the participants, by contrast, resilience and well-being were often seen as collective experiences, embedded in their family and community networks. As such, typical responses to the scale included “'How can you ask such a question?”; “I wouldn’t be human if I didn’t care about what goes on around me, would I?”; “… no, this is not in our culture [i.e., not to care about what goes on around oneself], of course I care and try to do something about it, if I can”; “… if I didn’t care about what goes on around me, I might as well be dead” (p. 96).
The lead researcher's final decision to modify the GHQ-12 by inserting idioms of distress into the instrument's item referring to depression was appropriate for the needs of the present study—that is, the adaptation of a brief mental-health screening instrument for non-specific psychological distress. Although the Tigrinya idioms did not constitute a complete semantic or conceptual equivalent, the decision to include them all in the final adapted instrument ensured that several possible interpretations of the construct were included in the final scale. While there may have been slight deviances from the intended meaning, this strategy retained comprehensibility.
This strategy may, however, be inappropriate for adapting assessment/diagnostic tools to the detection of specific disorders requiring far greater accuracy and sensitivity than screening instruments. The study's findings, along with other studies on Eritrean refugees’ mental health (Fennig & Denov, 2022), suggest that distress is more commonly expressed through somatic symptoms and local idioms of excessive thinking. These important findings were missed in the survey conducted as part of the CCA process—suggesting that, to elicit idioms of distress, rapid surveys cannot replace in-depth narrative interviews.
Moreover, the research team's difficulties with transferring concepts cross-culturally highlights the general complexities of translating mental health concepts across languages and cultures. Indeed, the idioms of distress included in the adapted GHQ-12 are not semantic equivalents of “depression”; rather, they are distinct idiomatic expressions embedded in larger cultural frames and systems of knowledge which cannot be perfectly captured by translating practices. As Good and Good (1986) note: In general, however, the referents of symbols, i.e., their meanings are aspects of a culture or a life world, not objects outside of language through which language obtains meaning. “Heart discomfort” for Iranians is not the equivalent of “heart palpitations” for Americans; it does not mean the same thing (Good 1977). It is a symbol that condenses a distinctive set of meanings, a culture-specific “semantic network,” for Iranians. Complaints of feeling impure in India refer to a semantic domain of profound cultural significance, one that regulates caste, sexuality, and social hierarchy; there simply is no equivalent among Americans. (p. 14)
To improve our understanding of what is “at stake” when Eritrean refugees say chincket—what they mean—we need to explore what this term conveys, both to the individual and to the larger Eritrean community in the local context (Lewis-Fernández & Kirmayer, 2019). The emphasis on context here is crucial since, as with other idioms of distress (Kaiser et al., 2013), the meaning of chincket may vary according to education, gender, duration of stay in the asylum country, and context of use. In this vein, future research could employ ethnographic methods to explore the complex web of meanings and modes of interpretation related to this idiom, and others.
Adapting Likert-type scales
Regarding the difficulties our study participants experienced with the Likert-type scale, it should be noted that this challenge is not unique to Eritrean refugees. Other scholars working in the cross-cultural mental health field have encountered problems when administrating instruments with Likert-type questions to their non-English-speaking refugee respondents (Baird et al., 2017; Ellis et al., 2019; Flaskerud, 2012). In these contexts, the very process of answering a questionnaire is often unfamiliar. As a result, researchers may end up eliciting responses which represent a misunderstanding of intentions rather than an accurate reflection of respondents’ emotional state (Kleinman, 1987). Indeed, the significant methodological difficulties relating to this format have sparked an ongoing debate concerning the cultural validity of Likert-type scales, leading scholars such as Flaskerud (1988) to ask: “is the Likert scale format culturally biased?” (p. 185). To which Flaskerud (2012) further argues that “invalid or meaningless data may be derived from such scales, especially when they are used with culturally diverse participants and those with little formal education” (p. 132).
Some of the shortcomings of research with self-report Likert-type scales in refugee populations can be addressed by piloting alternative approaches to quantifying symptom severity, such as the use of locally developed illustrations. For example, in Uganda, Bolton and Tang (2002) used illustrations of a person carrying an increasingly heavy weight to represent severity levels on a local function assessment instrument. Retaining the Likert-type scale and hiring interpreters/RAs to verbally administer the scale, as was done in the present study, is not recommended, however, since it may introduce bias and significantly compromise the validity of the adapted scale.
As demonstrated in the present study, interpreters administering the scale may intentionally or unintentionally alter the responses collected from participants. Our findings regarding participants’ tendency to conceal emotions suggests that the outward expression of negative emotions among Eritrean refugees is discouraged. We speculate that this tendency may be more pronounced among Eritrean men. However, our small sample size precluded examination of variation based on gender and other demographic factors, but it is an important element for future research.
Cultural norms and expectations relating to disclosure of distress may have influenced responses provided in the presence of the study's RAs who came from the same refugee community. Participants may have provided what they feel are socially desirable responses, under-reporting mental health symptoms and problems that were viewed as undesirable and over-reporting socially desirable characteristics and behaviors. Despite the possibility of bias, the decision to administer the GHQ-12 with the assistance of the team's RAs increased the study's local validity. However, it may have come at the expense of achieving reliability, comparability, and standardization.
More broadly, our finding regarding the measure's scoring system highlights that special care should be taken to ensure that refugee participants fully understand the purpose of screening. Refugees often come from contexts which generally have inexistent, or only nascent, histories of social research
Encouraging the disclosure of translation errors
Although not direct findings of the study, the research team encountered some challenges with the adaptation process which deserve noting. In the present study, power disparities between the research team and the refugee participants (arising from differences in social location, race, socio-economic status, and gender) at times precluded the full disclosure of translation errors. Identifying errors in the scale was often interpreted by participants in the focus group and pilot as challenging the authority of the lead (Western) researcher and, as such, avoided. Participants would often prefer to randomly select an answer than admit to the lead researcher that they didn’t understand a question on the scale—only later revealing this choice to the Eritrean RAs.
In refugee contexts, consequently, researchers should not assume that participants’ completion of the full scale is an indication that they have fully understood all its items or endorsed the translated version of the scale. Although power issues are present in every study, they are exacerbated when the participants are refugees—a population that is often considered particularly vulnerable due to the multiple challenges they face, including trauma, limited political protections, and poverty (Seagle et al., 2020). Building trust with participants and emphasizing that they may comment on mistakes or misunderstandings is essential if researchers are to gather truthful and accurate data reflecting refugees’ actual beliefs and feelings. Involving refugees themselves in the adaptation and administration of the scale process (e.g., as RAs or members of expert committees) is one promising strategy that can help build trust and mitigate potential methodological and ethical weaknesses.
Conclusion and implications for research and practice
This article has aimed to increase the evidence base on the cross-cultural adaptation of psychological scales for refugee populations, by exploring the challenges involved in adapting the GHQ-12 to the culture and context of Eritrean refugees residing in Israel.
Several difficulties emerged pertaining to conceptual non-equivalence, the structure of the measure's responses and scoring system, and acceptability. Overall, the results of the present study contribute to a growing body of evidence suggesting that the assessment of individuals from refugee backgrounds holds its own specific characteristics and challenges, which need to be taken into account to ensure the validity of cross-cultural findings (Davidson et al., 2010).
The difficulties encountered in the CCA process hold several important implications for researchers and practitioners wishing to cross-culturally adapt psychological measures for refugee populations. Correspondingly, several key recommendations are provided below:
Cross-cultural adaptation is an imperfect process. This study illustrates the inevitable compromises in the adaptation process and the potential bias that each of these compromises introduces. Despite its limitations, CCA appears to significantly improve detection of mental health problems in refugee populations. Cross-cultural adaptation should be preceded by ethnographic work. The research team's failure to capture the full range and nuance of Eritrean refugees’ local expressions of distress in the adaptation process emphasizes the necessity of combining CCA with in-depth, and preferably long-term, ethnographic engagement. The assessment of individuals from refugee background holds its own specific characteristics and challenges which need to be considered in the adaptation process. Our findings demonstrate that refugees possess unique cultural systems of knowledge while lacking familiarity with psychological scales. Moreover, they suggest that issues of power and trust are more pronounced when working with refugee populations. Cross-cultural adaptation can be a tedious process, requiring significant resources and time to complete. In our initial research protocol, the lead researcher did not plan to administer a screening instrument, let alone to undertake a multi-step adaptation process. This delay came as a reminder of the complexity of cross-cultural work. In retrospect, since the purpose of the study was not to compare data across cultures, it might have been simpler and more effective to have had a clinician conduct a culturally sensitive assessment interview with the help of a highly skilled interpreter. In adaptation studies, researchers should select a broad sample. This will make for a well-rounded tool that includes the perspectives of individuals with a range of distress experiences. With respect to this study, our exclusion criteria (severe mental illness) were put in place to protect participants from potential harm; by the same token, it prevented us from exploring their subjective experiences and thus limited the reliability of the adapted GHQ-12. Futures studies may wish to cross culturally adapt the GHQ-12 for use in more severely distressed patients. Validation is a crucial final step in any adaptation process. The small size of our research team—one investigator and two RAs from the Eritrean community—and our limited resources prevented us from conducting a cross-cultural validation study before administering the instruments. This limitation could have affected the study findings. In Israel and in other countries in which Eritrean asylum seekers and refugees reside, practitioners working in clinical and community settings often have neither the time nor the training to administer complex diagnostic interviews for detecting common mental disorders and psychological distress (Kiat et al., 2017). This lack of diagnostic capacity could be remedied by locally validating our adapted GHQ-12 and integrating it into the assessment of refugee clients. It is important to note that the Tigrinya version of the GHQ-12 was adapted from the original English version. Clinicians wishing to use the Hebrew version of the GHQ-12 would need to repeat the CCA process. Irrespective of how much care and attention is allocated to processes of adaptation, the extent to which mental health concepts can be translated across languages and cultures is still open to debate. Can the emotional worlds of individuals be faithfully translated (Barrett, 2017; Kleinman & Good, 1985)? These and other important epistemological and methodological questions will continue to challenge researchers seeking to conduct cross-cultural measurement. Hopefully, the current study will stimulate further investigation of this important area.
Footnotes
Acknowledgments
I am endlessly grateful to my local research assistants, Solomon Gebremariam and Tsega Bisrat, for their great insights and professional support.
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Vanier Canada Graduate Scholarships (Vanier CGS) Program, Social Sciences and Humanities Research Council of Canada (grant numberVanier Canada Graduate Scholarship).