
Abstract
Elevated rates of mental health difficulties are frequently reported in conflict-affected and displaced populations. Even with advances in improving the validity and reliability of measures, our knowledge of the performance of assessment tools is often limited by a lack of contextualization to specific populations and socio-political settings. This reflective article aimed to review challenges and share lessons learned from the process of administering and supervising a structured clinical interview. We administered the MINI International Neuropsychiatric Interview for Children and Adolescents (MINI Kid) and used the Clinical Global Impression (CGI) severity scale with N = 119 Syrian refugee children (aged 8–17) resident in ITSs in Lebanon. Qualitative data were derived from supervision process notes on challenges that arose during assessments, analyzed for thematic content. Five themes were identified: (1) practical and logistical challenges (changeable nature of daily life, competing demands, access to phones, temporary locations, limited referral options); (2) validity (lack of privacy, trust, perceptions of mental health, stigma, false positive answers); (3) cultural norms and meaning (impact of different meanings on answers); (4) contextual norms (reactive and adaptive emotional and behavioral responses to contextual stress); and (5) co-morbidity and formulation (interconnected and complex presentations). The findings suggest that while structured assessments have major advantages, cultural and contextual sensitivity during assessments, addressing practical barriers to improving accessibility, and consideration for inter-connected formulations are essential to help inform prevalence rates, treatment plans, and public health strategies.
Refugees and displaced populations have a higher incidence of mental disorders and psychosocial problems compared to non-refugee populations and other migrant groups (Charlson et al., 2019). These elevated mental health problems have been linked to high exposure to daily stressors, past and present traumatic events, political and financial instability, lack of opportunity, and poor access to services (Fernando et al., 2010; Jefee-Bahlou et al., 2014). However, there are significant challenges to the assessment of mental health and wellbeing in minority and displaced populations, due to limited validation of measures in specific local languages, dialects, and contexts; lack of integration of cultural differences into conceptualizations of mental health; and limited understanding of contextual influences on the expression and severity of mental health difficulties (Kirmayer et al., 2003). This is of particular importance within Syrian refugee populations, who have been displaced on an unprecedented scale in the Middle Eastern or Western Asia region and beyond, with poor access to basic living standards and freedoms, and no possibility of return to Syria. The assessment and treatment of mental health difficulties by state and non-governmental agencies in this population has been improving but is often hampered by a limited understanding of the social, cultural, and political context and its influence on the expression and experience of distress (Hassan et al., 2016). This understanding is vital to inform appropriate identification of mental disorders and treatments, without which mental health services risk missing or misidentifying cases, delivering inappropriate, ineffective, or even harmful treatments, and duplicating the disadvantage and distress that the interventions aimed to address in the first place (Kirmayer & Swartz, 2013). The present reflective article reports on the lessons learned whilst clinically assessing Syrian child and adolescent refugees during data collection for research with Syrian refugees in Lebanon (McEwen, Moghames et al., 2021), with the objective of disseminating learning and improving mental health assessments in this population.
Over one million people have been killed or seriously injured since the onset of the war in Syria 10 years ago, with more than 6.2 million people displaced, and millions more internally displaced (UNHCR, 2021a). More than half of the displaced population are children (UNHCR, 2017). Syrian refugees make up the majority of the government-estimated 1.5 million refugees in Lebanon, a neighboring middle-income country with a total population of 5.9 million (UNHCR, 2020). Lebanon is currently suffering from an unprecedented economic disaster, exacerbated by the COVID-19 pandemic, and reeling from the Beirut port explosions that killed hundreds of people and displaced thousands. Even before the economic crisis, Syrian refugees in Lebanon suffered from poor educational and economic opportunities, socio-economic insecurity, and widespread prejudice and discrimination (WHO, 2017). At that time, almost 80% of Syrian refugees in Lebanon were living below the poverty line, with 58% living in extreme poverty and unable to meet basic survival needs (UNHCR, 2017). This number is now almost 90%, with the average family earning 308,728 LBP per person monthly (UNHCR, 2021b), equivalent at the time of writing to US$13.42. Many refugees live in informal tented settlements (ITSs), rely heavily on food assistance, and are vulnerable to child labor, early marriage, and violence (El Arab & Sagbakken, 2019; Oxfam, 2017). Structural inequality, discrimination, and victimization in host countries like Lebanon exacerbate a sense of isolation and loss (Hassan et al., 2016; Thorleifsson, 2014). As a result, Syrian families in Lebanon are in a state of prolonged ‘temporariness,’ with no way to settle and no way to return.
Reliable research on the prevalence of mental disorders in Syrian refugee populations is limited (Hassan et al., 2015). In the existing literature, the most common mental disorders for displaced Syrian populations are post-traumatic stress disorder (PTSD), depression, and anxiety. In child and adult settled Syrian refugee populations in high-income countries, prevalence rates range from 11.4–32.2% for PTSD, 14.5–40.3% for depression, and 13.5–47.7% for anxiety (Georgiadou et al., 2018; Javanbakht et al., 2019; Soykoek et al., 2017; Tinghög et al., 2017). In low- and middle-income countries, prevalence rates range from 50.2–83.4% for PTSD, and 47.4–59.4% for depression (Acaturk et al., 2018; Eruyar et al., 2018; Kandemir et al., 2018; Mahmood et al., 2019). The only known study in Lebanon found a point prevalence for PTSD of 27% in Syrian refugee adults in the Beqa’a region (Kazour et al., 2017). The high prevalence of these disorders is in keeping with studies conducted in other conflict-affected populations (Charlson et al., 2019; De Jong et al., 2003), but the wide range also points to potential problems in estimating the prevalence of mental disorders.
A comprehensive review of studies on the mental health of Syrian refugee populations identified major limitations in the validity and reliability of data due to a lack of culturally-specific symptoms or idioms of distress in standard instruments, validation of measures using different populations (such as Iraqi or Palestinian refugees), a focus on pathology and not broader constructs of wellbeing and distress, and the overestimation of disorders by neglecting local context and life circumstance in the administration of tools and the assignment of diagnoses (Hassan et al., 2015, 2016). Empirical studies have highlighted a wide range of sub-clinical emotional, cognitive, physical, and behavioral and social problems, for both adult and child Syrian refugees, that may not be well reflected in prevalence rates. These may include frustration, a sense of loss of control, boredom, humiliation, somatic complaints (Almoshosh, 2015; Dimitry, 2012; Ehntholt & Yule, 2006; Hassan et al., 2016), interpersonal conflict (Dimitry, 2012), and violent play (James et al., 2014). Most assessment measures of child and adolescent mental health have been developed in North American or Western European populations and have not been extensively studied in Western Asia, nor in the context of war and displacement. Factorial analyses and standardized norms are not necessarily applicable across populations, cultures, and contexts, particularly when there are stark differences in the level of risk such as in populations affected by mass displacement, war, or poverty (Ehntholt & Yule, 2006). Structured assessments of mental health have major advantages in standardizing the assessment process, producing comparable data between populations and settings, and providing tools that can be used with few resources and by non-specialists (Kazour et al., 2017). However, the application of assessments developed in non-conflict North American and Western European contexts to low-resource settings and displaced populations risks incorrect estimations of the prevalence of mental disorders, mis-conceptualizing traumatic reactions, and missing local idioms and other expressions of distress (Summerfield, 2010). In Lebanon and neighboring countries, despite progress in the validation of existing instruments for children and adolescents (e.g., Karam et al., 2019; Zeinoun et al., 2013), there remains a shortage of reliable and valid assessment tools (Maalouf et al., 2019). This is particularly the case for Syrian refugees living in ITSs in Lebanon. The current limitations of assessment measures for this population and context have critical implications for screening and referring children in need of mental health care, establishing the prevalence of mental health problems to facilitate service planning, and conducting research that helps develop theory and guide the development of interventions.
Our recent research utilized a structured clinical interview, the Mini International Neuropsychiatric Interview for Children and Adolescents (MINI Kid 6.0; Sheehan et al., 2010), for the purposes of screening children for a clinical trial and examining the reliability and validity of a range of widely used questionnaires for depression, anxiety, PTSD, internalizing and externalizing behavior problems, and functioning in a sample of 8–17-year-old Syrian children living in ITSs in the Beqa’a region of Lebanon (ClinicalTrials.gov ID: NCT03887312; McEwen, Moghames et al., 2021; Pluess et al., 2019). Whilst we took care to use a well-established and locally translated interview, challenges associated with the administration of the interview and its interpretation arose that required clinical judgement and localized contextual knowledge to address. This article therefore aims to review and share the challenges and solutions generated throughout the process of conducting these structured mental health assessments with Syrian refugee children and adolescents in ITSs in Lebanon, in order to help support the work of mental health agencies, organizations, and services in the same setting.
Methodology
This article draws on clinical supervision records collected as part of a clinical trial of phone-delivered psychological therapy and research that aimed to validate screening questionnaires for internalizing and externalizing disorders against structured clinical interviews in 8–17-year-old Syrian refugee children in Lebanon (McEwen, Moghames et al., 2021; Pluess et al., 2019). The data included in this article were obtained from challenges recorded as part of data collection, and extensive observations, reflections, and discussions recorded through clinical supervision with the field workers.
Participants
For the larger cohort study from which records for participants were drawn, inclusion criteria were: (i) aged 8–16 years at recruitment; (ii) had left Syria because of the war in the past four years; and (iii) the caregiver gave informed consent and the child gave assent to participate. Settlements across the Beqa’a region were selected to represent a range of levels of vulnerability, based on UNHCR ratings, and 77 small–medium sized settlements were chosen. All eligible families in these settlements were offered inclusion and the resulting sample size for the original study was n = 1,594 child-caregiver dyads at baseline (McEwen, et al., 2022). A follow-up assessment was conducted 12 months later with n = 1,001 families.
A subsample of the original sample participated in structured clinical interviews. This subsample was weighted to reflect the original sample in terms of risk of mental health problems (based on whether or not they indicated that the child needed mental health services and their scores on several questionnaires used to screen for common mental disorders). The resulting sample of records is therefore approximately representative of the population from which it is drawn in terms of risk of mental health problems, as well as age and sex of the child. The total sample size of records of included families is n = 119.
The current study was granted ethical approval by the Institutional Review Board (IRB) at the University of Balamand, Lebanon (ref: IRB/O/011-19/1815) and approved by the Ministry of Public Health (MoPH) in Lebanon (ref: 11068/1/19). The clinical study on phone-delivered therapy was granted ethical approval by the IRB of the American University of Beirut (ref: SBS-2017-0429) and the MoPH (ref: 2017/4/49165).
Measures
Participants underwent a structured clinical assessment using the MINI International Neuropsychiatric Interview for Children and Adolescents (MINI Kid). The Clinical Global Impression (CGI) severity scale was used to assign a severity rating based on information collected during the MINI Kid assessment.
The MINI Kid
The MINI Kid (Sheehan et al., 2010) is a structured diagnostic interview for children and adolescents, assessing a wide range of mental disorders based on the Diagnostic Statistical Manual (DSM). The MINI Kid has been found to have acceptable reliability and validity for both community and clinical samples, with comparable psychometric properties to other structured diagnostic assessments (Duncan et al., 2018), albeit with some variation across disorders (Högberg et al., 2019). The Arabic version 6.0 for Lebanon was administered, as the more recent version 7.0.2 of the MINI Kid, based on DSM-5 criteria, was not available at the time of data collection. Separate questions that aimed to gather sufficient additional information to allow assessment of symptoms against DSM-5 criteria were developed by one of the authors (TB), an experienced doctoral-level clinical psychologist in Lebanon, to administer during the same appointment. The MINI Kid 6.0 Arabic version for Lebanon followed a systematic process of translation headed by a consultant with knowledge and experience in the field of clinical outcome assessments, including forward translation, back translation, review by the author of the MINI Kid, review by a local clinician and a local coordinator. Quality control by linguists and discussion with the consultant about translation decisions were included at each step of the process (Mapi Research Trust, 2021, p. 1).
Clinical Global Impression severity
Clinical Global Impression severity (CGI-s) (Busner & Targum, 2007) scores were assigned to quantify symptom severity and global functioning. The CGI-s is a summary measure based on clinical judgment using all available information, including symptoms, history, context, and functioning. Ratings ranged from 1–7 and the process of assigning a score was operationalized (see McEwen, Moghames et al., 2021), to assist clinical judgement and improve inter-rater reliability. The CGI-s has been extensively used for clinical and research purposes, and has been found to have acceptable validity and reliability when used for a range of psychiatric disorders (Spielmans & McFall, 2006; Zaider et al., 2003).
The assessment was conducted by a masters-level clinical psychologist in the majority of cases (n = 101) and trained mental health case managers in the remaining cases (n = 18). All assessors were Lebanese, native Arabic speakers, and experienced in working with Syrian refugee populations in Lebanon. Supervision and joint supervision were provided by a doctoral-level clinical psychologist (TB). Assessments were conducted with children and their parent(s) unless the child was 13 years old or more, in which case, depending on the comfort level of the child, they were interviewed alone. In these cases, parental report was taken separately and incorporated into decision-making. Final diagnostic decisions were made during regular supervision meetings, based on the following criteria: (i) definite diagnosis of a mental disorder assigned based on information from the MINI Kid and clinical judgement, and (ii) CGI-s score ≥ 4, indicating moderate to severe functional impairment and/or distress. Children with evidence of symptoms but not meeting criteria for a mental disorder were classified as having subclinical difficulties.
For reliability, N = 10 interviews were rated and coded separately by two independent raters. Interrater reliability was acceptable to excellent for most ratings, including the CGI-s score (intraclass correlation [single measures] = .78, p<.01) and diagnostic judgements (kappa = .47–1.00, all p<.05). It was not possible to calculate kappa for panic disorder, substance misuse, and ADHD because one rater had rated all children as not affected (i.e., rated as 0)—in these cases, raw agreement was 0.90; the small sample size for double coding and low prevalence of these disorders resulted in this problem in calculating kappa. Agreement for conduct disorders was poorer (kappa = .41, p = .08; see below for discussion about conduct disorders). Discrepancies in administration or coding were discussed in joint supervision sessions with all involved field workers to improve consistency in administration and coding.
Clinical supervision information was recorded by the supervisor (TB) and consisted of the final agreed-upon diagnoses for each child. Process notes were also recorded in a ‘challenges’ table that was updated after every supervision session, along with discussion, agreements and outcomes of solutions, and the IDs for the participants whose assessments triggered the discussion.
Procedure
Participants were contacted as part of the study and not self-referred. Eligible participants were contacted by telephone, and those that expressed an interest were visited at home (n = 114) or attended the clinic (n = 5) where consent/assent procedures were completed. The parental consent and child assent procedures were conducted in-person using IRB-approved forms in age-appropriate Modern Standard Arabic. Due to low literacy in the population, research staff also read out the forms and discussed any concerns using Arabic dialect familiar to participants. Staff also used visual aids to clarify study requirements (e.g., nature, order, and timing of study events). Both parents, where possible, and participating children gave written consent or assent to participate. If participants were unable to give written consent/assent, they either provided a thumbprint in lieu of a signature or a witness independent from the study team was asked to stay during the consent/assent process and confirm consent/assent (usually a trusted relative or friend). All participants were given a copy of the forms. If parental consent and child assent were given, assessment measures were then administered. Participants were recruited and assessed between December 2018 and August 2019. Where there was an indication of a need for services, whether or not they consented/assented to research, treatment was offered at no cost.
Supervision was conducted weekly via Skype, with monthly supervision in person at the clinic in Zahle, Beqa’a. During supervision, clinicians reported on (1) characteristics, context, and history of each child and family; (2) diagnostic criteria met using the MINI Kid; (3) symptoms and symptom clusters that did not meet diagnostic criteria; (4) qualitative descriptions of symptom clusters; (5) functional impairment and distress of the child to inform a CGI-s score; and (6) challenges or inconsistencies in conducting the assessment, using the measures, and in diagnostic decision-making, with careful consideration for culture and context. Alongside documenting the assessment outcomes for each child, every supervision session required record-keeping on (a) any changes in diagnostic assignments as a result of supervision, (b) any clinical risk and risk management plans, and (c) challenges and agreed-upon strategies to address challenges in future assessments. Challenges and suggested solutions were shared via email to the wider clinical and research team to ensure that issues were immediately addressed and that assessments remained consistent across clinicians and teams.
Analysis
Challenges that were recorded in clinical supervision were compiled by the supervisor (TB) and reviewed by the primary assessor (VK) to ensure the challenges were exhaustive. Question-specific challenges and solutions were listed separately in a table in order of MINI Kid entry by the supervisor (TB). Remaining challenges were then analyzed using Thematic Content Analysis independently by two members of the research team (TB and VK), in keeping with standard practice in qualitative analysis (Braun & Clarke, 2006). The challenges were first read and re-read with open coding for emerging themes, then organized with overlapping codes amalgamated into core themes. Themes were then compared between the two research members, and discrepancies resolved through discussion and third-party support from FM and PM. The final themes were approved with the consensus of the whole study team. Lastly, examples were selected by TB and VK to illustrate each theme.
Results
Thematic content analysis revealed five themes reflecting the main challenges of conducting structured clinical assessments in ITSs in the Beqa’a with Syrian refugee children: (1) practical and logistical challenges, (2) validity in interviewing, (3) sensitivity to cultural norms and meaning, (4) sensitivity to contextual norms, and (5) co-morbidity and formulation. These were the main discussions that dominated decision-making related to accessibility, assignment of diagnoses, and referral, and are outlined below. Examples for each theme are presented in Table 1. Detailed item-specific challenges and recommendations for the application of the MINI Kid in ITSs in Lebanon are provided in Supplementary Table S1.
Case examples, by theme.
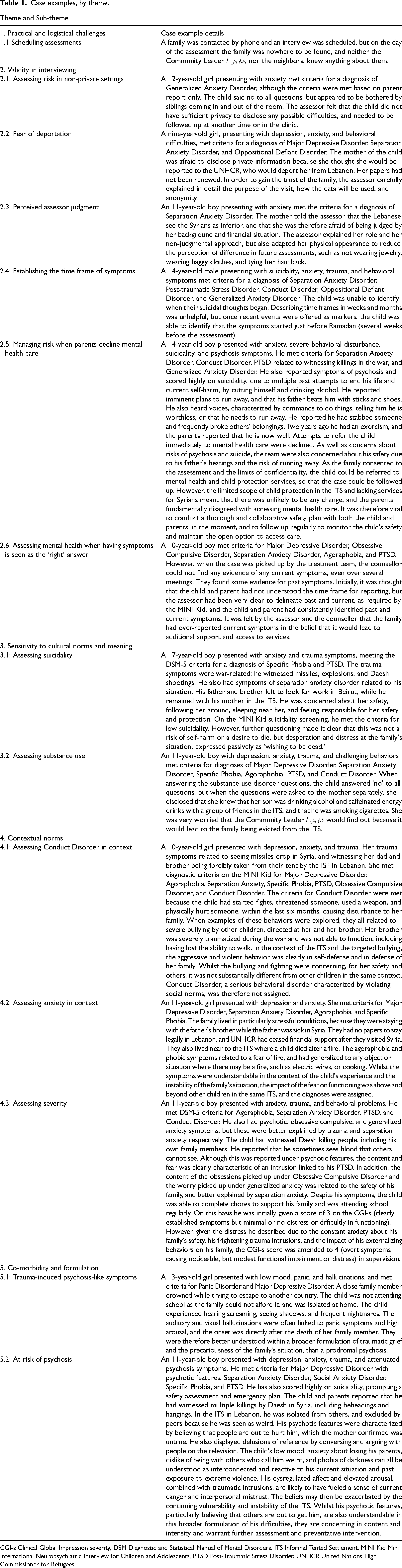
CGI-s Clinical Global Impression severity, DSM Diagnostic and Statistical Manual of Mental Disorders, ITS Informal Tented Settlement, MINI Kid Mini International Neuropsychiatric Interview for Children and Adolescents, PTSD Post-Traumatic Stress Disorder, UNHCR United Nations High Commissioner for Refugees.
Practical and logistical challenges
Practical and logistical challenges during data collection reflect the difficulties in conducting home-based assessments in ITSs with sufficient time and privacy. Challenges identified related to the often-changing plans of refugee families and competing demands on their time, their limited access to a phone, and their temporary residential locations, as well as limited access or availability of child protection and specialist mental health services.
The majority of interviews were scheduled a day in advance, but families’ plans would change quickly and they would often no longer be available at the agreed-upon time. They may have found work for the day, or had a UNHCR appointment or a medical appointment. Many families also shared a phone with other families, and often did not answer when called. Some families left the settlement or tent, for other tents or settlements, for cities, for Europe, or to return to Syria. A small number of families could not be found and even neighbors and community leaders did not know where the families had gone (see Table 1, example 1.1). These challenges highlight the changeable nature of day-to-day life in the settlements, and that typical diary-based appointment systems are limited in this context, instead requiring flexibility and speed in responding to families as soon as they have space and time. Assessors would call on average three times before an assessment, the first time to identify availability, the second to confirm (usually the day before), and the third just before traveling to the ITS. Additional practical challenges included emergencies related to the living conditions in the ITS, such as major floods and snow, that would cause families weeks of distress as they tried to protect their homes and belongings.
Other challenges related to limitations in the broader service structure, in terms of having viable options to be able to refer concerns arising from assessments to child protection services or specialized mental health care. In cases of suspected maltreatment, we often had to rely on individual case managers, predominantly employed through non-governmental organizations, to work with families to reduce maltreatment, and to monitor safety. In addition, children requiring specialist treatment had to be referred to general mental health services, as specialized providers could not be found in the area, such as in the case of psychological therapy for adolescents at high risk of psychosis.
Validity in interviewing
In addition to challenges associated with culture and context in using the MINI Kid, we also noted frequent concerns about the validity of answers, which were likely impacted by issues including privacy, trust, estimating timeframes, perceptions of mental health and stigma, and false positives driven by contextual factors.
Privacy
As the majority of assessments were conducted in people's homes in ITSs, we faced challenges in ensuring privacy and confidentiality. Tents tended to have large numbers of family members living under one roof, with canvas walls that did not block out sound, and often with only one room. This meant that siblings were often coming in and out of the room, or could be heard through the wall. This was not conducive to talking about difficulties (see Table 1, example 2.1), and may have impacted what was reported. For example, the reporting of substance use was lower than expected compared to the population average (Maalouf et al., 2016) and our clinical experience in the same setting. Assessors used different ways to overcome these challenges, trying to schedule meetings when siblings were out, or using visual aid material that the child could point to when he/she did not want to answer out loud. Visual aids included images of thumbs up and down or time frames depicted in diagrammatic form, that could be pointed to.
Trust
For some of the assessments, the assessor was only able to meet with the families once, and this was felt by the assessor to be insufficient to build trust. This was less of an issue for families in which a child subsequently received treatment. The building of a trusting relationship was found to be as important for the assessment process as for treatment (see Table 1, examples 2.2 and 2.3).
Estimating time frames
Establishing a time frame for symptom onset and development was challenging in the context, when even parents found it difficult to estimate duration or a point in time. Following instructions in the MINI Kid to use personalized timing, assessors used other ways to reference time than days and months, and used instead landmarks in time such as before or after Eid, or before or after leaving Syria (see Table 1, example 2.4). Visual aids were also helpful to convey a sense of time. Often, even short periods of time, such as two weeks, were difficult to conceptualize and required more regular events, such as fathers leaving for Beirut at the beginning of the week or going to the Mosque for Friday prayers, as reference points.
Perceptions of mental health and stigma
In some cases, particularly for children presenting with psychotic features, families believed that the child was possessed and brought them to a Sheikh to pray, declining to go to a psychiatrist or psychologist because they either did not believe that it was mental health related or because they feared the stigma of accessing mental health care. This made some questions difficult when the underlying etiological assumption was different from that of the family, and the assessor needed to respect the families’ beliefs whilst also assessing the child, providing psycho-education and referral options, and managing risk (see Table 1, example 2.5).
False positives
It was noted that poor living conditions and desperation fed into a contextual culture of giving false positives (i.e., reporting symptoms above and beyond what the child seemed to be experiencing), in the hope of receiving higher compensation or access to mental health, other services, or resettlement (see Table 1, example 2.6). Follow-up and exploratory questions, including reminding participants that there were no right or wrong answers, as well as detailed discussion in supervision were necessary to identify these false positives. In one family, a different child was presented to assessors at a follow-up assessment. It was felt that the family had done this in order to get both of their children assessed. Assessors tried to make it clear to families that any child or adult in the community could be assessed and access mental health services free of charge, to reduce the risk of this issue.
Sensitivity to cultural norms and meaning
Cultural differences in the meaning of a number of MINI Kid items were found, predominantly for suicidality, conduct disorders, substance use disorders, and panic. A large number of children and adolescents screened positively for a low level of suicidality on the MINI Kid based on positive responses to the same questions, all related to ‘wishing to be dead.’ With further clinical assessment for risk, it was clear that the child or adolescent had no active suicidal thoughts or plans. Instead, the questions they were saying yes to were culturally common ways of speaking, using ‘I wish I were dead’ ( اتمنى أن أكون ميتاً / أموت أتمنى أن / أموت ريتني) as an expression to communicate being tired or fed up, but without reflecting low mood or suicidality (see Table 1, example 3.1). Given the stigma surrounding suicide, we had also initially included a script to explain why we ask these questions, before asking them. However, it was noted that this lead-in seemed to coach the family into minimizing answers, and may have been counterproductive, assuming shame when it might not have been felt. We therefore removed the script, and only used it when families appeared offended or expressed offense. All assessors felt this strategy was more appropriate and that they were able to obtain more meaningful responses from children. Through open discussions about hopelessness and suicidal feelings, which were common in the sample at 16.5%, we were able to offer additional support to children and parents. The same script strategy had been used for substance use questions, with the same side effect, and was also removed. Concerns were raised that the script would contextualize substance use as shameful and reduce the likelihood of discussing it openly. Substance use, especially alcohol, is forbidden in most ITSs, and despite assessors’ efforts to provide a safe space to discuss it, few children (1.7%) reported use and none met criteria for a disorder (see Table 1, example 3.2). Finally, the word ‘crazy’ is used in the assessment of panic disorder (‘were you afraid you were going crazy?’). The Arabic equivalent ‘مجنون/ اخوت’ (majnoon) was felt to carry too much stigma and may cause offense to families, so the alternative ‘losing my mind’ or فقدت عقلك/صوابك (fakadet aaklak) was used instead.
Sensitivity to contextual norms
A recurrent theme during diagnostic decision-making centered on the extent to which symptoms were normal or adaptive in the context of displacement, poor living conditions, and social stress. This challenge strongly reflects the wider challenge of using assessment tools based on the DSM. The ethical dilemma was a constant concern. On one hand, a child may meet criteria for a disorder and require treatment, but on the other they may be given a psychopathological label for a rather normal or adaptive reaction to current stressors or circumstances. We were frequently concerned that such labels may over-emphasize individual pathology or lead to inappropriate treatment options, particularly for children meeting criteria for Conduct Disorder, Major Depressive Disorder (MDD current), Agoraphobia, Panic Disorder, and Obsessive Compulsive Disorder.
ITSs are not safe spaces for children, due to the poor infrastructure, lack of space, and the large number of families living in them. Many children fight with other children in order to defend themselves or their siblings. The settlements in the Beqa’a valley are also usually located between agricultural fields, lakes, and farms, which allow animals to enter. Many children described that they often beat animals because they get scared. In addition, the tents are small and densely populated, leading to frustration and animosity, and frequent fighting with parents and staying out late. These kinds of behaviors were being picked up as conduct disorder when in reality they were often adaptive responses to an overwhelmingly challenging situation (see Table 1, example 4.1). Furthermore, children who had recently experienced beatings at home, school violence (peers and teachers), or had lost access to school, met criteria for MDD when these symptoms could be understood as a normal reaction to recent loss or helplessness. Agoraphobia and Panic Disorder were also picked up to a greater extent during turbulent times in the ITSs, such as when there were more frequent Internal Security Forces (ISF) searches, arrests, destruction of property, and evictions; and after a fire in an ITS that killed a child. Anxiety spiked at these times, with fears related to seeing a soldier or hearing shouting, and frequent checking of stoves to prevent fire (see Table 1, example 4.2). Obsessive Compulsive Disorder's MINI Kid criteria were also commonly met on the basis of time-consuming praying and worry about family safety. However, the praying was often a coping mechanism within a religious context in which structured and frequent praying is encouraged, that gave children a sense of safety and reassurance in a higher power and purpose. The worry itself was also often normal within the child's experience, where risks to family safety were high. Identifying the relevance and ethics of a DSM-5 diagnosis when a child was experiencing an understandable reaction to difficult or even traumatic situations could only be resolved through discussion on a case-by-case basis, incorporating context and timing, and often involving other team members, with the best interests of the child at the center of the decision.
The CGI-s, which includes consideration of functional impairment and distress, was helpful in informing this decision, but again required taking context into account. Given that many children did not have much choice about their activities (such as needing to work to be able to meet basic needs), many were performing at higher levels of functioning than they would have done in another context, and this was not reflected in CGI-s scores unless subjective distress was given sufficient weight when assigning scores (see Table 1, example 4.3). Clinical judgments about subjective distress based on the overall assessment and presentation of the child were imperative to inform a valid level of severity.
Other contextual challenges specific to this population included picking up on depressive-like symptoms (appetite and sleep changes, fatigue) during fasting in Ramadan, a general lack of understanding of mental health terminology in the MINI Kid (for obsessions and compulsions, panic, agoraphobia, and mania in particular), separation anxiety related to non-parental figures such as older siblings and friends, and difficulty in assessing early cognitive and behavioral development when this coincided with the start of the war and trauma exposure. Clinical judgement on a case-by-case basis and with supervisor support was required to address all these challenges.
Comorbidity and formulation
Overall, comorbidity was high, with 52.9% of children meeting the criteria for more than one disorder. Out of all comorbid cases, 68.3% included a diagnosis of PTSD. In these cases, the comorbid disorders were often trauma related, such as separation anxiety, agoraphobia, behavioral problems, obsession and compulsions, worry, and visual and auditory hallucinations (see Table 1, examples 5.1 and 5.2). It was clear during assessments that many of these difficulties and disorders were connected, and part of a broader traumatic and adjustment reaction to the violence and displacement families had suffered. Whilst a diagnosis was helpful to inform the validation study by setting a reference standard with which to compare frequently used self- and parent-report mental health measures, and to inform eligibility for treatment, it was not sufficient to inform treatment itself. A broader formulation of the connections between experience, pre-existing difficulties, and symptomology was needed. This formulation was vital for clinicians to inform an overall conceptualization of how the symptoms developed and were being maintained, and how treatment should be organized to best address the needs of the child.
Discussion
This article aimed to review challenges and solutions derived from the administration and clinical supervision of a structured diagnostic clinical interview, using the MINI Kid and an operationalized approach to the CGI-s, with Syrian refugee children resident in ITSs in Lebanon. Whilst the use of structured questions was found to be useful in providing a framework for assessments, a number of challenges were faced which may affect the cultural and contextual applicability of DSM-based structured interviews in this population. The findings of this study are in line with past research on the mental health of Syrian refugee children that found a high level of distress (Charlson et al., 2019) as well as challenges in reliably assessing mental health using existing measures (Hassan et al., 2016). The findings are also in line with broader challenges in the administration of the MINI Kid and other structured diagnostic tools in other populations and contexts, with relatively high variability across disorders (e.g., Högberg et al., 2019).
Improving access to appropriate mental health assessments and treatment
We identified barriers in accessing vulnerable families, ensuring privacy and trust, and managing power dynamics in relation to perceptions of giving ‘right’ answers to gain compensation or access to services or resources. These barriers have been identified in other Syrian refugee contexts, in terms of both assessment and treatment. Hassan et al. (2016) identified issues of power, neutrality, and stigma, where refugees feel a loss of control and inferiority in their position, and require sensitive treatment planning to re-balance the power disparity to ensure that decision-making is collaborative. This is ever more important in the context of mental disorders, where disempowerment and the violation of basic human rights is widespread even in non-refugee settings (Puras & Gooding, 2019). It may also be related to the differential power relationship inherent in a research study. The challenge of privacy identified in this study has been less well-reported, and may be specifically relevant for home-based assessments, and treatment, in ITSs. Such settings are poorly constructed, with cramped spaces and thin walls. They are designed to be ‘temporary,’ and any attempt to ameliorate the structure or services results in retaliation from the Lebanese state. Given this, the spaces are not ideal for mental health care, but whilst clinic-based assessments are more common, home assessments were found to improve access given the costs and time burden associated with traveling to the nearest clinic. In a parallel intervention study, we found a high level of pretreatment dropout in the same population, largely associated with practical barriers to accessing the clinical setting (Hanna et al., 2022).
In order to address these challenges, we recommend that assessors are available quickly and at the timing, and place, that fits with the families’ current schedule. School times (which are often delivered in segregated shifts based on nationality and demand), UNHCR appointments, weather, and employment are changeable on a daily basis, and services must be able to respond to this. Appointment-based diary systems on a Monday to Friday, 9am to 5pm schedule are not suitable to match the needs of Syrian refugees in ITSs. Appointments must be available in the evenings and on weekends, factoring in Ramadan and agricultural harvest seasons, particularly if fathers are to be involved in their child's care. Assessments also need to be organized carefully to maximize the possibility of privacy. This includes asking about when siblings or other family members are most likely to be out of the home and arranging appointments accordingly, or inviting families to clinics and covering transport costs. Meeting families more than once is also likely to improve the validity of answers, when a trusting rapport has been built up. Differences in perceptions can also be more easily respected whilst still probing for clinical information, when it is done within the context of this trusting relationship. The tendency for agreeableness to seek additional compensation, resources, or services is endemic in this population, understandably, given the poor access to basic rights and services. This can only be addressed through a trusting relationship and by repeating to participants that any potential benefits received are not based on the answers given in the assessments, and that referrals can be made to mental health services and other services regardless of the outcome of the assessment. The tendency should be noted and considered when interpreting assessments. Experienced assessors are skilled at picking up on odd or unlikely answers, parental pressure on children to give the ‘right’ answer, and subtle requests for support or services. However, reflection and supervision is also crucial to ensure that these concerns do not become assumptions that could lead to unintentionally under-estimating distress or withholding referrals to care.
Cultural relevance
Challenges identified in this study related to culture are supported by literature critical of the use of DSM-based assessment tools to assess populations in the global south. The language of such tools is criticized for being inherently biased towards North American and Western European conceptualizations and expressions of mental health, which will inevitably miss or misinterpret other languages of distress (Kirmayer, 2001). Studies attempting to match idioms of distress to DSM-based psychiatric diagnosis have shown that expressions often do not map clearly onto specific disorders, but rather relate to broader categories, such as depression and anxiety (Cork et al., 2019), and that an integration of local idioms of distress into structured interviews is required to improve the relevance and accuracy of assessments (Kohrt et al., 2016). Syrian Arabic is bursting with expressions, metaphors, and analogies, which can be used to express concern or tiredness but also worry, dysphoria, and hopelessness (Hassan et al., 2015). Our experience of screening for suicidality is a good example of the risk of such idioms being misinterpreted, where expressions of tiredness can be interpreted as an immediate risk to safety. We echo the need to incorporate local idioms of distress and contextual understanding into the assessment process, and recommend follow-up and exploratory questions beyond those of screening questions for specific disorders, comprehensive training including role play and mutual observation, regular and in-depth clinical supervision, and trust in local clinical judgment, in order to reflect more accurately the presenting difficulties and make appropriate treatment referrals. We found the clinical judgment of field staff to be essential, and this cannot be easily manualized. The MINI Kid encourages rephrasing or using locally relevant examples to aid understanding, and we found this to be a vital part of the process. This is in line with research in other refugee populations, where building a trusting relationship, paying attention to linguistic and cultural nuance, and taking a flexible adaptive approach to assessments were core recommendations (Hsu et al., 2004; Wylie et al., 2018).
Contextual relevance
In addition to criticism about cultural appropriateness and relevance, the use of North American and Western European assessment tools with refugees has elicited criticism on contextual grounds. The underlying assumptions of these tools are argued to have individualized collective suffering, pathologized reactions to unbearable circumstances, and placed the origin of the difficulty in the individual instead of social environments rife with inequality and injustice (Summerfield, 2010). The DSM-based categorization of distress has long been questioned by leaders in the field of cross-cultural and global mental health, with a growing focus on understanding distress based on the experience of the surrounding general population, not clinical specialist settings (Patel, 2014), and on reflecting culture and context (Kirmayer, 2001). This can be illustrated through the example of Conduct Disorder. In the current study, many children met MINI Kid criteria on the basis of a list of behaviors and a cutoff derived from non-conflict affected and non-displaced populations. Even in high-income countries, conduct disorder and oppositionality are consistently found to be higher in families of low socio-economic status, particularly when the family live in a deprived neighborhood and have a low income (Murray & Farrington, 2010). The mechanism explaining this link is proposed to be the effect of deprivation and adversity on parenting capacity, practices, and monitoring (Fergusson et al., 2004). This is not to deny other risk factors related to individuals, such as genetic risks or impulsivity, but to acknowledge the environment and its influence on a child's behavioral socialization. The behavior of a child brought up in an ITS in Lebanon, who works on the street selling tissues every day, exposed to the weather, pollution, intimidation, and violence, cannot be compared to the behavior of a middle-class schoolchild in North America. A certain level of fighting, aggression, and oppositionality is normal, and may even be adaptive and promote survival. Research in other conflict-affected contexts has shown that aggressiveness is associated with resilience and lower PTSD symptoms (Weierstall et al., 2012). While the DSM-5 does explicitly encourage clinical judgment based on the child's context, albeit with remaining limitations in scope and practical utility (Bredström, 2019), a DSM-based tool will find this nuance harder to achieve. A checklist cannot categorize and quantify behaviors that are assumed to be universally acceptable or not. Such tools can provide a valuable structure, based on well-established broad categories of symptomology, that can be used between contexts and populations by trained non-specialists to inform comparable prevalence estimates, and inform treatment and referral. In our experience, however, additional exploration under the supervision of a specialist clinician and informed by local expertise is essential to explore risky and concerning symptoms, grounded in the environment and experience of the child and caregivers. We therefore recommend an awareness and integration of the child's social context into the assessment process, to inform diagnosis, formulation, and treatment. Specifically, follow-up questions must be asked in relation to whether the reported symptoms are above and beyond other children in the same context. When framed this way, the assessor is more able to reflect on the presenting difficulties in context, which can be supported through a supervision structure that provides space for reflective discussions about culturally and contextually grounded conceptualizations of the difficulties, to better inform diagnosis, treatment, and referral.
Formulating complex symptomology
We identified a broad range of inter-linking symptoms that did not clearly map onto separate individual diagnoses, and that could be better understood through an inter-connected formulation of experience rather than separate but comorbid disorders. The need for ‘joined-up thinking’ in assessing children, rather than ending the assessment with a list of comorbid disorders, is a core recommendation arising from this study. Structured assessments like the DSM-based MINI Kid tend to separate symptoms into clusters in a way that may be miscommunicated to families, particularly in low resource and non-specialist contexts. The message received by families at the end of the assessment process should be in the format of a digestible formulation, a narrative, in line with best practice in clinical psychology (Johnstone, 2017). This can help to normalize the child and family's reactive experience and validate their distress, whilst also providing a rationale for, and to inform, treatment.
Strengths and limitations
This is one of the few reflective studies to report on the challenges of assessing the mental health of Syrian refugee children, benefitting from a representative sample in ITSs in the Beqa’a, and comprehensive assessment and supervision of each case. The study is limited, however, by a small sample size that may not be representative of all Syrian refugees in Lebanon, nor of other refugees and other living conditions. It is also limited by the restricted time that assessors could spend with each family, by conducting most assessments in homes rather than clinics, and with families that were included in a research study and not those who sought mental health care independently. This means the sample included a range of severity of difficulties that may not be representative of help-seeking families.
Implications and conclusions
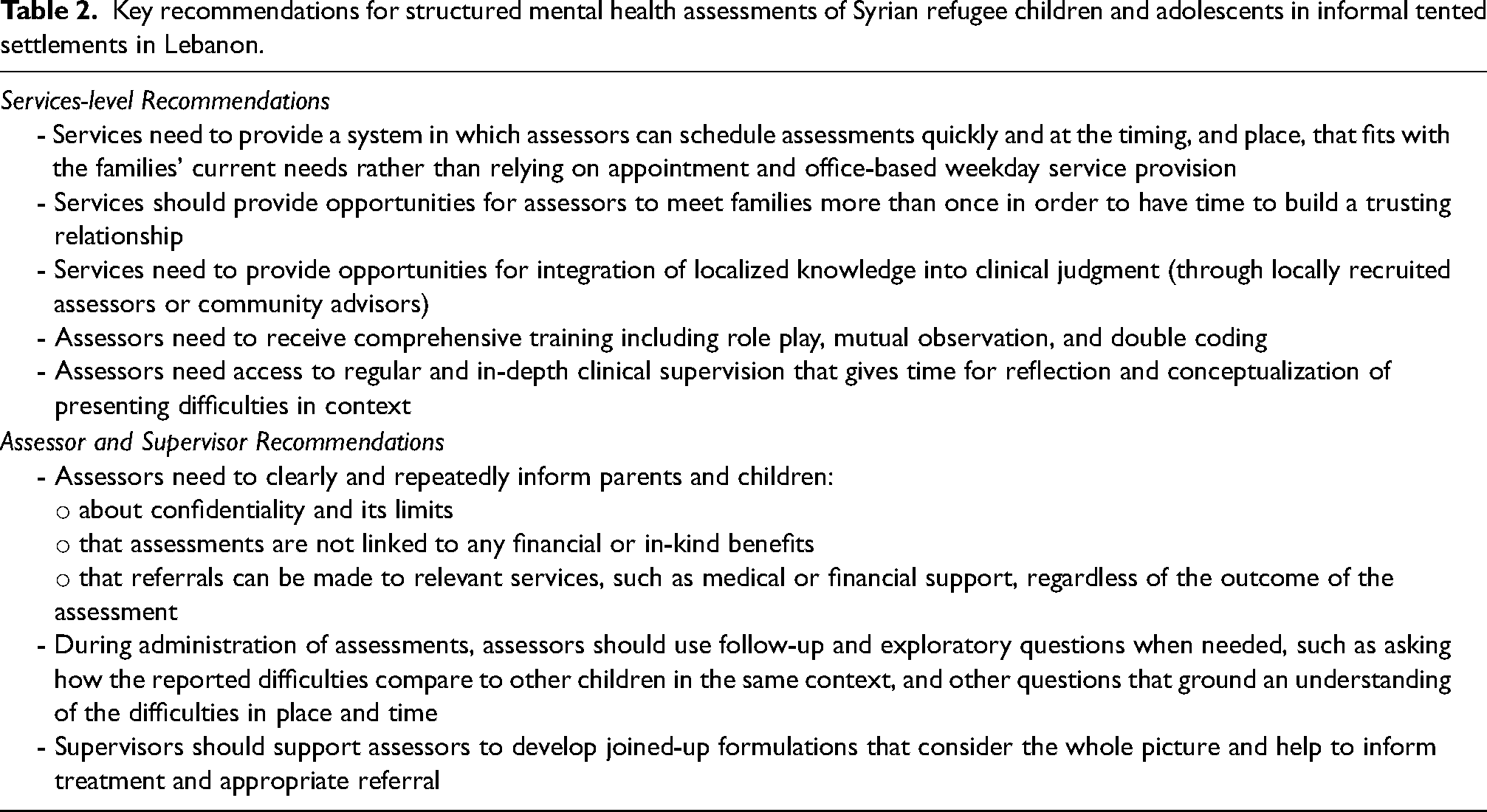
This study has identified core challenges in using a structured clinical assessment with Syrian refugee children and adolescents in ITSs in Lebanon, as well as ways to improve the relevance and quality of these assessments. Most significantly, this translates to the need for improved accessibility, sensitive follow-up and exploratory questions, regular supervision, incorporation of local clinical knowledge and judgement, and the conceptualization of inter-linked difficulties within the broader social context (see Table 2). These adaptations, specific to the population and setting, are essential to improve the accuracy and meaning of data on mental health, to estimate prevalence rates more accurately, to inform appropriate treatment plans, and to improve mental health systems delivery and reforms. The tendency to rely only on universal DSM-based criteria risks placing the pathology within the individual, which can be dangerous when applied to groups experiencing ongoing social injustice, poverty, and extreme inequality. Individualized thinking may lead to inappropriate treatment that neglects wider systemic and structural problems. Evidence from reviews of mental health and psychosocial support in conflict-affected and displaced populations repeatedly highlights the lack of attention to systemic and public health programs of care (Betancourt et al., 2013; Jordans et al., 2009, 2016). Through meaningful assessments that reject simplistic interpretations of mental health symptoms, that are sensitive to culture and context, we will be better able to address the complex individual and systemic influences on child wellbeing.
Key recommendations for structured mental health assessments of Syrian refugee children and adolescents in informal tented settlements in Lebanon.
Supplemental Material
sj-docx-1-tps-10.1177_13634615221105114 - Supplemental material for The culturally and contextually sensitive assessment of mental health using a structured diagnostic interview (MINI Kid) for Syrian refugee children and adolescents in Lebanon: Challenges and solutions
Supplemental material, sj-docx-1-tps-10.1177_13634615221105114 for The culturally and contextually sensitive assessment of mental health using a structured diagnostic interview (MINI Kid) for Syrian refugee children and adolescents in Lebanon: Challenges and solutions by Vanessa Kyrillos, Tania Bosqui, Patricia Moghames, Nicolas Chehade, Stephanie Saad, Diana Abdul Rahman, Elie Karam, Georges Karam, Dahlia Saab, Michael Pluess and Fiona S. McEwen in Transcultural Psychiatry
Footnotes
Acknowledgements
Data collection for the validation study was funded by an award from TIES/NYU as part of the 3EA | MENAT Measurement Initiative (Subaward: S4323-04). The cohort study is funded by the Eunice Shriver National Institute of Child Health & Human Development (NICHD; R01HD083387). The clinical trial on phone-delivered therapy is funded by Elrha's Research for Health in Humanitarian Crises (R2HC) Programme, which aims to improve health outcomes by strengthening the evidence base for public health interventions in humanitarian crises. R2HC is funded by the UK Foreign, Commonwealth and Development Office (FCDO), Wellcome, and the UK National Institute for Health Research (NIHR). Visit elrha.org for more information about Elrha's work to improve humanitarian outcomes through research, innovation, and partnership. The study was sponsored by Queen Mary University of London (QMUL). TIES/NYU, NICHD, Elrha and the sponsor played no role in study design, in the collection, analysis or interpretation of data, or in the writing of this report.
We warmly thank all participating families for their participation. Fieldwork was conducted with Médecins du Monde France (MdM) in Lebanon. We thank Patricia Moghames, Nicolas Chehade, Stephanie Legoff, Nicolas Puvis, Alaa Hijazi, and Zeina Hassan, and all other members of the research teams (![]() ) for their dedication, hard work, and insights.
) for their dedication, hard work, and insights.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Elrha’s Research for Health in Humanitarian Crises (R2HC), Eunice Shriver National Institute of Child Health & Human Development, TIES/NYU as part of the 3EA | MENAT Measurement Initiative, (grant number 28371, NICHD; R01HD083387, Subaward: S4323-04).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.