
Abstract
The Roma are Europe’s largest ethnic minority group, and often face discrimination and social exclusion. Social strife and lack of access to healthcare are associated with increased symptoms of psychopathology. We aimed to review evidence on mental health outcomes and on access to mental healthcare among the Roma population in Europe. We systematically searched five databases (PsycINFO, Global Health, Social Policy and Practice, Web of Science and PubMed) and conducted a grey literature search in August 2020. We identified 133 studies, 26 of which were included for final analysis. We present the results using a narrative synthesis. The available literature indicates a relatively high prevalence of anxiety, depression and substance abuse among Roma, and females seem to be more affected than males. Roma children exhibit more externalizing and internalizing disorders when compared with non-Roma children. Mental health and perceived well-being among the Roma population are strongly linked to social determinants of health such as housing or economic income. Access to mental healthcare is limited for Roma people because of several barriers pertaining to language, lack of information regarding available services, and the insurance and economic status of Roma people. Roma people report mainly negative experiences with mental health services, including a lack of understanding from healthcare providers, and instances of racism and discrimination. There is a need for more research on mental health and access to healthcare in Roma people. Future studies should be participatory in order to provide guidelines for mental healthcare that addresses the needs of the Roma population.
Introduction
Roma are the largest ethnic minority in Europe, with up to 12 million Roma living in the region (European Commission, 2014). Even though it is well-documented that Roma often face stigma and social exclusion across European states, their mental health is seldom studied (European Commission, 2014; Zeman et al., 2003). Currently Roma in Europe encompass several sub-groups, including Roma, Sinti, Kale, Boyash, Gypsies/Travellers, as well as Roma who have fully integrated into the majority communities (Alexiadou, 2018). Roma have lived in Europe since the 15th century as nomadic communities, often ostracized by the majority groups, and eventually targeted directly during both World Wars (Zeman et al., 2003). Roma have been discriminated against in employment, education, social situations and healthcare. O’Nions (2011) compared the situation of Roma living in Europe to an ‘apartheid’, in which Roma are, at least to some extent, denied most fundamental rights. Between 2004 and 2007, policy change primarily related to changes in legislation regarding discrimination of Roma, and awareness raising, was commenced and fuelled mainly by the European Union's (EU) anti-discrimination policy; however, most actions were left to Member States and remained largely unimplemented (O’Nions, 2011; Ram, 2007).
Research shows that access to healthcare for Roma is affected not only by socioeconomic status, but also by geographical isolation, lack of education on when to access care, communication obstacles, and by discrimination from healthcare staff (Földes & Covaci, 2012; Mladovsky, 2007). Furthermore, states often do not provide enough healthcare to underprivileged or vulnerable populations, such as Roma, who may not have access to health insurance and/or care, which makes them more at risk of health issues (Alexiadou, 2018). In addition, the needs of Roma populations across Europe lack representation both in research and advocacy, and without attention the health of Roma is rarely addressed by policy that could lead to change (Hajioff & McKee, 2000).
Although there is little research on the lack of access to adequate healthcare for Roma populations, there is even less research on mental healthcare access. Much like non-communicable diseases, mental health conditions have received much less attention than healthcare in general (Cook et al., 2013). However, several research projects and integration strategies have illustrated the importance of carrying out research on Roma health and healthcare access. One example is the Equi-Health project that ran from 2013 to 2016, which focused on Roma health, showing that involving health mediators from the community improves access to healthcare (International Organization for Migration, 2017). Integration strategies such as the EU framework for national Roma integration strategies up to 2020 and the recent revision until 2030, underline the importance of addressing health in relation to other socioeconomic factors such as improvement in access to safe housing and discrimination reduction (European Commission, 2020). Perhaps relating more to mental health, one of the targets of this new strategy is to ensure a five years longer life expectancy for Roma men and women. This goal is based on research showing that life expectancy is heavily impacted by mental health (Chesney et al., 2014).
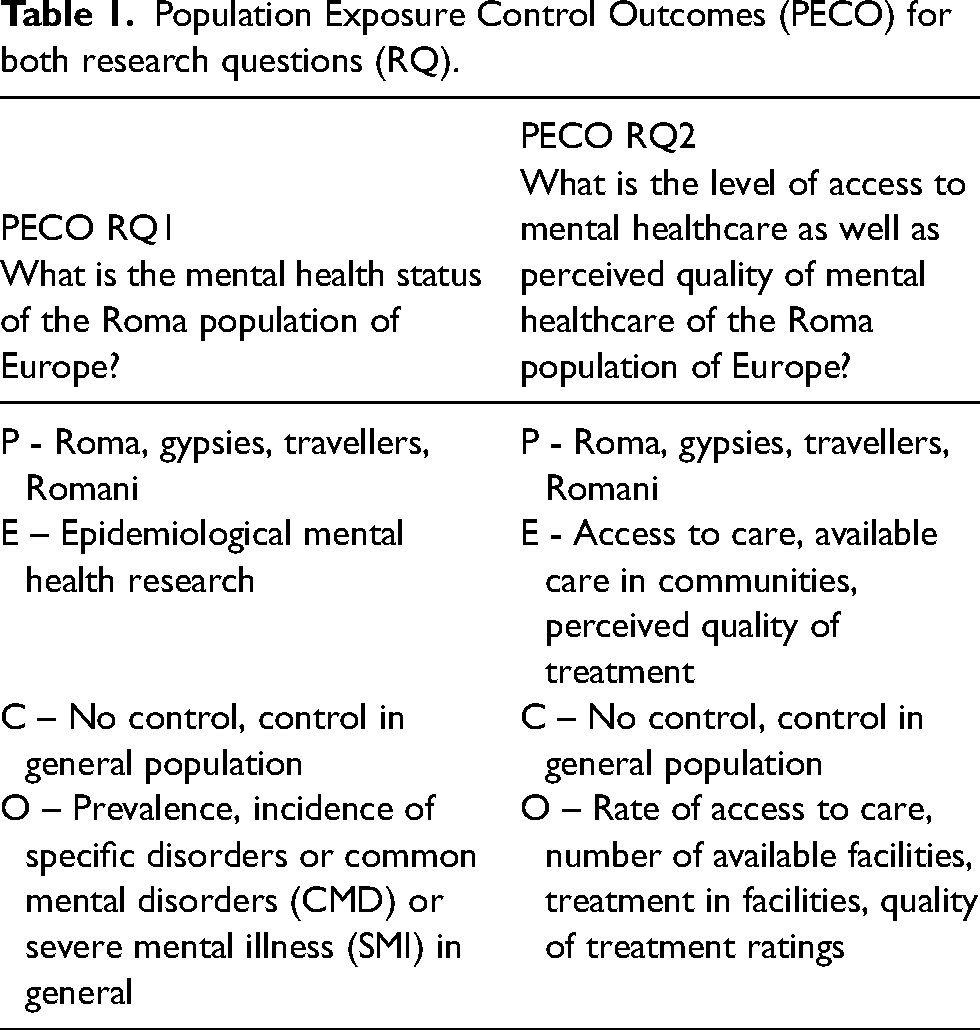
Against this context, we aimed to map mental health status and access to care among the Roma populations in Europe in order to answer the following questions: ‘What is the mental health status of the Roma population of Europe?’ and ‘What is the level of access to mental healthcare as well as perceived quality of mental healthcare of the Roma population of Europe?’. Mental health was defined as any diagnosed or self-reported mental illness as well as aspects of poor mental well-being such as stress. Access to mental healthcare was defined as the opportunities available to Roma to access psychiatrist, psychologist or psychotherapist care as well as the perceived quality of such care. Answering these questions should help in the process of designing and piloting interventions specifically focusing on the access to mental healthcare and mental healthcare literacy of Roma.
Methods
Scope of the review
We conducted a scoping review in order to explore the current literature and analyse the state of art with regard to the mental health status, morbidity and access to mental healthcare among Roma populations across Europe. We chose a scoping review method since it allowed to identify what research has focused on in this topic, and which concepts still remain to be explored (Schick-Makaroff et al., 2016). Furthermore, the topic of Roma mental health has not been extensively reviewed, which indicated the need to assess the literature via a scoping review (Levac et al., 2010; Lockwood et al., 2019; Munn et al., 2018; Pham et al., 2014). We followed the Joanna Briggs Institute guidelines for scoping reviews (Peters et al., 2015). This scoping review is reported according to the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) Statement which can be found in the supplementary materials.
Data collection
We systematically searched five different databases: PsycINFO, Global Health, Social Policy and Practice (Ovid), Web of Science and PubMed. We also utilized the meta search engine DogPile and the search engine Google Scholar for grey literature search in English, French, Spanish and Italian. The date of the last search was August 2020 for the above databases and December 2020 for grey literature. The terms used in the search were classified into three themes: Roma terms including words such as ‘Roma’ or ‘Romani’; mental health terms such as ‘mental health disorder’ or ‘mental well-being’; and mental healthcare terms such as ‘psychiatric care’ or ‘mental health facility’. Medical Subject Heading (MeSH) terms were also used for the appropriate databases. For literature in languages other than English, the above terms were translated into the appropriate language, and local terms were also searched. Titles and abstracts from 1980 and onwards were included. The following search strategy was used for Ovid databases:
(Roma or romani or travellers or gyps$ or romany or rommany or sinti or Romanichal or gips$ or romungro or Iovari or kale or lyuli or kaale or’ erlides or askhali).mp. (‘Common mental health disorders’ or ‘severe mental illness’ or mental health or mental or psychology or mental state or mental illness or mental ill health or wellbeing or psychological wellbeing) OR exp Mental Health/ (Care or mental healthcare or psychiat$ or psychiatric hospital or ‘mental health facility’ or psychiatric care) OR exp Mental Health Services/ 1 AND 2 AND 3
Study eligibility
There were two sets of inclusion criteria depending on the research questions. Table 1 shows the Population Exposure Control Outcome charts detailing inclusion and exclusion criteria for both research questions. Articles in any language were included. All study designs were accepted. Commentaries or opinion papers were excluded.
Population Exposure Control Outcomes (PECO) for both research questions (RQ).
Study selection
In the first stage of screening for abstracts and titles, two co-reviewers screened all of the data independently then discussed conflicts until they reached mutual agreement. In the second stage of full-text screening, the same two co-reviewers screened the data, following which conflicts were also discussed until mutual agreement was reached.
Data extraction and analysis
Data extraction was carried out by two independent co-reviewers (50% each), and conflicts were discussed. A data extraction tool was devised based on the information needed from the studies. All studies were classified according to the authors, origin, year of publication, sample characteristics, methods, and main results. The data were analysed using thematic analysis. The data were categorized and synthesized depending on the following factors: (1) study design, including sample size and type, sampling method and country of origin; (2) mental healthcare access factors, i.e. type of care accessed and description of experiences; (3) mental health outcomes factors, i.e. measures used to assess mental health outcomes and final outcomes.
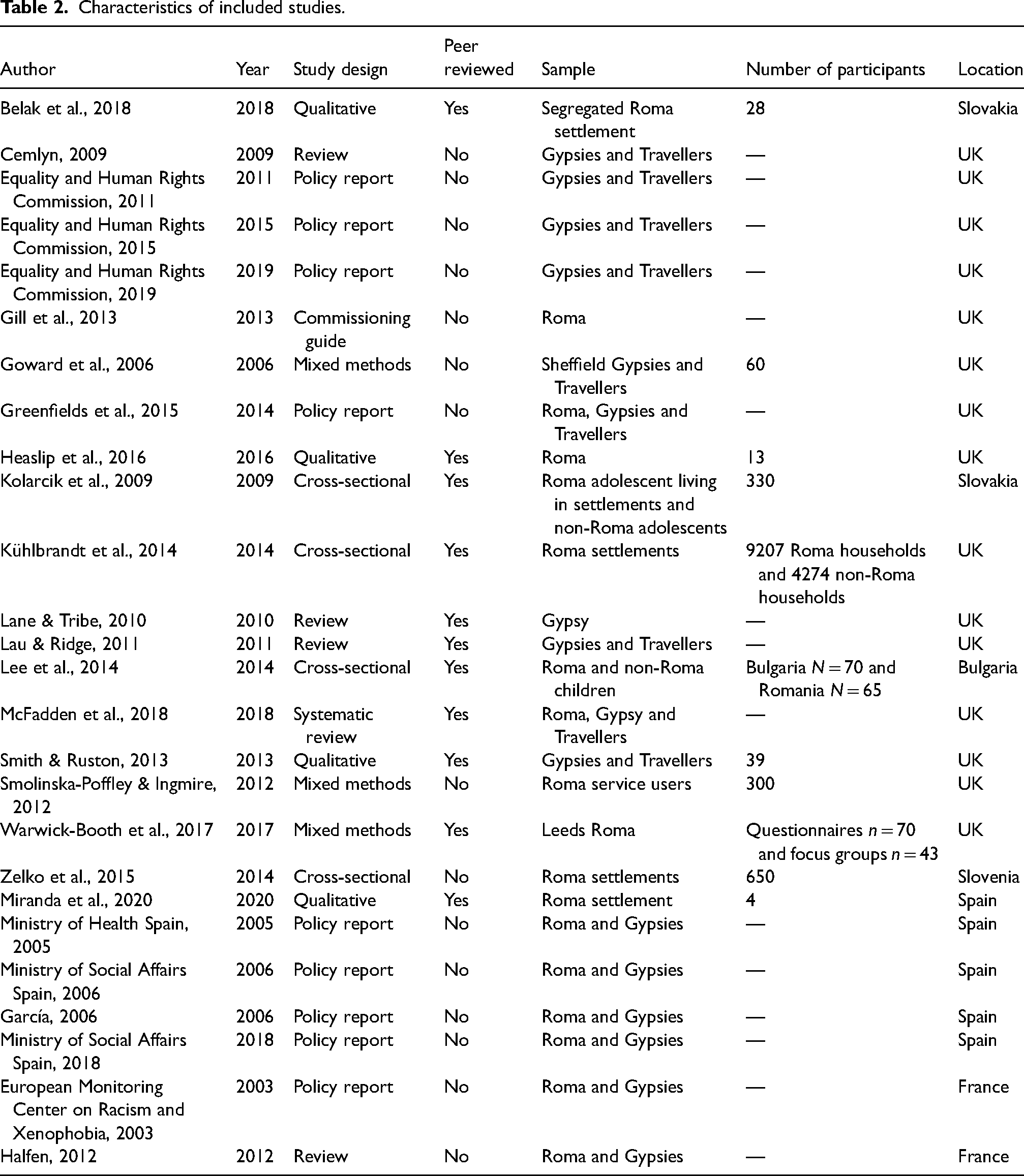
The data were then organized based on the research questions they pertained to. We assessed specific study characteristics in order to estimate gaps in the relative quality of evidence and generalizability. The characteristics were reported based on information such as design, whether the study had been peer-reviewed, population and year of publication. The hierarchy of evidence was used to assess whether a design was considered of relative higher or lower quality with reviews and randomized controlled trials being considered of higher quality than other designs (Greenhalgh, 1997). Also, if a paper was peer-reviewed it was considered of higher quality. Information on population and year of publication was used to assess the generalizability of the studies with more recent studies involving a larger spectrum of Roma participants (from different communities or from different countries) being considered more generalizable. The characteristics assessment was done during the process of data extraction by the same reviewers. All of the characteristics extracted can be seen in Table 2.
Characteristics of included studies.
Results
The total number of articles identified through all the databases and grey literature was 170, and 133 after removing duplicates. After the first stage of screening for abstracts and titles 55 papers were included. Of the 55 papers, 26 were included for final data extraction. Most papers that were excluded in the last stage, were excluded because they did not describe mental healthcare or mental health related outcomes. All the exclusion reasoning can be seen in the below PRISMA flow chart (Figure 1).
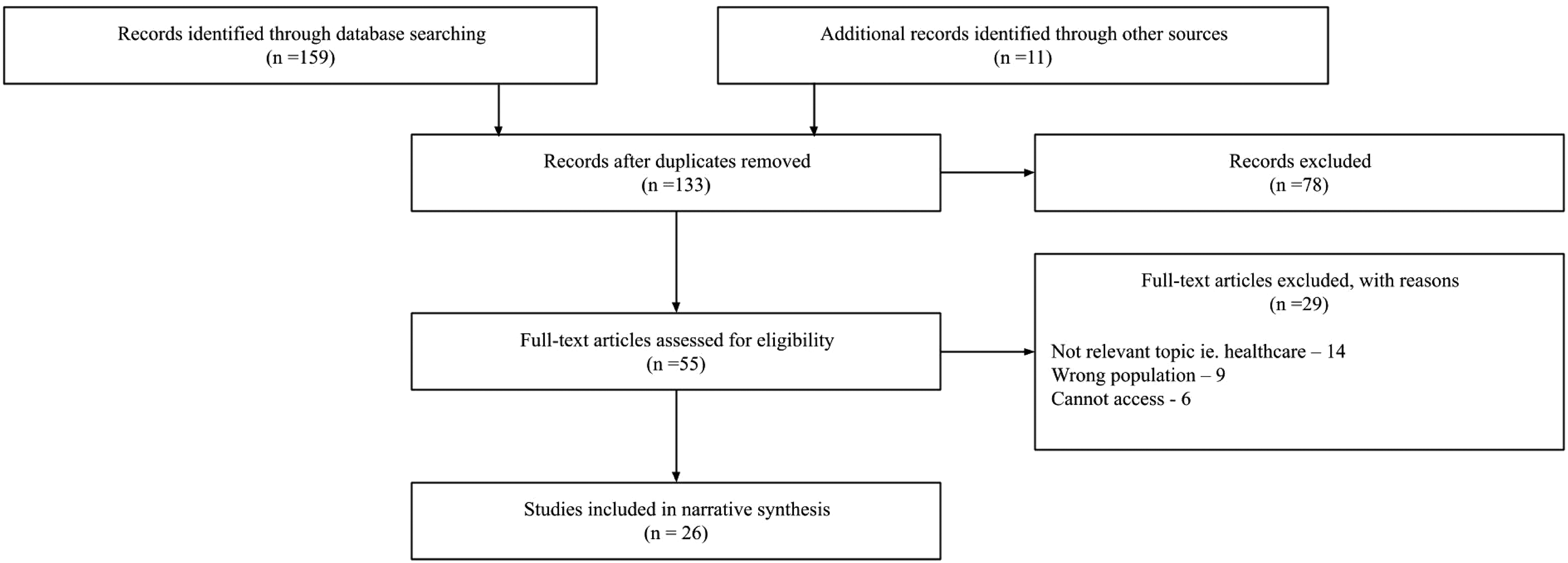
PRISMA 2009 flow diagram (Moher et al., 2009).
General characteristics of included studies
Table 2 shows the information extracted for the purpose of assessing the characteristics, quality and subsequently the generalizability of the included studies.
Most studies included (58%) were done in the United Kingdom (UK) compared with 11 (42%) outside the UK, mostly in Eastern European countries such as Bulgaria, Romania, Slovenia or Slovakia, or France and Spain (Belak et al., 2018; European Monitoring Center on Racism and Xenophobia, 2003; García, 2006; Halfen, 2012; Kolarcik et al., 2009; Lee et al., 2014; Ministry of Health Spain, 2005; Ministry of Social Affairs Spain, 2006, 2018; Miranda et al., 2020; Schick-Makaroff et al., 2016). The most prominent publication types were reviews and policy reports (57%) followed by empirical studies (42%). The study design for most of the empirical studies was equally a cross-sectional design (36%) or a qualitative design (36%), followed by a mixed method design combining qualitative interviews and cross-sectional survey collection (27%). Participants were mostly Gypsies and Travellers (38%), followed by Roma who are currently residing in the UK (19%) but have emigrated mostly from Eastern European countries. Finally, a proportion of studies focused on Roma living in Eastern European countries (15%), or Spain and France (26%). Most studies were done with adult populations, apart from two studies, one of which had adolescent participants and the other which had children (Kolarcik et al., 2009; Lee et al., 2014). Finally, approximately half of the studies (46%) worked with Roma populations living in underserved communities, single segregated settlements, Roma accessing specific social services or in governmental accommodations (Belak et al., 2018; European Monitoring Center on Racism and Xenophobia, 2003; García, 2006; Goward et al., 2006; Kolarcik et al., 2009; Kühlbrandt et al., 2014; Lee et al., 2014; Miranda et al., 2020; Smith & Ruston, 2013; Smolinska-Poffley & Ingmire, 2012; Warwick-Booth et al., 2017; Zelko et al., 2015).
Research Question 1: What is the mental health status of the Roma population of Europe?
For the first research question, 18 studies were applicable. Table 3 shows a summary of the studies. Twelve studies show higher levels of depression and anxiety in the Roma population compared with the non-Roma population or other minority ethnic groups, including one for children (Cemlyn, 2009; Equality and Human Rights Commission, 2019; European Monitoring Center on Racism and Xenophobia, 2003; Goward et al., 2006; Gill et al., 2015; Halfen, 2012; Lee et al., 2014; Ministry of Social Affairs Spain, 2006, 2018; Miranda et al., 2020; Smolinska-Poffley & Ingmire, 2012; Zelko et al., 2015). The six remaining studies report poor mental well-being in general, usually via self-report (Gill et al., 2013; Kolarcik et al., 2009; Lane & Tribe, 2010; Lau & Ridge, 2011; Smith & Ruston, 2013; Warwick-Booth et al., 2017). Three studies also report high levels of stress based on self-reports (Goward et al., 2006; Halfen, 2012; Warwick-Booth et al., 2017). A high presence of substance abuse was reported by three studies (European Monitoring Center on Racism and Xenophobia, 2003; Gill et al., 2013; Smolinska-Poffley & Ingmire, 2012). Furthermore, another two studies found a high suicide rate or high frequency of suicidal ideation (Lane & Tribe, 2010; Smolinska-Poffley & Ingmire, 2012). Roma women seem to have worse mental health outcomes than Roma men, as showed by one study (Lau & Ridge, 2011), and Roma children are prone to showing more externalizing and internalizing disorders compared with non-Roma children (Lau & Ridge, 2011; Lee et al., 2014).
Extracted data for studies relevant to Research Question 1 (N = 18).
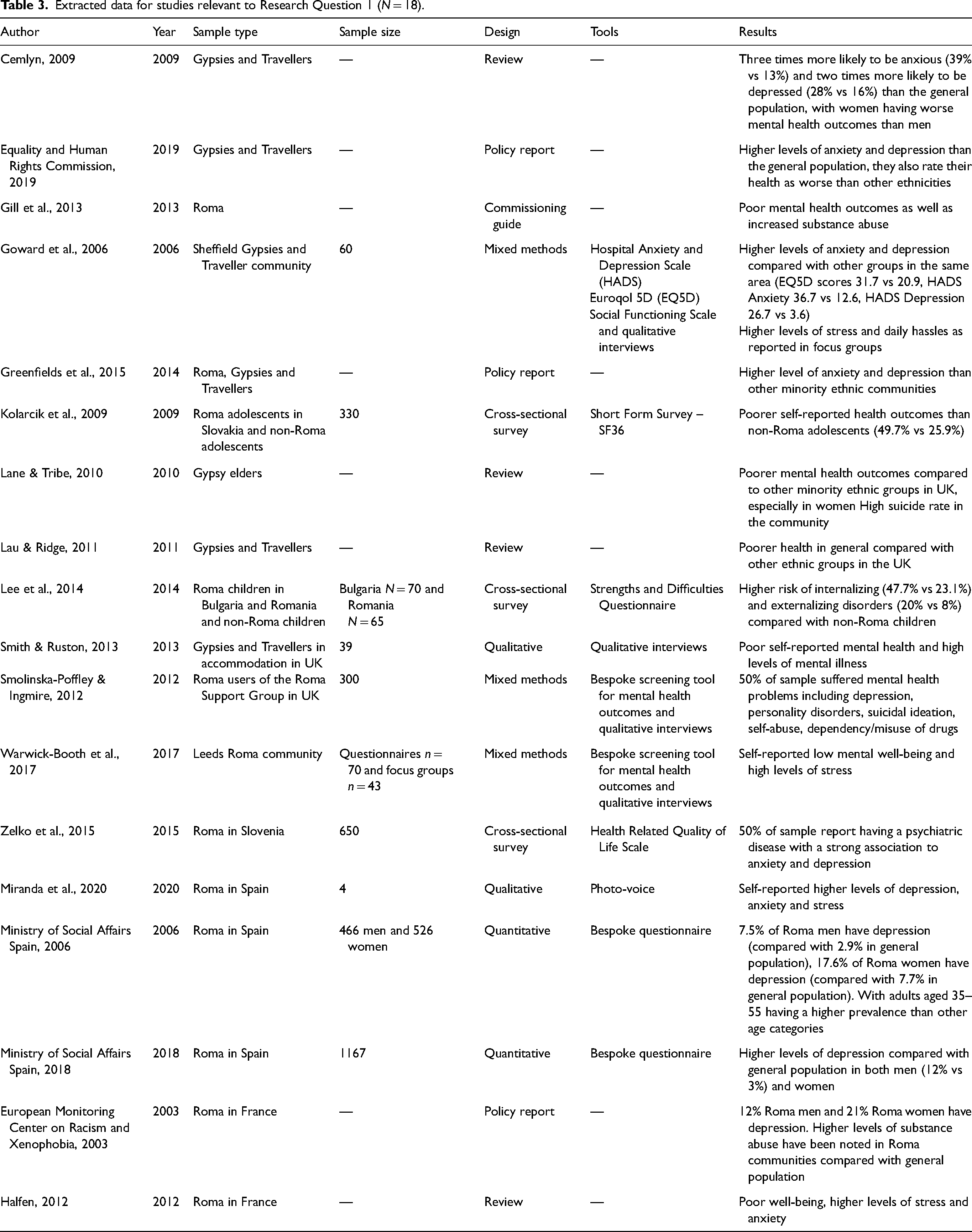
Nine of the included studies underline the impact of social determinants of health on Roma mental health. Gill et al. (2013) report that social exclusion is very strongly associated with mental health outcomes. A strong negative correlation between secure housing and mental health was found by Greenfields et al. (2015), and four other studies (European Monitoring Center on Racism and Xenophobia, 2003; Halfen, 2012; Ministry of Health Spain, 2005; Miranda et al., 2020; Warwick-Booth et al., 2017).
Finally, although Lane and Tribe (Lau & Ridge, 2011) also found a link between Roma mental health and social determinants of health such as housing security and economic status, they also found that family relations and links to the Roma culture or lack thereof, strongly impacted self-reported mental health outcomes.
In terms of the quality and generalizability of the above findings, 8 of 18 were policy reports or reviews (Cemlyn, 2009; Equality and Human Rights Commission, 2019; European Monitoring Center on Racism and Xenophobia, 2003; Gill et al., 2013; Greenfields et al., 2015; Halfen, 2012; Lane & Tribe, 2010; Lau & Ridge, 2011). The rest of the studies were mostly cross-sectional or mixed methods studies with cross-sectional surveys. However, quite often the number of participants was relatively low, with only three studies reaching larger samples (Kolarcik et al., 2009; Smolinska-Poffley & Ingmire, 2012; Zelko et al., 2015).
Most of the studies were from the UK, and eight were from East European countries (Slovakia, Bulgaria/Romania, Slovenia), Spain and France (European Monitoring Center on Racism and Xenophobia, 2003; Halfen, 2012; Kolarcik et al., 2009; Lee et al., 2014; Ministry of Social Affairs Spain, 2006, 2018; Miranda et al., 2020; Zelko et al., 2015). Only 7 of the 18 studies included under this research question were peer-reviewed (Kolarcik et al., 2009; Lane & Tribe, 2010; Lau & Ridge, 2011; Lee et al., 2014; Miranda et al., 2020; Smith & Ruston, 2013; Warwick-Booth et al., 2017). The studies were written between 2006 and 2019 with most being written five years ago and earlier.
Research Question 2: What is the level of access to mental healthcare as well as perceived quality of mental healthcare of the Roma population of Europe?
For the second research question, 16 articles were responded to inclusion criteria. Most of the articles describe several barriers Roma face when accessing mental healthcare or healthcare in general. These can be broadly categorized into three themes: language, lack of information and economics. In terms of language, Warwick-Booth et al. (2017) underline that most members of the Leeds Roma community, which mostly consists of emigrated East European Roma, lack the language capabilities to access appropriate care or to understand the care they are receiving. This links to the second theme; that is, the existence of an information barrier. Five studies highlight the fact Roma are often not capable of understanding the information or information is not properly explained by healthcare providers. This trend is often linked to low levels of education and literacy. Many are also unsure which mental healthcare services they should seek or the availability of healthcare services in general (Belak et al., 2018; Equality and Human Rights Commission, 2015; Goward et al., 2006; Smolinska-Poffley & Ingmire, 2012). Finally, the theme of economics represents the financial barrier that is often present for Roma individuals accessing mental healthcare. This was mentioned by four studies, and some also highlighted the fact that a lack of finances may lead to an inability to get insurance. Without health insurance many providers will not offer their services (Belak et al., 2018; Kühlbrandt et al., 2014; McFadden et al., 2018). Furthermore, it must be noted that another factor related to economics is housing security, which impacts whether the individual will have a fixed address and therefore also possibly documentation. This in turn impacts the likeliness of having health insurance and thus being able to access mental healthcare (Equality and Human Rights Commission, 2019; Kühlbrandt et al., 2014; McFadden et al., 2018).
It must be noted that McFadden et al.'s (2018) systematic review summarized Roma service user attributes that can act as barriers into three key themes: individual demographics (e.g. age and gender); concerns about health services (e.g. lack of trust, negative experiences); and individual preferences (e.g. depending on lay networks for information or advice). It is precisely informal lay networks, such as family or community members, that Smith and Ruston (2013) underline as one of the key barriers but also mediators of access to mental healthcare.
Experiences with mental healthcare services, or healthcare services in general, described in studies are summarized in Table 4. The three most frequent negative experiences were a lack of understanding from healthcare professionals for missing documentation, no permanent address or no insurance (Belak et al., 2018; Equality and Human Rights Commission, 2019; Kühlbrandt et al., 2014; Lane & Tribe, 2010; McFadden et al., 2018); a lack of relevant services for the Roma population either geographically or culturally (Belak et al., 2018; Equality and Human Rights Commission, 2011, 2015, 2019; Greenfields et al., 2015; Heaslip et al., 2016; Lane & Tribe, 2010; Ministry of Health Spain, 2005; Smolinska-Poffley & Ingmire, 2012); and finally, experiences of racism, discrimination or judgement (García, 2006; Gill et al., 2013; Greenfields et al., 2015; Lane & Tribe, 2010;; McFadden et al., 2018; Smith & Ruston, 2013).
Summary of Roma mental healthcare experiences.
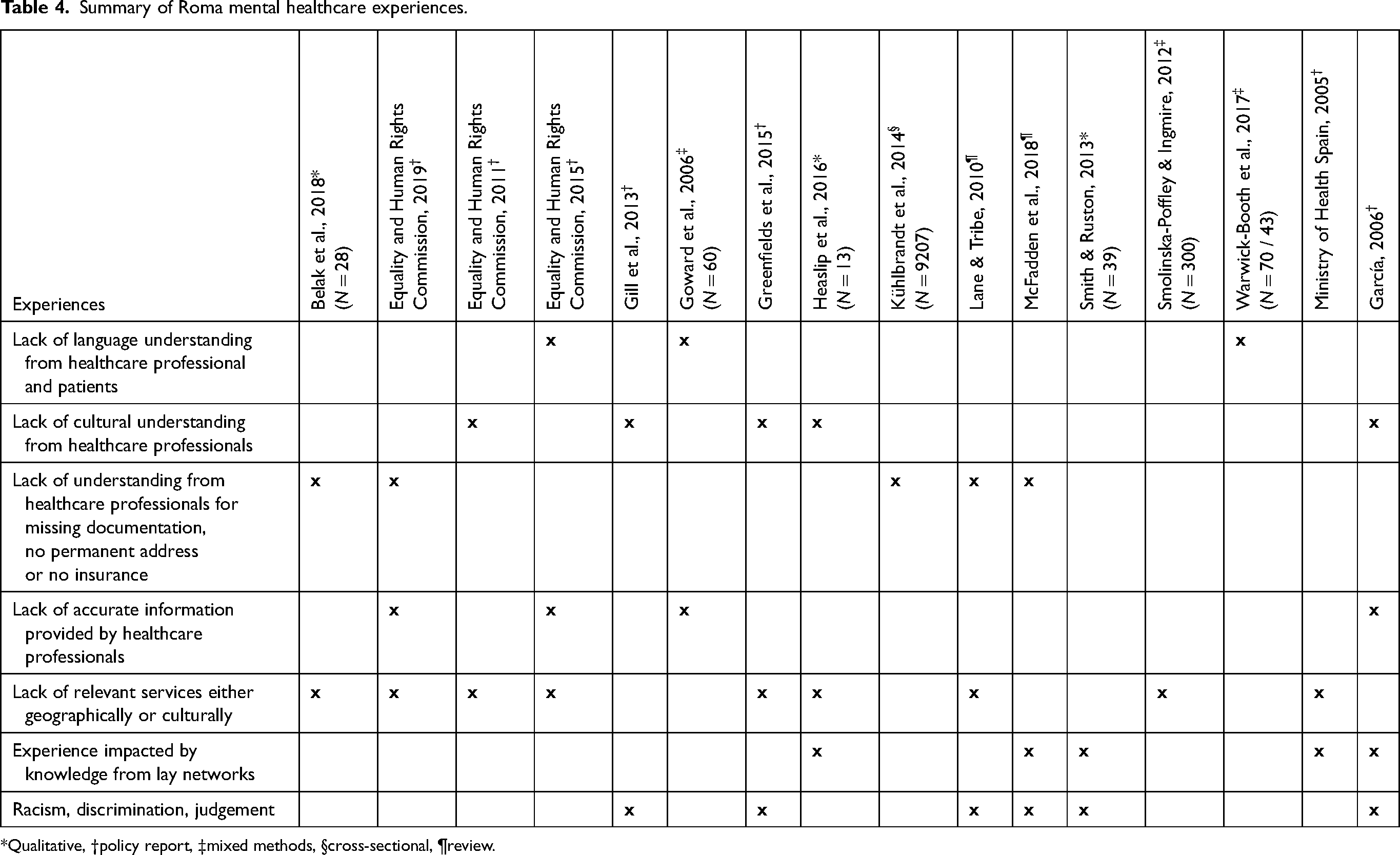
*Qualitative, †policy report, ‡mixed methods, §cross-sectional, ¶review.
With regard to the quality and generalizability of the studies included under the second research question, 8 of 16 studies were reviews or policy reports (Equality and Human Rights Commission, 2011, 2015, 2019; García, 2006; Gill et al., 2013; Greenfields et al., 2018; Lane & Tribe, 2010; Ministry of Health Spain, 2005) and one was a systematic review (McFadden et al., 2018). The rest of the studies were either qualitative or mixed methods designs. Most of the studies had relatively small sample sizes below 100, apart from two which had larger sample sizes (300 and 9207 respectively) (Kühlbrandt et al., 2014; Smolinska-Poffley & Ingmire, 2012). Only three studies were not from the UK but from Slovakia (Belak et al., 2018) and Spain (García, 2006 Ministry of Health Spain, 2005;); 7 of 16 studies were peer-reviewed (Belak et al., 2018; Heaslip et al., 2016; Kühlbrandt et al., 2014; Lane & Tribe, 2010; McFadden et al., 2018; Smith & Ruston, 2013; Warwick-Booth et al., 2017). The studies were published between 2006 and 2019 with most being published before 2015.
Discussion
To our knowledge, this is the first scoping review of mental health status and access to mental healthcare among the Roma population in Europe. The results of the included studies indicated that the mental health of Roma is poor compared with the general population. This conclusion is based on studies using diagnostic and self-report measures. The most commonly identified disorders were anxiety, depression or substance abuse. Roma women had worse outcomes than Roma men, and worse mental health outcomes were reported for Roma children when compared with non-Roma children. Furthermore, Roma experience a high level of self-reported stress and poor mental well-being.
In terms of Roma access to mental healthcare, there were three key categories of barriers: language barriers between Roma and healthcare providers; information barriers, i.e. Roma lack education and literacy but are also not given enough information to understand their rights and access to services; and economic barriers, which include a lack of health insurance or stable housing. Roma experiences of with mental healthcare tend to be negative mostly because of a lack of understanding towards and from the mental healthcare providers. Experiences of racism and discrimination are very frequent, and a lack of understanding of Roma culture is also very common.
Most mental health outcomes for Roma, as well as the barriers to access to mental healthcare, seem to be very strongly linked to social determinants of health such as education, economic status and secured housing. Although the studies in the current review identify such barriers, they fail to link them to a much larger burden of exclusion that Roma face. This exclusion is a compound issue of poverty and discrimination, which leads to impacts on education and access to social services (Goodwin, 2009; Klaus & Marsh, 2014). Furthermore, and perhaps most importantly, the Roma burden of exclusion has vast impacts on health and potentially mental health (Milcher, 2006). Therefore, if we speak of barriers to access to care or higher levels of mental illness in Roma communities, it must be understood that such issues are predominantly linked to economic and discrimination problems, which indicate a need for a much wider perspective on Roma mental health.
There are some limitations to the included studies, which highlight gaps in the literature. First, very few of the studies translated their questionnaires or other measuring tools into either Romani or the languages of the participants. This means that very few studies adapted their measures to the culture or idioms for expressing experiences of illness of the participants, and therefore, the outcomes may be biased (Haroz et al., 2017). This may also be applied to the topic of accessibility and perceived quality of care, because what Roma may perceive as poor quality may not be encompassed in typical measurement tools of quality of care (Rose et al., 2011). Second, most of the studies report on segregated or marginalized communities that are easily accessible. This fact, however, means that there is no available data on Roma who have integrated into the majority community. Furthermore, Kósa and Adany (2007) for example, underline that often participants may not wish to self-report their ethnicity as this information may be abused, leading to reporting bias.
Scarcity of research may also be related to the fact that researchers often come from the dominant culture, which means that they are in a position of power when researching on ethnic minorities such as the Roma (Tremlett & McGarry, 2013). Such a power dynamic often leads to reluctance on the part of Roma to participate in research. Munté et al. (2011) propose that for research to be truly balanced and representative of the needs of ethnic minorities, such as Roma, there is a necessity for communication with key leaders from the communities.
However, it must also be noted that the social context in which policies or research initiatives are being created is one in which Roma voices are often silenced (McGarry & Agarin, 2014). This means that for true participation to be effective, there is need for active bottom-up engagement, which would allow Roma community members to be part of active research (e.g. being part of the research team), and their subsequent involvement in advocacy within the community (Condon et al., 2019).
For the current review, the key limitation is that first, the findings depend vastly on the methods employed by the included papers, which in many cases are not clearly described. Many of the studies included small samples, which limited the possibility to draw conclusions. Furthermore, very few of the studies were peer-reviewed. This is especially critical in the case of policy reports or reviews. Second, double counting of studies was not taken into consideration; this means that some of the studies may be reported repeatedly in reviews, and therefore the results of the review may be overstating the evidence. This also limits our ability to accurately assess how large the gap in the literature is. Third, although study selection was carried out simultaneously by two reviewers, data extraction was divided in half between two reviewers with only partial cross-checks of data extraction decisions, and without second confirmation on the data extracted. Finally, the narrow definition of accessibility may have omitted the possibility that other forms of referral from different sectors may be a gateway to access to mental healthcare, for example referrals from housing services, social services or schools.
The results of the current review point to higher levels of anxiety, depression and substance abuse, as well as to low levels of mental well-being in the Roma population of Europe. However, the methodologies, time of writing and also the location of the studies are a limitation, with most being produced in the past 10 years ago, and almost exclusively in the UK. This means there is a need for updated research on the mental health status of Roma which should be carried out with clear methodologies, culturally adapted and in a vast range of countries and Roma communities. Roma access to mental healthcare seems to be limited by several barriers and hindered by a lack of preparedness on the side of healthcare providers to provide culturally adapted care for the Roma population. There is, therefore, a need to create services that are available and adapted to the Roma population. This would mean not only educating the Roma community on their healthcare rights, but also making sure that healthcare providers are prepared to provide care to this population. To achieve this, there is a need to ensure that Roma are centrally engaged in the process of service development and the creation of cultural awareness training programmes for mental healthcare providers, as well as in research relevant to their health.
Footnotes
Acknowledgements
We thank Daniel Chisholm for reviewing the manuscript and Tereza Převrátilová for searching French language databases.
Author Contributions
ZG initiated, planned, designed and coordinated the study, and led the writing of the manuscript. DC collaborated in the review process as a second reviewer in all stages from abstract and title screening to data extraction. PW supervised the study and contributed to its design, interpretation of the results and writing of the manuscript.
Data Availability
Not applicable to this article as no new data were created or analysed in this study.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministry of Education, Youth and Sports of the Czech Republic, (grant number Nr. LO1611, NPU I).