
Abstract
Exposure to violence, vulnerability due to lack of shelter, alienation due to stigma, the experiences of severe mental illness (SMI) and subsequent institutionalization, make homeless persons with SMI uniquely susceptible to trauma exposure and subsequent mental health consequences. This study aims to contribute to the development of culturally sensitive interventions for identifying and treating trauma in a population of homeless persons with SMI in Tamil Nadu, India by understanding the manifestations of trauma and its associated consequences in this population. Free-listing exercises followed by in-depth interviews were conducted with a convenience sample of 26 user-survivors who have experienced homelessness or were at risk of homelessness, and suffered from SMI. Topics explored included events considered to be traumatic, pathways to trauma, associated emotional, physical and social complaints, and coping strategies. Results indicate discrepancies in classification of traumatic events between user-survivors and the Diagnostic and Statistical Manual of Mental Disorders. Traumatic experiences, particularly relating to social relationships and poverty, mentioned by user-survivors did not match traditional conceptualizations of trauma. Positive coping strategies for trauma included being mentally strong, knowledge and awareness, whereas the main negative coping strategy is avoidance. User-survivors attributed their experiences of homelessness and SMI to past traumas. Differing views of trauma between user-survivors and mental health professionals can lead to misdiagnosis and under-recognition of trauma in this population of homeless persons with SMI.
Introduction
While mental disorders commonly associated with poverty in Low and Middle Income Countries (LMIC) include depression, schizophrenia, anxiety, intellectual disability, and suicidal ideation (Funk, Drew, & Knapp, 2012; Patel & Kleinman, 2003), trauma-related disorders in the context of poverty in LMICs is explored significantly less (Fodor et al., 2014). Challenges relating to the variability in conceptualization and diagnosis of trauma-related disorders over the years has hindered both research and clinical practice in this field (Jones & Cureton, 2014). There is ambiguity in the use of the term ‘trauma’, with many using the term to either refer to a wide range of negative events that perceivably produce distress, or to refer to the distress itself (Briere & Scott, 2006; Chadha, Malhotra, & Srivastava, 2013). For the purpose of this study, we will distinguish between traumatic events and trauma as a condition that follows as a consequence of a traumatic event.
Though the lifetime prevalence of exposure to traumatic events has been reported as 40 to 90% of the population (Breslau, Davis, Andreski, & Peterson, 1991; Breslau et al., 1998), the psychological consequences of traumatic exposure vary widely (Jones & Cureton, 2014). Only a minority of those exposed to traumatic events (approximately 24%) go on to experience clinically significant symptoms of Post-Traumatic Stress Disorder (PTSD) (Breslau et al., 1991). However, exposure to traumatic events has also been shown to increase susceptibility to other mental disorders, including major depressive disorder and anxiety disorders (Kessler, Sonnega, Bromet, Hughes, & Nelson, 1995; Shalev et al., 1998).
At present, most of the literature on trauma in India has focused on natural disasters, such as the 2004 tsunami that hit Tamil Nadu (Baddam John, Russell, & Russell, 2007; Bhushan & Kumar, 2012; Kar, Krishnaraaj, & Rameshraj, 2013), and ongoing conflict and civil unrest in the Kashmir region (Bhat & Rangaiah, 2015; Bhushan & Kumar, 2012; Kar et al., 2013). A few studies have focused on injury due to road accidents (Seethalakshmi, Dhavale, Gawande, & Dewan, 2006), intimate partner violence (Tichy, Becker, & Sisco, 2009), exposure to murder and death (Raju, 2005) and sexual abuse (Bhaskaran, Gaikwad, Chandrakanth, & Seshadri, 2016). Less attention has been paid in the Indian literature to other events that may also be considered traumatic (Pillai, Mehta, & Chaudhari, 2016). In particular, certain populations in India, such as the homeless or severely mentally ill, experience violations to their basic human rights and potentially traumatic events on a daily basis.
There are several reasons why homeless persons with severe mental illness (SMI) may be particularly vulnerable to traumatic exposure. First, persons with SMI are often subjected to high rates of sexual abuse, interpersonal violence and victimization – experiences considered to be highly traumatic (Mueser, Rosenberg, Goodman, & Trumbetta, 2002). Additionally, the development of a mental illness, institutionalization, and stigma can also be traumatic (Mueser et al., 2002). Homelessness also increases vulnerability to traumatic events. Individuals who are left without shelter for extended periods of time can develop a sense of helplessness, alienation, and a lack of security (Goodman, Saxe, & Harvey, 1991). Being homeless can also leave an individual more vulnerable to exposure to traumatic events, such as witnessing or experiencing violence or accidents (Hopper, Bassuk, & Olivet, 2009; Kipke, Simon, Montgomery, Unger, & Iversen, 1997). Finally, some individuals may be driven into homelessness as a consequence of traumatic events, such as domestic or sexual abuse (Hopper et al., 2009; Koegel, Melamid, & Burnam, 1995; Tyler, Hoyt, & Whitbeck, 2000).
A 2011 census identified a population of 18 million homeless individuals in India, with a growing number found in the country's urban centers (Kumuda, 2014). Due to its location and low-resource surrounding rural settlements, the city of Chennai, in Tamil Nadu, has the fourth highest homeless population rate in India with approximately 17,000 homeless individuals (Kumuda, 2014). With studies suggesting that a third of homeless populations worldwide suffer from some form of severe mental illness (Kumar, 2014; Levitt, Culhane, DeGenova, O'Quinn, & Bainbridge, 2009), and the consequent increased vulnerability to traumatic exposure, there is reason to believe that there may be gross under-reporting of trauma in this specific population.
There is a growing body of literature that supports the idea that cultural factors have an influence in shaping explanatory models for mental illnesses, including those related to trauma (Kendler, 2008; Pereira et al., 2007). Amongst the Acholi people in Northern Uganda, for example, traumatic events and subsequent effects have been expressed in the form of Orongo (animal) and Cen (human) spirit possession, where hunters and warriors experience vivid images of their victims pleading for their lives, as well as feelings of panic and fear, and avoidant behavior – emotional and psychological symptoms that seem to emulate modern-day PTSD (Ovuga & Abbo, 2016). In rural Kyrgyzstan, a negative attitude towards the expression of fear results in somatoform manifestations of stress disorders and serves as one explanation for the difficulties in diagnosing stress disorders such as PTSD (Molchanova, Agazade, & Dobryakov, 2016). These examples illustrate the importance of understanding both the cultural context and the language of distress used by specific target populations to describe their experiences of trauma.
There has been considerable debate on the cross-cultural validity of the conceptualization of trauma (Bracken, Giller, & Summerfield, 1995; Hinton & Lewis-Fernández, 2011; Patel, 2000). The use of assessment tools that lack adequate translation and validation for a specific target population can lead to misdiagnosis and inadequate treatment (Onyut et al., 2009). This study aimed to contribute to the development of culturally sensitive interventions for identifying and treating trauma in a population of homeless persons with SMI in Tamil Nadu by exploring local understandings of trauma and its associated consequences.
Methods
Qualitative data collection methods were employed by authors AG and SV to explore the existence and understanding of trauma from user-survivor – the designated term for persons that were previously homeless or at risk of homelessness that are now accessing care – perspectives, between the months of November 2015 to May 2016, and May to July 2017.
Ethics
This study is the product of a collaboration between the VU University Amsterdam, the Harvard School of Public Health, and The Banyan, a, non-governmental organization in Chennai, India. The study was approved by the Dutch Science Committee of the Institute for Health and Care Research (EMGO+) and The Banyan Internal Ethics Committee in Chennai. All participants gave written informed consent in their native language, Tamil, prior to the initiation of participation. Due to the nature of the interviews and their potential to bring up unwanted thoughts from the past, extra counselling was offered to all participants after the interviews, if required.
Sample
Using a maximum variation purposive sampling technique, 26 participants (20 women and six men) were recruited from Kanchipuram and Chennai districts in Tamil Nadu, through The Banyan – a mental health NGO that provides services to over 2,500 homeless persons and approximately one million individuals experiencing mental health needs across India (Narasimhan, Gopikumar, Jayakumar, Bunders, & Regeer, 2019).
Study participants, who had experienced homelessness with SMI or who were considered at risk of homelessness with SMI, who were above the age of 18 and could comprehend interview instructions, were recruited in Tamil (the local language) from among Banyan service users by author SV. Those at risk of homelessness were determined as individuals who currently lived in their own homes but shared common socio-cultural risk factors for homelessness including poverty, poor social/familial support, familial breakdown, and previous experiences of verbal or physical abuse (Caton et al., 1995; Kumar, 2014; Levitt et al., 2009). User-survivors were selected from various care networks within the Banyan (see supplementary material).
Data collection
Free Listing Exercises. Prior investigation through discussions with mental health professionals and first-language Tamil speakers allowed us to establish that while there was no direct translation in Tamil for the word ‘trauma’, most people agreed that the Tamil term ‘adirchi’ was closest in meaning. As a starting point for the exploration of trauma in this population, free-listing, a semi-structured interviewing technique aimed at gathering word associations to abstract concepts, was employed to generate systematic data on user-survivors’ first associations with trauma (Betancourt, Speelman, Onyango, & Bolton, 2009). Individual free-listing exercises were first conducted in Tamil by authors AG and SV with 26 user-survivors in a private setting, lasting approximately 10 to 15 minutes each. Beginning with the question “What do we mean when we say ‘adirchi’?”, we elicited as many associations with the term as possible. This was followed with questions asking “What types of events cause adirchi?” and “What are related problems of people with SMI who are homeless or at risk of homelessness?” Authors AG and SV probed for as many experiences and problems as possible and asked for short descriptions of each problem. Data generated from the free-listing exercises were compiled into a composite list of the items listed by the participants and grouped according to types of traumatic events, as well as types of physical, emotional and social complaints associated with trauma.
In depth semi-structured interviews. Following each free-listing exercise, an in-depth exploration of the concept ‘adirchi’ using semi-structured interviews with each participant was then conducted by authors AG and SV. The interview focused on additional aspects of trauma including: coping strategies, differentiation from other mental illnesses, and linkages between trauma, homelessness and mental illness.
Data analysis
All data were transcribed verbatim and translated into English from Tamil, using a professional transcriptionist proficient in both languages. Data was analyzed using Dedoose, a qualitative data analysis software program (Dedoose, 2018). Previous studies using a similar approach indicated thematic content analysis (TCA) to be the most suitable approach for data analysis (Betancourt et al., 2012) For this approach, transcripts were read by investigators independently, and then carefully examined for patterns across the data set, from which themes were derived (Smith, 1992). In addition, a random selection of transcripts was also analyzed by author SV of this study who is a clinical psychologist in the field; thereby confirming fidelity to codes and themes derived.
Results
Demographics of user-survivors
A little over half of the participants (n = 14) were previously homeless, while 12 were classified as being at risk of homelessness. The average age of study participants was 47 years, with the range from 29 to 75. Most participants were recruited from the ILO Banyan service (n = 10), with 5 from ECRC and ROP; 4 from MS, and 2 from UOP. At the time of recruitment, participants' clinical diagnoses were: schizophrenia (n = 11); bipolar affective disorder (n = 7); psychosis NOS (n = 2); substance induced delirium (n = 2); major depressive disorder (n = 1); and 3 participants that were yet to receive an official diagnosis.
Defining and differentiating trauma
Most user-survivors defined trauma as an ‘emotional shock’. In Tamil, this was most commonly referred to as ‘adirchi’ and in the case of a ‘big emotional shock’, was referred to as ‘per-adirchi’. Adirchi and per-adirchi were, however, frequently used interchangeably. This emotional shock occurs almost exclusively in response to a negative life experience, and one that was most often unexpected. Three major conditions for experiencing trauma emerged from the thematic analysis: (1) Trauma is linked to a single event or repeated exposure to a specific type of event; (2) The event usually occurred without warning; and (3) Trauma is unbearable and reflects an inability to cope.
In every interview, user-survivors claimed that the high levels of distress experienced were exclusively related to either a specific event in time, or repeated exposure to a specific type of event. Trauma does not occur without a specific cause. After my child died [I was] without my senses. I have been somewhere and they have handed [me] over to police. My mother has searched for me and she has found me and she has taken me along with her … it was traumatic to me. My son's death was traumatic to me. (ILO3, F) [I was a nurse, and one day] both [a] mother and [her newborn] baby [that were in my care] died. So there was lot of problems. Still, I was in [a] good state but my family members started torturing me, denying [me] food and water. Indirectly they started forcing me to leave the home … My family denying me their support was most traumatizing. (ILO2, F)
Lastly, trauma was defined and differentiated according to one's ability to cope. Respondents reported that trauma reflects an inability to cope with the distress that one has been subjected to. ‘Difficult situations’, on the other hand, are considered manageable in which individuals are able to cope: “[Things are traumatic if … ] they are unbearable; it is beyond the imagination of the person to think that such a [thing can happen]. It is an unexpected and unbearable experience.” (ILO10, F)
Types of traumatic events
Summary of the local conceptualization of trauma (adirchi).
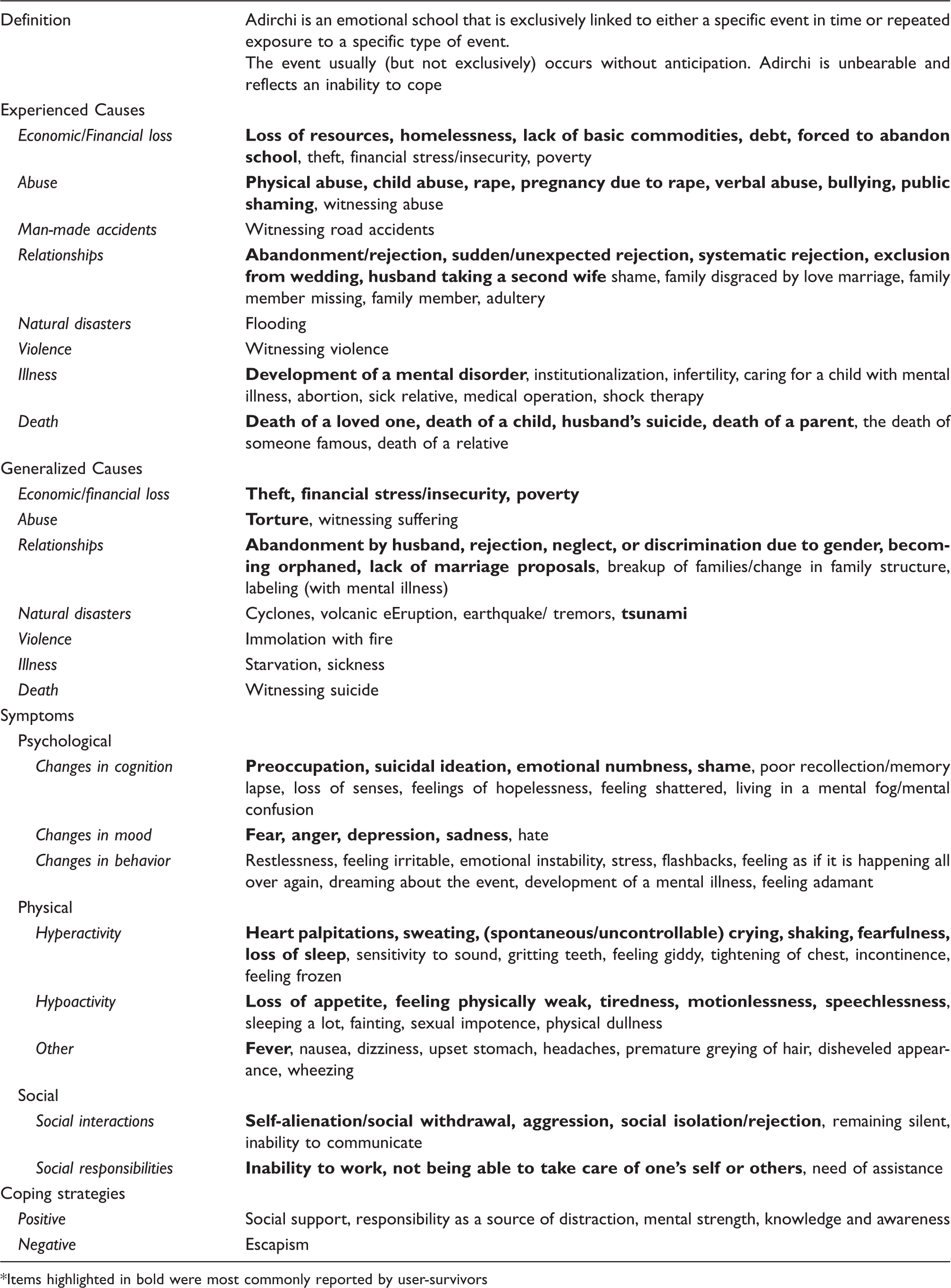
*Items highlighted in bold were most commonly reported by user-survivors
One user-survivor spoke about the distressing experience of being sexually abused by a family relative, and the subsequent shame and alienation it brought upon her by other family members. I will tell you whatever happened in my life. I have a brother … Sometimes, when I was asleep he would touch me. During that time, I didn't know how to react, but I was finding it very difficult. My sister used to scold me with abusive words, as though I was a bad girl. That is the reason for the first time I left my house and I came [here] because I was mentally shattered. (ILO9, F) I had a daughter. She told everyone that she was getting married, but she didn't inform me. That was very traumatic to me. My father and mother all of them joined together and got her married without informing me … I felt they were isolating me … disgraceful. In front of everybody, they didn't invite [me] and they [got married]. I was in that trauma. (ECRC3,F)
Traumatic experiences specific to Living with Mental Illness (PLWMI)
The most commonly mentioned traumatic events that user-survivors specifically relate to mental illness include the development of a mental disorder, stigma, abandonment, and institutionalization. One user-survivor spoke about the trauma of developing a mental illness, and the subsequent blame and regret that ensued: “I would think to myself, ‘Why is this happening to me’? Is it because my parents married [outside their caste]? Sometimes, I think like that. I think a lot about why I have ended up like this.” (ECRC5, F). A number of user-survivors also spoke about the trauma of stigmatization due to their mental illness. One user-survivor in particular spoke of the differential experiences of people suffering from mental illness compared to those suffering from physical ailments. I feel nobody understands them truly … if he is having some physical illness then there is acceptance, but if I tell people that I am having mental illness then they will say this man is a little demented or mad … [If] somebody is having diabetes, [then] nobody thinks there is something wrong with him. It is considered to be normal, but if I say I have paranoid schizophrenia, immediately people will think that okay this person is not normal. He is mental. (UOP2, M) Mental sickness is a trauma. Because we are mentally sick. [We] need understanding, and if [we] don't get understanding at home there is trauma. Where your behavior becomes irregular and aggressive or whatever, it is[different] from others. You get trauma if they don't understand. If the people around you don't understand, and when they get very upset and when they feel they are not able to keep [you] at home, and they put [you] in an institution, [you] get trauma because there is no place for [you] at home and [you] have been put here and it is worse here than there. (ILO7, F)
Traumatic experiences specific to homelessness
Abandonment, decreased safety, lack of access to basic needs, and sexual abuse were described as incidences of traumatic exposure resulting from homelessness. Respondents spoke about the vulnerability and fear they experienced when not having shelter: “I myself had a fear. I used to stay in Church, but still during nighttime when I was alone I used to be scared” (ILO9, F). One respondent spoke of the trauma he experienced when lacking all basic necessities for life: “All of them will go through trauma as I went through. Basic comfort of life is a must, first of all they should have a house, then clothing, then food, then money for expense.” (MS1, M)
Some clients spoke of the differential experiences of trauma for homeless women compared to homeless men. Homeless female respondents felt that they were more vulnerable to experiencing traumatic events. For women it is not safe, anybody will come and go … There is no safe drinking water, no safe home … any man can rape her and do something to her … so that way a woman suffers. [A man will manage]. (ILO10, F) [Men] don't have enough food … for food and for shelter they have to search … and ask anyone. [Out of] a hundred, [only] one person will help [with] giving them some money … Some way or the other [women] get the food. When a girl gives a smile … whatever it is, the guys will take care [of her]. (MS3, M)
Generalized traumatic events
Generalized traumatic events refer to hypothetical situations that user-survivors recognize as being traumatic, though they themselves have not necessarily experienced such a situation. Analysis revealed eight major types of traumatic events that were categorized as: natural disasters, violence, economic/financial loss, relationships, health and illness, death, abuse and man-made accidents (see Table 1).
While the homeless cohort went through some traumatic experiences that were not shared by the risk of-homelessness cohort (namely the experience of homelessness itself, abandonment and rape while living on the streets), it is worth noting that there were some similarities in the types of traumatic events experienced by both cohorts as well as in the number of traumatic experiences reported. Both cohorts have gone through experiences such as financial loss, loss of property, physical and verbal abuse, the sudden death of a close relative or loved one, social exclusion, and the development of their mental disorders which they have considered to be traumatic.
Regardless of duration of institutionalization, and inpatient or outpatient status, user-survivors experienced a number of similar types of traumatic events. Traumatic events relating to economic and resource loss, physical and verbal abuse, and development of illness were identified as the most commonly reported traumatic event that has been reported in all three groups, respectively. User-survivors in both long and short-term care services reported abandonment and rejection from family members, partners, and the community as common types of traumatic events – a finding that supports the hypothesis that patients tend to feel abandoned due to institutionalization, regardless of its duration. User-survivors in long-term care experienced additional traumatic events directly linked to their care facilities, including: forced institutionalization, abandonment by staff, bullying by fellow user-survivors, and traumatic experiences relating to mental health intervention practices that were applied during institutionalization.
Symptoms associated with trauma
During the free-listing exercises, user-survivors were asked to list as many problems associated with exposure to traumatic events as possible. Following the biopsychosocial model, these problems were grouped into emotional, physical and social symptoms.
Emotional symptoms
Emotional symptoms were characterized as any complaints relating to cognitive and behavioral practices as well as changes in mood. Respondents mentioned a wide range of such symptoms, many of which can be categorized under changes in cognition such as preoccupation and suicidal ideation. Changes in mood include feelings of fear, sadness, and anger. Other reported emotional symptoms included stress, emotional instability, and mental confusion (see Table 1).
Participant ECRC3 expressed feelings of numbness and preoccupation with thought in reaction to the traumatic event of being excluded from her daughter's wedding. Sometimes I will think about it. Sometimes when I think it over I will become blank. What am I doing … rather than thinking what I should be doing. I don't have understanding at all. Whenever I see a marriage procession, I will think even for my daughter it would have happened like this, but I was not able to see it. (ECRC3,F)
Physical symptoms
An extensive list of physical complaints due to trauma was generated from the free-listing exercise. The majority of these symptoms could either be classified under hyperactivity (high energy behaviors) or hypo-activity (low energy behaviors). The symptoms classified under hyperactivity included rapid heart rates, sweating, crying, fearfulness and shaking, whereas the majority of symptoms classified under hypo-activity included feeling physically weak, loss of appetite, motionlessness, and speechlessness. Other symptoms that could not be classified in either category include: fever, nausea, dizziness, upset stomach, and headaches.
Social symptoms
Social symptoms refer to negative effects on the individual's social interactions as a result of a traumatic experience. Results were classified as either symptoms of social interactions – those that reflect an inability to interrelate with others, such as self-alienation, social-isolation/rejection; or symptoms of social responsibility – symptoms that reflect levels of impaired agency in social such as: inability to take care of one's self or others or work. Respondent, UOP2 M, described his gradual separation from society and social responsibilities as a consequence of the child abuse he experienced. I feel estranged from society in general. You feel something is wrong with you and you don't want to face reality … Since I could never face reality I never really studied hard. I just had some vague goal like ‘I will do this and I will do that’, but I was not really focused and I was not goal-driven. I just lived in a mental fog. (UOP2, M)
Coping strategies for trauma
Coping strategies refer to the strategies used by user-survivors to handle the symptoms of their trauma. In many instances, these strategies have a positive impact on the wellbeing of the user-survivors. However, several negative coping mechanisms that may be detrimental to respondents' wellbeing were also mentioned.
Positive coping strategies
Many of the positive coping strategies mentioned by user-survivors can be grouped into four major themes: being mentally strong, having responsibilities to distract you, having a good level of knowledge and awareness concerning trauma, and having a good social support system.
Being mentally strong: User-survivors described the fact that survivors of trauma can only cope with it if they themselves can be bold and fearless. One user-survivor described being mentally bold as a more effective coping strategy than medication: “Even if I don't take it [my medication], I will be [fine]. At present I am bold, so if I don't take medication I am also fine.” (ILO5,F)
Distraction: Carrying out daily tasks, having the responsibility of caring for family, and getting a salary are all forms of distraction described as strategies to help one forget about their traumas, even for a brief moment: “If they will put them in that [job], they will be [better]. If you give them [a] salary, they will forget their illness for at least one day.” (ILO5,F)
Knowledge and Awareness: Described as paramount to improving wellbeing, one respondent emphasized that in retrospect, knowledge and awareness would have prevented the years of guilt and shame he experienced. If someone had told me at that age [about trauma], a lot of time could have been saved. If someone had told me at the age of 18, 19, or 20 when I was really struggling, when I didn't know what was going on, then I wouldn't be here today. I would definitely have been more functional working somewhere, I would have had a family … I started reading these books at the age of 26 or 27, but by that time it was too late. Half my life had gone. (UOP2, M) My family thinks … that I am normal, [that] I am perfectly healthy by taking these medicines. My doctor also says the same thing, taking these medicines my problem is resolved, but I feel enormous stress. I feel nobody understands me. (UOP2, M)
Negative coping strategies
Different forms of escapism were mentioned as negative coping strategies for trauma. One respondent described going away on a long trip in order to forget their troubles. Another respondent described his desire to become homeless. In this way, he hoped to be rid of all responsibility, in the hopes that all his troubles would go away. I have been thinking and I continue to think that one way out of this misery is to become a homeless person … . At least that is one of my coping mechanisms. By becoming a homeless person, I am just telling myself and the world that I am not going to take on this stress anymore. I have had enough. (UOP2, M)
Trauma pathways
One of the final themes that emerged from this study is the relationship between homelessness, trauma and mental illness. In their testimonies, several user-survivors expressed how they believed one led to the other. It was a recurring finding that user-survivors strongly believed that the experience of trauma has led to their mental illnesses and that these traumatic experiences are the reason why they were institutionalized.
One user-survivor expressed how the traumatic experience of her husband taking on a second wife had led to her mental illness: “My husband got remarried for the second time and brought in a second wife and from then on only I have become like this” (RC1, F). Another participant claimed that the development of her schizophrenia stemmed from the loss of her child during birth. As soon as I delivered [my] baby, they said the baby is dead. From then on this started to me. [I think they are related]. [At first] you get palpitations when your mind gets disturbed, and then later it is the same mind which gets upset. (RC5,F) In my house, they hit [me] and I was mentally upset. If we are happy then we can stay in the house itself and how nice that would have been. Because my husband hit me, I left my house and I came out and now it is very difficult. It has been fifteen years since I left my house and I came here. (ILO6, F)
Discussion
The results of this study highlight several important aspects of the experience and understanding of trauma in the homeless population of Tamil Nadu. The types of traumatic events experienced by the homeless and risk of homelessness cohorts were not found to differ greatly. We believe that due to their similar sociocultural backgrounds and socioeconomic standing – primarily low caste, wage-earning and poor individuals – members of both cohorts experienced similar types of vulnerabilities and daily stressors that put them at similar risk for exposure to trauma. Additionally, many of the traumatic events mentioned by the homeless cohort were experiences they faced prior to becoming homeless – further contributing to the similarities in experiences of these two groups.
There are several standardized checklists that reflect current DSM criterion for potentially traumatizing events. One trauma inventory commonly used in populations of persons with SMI is the Trauma History Questionnaire (THQ) (Hooper, Stockton, Krupnick, & Green, 2011). When comparing the traumatic events listed in the 24-item THQ with the list of traumatic events identified in this study, we found that most items on the THQ were relevant to the sample population of this study, with the exception of three items relating to exposure to dangerous chemicals, active participation in wartime, and forced sex labor. Despite this overlap, however, we observed that 12 of the traumatic events mentioned by respondents were not included in the THQ: sudden financial loss/loss of resources; adultery; partner taking on a second spouse; shame brought on family; abandonment by loved ones; lack of security/shelter; development of mental illness; stigma and institutionalization due to mental illness. These findings support the hypothesis that local conceptualizations of trauma strongly relate to social adversities and relationships among persons of low socioeconomic status in Tamil Nadu who are at risk of, or in situations of homelessness – a notion supported by previous epidemiological studies on trauma conducted in India (Pillai et al., 2016).
Many respondents reported that family disputes and subsequent shame and/or abandonment were important causes of trauma. This observation can be better understood by taking a deeper look at the role of familial and social relationships in the context of Indian society. As a whole, and despite broad cultural, ethnic, religious, linguistic, and socioeconomic variations, Indian society can be characterized as collectivist in nature, a view that emphasizes the importance of interdependence among people and stresses the priority of group goals as opposed to individual goals. The collectivist nature of Indian society is strongly reflected in family structure. The practice of extended family structures in which three or more generations reside within one household has been common throughout Indian history. While over the years, Indian family households are more commonly reducing to nuclear rather than extended family structures, unity and loyalty continue to be held in high esteem (Allendorf, 2012; Chadda & Deb, 2013). Broken ties and estranged relationships can cause great distress as reflected in many of the participant narratives in this study.
Comparing locally defined symptoms of trauma to DSM criteria for PTSD
In an effort to understand local symptomatology and idioms of trauma rendered as
Other theories of trauma
While several of the traumatic events and symptoms mentioned by user-survivors do not fit DSM criteria for PTSD, there are other theories that exist on trauma and its consequences that are worth considering. Psychiatrist Bessel van der Kolk has argued that chronic exposure to interpersonal traumas from childhood to adulthood results in very valid and debilitating psychological disturbances that do not necessarily meet the diagnostic categorization of PTSD as defined by the DSM. In his view, an exclusive focus on a categorical diagnosis of PTSD, may result in missing out on the full spectrum of post-traumatic psychopathology (van der Kolk, Roth, Pelcovitz, Sunday, & Spinazzola, 2005). From van der Kolk's perspective, the repeated childhood abuse experienced by user-survivor UOP2, followed by years of insecurity, suicidal ideation, and depression likely constitutes a trauma that may not be classified as PTSD as defined by the DSM, but may otherwise require medical attention.
Still more broadly, Francine Shapiro, the pioneer of Eye Movement Desensitization and Reprocessing (EMDR) considers the very classification of a traumatic event to be subjective. “By dictionary definition, trauma is any event that has had a lasting negative effect. We all know people who have lost jobs, loved ones, even possessions and who have truly suffered as a result. When you lose your piece of mind, or if you never had it, there can be serious physical and psychological consequences no matter what the cause” (Shapiro & Margot, 2004, p.1). With Shapiro's definition, the traumatic experiences of user-survivors, such as RC1 – a single mother in rural Tamil Nadu – who lost all her possessions in an attempt to repay a loan taken out to pay for her daughter's dowry and the story of user-survivor ILO10, whose husband left her because she was unable to bare children, would both be considered traumas.
The implications of divergent views as to what constitutes trauma in this specific population in India can be significant. A previous study on trauma in India found that most mental health professionals evaluate the impact of traumatic events on Indian populations using criteria derived from the DSM (Pillai et al., 2016). With these differing views, it would imply that based on their experiences, most user-survivors in this study would not classify as having experienced trauma. This mismatch between the lived experiences of individuals experiencing mental illness and the specialist labels of mental illness so commonly exercised by mental health professionals worldwide, has been described as “the credibility gap” (Patel, 2014). This credibility gap in turn contributes to the underreporting of the experiences of mental illness and the overall large treatment gap for mental illness experienced globally, and in south Asia in particular.
Strengths and limitations of study
This study adopted an exploratory approach, in which findings are based on the personal accounts and theories of the user-survivors in a population of homeless persons with SMI in Tamil Nadu. While this approach can accurately describe how patients experience trauma, it remains possible that patient delusions and symptoms caused by their mental illnesses may have at times distorted the facts and their recollection of the events. Nevertheless, the experience of trauma is highly subjective, and regardless of the facts of what has occurred, we believe that it is the patient's perception of that event that causes the experience of trauma. Additionally, due to the sensitivity of the topic, we believe that the number and types of traumatic experiences reported by user-survivors is an underestimate of actual prevalence rates. The reported number of instances of sexual violence (8%) for instance, are far below the average for this particular type of population. One study on women with SMI in India reported 34% of their cohort having experienced some form of sexual coercion (Chandra, Deepthivarma, Carey, Carey, & Shalinianant, 2003).
While the list of symptoms associated with trauma generated by the user-survivors serves as a starting point for the symptomatology of trauma in this context, many of the symptoms reported could also be part of an affective disorder or anxiety disorder. Further research on how user-survivors distinguish the symptoms of these three groups of mental disorders would be needed for a clearer description of the effects of trauma. Another important domain for further exploration would be the types of symptoms user-survivors associate with different types of traumatic experiences. Previous studies have indicated that different traumatic experiences have not only had an impact on the severity of symptoms, but also exhibit distinct symptom patterns (Kelley et al., 2009).
Several previous studies have explored the double burden of trauma in persons with SMI (Aakre, Brown, Benson, Drapalski, & Gearon, 2014; Álvarez et al., 2012; Lu et al., 2014; Minsky et al., 2015; Mueser et al., 2002). This study, however, adds to the sparse information available on patients' own accounts of their experiences with trauma in India. This research process has given user-survivors a voice to describe how they perceive and cope with situations of extreme distress. The diversity in responses towards triggers, symptoms, and coping strategies are a reminder of the importance of considering individual accounts when assessing trauma, and an important reminder for mental health professionals to consider the need for a shift towards patient-centered care.
Conclusion
This qualitative study of user-survivors' accounts of trauma in a homeless population of Tamil Nadu revealed a potential mismatch between local and DSM conceptualizations of trauma. This has important implications for research and clinical practice. Firstly, it points to the need for the development of more culturally appropriate approaches of identifying and addressing trauma that match local conceptualizations of health, illness, and distress. As described earlier, manifestations of trauma depend on cultural and societal responses to distress, coping mechanisms and perceived support (Kar et al., 2007). There is strong support for the notion that attempts to apply Western diagnostic criteria for trauma in different cultural settings has limitations. While universalist approaches may provide some benefit in gaining a global perspective on trauma, they may lack nuance or miss the mark altogether in local contexts where trauma is conceptualized differently (Patel, 2000). In order to be utilized by grass-root level providers of healthcare, more efforts are needed to develop protocol for identifying trauma from a local perspective (Patel, 2000).
Finally, this study sought to address current discussions on trauma among persons with severe mental illness. As van der Kolk argued, clinical work involving psychiatric populations rarely address traumatic experiences and its consequences (van der Kolk et al., 2005), yet high rates of traumatic exposure are evident in many studies of psychiatric disorders including schizophrenia, bipolar disorder, depression, and substance abuse (Aakre et al., 2014; Álvarez et al., 2012; Lu et al., 2014; Minsky et al., 2015; Mueser et al., 2002). The user-survivors in this study reported specific traumatizing experiences that negatively impacted their wellbeing and likely contributed to their mental illness. Due to the complexity of this double burden of homelessness and SMI, unresolved trauma might be impairing recovery. Unfortunately, because they often do not meet the standard DSM criteria for PTSD, these traumatic events may not be dealt with, hindering opportunities for effective treatment and recovery.
Supplemental Material
TPS909613 Supplemental Material - Supplemental material for “If somebody could just understand what I am going through, it would make all the difference”: Conceptualizations of trauma in homeless populations experiencing severe mental illness
Supplemental material, TPS909613 Supplemental Material for “If somebody could just understand what I am going through, it would make all the difference”: Conceptualizations of trauma in homeless populations experiencing severe mental illness by AR Gilmoor, S Vallath, B Regeer and JFG Bunders in Transcultural Psychiatry
Footnotes
Acknowledgements
The authors would first like to extend their sincerest gratitude to The Banyan for their continued support throughout the research process. It is only through their ceaseless dedication to the improvement of the wellbeing of their clients could this research ever be possible. The authors would also like to express their sincerest appreciation to the participants of this study – the user-survivors, whose narratives are a testament to the bravery and strength they continue to prove in their daily lives.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.