
Abstract
The relationship between vaccine hesitancy and antibiotic misuse remains complex and insufficiently understood, raising questions about whether these phenomena are directly connected or shaped by shared underlying factors. As vaccine hesitancy and antimicrobial resistance constitute intertwined public health challenges with serious implications for population well-being, it is crucial to explore how attitudes toward vaccination correspond with patterns of antibiotic use. This study examines antibiotic hesitancy and misuse among vaccine-hesitant parents in Portugal—a group often inclined toward alternative health practices in managing family health. Based on in-depth interviews with 31 parents, the findings reveal that participants critically reflect on medical interventions, frequently questioning the necessity and appropriateness of antibiotics. The study highlights consumption practices that diverge from biomedical guidelines, potentially increasing children’s vulnerability, and draws attention to the limited focus on antibiotic misuse in existing literature. Results confirm an interconnection between vaccine uptake and parental knowledge of antibiotics, suggesting that limited understanding of antibiotic roles is associated with delayed or refused childhood vaccination. Echoing patterns of vaccine refusal, parents who reject or selectively use antibiotics often adopt a ‘natural’ approach to health, reinforcing a broader social identity in which parents position themselves as experts in safeguarding their children’s well-being. These findings point to wider perceptions of risk surrounding conventional medicine and science in general, underscoring the need for more effective health communication.
Introduction
Antimicrobial resistance (AMR) is considered a major public health issue: causing more than 35,000 deaths every year in Europe. It is expected that a rise in AMR will lead to 10 million deaths each year at a global level. AMR may lead to prolonged hospital stays and rising healthcare costs (Rinaldi et al., 2025). AMR refers to the emergence of infections that can no longer be treated since bacteria have become resistant to antibiotics. AMR has been framed under the logic of the ‘One Health’ approach, which recognizes the interconnection between human, animal, and environmental health (Velazquez-Meza et al., 2022). Although antimicrobial resistance is framed in terms of this interrelationship, the solutions are often developed with a focus on individual behavior (Denyer Willis and Chandler, 2019). Research on AMR messaging suggests that it is underpinned by the ideal of self-defensive immunity and hygiene: citizens should autonomously seek information and act to self-govern their behaviors (Davis et al., 2022, 2023). Within this framework, citizens are blamed for inappropriate antibiotic use, although AMR is generated by social dynamics (Will, 2020). Antimicrobial resistance is a considerable threat to the health and safety of children: one in five deaths due to AMR happens in children (IHME, 2024). The overuse of antibiotics can physically harm children, as they are more susceptible to side effects such as diarrhea, allergic reactions, and fungal infections. These side effects often require observation in emergency departments, leading to an increase in healthcare costs (Sauerwein, 2020).
There is a need for a broader understanding of the complexity of AMR that takes into account the social and structural dimensions of our society (Kamenshchikova et al., 2021). While antibiotic prescription and consumption in the Global South may be a result of unsanitary conditions and be related to the prevention of infections (Denyer Willis and Chandler, 2019), in the Global North, antibiotic overuse has been identified as a product of defensive medicine and the disposition of medical care (Broom et al., 2017). Understanding the use of antibiotics requires examining the social context in which medical practice occurs. This encompasses the interactions among clinicians, especially the norms and hierarchies within the medical field (Broom et al., 2014), as well as the interactions between clinicians, patients, and their families (Stivers, 2002). The risk of harming an individual child might be overestimated by clinicians over the risk of AMR to society (Cabral et al., 2015). The act of prescribing may go beyond medical purposes and may be related to clinicians’ experiences and perceptions (Britten, 2008), as well as eventually parents’ needs for a medical solution to manage risk effectively (Knaak, 2010). Short-term risk reduction may be prioritized by clinicians when dealing with a critical situation over the long-term optimization of antibiotics (Caronia and Saglietti, 2017).
Nevertheless, while much research to date has focused on the overuse of antibiotics, misuse remains a significant challenge for the health and well-being of populations, particularly for children who are more vulnerable to infections. Misuse, whether through overprescription, self-medication, or the use of antibiotics inappropriately for viral infections, remains a critical issue, exacerbating the problem of AMR (WHO, 2022a). In parallel, vaccine hesitancy also presents a pressing concern, being a major public threat and compromising the health and well-being of children across the Globe. The relationship between vaccine hesitancy and antibiotic misuse is complex and not fully understood, leaving room for doubt as to whether they are directly connected or influenced by shared factors (Larson et al., 2014; Wagner et al., 2020).
Studies suggest there may be interconnections between vaccine hesitancy and antibiotic avoidance, often shaped by broader cultural and ideological factors. For instance, distrust in healthcare institutions, a preference for natural or alternative treatments, and ideologies surrounding self-care and personal responsibility for health play a significant role in shaping parental decision-making concerning vaccination (Crawford, 1980; Sulik et al., 2025). Parents who hesitate to vaccinate their children may also be inclined to avoid antibiotics, influenced by similar health beliefs and concerns. Nevertheless, while vaccine hesitancy and antibiotic avoidance may coexist, there may also be cases where one issue is present without the other (Lvovschi et al., 2022). Drawing on findings from the VAX-TRUST project, this study will investigate how vaccine-hesitant parents in Portugal perceive antibiotics and the decision-making concerning their use. While vaccine hesitancy remains relatively low in Portugal compared with other European countries (DGS, 2024), the country records one of the highest levels of antibiotic consumption in Europe, driven by high prescription rates (Machowska and Stålsby Lundborg, 2019). In this context, it is particularly important to understand the rationale underlying antibiotic use among vaccine-hesitant parents. Vaccination is one of the key interventions to address the emergence of antimicrobial resistance. By directly protecting against bacterial pathogens, vaccines can reduce the incidence of infections that require antibiotic treatment, thereby lowering antibiotic use and the associated selective pressure that drives the development of resistance. In addition, vaccines protect against viral pathogens for which antibiotics are sometimes inappropriately prescribed, or which predispose individuals to secondary bacterial infections through co-infection mechanisms (Anderson, 2022). Given that vaccine hesitancy and antimicrobial resistance represent interconnected public health challenges with significant consequences for population health, it is essential to examine the extent to which attitudes toward vaccination correspond with patterns of antibiotic use.
Background
Similarly to antimicrobial resistance (AMR), vaccine hesitancy ranks among the top 10 global public health threats, endangering the health and well-being of children and young people worldwide. These issues are interconnected, as low vaccination uptake can lead to a significant rise in infections, increasing antibiotic use and, ultimately, accelerating the development of antimicrobial resistance (Sulik et al., 2025). Vaccine hesitancy is a complex social phenomenon, broadly defined as a ‘motivational state of being conflicted about, or opposed to, getting vaccinated, including intentions and willingness’ (WHO, 2022b: 213). Research on vaccine hesitancy indicates that parents strongly criticize the current biomedical model and show a deep commitment to natural living (Mendonça and Hilário, 2023). A common belief among vaccine-hesitant parents is that long-term immunity is more effectively acquired through natural infection than through vaccination (Dubé et al., 2016). Engagement in labor-intensive parenting practices—often viewed as a means of strengthening a child’s natural immunity—has been identified as a key influence on decisions to delay or refuse vaccination (Reich, 2014). These practices aim to reduce a child’s exposure to perceived toxins and typically include breastfeeding, the consumption of organic foods, and the use of non-conventional forms of care (Mendonça and Hilário, 2023; Ward et al., 2017). At the core of these practices lies the deliberate regulation of a child’s exposure to perceived risks, a process that requires not only financial means but also significant commitments of time, education, and socio capital (Ward et al., 2017). These labor-intensive practices have been identified as a cultural logic of middle-class parents (Reich, 2014).
This strongly aligns with the ideology of intensive mothering, a concept introduced by Hays (1996) to describe a gendered ideal that promotes the expectation that mothers devote substantial time, energy, and financial resources to child-rearing. The mothers who adopt this intensive parenting approach tend to distinguish themselves from mainstream mothers by adopting an individualist approach toward health, one that considers their children’s singularity (Bobel, 2002). Within this ideology, parents—in particular, mothers—are cast as ‘risk managers’ and are therefore understood to carry a moral and social obligation to remain constantly vigilant and risk-aware (Knaak, 2010). This means that mothers often rely on their judgment to evaluate the risks and benefits of vaccination, rather than deferring to medical advice (Reich, 2014). Vaccine-hesitant parents often believe that placing blind trust in vaccines is seen as a potential risk and may harm their children (Hobson-West, 2007). This skepticism often extends to science more broadly, as many of these parents perceive pharmaceuticals in general as potentially harmful (Ten Kate et al., 2022). It is therefore essential to examine whether this logic shapes all health-related decisions made by vaccine-hesitant parents, particularly in relation to the use of antibiotics.
Methods
This article draws on data from a broader research project investigating vaccine hesitancy across seven European countries: Belgium, Czech Republic, Finland, Italy, Poland, Portugal, and the UK. Nevertheless, the present article focuses specifically on the data gathered in Portugal.
A qualitative research approach was employed, involving in-depth interviews with 31 vaccine-hesitant parents, conducted between November 2021 and May 2022. Participants were recruited through snowball sampling and social media. Although efforts were made to engage ‘alternative’ educational institutions, such as Waldorf schools, even though only one school responded to the invitation to participate (providing contact with a parent who agreed to be interviewed). The main inclusion criteria for participation were having a child aged six or under and having delayed or refused at least one recommended vaccine. Nevertheless, we decided to be more flexible regarding our sampling criteria, allowing the recruitment of parents with children older than six who had previously delayed or refused vaccination. Before the interviews, parents received an information sheet via email, outlining the VAX-TRUST project, and were asked to provide written informed consent.
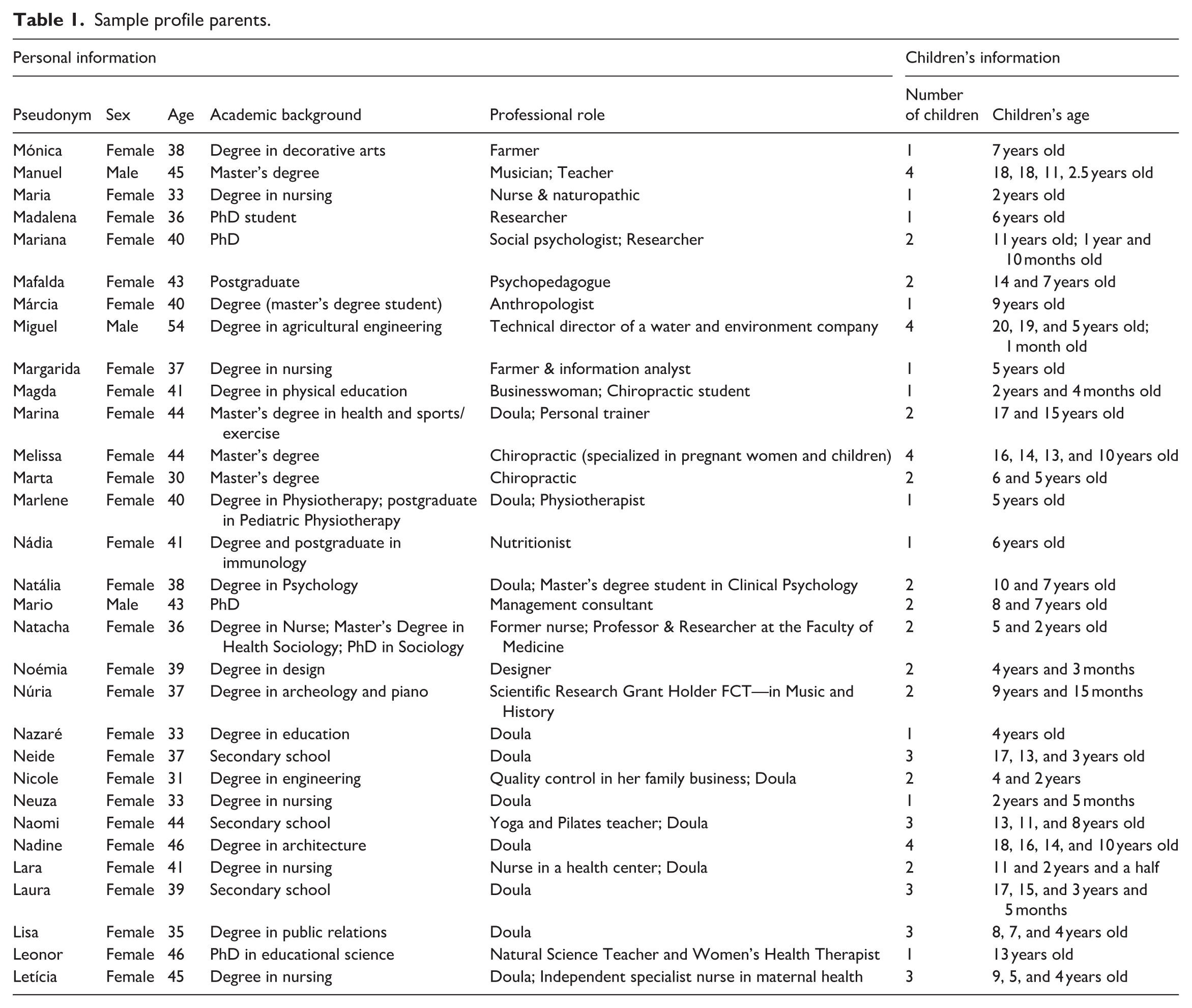
The interviews were conducted online via Zoom (between November 2021 and May 2022) by three experienced female research assistants, with each interview lasting between 39 minutes to 1 hour and 58 minutes. While their gender identity may have facilitated trust and rapport with the predominantly female interviewers, it also carried the risk of over-empathizing with vaccine-hesitant parents. Such risk was carefully monitored by the first author, who conducted frequent debriefing sessions in which they openly discussed the emotions and feelings that emerged during the interviews. This reflects the project’s alignment with an ethics of care framework. The interviews followed an interview guide developed by the team leader of the work package (Numerato et al., 2021), which was translated by the Portuguese national team and adapted to the research context. The interviews did not focus on antibiotic consumption, although the topic emerged spontaneously. Of the 31 parents interviewed, 28 were women and 3 were men, aged between 30 and 54. Most participants held university degrees (n = 28), and a significant number were employed in health-related fields, including doulas, CAM (complementary and alternative medicine) practitioners, nurses, and nutritionists (n = 21). A detailed participant profile is provided in Table 1.
Sample profile parents.
With participants’ consent, all interviews were audio-recorded and transcribed verbatim. Data analysis and coding were conducted in a series of systematic steps with the support of NVivo software. Following Braun and Clarke’s (2006) framework, an open coding process was initially employed to identify first-order themes concerning antibiotic use by vaccine-hesitant parents. Through a selective focus on antibiotic use, we advanced into more focused categories, which proved essential in unraveling the nuances and complexity of the findings. These focused categories were subsequently synthesized into core themes after a thorough review of the data. These core themes were discussed between the first and second authors. This helped to enhance the trustworthiness of the data analysis, as the first author’s gender identity and her experience as a mother of two vaccinated children (aged 5 and 9) could have made her judgmental toward certain views expressed by the interviewees. This highlights the process of critically reflecting on the researcher’s approach during data examination and coding. Data analysis followed an inductive approach, and theoretical saturation was achieved after this three-step process. Ethical approval for the study was granted by ICS-ULisboa, the host research institution for the VAX-TRUST project in Portugal.
Findings
Data collected in Portugal under the VAX-TRUST project revealed a compelling set of attitudes among vaccine-hesitant parents regarding the use of antibiotics in childhood. Four interrelated themes emerged from the analysis: (1) fear and reluctance toward antibiotics; (2) mistrust in healthcare professionals; (3) adherence to alternative health practices; and (4) commitment to a ‘healthy lifestyle’ as a preventive strategy.
Reluctance and fear toward the use of antibiotics in children
Vaccine-hesitant parents consistently expressed strong reluctance to administer antibiotics to their children, voicing concerns over their chemical composition, side effects, and long-term consequences for child health. Antibiotics were not merely seen as unnecessary in many cases, but as potentially harmful, invasive substances that compromised children’s natural development. “It doesn’t make sense to give a birthday cake full of sugar to a one-year-old, just like it doesn’t make sense to give antibiotics to a newborn. . .” (Maria, 33-years-old, 1 child)
Such views were grounded in a perception of antibiotics as synthetic and industrially produced, disconnected from what these parents consider ‘natural’ or ‘safe’ for children. Their fear often extended to the active ingredients, perceived to be harsh or even toxic, and to broader concerns about bodily integrity and microbiological balance. “These vaccines have an effect, and one of them is like antibiotics. They kill everything—the good and bad bacteria (. . .) You end up killing all the life in the gut (. . .) We are what we eat.” (Mário, 43-years-old, 2 children)
For these parents, antibiotics should only be used in specific and severe cases, when there is a clear bacterial infection and the benefits outweigh the risks. They believe that the regular use of such medication, especially in children, does not make sense, as they see excessive use as potentially disrupting the natural balance of the body’s microbiota, increasing antibiotic resistance, and weakening the immune system. They view the promotion of antibiotics as a common solution for health issues, particularly in children, as harmful and counterproductive, potentially leading to long-term complications. “Then people started to realize, and antibiotics themselves, too careful, too many antibiotics are harmful. Antibiotics save lives, but in excess, they do harm.” (Nádia, 41-years-old, 1 child)
For some parents, the rejection of antibiotics is not just a matter of skepticism toward their use but part of a broader, more comprehensive critique of pharmaceutical capitalism. They view the pharmaceutical industry as a profit-driven system that prioritizes financial gain over human health. These parents express concerns about the industry’s motives, particularly the perceived lack of transparency in its operations and the influence it has on healthcare practices. As one parent, Natália, shared: “The pharmaceutical industry scares me. What scares me even more is the lack of transparency. . . and the lack of questioning by people.” (Natália, 38-years-old, 2 children)
This sense of distrust is deeply rooted in a broader societal critique of the commercialization of health, where decisions about medicine and treatment are seen as more about profit margins than genuine care for well-being. For many of these parents, their skepticism toward antibiotics often goes hand in hand with a rejection of vaccinations, seen as another example of the pharmaceutical industry’s influence over public health. Marina, another participant, reflected on her own journey of questioning: “I felt that if it didn’t make sense to vaccinate my children - because, in my view, I’d be putting things in their bodies that weren’t healthy - then I started to question everything, right? Not just food, but also: does it make sense to give antibiotics?” (Marina, 44-years-old, 2 children)
This quote reflects a broader philosophy of ‘natural’ health, where parents seek to minimize what they perceive as undue medical interference in their children’s lives. What emerges from these narratives is the idea that antibiotics and vaccines are perceived as different manifestations of the same systemic issue: overmedicalization. These parents see both as products of a system that prioritizes chemical solutions over natural healing processes. In their view, the frequent use of antibiotics, like vaccines, is a form of unnecessary intervention that imposes on the child’s body, which should ideally be allowed to heal and develop its defenses without being subjected to frequent pharmaceutical treatments. This perspective reflects a growing movement toward questioning medical practices that, in their eyes, are driven more by economic incentives than by true health needs.
(Dis)trust in healthcare professionals and their prescribing practices
A central axis of resistance to antibiotics stemmed from mistrust in healthcare professionals and dissatisfaction with their prescribing behavior. Many interviewees criticized the overprescription of antibiotics, expressing the view that these medications were often prescribed without adequate diagnostic rigor or consideration of individual needs. For example, Madalena described her experience: “They prescribed antibiotics. . . but didn’t even check if it was viral or bacterial. The pediatrician just opened the question—whether antibiotics were even the right choice.” (Madalena, 36 years-old, 1 child)
This suggests that for some parents, antibiotics were prescribed as a default, without fully exploring whether they were the appropriate treatment, contributing to their skepticism toward medical recommendations. Madalena also shared another example where she questioned the necessity of an antibiotic: “At the time I just thought, okay, I’ll wait until tomorrow and see if he wakes up better. I gave him paracetamol so he’d sleep better, and said to myself: if he’s still unwell tomorrow, I’ll go buy the antibiotic and give it to him. But the next day, he was fine. So I never gave him the antibiotic. It was probably just an infection caused by teething that affected his ear a bit. But then the tooth came through, and the infection settled down. That was the only time I spoke to her [the pediatrician] again - never after that.” (Madalena, 36 years-old, 1 child)
This account highlights how parents actively question prescriptions and make their own decisions, guided by intuition or previous experience rather than blindly following medical advice. Similarly, Noémia recounted how she lost trust in her pediatrician’s judgment: “I went to the pediatrician, and she prescribed antibiotics. But we already didn’t really trust her anymore. I went to two or three other pediatricians (. . .) and they all said it was insane to give him the antibiotic she recommended.” (Noémia, 39-years-old, 2 children)
This demonstrates that, for many parents, the lack of trust in one professional leads them to seek second or third opinions, reinforcing the notion that parents are not passive recipients of medical authority but selective consumers who weigh medical advice against their understanding and knowledge. Moreover, some parents pointed out how such mistrust extended beyond individual doctors to the structure of medical interactions. For instance, Nicole described her experience with antibiotics as a process of continual doubt and second-guessing: “So we got the lab report later - it took a while - but when it finally arrived, it turned out that all the antibiotics I had been giving her weren’t the right ones. The report said she should’ve been taking something else, Clavamox or something like that. I went to the pediatrician and asked for the new prescription, and he was like, ‘Oh yes, it’s that one, that’s fine.’ So I got the prescription. . . but I never filled it.” (laughs) (Nicole, 31-years-old, 2 children)
This account reflects how parents, having lost trust, sometimes reject medical prescriptions entirely, even after receiving confirmation from healthcare professionals. Furthermore, the dynamics within medical encounters contributed to feelings of alienation, with parents describing a sense of being dismissed or judged when questioning prescribed treatments. As Noémia expressed: “They don’t leave much room for questions (. . .) The more questions I asked -‘Is this antibiotic really necessary?’ - the more it strained the relationship.” (Noémia, 39-years-old, 2 children)
This dynamic underscores how perceived disrespect or lack of meaningful dialog with healthcare providers can deepen mistrust, leading parents to override prescriptions. Neide, a 37-year-old mother of three, reflected on another instance of non-adherence: “I’ve been to emergency services before where they prescribed an antibiotic, and I didn’t give it to him—because I didn’t feel he needed it (. . .) I honestly don’t even know why she prescribed it in the first place. I think it was just out of precaution.” (Neide, a 37-year-old, three children)
This further illustrates that when parents feel their concerns are not addressed or validated, they are more likely to make decisions based on their assessments rather than adhere to professional advice. These experiences demonstrate that mistrust and dissatisfaction with healthcare professionals, combined with a lack of open communication, can significantly influence parental decisions about antibiotic use. The sense of being dismissed or judged during medical encounters often leads parents to make decisions based on their knowledge and instincts, contributing to patterns of non-adherence and resistance to prescribed treatments.
Turning to alternative health practices
Against the backdrop of biomedical skepticism, many parents described an active engagement with alternative health practices as substitutes for antibiotics. These included homeopathy, naturopathy, herbal remedies, dietary changes, and traditional knowledge passed through peer networks or family traditions. “I’ve treated myself with homeopathy at different points in my life and always had great results. When Martim was around four. . . I just thought it was too much [antibiotics].” (Núria, 37-years-old, 2 children) “I usually turn to homeopathy. Mainly homeopathy and also naturopathy (. . .) Because I started trying them and saw results.” (Marina, 44-years-old, 2 children)
These practices were not framed as fringe or secondary but as primary strategies for managing health. Parents often saw them as more holistic, respectful of the body’s rhythms, and better suited to treating the underlying cause of illness rather than suppressing symptoms. “It’s possible to manage with home remedies - like cleaning the nose with saline solution.” (Nazaré, 33-years-old, 1 child) “I use a natural method: monitor the symptoms for three days and see if there’s any improvement. I did that recently with a urinary tract infection Daniela had. She’s not showing any signs anymore. I still need to do a urine test - Júlia, remind me - I want to see how things are. But no, I didn’t give her antibiotics.” (Nicole, 31-years-old, 2 children)
For these parents, the preference for alternative treatments was driven by concerns about the potential harm of antibiotics and the discomfort they often cause children. In addition to avoiding processed medicines and chemical compounds, parents pointed to the logistical challenges and emotional distress associated with antibiotic use. As Nicole described: “It’s hard on me physically too - waking up every few hours to give medication, the whole routine. Just hearing the word ‘antibiotic’ made my daughter scream and cry. So I said, ‘Sweetheart, what should we do?’ I talk a lot with my kids, we have a dialogue. And she said, ‘Let’s try tea, Mommy.’ So I gave her rosemary baths, used citrine salt, which is antiseptic, and tried all that. I said, ‘Let’s see if this works.’ I don’t use deodorant, I try to go natural with these things. I make my own essential oils and massage oil because I suffer from hemorrhoids and I’m tired of taking medicine. It doesn’t make sense for hemorrhoids - we need to try something more natural.” (Nicole, 31-years-old, 2 children)
The role of online communities was also significant in disseminating and validating these alternatives. Through social media groups and peer-to-peer exchanges, parents could navigate health concerns while reinforcing norms that resist pharmaceutical interventions. Nicole shared how a social media group provided support for her: “I posted in the group and said, ‘Girls, my daughter has an infection. . .’ and the response was: sitz baths morning, afternoon, and night - with rosemary and essential oils.” (Nicole, 31-years-old, 2 children)
This illustrates the importance of these networks in reinforcing alternative practices and giving parents a sense of validation in their choices. Importantly, the preference for alternatives was often paired with an effort to find healthcare professionals who were open to integrative approaches - those willing to combine conventional diagnostics with alternative treatments. Marina, for example, said: “I’ve always chosen doctors who were medical doctors but also had alternative approaches (. . .) It made me feel safer.” (Marina, 44-years-old, 2 children)
Similarly, Núria reflected on her choice of pediatrician: “I decided to find a pediatrician who could support us, and I had great recommendations for her (. . .) I was on a waitlist for almost nine months, but eventually got in—and it was the best decision I made. When medication is needed, she prescribes it. When it’s not, we go with homeopathy. And it completely solved his recurrent ear infections.” (Núria, 37-years-old, 2 children)
This underscores how parents seek out professionals who respect their values and incorporate alternative approaches when appropriate. However, some parents acknowledged that antibiotics might be necessary in certain extreme cases. Nazaré, for instance, said: “But we’re also aware - and we trust our pediatrician - that when we’ve tried everything else and nothing is working, if antibiotics are needed, then they’re needed.” (Nazaré, 33-years-old, 1 child)
This reflects a conditional approach to antibiotic use, where avoidance is based on a personal threshold of severity and a strong sense of trust in the professional involved. Even in such cases, some parents had positive experiences with antibiotics. Nazaré shared: “We tried a cream for two days and it didn’t work. Then we switched to one with antibiotics - and it worked wonderfully.” (Nazaré, 33-years-old, 1 child)
The data reveal that vaccine-hesitant parents actively seek to avoid antibiotics in treating their children, instead opting for a variety of alternative health practices. Their motivations stem from concerns about the biological effects of antibiotics, as well as a desire to protect their children’s emotional and physical well-being. While they are not entirely opposed to medical interventions, their approach is shaped by a broader critique of pharmaceutical practices, preferring solutions that they believe are more natural, holistic, and aligned with their values.
Adopting a ‘healthy lifestyle’ as preventive strategy
Beyond moments of illness, many vaccine-hesitant parents embraced what they called a ‘healthy lifestyle’ as a foundational strategy to avoid medical intervention altogether. This lifestyle encompassed a range of practices aimed at promoting overall well-being and preventing illness through natural, non-pharmaceutical means. Parents emphasized specific dietary practices, such as limiting sugar and processed foods, reducing meat consumption, and promoting outdoor activities for their children. As Natacha explained: “We’re careful in other ways, like making sure they spend a lot of time outside, playing in nature, which we believe helps strengthen their immune systems.” (Natacha, 36-years-old, 2 children)
For many, these practices were not simply about avoiding medical interventions, but rather about fostering resilience and preventing illness before it occurred. The focus on outdoor play, fresh air, and exposure to nature reflects a belief in the body’s natural ability to fight illness, provided it is supported by a healthy environment and lifestyle. Food, in particular, played both a symbolic and practical role in these health strategies. Many parents saw proper nutrition as a preventive measure against illness, but also as a moral choice that aligned with values such as purity, responsibility, and control. As Naomi put it: “I’ve always been strict about their diet (. . .) They’re the ones who bring the healthiest snacks to school.” (Naomi, 44-years-old, 3 children)
This statement underscores how food choices were often framed as a form of discipline and responsibility, not just for health but as a reflection of parental values. By carefully curating what their children ate, these parents sought to maintain control over their family’s health, avoiding the influence of external, often commercialized, health systems. Similarly, Natacha described her family’s dietary approach: “At home, we follow a vegetarian diet, though we still eat meat and fish occasionally when we’re out. This choice is mainly for health and environmental reasons - we feel that reducing meat and fish is the right direction, not eliminating them entirely. Our children follow the same diet.” (Natacha, 36-years-old, 2 children)
This decision, rooted in both health and environmental concerns, reflects how dietary choices were part of a broader ethical framework in which food was seen as a key factor in nurturing a child’s well-being while also contributing to environmental sustainability. For these parents, avoiding processed and animal-based foods was a conscious choice that supported their vision of healthy living and holistic health, rather than relying on medical solutions like antibiotics. For many parents, the emphasis on food was not limited to nutrition alone but was part of a broader commitment to prevention. As Nazaré remarked: “Yes. It depends a bit, but we strongly focus on prevention through diet. . .” (Nazaré, 33-years-old, 1 child)
This focus on preventive measures rather than reactive medical treatments further reinforces their commitment to natural and holistic methods of maintaining health. Their lifestyle choices were not merely about avoiding illness but about cultivating a sense of responsibility for their children’s long-term health and well-being. Avoiding antibiotics, in this sense, was not just a reaction to specific prescriptions—it was embedded in a broader ethical and identity-based project of ‘natural parenting’. These parents framed their efforts not as reckless opposition but as conscious care rooted in autonomy, prevention, and critical engagement with dominant medical paradigms.
Discussion
The findings of this study are not in accord with those of Cabral and colleagues. (2015), who have found that parents tend to delegate responsibility for managing antibiotic use to clinicians. In contrast, the parents in our study do not always view clinicians as the sole experts, suggesting a shift in how medical authority is perceived. These parents regard themselves as the primary experts on their child’s health and, much like in the context of vaccination (Reich, 2014), sometimes rely on their judgment to assess the benefits and risks of antibiotic use, even when the child suffers from an acute illness (unlike what happened in Cabral et al. study). Research suggests that a lack of trust in healthcare professionals, as well as in the pharmaceutical industry, is at the heart of parents’ decisions to delay or refuse the vaccination for their children (Attwell et al., 2017; Yaqub et al., 2014). This distrust also seems to shape parents’ decisions about antibiotic use. While the role of trust has been widely examined in the context of vaccine hesitancy (Hobson-West, 2007), it has received little attention concerning antibiotic use in children. The complex interplay between trust and medication-seeking behavior has been highlighted in previous studies involving adult populations (Rinaldi et al., 2025). The current study shows that the lack of trust in healthcare professionals often prompts vaccine-hesitant parents to navigate the healthcare system in search of what they perceive to be the most appropriate solution for their children—one that aligns with their personal health beliefs. In their pursuit of the ‘truth’ about antibiotic use—mirroring their approach to vaccines—these parents engage in selective consultation, choosing healthcare providers who they believe support or validate their views (Deml et al., 2022). This aligns with the framing of patients as consumers, portraying parents as active, rational agents and informed decision-makers (Gabe et al., 2015).
Previous research on antibiotics has shown that antibiotic prescription by physicians can be influenced by their relationship with patients, as well as their feelings of responsibility toward an individual patient (Will, 2018). While previous studies have reported that physicians often feel pressured by parents to prescribe antibiotics (Cabral et al., 2015), this did not appear to be the case with vaccine-hesitant parents, who tend to favor alternative treatment approaches. Parental accounts suggest that, unlike findings from other studies (Wang, 2024), physicians in Portugal are generally reluctant to accommodate parents’ preferences when it comes to antibiotic prescribing decisions. When treating an unvaccinated (or vaccinated) child, physicians may eventually feel compelled to prescribe antibiotics as a protective measure for that specific child. Research by Cabral and colleagues. (2015) indicates that physicians are more likely to prescribe antibiotics when confronted with clinical uncertainty. This argument can be further extended to suggest that similar prescribing patterns may also arise in situations of social uncertainty. Vaccine-hesitant parents often deviate from what the biomedical model defines as ‘best’ parenting practices, which may lead physicians to perceive them as posing a potential risk to their children’s health. Echoing Rodrigues’s (2020) work on antibiotic use, this study highlights the importance of contextual rationales that shape certain consumption practices, which frequently diverge from biomedical notions of ‘rational’ or ‘appropriate’ use. In her work, Rodrigues highlighted how structural and relational factors can help explain certain consumption practices that do not align with the current biomedical model.
The study findings indicated that the refusal to use antibiotics on the part of parents is very much related to their lifestyle choices. These findings are consistent with existing research on vaccine hesitancy, which suggests that a commitment to ‘natural living’ is often viewed as a way to bolster the immune system, thereby diminishing the perceived need for medical interventions such as vaccines or antibiotics (Reich, 2016b). Similar to vaccines, antibiotics were perceived by these parents as artificial substances and, therefore, potentially harmful to their children’s ‘pure’ bodies (Brownlie and Sheach Leith, 2011). From the perspective of these parents, the refusal or delay of antibiotics—much like the hesitancy around vaccination—offers the child’s body an opportunity to strengthen its natural immunity (Lermytte et al., 2024). They believe that their preventive health practices not only minimize the perceived necessity of antibiotics but also reduce the need for vaccines. Similar to patterns observed in vaccine refusal, parents who reject or selectively use antibiotics often embrace a more ‘natural’ approach to health and well-being (Ten Kate et al., 2022). This illustrates a broader social identity within which parents are regarded as the experts, considering the health and well-being of their children (Wiley et al., 2020). The ideology of healthism (Crawford, 1980), evident in these parents’ accounts (Mendonça and Hilário, 2023), may conflict with the contemporary public health framework (Rodrigues, 2020).
The labor-intensive parenting practices described in the current study should be situated in middle-class privilege (Mendonça and Hilário, 2023). Following Reich (2016a), we argue that parental decisions—especially those made by mothers—regarding antibiotic use are shaped by their position ‘as educated, partnered and privileged’ (p. 683). The findings of the current study suggest that these parents often rely on an extended social network that sustains their decisions concerning non-antibiotic use. This is in accord with Reich’s work, who have noted that vaccine-hesitant parents have a higher social capital which ‘create and maintain subcultural norms that contradict broader social norms and provide sources of individual support for doing so’ (Reich, 2020: 7). The social identity of being a good parent—and particularly a good mother—is closely tied to the ongoing management of risk and the proactive engagement of health-promoting behaviors for their children (Deml et al., 2022). Studies on risk highlight the importance of situating risk within the lived experiences of individuals, emphasizing that risk is not static but a dynamic phenomenon, shaped and interpreted through everyday contexts and strategies of management (Webster, 2020). This is evident in the case of vaccine-hesitant parents, who believe that due to their preventive practices their children are not at risk of infectious diseases and therefore they do not need antibiotics. For these parents, the decision to withhold antibiotics from their children, much like the choice to delay or refuse vaccination, is closely tied to their understanding of what it means to be a ‘good parent’ (Casiday, 2007). This aligns with the ideology of intensive parenting, which conceptualizes parents as risk managers responsible for their child’s health and well-being (Romagnoli and Wall, 2012). Nevertheless, the health decisions these parents make may not always serve the best interests of their children (Yerkes et al., 2021). While these parents adopt health-promoting behaviors aimed at fostering their children’s well-being, such choices may unintentionally expose their children to greater vulnerability in the event of an actual infection. Risks of antibiotic misuse have not been sufficiently addressed, and therefore, the study draws attention to certain consumption practices that diverge from biomedical guidelines concerning the appropriate use of antibiotics, which might increase children’s vulnerability.
The findings of this study highlight a clear interrelationship between vaccine uptake and parents’ knowledge of antibiotics, suggesting that parents with limited understanding of the appropriate use of antibiotics are more likely to delay or refuse vaccination for their children. This observation is consistent with earlier research by Anderson (2022), which found that concerns about vaccine side effects are associated with individuals’ knowledge of appropriate antibiotic use in the management of infections. To date, the relationship between vaccine uptake and antibiotic consumption has received limited attention despite the interconnection between them. High vaccination uptake is expected to reduce antibiotic use, yielding benefits at both the societal level, by constraining the development of antimicrobial resistance, and the individual level, by minimizing the negative effects of antibiotic use on the microbiome (Anderson, 2022). This study provides valuable insights into the shared underlying factors linking vaccine hesitancy and misunderstandings about the role of antibiotics.
The study is nevertheless limited by its small sample size and the fact that most respondents are mothers. This is not unexpected, as vaccine hesitancy is low in Portugal, and mothers usually assume the main caregiving role. Furthermore, the sample was relatively homogenous, consisting exclusively of white individuals with high levels of education. This demographic composition is reflected in the findings, which align with the ideology of intensive parenting commonly observed among middle-class families, as well as with existing literature on vaccine hesitancy that highlights similar subcultural norms (Lermytte et al., 2024; Mendonça and Hilário, 2023; Reich, 2014). Future research could examine the perspectives of both mothers and fathers to gain a deeper understanding of their similarities and differences. Moreover, incorporating a more diverse sample with respect to educational background and economic capital may yield alternative insights into the topic.
Conclusion
The main findings of the study show that antibiotic hesitancy among vaccine-hesitant parents cannot simply be attributed to ignorance or irrationality. Rather, it is entangled in complex logics of resistance toward conventional medicine and, more broadly, science. The rejection of antibiotics is often justified through fears about industrial processes and biomedical overreach, mistrust in clinical authority, and an investment in non-pharmaceutical approaches to health. These parents are not disengaged but rather engaged differently with networks, philosophies, and practices that place bodily autonomy and natural living at the center of child-rearing. Understanding this orientation is essential for crafting more effective, empathetic, and context-sensitive health communication around AMR. While research on antimicrobial resistance (AMR) has largely focused on the overuse of antibiotics (e.g. Khazen and Guttman, 2021), less attention has been given to their misuse. This study highlights that misuse can also pose risks to children’s health, underscoring the need for further investigation into this dimension. Health policies should address vaccine hesitancy and the misuse of antibiotics as distinct challenges, while also considering the potential overlap between the two. Research has shown that integrated public health campaigns targeting both vaccine hesitancy and antibiotic misuse can be more effective in enhancing health outcomes and reducing the risk of antimicrobial resistance (Sulik et al., 2025; Wagner et al., 2020). If the overlaps between vaccine-related attitudes and understanding of antibiotic use identified in this study reflect broader parallels between forms of vaccine hesitance and parents’ comprehension of antibiotic use, then gaining deeper insight into how these phenomena intersect could be extremely valuable for enhancing public health communication as previously outlined by Anderson (2022). The study outlines broader perceptions of risk associated with conventional medicine and, more generally, science. Nevertheless, further research is needed to clarify this relationship, as parents’ perceptions of risk are complex concerning their children’s health.
Footnotes
Ethical considerations
Ethical clearance was obtained from Instituto de Ciências Sociais, Universidade de Lisboa.
Consent to participate
Written informed consent has been obtained from the parents who participated in the study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project has received funding from the European Union’s Horizon 2020 research and innovation program under Grant Agreement No. 965280. Fábio Rafael Augusto’s work is funded by national funds through the FCT – Fundação para a Ciência e a Tecnologia, I.P., under the Scientific Employment Stimulus – Individual Call (CEEC Individual), by project reference 2023.06935.CEECIND/CP2882/CT0002 and DOI identifier ![]() .
.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability statement
The data that support the findings of this study are available on request from the corresponding author. The data are not publicly available due to privacy or ethical restrictions.*