
Abstract
The aim of the study was to better understand the experiences of women living with a history of breast cancer by analyzing the metaphors they use to describe their experiences. Data were collected through individual narrative interviews with 10 women, who were between 4 years and 13 years post-diagnosis. Their narratives were analyzed using Interpretative Phenomenological Analysis. The results are presented from an existential perspective and are conceptualized using the metaphor of the home. Our interpretation suggests that participants were in search of a habitable world, seeking to (1) dwell in oneself, (2) dwell with others and (3) dwell in the world. The results were discussed using an intersubjective conceptual framework, enriched by the work of Stolorow on human suffering and emotional trauma. The study expands upon existing literature on the use of metaphors in cancer patients and contributes to reveal their richness and diversity, beyond the dominant war metaphor.
Keywords
Background
An increasing number of women are surviving breast cancer. The survival rate of breast cancer patients has improved in recent decades, such that today the 5-year survival rate is approximately 90% in North America (American Cancer Society, 2024; Ellison and Saint-Jacques, 2023). Yet, qualitative studies are still needed to understand the implications of having survived a life-threatening disease and being confronted with the symbolic and embodied traces that cancer leaves on one’s life in the long term. Research suggests that several years after a breast cancer diagnosis, most women continue to have medical, existential and relational concerns, as cancer leads to the experience of a disrupted sense of identity and corporality, altered relationships and fear of death (Le Boutillier et al., 2019; Smit et al., 2019). Indeed, many women struggle to find help to cope with these concerns and do not feel sufficiently recognized and validated in their persistent suffering (Fan et al., 2023).
This possible lack of validation and recognition during the remission period can contribute to women’s loneliness and complicate their existential journey (Assing Hvidt, 2017; Rosedale 2009; Ueland et al. 2021). After the end of oncological treatment, many women try to renegotiate their identity, body image and future, while family and friends encourage them to return to normalcy and rejoice in having “entered survivorship” and “beaten” cancer (Powers et al., 2016; Trusson et al., 2016).
This challenging situation faced by women who have survived breast cancer may be shaped by the prevalence of war metaphors in public and medical discourse about cancer, which depicts women as “strong heroines” and “triumphant winners”. For several decades, war metaphors have been the dominant representations of cancer, reflecting the “battle” of Western societies against cancer and, more broadly, human vulnerability (Marin, 2013). War metaphors (i.e., battle, combat, victory, military) can pose challenges to individuals in remission as they attempt to make sense of their suffering and awareness of finitude (Willig, 2011). They may feel that the war metaphor misrepresents their experience, as it inaccurately conveys a sense of cure, assumes a false sense of agency and demands a continuous optimism (Bodd et al., 2023). The combative representation of survivorship may also not capture either the ambiguity associated with concepts such as normality and health, often experienced by women in remission of breast cancer (Blows et al., 2012; Kaiser, 2008).
According to Paul Ricoeur (1978), metaphoric language and narratives are rooted in the very fabric of life. These faculties enable us to interpret and reconfigure our world over time and through ordeals. In healthcare, we know the importance of metaphors in cancer narratives. When metaphors are deployed, they have the potential to help patients in making their illness narrative more comprehensible and meaningful (Laranjeira, 2013). Metaphoric language can also facilitate emotional coping (Gustafsson et al., 2020) and communication about difficult topics (Casarett et al., 2010; Hui et al., 2018).
Susan Sontag’s (1978) seminal work, Illness as metaphor, has played a key role in drawing attention to metaphoric thinking related to illness. Her conclusion was that cancer is “encumbered by the trappings of metaphor,” and that it is vital to move beyond the metaphors present in popular discourse to avoid alienating people from a meaning that did not correspond to their singular experiences. Recent research on the use of metaphor in oncology still suggests that cultural conceptualizations of cancer are insufficient because they are predominantly limited to war metaphors, whereas the subjective experiences of cancer are highly complex (Parsi, 2016; Surh, 2021).
The literature indicate that cancer patients use metaphor themes of war and mystery to describe how cancer can be imbued with violent and unpredictable characteristics (Bodd et al., 2023). Also common, the journey metaphor may foster an existential view of illness, prompting reflections on identity changes and the finitude of life (Assing Hvidt, 2017; Bodd et al., 2023; Guité-Verret and Vachon, 2023). Other studies have explored blogs written by women with metastatic breast cancer and found other metaphors, such as the need to “unveil” cancer-related suffering (Guité-Verret and Vachon, 2021) and the feeling of being “imprisoned” and having their “lives put on hold” (Hommerberg et al., 2020). The view of metastatic illness as an “unfair battle” is prominent among other cancer patients, who acknowledged their lack of control and their desire to live with cancer rather than fight it (Hulse et al., 2024).
However, while many scholars and medical professionals have written about metaphors related to cancer in different ways, it must be said that empirical qualitative research has paid little attention to the personal metaphors of cancer patients, and even less to those of individuals in remission. In fact, the growing body of work on the use of metaphors in oncology (Harrington, 2012; Liu et al., 2024) reveals a serious lack of empirical and inductive research on personal cancer metaphors, since it consists mainly of editorial and theoretical articles or deductive research focused on examining the impact and function of war metaphors. The paucity of empirical and inductive research on cancer patients’ metaphors keeps research at a distance from spontaneous and diverse personal metaphors. The result is an incomplete understanding of their complex language and experiences. It is important to be critically sensitive to the implicit connotations of dominant metaphors (such as military ones) to foster individuals’ imaginative faculties to deploy alternate metaphors (Kirmayer, 2023).
Aim
Using an inductive approach, the current study aims to better understand the experiences of women who have survived breast cancer by analyzing the metaphors they employ.
The present study builds upon a previous study with a similar aim and design, where we specifically examined the “trace” metaphor used by women who have survived breast (Guité-Verret and Vachon, 2024). We found that these women had to adapt to four specific traces of cancer in their lives: the identity trace (i.e., cancer changes the way they live and perceive themselves as women and mothers, challenging their sense of biographical continuity), the existential trace (i.e., cancer makes them more aware of their mortality and limits, affecting their sense of security in the world), the bodily trace (i.e., cancer altered their self-perception and embodiment, leading to the an erosion of their self-recognition), and the narrative trace (i.e., cancer was part of their history and present identity, putting into question the concept of remission). The metaphor of the trace differs from the metaphor of the cancer hero living without any trace of cancer. We wanted to conduct complementary analysis to further explore the challenges of integrating these traces to inhabit the world.
Research paradigm and approach
This study was set within an interpretative paradigm (Ponterotto, 2005), adhering to a relativist view of reality. We believe that meaning emerges from the unique interactive dialogue between researchers and participants, who co-construct interpretations of the phenomenon they are studying. Smith et al.’s (2009) Interpretative Phenomenological Analysis (IPA) provided the theoretical and methodological framework. IPA focuses on exploring lived experiences in their own terms rather than fitting them into pre-existing categories. According to IPA, humans are inherently interpreting beings and participants’ narratives reflect their efforts to make sense of their experiences. Concurrently, researchers interpret reality, particularly the participants’ experiences. This is a “double hermeneutic,” wherein participants attempt to make sense of their experiences while the researchers interpret participants’ sense-making (Smith et al., 2009).
Given researchers’ interpretation of the studied phenomenon, a reflexive practice is required (Smith et al., 2009). IPA underscores that reflexivity entails neither disregarding knowledge nor setting aside subjective experience. IPA researchers initially strive to set aside their preconceived notions about the phenomenon to fully engage with each participant’s experience. However, they eventually draw upon their sensitivity and prior understanding of the phenomenon to deepen interpretation and stimulate imagination (Smith et al., 2009). IPA researchers must reflect on their pre-understanding and leverage it to enhance interpretation throughout analysis (Gadamer, 1989).
The rigor of our interpretative study was upheld using Tracy’s (2010) criteria. These included sincerity (e.g. transparency about methods and self-reflexivity on subjective values and inclinations), rich rigor (e.g. complexity of theoretical constructs and data interpretation), credibility (e.g. extensive use of quotes that support interpretations) and meaningful coherence (e.g. interconnectedness between literature, research foci and interpretations).
IPA is compatible with metaphor analysis. Human beings interpret their experiences by employing metaphors because they need to understand the meaning of what they are experiencing (Ricoeur, 1978). By definition, metaphors are a vivid source of meaning, producing a deviation from the usual use of words and thus enabling a re-description of reality (Ricoeur, 1978). Metaphors bring out a new way of questioning and living in the world. From a phenomenological perspective, the creation of metaphors enables humans to go beyond ordinary or scientific language. Metaphors thus take part to the subjectivation process that underpins the interpretation and integration of lived experience. The creation of metaphors is particularly interesting when it comes to the experience of cancer, as patients’ medical journey are at first strongly associated with a scientific objectification of their body/illness.
In the context of phenomenological research, participants’ use of metaphors during interviews signals important moments when they express and try to make sense of previously unarticulated or unexplored aspects of their experiences (Shinebourne and Smith, 2010). According to Ricoeur (1978), metaphors are a vivid source of meaning because they produce a departure from the usual use of words and thus enable a redescription of reality. Metaphors also create a departure from scientific language, enabling a subjectivation of reality, which is important in elaborating illness experience. This is why the creation of metaphors fosters the emergence of a new way of questioning and inhabiting the world (Ricoeur, 1978). Therefore, beyond thought, metaphorical language reflects existence and embodiment, that is, one’s feeling, sensing, relating, suffering, action, etc. (Finlay, 2015)
Methodology
Recruitment and participants
The study sample included 10 participants (see Table 1). We followed IPA guidance regarding the number of participants. Smith et al. (2009) recommend small samples of four to ten participants, depending on the researchers’ experience and interest in a more heterogeneous sample.
Medical and sociodemographic data on the participants.
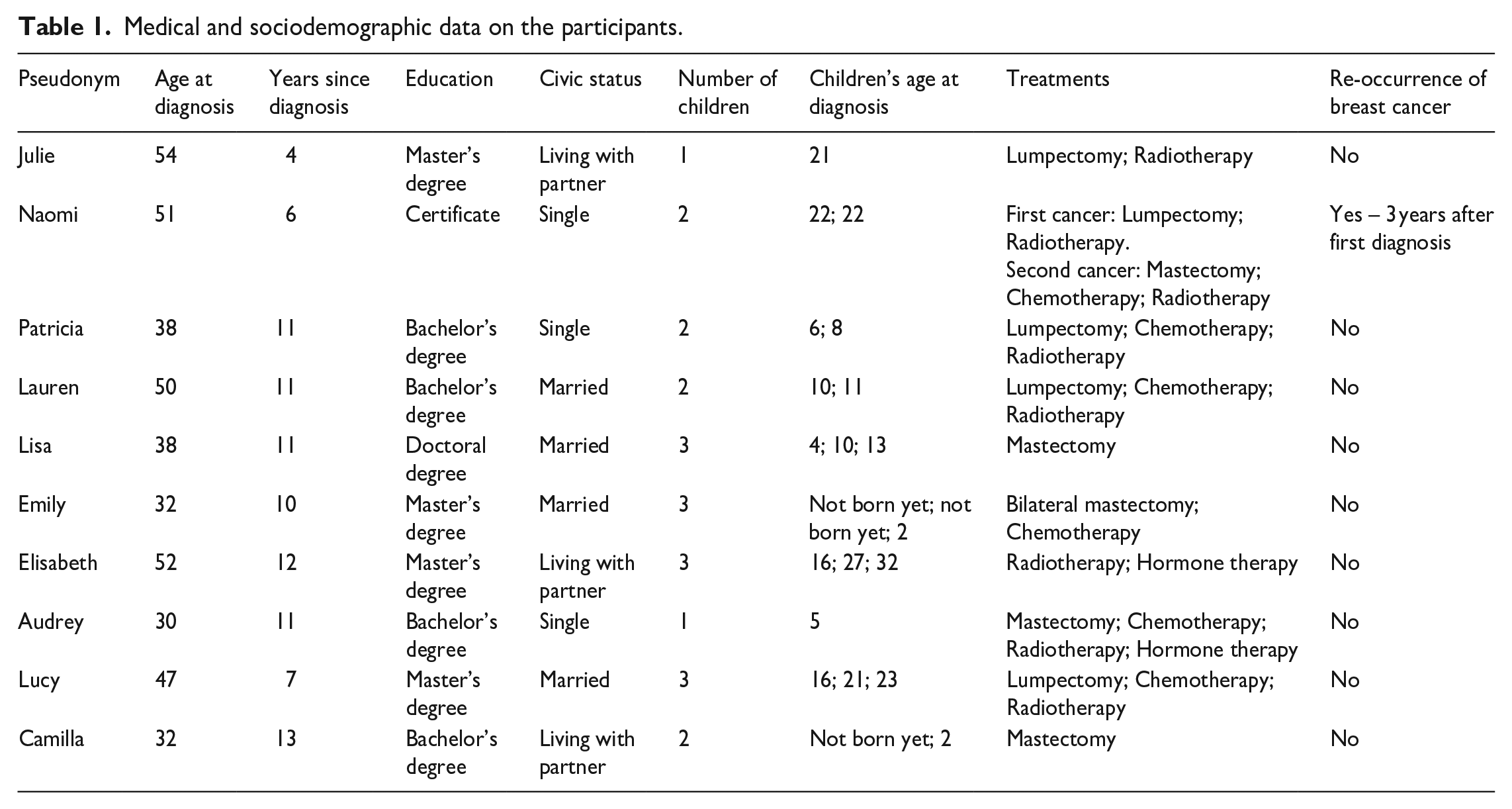
Recruitment was carried out via social media and local cancer organizations. Eligibility criteria included participants being 18 years or older, having received a breast cancer diagnosis and completed treatment at least 1 year prior and being proficient in French. Women who were interested and met the criteria were enrolled until we reached 10 participants. The mean age of the participants was 53 (range: 41–65 years old). Data collection for the participants spanned from 4 years post-diagnosis to 13 years post-diagnosis. One participant was not medically considered in remission from breast cancer.
Data collection
Individual interviews were carried out by the first author between November 2021 and January 2022. The interviews lasted between 60 and 180 minutes and were conducted at the locations chosen by the participants (n = 7) or virtually using an online platform (n = 3). Interviews were transcribed verbatim and anonymized using pseudonyms. Each interview began with the following statement: “Please tell me about your motivation to participate in this research study.” Afterward, we encouraged participants to tell their own stories using this question: “Can you tell me what has happened to you from the time you first suspected cancer until now?” As part of the dialogue, questions were asked to help participants deepen their understanding of their experiences: What do you mean by this? How do you feel about this? Do you have an image to describe this? Data collection was based on an inductive approach, which leads to a less structured interview. The interviewer has a single core interview question and how the dialogue unfolds will depend on how the participant answers this question in a personal and detailed way, but also how the interviewer supports the subjective elaboration of the story (Smith et al., 2009).
We did not ask about cancer metaphors, nor did we tell participants that we were paying particular attention to the metaphors they used. In line with Ricoeur (1978), we assumed that metaphors appear spontaneously in the process of making sense of experiences, and that individuals are not always aware that they are speaking metaphorically. While we did not impose metaphors on participants or artificially create metaphors, we did encourage them to develop a sense of their experience through our questions. According to Finlay (2015) says, the meanings of metaphors are not self-evident and therefore metaphors need to be “played with” and “worked through” in dialogue.
The study was approved by the ethics committee of Université du Québec à Montréal (no. 4615). Participants provided written consent to be in the research study and for publication. Because the research topic was sensitive, interviews was conducted very carefully. We tried to create a reassuring space where participants’ affects were welcomed, validated and integrated into dialogue. We were compassionately and responsively present, ready to “be with” each participant whatever emerged (Finaly and Hewitt Evans, 2022).
Data analysis
IPA (Smith et al., 2009) was used to understand participants’ experiences through the metaphors they spontaneously created. IPA is a flexible, iterative method for interpreting a particular phenomenon. It is more interpretive than descriptive, as understanding goes beyond a description of participants’ explicit statements. The analysis process was guided by Smith et al. (2009) and adapted for metaphor interpretation:
The first step involved immersing ourselves in the data. We read all the transcripts and took reflexive notes in the form of exploratory comments on each participant’s experience and context. We allowed space for our intuitions and affects, while trying to suspend our theoretical referents.
The next step was the analysis of a first transcript. We re-read this transcript with the intention of developing emergent themes and identifying any metaphors created by the participant. These themes and metaphors were compiled in a table, along with transcript quotes. We then searched for connections across emergent themes and began to link the metaphors and themes together.
We repeated step 2 with each of the other transcripts, attempting to bracket the ideas emerging from the analysis of previous cases as much as possible, while acknowledging that we were inevitably influenced by what we had already found.
The next step involved looking for patterns across cases. We linked the emergent themes and metaphors found in all the transcripts. To organize the themes and metaphors, we merged some themes or metaphors together, set aside uncommon or peripheral ones and established two levels of abstraction to generate sub-themes. At this stage, we began to think of the themes metaphorically to meet our objective of understanding the participants’ experiences in light of their metaphors. We went back and forth between the analysis and the transcripts to check the accuracy and meaning of the themes.
We then pushed the interpretation to a deeper level. The dwelling metaphor emerged from our reflection, as we felt it captured the meaning of the data as a whole. By mobilizing this metaphor, we metaphorically interpreted the participants’ metaphorical interpretations. We named each metaphorical theme accordingly (e.g. “Dwelling with others”). Metaphorical themes had to be supported by transcript quotes, in which at least one significant metaphor could be found. Again, we went back and forth between the analysis and the transcripts.
The final step was to write up the analysis. This process enabled us to deepen the interpretation and develop a better phenomenological description of the themes.
Theoretical perspective: The dwelling metaphor
Any phenomenon experienced by human beings can be conceived as the result of their belonging to a world and a body (Heidegger, 1962; Merleau-Ponty, 2013). Metaphorically, the body and the world are our fundamental “homes.” This conception of being invites us to consider what it means to “dwell” and sheds light on the concept of home often used metaphorically (Dekkers, 2011). In this study, data analysis led us to link the remission experience to the dwelling metaphor. We will introduce this metaphor by presenting what the literature has already discussed to clarify the theoretical perspective that guided our interpretation of the data, presented in the next section.
Dwelling can be conceived in terms of the delimitation and appropriation of a space, both real and symbolic, that contributes to the feeling of having a home and being at home (Bley, 2018). It is about finding one’s place, as opposed to feeling out of place (Marin, 2022). Dwelling refers to the sense of existing as an individual situated in a body and in a world, in need of intimacy and openness. In his later work, Heidegger (1971) stated that being at home was the fundamental aspect of human existence. To be a human being means to dwell, he asserted.
However, the world is not always or immediately habitable. The possibility of inhabiting the world depends on the place the individual assigns to themselves in the world and the place the world assigns to them. However, it also depends on the meaning the individual ascribes to their world and the meaning they attribute to their life accordingly. An uninhabitable world is one where the individual has no place because they cannot establish or feel sufficient links–in the sense of relationships and meanings–with themselves, others and the world. For the world to be habitable, it must be invested with subjectivity and meaning. It is habitable if it touches us and speaks to us (Heidegger, 1971). This is why the dwelling metaphor is connected to many fundamental notions in psychology and child development, such as security, comfort, reliability, belonging and holding (Finaly and Hewitt Evans, 2022).
Phenomenology does not rule out the paradox of dwelling. Home can lead to confinement or inauthenticity when an individual closes themselves off from the world or settles into familiarity or normativity (Heidegger, 1962). Moreover, while we generally think of “one’s place” as a guarantee of security, order and personal definition, it is also true that catastrophic life events can “displace” individuals, making them realize how limited and inauthentic the place they previously occupied was (Marin, 2022). For instance, a life-threatening illness may prompt a search for a more stable, peaceful and habitable world (Dekkers, 2011; Krabbe et al., 2023). Indeed, illness alters an individual’s habits and representations, disrupts their life story, creates an alienated contact with their body (Svenaeus, 2011). This can affect their capacity to dwell, while also triggering their need to dwell.
Results
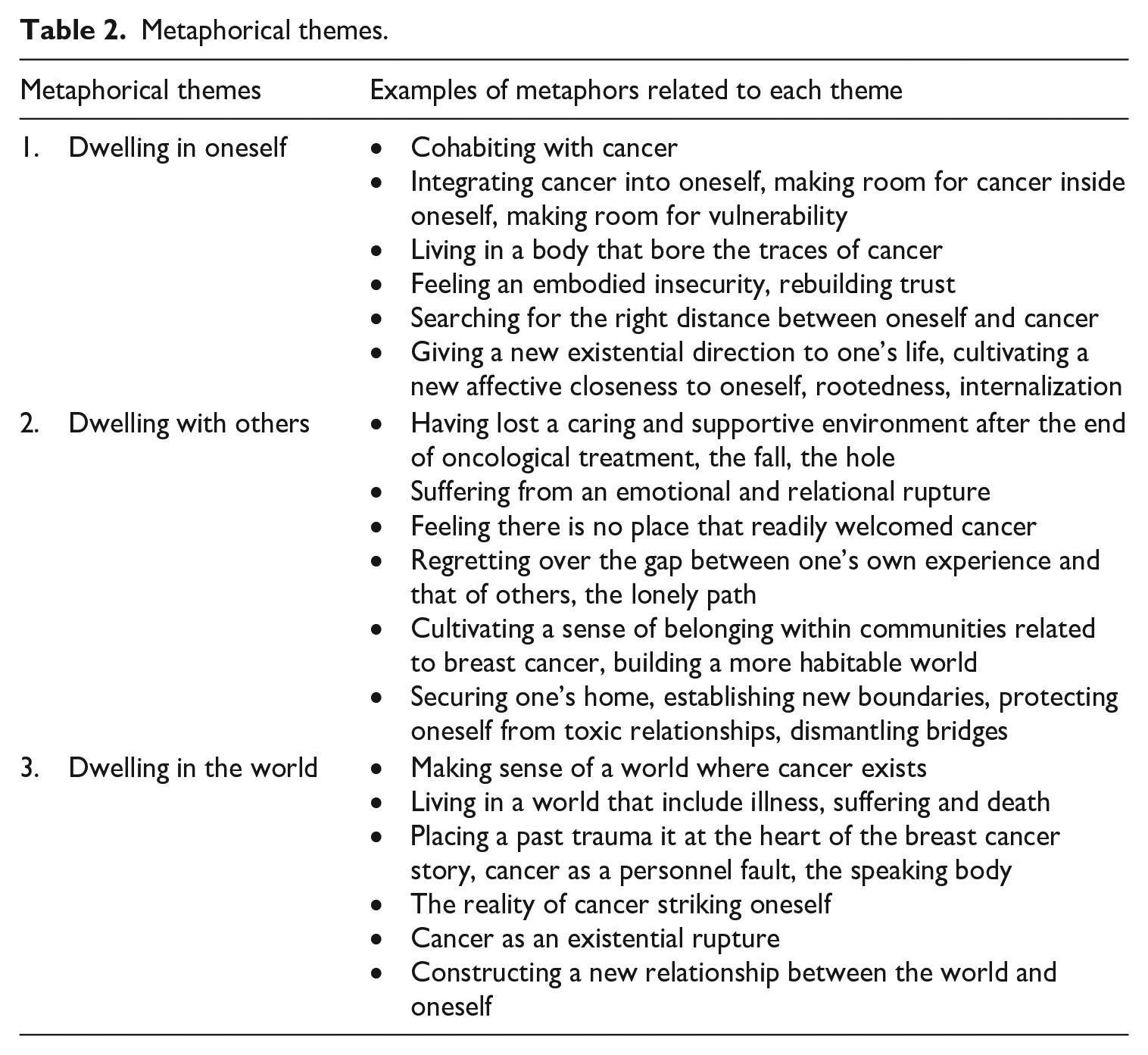
According to our interpretation, the dwelling metaphor captures the meaning of the experiences of women who survived breast cancer. Each participant sought a habitable world, aiming to (1) dwell in oneself, (2) dwell with others and (3) dwell in the world (see Table 2).
Metaphorical themes.
Dwelling in oneself: How to cohabit with cancer?
The participants described a complex process of integrating cancer into their bodies and into selves. It seems that they were driven by a persistent question: How can I cohabit with cancer? Living in a body that bore the traces of cancer and threatened by its recurrence proved challenging for many. Several participants lamented that their bodies no longer offered the guaranteed space of hospitality and protection they once did. Even years after treatments and surgeries, many did not feel comfortable in their own skin or recognize themselves in bodies altered in capacity, shape and sensation. Participants also feared that their bodies would once again host a cancerous tumor that could lead them to death. Therefore, their bodies became both a symbolic and physical place difficult to inhabit. It was as if they carried a sense of failure, risk or strangeness. This embodied insecurity appeared to affect their approach to life, now characterized by suspicion and powerlessness. This is what the metaphor of rebuilding trust suggests:
Cancer isn’t a car that hits you. It’s not a virus you catch. It comes from within you. I admit that it takes a lot of work to regain confidence, to rebuild trust in my body. There was somewhat of a betrayal. . . The post-cancer period is partly shaped by that. (Lucy)
According to our analysis, participants had to integrate the reality of cancer by negotiating its symbolic place within themselves. It seemed crucial to define the appropriate distance between themselves and breast cancer, so as not to disappear behind the disease, yet also not to deny its existence and impact on their experiences. Several participants seemed to conceive freedom as establishing this distance from cancer, though maintaining it was challenging due to the enduring traces of cancer in their lives. For instance, Naomi contrasted cancer with her “home” and endeavored to keep cancer out:
I don’t have cancer anymore! It’s not mine. I’ve got my home, and I’ve got my car. You know sometimes I’ll say: “my cancer”, then I try to bring myself back to saying THE cancer! [Interviewer: How does it make you feel to go from “my” to “the”?] Well, it’s just that the “my” is like keeping it with me! I don’t want it anymore! (Naomi)
Interestingly, at another point in her interview, Naomi mentioned that cancer had “saved” her by pushing her to make significant changes in her life. This ambivalent posture between distancing and integrating cancer was common among the participants. Many experienced a change in their relationship with themselves. It seems that cancer compelled them to confront their vulnerable selves, and over the years, they made room for it inside themselves. It appeared to us that this process involved a deliberate move toward self-care. This movement toward oneself contrasted with the pre-diagnosis period, which might have been associated with forgetting the vulnerable self. The metaphor of reorientation captures this interpretation:
It is true that having cancer defines who I am today. I choose myself differently. Now, I value things that are. . . crucial. Cancer forced me to change certain things, even if I’d rather not have had to. I’d say it’s a reorientation. (Emily)
It appeared important to the participants to give a new existential direction to their lives by cultivating a new symbolic and affective closeness to themselves, especially as cancer had taken up so much space. Connecting with themselves through a process of subjectivation of illness held the promise of greater freedom, solidity and security. This is reflected in the metaphors of rootedness and internalization:
I’m alive. It’s like I’m even more alive than ever. Cancer brought me closer to myself. I know my roots better, and, so, I don’t feel like a survivor! (Audrey) Even today, when I have scans or medical exams, I don’t feel like talking to other people about it. I’ve realized that I’ve lost the need to talk all the time about what I was going through. Cancer has internalized me. (Elisabeth)
In essence, participants were ambivalent about cancer; they questioned their ability to make room for cancer in their home and, simultaneously, to make room for vulnerability in their idea of themselves.
Dwelling with others: In search for a relational home
Most of the participants recalled the end of the oncological treatment, as it marked the loss of a caring and supportive environment (e.g. nurses, social workers, the chemo room). During treatment, they seemed to dwell this environment as a temporary home where they could settle in and be more authentic. Their concrete family homes, however, were no places that readily welcomed cancer and its existential meaning. After losing relationships with healthcare providers and hospital visits, many participants no longer experienced the reassuring feeling of being cared for and recognized as vulnerable human beings:
It was my last treatment. The nurse took the needle out and she said, “That’s it! You’re not coming back here, your journey has just ended!” I got out, got in my car. I was so helpless. I really found that part difficult because it was a place, you know like, I was so hyper-responsible when I was at home but when I was going there, it was a place where I could really let myself go. It was a place outside the house, where I’d go and settle in. . .You know, count on people. (Lucy)
The women’s stories highlight the suffering arising from the absence of individuals who watch over the vulnerable self and monitor the physical body to prevent tumor recurrence. It appears that loved ones and healthcare providers needed to witness their strength and restored health, often forgetting their vulnerability. The metaphors of the fall and the hole point to a emotional and relational rupture:
I feel like the caregivers are with you for so long and when it’s all over, they’re not there anymore. You know, just meeting the doctor is a relief because you know someone’s watching you. When you fall down all alone, with no one taking care of you, well, that’s when it hits you harder. (Patricia) People often think that when you’ve had an operation, when you’ve finished your treatments, that’s the end of it. You’re no longer a sick person, you’re no longer a person with needs. For me, that was like a hole. I realized that I was on my own. (Audrey)
After completing treatment, most participants sought a new relational home. It was as if they were looking for a more resonant world, that is, one that would be receptive to their experiences and where they could recognize themselves. Several participants expressed regret over the gap between their own experience and that of others, who they felt were either unaware of their enduring suffering or unwilling to acknowledge it. The metaphors of shock, the lonely path and the mirror echo this lack of resonance:
I’m ready to talk about it, but the people close to me, they’re somewhere else in their minds. I don’t believe they think about cancer every day now. If I talk about it, it’s like I’m taking them out of a state where they’re comfortable, and then bang!. . . Eventually, nobody’s interested anymore, you understand? Illness is a lonely road. (Lucy) Even after 10 years, I need to talk about it and people are exasperated because they don’t know what to say or do. People are not able to take it, to receive it, in the long term. It’s too painful, I think, because they see that remission isn’t quite there yet. In chronic or degenerative illnesses, patients are often alone because of this. It’s a mirror that hurts. (Audrey)
Many participants also sought to support other women affected by cancer, with whom they shared a more immediate resonance. They often found a sense of belonging within communities where they could connect (e.g. breast cancer organization, support group or dragon boat team). Through their compassion and solidarity, it appears they contributed to building a more habitable world. In the following quote, the use of the metaphor of repair suggests that restoring one’s relationship with the world and oneself is possible:
Three people close to me have been diagnosed with cancer and I’ve accompanied them. I’m still with them, because for some it’s not over. It gives so much meaning. . . It fixes something. You know, when I talk to them, I feel that deep down, I’m talking to myself too. It’s good for me. (Lucy)
Many participants also found it necessary to secure their homes. Several spoke of how illness had prompted them to protect themselves from toxic relationships. The remission period brought about an awareness of and the establishment of new boundaries between themselves and others, essential to cohabit with others. For many participants, this involved dismantling “bridges” between themselves and the world and building more suitable ones. As Lauren expressed though the metaphors of reframing and setting limits, not everyone is welcome in this new home:
I’m reframing my life. I made myself a frame, and I’m very comfortable with it. I don’t need everyone to love me. From now on, I have a limit. And when people abuse me, well that stops. It’s too much. It stops there. (Lauren)
Dwelling in the world: How to make sense of a world where cancer exists?
We found that participants grappled with how to make sense of a world that includes their cancer. Illness had disrupted many their beliefs and expectations about life, making their world largely incomprehensible and thus inhabitable. It seems that all participants had been confronted with the existential reality that the world includes cancer, suffering and death, thereby making them vulnerable. Implicitly or explicitly, they questioned the meaning of illness: Why me? Why breast cancer? Why now? We understood that over the years, they had created a narrative around what had happened and what they had experienced since diagnosis.
Some participants seemed to find answers to their existential questions by interpreting their traumatic life histories as the cause of breast cancer. For these participants, past trauma was seen as attributing meaning to the cancer, placing it at the heart of a history marked by suffering. Finding meaning and a cause within themselves allowed them to maintain their understanding of the world, as if cancer were a predictable consequence of an inherent evil. In Julie’s story, this is encapsulated by the metaphor of the fault:
I felt lost. I think that for people with long-standing traumas, cancer is often like a crack. It’s like a small opening. And then it intrudes, it enters into that crack, and it spreads. . . I remember my first thought was: I’m being punished. Because, when I was a teenager, my brother-in-law molested me. He touched my breasts. He was like my father, I adored him. . . I never said anything to anyone. . . When I got the diagnosis, I thought: Oh my God, this is my punishment, and it’s because of this that I have cancer. (Julie)
As a result of trauma, there is a crack in the wall of the house, and this crack is a sign that something serious is wrong with it. The self-attribution of cancer appears problematic as it situates the evil within oneself. However, it also enables one to locate within oneself the reason for this evil and its potential solution. In this way, it becomes possible to embark on a path of understanding and empowerment against profound powerlessness. For some participants, the remission period was a time of possible reparation through the creation of a world more inhabitable than ever before. The metaphor of the speaking body presents cancer as a warning that a change in trajectory is possible:
For me, it’s a kind of, you know when we say our bodies talk to us. This is me. I think our bodies talk to us. A friend of mine said: “I think you needed to rest!”. . . If it hadn’t been for cancer, I don’t know where I’d be today. I don’t know. (Naomi)
Other participants did not evoke past traumas during interviews but viewed cancer as a traumatic event in itself. Those participants focused on understanding the place of cancer in their current lives rather than in their past lives. For instance, many participants seemed to want cancer to occupy a more predictable place in their world in order to feel less insecure and powerlessness. This process manifested as/involved fluctuations/shifts between phases of ordinary life (characterized by forgetting the cancer experience and its reality) and periods when cancer resurfaced in their consciousness (leading to cancer-related suffering and thoughts, including intrusive recollections). This process is captured in the metaphor of the reality of cancer striking oneself:
There are days when I say to myself: Oh my God, it really happened! Cancer comes back any day. Like any trauma, I think it depends on how you feel about your day. You know, it’s a bit like mourning. There are times when you’re going to feel more vulnerable or more tired or more like this, and then bang! It hits you, and you won’t know why! It may have taken six months and then you ask yourself: How’d that hit me? It could be anything, something you’re not aware of. Your subconscious operates and you remember. Some other days you understand more why it’s hitting you. (Patricia)
In summary, we found that all participants tried to situate the reality of cancer within their new understanding of the world to make it habitable. The experience of breast cancer was a rupture in existence, and the return to everyday life after treatment involved searching for the meaning of this rupture and constructing a new relationship between the world and oneself. It should be added that at times, participants could conclude that the cancer had no meaning at all, which, in our view, is a way of giving meaning and even participating in the ongoing search for meaning.
Discussion
Cancer is a deep-felt confrontation with existential realities such as pain, isolation, death and meaninglessness; life takes on an unhomelike character. Therefore, it puts into question the way one inhabits the world. Cancer diagnosis and treatment weaken the structure of one’s home. During remission, one tries to rebuild a home, which will differ from the original in the way it is inhabited and understood. There is a transformation of home and its meaning structures as a result of the “transgressive encounter” with illness (Assing Hvidt, 2017).
In our study, one of the participants’ essential needs was to dwell, that is, to find a place in themselves, to feel at home in their bodies, to feel at home with their loved ones, and to experience the world as meaningful and “homelike” (Svenaeus, 2011). Yet meeting this need was not easy, as the house was permeable to cancer, which penetrated at every level (self, body, relationships, meaning of life, worldview). For the participants, searching for a habitable world was like an unfinished process of “reuniting” with oneself, others and the world (Krabbe et al., 2023). In light of this study, it seems difficult for participants to cohabit with cancer and find a sense of unity following cancer treatment. In fact, our results highlight the participants’ ambivalence toward cancer, which may stem from their trouble integrating their own vulnerability and mortality. This could be because in remission, the lines between illness and health, well-being and suffering, as well as alienation and autonomy become blurred (Blows et al., 2012).
To better understand this existential ambiguity, we can draw on Stroebe and Schut’s (1999) dual process model of coping with bereavement. This model illustrates a process of oscillation, where the grieving individual alternates between confronting the loss (loss-oriented attitude) and avoiding it (restoration-oriented attitude). Stroebe and Schut (1999) emphasize “the need for dosage of grieving, that is, the need to take respite from dealing with either of these tasks, as an integral part of adaptive coping”. (p. 197) Drawing a parallel with our findings, we observe that our participants were ambivalent about cancer and their vulnerable selves. Their experiences seemed to balance between two approaches to post-treatment life. At times, they made place for cancer in their homes, cared for their vulnerable selves by integrating it into their homes, struggled with the intrusion of cancer reality in their lives and hoped to receive support as legitimate vulnerable human beings. At other times, they distracted themselves from cancer, embraced life changes with great motivation, sought to distance cancer from their homes, and chose not to focus much to their vulnerability in order to feel empowered and responsible toward others. The women we encountered revealed that it is challenging to acknowledge human limitations and to make space in one’s home for highly complex emotions.
In this regard, the dwelling metaphor contrasts with the war metaphor often used in cancer medical discourse, which portrays cancer as an enemy to be battled and eradicated. Our study suggests that after undergoing treatments aimed at “fighting” cancer, participants shifted paradigm; they felt the need to “integrate” the reality of cancer in their homes, to “be at one with” the world while accepting that cancer and human finitude are part of that world. We consider that war metaphors should either be reinterpreted or complemented by metaphors that emphasize coexistence with cancer (Nie et al., 2016) and do not risk reducing a complex individual’s sense of self to that of a cancer-free survivor (Malm, 2016).
Intersubjective interpretation of the results: How to provide a home for ambiguity and trauma?
It is important to recognize that the quest for a habitable world and the search for meaning after a breast cancer diagnosis occurs within a specific cultural context. As Willig (2011) argues, capitalist ideology emphasizes individual responsibility (for health, resilience, success, certitude) but provides limited space to tie back to express ambiguity, powerlessness or frustration. The women we encountered lived in a world where inhabiting vulnerability was nearly impossible. This is particularly pronounced for women, who are expected to be strong—they are the ones who hold children’s unbearable emotions and hold the family home together. Yet, upon leaving the hospital after cancer treatment, whom do they return to? Under what roof can they freely express vulnerability and their emotions?
According to our findings, participants struggled to reconcile their limitations with their responsibilities. They sought to find their place, take care of themselves and manage their health independently. They also felt responsible to take care of their loved ones, sometimes even concealing their experience of vulnerability. Many participants hoped to redefine the boundaries of their homes by inviting individuals who could make them feel safe and connected. Despite these efforts, there was often a lingering sense of isolation, as if they bore a solitary burden (Ueland et al., 2021). To some extent, they were assuming care. This situation echoes feminist ethics of care, which assert that human beings make the world habitable by caring for both the world and themselves (Fleury, 2019).
We are concerned about these women who “wander” the world looking for help, connections and dialogue. We share the concern of MacDonald et al. (2021), who argue that as long as the pursuit of a biomedical cure dominates oncological care and confines care to the hospital, those who are cured but not healed may be forgotten. In this regard, the clinical work of Stolorow (2011) on emotional trauma is relevant to the question of how women who survived breast cancer can be supported in the context of a lack of support in their community and surroundings. Like many phenomenological-oriented researchers, Stolorow posits that an individual’s ability to integrate their suffering and life story is shaped by the responsiveness of their relational environment. Accordingly, Stolorow (2011) developed an intersubjective approach to trauma, which he defined as an experience of unbearable emotions. According to him, trauma is constituted in a relational context where suffering lacks a “relational home” for processing and understating. It is the absence of adequate attunement to one’s painful emotional experiences that renders them intolerable. The main idea is that every individual confronted with a traumatic event such as death-confrontation need a responsive other who can help them tolerate, articulate and ultimately incorporate this event. In therapy, the goal is for the patient to feel understood and held by the therapist, who serves as a relational home for trauma and existential vulnerability.
While we do not consider that all participants in this study suffered trauma, our results indicate that cancer can indeed be a traumatic event and be interpreted as such by women. Breast cancer is experienced as a confrontation with death (which calls into question invulnerability and immortality), treatments (which involve pain, powerlessness, objectification and distressing long-term memories) and biographical disruption (Bissler, 2012; Leano et al., 2019). Breast cancer can also be experienced as the repetition of a past trauma through the perception of a relationship between the trauma and the development of cancer (Niebauer et al., 2021). For some of our participants who experienced developmental trauma, breast cancer took on a meaning related to a well-known sense of insecurity and alienation. In this perspective, trauma and cancer share the fact that both can be intensely disempowering and alter one’s sense of self and place in the world (Niebauer et al., 2021). Similarly, trauma- and cancer-related suffering can be healed in the context of secure, supportive relationships with others (Assing Hvidt, 2013; Davidson et al., 2023). In accordance with Stolorow (2011), we believe that intersubjective-oriented therapists can play an important role in supporting people who have survived cancer, not only by trying to understand the suffering patient from their perspective, but also by welcoming suffering and facing it head-on. By doing so, the therapist “participates” in the painful emotions rather than avoiding or soothing them. The key feature of care is the importance of a secure place where the suffering patient can express the unspeakable to understand the incomprehensible.
While the benefits of intersubjective therapy are considerable, the care of women in remission of breast cancer should extend beyond healthcare professionals. It is advisable for interventions and research to be rooted in a holistic, even systemic approach that includes the women’s loved ones who can contribute to their well-being. For example, valuable knowledge can be borrowed from palliative care (MacDonald et al., 2021). Applying the principles of palliative care to remission care can establish congruence between women’s desire to achieve a habitable world and the availability of a relational home in which human limits are consciously acknowledged and shared. Women and their loved ones may learn to tolerate vulnerability together when it arises and allow themselves to be transformed it. For those who did not experience cancer, the challenge can be considerable: listening without immediately reassuring, allowing oneself to be touched by the vulnerable other and letting cancer enter the shared home.
Study contribution and limitations
This study makes an important methodological and empirical contribution to the understanding of cancer patients’ metaphors. It stands out for its design, which is based the non-disclosure of the study’s focus on metaphors. The approach highlights the value of non-directive, interactive dialogue in allowing participants’ creative, complex metaphors to emerge. Our inductive approach allowed us to present a rich symbolic conceptualization of breast cancer that complements the most dominant metaphors.
When we shared and dialogued with participants about the study findings, many of them told us they were moved by the findings and grateful that we had taken time to make their voices heard. For example, one participant said that she wished we could take this “message” to the medical teams. Another woman said that it helped her to “see things more clearly.” This feedback from participants points to the subjectivizing power of metaphors and dialogue. According to Tracy (2010), the dialogue between our interpretations and participants’ reflections enhances qualitative credibility.
A limitation of the study is the composition of its sample. Our results reflect the experience of 10 White women with middle to high socioeconomic status living in an urban setting, which shaped their understandings of themselves and the world. Additionally, all participants were mothers, which may have influenced how they wanted or were able to dwell with others. Despite the homogeneity of the sample, participants were at different points in the cancer trajectory, with one not in remission according to medical criteria. We analyzed the data regardless of the time since treatment.
Conclusion
This study contributes to ongoing discussions of metaphors used by cancer patients and expands the existing literature on metaphors related to remission, diversifying and honoring the complexity of metaphors and their implications. It describes the dwelling metaphor as a central representation of the experience of living after a breast cancer diagnosis. We understood that woman who survived breast cancer were searching for a habitable world, as they tried to dwell with themselves, with others and with the world. The cancer experience changed how they were present to themselves, how they related with others and how they made sense of a world where cancer exists. Dwelling was an ongoing existential process through which they learned to be in the world in a more vulnerable way. By focusing on cancer patients’ personal metaphors, this study promotes an essential first-person perspective regarding the experience of illness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent statements
The study was approved by the ethics committee of Université du Québec à Montréal (no. 4615). Participants provide their free, informed and ongoing consent to be in the research study. All participants were informed that they had access to professional support and free resources after the interviews.
Data availability statement
Data generated during the current study are available from the corresponding author upon reasonable request.