
Abstract
Theoretical and practical guidance on how to navigate uncertainties in healthcare are scarce. Here, we draw from Gibson’s ethic of openness to explore clinicians’ experiences navigating uncertainty with individuals who experience low back pain (LBP) and provide guidance on avenues for navigating uncertainty in LBP and healthcare more broadly. Our analysis suggests that clinicians practice within different philosophical commitments when providing care for individuals with LBP, with some of them aligning with a (post)positivist approach with pre-determined endpoints and others an ethic of openness, with no fixed endpoints and consideration of multiple options and perspectives. Based on our analysis, an ethic of openness may help to surface these philosophical commitments, creating space for possibilities other than denying uncertainty and oversimplifying (evidence-based) practice. We argue that an ethic of openness may assist clinicians to navigate uncertainty in fruitful ways – embracing uncertainty, engaging in reflexivity and creativity, moving clinicians to directions that are likely to best meet the needs of patients.
Introduction
Uncertainty is inherent to, and ubiquitous in, clinical practice. Healthcare decisions rely on imperfect data, limited knowledge and unpredictable outcomes that are far from binary (Simpkin and Armstrong, 2019; Simpkin and Schwartzstein, 2016). Although the evidence-based medicine (EBM) movement was proposed in an attempt to reduce uncertainty and better inform decisions that are made in uncertain contexts (Guyatt, 1991), the approach itself aligns with the philosophical view that scientific knowledge is never complete – one can never be sure of the magnitude of all potential effects of treatments or the power of diagnostic tests (Djulbegovic et al., 2009; GRADE Working Group, 2004). EBM researchers have therefore developed a hierarchy of research evidence to help users measure the credibility and reliability of empirical findings, whereby systematic reviews and randomised controlled trials (RCTs) are considered the highest level of evidence (Djulbegovic and Guyatt, 2017; Sackett, 1989; West et al., 2002) – a reflection of ‘real’ science (Holmes et al., 2006). Such a hierarchised approach has been criticised for being reductionist, exclusionary and normative with regard to scientific knowledge, acting as an oppressive structure that overrides diverse perspectives and ways of knowing for the sake of effectiveness and convenience (Foucault, 2003; Holmes et al., 2006: 7–8). Scholars argue that those attached to the idea of ‘evidence’ maintain a Newtonian, mechanistic worldview that perceives reality as objective and absolutely independent of the observer, the observer’s intentions and observations (Holmes et al., 2006). According to them, the hierarchy and norms of EBM ‘institute a hidden political agenda through the language and technologies deployed in the name of ‘truth” (Holmes et al., 2006: 183). Such an agenda has been equally criticised for ostracising other forms of knowledge (rejecting them for being scientifically unsound) and making professional judgement vulnerable to external control and managerial agents (e.g. insurance companies; Traynor, 2009).
EBM has also been criticised for the difficulties surrounding its practical application. For instance, there is currently no practical guidance on how to provide care in the face of uncertainty or how to simultaneously attune individual circumstances while integrating ‘research evidence’ (i.e. any information generated by any type of research utilising any type of research methodology (Chartered Society of Physiotherapy, 2024), henceforth called ‘evidence’). Furthermore, the increase of evidence in health sciences has been accompanied by high levels of complexity which can, ironically, increase uncertainty (Hancock and Mattick, 2020). Yet healthcare practice continues and clearly it is less ‘evidence’ based and certain than we tend to think (Haynes and Haines, 1998); we have an in-depth understanding of fewer conditions than we presume (Ioannidis, 2005). Low back pain (LBP) is one condition that we do not comprehensively understand.
Despite the plethora of research on LBP, there has been little progress in reducing the impact of LBP on individuals and society. Many aspects of LBP are not fully understood; causes of LBP are often uncertain. For example, many people without patho-anatomical changes experience LBP (Deyo et al., 1992), while some have such changes, but do not experience pain (Brinjikji et al., 2015). Uncertainty also pervades prognosis; although many people recover, most individuals experience recurrences and flares throughout their lifetime (Dunn et al., 2013; Itz et al., 2013). While several treatments have been proposed and tested for LBP, clinical trial evidence shows that treatment effects are moderate at best (Foster et al., 2018; Keller et al., 2007). Such findings have led some to argue that the effect of a given treatment may be optimised by identifying the subgroup a person belongs to (Fersum et al., 2010), but there remains uncertainty surrounding how to do this (Saragiotto et al., 2017). In short, uncertainty pervades LBP. Yet, there is little guidance on how to navigate uncertainty in clinical practice.
This paper examines how clinicians navigate uncertainty when working with people presenting with LBP. To set the scene, we first explain uncertainty in the context of pain medicine, then position our study within the uncertainty literature, drawing attention to the lack of theoretical contribution around how to navigate uncertainty in healthcare broadly, and in the context of LBP specifically. We then elaborate on the theoretical underpinnings which informed our analysis of empirical data regarding clinician approaches to managing uncertainty, Barbara Gibson’s ‘ethic of openness’, followed by our methods and results. Overall, we argue that an ethic of openness may help clinicians to navigate uncertainty.
Background
Pain science and the practice of pain medicine present challenges both philosophically and in terms of biological complexity – both are beset with uncertainty (Cohen et al., 2022). Perhaps not surprisingly, clinical practice involving people who experience LBP, the most common musculoskeletal pain complaint (Global Burden of Disease Group, 2017), is also surrounded by uncertainty. An ethnographic study on LBP care noted that both patients and clinicians expressed uncertainty during clinical encounters (Costa et al., 2022). The authors suggest that within this context, causes of LBP, prognosis and a mismatch between imaging findings and clinical presentation underpinned patients’ and clinicians’ uncertainty. Such uncertainties were often accompanied by emotions: frustration, anger and tiredness. Clinicians often attempted to reduce uncertainty and associated emotions by neglecting complexity and providing narrow answers to questions about LBP. But denying uncertainty also appeared to undermine patients’ informed decision-making about treatments. In contrasting scenarios, where clinicians acknowledged uncertainty, they provided reassurance and logical reasoning, personalising care, shifting power, adjusting language and disclosing risks. Notably, when clinicians acknowledged uncertainty and attended to entangled emotions, a humanistic model of care unfolded, whereby patients’ perspectives about broader aspects of their lives (e.g. feeling socially isolated) were welcomed and acknowledged during clinical encounters. Based on these findings, the authors offered strategies to help clinicians navigate uncertainty: (1) disclosing uncertainty upfront and subsequently providing information about what current population-based evidence suggests; (2) making time to acknowledge and explore patients’ emotions related to uncertainty. While these suggestions offer insights onto how to adeptly navigate uncertainty in LBP, they are unlikely to be sufficient as they do not provide insights into ways in which clinicians can navigate uncertainty within themselves.
Theoretical and practical guidance on how to navigate uncertainties in healthcare are scarce. Malterud et al. (2017) argues that there is a need to develop theoretical, clinical and practical strategies for embracing uncertainty. Likewise, Simpkin and Armstrong (2019) have called for research on how to discuss and reflect on uncertainties in clinical contexts. Drawing on findings from a narrative review, Simpkin and Armstrong (2019) identified approaches for communicating uncertainty to patients: (1) assessing patient preferences for communication; (2) adopting strategies to communicate risk and ambiguity; (3) providing emotional support; and (4) clarifying contingency plans. While such strategies are valuable, they are largely limited to how clinicians can communicate uncertainty to patients. Further research should provide guidance for how clinicians can navigate uncertainty more broadly: within themselves, with other clinicians and in broader aspects of care, such as research and education. Addressing this gap is important because uncertainty is ubiquitous in LBP care (Costa et al., 2022). Clinicians deal with uncertainty when navigating patients’ personal and social contexts, making therapeutic decisions, attending to emotions and mental health, communicating education about LBP, dealing with LBP research unknowns, managing conflicting advice between professions and more (Costa et al., 2022). Therefore, moving beyond the clinician-patient dyad is critical to understanding and improving the navigation of uncertainty in healthcare broadly, and in LBP specifically.
The quest to reduce uncertainty has been central to both healthcare practice and research. For instance, patients seek care when they experience uncertainty and clinicians often intervene in clinical investigations in order to reduce uncertainty (Fox, 1980). When uncertainty remains, patients may feel prompted to continue to seek care, whereas clinicians may conduct further tests and interventions in an attempt to resolve it (Ganguli et al., 2020; Pienaar et al., 2021). As this is often counterproductive, EBM has emphasised the use of clinical guidelines and challenged clinicians to question their reliance on pathophysiological reasoning (Greenhalgh and Papoutsi, 2018). The EBM approach argues that clinicians should be able to understand the research literature while following Bayesian principles of reasoning (Ashby and Smith, 2000) in order to apply its results to everyday practice (Evidence-based Medicine Working Group, 1992). Although there is a provision in the EBM tenants outlining that context (such as patient values and preferences) is important and research should be considered in this light (Djulbegovic and Guyatt, 2017; Evidence-based Medicine Working Group, 1992), in practice, an EBM approach often controls for uncertainties through probability estimates (Ashby and Smith, 2000). Concordantly, EBM seeks to reduce uncertainty by striving for uniformity, standardisation and control: using standardised tools, methods and outcome measures to evaluate knowledge, often through RCTs (Djulbegovic and Guyatt, 2017). Yet such an approach has not successfully addressed important challenges, such as the uncertainties surrounding the mismatch between clinical findings and patient presentations, and the mismatch between the ‘patient in the guideline’ and ‘patient in the consultation room’ (Greenhalgh and Papoutsi, 2018). Said differently, EBM offers a simplification of knowledge and reality using standards, but does not provide guidance on how to handle the uncertainties and complexities of real-world situations. Engebretsen et al. (2016) argue that this search for standardisation and minimisation of uncertainty may have adverse effects, such as hindering clinicians’ abilities to relate to patients’ stories and deterring creativity, reflective questioning, openness and critical thinking. Yet, guidance on how to navigate uncertainty while averting such adverse effects remains largely underexplored.
We aim to contribute to the healthcare uncertainty literature by providing theoretical and practical guidance on how to navigate uncertainty. We draw from clinicians’ experiences navigating uncertainty with individuals who experience LBP to address the following question: How do and should we navigate uncertainty when working with people who experience LBP? Our analysis seeks to address these questions by drawing on Gibson’s ‘ethic of openness’. In attempting to counter positivist tendencies of reducing and finalising concepts (Gibson, 2016), our inquiry did not limit uncertainty to one particular definition. Such an approach aligns with our post-critical theoretical stance (see below), which posits that there is no absolute meaning of a concept but only how it is used within a particular context and what it comes to mean to those who use it (Bourdieu and Wacquant, 1992). However, we placed a focus on how clinicians navigated their own uncertainties and those of patients as a starting point for our analysis.
Theoretical underpinning
Our study is grounded in post-critical theory, which is about ‘leav[ing] room for differing alternatives’ instead of ‘closing things down’ (Felski, 2017: 4). Post-critical theory has its origins in challenges to dominant assumptions that underpin principles of Western science (Foucault, 1966: 82). As such, it stems from an onto-epistemological base in which the ‘objective’ nature of knowledge is mediated by social contexts and structures (Gibson, 2016: 5). This theory asserts that all knowledge is perspectival; we always observe from a certain viewpoint, there is never a view from nowhere (Danermark et al., 2001: 8–9). Like post-structural and critical scholars, post-critical scholars refute the objectivist epistemology that underpins (post-)positivism. They reject the assumptions of an objective, neutral, and value-free science because knowledge and what counts as legitimate ways of knowing (epistemology) result from the historical conditions that precede individuals (Danermark et al., 2001: 8–9). What makes post-critical theory distinct from earlier critical theories is its incorporation of post-structuralism’s openness, specifically its enduring commitment to exploring other possibilities.
In sharp contrast, positivism postulates that reality is value-neutral, ahistorical and cross-cultural, separate from emotional, subjective and political contexts (Packer, 2017); post-positivism is a slight variation of positivism, which claims that a certain level of objectivity rather than absolute objectivity is possible and seeks to approximate the truth rather than aspiring to grasp it in its totality (Lincoln et al., 2018). Much contemporary EBM aligns with post-positivism (Djulbegovic et al., 2009; Engebretsen et al., 2016). EBM thus considers that if one goes about in the ‘right way’ (i.e. standardised methods, measures, RCTs), one can identify reality with considerable certitude (Crotty, 1998).
In an attempt to resist the dominance of (post-)positivism that underpins EBM in rehabilitation and address its limitations, Gibson (2016: 1) proposes (re)building rehabilitation by dismantling it through an ethic of openness. While this ethic of openness is not an onto-epistemological theory, it is an approach to practice and research grounded in a post-critical stance that draws from postmodern scholars such as Gilles Deleuze and Pierre-Félix Guatarri and the work of postconventional scholar Margrit Shildrick. Specifically, it builds on Shildrick’s ethic of openness (rooted in the scholarship of Jacques Derrida, Deleuze and other postfeminist scholars), in which she proposes a sustained critique of bioethics 1 (Shildrick, 1997: 212–213). That is, moving away from bioethics about the body to an ethics of the body that creates imaginative and fluid space to question taken-for-granted parameters such as normal/abnormal, and health/illness (Gibson, 2016: 25), to critically analyse the assumptions underpinning them to open up new possibilities for practice (Shildrick, 1997: 6–7). Notably, the critique Shildrick advocates for is not destructive (Shildrick, 2005: 9). Instead, its purpose is to expose the shortcomings, unreflective assumptions and contradictions of unchallenged structures. Shildrick (2005: 3) argues that the desire to distinguish between right/wrong and good/bad remains undiminished by bioethicists in the face of a set of developments marked by their problematisation of normative, oppositional, binaries. Gibson’s work on the ethic of openness is a useful extension of this work, by providing a conceptual framework to inform analysis that can be employed to understand the multiple effects of practices (Gibson, 2016: 13). Gibson’s ethic of openness is ‘most clearly understood as an ethic of doubt’ (Gibson, 2016: 13) that offers an application to the context of rehabilitation, with relevance for LBP. While is not a grand-theory, the ethic of openness provides a methodology for identifying, analysing and addressing the ethical dimensions of physiotherapy practice, facilitating a continuous transposition of theory and practice that promotes new ways of thinking and doing (Gibson, 2016: 137).
In the book Rehabilitation: a post-critical approach, Gibson argues that an ethic of openness develops from a position of uncertainty in which there is no predetermined right way to practice and prescriptive rules for determining action (Gibson, 2016: 13). As such, an ethic of openness is an approach to practice and research that can be employed to embrace uncertainty and understand the multiple effects of practices, including those which are hidden, unintended and potentially harmful. By adopting such an approach, we may change our attitude and assumptions about clinical practice and research, offering an opportunity for (r)evolution – both uncertainty and openness are essential to avoiding stasis and moving us in creative directions that best meet the needs of the people we serve. In short, an ethic of openness may enable us to navigate uncertainty in more productive ways.
An ethic of openness is central to our analysis, enabling us to attend to care practices, such as navigating uncertainty and the principles of care. To consider how practices address or exacerbate social problems (and how) in navigating uncertainty, we adopt a post-critical approach to analysis of interviews with clinicians about uncertainty while exploring the applications and demonstrations of an ethic of openness within this context.
Methodology and methods
We took a post-critical approach to analysis. That is, we focused on uncovering what is taken for granted as true in the context of uncertainty, without necessarily rejecting these ‘truths’ and acknowledging that they are provisional and always open to revision (Gibson, 2016: 6). Such a post-critical approach enables different ways of examining common issues of clinical practice, such as uncertainty. Our approach could also be described as post-qualitative inquiry as it foregrounds the application of theoretical concepts and tools directly to data without engaging with structured qualitative epistemologies or methodologies (St. Pierre, 2021). We used Gibson’s ethics of openness to explore clinicians’ discussions of navigating uncertainty in LBP. Specifically, we ‘plugged’ the ethics of openness to our data to think with this theoretical concept and disrupt the way in which uncertainty is navigated, creating spaces for other possibilities (Jackson and Mazzei, 2013).
Participants and procedure
After gaining approval from the Human Ethics Board of The University of Queensland [2021/HE001723], we advertised the study on social media (e.g. Twitter, Arthritis Australia website and Facebook page, University Newsletter) to invite clinicians to participate in an interview. Any registered healthcare professional in Australia with experience working with people with LBP were invited to participate. Clinicians interested in participating in the study emailed the first author [NC], who replied to their email and sent them a detailed description of the study and the consent form. Clinicians who returned a signed consent form were then scheduled for an interview. Of note, our sampling strategy was mostly based on convenience, with some purposive elements as we sought participants from different disciplines, settings (e.g. primary care, tertiary care, public sector, private sector) and experience levels. Recruitment ceased when we achieved a diverse sample and our analysis indicated that there was sufficient depth to expand on our phenomenon of interest (St. Pierre, 2021): how clinicians navigate uncertainty.
Data production
Interviews were conducted between September and December 2021 via video-conferencing software (Zoom) or telephone. The interviews were conducted by three members of the research team [NC, MD, KM]: all female physiotherapists and familiar with post-critical and post-positivist research approaches. During interviews, clinicians were asked to describe scenarios in which they navigated uncertainty with people who experienced LBP, the challenges they face when trying to navigate uncertainty in this context and what they thought helped them to do so. Interviews were audio-recorded and transcribed verbatim. We assigned pseudonyms to all clinicians prior to analysis to ensure confidentiality.
Data analysis
Our interdisciplinary research team includes researchers from health sociology, psychology, public health and physiotherapy, brought together by our shared interest in understanding how clinicians navigate uncertainty. Six of us have also been clinicians and five of us have sought healthcare for LBP. The reflections that follow are influenced by our combined experiences of examining assumptions that underlie clinical practice, enacting these assumptions, conducting transformative health research and engaging with theory. Our analytic processes involved co-analysing a subset of the interview transcripts in two team analysis meetings. Our discussions were initially inductive, guided by the following questions ‘What key words did you use to describe your impressions of the transcript’; ‘What stood out to you while reading the transcripts?’ and ‘What have you learned from clinicians’ stories/experiences navigating uncertainty?’. We also discussed the transcripts in light of our collective post-critical theoretical knowledges. The analysis meetings were recorded and NC produced analytic summaries which were shared with the team.
As we reflected on the data, we interpreted that clinicians’ responses (consciously or not) aligned with certain ontological and epistemological commitments when navigating uncertainty. Said differently, when analysing how clinicians navigate uncertainty in LBP care, clinicians’ philosophical commitments were apparent. In alignment with our post-critical approach, we aimed to consider the assumptions that unpinned their approaches to navigating uncertainty to create spaces for other possibilities. Within this context, co-authors NC, RO and JS then further explored the data with the concept of the ethic of openness in mind. The final step of (re)writing the results was crucial to the analytical process and included all authors’ input.
Results
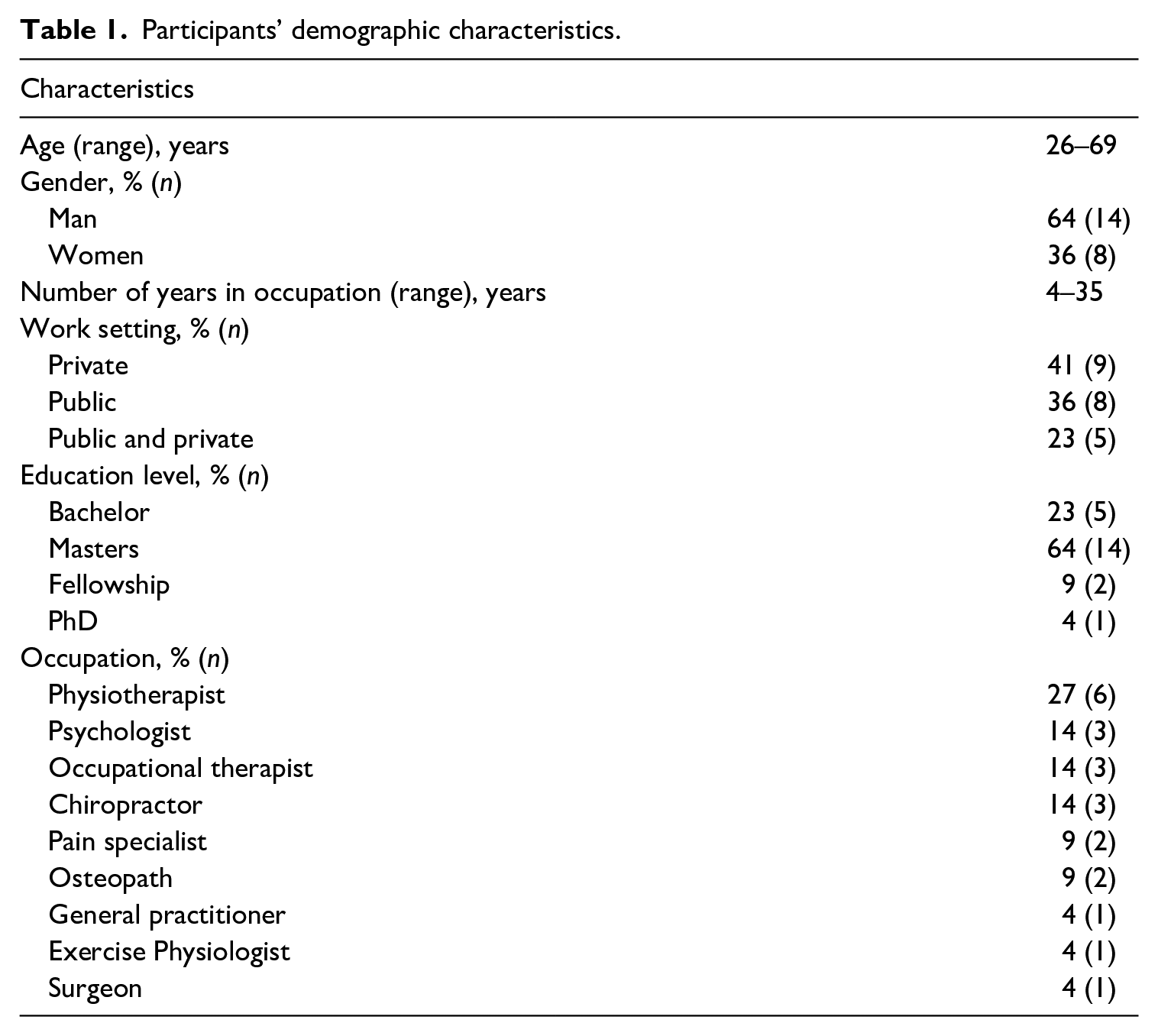
We interviewed 22 clinicians from various health disciplines, including but not limited to physiotherapists, psychologists, occupational therapists and chiropractors. They were aged between 26 and 69 years and had between four to 35 years of experience within their profession (see Table 1 for further details). Participating clinicians’ discussions of navigating uncertainty in LBP suggested that they used a variety of paradigmatic approaches to care, drawing from different philosophical commitments which impacted their patients and the care provided. The plurality of these approaches had an implicit relationship with uncertainty – with some approaches aligning with navigating uncertainty and others more suited to attempts to achieve certainty. Participants talked about paradigms, 2 frameworks, thought leaders and the way in which these were discussed usually aligned with (inadvertently or otherwise) at least two divergent understandings of reality – a (post)positivist approach, where clinicians have pre-determined notions of care and its goals; and an ethic of openness, where there is no fixed endpoint and clinicians navigate uncertainty in a way that aligns with an ethic of openness – sitting with uncertainty and considering multiple options and perspectives. We first discuss how the participants’ practices seemed to be located within different philosophical commitments, neoliberal managerialist imperatives and professional cultures; then consider how this relates to reflexive theorising (i.e. the surfacing of these philosophical commitments and dominant ideas that mediate practice). We will end by examining how and when they discussed elements that (implicitly) aligned with an ethic of openness and where these instances provided a way to navigate uncertainties in the context of LBP. Throughout, we use examples from the data and pseudonyms to maintain participants’ confidentiality.
Participants’ demographic characteristics.
Practicing within philosophical commitments, neoliberal managerialist imperatives and professional cultures when navigating LBP
Our analysis of clinicians’ discussions of their experiences navigating uncertainty identified that the way they did so was influenced by philosophical commitments, neoliberal managerialist imperatives and professional cultures. While there was no direct reference by participants to these, references to approaches to treatment, debates about treatment options and attempts to apply research presented by thought leaders to practice communicated more than the contexts in which participants experienced uncertainty – they shed light on wider factors that may hinder or support uncertainty being navigated well. For instance, Daniel points to the multiple proposals regarding how to understand and manage LBP: One of the postgraduate lectures I learned a lot from used to say that you can almost align your beliefs with a way of treating back pain, and there’s so much research available now that you can go and pick something that fits that, to be able to justify what’s happening. [Daniel - physiotherapist]
The quote above from Daniel points out that it is possible not to commit to any position but to pick and choose to interpret and explain what is going on. Such a view aligns with Gibson’s scholarship – all clinicians draw from particular philosophical commitments whether they do so consciously or not. Discussions in Daniel’s and other interviews suggest that these philosophical commitments are often aligned with (post-)positivism, with clinicians sticking to their idea of certainty to justify what is happening, based on the assumption that it is possible, or at least preferable to provide an answer that ‘fits’ [Daniel] what is happening. Likewise, others discussed the binary thinking that they felt underpinned clinicians’ views about LBP and/or treatments targeting LBP, which seemed to also draw on philosophical commitments aligned with attempting to locate certainty regarding a single answer (i.e. (post-)positivism): Unfortunately, in my opinion, physiotherapy for the most part is too stuck fighting each other within the context of ‘is manual therapy good or bad’, instead of just acknowledging that manual therapy helps calm the patient down enough that you can then actually have a rational conversation with them . . . that’s a really frustrating argument to be witnessing and be a part of. [Juan, physiotherapist]
Juan’s quote and discussion about hands-on treatment being appropriate at times indicate that common philosophical commitments underpinned by certainty and pre-determined endpoints may not be appropriate. Juan suggests that it might be more helpful to move beyond blanket rules about a treatment approach being ‘bad’ or ‘good’ for LBP. Instead, Juan creates room for consideration that touch may be helpful when considering the consultation session as a process, where some treatment approaches can help with other aspects rather than directly impacting LBP. Juan’s thinking there perhaps aligns with an ethic of openness – where the objective of an intervention can shift. Notably, Juan’s discussion of hands-on treatment can also be understood in light of its links with calls for self-management in LBP, underpinned by neoliberal managerialist imperatives that promote autonomous and resilient individuals who can shift the burden of healthcare from the state to the individual (Nicholls, 2021).
Although some clinicians expressed frustration regarding approaches that are based on single and certain answers, others openly discussed scenarios in which they adhered to what they could be certain about, such as content delivered by thought leaders in professional development courses: I’ve been to different courses, and at the end of the course, you feel so certain about exactly what’s going on and then [when I am working with patients] it’s never like that. There’s always gurus within physio that have told you this and that. Even the ones that I really believe in, like [Professor 1] and [Professor 2], they often will see low back pain patients [who have very specific conditions and are not] necessarily a good representation of the patients you see out in practice. So, it’s always coming back to you to try and putting that into practice. How is that relevant to your field practice? So yeah, I don’t I don’t feel as though, I mean, maybe those people are very certain. Obviously they do a lot of lecturing, so they seem always so certain that this is how you treat, but that’s never been my experience. I feel there’s such a broad range of people with back pain that it’s hard to be certain about everyone and I just, yeah, I, I am happy I’ve got enough knowledge that I can help people but still know that I’m lacking. There is still a lot to know in back pain. [Victoria, physiotherapist]
Here, Victoria discusses her view of well-known thought leaders who portray a single approach as ‘the’ way to treat LBP, which often sets professional cultures, expectations and dominant discourses about how physiotherapists should practice. Yet their fixed approaches (which we suggest align with post-positivist assumptions) create certainty only temporarily; when put into practice, the fixed theory does not apply to all people. This perspective situates such thought leaders as teaching set views, and thus, there is not enough variability to apply such theories to different contexts: at the individual level – there is a need to shift practice. There are significant gaps and variations between evidence and practice – research driven by reductive variables often fails to capture the multitude of informal caring mechanisms. Victoria’s statement suggests that neglecting uncertainty and assuming that all problems related to LBP will be solved by a definite (post-positivist) solution that applies to all may be unhelpful and futile. Here, it is possible that Victoria is (implicitly) arguing for a more relativist approach (there is a broad range of people with back pain) and perhaps emphasising ideas that align with an ethic of openness – challenging the knowledge and certainty of thought leaders and in this way somewhat rejecting the assumption that reality is value-neutral, acontextual and ahistorical. Said differently, thinking about LBP through a single approach, as some thought leaders suggest, can be limiting and narrow. Yet, as was common in the interviews, there remained strong elements of (post-)positivism in her talk.
Some clinicians discussed the uncertainties surrounding how to navigate care when patients have previously seen clinicians who draw from different paradigms and approaches to them. This lack of coherence across healthcare settings and disciplines seemed to impact the work that clinicians may need to (un)do: I probably find myself trying to educate people a little bit in terms of almost giving them a history lesson to try and provide some context for the reason that there is different paradigms. So, we might talk about MRI being invented in the early 70s, maybe 90s before it started to get used a little bit more. That means that if you go and see, say, an experienced GP, that they might have learned under a particular system over a period of time [. . .] And we might talk about the ways that pain science has changed over a period of decades as well. Things like [Gate Control Theory of Pain] and examples that work well for my simple brain. And I know that there’s much better explanation for it, but we’ll talk about things like. . .pain being a little bit closer to a light switch. And if we’re looking at some of the newer models of pain, there may be a little bit more to say that pain is more like a volume dial in your car and your radio, the things that might increase it over time and the things that might reduce it over time and talk about some of the basic ways that time might work under the new model, and why that explains some of the things that we didn’t understand well previously. [Daniel - physiotherapist]
Here, Daniel elaborates on how changes in the LBP literature and therapeutic approaches have shifted over time, which prompts him to give his patients a ‘history lesson’ about what was perceived as reality before versus now. Elements of this approach that Daniel puts forward align with an ethic of openness – by showing that ways of knowing are historically situated and unstable.
Daniel suggests that any treatment approach is incomplete or subject to reworking over time. Said differently, dominant knowledge changes over time. Interestingly though, he does not seem to apply the same thinking to the current paradigm – what he calls ‘newer models of pain’. He does not contest this here but says that they ‘explain some of the things we didn’t understand well previously’. Notably, most of the approaches are often underpinned by a (post-)positivist approach that seeks certainty and assumes that reality can be discovered through scientific observation and hypothetical-deductive reasoning, including the contemporary pain neuroscience he refers to at the end of this quote. Our interest is not which approach is ‘the truth’, but that there seems to be an imperative to adhere to a contemporary paradigm while dismissing previous ones without considering that two or more paradigms that may be perceived as competing and conflicting could both/all be of use. Holding ideas together seems to take us to a different point – rather than thinking of which paradigm is right, perhaps they all have rights and wrongs which vary across different contexts. Holding this tension brings in a different point of view – that what is true in one context may not be in another. Thinking in alignment with an ethic of openness, what is ‘true’ in one context is likely to be dependent on historical context, professional expectations, power issues, public expenditure, material contexts and more.
Reflexive theorising
Gibson’s ethic of openness calls for reflexive theorising – that is, the surfacing of philosophical commitments and dominant ideas that mediate practice. While some clinicians seemed to be unaware of the harmful effects that certain practices had on individuals, groups and institutions, others seemed to be aware of normative and dominant ideas that prevented uncertainty from being navigated well. In this section, we apply reflexive theorising to clinicians’ responses to expose how their practices might be helpful, harmful or both. In the following excerpt, Will reflects on the impact that the language used to communicate pain neuroscience may have on patients and clinical interactions: When we started thinking about central sensitisation, that was a tendency for people to say, “no brain, no pain”. People interpret that as “you are saying that it is in my head”. The biggest advocates of that have been [Professor 2] and [Professor 3]. Now [Professors 2 and 3], as you know, are two physiotherapists who created a pain education program but in my view, a much better response would be that pain is in your body, is in your central nervous system, but is also in your peripheral nervous system, your brain, everywhere. . .and that’s a much more holistic view. . .you know, it goes back to the concept of how “your brain responds” and we know that there is truth in that but to me that’s not a particularly useful sort of approach for the patient, it is often discussed in a clumsy way and ends up getting them nowhere. [Will, General Practitioner]
Here, Will seems to draw from his own experiences applying research findings to clinical practice to elaborate on scenarios where research findings may have unintended effects during clinical encounters, such as making patients feel dismissed or stigmatised by the idea that pain is in their head or creating counterintuitive discussions during clinical interactions. Reflecting on Will’s example while thinking with Gibson’s ethic of openness helps us to consider the multiple hidden effects of practice and potential unintended harms. While contemporary pain neuroscience may be helpful in many ways, it may also have unintended effects like the ones Will discussed. Acknowledging them helps to open other possibilities. Within this context, reflexive theorising can help to surface these philosophical commitments and what we are doing with these paradigmatic approaches. Gibson (2016) encourages clinicians and researchers to ask themselves, ‘what are you doing when you are doing what you are doing?’ (p. 137) In other words, ‘what are you doing for, with, and/or to someone and why?’ (p. 142) What people take for granted as right or true? How did they come to think this way? What are the unintended or hidden effects of current modes of thinking and acting? We have some evidence of this in this quote from Will – he seems to be aware of what he is doing, and some of its unintended effects. This type of reflection has the potential to help clinicians embrace uncertainty and analyse what they do, why they do what they do, how their practices might be helpful, harmful or both. It prompts clinicians to engage in an in-depth investigation of what they do on individuals, groups and institutions while helping them to also consider how their practices address or exacerbate problems. Our analysis of other participants provided insights into the potential unintended harm of using pain neuroscience when discussing the strategies they use to reduce uncertainty, namely excluding people from services (further explicated below): So, we use a funnel approach where people come in and they are given an overview of the service to start with. And that’s in a group environment. And what we hope is that they are listening, because there’s a very explicit slide in there that says, if you are looking for a diagnosis, if you are looking for a surgical fix, if you are still pursuing assessment and investigation, this is not for you. And it’s very clear and very explicit. And so, we try as much as possible to funnel out those people who go “Yeah, yeah, I still need to see the ortho or neurosurgeon” or whatever it is. . . . And so, the biggest challenge is trying to sell them, the central sensitization message around pain, trying to sell them pain as an output, trying to explain that the brain is, you know, overprotecting, and all of the messages that is the current understanding in chronic pain. [Ashley, psychologist]
Here, Ashley discusses a triage approach used at the pain clinic where she works which is intended to select patients according to their ‘readiness’ to stop seeking biomedical solutions so they can engage with contemporary pain neuroscience. This approach appears to aim at enabling patients to make informed choices whilst managing their expectations to avoid disappointing those who may be expecting a different approach or outcome. Ashley seems to be striving to act ethically (albeit through a narrow notion of bioethics) and to serve patients’ best interest. Yet, such a binary approach to triage may be harmful because it categorises patients in a way that creates a divide. That is, if you do not agree that this is the way of understanding pain, then you do not understand pain and the service we offer is not for you. While this approach might be underpinned by economic efficiency and managerialism of health systems and institutions and may be intended to optimise the use of resources (i.e. to prioritise patients who are more likely to engage with certain therapeutic approaches), Gibson’s ethic of openness suggests practices that rely on identifying and addressing deviation from the norm risks enabling and disabling in the same moment. For instance, the patients that are excluded by this ‘funnelling’ process are likely to be those who are socially disadvantaged, as understanding (and enacting) contemporary pain neuroscience often takes time and resources (Pate et al., 2019). Would it be ethical to exclude such groups of patients from the tertiary care services offered at pain clinics for this reason? Within this context, Gibson’s theorisation helps us to appreciate that education practices surrounding pain are imbued with ethical aspects that requires clinicians to adopt a position of continuous doubt – ‘Why are we doing this? Why this way? How does it affect people both positively and negatively? Does it need to change? How could it be done differently?’ (Gibson, 2016: 137).
Gibson’s ethics of openness offers an alternative to taking a single perspective as right or true in grappling with certainty – engaging in reflexivity, embracing uncertainty, remaining open to possibilities, changing attitudes and assumptions. Of note, Gibson does not intend for an ethics of openness to replace any other approach. An ethic of openness is a tool, not an ideology. It does not seek to prescribe a new truth, but it encourages us to remain open to creative potentials, resisting closure, categorisation and dogmatic approaches. Interestingly, the approach of openness proposed by Gibson seems to contrast with the professional training clinicians receive. When we asked clinicians what made it hard for them to navigate uncertainty within the context of LBP, participants often discussed their training. For instance, some clinicians argued that the training they received did not prepare them to navigate uncertainty or engage in reflexivity. Jackson’s excerpt offers an example: They want you to say, “Oh, it’s this condition, it will take this many weeks to fix. And we will do A, B and C. And it’s done”. And the reality is that it’s very rare that you find a patient that will go that way. So you don’t actually, you don’t actually spend a lot of time in that [uncertainty] area. . . . There is a desire to make musculoskeletal treatment certain . . . It’s really funny how people have to, we’re taught that way that it’s like, well, if it’s that test, it’s this problem. [Jackson, osteopath]
Jackson’s excerpt illustrates a common discourse in the data – training often leans on certainty. The healthcare educational system focuses on, and rewards people for, learning ‘facts’ and often equates uncertainty with failure. Using Gibson’s ethic of openness to reflect on Jackson’s statement helps to understand how the task of teaching students how to face uncertainty is just as important as teaching them how to use such tools to improve and inform treatment decisions. Gibson argues that healthcare disciplines are traditionally more concerned with discussing risks and benefits of treatment than with the task of reflecting on the hidden effects of practice and education.
In contexts where clinicians are unprepared to disclose uncertainty and patients are experiencing uncertainty themselves, clinicians’ practice may be guided by professional conventions, habituation, dominant discourses and expectations, which may be problematic if they do not reflect on the unintended consequences of their approaches and the philosophical commitments that underpin them. Will’s excerpt offers an example of how a certain framework may be used in attempts to reduce patients’ uncertainty: I think many people come to me uncertain so, that’s why they want to see a doctor. The majority of people have non-specific low back pain and then a lot of patients leave the consultation thinking “it is non-specific low back pain, there is not a lot I can do”. . . From the patient side, the uncertainty is that they don’t have any control over what is going on because they don’t understand it. So if people are given a framework, it may be that the pain is discogenic predominantly, it may be that the pain may be coming from the facet joints or maybe it is sacroiliac in nature . . . I think it is important that they have a framework that helps them to have some understanding . . . [Will, General Practitioner]
Here, Will holds a framework (pain is due to an anatomical structure) to give patients a sense of certainty in the face of uncertainty (non-specific LBP), hoping that both the certainty produced and the discourse that follows (self-management) will help patients to make progress. Our interest is not whether the pain is associated with an anatomical structural element or not, but that there seems to be a discomfort with uncertainty that prompts the clinician to settle on one way of knowing that is not open to criticism. Will seems to unreflectively rely on biomedical practice conventions and while he seems to see the positive effects of implementing his framework, he fails to acknowledge its potential unintended harms (e.g. prompting people to avoid movement in an attempt to avoid further damage). Reflecting on Will’s statement while thinking with Gibson’s ethic of openness helps us to consider the importance of engaging in reflexive theorising and being sensitive to the multiple hidden effects of practice that align with (post-)positivism and the pursuit of certainty – that is, the idea that one can identify the ‘real’ reason for the pain with objectivity and certitude. While such an approach might be problematic, it is important to acknowledge that Will likely intended to meet patients’ expectations as a way to help them to cope.
Navigating uncertainty through an ethic of openness
At times, participants seemed to align their practice with an ethic of openness – accepting ambiguity, adopting doubt, moving in new directions to accommodate patients’ emotions, reflecting on their own emotions and the effects of their practices. George, for instance, resisted the rigidity of a single philosophical commitment as the ideal approach to navigating uncertainty and instead, he confronted it: I’m holding multiple contradictory thoughts in my head. And it firstly says, trying to know which one to trust or which one to run with, and which one to discard, or, or trying to run with all of them at the same time. And not being able to just discard any of them. Is the person understanding what I’m saying? Do I talk with him? Do I explain their scan? Are we focusing on moving? Do we do hands on treatment? What’s their prognosis? What outcome measures do I use? Like seriously, like bringing up just about everything. [George, physiotherapist]
Here, George seems to align implicitly with Gibson’s ethic of openness – doubting the unassailability of the accepted truths of pain management (e.g. encouraging movement, avoiding focusing on scan findings and hands on treatment) and thinking beyond the boundaries of what many clinicians from his discipline would consider to be familiar. Although George did not explicitly question the hidden or unintended effects of his practice, nor what is considered a good outcome and why, he exhibited a commitment to openness by sitting with multiple options and uncertainties, embracing the idea that there is no predetermined right way to practice and demonstrating willingness to adapt and refine his approach. Similarly, Connor seemed to acknowledge the complexities and multiple elements of navigating uncertainty with people who experience LBP: I say “just be honest with people” but it is, is a lot is a lot broader than that, you know, it’s rapport, it’s body language, it’s tone, it’s environment, it’s light, it’s sound and smell, all in the context of a room, you know, like, comfort. And then the same thing with like listening to scholars or you know, people who have experience and evidence outside of the consultation room. And just that collation you have in your brain is happening constantly, through like the moment that person gets up out of there in the waiting room to the moment they leave, and even when they’ve left. . .you go home that night and you’re, you’re thinking about it. . . [Connor, chiropractor]
Here, both physical and non-physical aspects, both people in and outside the room, seemed to influence how Connor navigates uncertainty with his patients. Multiple paradigms (e.g. the post-positivism of evidence-based practice implied within ‘evidence outside of the consultation room’; the post-humanism of smells, light and sound), humans and non-human aspects seem to be at play in a dynamic manner, both before and after the clinical encounter. Connor’s reflections about his own practices indicate that these are not settled and instead, are open to revision. This type of thinking, which seems to align with Gibson’s ethic of openness, helps us to see how uncertainty can be navigated through constantly questioning, working and reworking again. The point is not to discard specific paradigms, but to be more aware of them and its (un)intended effects.
At times clinicians also seem to navigate uncertainty in a way that prioritises patients’ emotions and feelings: Uncertainty tends to create emotions in patients. . .so sometimes I repeat what the patient has said to me in a reformatted way. . .“If I was in your shoes, I would be feeling x”. . .or “I’m sensing you might be feeling disappointed”. So that’s, that’s how I deal with the patient’s uncertainty. [Sarah, pain specialist]
Here, Sarah discusses disclosing uncertainty and creating an opportunity to reflect on patients’ emotions with them, contextualising how these emotions may be shifting in response to it and making sense of the effects of the care she is providing with them. Likewise, some clinicians discussed how their own emotions related to uncertainty: There are benefits to the detachment. But it means that you can’t deal with something like uncertainty very well, because uncertainty undermines detachment, I think, because you, you can really only be detached from things that you either you don’t care about, or you care about but you know how they’re going to play out. If that makes sense. Otherwise, it’s hard. [Jackson, osteopath]
Jackson’s excerpt brings attention to how clinicians’ emotional responses to uncertainty may prompt them to care, with relevance for embracing an approach to working with people who experience LBP that moves beyond instrumentalism. This way of thinking concurs with Gibson’s ethic of openness – uncertainty can be used in productive ways and move us in directions that may be more likely to benefit patients.
When navigating uncertainty in a way that seems to align with an ethic of openness, some clinicians offered insights into some of the consequences that clinicians’ lack of openness to ways of knowing can have on patients: A lot of the time someone, a GP or someone tells them “your back is stuffed, you need to stop what you’re doing, or you’re going to end up in a wheelchair”. So that phrase is so commonly said. And it’s extremely, it’s criminal, really, because it’s extraordinary how psychologically destroying that statement is. [Liam – spinal surgeon]
Here, Liam discusses how clinicians themselves may have a damaging impact on one’s beliefs about their back, creating certainty about what they can/can’t do and what their future with LBP looks like. Reflecting on Liam’s statement in light of Gibson’s ethic of openness prompts us to consider that we may not necessarily reject all forms of classification employed in biomedicine and rehabilitation, but we lay them open to scrutiny. For example, the way in which clinicians assess, label and treat LBP contributes to sustaining ideas about what LBP is and how it should be dealt with. The task is then to enact ethics in a responsible way, reconciling competing variations in interpretation and identifying the implications for individual lives, with relevance for LBP care and healthcare more broadly. Using Gibson’s ethic of openness when exploring clinicians’ experiences with uncertainty helps us to consider that instead of establishing the truth or falsity of different paradigms, it might be helpful for clinicians to ask ‘what do [these paradigms] do?’ in the broadest sense possible. ‘What are the apparent/immediate effects and consequences [of these different paradigms]? [What are] the more latent or distal ones? What are the physical, psychological, social, political, cultural and existential consequences of [these paradigms when they are enacted in] teaching, research and [at] the clinic?’ (Gibson, 2016: 139). Answering such questions may avoid stasis and prompt opportunities for (r)evolution.
Taken together, the participants’ excerpts indicate that navigating uncertainty through an ethic of openness may create space for other possibilities rather than paralysing or simplifying practice. It can help to explore attitudes, assumptions and the philosophical commitments that underpin them, with relevance for surfacing the multiple effects of our practices and moving in a direction that better serves people who experience LBP.
Discussion
In this article, we draw from Gibson’s (2016) ethic of openness to offer theoretical and practical guidance for navigating uncertainty in healthcare broadly, and in LBP specifically. The insights presented here respond to calls for theoretical and empirical studies on how to navigate uncertainty in healthcare. Our analysis suggests that clinicians practice within a range of paradigms when navigating uncertainty with people who experience LBP. At times, we interpreted that their responses and ways of practicing as located within a (post-)positivist paradigm – sticking to certainty to justify what is happening, engaging in binary thinking, using pre-determined end points, leaning on thought leaders who propose ‘the’ way to treat LBP, failing to consider the unintended harms of their practices and actions that may prevent some groups from receiving care. Notably, such an approach seemed to intertwine with managerialist imperatives, practice conventions and habituation. Where they do embrace uncertainty, Gibson’s ethic of openness provides an analytical method that can be employed to challenge such stances – engaging in reflexive theorising, surfacing philosophical commitments, assumptions and the unintended and multiple effects of practices. When clinicians engaged in an ethic of openness, uncertainty seemed to be navigated in productive ways – being embraced, resisting the idea of fixed endpoints, considering a range of options and perspectives and reflecting on patients’ emotions. These findings offer a theoretical contribution to a small but growing body of research that provides guidance on avenues for navigating uncertainty more broadly in healthcare, and in LBP specifically. In this discussion, we discuss the importance of reflexive theorising and argue that an ethic of openness could be used as a tool to train clinicians in, and guide them on, navigating uncertainty in healthcare through relentless questioning and interconnectedness.
Our analysis, underpinned by Gibson’s (2016) ethic of openness, adds to scholarship on avenues for navigating uncertainty in healthcare by demonstrating the importance of surfacing clinicians’ philosophical commitments through reflexive theorising. In a field where certainty and (post-)positivism pervades, continuous questioning, surfacing assumptions, rethinking and engaging with different epistemologies can productively prompt us to identify how the way we navigate uncertainty impacts on individuals’ lives, potentially exacerbating social problems. While clinicians may not intentionally or consciously align their practice with (post-)positivism, the failure to consider the philosophical commitments – alongside historical and political factors – has likely impacted clinical practice, the care individuals receive and research alike (Braun and Clarke, 2024; St. Pierre, 2012). Our findings offer several examples that provide insights into why reflexive theorising (i.e. the surfacing of philosophical commitments) matters. For instance, Will discussed the impact the language used to communicate pain neuroscience can have on patients (e.g. feeling dismissed) and clinical interactions (e.g. counterintuitive discussions). Likewise, Ashley’s discussion about the ‘funnel’ approach used to select patients based on their ‘readiness’ to accept neuroscience-based pain education prompts us to consider its potential harms. While there is little doubt that neuroscience-based pain education can be helpful (Wood and Hendrick, 2019), it is important to note that it can also be problematic – or may detract from other important elements of providing ethical care – particularly when its merits are assumed to be obvious and its shortcomings are overlooked. Interestingly, some have discussed how neuroscience-based discourses reflect the language and practices of neoliberalism: shifting the attention from social problems to individual responsibility and self-regulation (Pitts-Taylor, 2010). Perhaps not surprisingly, people living with persistent pain have expressed negative attitudes towards neuroscience-based educational information (Weisman et al., 2022). Weisman et al. (2022) argue that although much of this information is claimed to be ‘truth’, they are opinions that draw from certain philosophical stances (i.e. dualism, neuroessentialism and homuncular views), with relevance to our argument that clinicians’ philosophical commitments require attention. Likewise, researchers may also benefit from both reflexive theorising and engagement with research paradigms other that (post-)positivism in RCTs and reviews. For instance, aligning quantitative research with critical theory may help to develop more equitable and inclusive research and practices alike (Fortuna et al., 2022; Slade et al., 2023). A pluralist approach to research, that is, consideration of multiple paradigms, may help us to see problems from multiple angles, fostering transformative scholarship (Laliberte Rudman, 2014).
With much of the literature focused on (post-)positivist RCTs, systematic reviews and meta-analyses, and little examination of how to address uncertainty and real-world messiness (e.g. differences in values and priorities of different stakeholders, vested interests, social and economic circumstances (Costa et al., 2024)), our analysis offers important insights into the role of an ethic of openness within the context of evidence-based pain science and practice. First, it suggests that uncertainty is a necessary stance that pushes clinicians to remain open to other possibilities rather than to paralyse or ossify their practices based on what the evidence suggests. Thus, clinicians may benefit from moving beyond binary thinking (e.g. ‘good’ or ‘bad’) to adopt a position of uncertainty through reflexive theorising – why do we do what we do? how does this affect people both positively and negatively? what are the unintended or hidden effects of current modes of thinking and acting? Such considerations are important because although findings from well-designed RCTs and reviews can offer great insights, these findings may be useless in facing a patient in the here and now (Wieringa et al., 2017). Within this context, reflexive theorising and an ethic of openness may prompt clinicians to develop competence in providing individualised care attuned to a patient’s circumstances. Ongoing critical review of the new evidence and constructively doubting of one’s decision (i.e. practicing with humility) are important aspects of being a clinician – uncertainty is not necessarily a threat to practice effectively (Papadimitriou et al., 2022).
Second, our analysis draws attention to the ethic of openness’ potential in assisting clinicians to navigate uncertainty without the adverse effects – such as reducing creativity and critical thinking – of standardisation and minimisation of uncertainty embedded in EBM (Engebretsen et al., 2016). To be clear, we are not arguing for a return of anecdotal evidence or the clerical authority of doctors. As Gibson argues, an ethic of openness does not intend to be an ideology or to prescribe a new truth. Rather, we suggest that an ethic of openness could be used as an analytical method to embrace uncertainty within the context of EBM and help clinicians to understand the multiple effects of their practices, including those which are hidden, unintended and potentially harmful. This is particularly important because, as Connor and other participants suggested, clinical practice may be informed by aspects other than the evidence. Ethnographic work by Gabbay and le May (2004) has shown that most clinical decisions rely on tacit and hard-to-explain knowledge influenced by past experiences, peers and contexts. Such findings support our call to enact an ethic of openness and surface clinicians’ assumptions and positionality.
Pain practice and healthcare are not simply a matter of making rational choices based on evidence. As Annemarie Mol suggests, the logic of care requires tinkering – taking care while an uncertain future unfolds (Mol, 2008: 12). Uncertainty is ubiquitous in LBP care and not limited to clinical aspects such as treatment effects and education about LBP (Costa et al., 2023). Clinicians also navigate human uncertainties related to personal, emotional, psychological, social, cultural and moral aspects. We argue that theoretical guidance on how to navigate uncertainty through an ethic of openness may guide intersections between mainstream science and human uncertainties. Likewise, it may prompt clinicians to attend to elements that generally receive less attention in healthcare (Mescouto et al., 2022).
As clinicians, researchers and lifelong learners, we need to develop capability and capacity to handle uncertainties: the unknown, the unpredictable and the emergent (Fraser and Greenhalgh, 2001). In alignment with previous research (Forbes and Toloui-Wallace, 2022; Gheihman et al., 2020), our analysis suggests that clinicians’ training may not adequately prepare them to navigate uncertainty or engage in reflexivity. In light of such findings, we argue that both pre-professional and experienced clinicians may benefit from training opportunities that prompt them to engage in reflexive theorising and provide them with opportunity for practice-based learning that fosters technical skills and understanding of how these skills align with values and assumptions (Billett, 2015).
Conclusion
This study draws from empirical data and offers theoretical guidance on potential avenues for navigating uncertainty in healthcare broadly, and LBP specifically. Using Gibson’s ethic of openness as a theoretical and methodological driver, we argue that uncertainty is a necessary stance that can surface clinicians’ philosophical commitments and multiple effects of their (evidence-based) practices. Embracing uncertainty through an ethic of openness is likely to move clinicians to creative, reflexive and ethical directions that are likely to best meet the needs of the patients they serve. The theorical contribution drawn from our analysis may be of interest to clinicians and researchers seeking to navigate uncertainty in fruitful ways.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: NC is supported by The University of Queensland (University of Queensland Stimulus Fellowship). JS is supported by the National Health and Medical Research of Australia (NHMRC: APP1157199).