
Abstract
This article explores healthcare professionals’ experiences of their work with patient communication in standardised cancer patient pathways (CPPs). The theoretical and methodological framework for this study is institutional ethnography. Data were collected through semi-structured interviews with 72 healthcare professionals, including general practitioners, specialist physicians and other hospital staff, in five Norwegian hospitals. The study reveals four aspects of communication work that illuminate how the CPP policy mediates the way healthcare professionals interact with patients through communicating continuity, communicating (by dodging) the dreaded C-word, communicating patient participation, and communicating the relevance of time. Healthcare professionals’ balancing of their different experiential realities run as a common thread through the four aspects of communication work identified in this study. The CPP policy, with its explicit focus on transparency, speed, and time frames creates challenges in an already delicate situation.
Keywords
Introduction
Providing high quality care is directed towards continually improving healthcare within the multiple, seemingly contradictory, ideals that shape the notion of what healthcare actually is (Grol et al., 2008). A prominent trend clusters around the discourse of patient-centred care, and the relationship between patients and their care providers. ‘Patient-centred care’ is rooted in a holistic approach to care that focuses on the interplay between biological, psychological and social factors that contribute to health conditions (Mead and Bower, 2000). It is a broad term that signals a philosophy of care that caters to the unique needs and wishes of the individual patient (Fix et al., 2018). Healthcare professionals are, to an increasing extent, expected to build a partner-like relationship with their patients (Beedholm and Frederiksen, 2019). A crucial part of this relational work concerns communication. Caregivers are expected to provide adequate information about all aspects of the condition, encourage patient participation and choice in decisions about their care, and be attentive and considerate of the subjective perspectives and experiences of the patient (Mazor et al., 2013; Mead and Bower, 2000).
A potentially conflicting trend involves different forms of bureaucratic control and guidelines that regulate clinical practice (Timmermans, 2005). Clinical practice guidelines and care pathways represent two types of guideline that target distinct aspects of care. Clinical practice guidelines emanate from the discourse of evidence-based medicine (EBM) and provide diagnostic and treatment recommendations based on best-available scientific evidence (Kredo et al., 2016). Care pathways function as an extension of clinical practice guidelines and concern the logistics, that is, ‘the sequence, timing and provision of interventions’ (Kredo et al., 2016: 123). As care pathways aim to promote standardised and efficient care, they may pose a challenge in achieving patient-centred communication. This makes care pathways worthy of study. In this article, as part of a larger study, I explore how healthcare professionals experience their work with patient communication in the context of standardised cancer patient pathways (CPPs). My study is guided by institutional ethnography. I aim to trace aspects of the social organisation that mediate this work, with the primary emphasis on how the CPPs – as ruling text – inform the way healthcare professionals communicate with patients.
Cancer patient pathways in Norway
The Norwegian health authorities introduced CPP as a national cancer policy in 2015. The policy targets the logistics and organisation of cancer care services. Currently, there are 28 pathways for different cancer diagnoses. The policy is anchored in clinical practice guidelines but address the timeliness of care by establishing maximum time frames for the diagnostic process, that is, from the moment the hospital receives a referral to the starting point of treatment (Figure 1). These time frames are monitored through a coding system and published on a national webpage. This policy places time as a core quality indicator in cancer care (Norwegian Directorate of Health, 2016a).
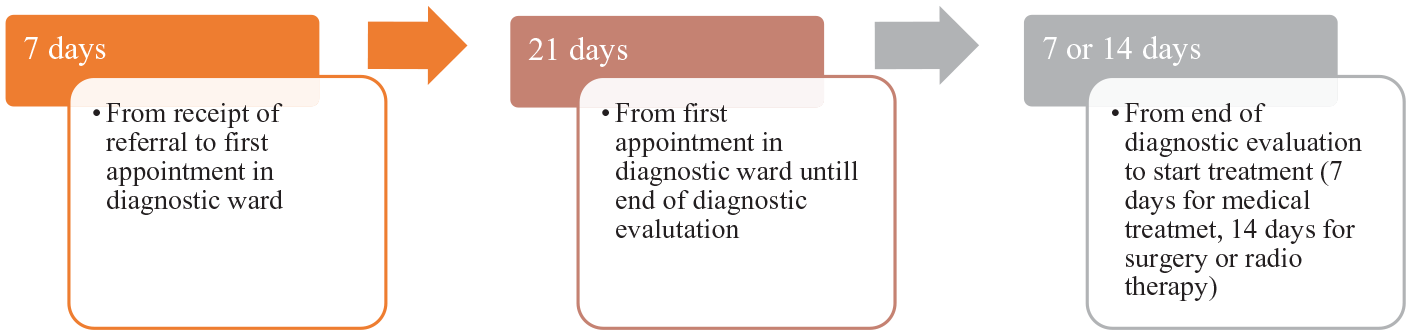
Example of CPP time frames for lung cancer (Norwegian Directorate of Health, 2016b).
A new position entitled ‘cancer pathway coordinator’, occupied by nurses or secretaries, was created following the introduction of CPPs. I refer to this group of professionals strictly as ‘coordinators’. The coordinators are responsible for making appointments to diagnostic testing and/or treatment, informing patients about their appointments and monitoring and perform the coding work of the CPP timeframes (Håland and Melby, 2021).
Most CPPs are initiated through a referral letter from a general practitioner (GP) to the hospital requesting a diagnostic assessment. Within the hospital, coordinators, nurses and specialist physicians (such as clinicians, radiologists, nuclear radiologists, surgeons, pathologists) must cooperate to ensure smooth and timely transitions between the various departments within and across hospitals (Næss, 2021). The diagnostic process culminates in a multidisciplinary team (MDT) meeting where the staff involved meet to discuss diagnosis and treatment alternatives (Næss and Håland, 2021).
The CPP documents also emphasise the principles of patient-centred care by declaring that all patients shall be provided with an individualised care trajectory that considers the patient’s wants, needs, and individual situation. As such, information, communication, and dialogue are defined as an important part of the CPPs. Håland and Melby (2017) outline how the CPP policy builds on the two opposing discourses of standardisation and individualisation. Standardisation refers to processes that organise practice towards greater efficiency, predictability and equality in treating patients, with specific guidelines dictating how things should be done and in what order. Individualisation refers to processes found in the patient-centred approach, such as patient participation, shared decision-making and personalised treatment modalities (Håland and Melby, 2017).
Thus, healthcare professionals must accommodate what may seem like the best of two distinct worlds. How to achieve this is not, however, neatly packaged and delivered in a straightforward procedure. It requires a delicate balance of discretionary judgement. As Timmermans and Epstein (2010: 84) warn, there is a great chance that ‘one person’s much needed standard causes another person’s suffering’. This underscores the importance of placing good communication at the heart of the clinical encounter. It is the key to establishing mutual understanding and ascertaining the needs and desires of individual patients (Ha et al., 2010; King and Hoppe, 2013).
Patient-centred communication
A large body of research attests to the relevance of communication in the clinical encounter for patients’ health and well-being (Arora, 2003; King and Hoppe, 2013; Ong et al., 2000). Studies indicate that patient-centred communication positively influences the quality of care across a variety of dimensions, including increased patient satisfaction, adherence to treatment and improvements in both physical and psychosocial aspects of health (Groves, 2010; Mazor et al., 2013; Street et al., 2009). Patient-centred communication is a powerful medium because of its multidimensional potential to influence the patient’s experience. It is communication that aims to nurture the relationships between patients and their professional caretakers; understand the patient’s perspective, needs, and social context; balance emotions and insecurities; make medical information understandable; and that empowers the patient to participate in important decisions about their care (Ha et al., 2010; McCormack et al., 2011).
It could be argued that patient-centred communication is particularly relevant in the context of cancer care due to the often serious and disruptive nature of cancer diagnoses (Arora, 2003; Hansen et al., 2018; Markides, 2011). It is also an aspect of healthcare where inadequate communication is regarded as a widespread problem (Thorne et al., 2005). As Fagerlind et al. (2008) note, a lack of continuity, due to the many different healthcare professionals involved, is a barrier to successful communication, and patients in general desire more information and more psychosocial and emotional support than they receive.
Much is written about the difficulties that the medical profession has with transparency and truth-telling in disclosing ‘sad, bad and difficult news’ (Fallowfield and Jenkins, 2004: 312). Although there is a move towards greater transparency in medical practice, physicians may still opt to conceal information from patients about cancer diagnoses and prognoses (Panagopoulou et al., 2008; Sarafis et al., 2014). De Giorgi et al. (2008) assert that many physicians have limited training in talking to patients about difficult topics, such as cancer, and that there are many reasons why certain information is concealed; the patient may not be receptive, or physicians may try to protect patients from psychological distress. However, physicians may also conceal negative information to protect themselves from the emotional distress associated with having to deliver bad news.
Disclosure of information is at the heart of the ideology that promotes patient participation and a more even distribution of power between patients and medical professionals. Notions of patient participation draw on a variety of discourses related to patient autonomy (Quill and Brody, 1996), empowerment (Schneider-Kamp and Askegaard, 2020), consumerism and citizenship (McDonald et al., 2007). In short, these discourses promote the patient’s rights, freedom and competence to be actively involved in all aspects of their care – the actualisation of which hinges on truthful and transparent disclosure of information (Zolkefli, 2018).
Although it is widely accepted that participation is beneficial for patients, empirical evidence suggests that there is a gap between the ideal of participation and the reality of actual practice (Angel and Frederiksen, 2015). In a literature review of health professionals’ perceptions of shared decision-making, Gravel et al. (2006: para 13) identify multiple factors that can present as barriers to patient participation. These range from attitudes and characteristics of both professionals and patients to structural factors, such as ‘time constraints’ and ‘lack of applicability to the clinical situation’. Solbjør and Steinsbekk (2011: e148) find that although many healthcare professionals value patients’ perspectives and knowledge, they value their own professional knowledge more, ‘thereby maintaining the hierarchical relation’. Hsieh et al. (2016) demonstrate how physicians use patient-centred language and perspectives to control patients’ preferences and needs. Notably, studies examining patients’ preferences for participation in cancer care paint a complex picture of wide variation in patients’ desired levels of participation (Gattellari et al., 2001; Keating et al., 2010; Sinding et al., 2010; Thorne et al., 2013).
Theory and methods
The findings of this article are based on data from qualitative interviews with healthcare professionals working in both primary and specialist care. The study is part of a larger research project evaluating the experience of introducing CPPs from the perspectives of patients and healthcare professionals. The Research Council of Norway and NTNU funded the project (project number 272665). In this article, I explore the experiences of healthcare professionals’ work with patient communication in CPPs. The theoretical and methodological framework guiding my contribution to the project is institutional ethnography.
Institutional ethnography (IE)
Sociologist Dorothy Smith developed IE as a methodological approach to uncover the workings of social reality (Smith, 1999, 2005). IE is based in an ontology that locates the existence of the social in the ongoing orchestration of people’s everyday activities. A key premise is that people’s activities and interactions are embedded in what Smith (2005) calls the ‘ruling relations’. Ruling relations refers to the textually-coordinated interconnectedness of human activity as it happens across time and place. Ruling relations, thus, have a translocal nature. The goal of IE is to discover how different ruling relations shape people’s everyday activities. The path to discovery begins in someone’s everyday experience: a standpoint. Starting in experience establishes a viewpoint from which it is possible to find traces of the ruling relations that shape (some aspects of) people’s lives. Further, the researcher can follow these traces into sites beyond the location of the standpoint informants to illuminate how people’s activities in a setting happen the way they do (Smith, 2006b).
Since my study was carried out as part of a larger project, I modified the use of IE to accommodate my research context. This means that IE guided the analysis of the interview material to a greater extent than the data collection process. I had a specific text-based form of ruling (CPPs) as a premeditated focus for the study. I chose to begin the analysis within the experience of physicians. Because physicians in this study represent a diverse group of medical professionals, they work in different locations across the institutional setting.
To enhance the understanding of the work involved in patient communication beyond the standpoint informants’ experience (Campbell and Gregor, 2004), I included interviews with nurses, cancer pathway coordinators and administrative staff. Surely qualitative interviews do not directly access work processes as they happen in real life but provide insight into people’s accounts, perspectives and experiences of their work. Although many IE studies triangulate methods and include observational data, it is possible to only use interviews (DeVault and McCoy, 2006). Smith (2005) explicitly emphasises that interviews are crucial to access lived experience.
Data collection and analysis
The article draws on semi-structured qualitative interviews, conducted from May 2018 to January 2020, with a total of 72 healthcare professionals. Ethical approval was obtained from the Norwegian Center for Research Data (Project number 58724). The research group interviewed multiple healthcare professionals working in different hospital departments across five geographical regions. This is consistent with IE’s focus on interconnected work processes (DeVault and McCoy, 2006). We concentrated our study on four CPPs: lung, prostate, breast and malignant melanoma. Breast, prostate and lung cancer were chosen because they are among the most common cancers, which provided access to informants with much experience with CPP for these patient groups. Malignant melanoma is less prevalent, but incidents are rising. This CPP was chosen because the hospitals in Norway had made less effort to achieve an integrated organisation of this diagnosis before the introduction of the CPPs. Informants were recruited using a combination of purposive and snowball sampling (MacDougall and Fudge, 2001). We ensured that all potential informants received both written and verbal information about the study, and those who agreed to participate signed a consent form.
The sample consisted of 12 GPs and 60 hospital staff working across five hospitals in Norway, both local and university hospitals. It included 27 specialist physicians (clinicians, surgeons, radiologists, nuclear radiologists, pathologists and administrative managers) as well as 11 nurses, 14 cancer pathway coordinators and eight administrative managers. The research team conducted 57 individual interviews with hospital staff, whereas three interviews were conducted with two informants at the same time. Four of the interviews with GPs were conducted as group interviews, whereas one GP was interviewed individually. The author conducted three group interviews, one dyadic interview and 21 individual interviews alone or with a research team member, while other research team members conducted the other interviews. All interviews were recorded, transcribed verbatim and anonymised.
IE researchers work with their data in diverse ways with a common aim to illuminate how everyday experience is shaped within translocal relations (Campbell and Gregor, 2004; Smith, 2006a). In the analysis of the interview material, I sought to identify how the informants’ work processes were shaped by ruling relations and discourses. Discourses are part of the ruling relations and, in short, refer to contextually-regulated collective understandings and practices. I used IE’s concept of ‘problematic’ as a key analytical tool. A problematic is often based on the identification of junctures or tensions – between what is actually done and translocal relations – that the researcher finds valuable to explore (Smith, 2005).
After identifying patient communication as an important aspect to explore, data were further analysed by extracting all reports (including those from other health professionals) that were relevant to patient communication under the heading: communication work. I used Smith’s (2005) ‘generous’ notion of work, which includes all forms of activity that take time and effort. This means that thoughts, feelings and talk, on a par with concrete actions, can also be defined as ‘work’. Statements were sorted by indexing different types of communication work and small problematics that were found in the data (source). Importantly, the analytical process proceeded in an interplay between reading, writing, reading and rewriting, looking for traces of ruling relations (Campbell and Gregor, 2004; DeVault and McCoy, 2006).
Communication work: A balancing act
I have named the overarching problematic ‘communication work: a balancing act between biomedical, psychosocial and political realities’. This is meant to capture the tension between different forms of knowledge that come into play while healthcare professionals work to establish good communication with patients in a system that is designed to move as quickly as possible. The problematic is informed by four themes pointing to different aspects of communication work in standardised care pathways: (1) communicating to ensure continuity; (2) communicating (by dodging) the dreaded C-word; (3) communicating patient participation; and (4) communicating the relevance of time. Each are discussed in turn.
Communicating continuity
A central aim of the CPP policy is to ensure continuity and predictability in the diagnostic process (Norwegian Directorate of Health, 2016a). Consistently, the informants in this study emphasise that providing information to the patient about what, how, why, and when things will happen is more important for continuity than fixed time frames. A shared experience among informants is that the CPPs has made it ‘easier’ to communicate in a more consistent manner, as healthcare professionals working in different locations are more tuned into each other’s work processes. As one physician states: It is easier to get the patient through. . . and. . . we think more alike, many of us in the organisation, it is easier to cooperate between departments because we agree that this is how we do things, with the patients. . . (Physician 13, hospital 1)
This suggests that healthcare professionals’ engagement with the CPPs synchronises their activities across locations (Smith, 2005). The interviews reveal that the work of communicating continuity relies on both consistent interdisciplinary interaction and a clear distribution of communicative responsibilities between healthcare personnel. Coordinators and nurses are responsible for conveying logistical and practical information about time, place and the preparation for examinations, while physicians deliver information of a medical/technical nature (e.g., diagnosis and treatment).
Nurses state that they work to create continuity by being present with the patient in consultations with the physicians, and by talking with the coordinators (and physicians) about what is needed, what has been said, what is being planned and when. After the medical consultation, the nurses continue the dialogue with the patient to provide detailed information about the events to follow. Thus, nurses ensure continuity across both practical and medical information and events. They also stress the importance of a compassion-based approach. This includes taking the time to listen and map out the patients’ personal situation and provide a phone number that the patient can call if they need to talk outside of the scheduled appointments. One nurse describes communicating continuity as a process: We give them everything we have of forms, give them the brochures, we have a book where we write down what they have received of information, how they reacted, what their family situation is, if they have a job, and then we call them the Tuesday after they received the diagnosis just to check in with how they’re doing and how they’re feeling because then it [the diagnosis] is a bit more processed. . .because the day they receive the diagnosis, I mean, it is so much [to take in] that they shut down and just want to go home. (Nurse 55, hospital 3)
As noted above, continuity in communication is a method to monitor the patient’s emotional and psychological well-being in connection with the processing of information. Nurses make sure patients receive information they can digest over time by providing them with written information, such as brochures, about the disease and upcoming treatment, and routinely call patients to check how they are doing. A vital aspect of nurses’ continuity work involves communicating their availability. As one nurse puts it: I tell them [patients] that if there is anything they want to talk about, they can call us. (Nurse 18, hospital 1)
This reveals a more nuanced approach to the temporal dimension of continuity than time frames. As cancer is often a distressing life-changing event (Mazor et al., 2013), repeated communication over time in accordance with the processing of each patient’s care is crucial to the patient’s well-being. However, physicians comment that their schedule is so tightly organised that they simply do not have time to engage with patients outside the confines of scheduled appointments. One physician explains: I have to deal with the patients that are here, in the hospital, I can’t sit half a day talking [on the phone] with patients that are not inside the hospital, although I do understand that they [patients] want that, and their GP wants that because they don’t have the details, this is advanced stuff, but. . .then the hospital needs to organise it. . .. (Physician 48, hospital 2)
This implies that, for physicians, the demand for medical expertise take precedence over the psychological and emotional well-being of patients. Physicians must rely on other healthcare personnel (such as nurses and coordinators) to create continuity through communication by filling in the gaps in patient–physician interactions. However, nurses and coordinators report that continuity sometimes breaks down due to a lack of communication from physicians. As one nurse remarks: It is unfortunate [. . .] I call the patient and say, “you have an appointment in two days” and the patient questions why. “Do I have cancer now?” And it is not my job to inform about that, the doctor should have informed the patient and said, “you have a serious diagnosis and you will receive an appointment with the oncologist”. (Nurse 72, hospital 5)
In the situation depicted above, the patient’s cancer diagnosis has been identified and the referral for medical treatment has been generated without first informing the patient. This is a breach of the CPP guidelines’ emphasis on patient involvement in decision-making (Norwegian Directorate of Health, 2016a), which puts the nurse in a difficult situation when calling to inform about the upcoming appointment. It is not part of a nurse’s job description to disclose a diagnosis. Other informants report similar experiences along the pathways. For example, coordinators mention that they frequently encounter patients who do not know that they have been referred for diagnostic assessment. Informants argue that this is an area in need of improvement; to further enhance continuity, physicians must consistently make sure that their patients are informed before sending the referral. It is also desirable that they relay (to other healthcare personnel) what kind of information has been disclosed to the patient.
Communicating (by dodging) the dreaded C-word
Before the CPPs were introduced, then you would say to the patient that “we found something that we need to figure out”, right, “we are not quite sure what it is. . .” right, but once you’ve said the C-word. . .. (Physician 17, hospital 1)
The quote above suggests that there is something about the CPPs’ reference to the word cancer that triggers a change in the communication with patients. This is tied to the CPPs guideline stating that patients shall be informed about being referred to a CPP (Norwegian Directorate of Health, 2016a). When informants discuss the relevance of providing patients with information about CPPs, the dilemma of truth-telling in medical practice come into play (Buckman, 1996; Zolkefli, 2018). As one coordinator says it: There are a lot of patients, and I think there are many that still don’t know that there is this thing called CPP and that there is a coordinator who is there and that can help them if they have any questions (Coordinator 58, hospital, 3)
With few exceptions, informants across all professions express the view that information about CPPs is not a priority when communicating with patients. The interviews indicate that there is a lack of clarity regarding who is responsible for informing patients about CPPs. Hospital staff argue that it is the GP’s task to inform patients about the CPPs upon referral to the hospital, thus hospital staff assume that if patients know about CPPs it is because they have been informed by their GPs.
Talking about the CPPs with patients is described as challenging because it contains the word cancer, which anticipates a diagnosis. Informants state that there is a pervasive fear associated with cancer in society that triggers a distress on the part of both themselves and their patients. GP 3 illustrates this when he says that: ‘cancer is a demanding field to be in because ‘cancer, or cancerphobia, it’s like a ghost, constantly haunting patients, and society. . . so it is a demanding field to be in’. The GPs underscore that being referred to a CPP can be a frightening experience for many patients, and they do not want the patient to leave their office more afraid than they were on entering. Because there is so much fear associated with cancer, information must be tailored to fit the psychological make-up of each patient, as people have different thresholds for what they can manage. One GP elaborates: I guess it depends on the patient, if I know that this is a frail leaf, she’ll fall to the ground if I use the word cancer, then I don’t, but I use the word pathway and explain that within this number of days, you are supposed to be scheduled for a conversation and examination [at the hospital] and a plan will be made. And I do say that I can’t rule out cancer, or I say that unfortunately I suspect that it could be something serious. (GP 7)
The GP above describes a strategy, shared by other GPs, of excluding the word ‘cancer’ in favour of the word ‘pathway’ when managing uncertainties about the patient’s symptoms or what information is appropriate in the specific situation. However, some GPs did state that they are more open with patients when they suspect cancer. One GP outlines her tactic when referring patients to a CPP in the following manner: [. . .] Now in many places in Norway, you can read the referral that your doctor has written about you when you log on [to a digital health platform], so you must be very cautious about what you write so you don’t increase the [patient’s] worrying. Therefore, before it was easy to be misunderstood, because you’re kind of trying to wrap it in, but it still could be cancer, and you don’t want to write the word cancer. . . so now I’ve kind of just checked off for CPP [a check-box in the referral document], written cancer in the text and told the patient “don’t freak out if you get a letter saying cancer patient pathways because that is a trick we use to get you in fast, and you do want to know if this is something or not, fast, right?” And they just say, “yes I would like that”. (GP 1)
Thus, CPPs seem to create a dilemma in relation to truth disclosure in the patient–physician communication, precisely because of the need to introduce the word ‘cancer’ somewhat prematurely. This problem did not exist before (at least not to the same extent), as GPs could communicate in more obscure language and bypass a (longer) discussion about the likelihood of a cancer diagnosis. Strikingly, most hospital staff agreed that it is not particularly relevant to inform patients about CPPs. What matters is that they do the actual work involved in fulfilling the CPP guidelines. Below, two specialist physicians reflect over whether it is important that patients know that they are part of a CPP: No, I really don’t know, I’ve rarely mentioned it as a part of this, of patients’ cancer treatment. I think, I believe people have enough to deal with, the fact that there is cancer discovered and it is not important that it is entitled Cancer Patient Pathways. (Physician 49, hospital 3) It [information about CPPs] will probably lead to some patients becoming more demanding about when they should receive treatment. So, you could say that the consequence of us providing this information would be that they [patients] point out when time frames are breached. (Physician 47, hospital 3)
In these accounts, two distinct discourses shape how information is concealed from patients. In the first quote, the reasoning is framed as consideration for the patient’s well-being, that is, not overloading the patients with redundant information. In the second quote, the physician considers the consequences for his own professional autonomy, which raises the question: does a more informed patient lead to a more demanding patient? This is connected to the discourse about patient’s rights and power to interfere with a physician’s work. Consistent with Hsieh et al. (2016), these statements illustrate that, by carefully selecting what information they share with their patients, physicians’ can subdue patients via coded communication.
Communicating patient participation
Most informants talk about patient participation solely in conjunction with treatment decisions, that is, after the diagnosis is established. One physician, in recalling a recurring dialogue in the MDT meetings with physicians from a neighbouring hospital, describes how patient participation is diversely valued and practiced: Well, I mean [the staff at] [name of hospital] are very concerned about that, because they always say, “but what does the patient want?” Now patients are supposed to co-decide, and then we’re at a loss for an answer. . . “patients, they do what we say”, “yes, ok, but you must ask the patient, are they willing to undergo surgery? [. . .]” So, I think the [name of hospital] are trying to train those who refer patients [for treatment] that they have to engage in that conversation with their patients prior to [referral]. (Physician 34, hospital 2)
The statement reveals the collision of two opposing discourses: the paternalistic approach referring to the patient as passive and compliant, and the patient-centred approach encouraging active participation (Sandman and Munthe, 2010). It demonstrates the translocal relational nature of textual modes of ruling (Smith, 2005). When guidelines for patient participation are activated by certain individuals in specific settings, as in this case where the physician in the other hospital consistently reject referrals before the patient has been thoroughly consulted, practices begin to coalesce in a new direction.
How then do physicians practice patient participation? What does that entail in cancer care? The physicians in this study, echoing findings from other studies about patients’ preferences (Gattellari et al., 2001; Keating et al., 2010; Sinding et al., 2010; Thorne et al., 2013), express that patients are so diverse that they range from hardly wanting any information or participation, to scrutinising the internet and wishing to explore every possible avenue before deciding. Physicians highlight the fact that patient participation in cancer care is complicated; not only do the available alternatives differ between cancer types and the cancer characteristics, they also rely heavily on patient factors (e.g., age, comorbidity, overall physical and mental condition, life situation and patient initiative). Here is an excerpt from an interview with a physician speaking about her work with patient participation:
It is probably different from physician to physician. They could, you’d say that this [cancer] could be treated in different ways, and then it is. . . if they can have surgery that is the gold standard, and you have to sort of convey that, but if they [patients] are weak or something like that, you’d sort of say ‘in your case I think it is appropriate to. . . the best treatment for you is radiation therapy’. And, it is probably silly to be talking too much about surgery if you know that they could barely handle it, but you do tell [patients] that there are different roads leading to Rome; you try to say that.
Yeah, how does the patient deal with that? I mean, do they ask, want to know as much as possible?
It’s a bit up and down. Yes, a bit up and down.
Yeah, have they searched online, are they very. . .?
Yes, younger patients often search online. They’ve been searching and have learned about different types [of cancer] and ask about that and stuff, yes, but the older [patients] they don’t have as much. . . they listen more closely to the doctor; it is a different school.
Yes, but do they have what they need to. . . kind of, is there really anything to co-decide in?
Well, you could say that, yeah, that you are on the border, kind of, you have a lot of illnesses, we cannot guarantee that you can tolerate surgery very well, it will set you back, maybe it would be better for you to do. . . and then they just have to make a decision on the basis of what we say. And some ask, ‘what would you do?’ So, they are supposed to [co-decide], but you can’t give them so much co-determination that they end up regretting the choice they made. (Physician 30, hospital 2)
This excerpt illustrates how the work of incorporating the principle of patient participation is tailored to the unique situation of each patient. It reveals an inherent tension between professional responsibility and the ideal of patient autonomy, which can be bent accordingly (Hsieh et al., 2016; Sandman and Munthe, 2010). The physician describes the need to control the situation from a professional point of view to protect the patient. She mindfully chooses what to emphasise when talking to her patients about different treatment alternatives. Why would you bring into play something that may be too strenuous, even if is technically possible? On the other hand, why shouldn’t the patient be the judge of their own limitations? These are difficult questions that physicians balance in their daily work, and that challenge the notion that transparency and patient participation are unequivocally in the patient’s best interest (Pilnick and Dingwall, 2011).
Concurrent with Dew et al. (2019), physicians in this study embrace different approaches. While some state that they try not to interfere with the patient’s decision, others emphasise that it is part of their job to provide as clear a recommendation as possible. As one physician puts it: ‘what is most important is that patients learn what is the optimal treatment for their disease, and that it happens fast and that they receive information that matches the knowledge they may have about medicine, surgery and cancer because that varies greatly’ (Physician, 67, hospital 4). This, informants argue, is tied to their work ethic and embedded in the clinical practice guidelines. Physicians are responsible for providing recommendations that aligns with professional standards. Ultimately, they are the ones in charge; patients cannot demand certain types of treatment if they conflict with the physician’s professional assessment of what is best in the situation in question.
Communicating the relevance of time
Thorne et al. (2013: 291) remark that it often takes time for cancer patients to develop the confidence to partake in decisions about their care, even though ‘key decisions are often required during the earliest stages of the experience, when emotionality is intense, relationships are new, and information overload is occurring’. The relevance of time in cancer care is multifaceted. According to Maiga et al. (2017: 1796), timeliness of care is ‘among the few modifiable factors’ that cancer care professionals can control. Similarly, it could be argued that temporality, that is, the pace at which the sequence of events is carried out, is also one among the few aspects over which it is possible for cancer patients to exert their influence.
The CPPs establish temporality as a core quality indicator of cancer treatment whereby ‘faster’ connotes ‘better’ (Malmström et al., 2018). Most informants agree that faster is beneficial for the overall well-being of the patient. Waiting, whether for a diagnosis or to start treatment, is described as a significant source of stress in an already-difficult situation. However, healthcare professionals also experience the idea that faster equals better as a double-edged sword, because patients have different temporal preferences. Sometimes the scheduling can be too tight. Here are excerpts from two informants illustrating this predicament: Sometimes [patients] ask about waiting times and stuff like that, and sometimes we say that “you are supposed to have surgery within a certain amount of time”, right, and patients react differently when they receive a diagnosis. Some are like “oh my God, I am scheduled for surgery within 14 days already, that was very fast”, and some get terrified because of that. Then it is important that we tell them why. I mean, we have to tell them that we have deadlines, right, and then the CPPs might be mentioned, that the government has given us a set of deadlines, and we need to keep to the deadlines. (Nurse 18, hospital 1) Once I experienced being yelled at by a patient saying, “you don’t allow him to make his mind up!” [. . .] these people, they were irritated because they meant that he had to breathe on his own, he had to, as he didn’t like all the machinery. He had to approach it at his own pace. (Physician 48, hospital 3)
These statements illustrate that patients can respond differently when grappling with a cancer diagnosis and treatment recommendations, and, although the CPPs deadlines can be helpful, they can also be disconcerting. Some patients, informants note, need more time to process their changed situation. The fast-paced trajectory can signal a kind of danger that elevates fear and anxiety. As one nurse remarks: Suddenly two weeks becomes crucial, right, and that can create some fear in a patient who has been living with this cancer for months. It’s not like we know—with cancer, it could have been there for months. (Nurse 65, hospital 4)
Cancer is not the only thing that is happening in patients’ lives. Prostate cancer patients, in particular, informants report, regularly request postponing their treatment in favour of, for example, going on a planned vacation. One physician explains that since cancers evolve differently, being diagnosed does not necessarily mean a medical emergency in need of immediate intervention: Theoretically, it will always be like, I mean, at one particular point in time, that cancer will spread, right, and it’s a matter of intervening before that happens. But it is. . . most cancers don’t spread from one day to the next. Kidney cancer, for example, right, so if the time frame was three months longer, that would not matter. (Physician 15, hospital 1)
The physician’s assertion highlights the fact that the politically-established time frames do not always mirror the medical or psychosocial reality experienced in clinical practice. In many situations, there is room for greater flexibility from a medical perspective, but accountability to time frames adds pressure to the communication process. Sometimes there is more time, from a medical perspective, than the CPP guidelines allow.
Concluding remarks
By using IE to explore the social organisation of communicating with patients from the standpoint of physicians, a complex picture of interdisciplinary interaction in conjunction with different ruling ideals emerged. It is evident that healthcare professionals work with patient communication is primarily informed by the biomedical paradigm and the organising of events around information pertaining to the process of discovery and treatment of the cancer. However, as cancer is often a stressful and fear-inducing diagnosis, informants across all professions recognised the importance of tending to the patient as a whole person with both biomedical and psychosocial needs. The CPP policy, with its specific focus on transparency, speed, and monitoring of time frames, creates new challenges for an already delicate situation. The increased focus on patient participation challenges the efficiency required by the CPPs, as more informed patients yield more time-consuming communication. In different ways, the balancing of different experiential realities runs as a common thread through the four aspects of communication work disclosed in this study.
The CPP policy compels healthcare professionals to collaborate in a tightly and consistent manner, which, in turn, improves continuity in communication with patients. Continuity of care rests on a clear division of communicative responsibilities between practical and medical information. However, continuity in communication moves beyond providing patients with adequate information about examinations, diagnosis, treatment, and sequences of events. It involves bringing all these different aspects together and assisting patients in the processing of both the information and their situation over time. While (hospital) physicians focus their interaction with patients on the biomedical aspects of care within the bounds of scheduled appointments, nurses (and to some extent coordinators) emphasise their availability, their presence and the psychosocial support they can provide. The study reveals a subtle disjuncture between physicians and other healthcare professionals. Informants remark that sometimes physicians refer patients for diagnostic tests or treatments without adequately informing patients about their actions, which complicates the communication work of those on the receiving end of these referrals. However, as Dew et al. (2019) note, informing does not automatically signify understanding. How physicians articulate the information and phrase their questions influences both patient perception and participation. This suggests that it is just as important that physicians take the time engage with their patients in ways that ensure that a mutual understanding is achieved.
Physicians’ accounts of their work with patient communication indicate a sensitivity to the diverse needs of patients, but also that physicians are juggling what might be called ‘physician–centred’ and ‘patient–centred’ approaches. This is evident in their emphasis on how information must be tailored to fit the needs of each patient, and how they choose to use their professional power to restrict certain types of information as they see fit. This is a practice that has implications for the autonomy of patients but is justified as being an act of consideration for the patient’s psychosocial and emotional wellbeing. In a different framing of events, however, physicians regulate information to prevent patients from activating their rights and initiating complaints.
The CPP policy signals that, to achieve quality of care, it is crucial for healthcare professionals to get the patient diagnosed and in treatment within a specific time frame. Activating their biomedical knowledge, healthcare professionals argue that although time matters, CPP time frames create an artificial impression that all cancers must be treated with the same urgency, and that all patients have the same temporal needs and desires. This study reveals how CPPs organise physicians’ work in a way that can be at odds with their knowledge and expertise in relation to each individual patient. The policy seems to hook people, both staff and patients, into a standardised system through which they might lose touch with their human experiences. An important pitfall is that healthcare professionals become actors on a cancer assembly line, whereby their professional judgements as well as the individual preferences of patients, are subordinated to the ruling principles of the CPPs. Paradoxically, this preclusion of relational practices happens inside ideological investments in patient-centred care and collaborative decision-making.
Footnotes
Acknowledgements
I would like to thank the informants for their participation in this study. I would also like to thank all the research team members: Erna Håland, Line Melby, Gudveig Gjøsund, Anita Das, Berit Brattheim, Marit Solbjør, Heidi Gilstad and Kari Sand, as well as Kari Nyheim Solbrække and the anonymous reviewers for assisting with their constructive feedback which helped me to improve the article.
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study is part of a larger research project evaluating the introduction of CPPs in Norway, funded by the Research Council of Norway (project number 272665) and the Norwegian University of Science and Technology.