
Abstract
Persuasion knowledge is personal knowledge about persuasion attempts that has an effect on the way people respond to these attempts. Persuasion attempts are made to effectively handling the Covid-19 pandemic, which is dependent on high public compliance with vaccination programs. Drawing on the idea of persuasion knowledge, we aimed at elaborating the various categories of perceived information gaps experienced by vaccine hesitants during the Covid-19 vaccination campaign. At the beginning of 2021 we conducted 20 in-depth interviews with Israelis who had decided not to be vaccinated against Covid-19. Analysis of the interviews revealed three main categories of information gaps experienced by the interviewees: missing information, manipulated information, and discrepant information. We analyzed how these are associated with distrust and may impair the persuasion efforts of governments and health authorities. Perceived information gaps, as part of persuasion knowledge, may increase negative responses, and therefore constitute an important factor in persuasion campaigns.
Introduction
Information is a key component of vaccination decision-making, but it also presents several challenges in the form of misinformation and incomplete information, as well as inconsistent and complicated scientific information.
Information gaps are defined as a disparity between what is known and what needs to be known by the decision maker (Ben-Haim, 2004). The concept of information gap can also refers to people’s access to information or to their information analysis skills (Compaine, 2001). In this article we follow Golman and Loewenstein’s (2018) use of the concept of information gap as a question that one is aware of but is uncertain as to which of the possible answers to adopt. People may form beliefs about information gaps and the likelihood that a particular piece of information is either correct or misleading (Golman and Loewenstein, 2018), and act accordingly.
Information gaps are absent from the discourse concerning trust in information sources during persuasion attempts. People need to rely on information that is meaningful and real to them for better decision-making. Qualitative and reliable information is therefore a prerequisite for better decision-making (Golman and Loewenstein, 2018). Information that is presented during campaigns aimed at influencing people’s attitudes, decisions and actions, contributes significantly to successful persuasion.
To address this lacuna in the research literature we examined various categories of information gaps perceived by Covid-19 vaccine hesitants in Israel, information gaps that lead them to distrust of the government, health professionals and the media, and refusal to be vaccinated. Understanding information gaps can contribute to persuasion efforts targeted at influencing public opinion and behavior.
In this article we highlight the importance of information gaps as part of persuasion knowledge (Friestad and Wright, 1994); information gaps that undermine the success of persuasion campaigns and even provoke resistance. Understanding them are therefore important for the achievement of high public compliance with the vaccination campaigns, especially in times of crisis such as the Covid-19 pandemic which requires the provision of information on the one hand and decision making on the other.
Vaccine hesitancy and trust
The concept of vaccine hesitancy refers to concerns that people have regarding vaccination (Dudley et al., 2020) and to the resultant delay in acceptance or refusal of vaccines despite availability of vaccine services (Sage Working Group on Vaccine Hesitancy, 2014). Determinants of vaccine hesitancy are complex and context-specific, with lack of confidence and public trust figuring prominently among them (Larson et al., 2014). Confidence refers to trust in the effectiveness and safety of vaccines themselves, in the system that delivers them, and in the policy-makers who determine vaccine guidelines (Sage Working Group on Vaccine Hesitancy, 2014). When official sources of information, such as governments or leaders, restrict information or deliberately disseminate misinformation in order to reassure anxious publics, they jeopardize their own credibility and create a climate for the viral spread of unfounded speculations and conspiracy theories (Larson, 2020).
The Covid-19 pandemic is unique both in its extensive scope and impact and in the very rapid and relatively innovative path of vaccine development. As in other cases, lack of trust has been suggested as a prominent factor of Covid-19 vaccine hesitancy. This lack of trust is seen to derive from the rapid development and emergence of the vaccine and its unknown side effects; distrust of the pharmaceutical industry and medical profession; and conspiracy theories such as clandestine pacts between the government and the pharmaceutical industry (Chevallier et al., 2021).
The Covid-19 virus has triggered a combination of unverified information, misinformation and intentionally manipulated disinformation (Larson, 2020), with the large amount of contradictory information adding to the confusion (Strully et al., 2021). The conflicting, inconsistent and biased information presented by the various authorities and health organizations regarding the Covid-19 virus has given rise to uncertainty and distrust in the vaccines (Wilson et al., 2020).
Persuading people who have doubts about or oppose vaccination is difficult, especially considering the flood of misinformation on social media and from anti-vaccine activists. The amount of misinformation regarding Covid-19 on social media is amplified by past misinformation regarding vaccines. De Giorgio et al. (2022), found that participants whose information derived from social networks, blogs, forums, or encounters with other people, were more likely to unvaccinate compared with participants whose source of information was the TV, radio, or their general practitioner. Subscribing to anti-vaccination ideas is also correlated with a belief in other conspiracy theories (Goldberg and Richey, 2020). The public might perceive government attempts to enforce vaccination as a conspiracy and lose trust when government decisions are based upon incomplete, inaccurate, or misinterpreted data (Atkinson and Atkinson, 2021).
Such a situation aptly exemplifies public crisis communication. A crisis is a situation where personal health and safety is mitigated (Abbaspour et al., 2021). Its unexpected and brutal nature arouses feelings of urgency and uncertainty. Crisis communication aims to distribute accurate and relevant information, reduce uncertainty and ensure informed decision-making (Olsson, 2014). While crisis communication is essential for saving lives and plays a major role in disaster and crisis mitigation efforts, the public often tends to misinterpret messages, ignore warnings, and generate false rumors (Glik, 2007). Information on how to act is best delivered by experts (Olsson, 2014); there are, however, differences in the public’s perception of risk and in their willingness to respond and adhere to risk mitigation strategies. Contradictory information may increase misunderstandings and reduce people’s perception of risk while misinformation disseminated on social media triggers emotional responses and increases anger (Malecki et al., 2021).
The attempts at persuasion themselves may lead to persuasion knowledge—the knowledge people have when they believe someone is trying to persuade them. This knowledge may, in turn, lead to a reaction to the very attempts at persuasion, a reaction that can be contrary to the interests of the persuader.
Persuasion knowledge
“Persuasion knowledge is personal knowledge about persuasion attempts that consumers develop and use whenever they believe they are targets of persuasion” (Isaac and Grayson, 2016: 570). Friestad and Wright (1994) developed the Persuasion Knowledge Model around the basic idea that consumers use knowledge regarding persuasive attempts to identify the intentions of the individuals or entities attempting to persuade them (Campbell and Kirmani, 2000). A persuasion attempt is defined broadly as “the perception of an agent’s strategic behavior in presenting information designed to influence someone’s beliefs, attitudes, decisions, or actions” (Friestad and Wright, 1994: 2).
Consumers are able to use their persuasion knowledge to identify that an agent is attempting to influence them and respond by taking advantage of the process to achieve their own goals (Campbell and Kirmani, 2000). Consumers’ persuasion knowledge influences their responses to the persuasion attempts so it is important to understand under which conditions persuasion knowledge leads to positive or negative results for those who wish to persuade (Eisend and Tarrahi, 2022).
According to Campbell and Kirmani (2000), customers’ suspicion increases in proportion to their level of awareness that someone is trying to profit from their purchase. Although the benefit accruing to service providers is of a different kind, people who possess persuasion knowledge remain alert and suspicious toward what they perceive as opportunities for the service providers. The mere anticipation of a persuasion attempt is sufficient to arouse their distrust and customers may suspect that the information is incomplete, biased, and manipulative even when the service provider presents information that contains no recommendations (Ngamvichaikit and Beise-Zee, 2014).
While the Persuasion Knowledge Model is originally a consumer behavior model (Campbell and Kirmani, 2000; Friestad and Wright, 1994), in the current article we apply it in the context of vaccination campaigns which, as a credence service, refer to patients rather than to consumers. Like in marketing, in matters of health, patients’ perception of manipulative intent might result in behavior which is the opposite of what was intended (Weber et al., 2021).
The aim of the present article is to examine the way people’s perception of information communicated to them as a persuasion attempt impacts their responses and willingness to comply. To this end, we analyzed the Covid-19 vaccination discourse in Israel during the widespread vaccination campaign at the beginning of 2021 that included intense persuasion efforts to encourage people to vaccinate.
Israel was one of the leading countries to launch a massive vaccination campaign following the “real-world epidemiological evidence collaboration agreement” signed with Pfizer and BioNTech SE pharma company. During the vaccination campaign, while morbidity rates remained very high, the vaccines were available and accessible. A government campaign encouraged people to be vaccinated and sanctions were imposed on those who did not. Nevertheless, some chose not to be vaccinated despite the potentially negative consequences of this decision. The immense efforts invested in persuading people to be vaccinated against Covid-19, and the significant numbers of those who remained unconvinced, led us to probe more deeply into the perceptions and motives of those Israelis who decided against being vaccinated against Covid-19.
We focused on the Israeli case since Israel was the first country to achieve a high vaccination rate following a rapid and effective rollout of the initial phase of Covid-19 vaccines at the end of 2020 (Rosen et al., 2021), and a mass vaccination campaign, in the media and through official messaging. However, our analysis and conclusions are relevant not only to the understanding of the ways people respond to persuasion in the context of the Covid-19 pandemic and other vaccination campaigns, but we believe that they may contribute more extensively to a better comprehension of health persuasion campaigns in general.
Methodology
During February-March of 2021, in the midst of Israel’s vaccination campaign, we conducted semi-structured in-depth qualitative interviews with 20 secular Jewish Israelis who had decided against vaccinating for Covid-19. Only secular Jewish participants were included since factors relating to religiosity and national-ethnic identity were found to affect Israel’s Covid-19 vaccination rates. The Arab and ultra-Orthodox (religious) Jewish minority populations exhibited a tardier and lower vaccine uptake than the general Jewish population in Israel. However, following culturally tailored interventions (e.g. working closely with community and religious leaders; using tailored language in advertising Covid-19 vaccines; and adopting a culture-specific approach to each population), these gaps were narrowed, although not fully eliminated (Muhsen and Cohen, 2021).
We followed the principles of “snowball” sampling in our recruitment of participants, a method employed extensively in studies dealing with sensitive matters (Liamputtong, 2007). We chose to reach out initially to participants on a personal basis, relying on our existing social, professional and familial network, reaching out thereafter from one participant to another on a personal basis, following the participants’ recommendations. This method enabled us to establish a relationship of trust with individuals who might at times be skeptical. Since this recruitment method may limit heterogeneity and create bias among participants, our interviewees were drawn from diverse age-groups, localities and occupations so as to maximize poly-vocality.
Interviewees include 12 men and 8 women ranging in age from 21 to 66 (average 43). Nine of whom are married with children; four divorced with children; one engaged to be married and two singles (one of them with two children). Their relatively high level of education—three have a secondary school education; three have diplomas in further studies and the remainder all possess a tertiary education (nine BA/BEds, four MAs, and one PhD)—is a factor that might positively impact their health literacy.
The interviews lasted between 45 and 75 minutes. We questioned the participants about their attitude toward vaccination in general and the Covid-19 vaccine in particular; about their opinion regarding the pros and cons of vaccination; about their decision-making process not to be vaccinated against Covid-19; and about the various sources of information they encounter: friends and family, colleagues, spiritual authority figures, governmental campaigns, online sources, and the media. Our inquiry also sought to identify what, in their eyes, constitutes a reliable source of information. The questions were neutrally formulated and did not reflect any bias regarding any potential benefit or harm deriving from the vaccine.
About half the interviews were conducted in locations convenient to the interviewees (their home or workplace) and about half were conducted via the Zoom application given the restrictions placed on meetings due to the Covid-19 pandemic. Oral informed consent was obtained prior to commencing the interview.
Interviews were tape-recorded and then transcribed verbatim. A thematic analysis (Braun and Clarke, 2006) was conducted to identify key themes. The process included six stages: first, reading and re-reading the data and noting initial ideas; second, systematically coding interesting features of the data and collating data relevant to each code; third, gathering codes into potential themes; fourth, generating a thematic “map” of the analysis; fifth, refining each theme, and laying bare the overall story the analysis tells; and finally, preparing a scholarly report of the analysis.
We applied this general scheme using two cycles of coding. In the first cycle of coding, we followed Saldana’s (2016) coding methods and adopted the “descriptive” coding strategy, focusing on codes applied to a basic topic from the data. Descriptive codes can be used to locate something that is easily identified in the text such as “online information,” “governmental information,” and “media information” in the present interviews. At the outset, the second and third authors analyzed a few interviews in parallel and their results were compared to ensure compatibility of the codes selected for analysis. Once consensus was reached, the second author analyzed the interviews using Atlas.ti v7.5.17 textual analysis software. While we did not raise the issue of information gaps with the interviewees, the existence of such gaps was clearly demonstrated in what they said. We therefore decided to create a second cycle of coding.
In the second cycle of coding, we chose to focus on the subject of “information gaps” (a concept deriving from the theoretical field of Information Studies), highlight the quotes relevant to the subject and organize them into the three categories that currently appear in the Findings section. In doing so, we followed Huberman and Miles’s (1994) emphasis regarding the necessary connection between a theory and its concepts and the empirical indicators that are reflected back through the concepts to the theory.
Findings
The interviews with the Israelis who chose not to be vaccinated reveal three main categories of information gaps: missing information, manipulated information and discrepant information (Figure 1). The interviews included claims about missing information which the interviewees perceived to be the result of concealing information and silencing the voices of vaccine opponents; about information manipulated by the government and the media through distortion, biased interpretation and exaggeration; and about discrepancy—a gap between personal knowledge and the information presented by the media; between competing authoritative sources and policies that are perceived as illogical. The interviewees responded to these gaps with suspicion and distrust which paved the way to vaccine hesitancy and refusal.
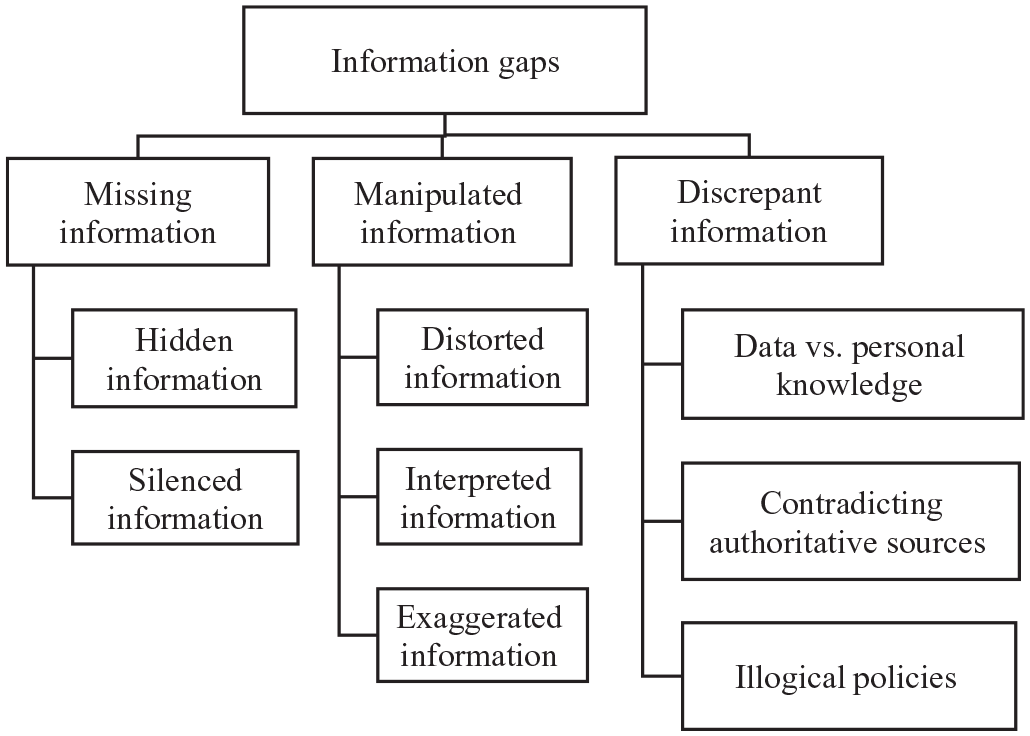
Categories of information gaps.
Missing information
Most interviewees (henceforth referred to by pseudonyms) believe that the government conceals information from the public and silences dissident opinions so that the information they do receive is lacking and incomplete. The hiding of information is perceived by some of the interviewees to be caused by censorship of some of the data by the government as well as by the mainstream media which cooperates with the government in order to present the public with a one-sided picture of the pandemic. This alleged concealment creates suspicion among some of the interviewees.
At least if they [the government] were transparent in all their actions, but that’s not the case. All records of the Corona cabinet’s discussions in Israel will remain confidential for 30 years. (Uri)
A few interviewees note that some details included in the contract signed with Pfizer were hidden from the public.
The contract with Pfizer is mostly redacted. One of the things that is blacked out there is the date. . . The date is a very, very important factor in the political decisions made here. (Lili)
Other information that was hidden from the public, according to some of the interviewees, is information about the side effects associated with the Covid-19 vaccine.
[Information was hidden] to prevent people from seeing the truth. There are real cases that are not talked about. It was not mentioned that a 24-year-old suddenly collapsed after the second dose of the vaccine; that a 26-year-old died a few days after the second dose; that some pregnant women started bleeding and other pregnant women aborted after the second dose. (Nadav) This specific vaccine is problematic. . . We see a lot of mortality from myocarditis, from strokes. We see it, although they hide it, the information is there. It won’t help, the information exists. (Lili)
Some interviewees feel that the media, which is supposed to expose information that the government withholds from the public, is in fact cooperating with the government and its agencies. This evokes antagonism and distrust among them.
The media does not present the things that it should present. The media conceals things. . . it does not promote a real discussion about what is happening. (Roni) I see that in the newspapers; every day there is a report regarding a young Corona patient who fell ill and died, okay? But I don’t see anything written about my friend who was vaccinated and had a stroke, [the vaccine] paralyzed half her face; about my other friend’s sister-in-law, a perfectly healthy 42-year-old woman who died within a week of receiving the vaccine. I do not see any of these in the newspaper. (Ohad)
Some of the interviewees not only point to the intentional hiding of information but also claim that the voices of vaccine opponents are silenced. The silencing is perceived as a method used by the government and the media to quash opinions that are contrary to the government’s official positions regarding the disease and the different ways to cope with it. The absence of another point of view, another voice, from the discourse, prevents balanced information from reaching interviewees and damages their trust in the information that has been given to them.
If I see that one group is being silenced I do not believe [the information]. Why did you silence them? Maybe they’re talking nonsense, okay, so what? They are allowed to speak. (Ohad)
The silencing takes place, according to interviewees, not only in the traditional media but also on social media, a sphere where a more open discussion could be expected.
It’s not just the [traditional] media, it’s all the social media. After all, every post that is written [against the vaccine] that goes up on Facebook. . . for some reason is eventually censored and disappears. (Nadav) Facebook has censored a thousand of my posts. . . If they silence these posts, then it shows they are frightened of something. If it did not bother them then okay, let there be some crazy people talking against vaccines, what do they care? But they are afraid. . . I actually want to hear what the silenced people have to say, I want to know why are they being silenced. (Orly)
In particular, a few interviewees are outraged by the silencing of certain physicians who are Covid-19 vaccine opponents. As physicians, they are generally perceived as a professional and reliable source of information, but in this context, they are silenced and excluded from the discourse.
The [medical] license of a doctor who said that the Corona vaccine is ineffective was revoked. . . They want me to believe but show me only one side and do not allow the other side to express themselves. (Ohad) Wherever there is a discussion on vaccination, one opinion is given voice. . . but the other voices are not expressed at all. I mean the very fact that the discussion was so one-sided is what made me suspicious. (Ido)
Manipulated information
Some interviewees claim that the information about Covid-19 disseminated by the government and the media is manipulated, and even if not always knowingly falsified, it is distorted so that public opinion can be shaped to serve the needs and goals of the government. These interviewees addressed the various means by which information is manipulated: distortion, interpretation, and exaggeration, which includes the use of intimidating rhetoric.
Regarding their claims that information is distorted, the interviewees offered the following comments: I do not believe them. I can tell that they often “play games” with the data. They increase something, decrease something and. . . it’s really difficult to know what the real situation is. (Yonatan)
The interviewees’ feeling that the information is distorted is rooted in the lack of clarity regarding the epidemic’s data: the number of verified people infected with the virus per day, the exact death toll, and the victims’ cause of death.
I’m not sure that everyone who is diagnosed as infected with Covid-19 is really sick. I mean there is also the matter of distrust. . . I think they “play” a lot with the numbers. (Yonatan) A 23-year-old patient collapsed [after vaccination]. . . I really remember that. So I feel distrust, especially since the first report stated that in the end the cause of death was unknown. . . I really do not believe the information. (Ohad)
Regarding the interpretation of information, some interviewees feel that the government should only supply data, numbers and dry facts without confusing the issue with possibly tendentious interpretations, explaining that in their view interpreting the facts is superfluous and undermines their trust in the data presented.
Whether lockdowns help or not, for example, is already an interpretation, it’s not a fact that the Ministry of Health issues. . . I’m not the naïve spectator who will just accept it. . . it’s not all facts. . . It intensifies my suspicion that someone here sees things in an emotional and contaminated way (Eli) This [what politicians say] is not something you can doubt or not doubt, because it is not a fact. You can agree or disagree; believe or disbelieve, but there is nothing here that is presented to you as a scientific fact. (Avi)
Some of these interviewees expect “clean” information, uncontaminated by government propaganda.
I’m not looking for an answer, I’m looking for information. . . so I say okay, when it comes to pure data they have nothing to lie about. (Ohad) When the WHO publishes dry numbers these are real numbers, when it publishes percentages it is a lie. . . Our ability to present statistical data is indeed amazing. . . how easy it is to distort data in statistics, how easy it is to present something that is incorrect. (Avi)
Another means of manipulating information about Covid-19 mentioned by some of the interviewees, is deliberate exaggeration of the situation. They expressed a desire to get a more accurate and proportionate picture of the pandemic.
Mortality rates went up so they took that word – “up” - and inflated it, yeah? But. . . the bottom line is that the mortality rates went up quite negligibly. (Maor)
According to some of the interviewees, exaggeration as well as distortion of information by the government and the media, are sometimes used as a tactic designed to motivate the public into action. At times, the goal is to instill fear or anxiety as a means of controlling their behavior. Two of the interviewees explained how the intimidation tactic works.
I do not believe them; I do not believe. Someone in the Ministry of Health says. . . my strategy is to scare and in the name of that strategy I am allowed to distort the facts. (Eli) I absolutely do not believe them, because I see this as a process of intimidation, it is a kind of brainwashing. Unfortunately, some people have since accepted it, which is why they wanted to be vaccinated. (Nadav)
While this rhetoric of intimidation arouses feelings of antagonism and fear in the interviewees, their fear is of being manipulated by the government rather than of the disease itself.
It scares me. The lack of transparency, the social pressure, the fact that the media is constantly preoccupied with it. All the time. From the beginning of Corona, news coverage has been non-stop. I’m really in shock, it’s something that I haven’t experienced before. All day one sees intimidation, intimidation, intimidation and everything is presented in such a stressful tone. . . I do not like all this hype around Corona, I do not like it. (Nadav)
Discrepant information
In addition to the interviewees’ claims about missing and manipulated information, they described experiencing discrepancy. This experience is a literal expression of information gaps—a gap between personal knowledge and the information presented by the media; discrepant information obtained from competing authoritative sources and policies that are perceived as illogical.
I have not heard of anyone around me who has died or been seriously ill and hospitalized. . . Where are the dead? I do not know. I do not see them, not in my circles, not in the circles of people around me. (Eli)
Some of the interviewees describe conflicting information they receive from various authoritative sources Sadetzki [Prof. Sigal Sadetzki was the head of public health services in the Israeli MOH during the first wave of Covid-19]. . . said there was no need for masks and Anthony Fauci first said they are unnecessary and then said afterwards that there is a need for them. So I say, let’s wait a moment, they keep changing their minds. . . and these are respected people. (Orly)
On top of the discrepancies experienced between their personal knowledge and the information given to them as well as the confusion created by contradictory information, few interviewees also report a sense that some of the policies and top-down decisions regarding the managing of Covid-19 are illogical. The perceived irrationality of the decisions undermines their trust in the government and the health authorities.
Take for example mask exemption for sick people - what is the point?. . . It does not make sense in any circumstances, and it is also cannot be implemented. There were also all sorts of ridiculous instructions regarding kindergartens. The kids are divided into various groups but then, at lunch time, everyone mixes. . . This is not how it should be done when there is a serious epidemic. (Ela)
Discussion
Generally, persuasion campaigns should be critically judged: resistance toward persuasion campaigns is not inherently negative and may actually represent a positive act. However, in the case of public health different criteria might apply. While persuasion campaigns should always be critically scrutinized, in the case of vaccination during a pandemic, when solidarity is crucial and the work of the healthcare authorities is beneficial to public health, persuasion campaigns run by health authorities have merit.
The findings drawn from this exploratory research make several contributions to the literature on persuasion knowledge, public health campaigns, and the better understanding of vaccine hesitancy.
First, researchers have so far not addressed information gaps in the context of persuasion knowledge. Our study identifies information gaps as important factors in persuasion attempts and points to their potential negative effects. It has already been suggested that persuasion knowledge can increase negative responses and lead to less favorable evaluations of persuasion attempts (Attaran et al., 2015; Campbell and Kirmani, 2008). A meta-analysis (Eisend and Tarrahi, 2022) showed that persuasion attempts using sources not deemed transparent may increase persuasion knowledge effects that are unfavorable and lead to primarily emotional and behavioral coping responses rather than cognitive ones.
In the present study it was likewise found that the information gaps associated with persuasion knowledge may create an effect opposite to the one desired. According to the interviewees, they experience three categories of information gaps associated with the discourse surrounding Covid-19 vaccines: missing information, manipulated information, and discrepant information.
The missing information includes both hidden information such as missing data or censored facts, as well as silenced information; for example not giving voice to those who express opinions that deviate from the authorities’ position regarding Covid-19 and its management. A similar feeling was found in a study by Ernest-Samuel and Uduma (2022). The government’s lack of transparency in providing news and information about Covid-19, was perceived as a form of censorship and adversely affected public trust.
The interviewees in our research believe that some of the information regarding Covid-19 is manipulated by various means including data distortion, presentation of interpretations instead of facts, exaggerated information and the use of intimidating rhetoric. They also experience a painful gap between their personal knowledge and what is presented by the media, contradictory information obtained from competing authoritative sources and official decisions that are perceived as illogical. The negative impact of contradictory information has been discussed in Strully et al. (2021) and Malecki et al. (2021). It was found to create confusion and distrust, and undermine experts’ authority.
It can be assumed that the information gaps experienced by the interviewees stem from their personal knowledge and experience, but also from their persuasion knowledge; for example from their belief that they are being subjected to persuasion attempts. We assume that in the case presented here, the combination of persuasion knowledge and information gaps was a contributing factor in the decision not to be vaccinated. Second, this article may also have implications for public health campaigns. Today there is usually more information available than is needed for decision-making; the challenge for policymakers is not only to convey reliable information but also to understand how to present the information so that it can be of practical use in decision-making.
The credibility associated with information sources is the most tested variable in persuasion research (Wallace et al., 2020). The credibility of a specific source is traditionally perceived as a combination of expertise (based on knowledge and experience) and trustworthiness. Studies indicate that credibility has an important impact on people’s attitudes and eventually on their decisions (Wallace et al., 2020). Surveys in the United States, for example, suggest that physicians, nurses, and pharmacists remain the most highly trusted professionals (Bloom et al., 2020).
Our findings indicate that when experiencing information gaps associated with persuasion knowledge, health professional, and authoritative sources are sometimes perceived as unreliable despite their expertise. People suspect the information provided by these professionals and point to the information gaps they experience as causing distrust and doubt. They therefore act against what they are persuaded to do, in this case—to be vaccinated.
In this context, the present article can also contribute to media studies and medical sociology (Seale, 2003). Contemporary life offers many sources of knowledge, most notably and with the most pervasive influence—the mass media. Media consumption provides a basis for constructing a self-identity, allowing people to choose from a plethora of channels and content media a portrayal that fits their view. The popular mass media play an important role in undermining trust in professional authority in health matters by presenting ordinary people and elevating them to the status of “heroes” who command considerable authority (Seale, 2002).
People also encounter in the media a variety of resources to draw upon in telling the story of their selves, which may also influence their health decisions and the nature of their response to health policies. People’s behavior may be heavily influenced by resources and knowledge accessed from various mass media. However, today’s media audience is diverse and can either resist or align themselves with media content (Seale, 2002). In our case, interviewees’ selection and interpretation of media information and explanations was perhaps governed by their critical view of the governmental experts’ vaccination persuasion campaign.
Third, the present article’s findings can help to better understand vaccine hesitancy. We cannot automatically assume the high uptake of newly recommended vaccines, such as the Covid-19 vaccines. The willingness to be vaccinated is affected by what is said, the way it is said, and who says it. Bloom et al. (2020) indicate that it is difficult to persuade people who have doubts about or oppose a particular medical recommendation, especially when they are exposed to a flood of misinformation on social media and from anti-vaccine activists (Bloom et al., 2020).
However, according to Turner et al. (2021), the medical community is often focused on correcting rumors and misinformation, instead of understanding and addressing the emotions and beliefs that form the basis for the spread of these rumors. As Schoch-Spana et al. (2021: 6004) wrote: “Vaccine uptake, and especially the widespread acceptance of vaccines, is a social endeavor that requires consideration of human factors. . . A thoughtful vaccination campaign is critical to ensure COVID-19 vaccine uptake.” The experience of information gaps associated with persuasion knowledge is at the base of vaccine hesitancy to the point of vaccine refusal.
When it comes to persuading people to be vaccinated, one of the challenges is to provide evidence-based information in clear and appropriate language, acknowledging that perceived information gaps weaken the message and undermine confidence in the source of information. Information gaps are therefore an important aspect of understanding vaccine hesitancy and the motives behind it as well as formulating better ways to cope with it.
Limitations of the research
This is a preliminary exploratory study on the subject of information gaps in the context of persuasive knowledge and mistrust. As mentioned previously, information gaps are absent from the discourse concerning trust in information sources during persuasion attempts. Since this study is based on a particular case study, future research in other contexts needs to examine other classifications of information gaps, which may reveal further categories. The present study is also pioneering in its examination of the role that information gaps play in the persuasive knowledge of vaccine hesitants. Since the methodology of qualitative research doesn’t rely on representative samples (Boddy, 2016), the motives of vaccine hesitants and the way in which persuasion knowledge is perceived and influences health decision-making should be further explored as well, involving a larger number of respondents.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.