
Abstract
General practitioners are tasked with determining the nature of patients’ emotional distress and providing appropriate care. For patients whose symptoms appear to fall near the ‘boundaries’ of psychiatric disorder, this can be difficult with important implications for treatment. There is a lack of qualitative research among patients with symptoms severe enough to warrant consultation, but where general practitioners have refrained from diagnosis. We aimed to explore how patients in this potentially large group conceptualise their symptoms and consequently investigate lay understandings of complex distinctions between emotional distress and psychiatric disorder. Interviews were conducted with 20 primary care patients whom general practitioners had identified as experiencing emotional distress, but had not diagnosed with major depressive disorder. Participants described severe emotional experiences with substantial impact on their lives. The term ‘depression’ was used in many different ways; however, despite severity, they often considered their emotional experience to be different to their perceived notions of ‘actual’ depression or mental illness. Where anxiety was mentioned, use appeared to refer to an underlying generalised state. Participants drew on complex, sometimes fluid and often theoretically coherent conceptualisations of their emotional distress, as related to, but distinct from, mental disorder. These conceptualisations differ from those frequently drawn on in research and treatment guidelines, compounding the difficulty for general practitioners. Developing models of psychological symptoms that draw on patient experience and integrate psychological/psychiatric theory may help patients understand the nature of their experience and, critically, provide the basis for a broader range of primary care interventions.
Introduction
The majority of mental health problems are managed in primary care (Cornford et al., 2007; Mitchell et al., 2009). As such, general practitioners (GPs) play a fundamental role in working with patients to determine the nature of their symptoms and to agree on appropriate care. The effective detection of psychiatric conditions such as major depressive disorder (MDD) is imperative to ensure presenting patients are offered evidence-based treatments (Mitchell et al., 2009). It is also important to avoid over-diagnosis and related over-treatment (Dowrick, 2013), exposing patients to unnecessary risks associated with antidepressant intervention (Fergusson et al., 2005). However, when considering mental health, determining the boundaries between non-disorder and disorder is complex, and GPs report difficulty distinguishing between distress caused by ‘problems of living’ and psychiatric illness (Johnston et al., 2007).
Part of the difficulty GPs face is that the nature of depression, for example, is often unclear. Although defining and identifying severe depressive disorder may be relatively straightforward, with less severe cases the overlap between indicators of disorder and ‘normal’ negative affective states increases (Horwitz and Wakefield, 2007). In this more complex middle ground, the nature of mental disorder itself is heavily debated (Ridge et al., 2015; Stein et al., 2010). The Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) of the American Psychiatric Association places an atheoretical focus on the presence and duration of a range of symptoms, as well as their associated functional impairment, in guiding the identification of depressive disorder. Although this simple approach may enhance reliability, the DSM-5 also notes that responses to a significant loss may resemble a depressive episode, concluding that determining whether disorder is present requires ‘the exercise of clinical judgment based on the individual’s history and the cultural norms for the expression of distress in the context of loss’ (American Psychiatric Association (APA), 2013: 161).
Adding to complexity, the term ‘depression’ is widely used to describe different phenomena (Beck et al., 2009). Depression can refer to symptoms related to several health conditions: a mood state; a syndrome, as in a major depressive episode (MDE); and a psychiatric disorder as in MDD. The recommendations for treatment and implications for the individual differ substantially depending on the particular meaning drawn on when the term is suggested. For instance, depression as MDD may validate the use of pharmacotherapy. Use of depression to describe low mood, however, would make this treatment strategy inappropriate. In such a multifaceted and contested area, qualitative research is important to ensure pragmatic (Hickie, 2007) and ontological (Wakefield, 2007) debates remain grounded in patients’ experience.
Qualitative research on patients’ experience of mental health problems has primarily been positioned within the sphere of MDD or depression as a condition (Buus et al., 2012; Chambers et al., 2015; Cornford et al., 2007; Gask et al., 2003; Kadam et al., 2001; McCann et al., 2012). Subsequently, research has focused on how patients’ understandings and representative models of their condition affect their understanding of and engagement with treatment (Brijnath and Antoniades, 2016). Buus et al. (2012) discussed how patients’ models focus on psychosocial causes to enable ‘concrete opportunities for personal management of the illness’ (p. 22) while remaining adaptable to incorporate biological narratives that work to legitimise the taking of antidepressant medication (Malpass et al., 2009). Johnston et al. (2007) reported similar findings, with some patients willing to accept biological explanations, while others rejected a medical cure, stressing the importance of self-management. With regard to phenomenological experience, qualitative research on MDD frequently emphasises its destructive, all-encompassing quality; patients draw on metaphors of being in ‘pits with no escape’, of ‘dys-existing’ in ‘dark tubes with no ends’ and of having no reason to wake up (Kangas et al., 2001; McCann et al., 2012).
There has been less qualitative research with patients who are near the complex boundaries of symptom expression, where disorder may be considered but is not certain. GPs are likely to see a large number of patients in this middle ground; Mitchell et al. (2011) suggest that up to 41 per cent of primary care patients experience emotional distress. How practitioners interpret these patients’ symptoms is pivotal. One GP’s interpretation of depressive disorder at this point could start a patient on a particular illness journey, with consequences including long-term pharmacological treatment (Kendrick et al., 2015). Another may contextualise patients’ symptoms within their life situation, offering normalising narratives and making behavioural suggestions (Dowrick, 2009). Both paths will potentially have a substantial impact on patients’ lives and future consulting.
In this qualitative study, we explored how patients presenting with emotional distress who were not diagnosed with MDD conceptualised their experience. Examining how these patients frame the nature of their symptoms may help inform communication strategies and appropriate care approaches for this large group. It may also inform ways of conceptualising distinctions between emotional distress and psychiatric disorder that are most likely to be useful in primary care practice.
Method
Participants
In total, 10 primary care practices in the south of England identified patients for the study, recruited through the local National Institute for Health Research (NIHR) Clinical Research Network (CRN). A purposive sampling strategy was used. Practices were asked to identify patients who had consulted within the last 3 months for whom their GP had listed a distress-related Read code in their notes. (Read codes are a coded thesaurus of clinical terms used in the National Health Service (NHS), developed by Dr James Read in 1985.) This was extended to 12 months during the study to increase the numbers recruited in the short recruitment window (March 2013 to September 2013). Distress codes were defined as codes related to emotional symptoms, rather than diagnostic depressive disorder classification. Example codes included were ‘low mood’, ‘depressed mood’, ‘emotional problem’, ‘feeling stressed’, ‘stress-related problem’ and ‘anxious mood’, while example codes excluded were ‘Depressive Disorder’, ‘Depressive Episode’ and ‘Major Depressive Episode’. We asked practices to add additional codes that their particular practice used based on provided examples. Due to the close relationship with stress and anxiety, we also permitted the inclusion of anxiety disorder codes. Practices were asked to exclude patients currently on antidepressant medication and those with recorded scores of >10 on the Patient Health Questionnaire-9 (PHQ-9; suggested to indicate possible MDD (Kroenke et al., 2001)). Identified patients were sent a study pack inviting them to contact the research team if they were interested in taking part.
A research assistant screened interested patients over the telephone. Initially, in an attempt to screen out those who may have current MDD, we used the PHQ-9 score of 10 (Kroenke et al., 2001) to identify and exclude patients with likely current MDD. However, as has been noted (Cameron et al., 2008), the PHQ-9 appeared to have relatively low levels of specificity at a cut-point of 10, and it became apparent that high scores on only a few elements of the scale (e.g. tiredness, trouble concentrating, difficulty falling asleep) were taking patients over the cut-point (e.g. new mothers). Following ethical review, patients with a PHQ-9 score of <14 were considered eligible as long as they scored 0 on question 9 regarding self-harm or suicidal ideation.
Interviews
The interviews were semi-structured and consisted of two parts. The focus for this study was on the first open-ended part of the interview (in the second part patients were asked to look through and provide ‘think-aloud’ feedback on draft online materials for stress). The open-ended interview focused on patients’ experiences that led to them consulting with their GP. Interviewers paid particular attention to following up patients’ descriptions of their emotional experience and ideas about disorders. The majority of interviews were conducted by co-author J.M. Two research fellows experienced with qualitative methodologies completed the additional four interviews. Face-to-face interviews were conducted with participants either in the participant’s own home or in a hired room at their primary care practice between February and September 2013. Interviews were audio-recorded.
Analysis
While interviews were taking place, A.G. and J.M. met regularly to discuss areas covered by participants, and the interview guide was refined as the interviews continued. All interviews were transcribed verbatim. Transcripts were read and reread by A.G. both during and after the data collection period. An inductive thematic analysis approach (Braun and Clarke, 2006) was used to analyse the data drawing on methods of constant comparison (Walker and Myrick, 2006). A.G., M.S. and S.W. independently coded the first three interviews and met to agree on preliminary codes. Following the continued coding of half the transcripts, A.G. developed a draft coding frame that was discussed and agreed by A.G., M.S., S.W. and M.M. S.W. independently coded an additional three transcripts using the coding frame; discrepancies were minor and strategies for resolution were implemented. Codes were then clustered into higher level descriptive themes, where both within- and between-participant contradictions and inconsistencies were considered. Theme labelling and interpretation were continually discussed in regular meetings held between A.G., M.S. and S.W. Once consensus was reached, resulting themes were discussed and agreed with a larger team including A.G., M.S., S.W., T.K. and M.M. Saturation was reached for the major themes. NVivo 10 for Mac was used to facilitate the analytic process. Pseudonyms have been used throughout.
The core analysis group had a diverse range of backgrounds: A.G. is a research psychologist; M.S. is an academic GP; S.W. is an allied health professional and research fellow; M.M. and T.K. are GPs by background and professors of primary care with special interests in mental health. Our epistemological position may be best characterised by subtle realism (Hammersley, 1992), aiming for objectivity while acknowledging the role of language in constructing accounts. Our goal was for a pragmatic analysis – increasing understanding of this area from a patient perspective and leading to suggestions for future research and practice.
Ethics
This study was reviewed and approved by an NHS Research Ethics Committee (Ref 12/SC/0352).
Results
Over the 6-month study recruitment period, practice staff identified 316 patients who were sent information about the study, along with study staff contact details. Overall, 40 patients responded and were contacted by our researchers. In total, 20 patients were screened out over the recruitment phase: 5 were currently being treated with antidepressants, 10 had a depression severity score that indicated a high possibility of MDD, 4 were uncontactable and 1 was no longer interested in taking part. The remaining 20 patients participated in interviews and their demographic characteristics can be found in Table 1.
Demographic characteristics of study participants.
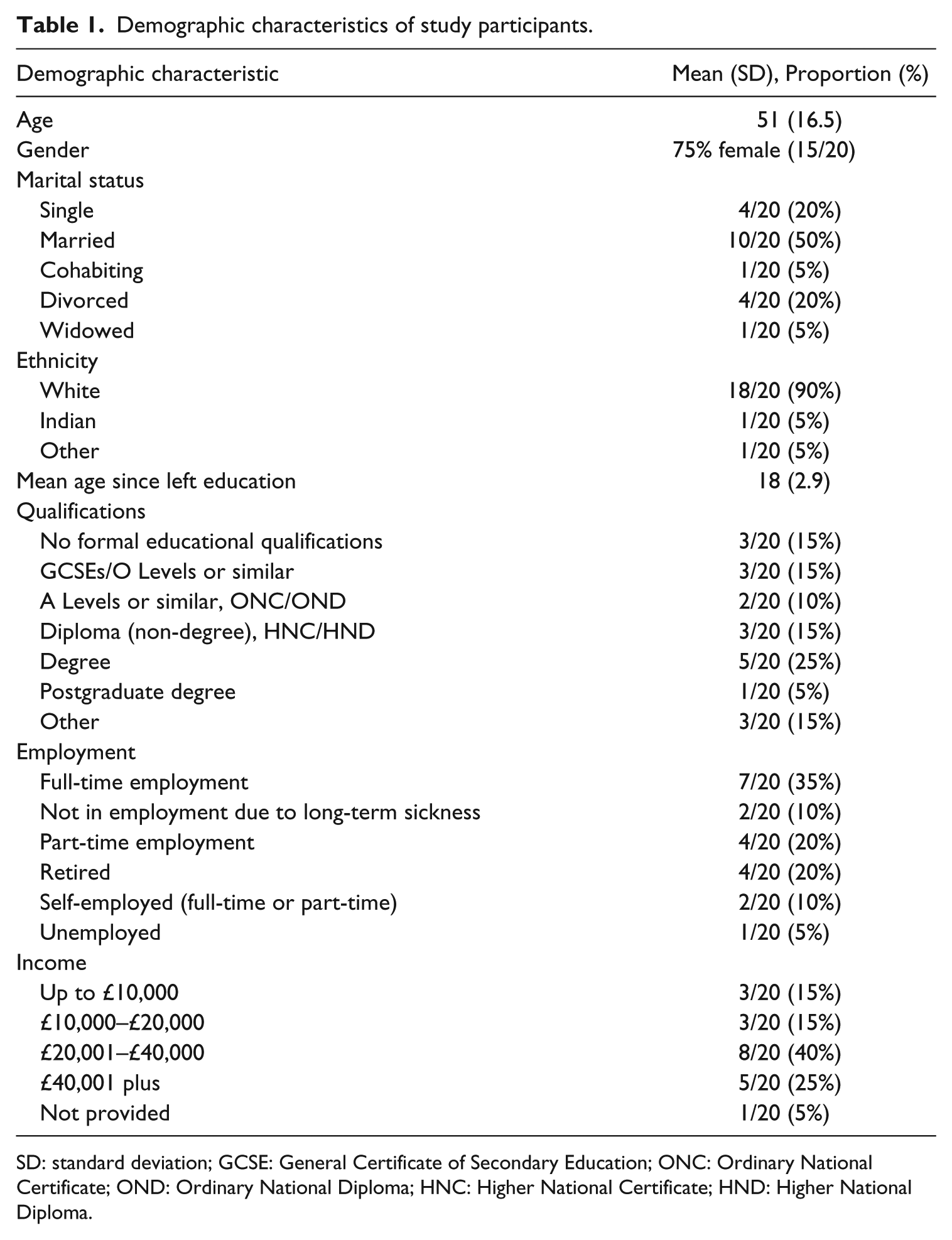
SD: standard deviation; GCSE: General Certificate of Secondary Education; ONC: Ordinary National Certificate; OND: Ordinary National Diploma; HNC: Higher National Certificate; HND: Higher National Diploma.
Findings
Participants talked in detail about the biographical history leading to their GP consultation. This included complex narratives about a wide range of family, relationship and occupational stressors. Reasons, expectations and experiences of consulting were also discussed. Broadly, participants went to their GP seeking further understanding of their experience and for solutions. Our primary analysis for this article focused on how participants described their emotional experience and how this related to their understandings of psychiatric disorders. With this focus, our analysis resulted in the development of four primary themes: difficulties coping, the stress experience, considering depression and ongoing anxiety. These themes and related subthemes are discussed in the following section.
Difficulties coping
The majority of participants referred to difficulties coping as a key part of why they attended primary care. Within this theme, there was a division with some participants giving primacy to a specific life circumstance or event, or cluster of life difficulties, and a smaller number who focused on specific problems they were having with their emotional states.
‘Too much’
Participants often described their experience with reference to a build-up of life events or situations becoming too much to deal with. Some participants listed difficult events and noted the point where the consultation with the GP was instigated. As part of these descriptions, it was common for participants to mention that they were normally ‘a coper’, but these particular stress instances were different. For some participants, where work was implicated in their emotional experience, talk regarding difficulties occurred in the context of negotiating time off work as part of the consultation with the GP:
The reason I went to my GP to talk about stress was um the fact that I live in a converted house, flats, and I’ve had two very disturbing neighbours and at the same time um, going self-employed at work and having lots of … just lots of pressure at work as well, and either or I can deal with, but together I was finding it really difficult. (Christopher) I think because I was so distressed with what my dad had ahead of him and the need for me to be supportive there that I really felt … I knew that I couldn’t continue at work because I couldn’t provide patients with the care that they needed and I knew that compassionate leave would be three days and I still wouldn’t be able to cope after that. So that was really my motivation for going to see the GP; that I knew that I couldn’t do the two. […] I would say that ordinarily I’m very much a coper. I’ve never asked for time off work to do with stress or anything like that before. So I’m very resilient and very much a coper. But this was too much. (Anna) I just think there’s a whole raft of things that are going on but being in pain everyday for eight months, which was what it was at the time, was getting me down, on top of the [traumatic event], on top of not having my husband, on top of then being really ill afterwards and nobody really taking acknowledgement of that um, yeah, I just think the few combinations of all those things has just made me, you know, feel a bit down in the dumps. (Tanya)
Within this theme, the descriptions provided by participants show that it is often a series of events or stressors coinciding that seem to lead to a ‘tipping point’ and subsequent need for the GP to help provide ways to manage associated psychological distress. These descriptions also clearly map onto understandings of psychological stress as driven by demands going beyond an individual’s perceived psychosocial and environmental resources (Lazarus and Folkman, 1986). In relation to participants’ use of language around coping, Greco et al. (1993) suggest that there is a moral, societal obligation to be healthy, and in this instance, to cope. Use of these phrases like ‘I’m very much a coper’ may be part of the work that participants do in the interactions to confirm their membership of this group despite their stress experience.
Problems with feelings/states
A small number of participants focused on problems with their own emotional experiences, over and above particular stressful life events. These participants noted the appearance of patterns and trajectories in their negative emotions. In this small group, participants reported previous experience of treated depression or anxiety. They described having to deal with and worry about ‘going back’ to unwanted states:
I could sort of see that I was kind of going downhill quite, quite quickly, you know, with certainly the physical and just sort of feeling so bogged down by all of the, you know, feelings and all that kind of thing, it was just getting me really down. (Gemma)
Despite reports of a history of treated depression or anxiety, these participants were included in this study on the basis of GP non-diagnostic distress codes. Our eligibility criteria may have picked up a full range of patients in this complex ‘non-diagnosed’ middle ground, including patients whose symptom descriptions seem to place them nearer to MDD, and its associated qualities (see Kangas et al., 2001). This provided the opportunity to explore similarities or differences in the way these participants considered their symptoms compared to the rest of the sample. For instance, in the presence of stressors including a long-term health condition and exams, Gemma appeared to be vigilant for the emergence of symptoms, indicating a return to what she perceived to be ‘depression’.
Life events are strongly associated with the onset of depressive disorder (Kendler et al., 1999); however, there may be a ‘window’ in which coping difficulties and emotional responses to these events are deemed to be expectable by both patients and GPs. The small group of participants whose talk had moved from concern about the stressor to concern about the emotion may indicate an important shift: when difficulty with emotion regulation begins to take primacy over stress-coping processes (Terluin et al., 2006), narratives regarding dysfunction may be more appropriate.
The stress experience
Participants drew on a diverse variety of terms to describe their experience, including ‘stressed’, ‘frustrated’, ‘agitated’, ’worry’, ‘concern’ and ‘upset’. Although terms were commonly used together, it appeared that activated emotion terms (Russell, 1980) were more common than terms such as feeling low, or sad, in our sample. The majority of participants’ descriptions of their emotional experience were closely tied with descriptions of life stressors and frequently overlapped with notions of coping and failures to cope. For instance, Paige’s descriptive terms for her experience below resulted from the growing pressure of frequent scrutiny of her working practices in a health setting in addition to a failed relationship:
I think just ‘stressed’ and ‘agitated’. Um, yeah, I think mainly … mainly ‘stressed’ and ‘agitated’. But just a bit of an emotional wreck really. (Paige) Um, it may be an obvious word but ‘stressed’, and the word ‘stress’ means to … where you have got excess pressure on something. Um, I felt ‘pulled apart’ um, ‘uptight’, ‘sleepless’. I felt ‘annoyed’, ‘resentful’ um, I don’t know if there is a word to recreate the alarm going off but … ‘pressured’, I suppose, ‘alone’ um, that’s a good question. Um, ‘unconfident’, ‘small’, if you like um, ‘tense’. Um, in a way you kind of lose interest in things as well, so you feel ‘uninterested’, you kind of want to withdraw, you feel ‘withdrawn’ um, I suppose those … I suppose that’s it really. (Christopher)
At times during the interviews, terms such as distress, stress and depression were used as prompts to trigger discussion around these concepts. Janet found herself breaking into tears often due to her son becoming increasingly difficult and withdrawn; her husband suggested she see her GP. Below, Janet works through each term at points in this interaction while describing her preference for ‘distress’. Stress is used to describe something that ‘everybody’ draws on so far as to lose its salience, but also as a condition; suffering from ‘stress’ is closely related to ‘depression’, and these are constructed as concepts that in the past were open to questioning:
That was something that we were trying to decide through these interviews, what is the best word to use, stress or distress? So which … do either of those fit with you?
In a way I suppose ‘distress’ is less um, I don’t know, what’s the word? Of an in word because ‘stress’, everybody suffers from like stress … and, you know, fifty years ago people would have said, ‘What do you mean stress? There is no such thing. Depression, what’s depression? People need to get off their backsides and go and do something. Um, so I think yeah, I think “distress” is quite a good word because you are “distressed” at a particular time’. (Janet)
This is an example of a process that appeared to reoccur across many of the interviews. It was common for participants to use descriptive affect terms fluidly, drawing on multiple meanings within brief exchanges.
Broader descriptions and metaphors
Moving beyond specific terms for feelings/emotions, participants used various metaphors and broader conceptualisations to describe their experience. These descriptions often worked to emphasise severity in these participants’ narratives. Participants referred to feeling helpless within a specific life context, or like their ‘world was caving in’. As with the talk around coping, some participants emphasised that they are ‘normally quite strong’. Debra used the term ‘nervous breakdown’ to describe the extent of her experience and reaching a point where ‘medical support’ may have been necessary:
My husband was very poorly, they hadn’t discovered it was his [health condition], I’d imagined all sorts of things was going on, it had gone on for about … well eighteen months, it had really driven me mad, we had moved into a wreck of a bungalow that we were trying to do up, he couldn’t cope mentally. […] So it was horrible. I don’t ever want to go back to anywhere like that. I think it was probably as near as I, I don’t know about a nervous breakdown, I don’t think I’ve ever had one, but it could possibly be the nearest I ever came to needing um support, medical support. (Debra)
Jennifer described the severity of her affective experience in the context of a complex issue centring on her daughter and her ex-partner:
I used to get a burning feeling in my body, my head used to feel like it was going to explode, I felt like I didn’t have any … any room, my head was full all the time, I had no room to think about anything else except my daughter, you know, and everything else, you know, you know, my bills didn’t slip, I always paid my rent, I always paid my bills because that I connected with my daughter, you know um, but it’s um yeah, it is, it is those triggers, I remember the GP saying to me, ‘If you recognize the triggers’, you know, ‘it’s how you deal with those triggers and how you can control them so that they don’t escalate into something else’. […]. You feel like your whole world is caving in on you and I’m quite a strong person, I like to think I’m quite strong, but that just … that knocked me sideways, it just knocked me sideways and I was very poorly with it really. (Jennifer)
In these descriptions, there was an inherent conflict with notions common in the research literature, including ‘mild’ or ‘subthreshold’ depression (Volz and Laux, 2000). GPs have determined that these patients did not have depressive disorders, but it became clear that their emotional experience was far from mild. Psychological disorders are commonly conceptualised as lying on a continuum, and as severity increases and function decreases, the possibility of being classified and treated as having a disorder gets higher (Geraghty et al., 2015). However, in the reality of primary care practice, this approach may reflect an oversimplification and it is likely that GPs were drawing on other models to inform their decision-making process.
Considering depression
Throughout the interviews, participants often reached a point in the interaction with the interviewer where they considered their experience in relation to their own held notions of ‘depression’. For many, this topic arose naturally during the course of the interview; for others, the interviewer carefully prompted discussion of the term in order to explore participants’ conceptualisations. Within this area, patients talked about comparisons between stress and depression; depression as a serious mental illness with negative connotations; and seemingly, depression as representing low mood or sadness.
Depression or stress/distress
A number of participants actively considered differences between their perception of ‘depression’ and their experience. Mary experienced a long-term health condition which was causing her to struggle emotionally. Her rejection of ‘actual’ depression points to the noted difficulty researchers may encounter when drawing on symptom counts as a means of identifying the disorder; many symptoms included in psychiatric syndromes are also a ‘normal’ part of life and functioning (Horwitz and Wakefield, 2007):
Yeah. So you mentioned there that you were maybe feeling a little bit down, could you tell me a little bit more about that?
Um, well I see … I don’t think it was actual depression or anxiety but it does throw out those sort of symptoms.
Another participant, Anna, had experience of working in a mental health setting. She spoke about consensus reached between herself and her GP that her symptoms were not depression. Instead, they reflected a reaction to a stressful situation, caring for her father with a life-threatening health condition:
Do you think there’s a distinction between the two or … [Referring to stress and depression]?
Yeah, there is. I knew that I wasn’t going to the GP because I was depressed because I knew that I wasn’t. So she said, I completely agree with you, you’re not. You’re reacting to a very distressing situation.
In Janet’s description of not being offered or wanting ‘anything’, it appears that she used her awareness of the triggers, in this case her son, as an indicator to differentiate her distress from something that would indicate treatment such as mental illness. The association implied in Janet’s talk aligns closely with the often-overlooked component of the DSM definitions – that severe symptoms as part of a culturally expectable reaction to stressors are not mental disorders (APA, 2013):
She just said that she wanted to see me. So I went in and just, you know, just we discussed him and referred him to the consultant and what have you, but I mean I wasn’t offered anything but I didn’t want anything because I know what’s causing it. (Janet)
Some participants were uncertain regarding the nature of their symptoms. Consulting with the GP provided a way to addressing this uncertainty. The quote below suggests cut-points on quantitative severity scales may have been used by Tanya’s GP in order to determine treatment, and presumably the presence of depression:
It’s the same with depression, I am not an expert so I don’t know. All I know is that I did a test at the doctors and she said if I’d have got one more point she’d be thinking about putting me on antidepressants. (Tanya)
The small number of participants in our sample who reported previously treated depression directly reflected on how it might compare to distress experiences. Again, ways of conceptualising varied through the descriptions, from distress being at the mid-section of a scale to an experience with distinct notable qualities, including the maintenance of a sense of self which was lost in the experience of depression:
And how do you think this experience compares to kind of the depression expression, do you think it is different or similar?
It’s similar. If I put it on a scale of one to ten where zero would be completely happy with life and ten would be, you know, locked in a room with a padded cell, the depression was eight and this was about a four or five. The stress was probably four, probably five actually when I think about it because at no stage … with depression I felt out of control, completely out of control. With the stress with the three things that were happening, you know, home, work and health, I knew these things were coming in at me but I always felt that sense of self and that these things were coming at ‘me’, there was still a ‘me’ in the middle.
Um, so to me I’ve had … I’ve had post-operative depression in the past and that was something totally different to what the baby blues was. I’ve never had depression from an organic form, I’ve just … I’ve had it from having an operation. Um, if you can call what I have now depression, I don’t know. But when I had it after my operation I was um staring at a wall for a month … (Tanya)
Steph, who reported multiple health conditions, describes frustration at not having her own understanding of differences between distress and depression acknowledged by health professionals:
And I think, I’ve not got depression, you know, and that’s something my psychologist get’s really annoyed about because I do feel like everything, no matter what I seem to feel, I kept being told that that was just my depression, but I wasn’t depressed, you know, anymore, I knew if I was depressed, I’d been to hell and back with it so I knew what it felt like and I wasn’t depressed, I was on the top of the world, I was just tired and in pain and, you know, things like that. (Steph)
Depression as being ‘mentally ill’ or viewed negatively
Some participants described their experience, suggesting they perceived depression to be associated with shame and stigma, talking in terms of ‘mental illness’. For some participants, it is possible that concern regarding stigma may have driven a need to assert that they are not ‘mentally ill’. However, descriptions could also be a function of participants noting suggested important differences between distress and depression (Terluin et al., 2006). This tension again highlights the complexity in this area:
It’s almost like I don’t want to say like any word like ‘depressed’, ‘depression’ and I don’t like to say anything like that. I just … I … I can’t really explain it, I just don’t … I don’t like … I don’t know. I think because there is … it’s … it’s … it’s not shameful, but I suppose because there is still a stigma attached to mental illness, I don’t even like saying, you know, I’m ‘mentally ill’ because I think, well, that makes me sound like I’m crazy, you know, like I’m psychotic, and that’s not true. (Gemma)
Debra refers to ‘real depression’ and her dislike for the term due to the perceived stigma. She also appears to move between conceptualisations: from dislike for the term due to stigma, to working to describe how the depression associated with mental illness might be different from stress processes, then back again to the possibility that she was depressed, but avoided the term again due to concerns about stigma. As previously mentioned, this fluidity was common as patients attempted to make sense of their symptoms:
Real depression is a bad one and people do suffer from it but always people say pull your socks up or pull yourself together. So depression I don’t like, although I was depressed, there is no getting away from that, I was. But I think distress is a really good word.
Why do you think you wouldn’t like depressed, because you kind of said I was depressed?
I think because you associate it with mental illness and this isn’t a mental illness, this is … you’re in this little fog at this particular moment and there is a way out but you need a little bit of support and guidance through it and you need to be able to … you need to talk it through … and that might take months. So it probably is a depression but I think people … there is a stigma attached to depression, I think, which is why you don’t want to use it.
Depression as mood
Through a number of descriptions, it appeared that the term depression was being spoken about in a different manner. Rather than being associated with mental illness, it seemed depression was used as a term to refer to sadness or low mood. Robert discussed feeing low after ‘not taking to retirement very well’:
Yeah, I think … I think I’m more prone to a bit of depression now and I get a bit depressed about being old [laughs]. And look around and what I do see around sometimes doesn’t fill me with, you know, … got one or two people that are sort of falling off with cancer, you know, young people … but that’s natural to feel … to feel concerned, depressed, annoyed. (Robert)
Nancy used her tearfulness as an indicator that she might be depressed, when consulting her GP. The quote below highlights that GPs may sometimes reflect this question back to the patient, who will then draw on their lay understanding to determine the nature of their experience:
Then one day I went in, I was so tearful and she said, ‘Do you think you are depressed?’ I said, ‘Well, I suppose I am a bit because I am crying’. (Nancy)
As noted in the literature, the term depression is used by researchers to cover a range of processes from low mood to psychiatric disorder (Beck et al., 2009). This is also mirrored in lay discourse and can cause frustration as the below participant highlights:
It really annoys me when people say, ‘I feel really depressed today’ because I think you have no idea what it feels like to be depressed, you’re feeling down, you’re having a bit of a down day, you’re having a bit of a bad time, you know, you are not having … feeling depressed. (Steph)
The variety within this theme suggests that it may be useful for GPs to draw out the patients’ conceptualisation if depression is brought up in consultations. As models for symptoms are likely co-constructed by the patient and the GP, it is also important to ensure GPs collaborate with patients to construct conceptualisations that are most likely to be of benefit, for instance, aligning with appropriate, evidence-based care such as self-management approaches as opposed to antidepressant treatment.
Ongoing anxiety
While this analysis has focused more prominently on depression, anxiety symptoms are also reported to be prevalent in primary care, with mixed depression and anxiety particularly common (Walters et al., 2011). The term ‘anxiety’ was used and discussed to a lesser degree than depression in our sample. When anxiety was used, it appeared that some participants were talking about a general anxiety, closer to clinical conceptions of generalised anxiety disorder (Ruiz et al., 2011). Patients drew on scales in order to describe ongoing low-level anxiety and also focused on physical symptoms:
If something crops up, and invariably something that I can’t control, um that can give me cause for anxiety then I will be anxious and I will go like that. Um, but generally speaking I’m not like that. Although um, I believe if we say the anxiety scale is zero to ten, ten being bad um, I believe that I’ve probably normalised a certain level of anxiety anyway, say about a three. So when I become anxious I, you know, I’m more likely to go to ten a lot quicker than someone else would because I’m already operating on three, which I’m perfectly happy operating on because I’ve normalised it at the end of the day. (Peter)
So I might just start off by asking you did you go to your GP to ask about a specific stressful experience or stress in your life?
Stress in my life more than an experience, just ongoing anxiety. Physical anxiety um, constricted muscles, tight jaw um, quite a high heart rate and just feeling anxious. Um, and that has gone on for years and years, maybe eighteen years. (Sheila)
I’m currently on medication for anxiety um, although it’s only sort of really … it only like really affects like palpitations, so it doesn’t affect, you know, it doesn’t sort of improve your thoughts or anything, it just literally affects heart palpitations. Um, so I’ve … but, yeah, I mean anxiety has sort of been, again, certainly within the last year or so, has sort of been quite up and that could be tied into the sort of stresses of my studying, but it’s sort of hard to know where that, you know, where that ties in. (Gemma)
Anxiety or feeling anxious occurred less often when discussing specific stressful life events and subsequent reactions, where terms such as stressed, frustrated and agitated were used more commonly. This suggests that participants used the term anxiety with a greater degree of specificity than the often ambiguous use of the term depression.
See Figure 1 for a schematic of terms used by participants. Terms are placed within overlapping spheres to illustrate possible relationships between the concepts arising from our analysis.
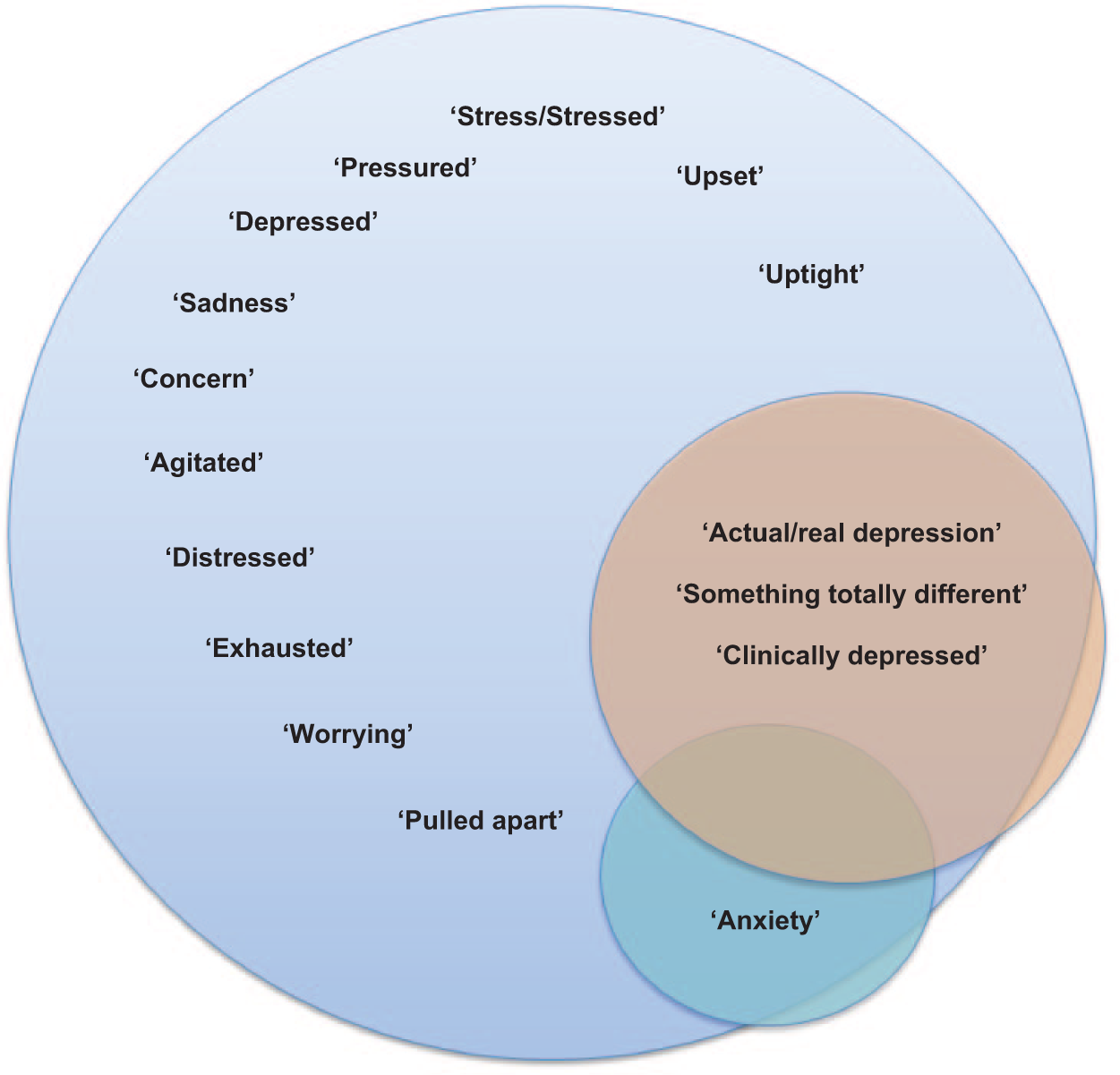
A schematic of terms used by participants.
General discussion
The majority of participants in this study described what appeared to be a relatively severe emotional experience, related to a perceived inability to cope with significant life stressors. A small number of participants focused on concern about affective states as their primary issue; these patients reported previous experience of treated depression or anxiety. Although some were unsure, patients often considered there to be a difference between their experience and how they conceptualised depression – as something that was phenomenologically distinct or as a mental illness. However, there was variation in their use of the term, with some seeming to use depression to refer to low mood. Anxiety was used less frequently. Where participants mentioned anxiety, they referred to underlying generalised symptoms.
Psychiatric models currently drawn on in primary care research (Kravitz et al., 2013; Kroenke et al., 2001; Mitchell et al., 2009) and recommended for practice (Arroll et al., 2010) often indicate disorder when the severity and duration of symptoms reach a predefined threshold and cause impairment. These models may fail to reflect the complexity in the multifaceted, context-driven narratives presented by patients or the subtleties of meaning inherent in terms presented. Participants in our sample readily described severe and ongoing symptoms relating to enduring contexts, causing impairment, yet were not diagnosed with depressive disorder by their GPs. This could be interpreted as under-detection (Kessler et al., 2002); alternatively, GPs could be appropriately questioning the applicability of such models with particular patients. Although rarely noted in the literature on depression in primary care, simplified unitary models of depression, for instance, are debated in the wider psychiatric literature (Nesse, 2007; Parker, 2000, 2005; Wakefield, 2007).
Similarly, disorder terms referred to in the literature that might be considered relevant for the majority of our sample include ‘subthreshold’ (Pincus et al., 1999), ‘subsyndromal’ (Lyness et al., 2007), and ‘mild’ (Baumeister, 2012) depression or ‘unspecified depressive disorder’ (APA, 2013). However, these concepts are rarely defined beyond a symptom count (e.g. fewer than MDD) and duration with some level of impairment. Without reference to aetiology or prominent psychological processes that may drive these ‘depression spectrum disorders’, it is difficult to determine whether or not these terms offer an accurate description of patients’ experience, and therefore whether they are likely to be helpful for both the patient and the GP. Certainly, the experiences of many of our participants were not ‘mild’, indicating this terminology may not map onto patients’ experience.
Participants often drew on theoretically coherent conceptualisations of their emotional experience. Going beyond symptom counts and further into the literature, there are many parallels between participants’ focus on the inability to cope and decades of stress research (Lazarus and Folkman, 1986); cognitive appraisals and coping are consistently shown to be key in distress/emotional processes (Gross and John, 2003; Skinner et al., 2003). Importantly, distinctions made by some participants between their experience and their concept of depression map directly onto definitions and guidance in the DSM-5, and theory proposed by researchers (Mulder, 2008; Nesse, 2007; Terluin et al., 2006; Wakefield, 2007). In prominent but rarely referenced sections of the manual, it is made clear that reactions to losses and common stressors, that occur in culturally expectable circumstances, despite appearing similar, are not mental disorder (APA, 2013: 20, 161). Rather, mental disorders such as depression are driven by dysfunctioning internal systems: affective, cognitive, developmental or biological (APA, 2013). Thus, severe emotional distress related to high levels of occupational pressure coinciding with parental terminal illness, for instance, may be coherently argued as ‘not actual depression’ although the impact for the patient may be both severe and disabling.
The application of expanded models of psychiatric disorder and psychological symptoms may provide helpful routes forward. As a starting point, propagating the full description of mental disorder from the DSM-5 may have an important effect, in particular, the notion that disorder is not simply indicated by the presence of symptoms or syndromes and their severity, duration, and functional impairment; context and circumstance also need to be considered in clinical judgements (APA, 2013). This necessitates more research to help clinicians identify core depressive disorder features that may more accurately distinguish between psychopathology and a stress response.
We have noted that the DSM contains statements outlining distinctions between distress and mental disorder. Unfortunately, it is extremely rare to see these sections acknowledged. Without considering context, the concerns of many may be justified, and the DSM can be seen to promote an atheoretical focus on de-contextualised symptoms, lack specificity and often lead to the over-identification of mental disorders (Dowrick, 2009, 2016; Horwitz and Wakefield, 2007; Mulder, 2008; Shorter, 2013; Wakefield, 2007). This is particularly the case for patients experiencing severe distress who may share many symptoms listed for MDD, despite not experiencing psychopathology.
For patients consulting with emotional distress that does not fit with full criteria for major depressive or generalised anxiety disorders, current interventions are limited. Antidepressants developed to treat a proposed biological basis of MDD may not be appropriate with regard to mechanisms and may have substantial and long-lasting adverse effects (Moncrieff, 2009). Low-intensity Cognitive Behavioural Therapy (CBT) may be of use, although these patients may find rationales regarding, for example, the cognitive triad (Beck et al., 2009) harder to relate to, particularly if they attribute the cause of their distress to an overt social or environmental stressor. In our sample, patients reported that GPs primarily offered reassurance, time off work or medication to help sleep; however, with limited options, GPs may label patients as depressed simply as a means of allowing access to broader range of treatment to a patient they see as in need. Developing low cost interventions grounded in patient experience that map onto expanded models of psychological symptoms is important (Muñoz et al., 2016). These could range from digital interventions to GP delivered micro-interventions (Moore et al., 2013) that demedicalise and point towards self-management strategies (exercise, behavioural activation). This would enable GPs access to a diverse range of options that more closely fit the nature of the symptoms and concepts presented by patients.
The following limitations should be considered with our work. The sample was relatively small and is therefore only representative of those patients consulting with emotional distress willing to discuss their experience in detail. Additionally, our sample was predominately White. Conceptualisations of emotional distress vary cross-culturally (Kokanovic et al., 2008); as such, our themes may have differed if we had sampled across range of cultural backgrounds. GPs’ conceptualisations are important, and this element was not covered in this article. Our group has forthcoming work that will include GPs’ perspectives. This is a reading of the data from the lead author’s (A.G.) perspective as a psychologist; thus, analysis has focused on psychological interpretations. If read at a sociological level, more emphasis may be placed on the agendas of patients and moral discourses around disorder. Nonetheless, we held regular cross-disciplinary data discussion meetings with M.S. (academic GP) and S.W. (allied health professional) from the outset of coding, as well as discussion meetings with the wider team, to ensure interpretations were cross-checked with the data from multiple perspectives.
To conclude, when individuals consult in primary care with concerns about their mental health, they enter complex territory. The present research landscape is composed of disorder terms used with multiple meanings, ‘subthreshold’ notions and definitions based on severity measures. These constructs can be difficult to assimilate with patient and GP perspectives in the clinical encounter. The triangulation of in-depth patient experience with robust psychological/psychiatric theory may provide novel frameworks for research and practice that lead to improved primary mental health care.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the National Institute for Health Research School for Primary Care Research (NIHR SPCR), grant number 162. The views expressed are those of the author(s) and not necessarily those of the NHS, the NIHR or the Department of Health.