
Abstract
Mental health care for older people is a significant and growing issue in Australia and internationally. This article describes how older people’s mental health is governed through policy discourse by examining Australian Commonwealth and South Australian State government policy documents, and commentaries from professional groups, advocacy groups and non-governmental organisations. Documents published between 2009 and 2014 were analysed using a governmentality approach, informed by Foucault. Discourses of ‘risk’, ‘ageing as decline/dependence’ and ‘healthy ageing’ were identified. Through these discourses, different neo-liberal governmental strategies are applied to ‘target’ groups according to varying risk judgements. Three policy approaches were identified where older people are (1) absent from policy, (2) governed as responsible, active citizens or (3) governed as passive recipients of health care. This fragmented policy response to older people’s mental health reflects fragmentation in the Australian policy environment. It constructs an ambiguous place for older people within neo-liberal governmental rationality, with significant effects on the health system, older people and their carers.
Introduction
Mental health problems are experienced across the lifespan. For older people (aged 65 years and over), mental health problems may develop late in life (such as dementia) or may have been present for many years (such as schizophrenia or bipolar disorder). Numbers of both types of mental health problems are rising across the globe, attributed to population ageing (Hendrie et al., 2014).
Different rates of mental health problems are reported for older people depending on the context. In a review of international literature (from 1988 to 2009), rates of depression in older people living in community dwellings were found to range from 6% to 20% (National Ageing Research Institute, 2009). In Australia, a review of administrative data to explore the prevalence and characteristics of people with depression in residential aged care (2008–2012) found symptoms of depression are reported in over half (52%) of permanent aged care residents and just under half (45%) of people entering aged care for the first time (Australian Institute of Health and Welfare, 2013). A study of older adults (aged 70 years or older) admitted as an emergency to a general hospital in the United Kingdom found a high prevalence of mental health problems in the sample population (Goldberg et al., 2012).
The provision of sustainable and effective mental health care for older people is a significant and growing issue in Australia and internationally. The way we respond to a social problem is arguably just as important as the problem itself, in that it ‘both sustains and frames the existence of a problem’ (Galitz and Robert, 2014: 182). While Australia has adopted similar ideas and strategies as other developed countries to address mental health and ageing in policy, local context shapes how these strategies are applied. Of particular relevance is a constitutional division in responsibility for health care in Australia, where the Commonwealth government is responsible for primary care, dental care, aged care, the education of the health workforce and pharmaceuticals. State and Territory Governments are responsible for managing the public hospital system, with greater responsibility for direct health-care delivery including mental health (Petrich et al., 2013). As such, governance of service delivery occurs over two levels contributing to different policy foci and agendas. Furthermore, Australian policy-makers experience issues of access arising from the distances to be covered by rural services. In South Australia, for example, this is reflected in a separate governance structure for rural health (Country Health SA). The discussion that follows uses Foucault’s concept of ‘governmentality’ as a theoretical framework for a policy analysis and demonstrates the varying ways in which mental health and ageing are problematised within the Australian policy context.
Governmentality, problematisation and discourse
Governmentality refers to the relationship between government and thought (Foucault, 1991) or the mentalities, rationalities and techniques of government (Rose, 1998). Analysis focuses on how to govern and the subjectivities or ideas about citizenship that these encompass; that is, on ‘who can govern, what governing is [and] what or who is governed’ (Gordon, 1991: 3). The term ‘government’ here describes ‘a form of activity aiming to shape, guide or affect the conduct of some person or persons’ (Gordon, 1991: 2).
Central to the analysis of governmentality is problematisation. Problematisations are ‘the everyday practices where conduct has become problematic to others or oneself’ and the attempts to ‘render these problems intelligible and, at the same time, manageable’ (Rose, 1998: 26). In relation to policy, what is problematised and how it is constructed as a problem reflect existing governmental rationalities, with policy solutions following from the manner in which the issue is constructed. Policy, from this perspective, ‘is not considered simply a response to existing social problems’; what is problematised is related to current ideas about citizenship and ‘postulated solutions are seen to frame “problems” in such a manner that the recommended interventions become self-evident’ (Henderson and Fuller, 2011: 188).
Older people’s mental health is formulated as a problem for government through discourse, defined as ‘practices that systematically form the objects of which they speak’ (Foucault, 1972: 49). Discourses create ‘regimes of truth’ (Foucault, 1980), which are acceptable formulations of, and solutions to, the problem. A policy analysis of older people’s mental health, therefore, involves exploring how the ‘problem’ is discursively produced and rendered governable.
Analysing policy representation through a governmentality lens offers a critical perspective of older people’s mental health. According to Dean (2002), through a governmentality analysis we can reveal the dissonance and disjunction between programmatic rationalities (philosophies, mentalities or theories) and their ‘effects in the real’. For example, in a paper exploring choice in health care decision-making for older people, Hicks et al. (2012) discuss the ways in which the notion of ‘choice’ functions to deflect the discussion away from differences between what health-care systems offer and clients’ needs.
In what follows, we critically examine Australian policy to explore the dissonance between programmatic rationalities for the governance of older people and mental health and their ‘effects in the real’. This analysis is timely given the proliferation of crisis discourses in politics and the media in relation to the ‘ageing population’, with concerns about state spending in the context of anticipated increases in health care costs heightened as a result of the global financial crisis (Jacobs, 2013). This is likely to have had a significant effect on how older people and mental health are problematised in policy both in Australia and internationally (Neilson, 2009).
Methods
A discourse analysis was conducted following Arribas-Ayllon and Walkerdine’s (2008) methodological guidelines for conducting Foucauldian discourse analysis. The guidelines were developed in such a way as to ‘avoid delimiting a Foucauldian analytic to a set of formal principles but offer some methodological signposts’ (Arribas-Ayllon and Walkerdine, 2008: 98). The guidelines are presented in Table 1.
Methodological guidelines for conducting Foucauldian discourse analysis (Arribas-Ayllon and Walkerdine, 2008: 98–99).
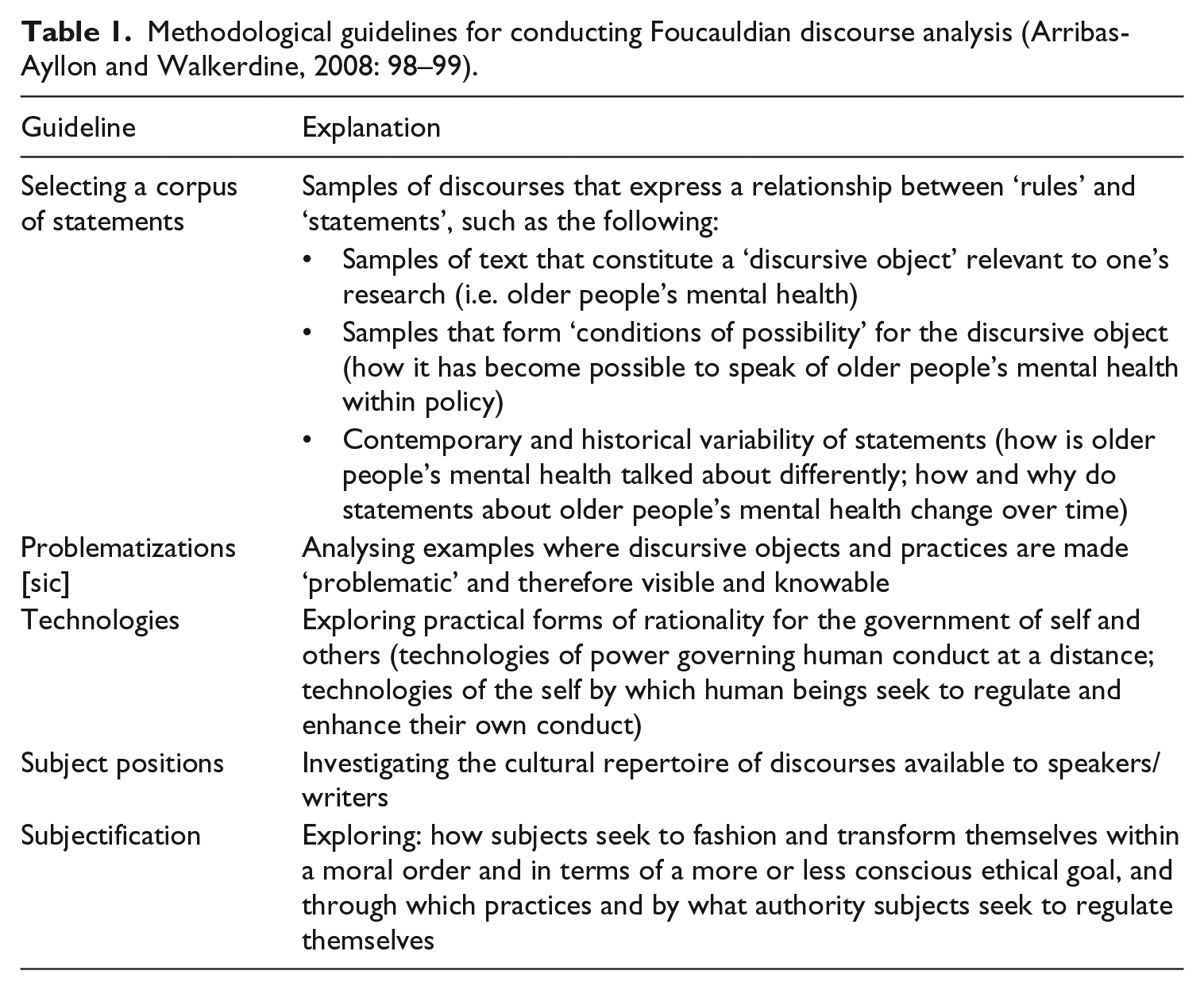
A variety of policy-related texts were selected that constitute the discursive object of ‘older people’s mental health’. An online search of websites for the Australian Department of Health and Ageing and the Department of Families, Housing, Community Services and Indigenous Affairs, in addition to the South Australian Department of Health, was conducted. Health, mental health and aged care policy documents published by Commonwealth and South Australian Governments between 2009 and 2014 were collected for analysis. The starting point of 2009 was selected because this was the year the revised National Mental Health Policy was released. This is a key mental health policy and the basis for the most recent national mental health plan (Fourth National Mental Health Plan). The inclusion of both Commonwealth and State government policy documents was necessary because of the division of constitutional responsibility for health care. South Australia was chosen as the case study for State-based policy because it is one of only two Australian States that provides mental health services exclusively focused on older people.
A Google search was undertaken using the terms ‘mental health’, ‘policy’ and ‘older people’ to obtain commentaries from professional groups, advocacy groups and non-governmental organisations in Australia. These documents contribute to the evolution of policy through submissions to government, in addition to representing how the ‘problem’ of older people and mental health can be thought about differently (Bacchi, 2009). Their inclusion allows the analysis of the broader cultural repertoire of discourses available to speakers/writers and the contemporary and historical variability of statements (Arribas-Ayllon and Walkerdine, 2008).
The texts were analysed to explore the discourses through which older people’s mental health is problematised and policy solutions – the technologies, subject positions and subjectification – underpinned by these discourses. The initial analysis was conducted by C.O. This analysis was presented to the rest of the research team and was discussed and refined during research team meetings.
Results
A total of 22 government documents were identified across the areas of mental health, aged care, health care, primary health care and rural and remote health (see Table 2), including 15 Commonwealth and seven South Australian policy documents. As Table 2 indicates, older people and mental health are absent from a number of policy documents and only minimally referenced in key Commonwealth documents relating to aged care and mental health, with no policy solutions or actions offered. This may reflect a lack of responsibility for service delivery in this area. The Productivity Commission report Caring for Older People identified policy solutions within the document, but action to address mental health care for older people was not included in the executive summary report (the Productivity Commission is the Australian Government’s independent research and advisory body on a range of issues affecting the welfare of Australians).
Problematisation of older people and mental health.
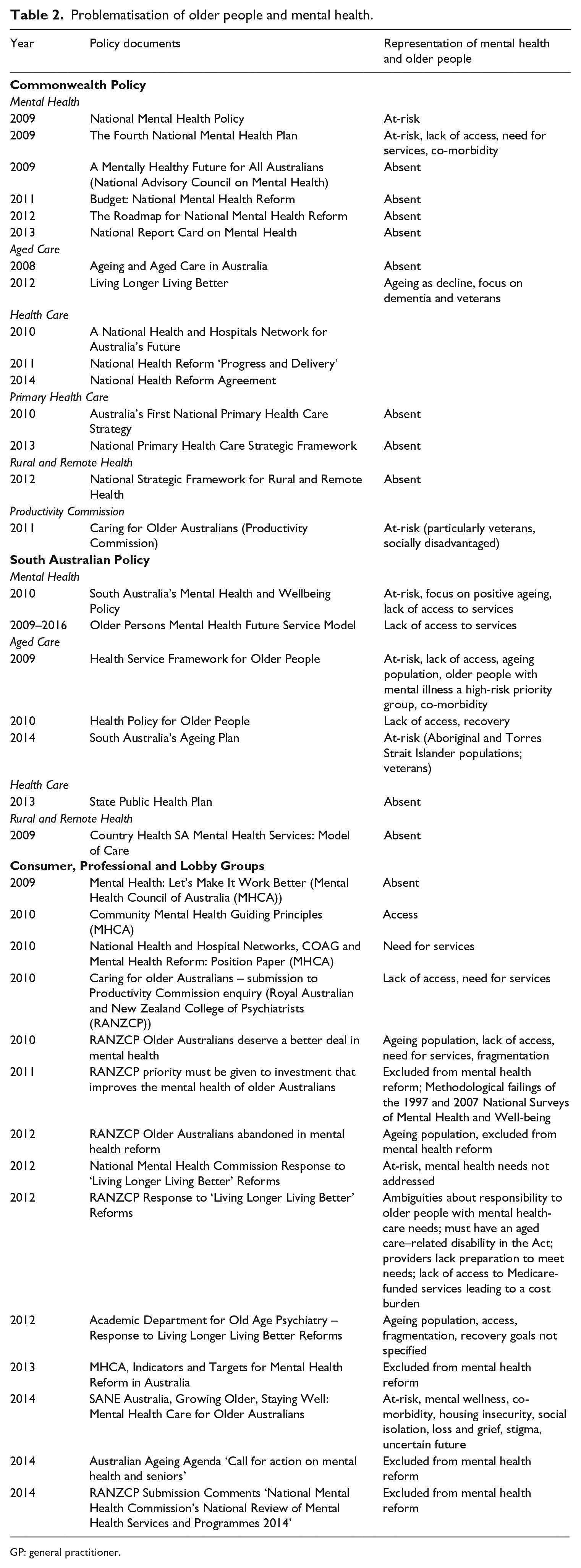
GP: general practitioner.
Of the seven South Australian policy documents, older people are referenced in relation to mental health in two specific mental health documents (South Australia’s Mental Health and Wellbeing Policy and the Older Persons Mental Health Future Service Model) and three aged care documents (Health Service Framework for Older People, Health Policy for Older People and South Australia’s Ageing Plan). The more detailed approach in South Australian documents may reflect the responsibility State governments have for direct service delivery of specialist mental health services.
A total of 14 documents from professional groups, advocacy groups and non-governmental organisations were identified. Of these, ten addressed the issue of older people and mental health specifically as the key focus of the document and three addressed older people and mental health as part of broader discussions about mental health care in Australia. A key document of the Mental Health Council of Australia (Mental Health: Let’s Make It Work Better) did not mention older people.
The problematisation of older people and mental health: discourses
The analysis revealed three interconnected discourses through which mental health and older people are problematised in Australian policy; namely ‘being at-risk’, ‘ageing as decline and dependence’ and ‘healthy ageing’. We begin with a description of the discourses, followed by a discussion of three policy approaches to addressing the ‘problem’ of older people and mental health that are underpinned by these discourses.
Being at-risk
The dominant discourse through which the ‘problem’ of older people and mental health is represented is one of ‘being at-risk’. Although older people and mental health are rarely mentioned in Commonwealth policy, where they are mentioned the policies identify groups of individuals deemed to be at increased risk of mental health problems and, therefore, requiring targeted risk management. For example, both the National Mental Health Policy and Fourth National Mental Health Plan note that certain life stages, including ageing, may be associated with increased risk. The Plan includes discussion about the need for coordination between primary care and specialist mental health services in the community, again with reference to older people. In addition, the Plan discusses the need for early intervention and a collaborative whole-of-government approach to managing risk so that service systems are able to respond to the needs of people of all ages.
A risk discourse is also evident in South Australian policy, where mental health policy emphasises the importance of understanding and addressing the increased risks of mental illness in certain population groups, including older people (South Australia’s Mental Health and Wellbeing Policy). South Australia’s Ageing Plan, Health Policy for Older People and Health Service Framework for Older People state that older people are at increased risk of mental health problems and dementia. Specific risk factors are not identified in South Australia’s Mental Health and Wellbeing Policy, with older people simply referred to as being ‘at-risk’, while the Health Service Framework for Older People identifies risk factors of social isolation and experiencing grief and loss. Discourses of risk are also prominent in commentaries from professional groups, advocacy groups and non-government organisations.
Ageing as decline/dependence
Alongside a representation of older people as being at-risk is one where ageing itself is represented as the problem to be addressed in policy. This representation is underpinned by a discourse of ageing as decline and dependence. An appendix of the Fourth National Mental Health Plan focusing on ageing discusses the problem of an increased proportion of older people in the population. Older people are represented as being at increased risk of mental and physical health problems, with co-morbidity a particular issue. They are also represented as being reliant on family and friends, as having difficulty with mobility and as accessing specialist psychiatric services at lower rates than younger people.
The discourse of ageing as decline/dependence can also be seen in the Commonwealth Living Longer, Living Better Reform to the Aged Care Act. The reform responds to concerns about a rapidly ageing population and the need for changes in the current aged care system to keep up with future demand. The reform refers to older people and mental health in the provision of additional Home and Community Care (HACC) funding to older people with dementia. The purpose of HACC funding is to ‘provide a comprehensive, coordinated and integrated range of basic maintenance and support services for frail aged people and those with disabilities so that they can reside independently in their own home’ (Vecchio, 2013: 356).
A discourse of ageing as decline/dependence also occurs in South Australian policy documents in discussions of the complexity of health problems faced by older people, increased demand on the health system from an ageing population and reduced access to primary health care services creating an increasing burden on emergency departments. This discourse is less evident in commentaries from professional groups, advocacy groups and non-governmental organisations, aside from identifying a need to recognise older people as a ‘distinct and vulnerable’ and a ‘special needs’ group in the Aged Care Act (National Mental Health Commission Response to ‘Living Longer Living Better’ Reforms; RANZCP Response to ‘Living Longer Living Better’ Reforms).
Healthy ageing
The final discourse identified is ‘healthy ageing’. This discourse was only found in South Australian documents, where there is a differentiation between the general population of older people and older people with a mental illness. A healthy ageing discourse was identified in policy solutions addressing the general population of older people represented as ‘at-risk’ of mental health problems. In particular, services aim to target at-risk groups of older people and support them to maintain their physical and mental health through primary health care focused around healthy ageing strategies, prevention and early intervention (South Australia’s Mental Health and Wellbeing Policy). This approach is a key principle of South Australia’s Health Service Framework for Older People.
Policy approaches to the ‘problem’ of older people and mental health: technologies, subject positions and subjectification
The policy approaches to the ‘problem’ of older people and mental health reflect a neo-liberal philosophy of governance that emphasises the role of economic markets, rather than government intervention, to govern social and economic life (Rose and Miller, 1992). This is the main form of rationality (technology) for the government of older people and mental health in Australian policy. In what follows, we introduce and describe neo-liberalism as a technology of government, and the subject positions and subjectifications associated with it, followed by a discussion of the ways in which neo-liberalism is evident in Australia’s policy response to mental health and older people.
Neo-liberalism rose to prominence in the 1970s as a dominant policy framework in a number of countries, such as the United States, the United Kingdom and China, both voluntarily and as a response to the pressures of globalisation (Harvey, 2005). Market-based health sector reforms have been implemented internationally through the promotion of neo-liberal policies by multilateral and bilateral organisations such as the World Bank, with a range of negative implications particularly in terms of access to care among the poorest (Lister and Labonte, 2009).
While there is no single form of neo-liberalism (Brenner et al., 2010), when applied to governing health care in contemporary Western democratic societies, neo-liberalism is generally characterised by the government of individuals as rational, active consumers of health care, responsible for maximising their own health and well-being. In Australia, this understanding of the consumer of aged care services has contributed to the marketisation of these services evident in increasing licensing of private-for-profit service providers, competitive tendering for service provision, enabling consumers to purchase service packages and use of personal funds to purchase higher quality services in the community and increasingly within residential aged care (Brennan et al., 2012; Meagher and Szebehely, 2013). Underpinning this strategy is the belief that the creation of markets will ensure quality through consumer choice between competing services and greater consumer control of these services (Brennan et al., 2012).
A second component has been the emergence of the notion of ‘active’ ageing (also termed ‘healthy’ or ‘positive’ ageing) as a neo-liberal policy response to ageing populations. Active ageing refers to ‘individual or collective strategies for optimising economic, social and cultural participation throughout the life course’ (Lassen and Moreira, 2014: 33). Yet, as Moulaert and Biggs (2012) discuss, there has been a shift from broader concerns with health, well-being and quality of life in early conceptualisations of active ageing to a narrow, neo-liberal focus on the more restrictive (economically) productive dimensions.
The notion of active ageing is not pervasive in policy. As Powell (2014) has discussed, the relationship between older people and the state has been reconfigured within a neo-liberal governmental rationality in such a way as to construct an ambiguous place for older people where they are viewed as both a resource (active citizens participating in work/work-like activities) and as a problem (in terms of poverty, vulnerability and risk). As a resource, they are governed as ‘independent self-managing consumers’; when viewed as a problem, they are governed as ‘dependent and unable to commit to self-management’ (Powell, 2014: 109). These are the forms of subjectification associated with the problematisation of older people and mental health in Australian policy.
Thus, as Clarke (2005: 457) has identified, neo-liberalism involves diverse strategies ‘that differentiate the population and apply different practices to the “target” groups’ according to varying risk judgements. Neo-liberalism is associated with divisions based on a capacity to manage risk between ‘active citizens’, who accept responsibility for managing lifestyle risk, and ‘“targeted populations” … who require interventions [emphasis in original]’ (Dean, 1999: 167). The emergence of an economically reformulated ‘active ageing’ discourse in neo-liberal policy means that ‘no aspect of life should be excluded except perhaps the encroachment of physical and mental incapacity where the consumption of aged care takes over’ (Moulaert and Biggs, 2012: 34).
This diversity was evident in our study where three policy approaches were identified through which the ‘problem’ of older people and mental health is governed.We identified that older people are governed as absent/unimportant, as passive recipients of care or as active consumers through the interconnection of discourses of risk, of ageing as decline/dependence and of healthy ageing. These are the subject positions associated with the problematisation of older people and mental health in Australian policy. The three policy approaches, and the dissonance and disjunction between a neo-liberal programmatic rationality and its ‘effects in the real’ in relation to these approaches, are now discussed.
Commonwealth policy ‘absence’
The analysis of Commonwealth policy reveals that while there is a general recognition that older people experience mental health problems and that they have specific service needs, they are absent from policy solutions and priority actions. The RANZCP has discussed this absence in a number of position papers and submissions to the government. Most recently, the RANZCP (2014) stated, ‘Reform and funding of mental health services for older people continues to be neglected, with older people at significant risk of ongoing decline in mental health care’ (p. 4). The RANZCP and organisations such as the Mental Health Council of Australia, the National Mental Health Commission, the Academic Department for Old Age Psychiatry and the Australian Ageing Agenda have all expressed concern that older people with mental health problems have been ignored and overlooked in mental health and aged care reform.
The RANZCP (2011, 2012) describes the inadequacy of planning for the mental health needs of older people that is evident in the exclusion of older people from aspects of mental health reform. This includes the exclusion of older people with dementia and those living in residential aged care facilities from increased access to mental health care through Medicare reimbursement. They also note the absence of priority actions and recommendations for older people in documents such as the Fourth National Mental Health Plan, the 2011 Productivity Commission Report into Aged Care and the 2011 Independent Mental Health Reform Group’s ‘Blueprint’ for mental health services in Australia. There are no preliminary performance indicators related to older people’s mental health, with mental health of people aged 65 years or older explicitly excluded from other measurements of success, in The Roadmap for National Mental Health Reform 2012–2022.
The relative absence of older people reflects an interconnection of discourses of ageing as decline/dependence and of risk, whereby this risk is not afforded priority in policy. Instead, there is a focus on younger people as the ‘target’ risk group in the strategies and priorities for action for mental health in Australia (Roberts, 2011). The focus on younger people can be seen in the priority areas and indicators outlined in the Fourth National Mental Health Plan, which focus on young people and in particular on increasing the participation of young people with mental illness in education and employment.
The focus on young people has been attributed to the influence of a 2011 report by a prominent Australian of the Year Patrick McGorry, who promotes early intervention between the ages of 12 and 25 years as the most effective way to limit the onset or severity of mental illness (Boag, 2013). Another important factor relates to the 1997 and 2007 Australian National Surveys of Mental Health and Well-being, which provide important statistical information on the rates of mental health problems, and therefore mental health risk, in the Australian population. These surveys have been criticised for using methods that are unsuitable for older people and for excluding older people with dementia or living in residential aged care, thus under-reporting rates of mental health problems in older people (RANZCP, 2011).
The Commonwealth policy ‘absence’ is also reflective of broader concerns about ageism and taken-for-granted assumptions about ageing. This is particularly the case in Western society where a bio-medicalised lens unproblematically associates ageing with the body’s decline (Phelan, 2011) and an economically determined policy perspective positions older people as ‘unproductive and a burden on society as a whole’ (Biggs, 2001: 306). Ageism has been described as ‘a prevalent social attitude that overvalues youth and discriminates against the elderly’ (McAllister and Matarasso, 2007: 149), an attitude that is evident in Commonwealth mental health policy that views the ageing population as a problem and focuses policy action on young people. As Phelan (2011: 898) points out, ageism in health care is evident in views of health deterioration ‘as part of the “normal” ageing process, resulting in a fatalistic attitude towards what intervention will achieve’. The lack of policy solutions for older people suggests an inevitability of decline in old age and that money is better spent on minimising disability in young people to enable them to participate in education and employment, leaving older people without the necessary services to support their care needs.
Active consumers
In contrast to the Commonwealth policy absence, South Australia’s policy response differentiates between two target groups of older people – the general population of older people who are at-risk of developing a range of physical and mental health problems and the high-risk priority group of older people with mental illness. We begin with a discussion of the general population of older people, who are governed through the interconnection of discourses of ‘risk’ and ‘healthy ageing’ as active consumers of mental health care and individually responsible for addressing risk.
The policy solution involves the provision of integrated primary health care services that offer support and interventions to assist older people to modify risk factors and maintain their physical and mental health and their social connectedness (Health Service Framework for Older People). A priority in South Australia’s Mental Health and Wellbeing Policy is to integrate and co-ordinate mental health services for older people across the primary health, aged care and specialist mental health sectors; integrated care is also emphasised in documents by professional groups, advocacy groups and non-governmental organisations. In South Australia, this model involves community health centres led by general practitioners (GPs) as the first point of contact with the health-care system, with an emphasis on illness prevention and early intervention for at-risk older people. This reflects neo-liberal concepts of governance through reliance on private services, such as GPs and privately funded mental health professionals, to provide many aspects of care (Henderson, 2005).
Targeting mental health care towards at-risk individuals places the responsibility onto the individuals themselves and those who care for them, such as family, to seek care, modify risk factors and maintain their mental health and thereby achieve ‘healthy ageing’. Thus, the Health Service Framework for Older People (2009) states,
South Australian GP Plus Health Care Centres … will increasingly help older people take control of their health care, stay healthy and out of hospital. These centres and a range of other primary health care services will promote opportunities for older people to maintain and enhance their wellbeing and independence … (p. 13)
This will be done through, for example, an increased focus on healthy physical and mental activity, access to annual health checks including physical and mental health reviews, and grief and loss counselling, with the purpose of ‘helping older people reduce or manage risk factors for the onset of mental illness’ (Government of South Australia, 2010: 12). Through this approach, the older person becomes an active subject of mental health policy, having personal responsibility for their mental health and well-being.
This policy approach is based on a range of assumptions about the effectiveness of GPs as the first point of contact for mental health problems and the willingness of older people to discuss mental health problems with their GPs. Yet, this may not reflect the reality of how older people and their GPs address mental health problems. The RANZCP (2010) has commented that GPs may not have the skills to manage mental illness. The use of GPs as the first point of contact is particularly problematic with older clients. GPs and other primary care practitioners reportedly view depression as ‘understandable’ and ‘justifiable’ in older people due to loneliness, social isolation and reduction in function (Burroughs et al., 2006). Older people appear to share this view and consider depression not to be a legitimate illness to take to GPs (Burroughs et al., 2006). Thus, GPs may not be best placed to respond to older persons’ help seeking around mental health, calling into question the notion of older people as active participants, capable and willing to seek help from a responsive system.
Passive recipients of care
In the Health Service Framework for Older People, there is a separate section discussing ‘Older people with mental health conditions [mental illness] as a high-risk priority group’. For this group, risk discourses interconnect with discourses of ageing as decline/dependence in a different way to that identified in Commonwealth policy, where the interconnection leads to older people being excluded. By contrast, the interconnection of the two discourses here results in older people who are labelled as high-risk being governed as passive recipients of targeted interventions. This occurs through reference both in the policy and non-policy documents to increased demand for mental health care in an ageing population with pre-existing mental illness and mental illness first developed in later life, and the difficulty for this group in achieving optimal management of their health due to co-morbidity.
The primary problem identified for older people with mental illness is one of lack of access to specialist health services. The solution is presented as one of increasing service availability, particularly through facilitating access to specialist services (e.g. through co-location of Older People’s Acute Assessment Services and Older People’s Acute Medical units in general hospitals with acute mental health units to facilitate consultation and liaison, Health Service Framework for Older People). The Older Persons Mental Health Future Service Model, which defines the scope and actions for future service delivery across South Australia, similarly focuses on ensuring adequate access to specialist mental health services in a range of locations, including the community, general hospitals and residential aged care.
This representation of the problem of older people with a mental illness assigns them a passive subject position where they are embedded in and passively dependent on the care and support provided by mental health professionals (and carers). An indication of this passive subject position is the lack of reference to the mental health recovery framework; this concept, widely referenced in relation to other at-risk populations (particularly young people), emphasises the active role of the consumer in achieving personal recovery goals (Drake and Whitley, 2014). Furthermore, policy solutions are individualised and oriented around early intervention, with no discussion of illness prevention or mental health promotion strategies, reflecting a fatalistic attitude of inevitable deterioration in older people (Phelan, 2011), discussed above. This fatalism contrasts with the representation of older people without mental illness who are viewed as having the capacity and responsibility for managing their own health and well-being through undertaking screening and self-management activities.
Discussion
Reading Australian Commonwealth and South Australian policy through a governmentality frame supports an analysis that sheds light on older people as governed by discourses of ‘being at-risk’, ‘ageing as decline and dependence’ and ‘healthy ageing’. The result is a fragmented policy approach to addressing the ‘problem’ of older people and mental health, reflective of a fragmented policy environment in Australia and underpinned by a neo-liberal governmental rationality.
The discourses identified in this analysis can be seen in policy internationally, particularly the emergence and proliferation of discourses of active/healthy ageing. Active/healthy ageing was promoted to challenge assumptions about negative views of ageing and to facilitate the ongoing social and political engagement of older people. With growing concerns about the capacity to support ageing populations, the concept was adopted and reformulated within neo-liberal policy internationally (Moulaert and Biggs, 2012). What is interesting in our analysis is the continuity of passive ageing and negative views of older people as unproductive alongside the emergence of active/healthy ageing in Australian policy. In particular, three policy approaches were identified through which the ‘problem’ of older people and mental health is governed. Older people who are considered able to commit to a market approach to mental health are governed as responsible, active citizens, expected to take personal responsibility and self-manage risks to their well-being to ensure their ongoing productivity. When discourses of risk and ageing as decline/dependence interconnect, older people are governed as a problem and either excluded from policy solutions or governed as passive recipients of health care. It would be worthwhile exploring the extent to which international policy reflects a similar fragmented approach.
This governmentality analysis has demonstrated the consequences (‘effects in the real’) of a neo-liberal approach to older people and mental health, both on the health system itself and on older people and their carers. In particular, the expectation that older people can and should take personal responsibility for managing risks places the burden of care onto older people and their carers, while structural factors, such as stigma and social determinants of mental health, are not adequately addressed (Henderson, 2007). A number of social determinants of mental health problems have been identified, such as poverty, housing instability, social exclusion or isolation and poor access to quality health care, and addressing these could have a substantial public health impact (Shim et al., 2014). A consequence for older people who are considered unable to meet the commitment to the market, either through assumptions about their (economic) value or about the capacity of older people with mental illness to be active participants in their care and recovery, is that they are governed in ways that ‘are often oppressive and impersonal’ (Powell, 2014: 112). This includes the failure to adequately fund mental health services for older people and a failure to address mental health recovery.
A further consequence is that ageist views about older people’s value and capacity are reinforced in an economically driven political landscape that values participation in work and work-like activities above other forms of social engagement (Moulaert and Biggs, 2012), justifying the exclusion of older people from mental health reform. Finally, as Moulaert and Biggs (2012) have discussed, the focus on older people’s participation in work/work-like activity means that ‘mature identity comes to consist of “more of the same” in lifecourse terms, and diversity of identity with all its promise of alternative forms of social engagement enabled by a long life, will be lost’ (p. 38).
Ultimately, the fragmentation evident in the problematisation of mental health and ageing in Australian policy leads to a dispersed and convoluted system that is difficult to navigate, providing a significant barrier to addressing the ‘problem’ of older people and mental health. Difficulties in determining where the person ‘fits’ in a fragmented policy environment, and whether older people are ultimately worthy of service provision, are likely to make it easier for health professionals to shunt older people between services. Difficulties in navigating the system also lead to older people being housed in residential facilities where their mental health needs may not be adequately understood or addressed due to lack of training in how best to support mental health or manage patients with a mental illness (Moyle et al., 2010).
Obtaining policy consensus on the ‘problem’ of mental health and older people will greatly contribute to more effective policies for this group of people. A first step may be, as Moulaert and Biggs (2012) suggest, to shift the focus towards ‘desired’ rather than ‘active’ ageing. This could enable the recognition of a multiplicity of mature identities and the valuing of older people and their contributions beyond an economic imperative.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research reported in this paper is a project of the Australian Primary Health Care Research Institute, which is supported by a grant from the Commonwealth of Australia as represented by the Department of Health and Ageing. The information and opinions contained in it do not necessarily reflect the views or policy of the Australian Primary Health Care Research Institute or the Commonwealth of Australia (or the Department of Health and Ageing).