
Abstract
This study aimed to identify guiding principles to underpin assessment and diagnosis of autism to improve the quality, consistency and accuracy of services provided to individuals and their families. An online survey and focus groups were used to capture community perspectives of members of the Australian autistic and autism communities. A total of 871 individuals participated across the research activities, including autistic individuals (n = 253), parents of autistic individuals (n = 344), practitioners (n = 325) and members of organisations with an interest in the assessment and/or diagnosis of autism (n = 115). Three overarching themes, encompassing 15 codes, representing the principles that should underpin practice across the assessment and diagnostic process were developed (a) placing the person at the centre of the process; (b) understanding and valuing the whole person and (c) improving quality and access. Assessment and diagnosis for autism should go beyond diagnostic decision-making to include understanding of individual needs and identifying support pathways. The principles identified serve as a first step to guiding practitioners in their approach, ensuring they work in ways that promote best practice, reflect the perspectives of autistic people and engender meaningful outcomes for individuals and families that are independent of receiving a diagnostic label.
Lay Abstract
This study looked to identify principles of practice that could help make autism assessments and diagnoses better for autistic people and their families. To do this, the researchers asked people from the autism community in Australia to share their thoughts through an online survey and focus groups. A total of 871 people took part. This included autistic adults, parents of autistic children, professionals like psychologists and speech pathologists and people from autism-related organisations. From what people said, three main ideas stood out: (a) putting people at the centre of the process, (b) looking at the whole person and (c) improving quality and access to services. The study found that getting a diagnosis is just one part of the process. It is also important to use the assessment to help people understand themselves better and find the right support. The principles highlighted in this study can help guide professionals to do a better job when assessing autism. They encourage practices that are respectful, person-focused and based on what autistic people and their families say is important. This can lead to better outcomes for everyone, no matter whether a diagnosis is given or not.
Autism is a lifelong neurodevelopmental condition with a highly heterogeneous presentation (American Psychiatric Association [APA], 2022). Autism-related characteristics and individual strengths, challenges and support needs can vary substantially both between, and within, individuals. While the diagnostic label in and of itself can be informative, it is not sufficient on its own to inform individual priorities and pathways for support. Rather, a comprehensive assessment of functional strengths and needs provides the foundation for individualised, strength-based planning for supports where relevant, irrespective of diagnostic outcome (Lord et al., 2022). However, the process, quality, consistency and accuracy of assessment and diagnostic approaches are highly variable in practice. Moreover, it has become increasingly acknowledged that the preferences of the autistic and autism communities should be a key factor in guiding the approach to assessment and diagnosis (Lord et al., 2022; Penner & Lai, 2023). Indeed, more broadly, the integration of the best available research evidence and clinical expertise with the individual preferences of the client is the cornerstone of evidence-based practice (Sackett et al., 2000). In this study, we explored community perceptions of how the assessment and diagnosis process could be improved within the context of current diagnostic criteria (i.e., Diagnostic and Statistical Manual of Mental Disorders [5th ed.; DSM-5], International Classification of Diseases [ICD]-11).
Currently, autism is diagnosed based on observation and/or reports of behavioural and developmental indications (APA, 2022). As a result, the quality, consistency and accuracy of assessment are determined in large part by the practitioners involved in the assessment and the context within which they operate. This includes considerations regarding (a) the number, qualifications and competencies of practitioners involved, (b) the time and financial costs to individuals and families and (c) the availability and selection of culturally appropriate assessment tools, which can all impact the outcomes of assessment, including the clients’ experience (Crane et al., 2018; de Broize et al., 2021; Gerlach et al., 2022; Lilley et al., 2019). It is concerning, therefore, that recent reviews examining the range of experiences and perspectives of people going through the assessment and diagnostic process, globally and across the lifespan, have identified that many autistic adults and parents of autistic children experience distress and dissatisfaction with the process (Small & Belluigi, 2023; Wilson et al., 2023). The often negative, deficit-focused approach to assessment and the impact of this on people’s wellbeing and feelings of not being believed or having concerns validated have emerged as key barriers and determinants of dissatisfaction in the assessment process (Lewis, 2017; Wilson et al., 2023):
Nobody wants their negative side highlighted all the time. (Wilson et al., 2023, referring to a quote in Crane et al., 2018, p. 3766) [The therapist’s] continual refusal to even consider ASD as a contributing factor left me feeling pigeon-holed. Like he was more interested in fitting me into the category he wanted than actually listening to me and respecting my own thoughts and feelings on the issue. (Lewis, 2017, p. 2417)
For practitioners, a lack of competency, knowledge and training, as well as a lack of time and under-resourcing, have been identified as their key barriers (Freeman & Grigoriadis, 2023; Howes et al., 2021).
This research investigating client and practitioner experiences of the assessment and diagnostic process highlights the existing gaps between current practice and what research and the autistic and autism communities consider best practice. Practice guidelines are intended to set a standard for best practice, informed by the best and most recent evidence available. However, approaches and standards of practice vary across countries and continents (Lord et al., 2022). As such, it is important to understand stakeholder experiences within specific countries, and their associated political and social contexts, to inform best practice recommendations for autism assessment and diagnosis within that country.
In Australia, which was the focus of the present study, autism has been a formally recognised diagnosis since 1980, when the third edition of the Diagnostic and Statistical Manual (APA, 1980) was published. Like many other countries, the number of individuals with an autism diagnosis has increased over time, with current estimated prevalence rates of autism in Australia comparable to global estimates at approximately 1%–4% (May et al., 2017, 2020; Zeidan et al., 2022). While childhood diagnoses predominate, current trends also indicate increasing rates of adulthood diagnoses (Australian Institute of Health and Welfare, 2017; Huang et al., 2020). The National Guideline for the assessment and diagnosis of autism spectrum disorders in Australia (referred to herein as the ‘Guideline’), which was first published in 2018 (Whitehouse et al., 2018) and approved by the National Health and Medical Research Council, recommends that the process of assessment include a comprehensive needs assessment (combining a medical evaluation and assessment of functioning) and diagnostic evaluation when relevant, with referral to supports made at any time irrespective of diagnostic outcome.
Recommendations in the 2018 Guideline were developed through an evaluation of existing international evidence paired with comprehensive community consultation in Australia that included representation from the autistic and autism communities. A notable aspect of this guideline, that distinguished it from others at the time (National Institute for Health and Care Excellence [NICE], 2011, 2012; New York State Department of Health, 2017; New Zealand Ministries of Health and Education, 2016), was the inclusion of recommendations relating to Guiding Principles, in addition to specific recommendations for aspects of the assessment and diagnostic process. These included that assessment and diagnostic services should be evidence-based, individual and family centred, reflect a holistic framework, be strength-focused, promote equity and reflect a lifespan perspective. Theoretically, while specific recommendations regarding aspects of assessment and diagnosis may vary between countries to reflect different cultures, contexts and workforce characteristics, guiding principles may have more universal utility and relevance. Therefore, exploring community views regarding the principles that should underpin accurate, safe, timely, appropriate and accessible assessment and diagnostic services in Australia has the potential to inform efforts to improve the same services internationally.
The 2018 Guideline, which was updated in 2023 (Goodall et al., 2023), provided an opportunity to undertake a comprehensive community consultation process regarding the assessment and diagnostic process in Australia. The Guideline Development Group consulted with members of the autistic and autism communities to explore their experiences, views and preferences regarding the assessment and diagnostic process, including the overarching principles that should guide practice. The purpose of this article is to share the findings in relation to the Guiding Principles that emerged from the consultation process, thus informing efforts locally and internationally to improve the quality and experience of assessment and diagnostic services provided to individuals and their families.
Method
Design
A qualitative approach employing an online survey and focus groups and the Framework method of analysis (Gale et al., 2013) was used to explore community experiences, views and perspectives regarding the autism assessment and diagnostic process in Australia. The study was co-designed, with members of the research team representing a variety of perspectives including as autistic individuals, parents and family members of autistic children, practitioners and researchers. Ethics approval was obtained from the Griffith University HREC (ref no: 2022/780).
Participants
Recruitment
Participants were recruited primarily through an email distributed via the mailing list (n = 25,432 recipients) of the organisation that commissioned the research (Autism CRC), with advertisements also shared on social media channels (Twitter, Facebook). The research group also shared the invitation to participate with (a) 39 organisations that had previously provided feedback on the development of a recent separate guideline (Trembath et al., 2022) and (b) 10 organisations that support or represent Aboriginal and Torres Strait Islander Peoples. In addition, the research team and individuals who served as members of a broader Reference Group to support the update of the Guideline were encouraged to advertise the community consultation activities through their organisations/members, professional networks and social media channels where relevant.
All relevant stakeholders across the autistic and autism communities were eligible to participate in an online survey, including autistic people of any age (with or without a formal diagnosis); parents, caregivers and family members of autistic individuals; practitioners involved in assessment and/or diagnosis of autism; members of organisations/bodies/groups that have an interest in the assessment and/or diagnosis of autism; and any other relevant stakeholders (e.g., informal support people, researchers, educators). Where autistic individuals under the age of 18 participated, they were required to discuss their participation with a parent/caregiver who provided consent on their behalf. A total of 810 participants provided informed consent to participate in the online survey. Among those, five people provided informed consent; however, they indicated in response to the final survey question that they would not like their information to be used. A series of focus groups was also conducted with autistic adults, family members and practitioners who were 18 years or over and resided in Australia. A total of 246 registrations for 96 focus group positions (i.e., 12 slots across 8 focus groups) were received. Of these, 68 participants attended their allocated focus group. One participant was excluded from analysis following their participation in a focus group, as they did not meet the criteria for inclusion (i.e., it became apparent during the focus group that they were not an Australian resident, as previously indicated in their registration). Of the remaining 67 participants, 66 provided some details about themselves and their child(ren), where relevant.
Demographics
The study included 871 participants (online survey n = 805, focus groups n = 66). Participants brought a range of (and often, multiple) perspectives to the consultation activities. The online survey included 232 autistic individuals (74% with a formal diagnosis; 4% currently being assessed; 16% self-identified, no formal diagnosis; 6% did not provide this information), 325 parents/caregivers/family members of an autistic person, 298 practitioners involved in the assessment or diagnosis of autism and 115 members of organisations or groups that have an interest in the assessment and/or diagnosis of autism. Seventy-two people identified as bringing ‘other’ perspectives, which included a diverse range of roles including support workers, people offering informal support and advocacy, managers of services, consultants, educators and people involved in delivering therapies or services that did not include assessment and diagnosis (e.g., music therapist, therapy assistant, behaviour support). For those who attended focus groups, 21 (31.3%) individuals participated in groups where the common shared experience was being an autistic adult, 19 (28.4%) individuals participated in groups where the common shared experience was being a parent or caregiver of an autistic child, and 27 (40.3%) individuals participated in groups where the shared experience was being a practitioner who provides assessment and/or diagnostic services to autistic individuals. The majority (95.5%) of participants were adults (aged 26 years and over) and identified as female (83%). Two participants identified as Aboriginal and/or Torres Strait Islander. There was representation from every state and territory in Australia. A full breakdown of participant characteristics is published in the Guideline (Goodall et al., 2023) and also provided as Supplementary Material to this article (see Supplemental Tables S1 to S8).
Measures
Online survey
The survey was developed to capture the experiences, views and preferences of members of the autistic and autism communities with an interest in the assessment and/or diagnosis of autism. In addition to demographic information, the final survey (see Supplementary Materials for the complete survey) included open-ended questions that were structured to collect information related to (a) people’s current experiences and/or views of assessment and/or diagnosis in Australia, (b) important considerations for each aspect of the assessment and/or diagnostic process covered by the guideline (i.e., Guiding Principles, referral, assessment of functioning, medical evaluation, diagnostic assessment, safety and wellbeing) and (c) the 2018 Guideline and the 2023 update (e.g., anything that should be changed or addressed, and barriers and enablers to implementation of the recommendations). Participants could respond to all sections using word-limited free-text boxes and could also submit a piece of art for Section (a). The survey was estimated to take between 10 and 60 min, depending on which sections participants completed. For this study, only questions in Sections (a) and (b) were included in the data analysis.
The development of the online survey was informed by (a) the structure and content of the online community consultation activities used as part of the development of the related Guideline (Trembath et al., 2022), (b) the content of a Delphi survey used as part of the development of the original Guideline (Whitehouse et al., 2018) and (c) the set of questions developed by the research team involved in the update to the Guideline to address the study aims. An iterative approach was undertaken in developing the survey, whereby three members of the research team (R.S., K.J.V., D.T.) led the initial drafting of the survey, which was then shared with remaining members who were invited to review and provide feedback. All feedback was considered and incorporated where appropriate. Survey data were collected and managed using the REDCap electronic data capture tools hosted at Griffith University, a secure, web-based software platform designed to support data capture for research studies (Harris et al., 2009, 2019) and piloted by members of the research team for clarity and functionality. Feedback provided through the piloting process led to further minor modifications before the survey was finalised ahead of distribution.
Focus groups
In line with the online survey, the focus groups aimed to understand the experiences, views and preferences of (a) autistic people, (b) family members of autistic people and (c) practitioners regarding assessment and/or diagnosis of autism. Participants first completed a short demographic survey, which was coded in REDCap. During focus groups, a semi-structured question guide was used to encourage open discussion on issues that were most important to participants, while maintaining focus, and largely mirrored the questions presented in Section (a) of the online survey (see Section ‘Online survey’) and included:
What is, or was, good about the way assessment and/or diagnosis happens in Australia?
What is, or was, bad about the way assessment and/or diagnosis happens in Australia?
What would you like to see change in the way assessment and/or diagnosis happens in Australia?
Thinking to the future:
a. What principles are important for the assessment and diagnostic process?
b. What can practitioners do to help ensure the safety and wellbeing of individuals and their families?
Participant responses to all questions were included in the analysis for this article if they were coded under the identified principles.
Procedure
Online survey
Participants accessed the online survey via a secure link and were first presented with a short video outlining what participation in the survey would entail and the accessibility features of the survey platform. Following this, participants were presented with a Participant Information Statement and Consent Form. All participants were required to provide informed consent, indicated by agreeing to participate via a checkbox, before accessing the survey questions. For individuals who were under the age of 18 years, or could not provide informed consent independently, a parent or guardian was asked to provide consent on their behalf and assist them (as necessary) to complete the survey. Participants were provided with multiple pathways to navigate through the survey, including the capacity to skip sections and/or exit the survey at multiple points. At the completion of the survey, participants were able to indicate whether their responses should be included in the analysis.
Focus groups
Participants accessed a registration survey via a secure registration link. Participants first read the Information Statement and were required to indicate consent before providing their details and availability to attend an online focus group. The registration survey for the first round of focus groups was closed following a 2-day recruitment period, due to total registrations exceeding available places (n = 142 registrations for 72 positions). Registered individuals were allocated to a focus group based on their preferences and in consecutive order of receiving their registration, with 12 individuals allocated to each of the six groups and five waitlist positions available. A further three focus groups were advertised, with recruitment occurring over a 5-day period. Individuals who were not allocated to a group in the first round were contacted and provided an opportunity to indicate their preferences to attend one of the additional groups. A random number generator was then used to assign the remaining registered individuals (n = 104 new registrations, n = 5 individuals from Round 1) to a group, with 12 individuals allocated to each of the six groups and five waitlist positions available. All registered participants were emailed to indicate their assignment to a focus group, waitlist, or to direct them to the online survey if they were not allocated. A total of nine focus groups were conducted – three for each participant group.
Each focus group was facilitated, via Microsoft Teams, by two members of the research group across a 3-week period (November 15 to December 2, 2022), and where possible, included both an autistic and non-autistic facilitator. Facilitators provided an introduction to the Guideline development process, before presenting the focus group questions one at a time (allowing approximately 30 min per question). A copy of the PowerPoint presentation that was used for all nine focus groups is provided in the Supplementary Materials. Focus groups were recorded for transcription purposes, with the auto-transcription output edited for clarity and to anonymise participant information prior to coding.
Data analysis and credibility
Prior to analysis, screening of participant responses to the online survey was completed by a member of the research team. While there was no financial incentive to participate in the online survey or focus groups, attempts were made to identify and remove any suspicious responses (e.g., bot responses). This included the removal of any duplicate responses and any responses with similar patterns of responding to quantitative aspects of the survey that were submitted in quick succession. Data analysis was only completed on the remaining responses.
Following the framework method of analysis (Gale et al., 2013), a framework was developed to code data gathered during the community consultation. Of relevance to the current study, the coding framework reflected principles that might be important during the assessment and/or diagnosis of autism. A preliminary framework was developed by two of the authors (E.H., D.T.) and drew on (a) principles outlined in the 2018 Guideline (Whitehouse et al., 2018), (b) principles outlined in the National guideline for supporting the learning, participation and wellbeing of autistic children and their families in Australia (Trembath et al., 2022) and (c) preliminary analysis of the first 100 participants who responded to the online survey. The preliminary framework included 14 codes. The coding team was also able to apply an ‘Other’ code to any responses that it felt did not fit with an existing code to ensure that novel, including contrasting, views could be accounted for in the coding process. The ‘Other’ code was then further analysed for the current study, with a 15th code (intersectionality) created during re-analysis.
The coding of participant responses relevant to the current study was completed by a team of three individuals. The second author, who has lived experience of autism as a late-diagnosed autistic female (assigned at birth), coded the included online survey responses and autistic adult focus group transcripts. Two research assistants with expertise working with autistic clients and their family/supporters in allied health roles (as a speech pathologist and occupational therapist) completed coding of the remaining focus group data and were allocated transcripts for the participant group that best aligned with their experience and expertise. All data were systematically read and coded in NVivo Version 13 (R1; Lumivero, 2020), with multiple codes able to be applied where appropriate. The coding team met weekly during the coding process to discuss their experiences while coding the data, any personal challenges that arose from being exposed to sensitive and at times confronting personal stories shared by respondents, and to work through any queries and/or potential misunderstandings in interpretation of the coding framework. Memos were created during the coding process enabling post hoc reflections on any patterns that were emerging from the data (e.g., prominent themes); differences, contrasts and/or contradictions in the responses; any challenges experienced in assigning codes; suggestions for possible new or revised codes; reasons for why they may have coded a specific way or anything else they felt was significant about the data. These memos enabled coders to reflect on how their personal experiences might influence their coding of participant responses, and created an audit trail, to inform the coding process and interpretation of the data and to support the coding team in their work.
After applying the preliminary coding framework, participant data were charted into a series of matrices. The research team adopted an iterative approach, using a combination of inductive and deductive processes to move from discrete principle codes to overarching themes. This included R.S., R.W., K.J.V. and D.T. meeting on multiple occasions to propose themes and discuss differences in interpretation. The final themes were then shared with the broader project team, with no further changes suggested. Multiple approaches were used to help ensure the credibility of the coding process, including coding being completed by individuals with relevant expertise, the use of a standardised codebook and training procedures, ensuring daily on-call support and weekly team meetings for fidelity and support purposes, and ultimately presenting evidence using people’s own words in preparing the evidence summaries. In presenting supporting evidence, the following abbreviations have been used to highlight participant perspectives: A for autistic individuals, Pa for parents/caregivers, F for family members, Pr for practitioners, Org for individuals representing organisations and Oth for other perspectives. A breakdown of support for discrete codes across both consultation activities is provided in the Supplementary Materials (see Supplemental Table S9).
Results
The analysis resulted in a total of three themes, encompassing 15 individual codes, related to principles which should underpin practice across the assessment and diagnostic process (see Figure 1). These themes, along with illustrative quotes, are presented in the following sections.
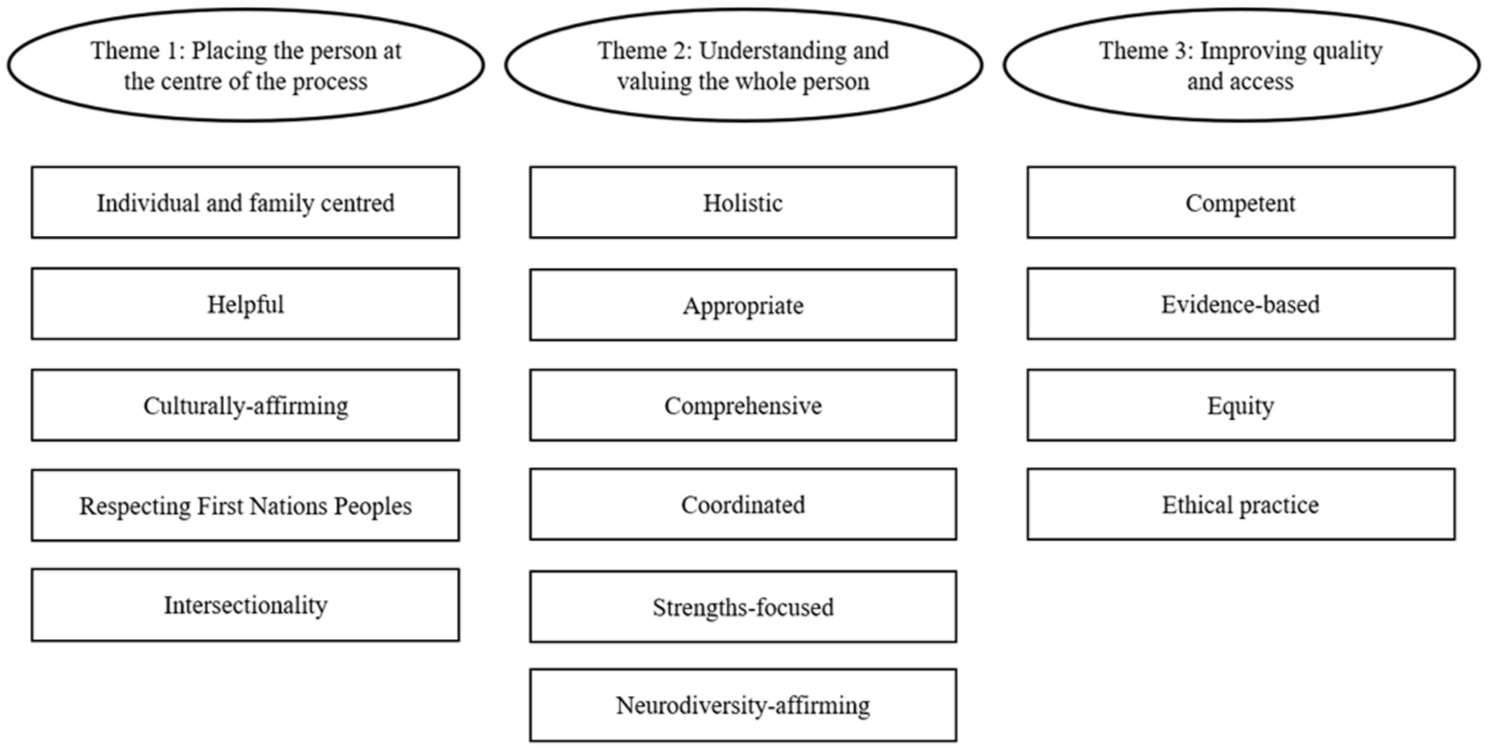
Themes and individual principles.
Theme 1: placing the person at the centre of the process
Participants emphasised the importance of placing the person, and where relevant their family, at the centre of all aspects of the assessment and diagnostic process. A common sentiment was the need for individual- and family-centred services where practitioners ‘tailor [an] approach that works for the client or their caregivers to be able to tell their stories in a way that’s most helpful to them’ (ID137, Pr), including in their consideration of the tools employed which may not capture ‘modern understanding[s] of the variety of autism presentations’ (ID137, Pr). Participants shared examples of helpful experiences, such as practitioners taking ‘time to explore and explain what autism means for each individual’ (ID555, Pr/Org) and providing support for newly diagnosed individuals to come ‘to terms with hidden disability’ (ID443, A/Pa). Post-diagnostic support was also suggested as key to helpful service; however, this was often not the experience of participants, as one parent shared, ‘. . . we were not given any plan of what to do next following diagnosis, so we were just as lost afterwards’ (ID406, Pa). One practitioner emphasised the need for colleagues to provide a ‘rationale for diagnostic decisions/why specific diagnostic criteria were met/not met’ (ID924, Pr/Org), if they are to be helpful to individuals and families in understanding the assessment outcomes and next steps.
In placing the person at the centre of the process, participants suggested that practitioners should adopt an approach that is both ‘culturally sensitive’ (ID976, Pr) and culturally affirming, which also respects First Nations Peoples in the Australian context. The application of this primarily involves acknowledgement and ‘consideration of cultural differences’ (ID67, A/Pa/Pr) and working with members of these groups in ‘culturally safe and appropriate’ (ID415, Pr/Org) ways. This was of particular importance in respecting First Nations Peoples, with one participant highlighting that ‘access in rural and remote areas, and for Indigenous Australians is still poor’ (ID992, Pr), while another related the need for ‘equity of available assessments’ (ID944, Pr) for this population. Overcoming this inequity requires practitioners to have ‘self-knowledge and cultural awareness’ (ID40, Pr), in addition to awareness of their own inherent biases; ‘so often in remote areas people look for FASD (don’t get me started on the systemic racism of this bias) but often miss or don’t even look for neuro-differences’ (ID67, A/Pa/Pr). Participants further emphasised a need for recognition of the limitations of current standardised assessment tools that ‘are not neuro affirming [or] sensitive to gender and cultural differences [sic]’ (ID268, Pr) and ‘culturally biased as not enough is known about how autism looks in adult migrants’ (ID49, A/Pa).
Beyond considerations of culture, participants also highlighted the need for practitioners to have awareness of intersectionality, including the interplay between autism, gender and other psychosocial factors. Participants called for ‘more awareness and identification for autism in girls, women, non-binary and high-masking people’, who may not demonstrate behavioural characteristics of autism in line with male-centric perceptions of autism. It was also deemed important that practitioners have ‘more understanding of gendered differences and masking behaviours’ (ID52, A/Oth) that are commonly used by those who are assigned female at birth and gender-diverse individuals (and others with a more internalised presentation) to conceal their autism characteristics. A similar point was also asserted by an autistic parent, who highlighted that, in their experience, practitioners need to have ‘better knowledge and experience with female presentation and high masking abilities . . . [and] stop assuming that the ability to make eye contact, have social skills, and academic success, means that autism cannot be possible’ (ID194, A/Pa). Concern was also raised by one practitioner regarding ‘diagnostic overshadowing’, who shared their observation that ‘if a client has a background of trauma, the autistic behaviours are ignored by many clinicians’ (ID78, Pr).
Theme 2: understanding and valuing the whole person
Participants stressed the importance of holistic approaches which make every effort to understand the individual, their family (where relevant) and their broader context. One participant (ID54), who identified as both an autistic parent and practitioner, highlighted that services at all ages should mirror the holistic approach they had seen routinely adopted for assessment and diagnosis of autistic children, involving looking ‘cross-contextually, getting relevant information from a variety of sources. [Considering] neurocognitive assessment in addition to social factors’. They reported that assessment of adults was often ‘subpar’, failing to adopt a whole-person approach to understanding experiences. Instead, an appropriate process goes beyond ‘ticking the box’ for an autism diagnosis and seeks to understand a ‘. . . person’s journey and experiences and seeking to find what may be the best explanation of what is happening for them’ (ID736, Pr).
Comprehensive approaches to assessment and diagnosis were encouraged, including those that investigate ‘a wide range of stuff . . . rather than just for assessing for autism only’, including masking and common co-occurring conditions, that provide clients with ‘a detailed picture’ (ID6, A) of their individual profile. Although the importance of a coordinated, collaborative approach between practitioners was desired, many noted that this was not their experience. On the contrary, a ‘disconnect’ (ID812, Pr) between medical and allied health practitioners and between the public and private sectors was emphasised. Lack of a coordinated, collaborative approach between practitioners translated as clients having to ‘coordinate between services’ (ID634, Pa) themselves, with one autistic adult (ID440) reflecting that ‘all of the work is left up to me, I am solely responsible for advocating and organising myself’ and the experience described as a ‘nightmare’ by one parent (ID634).
In reinforcing the need to understand and value the whole person, a common sentiment, expressed in participants’ responses, was the need for practitioners to adopt strength-focused practices that embrace and affirm neurodivergent individuals. When demonstrated in practice, strength-focused approaches, which closely align with neurodiversity-affirming practice, included practitioners being ‘. . . more neuro-affirming and less about projecting neurotypical norms’ (ID268, Pr), when talking about autism. This was described as a starting point for a professional relationship and process that seeks to ‘support the person in coming to terms with their identity’ (ID 578, A/Pr) and celebrates the ‘uniqueness of each [autistic] person in the community’ (ID486, A). While neurodiversity-affirming practice was encouraged, this was not without acknowledgement of the need to balance strengths with the challenges faced by the individual. As one autistic adult shared:
I find that purely strength-based approaches can be invalidating and disempowering as they can talk about ‘superpowers’ and all these other benefits that autistic can have but the reality is that is not why the majority are seeking a diagnosis and they want to know that their difficulties are heard and understood. (ID985, A)
Within a clinical context, this was considered achievable, as a practitioner who was both a parent and an autistic adult themselves noted:
We can identify the deficits and the weaknesses. We can always weave in the strengths and the beautiful parts of the person. I think that’s really important as well. So I’m working hard to do that on my end over here. (ID48–A/Pa/Pr)
Theme 3: improving quality and access
Participants emphasised the need for higher quality service provision and more equitable access, including in relation to practitioner competency, evidence-based practice and equity. Many autistic participants indicated that practitioners having knowledge and understanding of the ‘diversity in autism presentation’ and ‘impact of masking on mental health and presentation of ASD’ (ID159, A) as central to being competent. Participants also emphasised that ‘stereotypes need to be put aside’ (ID180, Pa) and spoke of the negative consequences when this does not occur, with one autistic parent (who also identified as a practitioner) reflecting that ‘. . . if you encounter someone who does not understand autism or thinks that they understand autism and are set in that old sort of way of thinking, it is a very negative experience’ (ID2, A/Pa/Pr). Having relevant experience in ‘the age group being assessed’, being ‘trained in [the] assessment tools they use’ (ID822, Pr) and ‘hold[ing] relevant qualifications including in differential diagnosis’ (ID689, Pr) were also strongly linked to expectations regarding practitioners’ competency.
Critical to providing safe and effective service was the need for practitioners to be ethical. When demonstrated in practice, participants described being ethical as practitioners ‘working within their professional scope’ (ID758, Pr) and knowing when to refer on if ‘they can’t help’ (ID606, A). Unfortunately, participants had encountered examples of inappropriate practice during the assessment and diagnostic process which ranged from ‘gate keeping’ (ID67, A/Pa/Pr) of referrals, to practitioners refusing diagnostic services, as one parent (ID571) describes; ‘one practitioner refused to even meet our child . . . so some practitioners are not completing the process before forming a judgement’. On balance, participants were also cognisant that individuals should ‘not [be] pressured by professionals to pursue assessment/diagnosis if not meaningful to them’ (ID760, Org). Communication with individuals was considered critical to engaging in ethical practice, with participants emphasising the importance of practitioners ‘being really specific about what they do, giving options for different levels of complexity and different outcome desires and being really upfront about the cost too’ (ID11, A/Oth). One autistic practitioner and parent (ID51) reflected on the importance of transparency, noting that ‘We can openly and clearly state what our training and experience is around autism, diagnosis and support, and assessment. And if we’re not at, you know, competent we need to state that’.
Training delivered and/or informed by autistic people was perceived as a core means of ensuring practitioner competency, with one autistic participant asserting the need for ‘training that was run by or at very least developed by an autistic person in order to be accredited, to be competent, to diagnose and assess all forms of autism’ (ID11, A/Oth). This sentiment of ‘prioritis[ing] autistic voices’ (ID250, Org) was also reflected in participants’ expectations of evidence-based practices to be used in assessment and diagnosis. While evidence-based assessments, including the use of standardised diagnostic tools, were often acknowledged as an important component, participants recognised the ‘harms that can occur from non-affirming approaches to assessment and treatment’ (ID250, Org). Participants stressed the importance of practitioners using the latest information from research and up-to-date evidence-based tools ‘rather than outdated, outmoded, gender-based screeners’ (ID596, A/P/Oth).
Regarding equity, the prohibitive cost often associated with accessing assessment and diagnostic services, which are exacerbated for some groups (e.g., culturally and linguistically diverse, First Nations Peoples, low-income households), was frequently mentioned as a barrier to diagnosis, with a call from participants to create more affordable pathways ‘for people to access a diagnosis, particularly those that are disadvantaged’ (ID159, A). Additional factors that contributed to reduced equity were a lack of available services and extensive waitlists where services did exist. While some parents reported being able to access services for their child ‘relatively soon’ after referral (ID774, Pa), others were not as fortunate; ‘The time wasted just waiting to get into see someone, anyone! We desperately needed help and had to wait 8 months until we could get into a paediatrician’ (ID152, Pa). The extended wait times were further highlighted as being inconsistent with best practice guidelines; ‘the wait for the assessment from the time of referral is much, much longer than the evidence-based timeframe. Most individuals are waiting 2 years+ for the assessment’ (ID244, Pr).
Discussion
In an effort to improve the quality, consistency and accuracy of autism assessments and diagnostic services, we conducted a nationwide consultation in Australia with autistic individuals and the broader autism community through surveys and focus groups. Analysis of participant responses highlighted principles which should underpin the assessment and diagnostic process, which were organised across three central themes. This work extends on research which seeks to understand the experiences, views and perspectives of the autistic and autism communities, recognising their valuable contributions to informing evidence-based best practice in the assessment and diagnosis of autism.
The need to place the person, and where relevant their family, at the centre of all aspects of the assessment and diagnostic process, was reflected in the first theme. The importance of cultural sensitivity was highlighted, particularly towards Australian First Nations Peoples who face disadvantage and additional barriers to accessing supports due to the enduring impacts of colonisation (Gatwiri et al., 2021). With the prevalence of autism thought to be similar among Aboriginal and non-Aboriginal peoples in Australia (Bailey & Arciuli, 2020), this signals a potential positive shift, recognising the importance of addressing disparities in accessing support, particularly in remote communities with increased risks of missed or underdiagnosis of autism (Roy & Balaratnasingam, 2010). The need for practitioners to consider the role of intersectionality, the interaction between an individual’s identity and broader psychosocial factors that impact their experiences (Cascio et al., 2021), was further highlighted as critical to the assessment and diagnostic process for autistic individuals. The relevance of intersectionality has previously been highlighted in research relating to the impact on autistic people specifically (e.g., Cohen et al., 2022; Sassu & Volkmar, 2023), as well as the broader community (e.g., Filia et al., 2022; Maestripieri, 2021; Young et al., 2021). Our findings illustrate why consideration of intersectionality and adopting an individual- and family-centred approach matter in the context of autism assessment and diagnosis, and how a lack of knowledge and understanding by practitioners can impact upon the helpfulness, accuracy and timeliness of the assessment and diagnostic process, as well as individual wellbeing. The clear clinical implication for practitioners is to broaden their knowledge and awareness, challenge their biases and aim for helpful, respectful and culturally affirming assessments for all clients.
Theme 2 underscores the importance of both understanding and valuing the whole person in any approach to assessment and diagnosis. It is increasingly recognised that the assessment and diagnostic process for autism needs to go beyond diagnostic decision-making to include an understanding of individual priorities and pathways to better support immediate and longer-term outcomes for autistic individuals (Lord et al., 2022). Participants further highlighted the necessity for coordinated and holistic approaches to the assessment and diagnostic process. Assessment, diagnosis and referral for post-diagnostic supports must be considered in conjunction, as they are intrinsically related and interdependent in ensuring a safe, seamless and supportive experience for individuals and their families (Lord et al., 2022). Participants notably expressed the need for a nuanced approach to assessment and diagnosis – one that maintains acknowledgement and respect for diversity and the inherent strengths of autistic individuals, without diminishing the importance of properly addressing and supporting the challenges an individual experiences. This is consistent with the growing shift towards neurodiversity-affirming clinical practice, which has been reflected in research (Sulek et al., 2024; Waddington et al., 2023), policy (Trembath et al., 2022) and practice (Schuck et al., 2022; Van Den Plas et al., 2024) more broadly in recent years.
It is important to note that the neurodiversity movement is not without its critics, with arguments made that the movement is not representative of the broad spectrum of strengths and challenges of individuals with a diagnosis, particularly those who would be considered more severely impacted by their disability as conceptualised within a medical model (Russell, 2020). While the authors acknowledge this, among broader criticisms of a neurodiversity-affirming approach, we believe that adopting a neuro-affirming and strength-based approach to diagnostic evaluation, which recognises and validates challenges, in no way diminishes or alters the relevance or interpretation of diagnostic criteria. The principles outlined in this article highlight the importance of acknowledging all autistic people (and their families/supporters where appropriate), regardless of the level and complexity of their support needs, and tailoring assessment to the individual. Doing so does not ‘de-prioritise’ the needs of those autistic people who experience a higher degree of disability but rather allows for the process to be more equitable and inclusive.
The third theme highlighted that approaches to improving quality and equitable access to assessment and diagnosis are required to ensure that the process is timely and accessible for everyone. Among the principles identified was the need for increased practitioner competency, particularly as it relates to understanding the diversity of autism presentations and the impact of masking on mental health and wellbeing. Given the links between masking and camouflaging – more commonly reported among autistic females – and poorer mental health outcomes (Cook et al., 2021), ensuring practitioners are well-trained, knowledgeable and free from gender-based stereotypes may improve diagnostic experiences for those assigned female at birth and others with more internalised or nuanced presentations. The ethical responsibilities of practitioners were also emphasised, including ensuring that they work within their scope of practice and are transparent with clients about their knowledge and experience. This theme also stressed the need for clear communication with clients following assessment and/or diagnosis and consistency in post-diagnostic guidance and support. This inconsistency in providing post-diagnostic support, despite its high desirability, reflects the experiences of parents of autistic children and autistic adults internationally (Crane et al., 2018; Makino et al., 2021; Milner et al., 2019), indicating that this is an area of practice that requires improvement globally. The highlighted need to increase equity of access to assessment and diagnosis also aligns with experiences in other Western countries, with the high financial cost associated with accessing assessment and diagnosis, limitations in the availability of appropriate practitioners and associated waitlists consistently shown as pervasive barriers (de Broize et al., 2021; Howes et al., 2021; Legg & Tickle, 2019; Martinez et al., 2018).
Limitations and future research directions
The strengths of this study lie in its large sample size and recruitment of a diverse range of stakeholders from both the autistic and autism communities. Drawing on both survey and interview methodologies, we were able to gain a rich insight into participant experiences, views and perspectives. A strength of the study is that there was strong representation from female participants. While this is not unusual in survey research, with higher levels of female-to-male participation often observed (Wu et al., 2022), it is important to the aim of this study given under-representation of females in autism research more generally (Nordahl, 2023) and biases in clinical practice preventing females from being diagnosed (McCrossin, 2022). However, this work was not without limitations. While we were able to capture the views of autistic individuals, these were largely adults who received their diagnosis in adulthood, with only five participants identified as being under the age of 18 years. Furthermore, we did not collect additional details from autistic respondents regarding any co-occurring conditions, such as intellectual disability. Despite attempts to ensure the accessibility of the research methods used in the current study, this group and other autistic individuals who communicate in ways other than speech were under-represented in the current study. It is likely that these individuals were systematically excluded from participating in focus groups and may have also experienced difficulties responding to the survey (although utilising a support person was encouraged). It will be important for future work to determine the relevance of the identified principles to autistic children and young people, those with co-occurring diagnoses and those with communication differences through employing developmentally appropriate and accessible methodologies. It is also worth noting that 16% of the autistic cohort had no formal diagnosis of autism and instead indicated that they self-identified as autistic. While a lack of formal diagnosis in this subgroup may reflect differences in the conceptualisation of autism as an identity rather than a disability, it could also be due to several identified barriers in accessing an autism diagnosis, particularly in adulthood (Overton et al., 2024). It has also been argued that self-diagnosis may lead to misdiagnosis or a reduction in access to supports that would otherwise become available if a formal diagnosis were pursued (David & Deeley, 2024). While the broader exploration of self-diagnosis in the context of the autistic identity was outside the scope of the current project, future work may seek to determine whether differences in self- versus formal diagnoses exist within the explication of the identified principles.
Furthermore, while recruitment for both consultation activities engaged peak bodies representing First Nations peoples in Australia, this cohort was a small minority (2.6%) of the current sample. Encouragingly, the importance of culturally responsive assessment and diagnosis was among the principles identified; however, future work is required to ensure these findings hold relevance for First Nations communities. Finally, more effort could have been made in the current study to understand the types of participants responding, including participant gender (not captured in the survey), closer investigation of socio-economic status, and identification of whether participants from rural and remote communities were adequately represented in the current sample. Given these characteristics can impact access to, and experience with, the assessment and diagnostic process, it will be crucial to ensure a representative sample in future research.
Conclusion
The principles identified in the current study provide a starting point for clinicians involved in the assessment and diagnostic process for autism to reflect on their own practice. Given the inherent overlap between some of the identified principles, clinicians should consider these collectively when approaching assessment and diagnosis. Importantly, clinicians should always maintain a strong focus on the individual in front of them, and how these principles may be applied in practice in a way that best supports their individual needs and the identification of personalised support pathways.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251406094 – Supplemental material for Community views on the assessment and diagnosis of autism: Principles to guide clinical practice
Supplemental material, sj-docx-1-aut-10.1177_13623613251406094 for Community views on the assessment and diagnosis of autism: Principles to guide clinical practice by Rhylee Sulek, Rachelle Wicks, Emma Hinze, Nicole Dargue, Briohny Dempsey, Emma Goodall, Libby Groves, David Trembath, Hannah Waddington, Andrew JO Whitehouse and Kandice J Varcin in Autism
Footnotes
Acknowledgements
The authors thank all the members of the autistic and autism communities who shared their experiences as part of the development of the guideline.
ORCID iDs
Ethical considerations
This study was approved by the Griffith University Human Research Ethics Committee (approval number 2022/780). All participants provided informed consent, electronically, prior to their participation in the research activities.
Ethical approval and informed consent
Ethical approval was granted by the Human Research Ethics Committee at Griffith University. Participants were required to indicate their consent electronically by clicking ‘I agree to participate’ prior to entering the survey or upon registering their interest in joining a focus group.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The project was funded by Autism CRC to update The Guideline (2023). D.T. (Griffith University; Telethon Kids Institute) and E.G. (Griffith University) were appointed co-chairs of the Guideline Development Group, and Griffith University and Telethon Kids Institute received funding from Autism CRC to support this work. D.T. contributions were in-kind, with funding used to employ E.G. and research fellows/assistants to support the work, to support community consultation activities and to pay honoraria to the GDG members.
Data availability statement
Data relating to this study are available from the corresponding author (R.S.) upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.