
Abstract
This study examined differences in referral and diagnosis based on sex recorded at birth (hereafter, ‘sex’), using case notes from 408 individuals diagnosed by 30 multidisciplinary teams across Scotland. Analyses focused on male-to-female ratios and median ages at referral and diagnosis across attention-deficit/hyperactivity disorder, autism and intellectual disability. The lifespan male-to-female ratio across all diagnoses was 1.31, varying by category and age. In autism, the male-to-female ratio was 2.21 for children under 10 years, but there were more females in adolescence (male-to-female ratio = 0.79) and adulthood (male-to-female ratio = 0.94). Across the lifespan, combining all diagnoses, females were referred later (median ages: 14.4 vs 19.7 years; p < 0.001) and diagnosed later (median ages: 15.2 vs 20.2 years; p < 0.001), indicating a 5-year delay. Among autistic children and adolescents, females were referred later (median age: 7.5 vs 10.5 years; p = 0.002) and diagnosed later (median age: 9.3 vs 11.9 years; p = 0.003). However, no significant differences were found in age of referral or diagnosis for autistic adults. Overall, the results indicate increasing balance in sex ratios with age, greater asymmetry in younger age groups, and consistent delays in referral and diagnosis ages for females.
Lay abstract
This article looks at how males and females are diagnosed with neurodevelopmental differences including autism, attention-deficit/hyperactivity disorder (ADHD) and intellectual disabilities. It studies the case notes of 408 people (adults and children) assessed by 30 different teams during their diagnosis process. The results show overall that more males were diagnosed with neurodevelopmental differences and that males are diagnosed at younger ages compared to females. The increased diagnosis of males compared to females is most common in younger ages, but and as people get older, the number of males and females diagnosed becomes more equal, showing that more women are coming forward for and being diagnosed, for example with autism and ADHD. This research shows that although there are increasing amounts of females diagnosed, that girls and women are still missed when they are young, with more boys gaining a diagnosis as children. It seems there is a pattern of females being diagnosed at later ages (meaning less access to support and self-understanding). The study calls for better diagnostic practices and more research to address these gender differences.
Introduction
Neurodevelopmental differences are lifelong (Coghill & Sonuga-Barke, 2012; Happé & Frith, 2021) and heterogeneous (Davies et al., 2023; Ismail & Shapiro, 2019; Thapar et al., 2017) and include autism, attention-deficit/hyperactivity disorder (ADHD) and intellectual disabilities (ID) (American Psychiatric Association, 2013). In a recent US survey, the population lifespan prevalence of all neurodevelopmental differences was 17.8% (Zablotsky et al., 2019). Global autism prevalence is commonly reported at 1%–2% (Elsabbagh et al., 2012; Kim et al., 2011; Polanczyk et al., 2015); however, diagnostic rates have risen rapidly in recent years (Brugha et al., 2016; O’Nions et al., 2023). A study in England estimated adult autism diagnosis prevalence at 1.1% but acknowledges that this figure is an underestimate (Brugha et al., 2016). In the United States, it was reported that 1 in 36 children aged 8 had been diagnosed autistic in 2020 (Maenner et al., 2021). The global prevalence of ADHD is higher still, with pooled estimates for children around 5% (Polanczyk et al., 2015), and some recent studies suggesting higher prevalence up to 8.4% (Danielson et al., 2018). Recent studies suggest that 3% of adults have ADHD (Ayano et al., 2023).
Timely diagnosis is essential for securing appropriate support, yet neurodivergent females are often underdiagnosed, misdiagnosed or face greater delays (Lockwood Estrin et al., 2021). Many report inequities and delays in the assessment process (Leedham et al., 2020; Zablotsky et al., 2019). A well-established finding in the literature is that the prevalence of neurodevelopmental differences tends to be higher in males than in females. A recent study found 1.22% of all males and 0.35% of females were diagnosed autistic in England, with the highest prevalence in 15- to 19-year-olds (males: 4.40%, females: 1.37%) (O’Nions et al., 2023). While in the United States in 2020, 4% of boys and 1% of girls across the population were diagnosed autistic (Maenner et al., 2021). A recent review (Bolte et al., 2023) found male-to-female ratios of 1.7 across all neurodevelopmental differences, 2.3 for childhood ADHD and 3 for autism across the lifespan. In Scotland, where the current research was completed, previous research examined male-to-female ratios in autism diagnosis in 2014 in a clinical population of 150 children and adults seeking assessment. This earlier study found that girls faced longer delays before referral and diagnosis than boys, and that males comprised a higher proportion of referrals and diagnoses overall (Rutherford et al., 2016).
A key issue underpinning sex ratios is whether neurodevelopmental diagnosis rates should be equal or if there are inherent differences. Biogenetic factors are proposed to play a role, but differences also arise from social and other factors (Loomes et al., 2017). The perception that neurodevelopmental differences are a male phenomenon contributes to higher diagnostic thresholds for females, wherein women need to display greater levels of distress to access services and support (Lockwood Estrin et al., 2021). Masking or ‘camouflaging’ is another important aspect (Ai et al., 2022; Beardon et al., 2019; Libsack et al., 2021; Livingston et al., 2019; Miller et al., 2021). Researchers are now proposing that neurodivergent females may experience or display greater degrees of masking through female roles and socialisation to ‘blend in’, which may have a further impact on diagnosis timing (Lockwood Estrin et al., 2021). Lack of awareness of underlying neurodivergence contributing to eating disorders, depression and anxiety, along with overlap between mental health diagnoses and neurodevelopmental differences, means women and girls are misdiagnosed (Carpita et al., 2023).
Evolving approaches to neurodivergence assessment, particularly recognising lifespan prevalence, are relevant to this study. Historically, neurodevelopmental differences were viewed as paediatric, resulting in low adult diagnosis rates (O’Nions et al., 2023). However, adult diagnoses have risen substantially (Russell et al., 2022). Broadening diagnostic criteria, improved staff knowledge, increased societal awareness and generally improved availability of services have been factors in rising rates (Brugha et al., 2016). Concurrently, support efforts have begun to shift from focusing on individual diagnoses, such as autism, to addressing co-occurring neurodevelopmental differences. The ‘ESSENCE’ framework highlights interconnections and overlap between diagnoses, leading to a shift from a singular diagnosis to a broader multi-condition or ‘neurodevelopmental’ assessment (Gillberg, 2010, 2021).
Shifts in perspective on how to assess neurodevelopmental differences align with the neurodiversity paradigm (Lang et al., 2024; Maciver et al., 2022; Male et al., 2020; Rutherford & Johnston, 2023; Rutherford et al., 2021). Supports that ‘normalise or cure’ are increasingly criticised (Chapman, 2021; Pellicano & den Houting, 2022; Schuck et al., 2022). While neurodevelopmental differences can and do result in disability and vulnerability, differences themselves are non-pathological (Dwyer, 2022; Dwyer et al., 2022; Pellicano & den Houting, 2022). Disability, in this view, arises from environments designed for the neurotypical majority, consistent with the ‘social’ model, which highlights the role of environmental factors in shaping outcomes (Cherewick & Matergia, 2024). There has also been a parallel shift away from deficit language (Botha et al., 2021; Bottema-Beutel et al., 2021; Bury et al., 2023; Constantino, 2018; Donaldson et al., 2017; Dwyer, 2022; Dwyer et al., 2022; Harris, 2016; Kenny et al., 2016).
A key issue is how to describe ‘males’ and ‘females’. This study uses a binary understanding of sex (male/female) due to the structure of the data, which relied on medical records which recorded sex as such. However, it is crucial to recognise how being ‘male’ or ‘female’ is a diverse experience for transgender, non-binary and other gender-diverse people who do not fit the male/female dichotomy that dominates research. This limitation may be particularly impactful in the study of neurodivergence, as gender-diverse individuals are known to be disproportionately represented in this population (Corbett et al., 2023; Kourti & MacLeod, 2019; Strang et al., 2023; Warrier et al., 2020).
Addressing sex-related differences can improve diagnosis processes, leading to better support and self-understanding (Rea et al., 2023). Few studies have examined real-world clinical samples of children and adults across neurodevelopmental differences. Most research tends to focus on research cohorts, children, autism or ADHD in isolation (Bolte et al., 2023), with limited exploration of differences at each stage, including referral and assessment (Rutherford et al., 2016). Differences in age of diagnosis for females highlight the need for sex-sensitive diagnostic processes, while delayed identification during referral stresses the importance of raising awareness.
The current study
A key aim of the current study is to revisit sex ratios and ages of referral and diagnosis in Scotland, building on an earlier study of autism diagnosis (Rutherford et al., 2016). Using a larger dataset, the study examines diagnostic processes across a broader range of neurodevelopmental differences, including autism, ADHD and intellectual disability, addressing the following research questions:
What are the male-to-female ratios among those referred for a neurodevelopmental assessment, across different age groups and diagnoses?
Are there sex-based differences in age of referral and age of diagnosis, and do these vary by final diagnosis?
Have male-to-female ratios in autism diagnosis changed since the earlier study?
This work was part of a national programme of work in Scotland to improve lifetime experiences and outcomes for neurodivergent people. The Scottish Government funded the authors of this study, the National Autism Implementation Team (NAIT), to establish comprehensive neurodevelopmental support pathways (Maciver et al., 2022; National Autism Implementation Team, 2021, 2023; Rutherford et al., 2021; Rutherford & Johnston, 2023). The NAIT team comprises neurodivergent and neurotypical individuals and is multidisciplinary, including researchers and practitioners from Psychiatry, Education, Speech and Language Therapy, and Occupational Therapy. As integrated members of the research team, neurodivergent researchers contribute to the planning and design of studies and decision-making related to study outcomes. The team collaborates with academics and neurodivergent people to champion evidence-informed practices and neurodiversity-affirming work, with a focus on multi-professional and cross-sector practice and partnership with neurodivergent individuals (Curnow, Rutherford, et al., 2023; Curnow, Utley, et al., 2023; Maciver et al., 2022; Maciver et al., 2023; National Autism Implementation Team, 2021, 2023; Rutherford et al., 2021; Rutherford & Johnston, 2023).
Methods
Participatory methods
NAIT was inspired by the needs and interests of stakeholders from the neurodevelopmental community, including young people and adults with lived experience, families and user groups. Neurodivergent people have been involved in a range of ways, including as researchers in the NAIT team.
Ethical approval
Ethical approval was received from Queen Margaret University Ethics Committee. Analysis was based on an anonymised dataset containing routinely collected clinical data, so no consents were sought from individuals. Consent for data access was granted by the NHS Scotland Public Benefit and Privacy Panel for Health and Social Care.
Study design
The study was designed as a cross-sectional, retrospective case note review of individuals seeking assessment for neurodevelopmental differences in diagnosing teams across Scotland.
Context: Scotland diagnostic services
In Scotland, diagnosis is managed within secondary care or community health, and funded by the Government, ensuring high standards, strong governance and robust training. However, challenges such as long waiting times, staffing shortages and gaps in service provision, particularly in rural areas, are common. Service delivery varies across areas, with differences in clinic availability, prescribing practices and access criteria. In some regions, neurodevelopmental assessments for different conditions, such as autism and ADHD, are poorly integrated, leading to separate services and waiting lists, complicating the provision of comprehensive services. Adult referral criteria often require moderate to severe mental illness, creating access barriers.
A total of 14 Health Boards oversee services. For children, assessments typically begin through GPs, with education staff frequently making referrals. Some regions have open referral systems. For adults, while there are examples of open referral systems, referrals usually start with GPs or psychiatrists, who then refer to secondary adult mental health services. Children’s services are provided by community multidisciplinary teams, including allied health professionals and paediatricians and may involve Child and Adolescent Mental Health Services (CAMHS) for those under 17/18. Newer neurodevelopmental services use a single multidisciplinary pathway combining community child health, Allied Health Professionals and CAMHS. Adult pathways are mostly psychiatry-led, less accessible, more specialised and typically condition-specific. National diagnostic guidelines, based on evidence and consensus, are widely used for autism and ADHD across the lifespan (Scottish, Intercollegiate, Guidelines, & Network, 2009, 2016). Guidelines align with internationally recognised practices. Both children and adults undergo assessments involving history-taking and observation. For children, wider informant interviews are conducted with family members, caregivers and school staff. These are less common for adults, though occasionally used.
Diagnosis follows Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) or International Classification of Diseases, 11th Revision (ICD-11) guidelines and typically involves multiple meetings. Most individuals attend between two and six meetings or appointments, though the actual number of meetings can vary. Adults are often diagnosed by an individual practitioner, while children’s assessments are completed by a multidisciplinary team. Assessment tools used include the Autism Diagnostic Observation Schedule-2 (ADOS-2), ADHD Rating Scale-IV (ADHD-RS-IV), Social Responsiveness Scale (SRS) and Conners ADHD Rating Scales for children, and the Diagnostic Interview for ADHD in Adults (DIVA), Diagnostic Interview for Social and Communication Disorders (DISCO), Autism Diagnostic Observation Schedule-2 (ADOS-2) and Autism Diagnostic Interview–Revised (ADI-R) for adults. For adults and children, intellectual disability is typically defined as IQ of less than 70.
National guidelines and tools exist for neurodevelopmental-wide children’s assessment (see Rutherford et al., 2021), but no similar guidelines or pathways are in place for adults. Around half of Scottish areas offered neurodevelopmental-wide assessments for children, but none for adults existed at the time of the study.
Sampling
All health board areas were approached, with voluntary participation sought. Participation was confirmed by senior managers, with 10 out of 14 boards consenting (4 boards declining and citing work pressures). In the absence of a central public register of diagnosing teams, senior managers within participating boards identified and volunteered teams that routinely conduct neurodevelopmental assessments. Once teams had been identified, team-specific case quotas were established based on their size and likely referral rate (health boards with larger populations were asked to provide more cases, and smaller areas asked to provide fewer). Diagnosing teams were classified as ‘adult’ or ‘child/adolescent’ services based on their service classification.
The inclusion criteria for cases were as follows. For younger people’s services: individuals referred for neurodevelopmental assessment, Autism, Fetal Alcohol Spectrum Disorder, Attention Deficit Hyperactivity Disorder (ADHD), Developmental Language Disorder, Developmental Coordination Disorder, and/or Intellectual Disability. For adult services: individuals referred for assessment for Autism, Attention Deficit Hyperactivity Disorder (ADHD), and/or Intellectual Disability assessment.
Each diagnosing team compiled all cases meeting the inclusion criteria completed within the preceding 12 months. To ensure the data captured contemporary practices and outcomes, cases were selected for inclusion consecutively in reverse chronological order, commencing with the most recently completed case and proceeding backwards until the required quota was met. Teams participated between October 2021 and May 2022.
Analysis
Analyses were conducted in R (R Foundation, Vienna, Austria). Cases with missing or non-male/female sex data (n = 6) were excluded from all analyses. Age groupings were defined by age at referral as follows: ‘younger children’ (0–9 years 11 months), ‘adolescents’ (10–18 years 11 months), ‘adults’ (over 18 years 11 months), ‘children & adolescents’ (0–18 years 11 months) and ‘lifespan’ (all individuals). Subgroups were defined by diagnosis: ‘Any ND diagnosis’ (Autism, ADHD, Developmental Language Disorder, Developmental Coordination Disorder, and/or Intellectual Disability), ‘Autism diagnosis’, ‘ADHD diagnosis’, ‘ID diagnosis’ (each representing individuals with that diagnosis, who may have additional diagnoses) and ‘all assessed’ (all referred individuals, including those with no diagnosis or non-neurodevelopmental diagnoses).
To address research question 1 (male-to-female referral ratios for neurodevelopmental assessment across age groups and diagnoses), we calculated the male-to-female ratio (MFR) by dividing the number of males by the number of females, expressed as males per female, for the ‘All assessed’, ‘Any ND diagnosis’, ‘ADHD diagnosis’, ‘Autism diagnosis’ and ‘ID diagnosis’ groups, in all age groupings (lifespan, adults, children & adolescents, adolescents, younger children).
To address research question 2 (sex-based differences in age of referral and diagnosis, and whether these differ by final diagnosis), we compared median ages at referral and diagnosis between males and females in the ‘All assessed’, ‘Any ND diagnosis’, ‘ADHD diagnosis’, ‘Autism diagnosis’ and ‘ID diagnosis’ subgroups in age groupings ‘Lifespan’, ‘Adults’ and ‘Children & Adolescents’ using the Wilcoxon rank-sum test, with p-values reported and a significance level of 5%.
To address research question 3 (changes in male-to-female ratios since prior research), we compared MFRs for the ‘Autism diagnosis’ subgroup to historical data from Rutherford et al. (2016). Directly comparable analyses are male-to-female ratios by age group using the same age cut-offs. Rutherford et al. (2016) completed a retrospective case note analysis of 150 individuals. The study employed random sampling to select 16 diagnostic services (8 child, 8 adult). Their sample included the 10 most recent autism diagnoses within the prior 24 months from each service.
Results
The study covers 10 out of 14 (71%) of Scotland’s health boards, representing approximately 4.8 million people, or 89% of the Scottish population. Data were provided by 30 diagnosing teams, including 12 adult (202 cases; M age at referral = 29.9 years, SD = 10.5, range = 15.8–71.1; 98 females) and 18 children’s teams (206 individuals, M age at referral = 8.99 years, SD = 4.6, range = 1.4–17.9; 76 females). There were 174 females and 228 males included in total; 6 individuals with missing or ‘other’ sex data were identified and excluded from this current analysis. Most (c. 85%) individuals received a neurodevelopmental diagnosis upon completing the assessment. Autism and ADHD were the most common diagnoses. White individuals (including White Scottish, White Other British and White Other) constituted the majority (c. 77%). Other ethnicities, approximately 4% of individuals were included, and 18% of individuals had no recorded ethnicity data. Complete demographics of the study are included in additional file 1 (supplemental material).
Male/female ratios
With regard to the first research question (male-to-female referral ratios for neurodevelopmental assessment across age groups and diagnoses), among all individuals referred for assessment across the lifespan (n = 402), the MFR was 1.31. For those diagnosed with any neurodevelopmental difference, the MFR was 1.29. The highest lifetime MFR was observed in individuals with an intellectual disability (ID) diagnosis (MFR = 2.00), followed by autism (MFR = 1.26) and ADHD (MFR = 1.20). When analysed by age group, differences were observed. In adults (age > 19 years; n = 185), the overall MFR for referred individuals was 0.97, that is, under 1, indicating a slightly higher number of females. The MFR for those diagnosed with a neurodevelopmental difference was similar at 0.95. Only adults with an ID diagnosis showed a higher number of males (MFR = 2.33), while autism (MFR = 0.94) and ADHD (MFR = 0.73) diagnoses had more females. When combining children and adolescents into one group (age 0–19 years; n = 217), the MFR indicated more males than females, with a ratio of 1.71 for both referred and diagnosed individuals. The highest MFR was observed in individuals with an ID diagnosis (MFR = 3.75), followed by ADHD (MFR = 3.60) and autism (MFR = 1.45). In the adolescent age group (age 11–19 years; n = 91), the MFR for referred individuals was 1.12, and for those diagnosed with a neurodevelopmental difference, the MFR was 1.05, showing slightly more males in both groups. The highest MFR was observed in ADHD (MFR = 2.29). However, more females were diagnosed autistic (MFR = 0.78), while the MFR for ID diagnosis was 1.00, indicating equal males and females. In the ‘younger children’ age group (age 0–10 years; n = 126), a higher male-to-female ratio was observed in both referred individuals (MFR = 2.41) and those diagnosed with a neurodevelopmental difference (MFR = 2.53). The highest MFR was observed in ADHD (MFR = 6.67), followed by ID (MFR = 3.33) and autism (MFR = 2.21). Full details are in Table 1.
Male-to-female ratios (MFR) of individuals referred for neurodevelopmental diagnostic assessment.
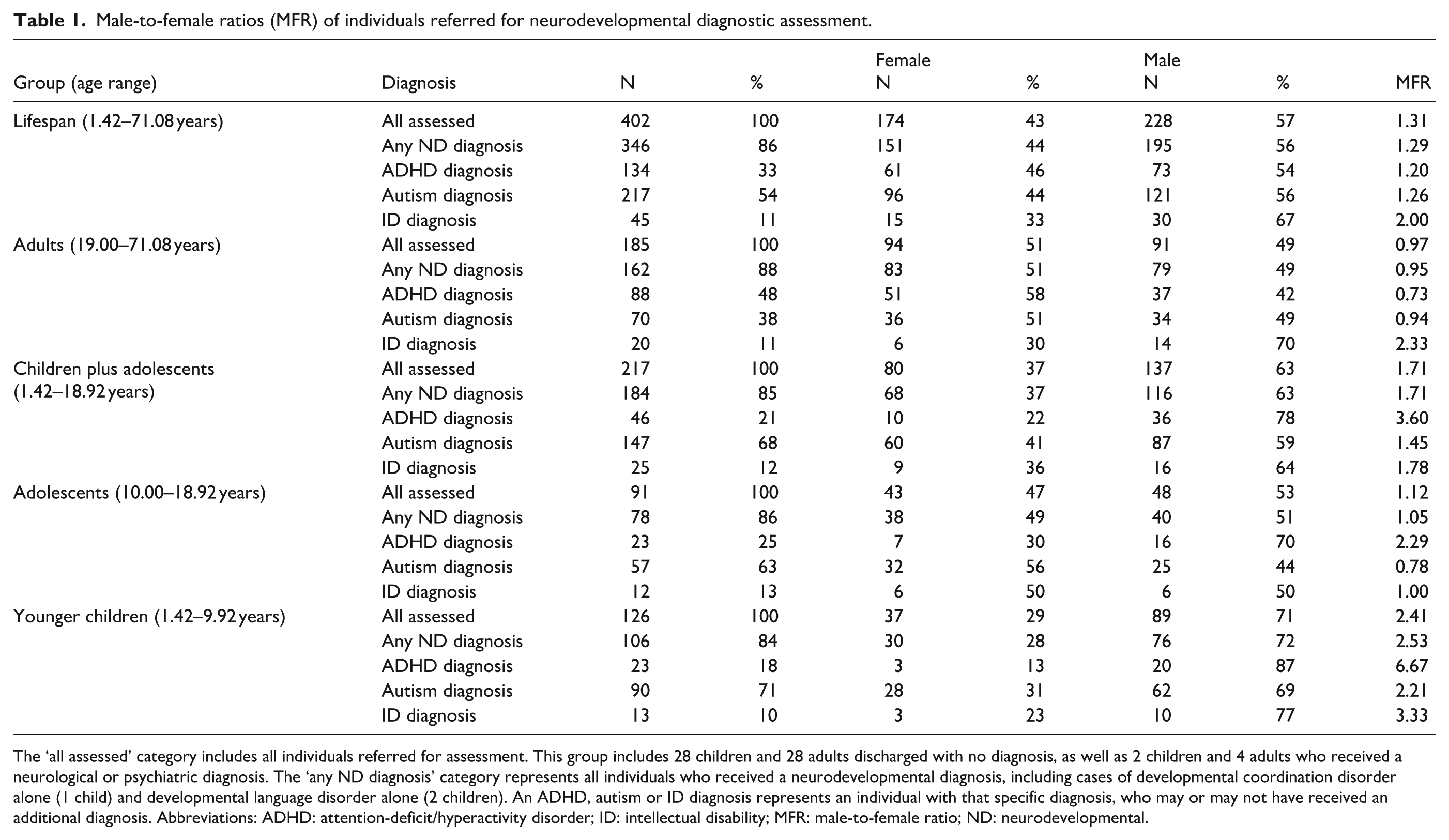
The ‘all assessed’ category includes all individuals referred for assessment. This group includes 28 children and 28 adults discharged with no diagnosis, as well as 2 children and 4 adults who received a neurological or psychiatric diagnosis. The ‘any ND diagnosis’ category represents all individuals who received a neurodevelopmental diagnosis, including cases of developmental coordination disorder alone (1 child) and developmental language disorder alone (2 children). An ADHD, autism or ID diagnosis represents an individual with that specific diagnosis, who may or may not have received an additional diagnosis. Abbreviations: ADHD: attention-deficit/hyperactivity disorder; ID: intellectual disability; MFR: male-to-female ratio; ND: neurodevelopmental.
Sex differences in age of referral and age of diagnosis
With regard to research question 2 (sex-based differences in age of referral and diagnosis, and whether these differ by final diagnosis), analysis revealed statistically significant lifespan differences, indicating that males seeking assessment were referred earlier (median ages: 14.4 vs 19.7 years; p < 0.001) and diagnosed earlier (median ages: 15.2 vs 20.2 years; p < 0.001) than females. Subgroup analysis revealed further statistically significant sex differences for lifespan autism and ADHD, but not for intellectual disability. For lifespan autism, males were referred earlier (median age: 9.6 vs 15.2 years; p = 0.005) and diagnosed earlier (median age: 11.5 vs 16.6 years; p = 0.003). For lifespan ADHD, males were referred earlier (median age: 19.6 vs 25.0 years; p < 0.001) and diagnosed earlier (median age: 20.9 vs 25.5 years; p = 0.002). For individuals referred for assessment under 19 years of age, males seeking assessment were referred earlier (median age: 8.1 vs 10.9 years; p = 0.002) and diagnosed earlier (median age: 10.1 vs 12.1 years; p = 0.008) than females. Subgroup analysis showed statistically significant sex differences for the < 19 years group for autism, but not for ADHD or intellectual disability. For autism in the < 19 years group, males were referred earlier (median age: 7.5 vs 10.5 years; p = 0.002) and diagnosed earlier (median age: 9.3 vs 11.9 years; p = 0.003). In the adult subgroup (age > 19 years), no statistically significant sex differences were found in referral or diagnosis timing in any analysis. Full details are in Table 2.
Comparison of median ages for referral and diagnosis.
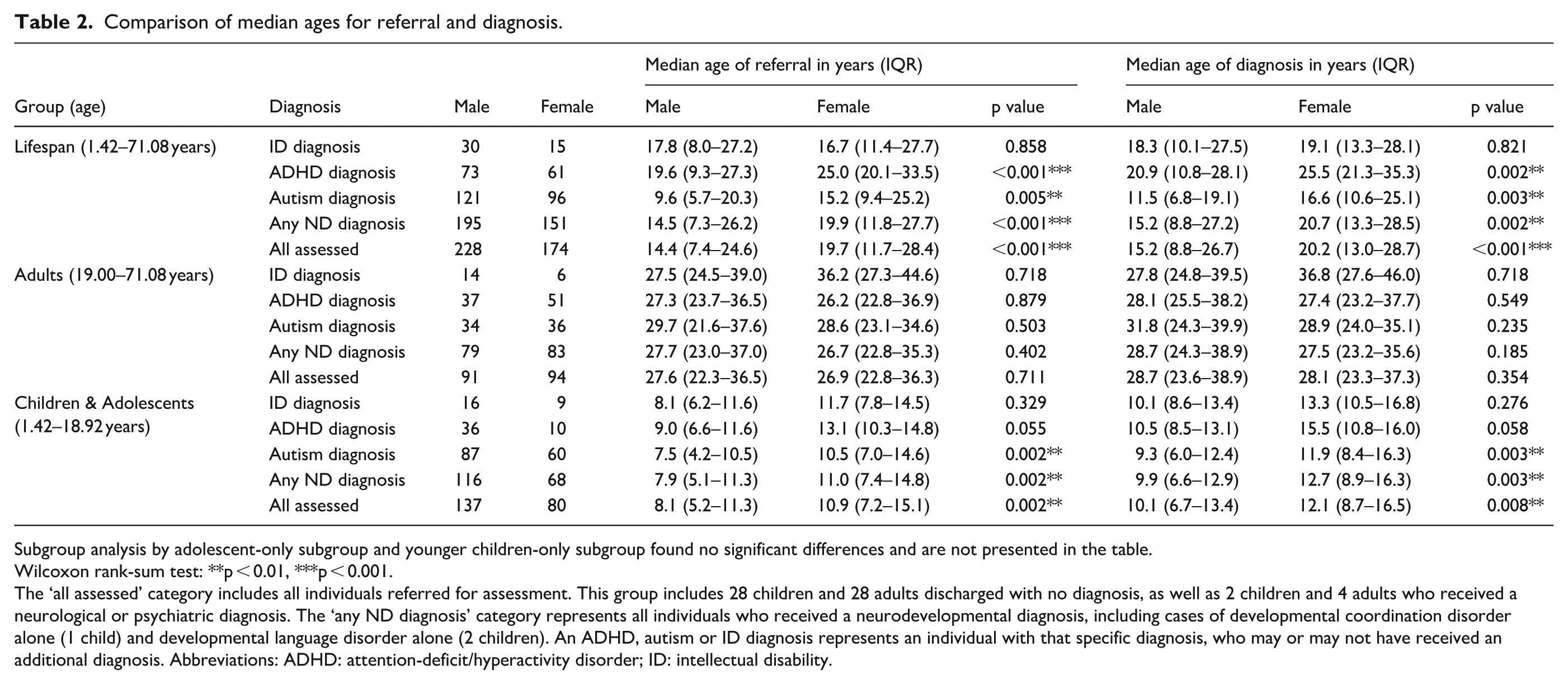
Subgroup analysis by adolescent-only subgroup and younger children-only subgroup found no significant differences and are not presented in the table.
Wilcoxon rank-sum test: **p < 0.01, ***p < 0.001.
The ‘all assessed’ category includes all individuals referred for assessment. This group includes 28 children and 28 adults discharged with no diagnosis, as well as 2 children and 4 adults who received a neurological or psychiatric diagnosis. The ‘any ND diagnosis’ category represents all individuals who received a neurodevelopmental diagnosis, including cases of developmental coordination disorder alone (1 child) and developmental language disorder alone (2 children). An ADHD, autism or ID diagnosis represents an individual with that specific diagnosis, who may or may not have received an additional diagnosis. Abbreviations: ADHD: attention-deficit/hyperactivity disorder; ID: intellectual disability.
Comparison of current data with earlier study in Scotland
To address research question 3 (changes in male-to-female ratios since previous research), data from a 2014 study (Rutherford et al., 2016) were used, which reported male-to-female ratio data for individuals seeking an autism diagnosis, applying the same age cut-offs as the current study. A comparison of findings is presented in Table 3. Comparison shows a reduction in male-to-female ratios across all age groups. The most pronounced change is observed in younger children (0–9 years), where the ratio fell from 5.50 to 2.21. Decreases across adolescents and adults indicate a trend towards more recognition of older autistic females over time.
A comparison of MFR data with Rutherford 2016 (autism only).
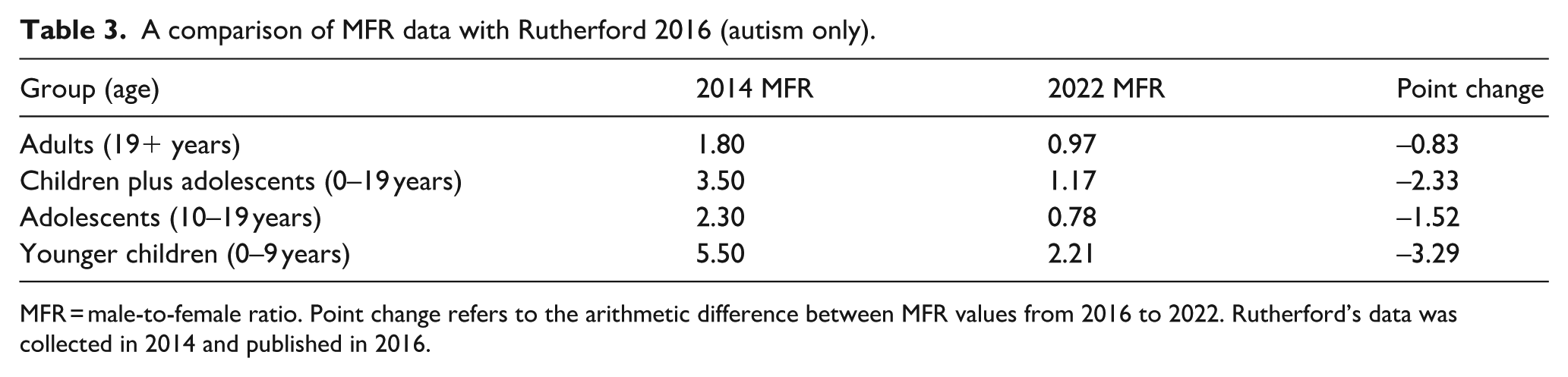
MFR = male-to-female ratio. Point change refers to the arithmetic difference between MFR values from 2016 to 2022. Rutherford’s data was collected in 2014 and published in 2016.
Discussion
This study examined male-to-female ratios (MFRs) and ages at referral and diagnosis among individuals seeking assessment for neurodevelopmental differences. Results indicate that more females are now being identified and diagnosed compared with data from 2014. Sex ratios are more balanced at older ages; however, a marked male–female asymmetry persists in younger groups. Males were referred and diagnosed earlier than females, with median age differences exceeding five years in some cases. These age gaps are significant from a clinical and developmental perspective. Findings suggest that there is a delay in identification and referral of females.
Our analysis offers insights into male/female ratios for neurodevelopmental differences, providing a view that contrasts with the narrower focus of previous research. While most studies concentrate on specific diagnoses, we examined these collectively. Our findings broadly correspond with prior research showing higher male ratios for developmental differences in children than adults (Zablotsky et al., 2019). Precise lifetime male-to-female ratios are not well established for neurodevelopmental differences as a broader group, although an MFR of 1.7 for children has been reported (Bolte et al., 2023). Our study’s ratio of 1.71 for individuals with any neurodevelopmental diagnosis under 19 years aligns closely with this figure.
Considering the previous Scottish research provides an opportunity to evaluate changes over time. The comparison to data from 2014 (Rutherford et al., 2016) suggests a consistent reduction in male-to-female ratios in autism across all age groups over time. The most substantial shift occurred in younger children, who, while still displaying the highest MFR overall (showing more males), experienced the largest overall decrease. Among adolescents, there was a smaller reduction, but the data showed a reversal, with females outnumbering males in the most recent assessment. Adults demonstrated the smallest change overall, but also showed a reversal in MFR, with slightly more females than males identified. Despite this, females, and particularly younger girls, still experience later diagnoses compared to boys, with delays occurring before referral, a finding supported by recent international studies (Smith et al., 2024). Reductions in ratios reflect changes in identification of girls and women, with several interacting factors affecting this. Evolving diagnostic practices, including broader criteria emphasising more diverse presentations, and clinician training (Cook et al., 2024; Murphy et al., 2023), have likely altered recognition. Increased assessment-seeking by females has also been fuelled by greater public awareness, online neurodivergent communities and advocacy, particularly among older women recognising traits later in life (Leedham et al., 2020).
A review of individual diagnoses and wider research is also enlightening. For ID, our study’s lifespan MFR of 2.00, with a ratio of 2.33 for adults and 1.00 for children and adolescents combined, aligns with the reported ranges of 1.0–2.2 for children and 1.1–1.4 for adults (Bolte et al., 2023). Our higher ID ratio for younger children (3.33) may reflect early identification trends and the relatively small numbers included in our research with this diagnosis. In ADHD, our lifespan MFR of 1.20, with higher MFRs of 3.60 for children and adolescents and 6.67 for younger children, contrasts with the literature, which indicates ratios of 2.3 for children and 1.6 for adults (Bolte et al., 2023). Our MFR of 0.73 for adults (showing more females than males with ADHD diagnosed in this cohort) could suggest an emerging trend of older females seeking assessment for ADHD in Scotland. Within our adult sample, ADHD was common, with 42% of adults diagnosed with ADHD (48% of adult females and 38% of adult males received an ADHD diagnosis on completion of their assessment). Conversely, in children, ADHD was less common, with a diagnosis rate of 12%, with 8% of girls and 15% of boys diagnosed. For autism, our lifespan MFR of 1.26 contrasts with the literature’s typically higher ratio of 3 males for every female (Bolte et al., 2023). We observed ratios of 1.45 for children and adolescents and 2.21 for younger children, with an unusually low ratio of 0.94 for adults. This again indicates an emerging trend of older autistic females seeking assessment.
Evidence found of sex-associated differences warrants further consideration of why this might be the case. As noted, we found neurodivergent females are more likely to receive their diagnosis later, and that there were slightly greater numbers of women represented in adult diagnostic groups. This suggests a higher likelihood of females being missed during childhood. It is clear from the wider literature that neurodivergent girls and women experience barriers to earlier diagnosis and lower diagnostic rates compared to their male peers (Zener, 2019). An estimated 80% of autistic females remain undiagnosed by age 18 (McCrossin, 2022). Similar disparities exist in ADHD assessments, where diagnostic rates reflect a male bias in childhood but show more parity in adulthood, suggesting delayed identification in younger girls (May et al., 2019).
The full range of mechanisms by which sex or sex-related attributes could influence neurodevelopmental profiles, and the late recognition of girls and women, involves interacting biological and psychological processes (Bolte et al., 2023). For both autism and ADHD, diagnostic markers in females often emerge later, particularly during later adolescence or young adulthood (Lai et al., 2015). The DSM-5 (American Psychiatric Association, 2013) notes that individuals may be referred later in life when demands begin to exceed coping mechanisms. Historically, the core diagnostic characteristics of autism were established through observations of boys (Van Wijngaarden-Cremers et al., 2014), leading to tools constructed with unconscious biases against female markers (de Giambattista et al., 2021). Current diagnostic instruments and processes, based mainly on males, may therefore fail to capture the nuanced ways gendered expectations influence presentation of neurodivergence. It has been proposed that in the expression of neurodivergent traits across men and women exist mainly at the level of behavioural exemplars, the same characteristics are expressed but are manifested as different behaviours, and not all of these are assessed for in current diagnostic tools (Cook et al., 2024). For example, neurodivergent girls and women may present with fewer observable traits, have more advanced social skills or have more socially acceptable special interests (Zener, 2019). Masking and camouflaging strategies, commonly employed by neurodivergent females, can also delay diagnosis (Hull et al., 2017; Tubio-Fungueirino et al., 2021).
Diagnosis is also influenced by societal assumptions (Lockwood Estrin et al., 2021). Poorer recognition of females at a younger age suggests that family and social factors play an important role. Parents may interpret behaviours differently based on gender, with needs of boys more likely to prompt concern and referral than similar behaviours in girls (Geelhand et al., 2019). Stigmatisation may prevent parents from making their children aware of their autism (Urbaniak & D’Amico, 2025). Media portrayals further exacerbate disparities, with newspapers, films and television portraying autistic males more frequently (Karaminis et al., 2025). These societal influences and gendered expectations that encourage girls to conform or mask their traits may contribute to delayed recognition and referral.
Later timing of diagnosis highlights the linked issues of underdiagnosis and misdiagnosis. Co-occurring or secondary mental health challenges are also important considerations. Over 70% of autistic individuals experience one or more co-occurring lifetime psychiatric conditions (Curnow, Rutherford, et al., 2023; DeFilippis, 2018). Previous literature also suggests that later-diagnosed women and girls are more likely to have their experiences misunderstood as internalising conditions and misdiagnosed with eating disorders, borderline personality disorders, anxiety and depression (Bougeard et al., 2021; Smith et al., 2024; Young et al., 2020). Co-occurring conditions more frequently seen in females may mask or delay diagnosis, while traits more commonly associated with boys, such as hyperactivity, may expedite the process (Dan, 2021). Mental health challenges resulting from misdiagnosis, missed diagnosis and years of living in unsupportive environments lead to secondary issues like anxiety or low mood, which are then misinterpreted as the primary condition (Lockwood Estrin et al., 2021). This misinterpretation can lead to a lifetime of poor self-understanding, limited access to appropriate support and inaccurately targeted interventions.
Practice implications
It is important to acknowledge that these findings do not represent a straightforward picture. The assumption that higher rates of diagnosis reflect an accurate representation of prevalence should be treated with caution. Increases may reflect improved availability and access to services, particularly for adults, as well as greater awareness of female presentations in clinicians and society. Diagnostic patterns are shaped by a complex interplay of need, demand, service structures and professional decision-making. Nevertheless, while the evidence is not definitive, the study offers suggestions that will likely be useful in guiding service development and professional practice.
Findings highlight the need for greater awareness and earlier identification of neurodivergent females, particularly in younger age groups. Current disparities in referral and diagnosis ages, which favour males, point to barriers in accessing assessment and support. Consideration is also needed for older adults. In this study, 34 individuals were diagnosed after age 40, with the oldest at 71, reinforcing concerns that many remain unidentified for extended periods (Robison, 2019). Later referrals and diagnoses for ADHD also indicate systematic challenges that require action.
To reduce missed or incorrect diagnoses, clinicians must be confident in identifying neurodivergence in both males and females. Service models have historically assumed a lower prevalence and a male majority. Future provision must instead recognise higher population rates of 10%–17% (Bolte et al., 2023; Maciver et al., 2023) and the over-representation of neurodivergent people in mental health services (Eberhard et al., 2022). This shift requires updated professional learning, a move away from reliance on specialist teams, and the inclusion of neurodivergent voices in service design.
Assessment and support should be embedded across mainstream health and education, using a lifespan, neuro-affirming approach. Non-specialists, including primary care, educators and parents, should be trained to recognise differences and provide early, low-level support. Such supports can address emerging needs, reduce escalation and prevent missed opportunities for recognition. Professionals must also reflect on male-oriented biases, while mental health services should routinely assess for neurodivergence across the lifespan. Adult services, in particular, must be prepared to support women who may have masked for many years. Achieving this will require comprehensive professional development across multiple levels and disciplines, alongside significant increases in workforce expertise and resourcing.
Future research
Recent research has identified priorities for autistic adults in Scotland, including mental health support, diagnosis and the needs of women (Cage et al., 2024). These priorities align with global research (Benevides et al., 2020; O’Neill & O’Donnell, 2024). Studies that drive meaningful change are also widely supported (Roche et al., 2021). Our research reaffirms the critical need for research into diagnostic pathways, particularly for females. The ‘lost generation’ of women diagnosed later in life shows the significant gap in earlier diagnosis. This should include a focus on understanding female presentations, which are often overlooked, why younger neurodivergent girls face delays in the diagnostic pathway, and examining masking/unmasking, an area with particularly limited empirical research (Miller et al., 2021). In addition, research should investigate how internalising diagnoses, such as depression or personality disorders, can mask or mislead the identification of autism and ADHD in women (Au-Yeung et al., 2019).
In Scotland, adult neurodevelopmental services typically have thresholds that require moderate to severe mental illness. An area of investigation is to explore reasons for referral, hypothesising that females may be referred for mental health concerns, with the possibility of neurodivergence emerging later. Longitudinal research into referral reasons across the lifespan would also offer valuable insights to help address why neurodivergent girls are overlooked in early years. Such research would support the need for referrer-based education, for example, for paediatricians and families.
A final key direction is defining what constitutes a neuro-affirming assessment and diagnostic processes (Rutherford & Johnston, 2023). This requires prioritising coproduction and collaboration with neurodivergent individuals. Historically, support and diagnostic assessments have been framed within a medical, crisis-oriented model (Bottini et al., 2024). Shifting to a neuro-affirming, rights-based model could lead to more anticipatory support and different approaches to assessment and diagnosis.
Limitations
Our findings and Rutherford et al.’s share similarities, but comparisons are limited by methodological differences. Both studies used retrospective case note reviews. However, Rutherford et al. randomly sampled services, extracting data on the 10 most recent autism diagnoses (n = 150), while our study invited voluntary participation and consecutively sampled cases in reverse chronological order (n = 217). Our voluntary participation may have attracted ‘well-performing’ services with more efficient processes. However, broader sampling also likely captures a wider range of current practices than the previously narrower sample.
Further limitations include the relatively small sample size, which limits conclusions, particularly for subgroups. The sampling reflects recent clinical practice but does not include all services across Scotland. As noted, reliance on voluntary participation may not have captured a representative population of diagnosing services. This approach was chosen to minimise impact on staff and technical burden. Still, it may have excluded teams under operational strain (who may have self-selected not to participate), potentially missing important data.
Limitations relating to the detail of data collected include the absence of information on the level of ID. In addition, the number diagnosed with ID in our study was very small and would not allow for meaningful subgroup analysis. We did not gather data on co-occurring mental health conditions. This restricts our ability to explore factors such as the influence of mental health conditions on later referral. Furthermore, sex was recorded according to sex assigned at birth rather than gender identity.
Biases associated with the adult data should be acknowledged. Comparing findings across the lifespan is challenging, as adult services typically focus on individuals with more severe mental illnesses, while children’s services adopt a universal approach. Outcomes for adults are also influenced by long-standing, complex issues such as severe access problems and the dismissal of referrals in primary care. This study did not explore these service gaps and issues, nor was their potential impact on girls and women examined.
Conclusion
Demographics of people seeking assessment and diagnostic practices are changing, leading to changes in identification of neurodivergent females, yet barriers and delays persist, particularly for younger girls. The study revealed more males in childhood referrals and diagnoses, which balanced out with age. Despite this, males continue to be referred and diagnosed at younger ages compared to females. It appears there have been positive changes in identifying autistic females since the previous 2014 research completed in Scotland. Nevertheless, our findings emphasise the need for ongoing refinement of diagnostic practices and further research to address sex-related issues in neurodevelopmental assessment.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251383343 – Supplemental material for Are we getting better at identifying and diagnosing neurodivergent girls and women? Insights into sex ratios and age of diagnosis from clinical population data in Scotland
Supplemental material, sj-docx-1-aut-10.1177_13623613251383343 for Are we getting better at identifying and diagnosing neurodivergent girls and women? Insights into sex ratios and age of diagnosis from clinical population data in Scotland by Donald Maciver, Anusua Singh Roy, Lorna Johnston, Marie Boilson, Eleanor Curnow, Victoria Johnstone-Cooke and Marion Rutherford in Autism
Footnotes
Acknowledgements
We wish to thank and acknowledge the contributions of stakeholders, the Scottish Government, neurodivergent people who are experts by experience and families, and health and education professionals who have supported this work. Special thanks are due to the diagnosing teams for their time and effort in extracting data for this study.
Ethical considerations
Ethical approval for the study was obtained from the Queen Margaret University Ethics Committee and the NHS Scotland Public Benefit and Privacy Panel for Health and Social Care.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The National Autism Implementation Team completed this work and are funded by the Scottish Government.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Data availability statement
Please contact the corresponding author for study data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.