
Abstract
Autism is a neurodevelopmental condition, characterized by altered social communication and repetitive behavior. Typically diagnosed in early childhood, screening and diagnosis at a later age can be challenging, particularly in girls who exhibit a wider range of behaviors and characteristics. This study aimed to examine the Childhood Autism Spectrum Test–Hebrew version in a clinically referred Israeli sample, and to identify items that best discriminate between autistic and non-autistic boys and girls. Parents of 211 autistic (retrospectively reviewed) and 192 non-autistic children, aged 4–12 years, completed the Childhood Autism Spectrum Test–Hebrew version. Results indicated good discriminatory power, with an area under the curve of 0.93. A cutoff of 9 offered optimal sensitivity of 0.93 and specificity of 0.82. The addition of a more focused sex-specific analysis using items that best discriminated autistic from non-autistic boys and girls significantly improved the overall identification rate of autism, particularly in girls. The Childhood Autism Spectrum Test–Hebrew version was positively correlated with the Autism Diagnostic Interview–Revised but not with Autism Diagnostic Observation Schedule-2. Findings underscore the importance of considering sex differences in autism screening and the potential value of sex-specific screening. Future research should focus on replicating these findings in a larger, diverse, prospective study.
Lay abstract
Autism is a neurodevelopmental condition, characterized by social communication alterations and restricted, repetitive behaviors. Typically diagnosed in early childhood, screening and diagnosis at a later age can be challenging, particularly in girls who exhibit a wider range of behaviors and characteristics. Our study set out to examine the effectiveness of the Hebrew translation of the Childhood Autism Spectrum Test, a parent report questionnaire, in identifying these diverse characteristics of autism within an Israeli sample of boys and girls. We examined parent reports on 403 (211 autistic, 192 non-autistic) children, aged 4–12 years. Results revealed the Childhood Autism Spectrum Test–Hebrew version was a valuable tool in differentiating between autistic and typically developing children, correctly identifying 93% of children with autism and 82% of typically developing children. In addition, specific items of the Childhood Autism Spectrum Test–Hebrew version were particularly useful in differentiating between autistic and non-autistic boys and autistic and non-autistic girls. Using these items, in addition to the overall score of the questionnaire, increased the correct identification of children as autistic or typically developing, especially in girls. The Childhood Autism Spectrum Test–Hebrew version test results corresponded well with the Autism Diagnostic Interview–Revised, which relies on parental input, but not with the clinician-administered Autism Diagnostic Observation Schedule-2. Our findings highlight the potential benefits of gender-specific tools to better support correct identification of autism in boys and in girls. More research is recommended to further explore these gender differences and to validate our findings with a larger, diverse group.
Background
Autism spectrum disorder (ASD) represents a diagnostic conundrum in the field of neurodevelopmental disorders. While early markers of autism can be identified in the first 2 years of life (Barbaro & Halder, 2016), many children receive a formal diagnosis only around the age of 5 years (van ’t Hof et al., 2021). This diagnostic timeline varies based on geographical and regional contexts (Kentrou et al., 2019; Rutherford et al., 2016). Current data suggest that in the United States, 1 in 36 eight-year-olds is diagnosed with autism (Maenner et al., 2023). In Israel, the prevalence ranges between 1.56%–1.83% for this age bracket (Dinstein et al., 2024). Since autism diagnosis relies on behavioral measures, the more salient its manifestation, the earlier the diagnosis can be made. However, for those individuals who have a more subtle manifestation of autism, or for those with good intellectual capacities, diagnosis may be delayed until the demands for social functioning exceed available resources (American Psychiatric Association, 2022). Contributing to this challenge are coexisting psychiatric conditions, found in 85% of those diagnosed with autism (de Giambattista et al., 2021). To improve the quality of life and long-term outcomes of autistic people, diagnosis should be offered as early as possible (Remington et al., 2007; Vivanti et al., 2016). Hence, the school-aged children whose autism diagnosis has been missed at early development should be offered appropriate screening and diagnostic services (Soke et al., 2018). However, as a result of its heterogeneous manifestation, and of overshadowing by co-occurring conditions, autism may be more difficult to diagnose in older children. Moreover, with greater emphasis placed on early diagnosis, clinicians working with school-aged children may be less experienced in diagnosing autism (Soke et al., 2018).
Detecting autism in girls and boys
The last decade has seen a sharp increase in the diagnosis of autism in females. However, autism is still more common in males. According to the latest report from Autism and Developmental Disabilities Monitoring (ADDM), the overall male-to-female prevalence ratio was 3.8, with overall ASD prevalence of 43.0 among boys and 11.4 among girls (Maenner et al., 2023). When examined separately in individuals with and without intellectual disabilities, male-to-female ratio reached 11:1 in individuals with autism and no intellectual disabilities, whereas this ratio dropped to 2:1 in individuals with autism and moderate-to-severe intellectual disabilities (de Giambattista et al., 2021). Recent studies with large cohorts of children report greater female representation, with sex ratios of 2–5:1 (Lai et al., 2015). Nevertheless, current reports argue that female representation in research is still lacking, due to over exclusion of females from research studies (D’Mello et al., 2022), or to unique profiles of autistic features in females (Hiller et al., 2016). It has been argued that these diagnostic caveats, if given proper attention, could balance the sex ratio (Burrows et al., 2022). A meta-analysis examining the male to female ratio in autism research suggested that in studies that actively tested participants for autism, there were on average 24 girls per 100 cases of ASD, whereas in studies which relied on participants’ existing ASD diagnoses there were only 18 females per 100 ASD cases. The authors concluded that there are girls in the general population who, if assessed, would meet the criteria for autism, but who do not end up with a clinical diagnosis (Loomes et al., 2017). If indeed, the real number of autistic girls is close to that of boys, then screening tools that are adjusted for girls may help identify them more effectively.
Several explanations for sex differences in the autistic spectrum have been suggested over the years. One explanation viewed the differences in the frequency between males and females on the autism spectrum as real, suggesting that autism is an expression of an extreme male brain (EMB) (Baron-Cohen, 2002). The female “protective” effect (FPE) model, contrary to the EMB, assumed there are specific factors that protect females from developing autism, arguing that females need a greater genetic/mutational load to develop autism (Jacquemont et al., 2014). Another perspective suggested that females are more inclined to camouflage, or at the very least, are more motivated to disguise some of their autistic characteristics (Attwood, 2008), and that this may be the reason for female’s later identification and diagnosis on the autistic spectrum. Furthermore, the camouflaging of autistic traits in females could have resulted in the construction of autism criteria based mostly on male behavior (Lai et al., 2017). Therefore, focusing on the unique characteristics of autism in females may allow for better understanding of their needs and adaptation of services offered to them. Interestingly, the examination of sex differences in the manifestation of autism symptomatology has come up with conflicting findings over the years. Overall, no consistent sex differences have been found either for the social communication (SC) or for the restricted, repetitive behaviors (RRB) clusters (Song et al., 2021), highlighting the need for a more fine grained examination of sex differences in autism.
The Childhood Autism Spectrum Test
The Childhood Autism Spectrum Test (CAST; Scott et al., 2002), previously known as the Childhood Asperger Syndrome Test, has gained evidence as a useful screening instrument for identifying subtler or milder manifestations of autism, in kindergarten and primary school-aged children (4–11 years) (Baron-Cohen et al., 2009). The cutoff point set by the authors was 15. The CAST has been translated and adapted into over 22 languages and cultures.
Psychometric properties of the CAST have been reported for the Spanish, Mandarin, Bulgarian, and Brazilian translations (Morales-Hidalgo et al., 2017; Ribeiro et al., 2022; Sun et al., 2014a; Vulchanova, 2016), but only the Spanish study examined a suitable cutoff for their sample (15 and 13 for a shortened version of the CAST). In the context of screening, it is essential to note that different values and cutoffs should be considered when screening the general population versus a clinically referred population (which is the case in the current study). The prevalence of the condition may be significantly higher in referred populations, necessitating a more sensitive cutoff. A sensitive screening tool can be advantageous in improving services in tertiary diagnostic centers (Golan et al., 2023).
When defining the clinical cutoff for autism screeners, there have been suggestions to utilize positive predictive value (PPV) and negative predictive value (NPV) in determining appropriate levels of specificity and sensitivity (Bezemer et al., 2021; Parikh et al., 2008). PPV represents the likelihood that individuals who surpass the cutoff actually have autism, and NPV – the likelihood that individuals who score below the questionnaire’s cutoff do not have autism. PPV and NPV account for the prevalence of the condition within a given population, in our case- children reffered for autism assessment in tertiary diagnostic centers. The original CAST exhibited a sensitivity of 100% and a specificity of 97% in detecting autism, although the PPV was only 50%. Therefore, it was recommended to utilize the tool in a clinical setting where the prevalence of true positives may be higher (Williams et al., 2005), as tested in the current study. The CAST has been used widely in Israeli clinical settings, but only one study reported preliminary findings with a specificity of 91.4% and a sensitivity of 93.3% for a cutoff of 12 (Gev, 2014). However, since most of this reported autism group was diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (4th ed.; DSM-IV) criteria, these findings should be considered carefully. Therefore, the current study examined the psychometric properties of the CAST in a clinically referred sample of Israeli children.
Sex differences on the CAST
So far, sex differences on the CAST were examined mostly in a general population sample. CAST scores were used to investigate sex differences in a Social Communication Research and Epidemiological (SCORE) study in UK primary schools (Baron-Cohen et al., 2009). Williams et al. (2008) found that in a British general population sample, boys scored significantly higher than girls. This pattern was also found in studies of the Spanish and Mandarin versions of the CAST (Morales-Hidalgo et al., 2017; Sun et al., 2014b). Dworzynski et al. (2012) screened children from the general population for traits of autism at the age of 8 years using the CAST and reported that girls who exhibited traits of autism and met the diagnostic criteria for ASD often had additional behavioral problems or lower cognitive abilities. This pattern was not observed in boys with similar autism traits. This suggests that the current diagnostic process might overlook autistic girls unless they exhibit additional problems, potentially indicating a bias in the diagnostic criteria or practices toward the male presentation of autism. To our knowledge, no study has examined differences between clinically diagnosed autistic girls and boys on the CAST. Moreover, the understanding of how sex may alter the characteristic features of autism as described by the CAST remains limited.
The current study
This study aimed to (1) find the appropriate cutoff on the Hebrew translation of the CAST (henceforth CAST-Heb) on a clinically referred sample, bearing in mind PPV and NPV, and (2) to determine what items best discriminate, separately, between autistic and non-autistic boys and between autistic and non-autistic girls. In addition, (3) this study sought to analyze the correlations of the CAST-Heb with Autism Diagnostic Observation Schedule (ADOS) and Autism Diagnostic Interview–Revised (ADI-R) as a validity analysis, and the questionnaire’s internal consistency for reliability analysis.
Method
Participants
The total sample consisted of 403 children aged 4–12 years. The clinical group included 211 children: 170 boys (age: M = 8.72, SD = 2.29) and 41 girls (M = 8.68, SD = 2.41), whose records were retrieved from two clinical centers, operated by OTI – the Israeli Association for Autism. These two tertiary centers provide diagnostic assessment services for children and adults with autism. The CAST-Heb was completed by parents as a preliminary stage of their application for diagnostic assessment, and before an ASD diagnosis was given. Demographic data of the clinical group were collected from the client’s records. A waiver of consent for this retrospective record review was given by the Ness Ziona–Be’er Ya’akov Mental Health Center’s Helsinki Committee (#543). Children in the clinical group were diagnosed by psychologists and child psychiatrists according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) criteria. Diagnoses were based on the ADI-R and the ADOS-2.
The non-autistic sample consisted of 192 participants (92 girls), aged 6–12 years (boys: M = 8.87 and SD = 1.93, girls: M = 8.88 and SD = 1.94). Non-autistic participants’ parents were recruited from the general community through their acquaintance with undergraduate research assistants. Children with a parent-reported diagnosis of autism or children attending special education were excluded from this sample. Ethical approval for the non-autistic sample was given by the first author’s department of psychology ethics committee. The two groups were comparable on age (t(398.12) = −0.77, NS) and residence place type (χ2(1) = 1.43, NS). However, there were significant differences in the boy-to-girl ratio, with a greater representation of non-autistic girls (χ2(1) = 36.89, p < 0.001). To rectify this imbalance and ensure a comparable boy-to-girl proportion for the analyses of the entire sample, a random exclusion of 68 non-autistic girls was conducted, resulting in group comparability on sex (χ2(1) = 0.000, p = NS).
Measure
The CAST (Scott et al., 2002) is a widely used questionnaire to screen for autism in children. It consists of 37 items, including 31 target items that assess specific autism-related behaviors. Parents or caregivers complete the questionnaire by indicating “yes” or “no” for each behavior. Scores range from 0 to 31, with higher scores indicating more autism-related behaviors. The CAST has gained evidence as a useful screening instrument for identifying subtler or milder manifestations of autism, in kindergarten and primary school-aged children (4–11 years) (Scott et al., 2002). The CAST test–retest reliability was found to be good, with a kappa statistic for agreement of 0.70 and a correlation between the two test scores of 0.83 (Spearman’s rho). The CAST has good test–retest reliability in a large sample of children from mainstream schools (Williams et al., 2006). The sensitivity of the original version of CAST, at a designated cutoff point of 15, was 100%; the specificity was 97%; and the PPV was 50% (Williams et al., 2006). The Hebrew version of the CAST has been translated by the last author, with support of the original instrument’s creator.
Analysis
Power analysis was performed for a balanced one-way analysis of variance (ANOVA) on the current sample, with four groups (autistic boys, autistic girls, non-autistic boys, and non-autistic girls). The achieved power for detecting a medium effect size was as follows: autistic boys (power = 1.00), autistic girls (power = 0.99), non-autistic boys (power = 1.00), and non-autistic girls (power = 1.00).
Receiver operating characteristic (ROC) curve analyses were conducted in SPSS, version 23. The determination of the optimal cutoff value, sensitivity, specificity, PPV, NPV, and accuracy in a clinically referred population was performed using R Studio (version 2023.03.1+446). This population had an incidence rate of 68%. This incidence rate was ascertained from data gathered across the clinical centers that participated in this study, reflecting the observed positive diagnostic outcomes. KR-20 was computed to examine internal consistency. Pearson correlations between CAST-Heb scores and participants’ age were calculated for the entire sample and separately for each sex. Correlations between CAST-Heb scores and ADI-R and ADOS-2 scores were calculated for the clinical group only. Finally, to understand the role of discriminating items in boys and in girls, two separate discriminant analyses were conducted.
Community involvement
There was no community involvement in this study.
Results
Mean CAST-Heb scores were computed based on sex and diagnosis categories, after rectifying a previously observed imbalance in the boy-to-girl proportion across the groups (see Table 1).
Mean CAST-Heb Scores by Group and Sex.
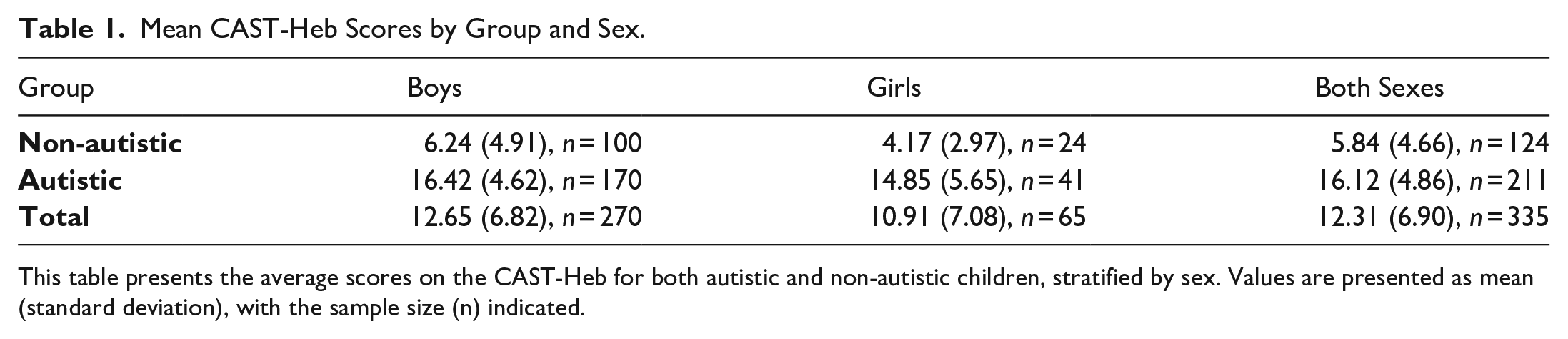
This table presents the average scores on the CAST-Heb for both autistic and non-autistic children, stratified by sex. Values are presented as mean (standard deviation), with the sample size (n) indicated.
A univariate ANOVA was conducted to test the effects of sex and diagnosis (autistic/non-autistic) on CAST total scores. Results, illustrated in Figure 1, indicated a significant main effect for sex (F(1,331) = 7.18, p < 0.01, ηp2 = 0.02) and diagnosis (F(1,331) = 235.73, p < 0.001, ηp2 = 0.42). However, the interaction effect between sex and diagnosis on CAST-Heb scores was not statistically significant (F(1,331) = 0.137, NS), indicating that group effects on CAST-Heb scores did not differ significantly between boys and girls. The model explained 53.0% of the variance in CAST-Heb scores (adjusted R2 = 0.53).
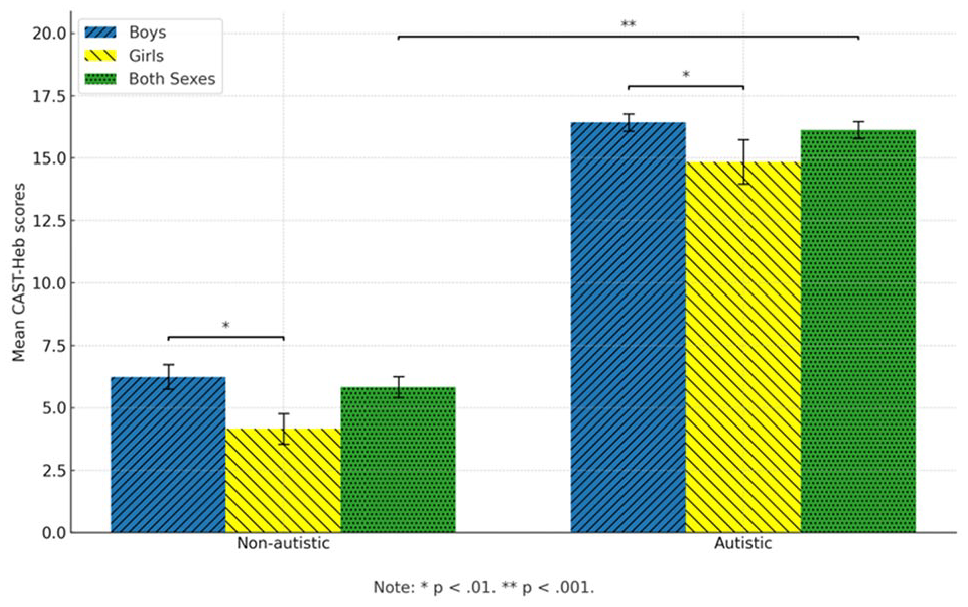
Mean CAST-Heb scores across two diagnostic groups (non-autistic and autistic) stratified by sex (boys, girls, both sexes). Error bars represent the standard error of the mean. Significance levels are indicated by horizontal lines, with p < 0.01 comparing boys and girls within each diagnostic group and p < 0.001 comparing non-autistic and autistic groups for the combined sexes.
Reliability for the CAST-Heb questionnaire’s 31 items was determined using KR-20, a measure of internal consistency specifically suited for dichotomous items. The reliability was found to be high (KR-20 = 0.90). Further subgroup analyses revealed varying reliability estimates across different groups, categorized by sex and diagnostic status. KR-20 was 0.86 for non-autistic boys and 0.79 for autistic boys. For non-autistic girls, KR-20 was 0.70, whereas for autistic girls, it was 0.82. The diagnostic performance of the CAST-Heb was evaluated using ROC analysis. To calculate the optimal cutoff, we used the “cords” function from the pROC package in R to retrieve the cutoff that maximizes the Youden’s index which takes into account both the sensitivity (true positive rate) and specificity (true negative rate) of the classification model. It measures the effectiveness of the model in correctly identified positive cases and correctly identified negative cases simultaneously.
As shown in Figure 2, the CAST-Heb demonstrated good discriminatory power, with an area under the curve (AUC) of 0.93. The optimal cutoff value for distinguishing between positive and negative cases was determined to be 9. At this cutoff, the test showed a sensitivity of 0.93, indicating a high rate of correctly identifying autistic children. The specificity was 0.82, suggesting a more modest, but still good ability to correctly classify non-autistic children. Accounting for the high prevalence in this clinically referred sample, PPV was 0.92 and NPV was 0.85. A total of 96% of the autistic boys, but only 80% of the girls, will have been correctly referred to diagnostic assessment according to this cutoff.
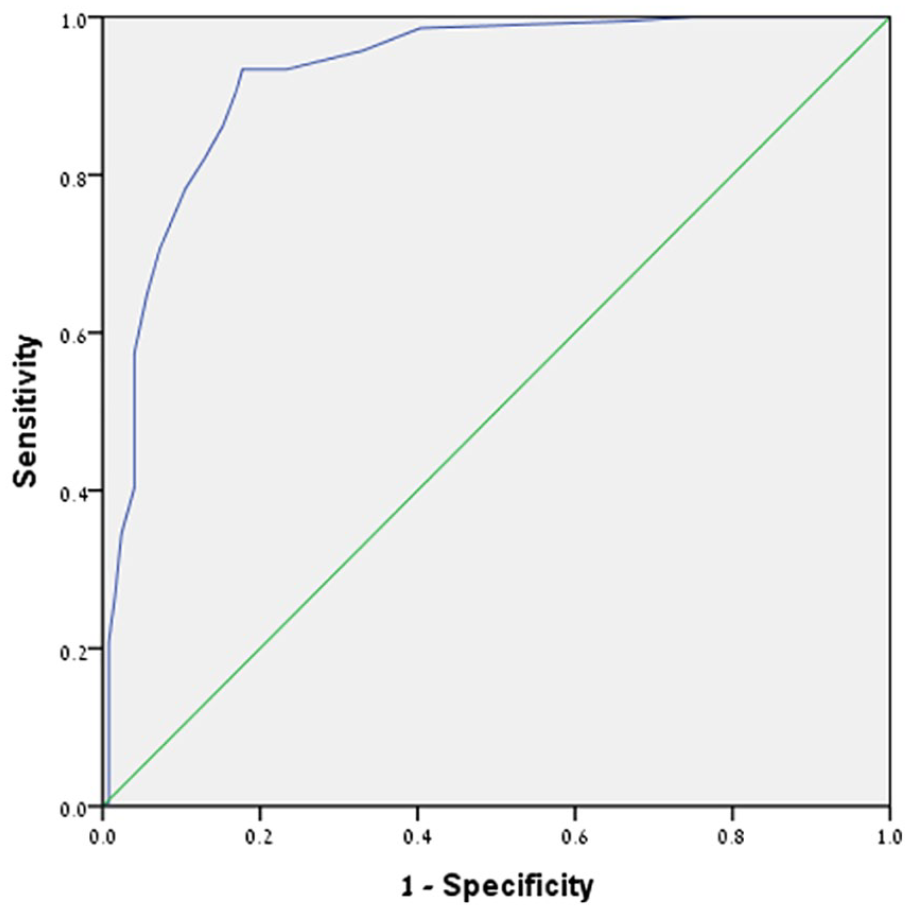
Receiver Operating Characteristic (ROC) Curve for the CAST-Heb. This graph displays the sensitivity versus 1-specificity of the CAST-Heb at varying thresholds, providing insights into the tool’s diagnostic performance in distinguishing between autistic and non-autistic individuals.
Separate analyses by sex
To further investigate the discriminatory power of individual CAST-Heb items, we conducted separate discriminant analyses for boys and girls, thus permitting a specific examination of classification outcomes within each sex group. A stepwise method was applied in the discriminant function analysis, aiding in the identification of items with the most significant effect on classification. For the analysis in girls, we used the entire sample of non-autistic girls (n=92). This decision was made to enhance the robustness of our analysis by relying on the full sample of data collected from females. This was made possible since, unlike other sections, this particular analysis did not require adjusting the autistic to non-autistic ratio between sexes.
The discriminant analysis functions were significant for boys (Wilks’ Lambda=0.44, χ2[6] = 219.68, p < .001) and girls (Wilks’ Lambda=0.27, χ2[6] = 168.98, p < .001) alike. Of the CAST-Heb items, six showed significant discriminative power for boys, and another set of six did the same for girls. One of these items, Item 1 (“Does s/he join in playing games with other children easily?”), was common across both sexes, suggesting some overlap in the factors contributing to classification outcomes for boys and girls. However, the remaining discriminative items for each sex were distinct, pointing to unique elements playing a role in the classification of autism traits for boys and girls. The varying significance and direction of the standardized canonical coefficients further underline these sex-based distinctions. Detailed findings for each sex are provided in Tables 2 and 3.
Canonical Discriminant Analysis of CAST-Heb Items for boys.
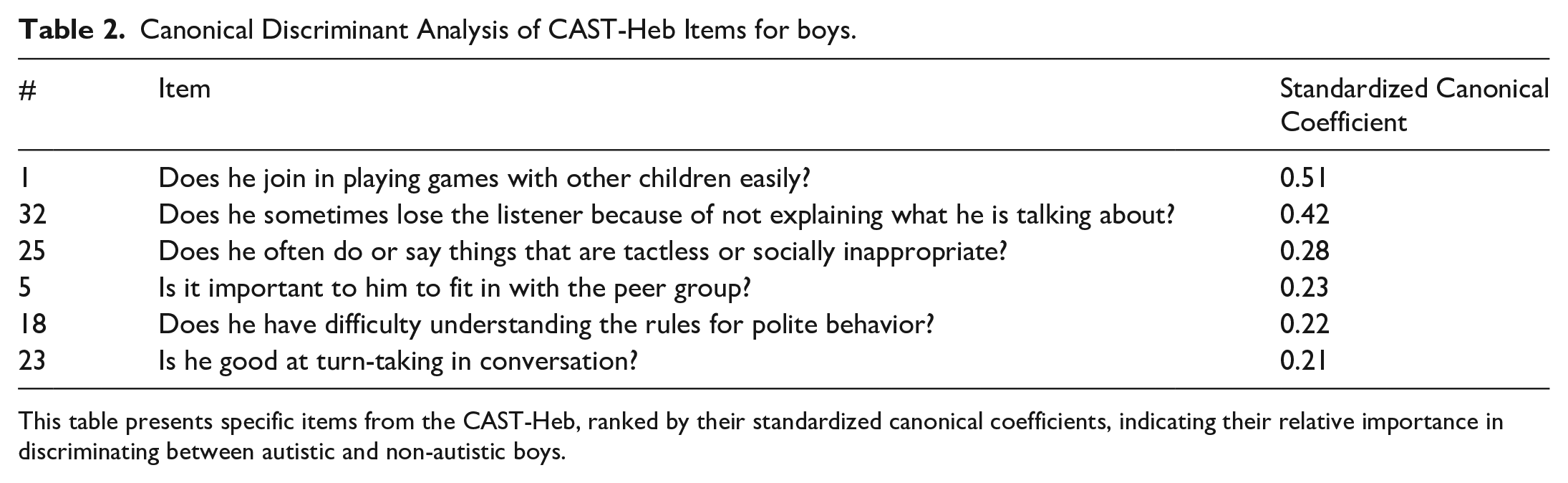
This table presents specific items from the CAST-Heb, ranked by their standardized canonical coefficients, indicating their relative importance in discriminating between autistic and non-autistic boys.
Canonical Discriminant Analysis of CAST-Heb Items for girls.
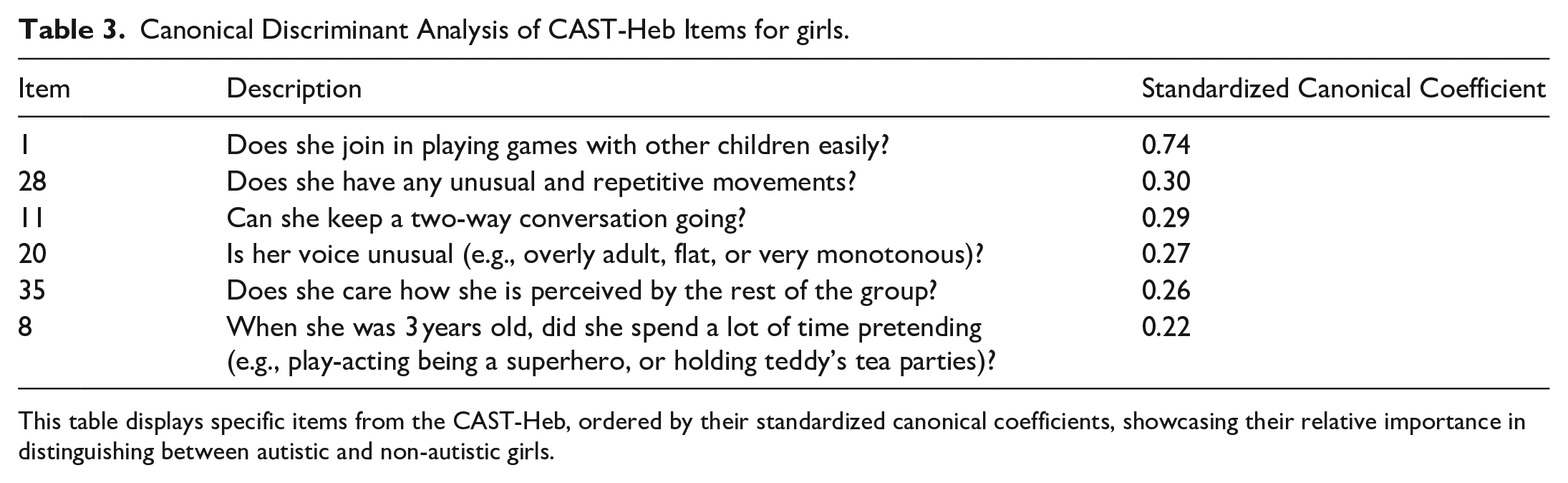
This table displays specific items from the CAST-Heb, ordered by their standardized canonical coefficients, showcasing their relative importance in distinguishing between autistic and non-autistic girls.
Having identified the initial CAST-Heb cutoff score of 9, we proceeded to further analyses. The goal was to use key sex-specific items for better identification of autism in individuals who initially scored below the cutoff. From the discriminant analyses, we identified six significant items for each sex. These selected items were utilized in a manner akin to the methodology adopted in the Modified Checklist for Autism in Toddlers (M-CHAT) as implemented by Robins et al. (2001). Based on a cutoff of at least two positive items, we were able to correctly identify an additional 50% of the remaining autistic boys and 75% of the girls who initially scored below the cutoff. This two-stage analysis significantly improved the overall identification rate, increasing it to 98% for autistic boys and 95% for autistic girls. It should be noted that this approach could have resulted in over-referral for diagnosis in 3% of non-autistic boys and 4.17% of non-autistic girls.
To elucidate potential associations between CAST-Heb scores and age, we performed Pearson correlation analyses. For the entire sample, and separately for boys and girls, no correlations were statistically significant (r = 0.07, p = NS, r = 0.09, p = NS, and r = 0.41, p = NS, respectively). Thus, our results indicate an absence of a significant association between CAST-Heb scores and age in this study’s sample.
Further, we investigated the relationships between CAST-Heb scores and scores on the ADI-R and ADOS-2 measures, which were available only for the clinical group. We found significant positive correlations between CAST-Heb scores and ADI-R social interaction (r = 0.50, p < 0.001), communication (r = 0.56, p < 0.001), and RRB (r = 0.33, p < 0.001) index scores. This indicates that higher CAST-Heb scores were associated with more reported symptoms in these ADI-R domains.
However, there were no significant correlations between CAST-Heb scores and ADOS-2 Social Affect (SA) (r = −0.05, p = NS) or RRB (r = 0.09, p = NS) scores.
Our sex-specific analysis showed similar associations between the CAST-Heb scores and the ADI-R domains. For boys, the CAST-Heb scores showed significant positive correlations with all three ADI-R domains: social interaction (r = 0.51, p < 0.01), communication (r = 0.58, p < 0.01), and RRB (r = 0.33, p < 0.01). For girls, the CAST-Heb scores were significantly correlated with both social interaction (r = 0.49, p < 0.05) and communication (r = 0.42, p < 0.05), but the correlation with RRB failed to reach significance (r = 0.30, p = NS). Interestingly, in both sexes, there were no significant associations between the CAST-Heb scores and any of the ADOS-2 index scores.
We have also examined the correlations between ADOS-2 and ADI-R measures for boys and girls: For boys, ADI social interaction and ADOS-2 SA were significantly positively correlated (r = 0.17, p < 0.05). In addition, a positive correlation was observed between ADI-R communication and ADOS-2 SA (r = 0.1
Discussion
This study aimed to determine the appropriate cutoff for the CAST-Heb in an Israeli clinically referred sample and to identify the items that best discriminate between autistic and non-autistic boys and girls. The study also sought to analyze the CAST-Heb’s internal consistency and criterion validity.
The results of the study revealed that the CAST-Heb demonstrated good discriminatory power, with an AUC of 0.93. The optimal cutoff value for distinguishing between positive and negative cases was determined to be 9. At this threshold, the test showed a sensitivity of 0.93, indicating a high rate of correctly identifying autistic children. The specificity was 0.82, suggesting a more modest, yet still good ability to correctly classify non-autistic children. These findings are consistent with previous research that has demonstrated the utility of the CAST as a screening instrument for autism in population samples (Scott et al., 2002; Williams et al., 2006).
Interestingly, the study found that different items on the CAST-Heb had significant discriminative power for boys and girls, separately. This suggests that parents recognize different behaviors as indicative of autism in boys and in girls, which is consistent with previous research on sex-specific autism phenotype (Dworzynski et al., 2012; Lai et al., 2015). This highlights the importance of considering sex differences when screening for autism and suggests that the CAST-Heb may need to be adapted or interpreted differently for boys and girls.
The two-stage analytical process employed in this study demonstrated a significant improvement in the overall identification rate of autism, particularly for those individuals who initially scored below the cutoff on the CAST-Heb. In the first stage of the process, we were able to correctly identify 96% of autistic boys and 80% of autistic girls. However, it was in the second stage, using the selected discriminant items identified through discriminant analyses, that we saw a substantial increase in identification rates. Specifically, we were able to correctly identify an additional 50% of the remaining autistic boys and 75% of the girls who had initially scored below the cutoff. This resulted in an overall identification rate of 98% for autistic boys and 95% for autistic girls.
This suggests that a two-stage screening process, which includes an initial screening followed by a more focused analysis using key discriminant items, may be more effective in identifying autism, particularly in children showing a more nuanced presentation of autistic features, who may not meet the initial cutoff. Notably, although our examination of the sex-specific items aimed to improve the accuracy of screening in girls, we found it was also beneficial for boys. This approach could be especially useful in clinical settings where sensitive identification, leading to appropriate intervention, is vital. It should be noted, however, that this approach could potentially lead to over-referral for diagnosis in a small percentage of non-autistic children. To control this limitation, clinicians are advised to back up parent-reported screening with additional sources of information, such as teachers.
The study also found significant positive correlations between CAST-Heb scores and ADI-R social interaction, communication, and RRB index scores. This indicates that higher CAST-Heb scores were associated with more reported symptoms in these ADI-R domains. However, there were no significant correlations between CAST-Heb scores and ADOS-2 SA or RRB scores. This discrepancy may be due to differences in the constructs measured by the ADI-R and ADOS-2, or it may suggest that the CAST-Heb, as a parent report measure, is more closely aligned with the ADI-R in its assessment of autism-related behaviors.
Therefore, while the preliminary results of this two-stage process are encouraging, it is particularly important to consider the potential benefits of multi-informant screening. Research has demonstrated that parent reports on screeners are associated with the ADI-R (Corsello et al., 2007), while teacher reports, offering a more social observation, are linked to the ADOS-2 (Constantino et al., 2007). This suggests that integrating both parent and teacher reports could enhance the accuracy of the screening process.
The findings from our study suggest that the items that discriminate autism in boys tend to be more focused on SC behaviors, whereas discriminating items for girls represent a broader scope of behaviors, including SC and the RRB, as well as non-specific features such as imaginative play. This difference may reflect the complex and often subtle ways in which autism manifests in girls (Lai et al., 2015). Autistic girls often exhibit a wider range of behaviors and characteristics, some of which may not be traditionally associated with autism, making their diagnosis more challenging (Hiller et al., 2016). Hence, sex differences should be considered in the screening and diagnosis of autism, with a more nuanced approach employed in the screening of girls. Our findings highlight the potential value of developing sex-specific screening tools or criteria that can more accurately capture the diverse ways in which autism can manifest in both boys and girls. This is akin to other screening tools, such as the Social Responsiveness Scale-2 (SRS-2), which also address sex differences in their screening process (Constantino & Gruber, 2005).
In light of this study’s insights, there is a compelling argument for reassessing the current framework of screeners like the CAST-Heb. The evident disparities in autistic presentations between girls and boys call for the refining of existing items or potentially incorporating new ones that resonate with these sex-specific nuances (Burrows et al., 2022). In addition, there may be merit in contemplating the development of new sex-tailored screening tools that can offer a more nuanced initial diagnostic approach. Engaging with the autistic community on one hand and with clinicians offering diagnostic assessments on the other, garnering insights into the feasibility and potential challenges of making adaptations to screening and diagnostic tools is advised. In the meantime, as such a process may be time-consuming and require substantial resources, sex-specific analyses of existing screening instruments, in pursuit of unique identifiers of autism in girls and boys, may aid in improving screening accuracy.
Interestingly, although the CAST-Heb was positively associated with ADI-R (but not ADOS-2) scores for both boys and girls, discrepancies emerged between the sexes when comparing clinician-observed ADOS-2 and parent-reported ADI-R assessments: While parents of boys’ reports of SC symptoms on the ADI-R were positively associated with clinician observations on the ADOS-2, a negative association was found between girls’ parent-reported communication symptoms on ADI-R and clinician observations of SC difficulties on the ADOS-2. This contrast highlights potential challenges in autism diagnostic assessment for girls. As previously reported (D’Mello et al., 2022), autism standard diagnostic tools may miss females, especially if they have not been revised to reflect recent modifications in the way autism is perceived along the spectrum and between sexes. The ADI-R, which is based on DSM-IV classification, is such an example, and our results demonstrate the need for a revision of this important clinical instrument, with an emphasis on the SC features that are more characteristic of girls.
Several limitations of this study should be acknowledged. First, our autistic group was derived from a clinically referred population. As such, the findings are not fully representative of the broader autistic spectrum present in the general population. The inherent nature of case–control studies, like the present one, might not capture the heterogeneity of the entire population or account for the types of non-autistic children who are referred for clinical evaluation. This questions the applicability of our findings as a general screening tool and limits them to clinically referred children. Further research is needed to assess the utility of the CAST-Heb for screening of girls and boys in the general population.
Second, our methodology relied on a retrospective record review from tertiary autism clinics. This approach may introduce biases and produce different results compared to studies conducted in more generalized psychiatric or child development settings.
In addition, our study did not characterize the IQ of our sample. This omission is notable as the ability to generalize these findings to populations with more compromised cognitive and language abilities might be limited.
A further limitation to consider is our use of convenience sampling in the non-autistic group, which might not provide a fully representative snapshot of the population under study.
Finally, while our study did shed light on some sex differences, the nature and scope of our research did not allow for an exhaustive investigation into this aspect. Future research should aim to replicate our findings in a larger, more diverse, and prospective sample. A valuable direction for subsequent studies would be to characterize the measurement properties of the CAST-Heb in a clinically referred sample, especially contrasting those who did receive an ASD diagnosis versus those who did not.
In conclusion, this study provides valuable insights into the use of the CAST-Heb as a screening tool for autism and highlights the importance of considering sex differences in the characterization of autism. The findings suggest that the CAST-Heb is a useful tool for identifying Israeli autistic boys and girls. Further research is needed to understand these sex differences and to consolidate future sex-sensitive screening tools.
Footnotes
Acknowledgements
The authors wish to thank OTI’s Bayit Echad Clinics for allowing access to their records and Noam Shachar for assisting with data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michael Terner was supported by Bar-Ilan University president’s scholarship. Other authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
A waiver of consent was granted by the Ness Ziona–Be’er Ya’akov Mental Health Center’s Helsinki Committee (#543) for the retrospective review of records in the autism group. Ethical approval for the non-autistic group was given by the last author’s department of psychology ethics committee. Parents of all non-autistic participants provided written informed consent.