
Abstract
There has been limited research to date into contextual factors hindering or supporting the successful implementation of neuro-affirming practice in support for Autistic and otherwise neurodivergent adults. We used a Realist Evaluation approach to explore key contexts affecting neuro-affirming practice. A preliminary programme theory of key aspects of support was developed. Views on current practice were sought through structured interviews with 32 senior professionals in leadership roles within Health and Social Care services in Scotland. This study identified important contexts shaping the implementation of neuro-affirming practice for adults. Results indicate widespread professional support for modifying practice to better accommodate neuro-affirming ideas, and scope to achieve this. However, some contexts, including limited resources, restrictive eligibility criteria and rigid service structures, hinder progress. Growing demand for services was often viewed as a restrictive context, but it also offered a chance to rethink conventional, one-size-fits-all models and adopt neuro-affirming approaches. The study is important in addressing a current gap in research into professional perspectives of the contexts required to develop transdiagnostic, neuro-affirming approaches and pathways for Autistic and neurodivergent adults. The insights from this study may offer transferable practice approaches, applicable across different countries with similar healthcare contexts.
Lay abstract
Delivery of neuro-affirming adult support pathways for Autistic and other neurodivergent adults by Health and Social Care institutions can be affected by different contexts. However, there is limited research to date into the most supportive contexts for effective neuro-affirming practice. This study aimed to explore the most beneficial contexts for neuro-affirming approaches, and barriers to this. We did this by using existing research to develop a theory about the most helpful approaches to support for Autistic adults, then gathering the views of 32 senior professionals in leadership roles within Health and Social Care services to explore supports and challenges they experience in implementing these approaches. The study identified important contexts for delivery of neuro-affirming practice and how these might be achieved. Some contexts, such as limited resources, restrictive eligibility criteria and inflexible service structures, could limit progress. However, although these were often seen as barriers, they also offered a chance to rethink one-size-fits-all models and adopt neuro-affirming approaches. This study is important in addressing a current gap in research into professional perspectives of the ways neuro-affirming approaches can be developed in practice, to support Autistic and neurodivergent adults. The insights from this study may offer transferable lessons, applicable across different regions and countries.
Keywords
Introduction
Many Autistic and other neurodivergent adults do not require ‘interventions’ in the traditional sense. They have a particular neurotype, rather than ‘treatable’ diseases or disorders. Current diagnostic criteria, the Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) and International Classification of Diseases, 11th Revision (ICD-11), are at odds with evolving community language and continue to use the term ‘Autism Spectrum Disorder’ with criteria based on a medicalised, deficit model. In addition, persistent stigma and unsupportive environments continue to contribute to higher rates of physical and mental health needs, and disability and occupational challenges (Crowson et al., 2023; Tamura et al., 2025; Wigham et al., 2023). These challenges are heightened for individuals with multiple marginalised identities, leading to further difficulties accessing needed services and support within healthcare and across wider contexts (Hersh et al., 2022; Hotez et al., 2024). Neurodivergent adults often need reasonable adjustments in educational and workplace settings (Vincent & Fabri, 2022; Thorpe et al., 2024) along with additional support provided across sectors, including health, social care, education, employment, and community outreach. Support typically combines formal initiatives, such as diagnostic assessments and mental health services, alongside informal supports, including third-sector and peer support. Provision is usually organised around the stages before, during and after diagnosis. Prediagnosis support may include meetings, information and education. The diagnostic assessment itself is often seen as a form of support, offering self-knowledge, validation, and access to a peer community (Cook et al., 2024; Curnow, Rutherford, et al., 2023; Milton & Ryan, 2022; Wilson, et al, 2023). Postdiagnosis, follow-up meetings and signposting to local and national support options, including self-help, group support, and mental health or psychoeducational resources, are common.
There is strong advocacy for multifaceted professional practice that addresses a range of neurodevelopmental differences. High levels of co-occurrence and overlap between the experiences and support needs of Autistic people and those with other diagnoses, such as attention-deficit/hyperactivity disorder (ADHD), highlight the need for practice that extends beyond strict diagnostic categories (Fernell & Gillberg, 2023; Rong et al., 2021; Rutherford & Johnston, 2022). In exploring the intersection of autism and ADHD, it is also important to recognise the concept of ‘AuDHD’, a more recent term since combined autism and ADHD diagnoses became possible, used to describe dual diagnoses as an entity specific to ‘AuDHDers’, whose experience is different to individuals with singly-diagnosed autism or ADHD (Craddock, 2024). Furthermore, many individuals seeking mental health support are neurodivergent, whether diagnosed or not (Dallman et al., 2022; Galvin et al., 2025), and broader awareness of neurodivergence among mental health professionals is an important issue (Curnow, Utley, et al., 2023; Galvin et al., 2025; Patten et al., 2024). Recent evidence suggests traditional mental health support may be ineffective or harmful if not adapted for neurodivergent people (Paynter et al., 2025), and support approaches should include pathways for neurodiversity awareness, and clear routes for diagnosis and support (Rutherford et al., 2021).
Health and social care systems, and the professionals within them, play a crucial role in making support accessible. Frameworks, service models, policies, professional knowledge and collaboration across health, education and workplace settings all shape the support provided. A key focus is ensuring support is grounded in ‘neuro-affirming’ principles (Dallman et al., 2022; Rutherford & Johnston, 2022). Understanding how to do this remains a substantial challenge. While international guidelines and research do provide some indicators (Autism Europe, 1992; de Broize et al., 2022; Goodall et al., 2023; Haute Autorité de Santé, 2017; Holtom & Lloyd-Jones, 2022; National Institute for Health and Care Excellence [NICE], 2021; Scottish Intercollegiate Guidelines Network [SIGN], 2016; Whaikaha – Ministry of Disabled People, 2022), definitions of neuro-affirming practice are still contested and in development (Flower et al., 2025). The foundational ideas come from the neurodiversity paradigm, prioritising self-understanding, acceptance and the valuing of diverse neurotypes. The term ‘neuro-affirming’ means lifespan, strengths-based support which is not diagnosis-dependent (Rutherford & Johnston, 2022). This requires a move from the medical model of disability and working with the neurodivergent community in redressing societal historical power dynamics, to update the social model of disability in line with neuro-inclusive approaches (Dwyer et al., 2025; Shaw et al., 2025). Walker (2021) draws on the views of the neurodivergent community to define the neurodiversity paradigm, as built on three core tenets: that individual diversity in neurocognitive styles is a natural and important element of human society; that the perception of a ‘right’ or ‘wrong’ style of human brain functioning is a social construct, not a fact; and that societal attitudes to neurodiversity are shaped by the prevailing social power dynamics and inequalities, however, that in the right contexts diversity can drive positive societal shifts (Walker, 2021). Therefore, central to neuro-affirming practice is the shift away from disorder-focused perspectives and language. It is important to focus on developing neuro-inclusive environments, recognising that needs can arise from the interaction between an individual’s neurotype and their environment, and are not solely due to individual limitations or difficulties. Meaningful partnerships and co-production with neurodivergent individuals and communities are fundamental aspects of neuro-affirming practice (Beresford & Mukherjee, 2024; Lerner et al., 2023; O’Neil Woods & Estes, 2023; Rutherford et al., 2023). Multidisciplinary teams comprising skilled and knowledgeable professionals are a key element of effective healthcare provision for neurodivergent adults (Crane et al., 2019; Doherty et al, 2023; Unigwe et al, 2017), and it is crucial to ensure the meaningful involvement of neurodivergent adults in planning and delivering individual supports, in line with the principle ‘Nothing about us without us’.
Neuro-affirming practice is an emerging and complex concept, and there remains a significant gap in understanding the essential contextual factors required for its effective implementation within public services. To successfully integrate these practices, evidence-informed insights are necessary. The objective of this study was to analyse information from health and social care practitioners in Scotland regarding current practice in supporting Autistic adults and those with ADHD, Fetal Alcohol Spectrum Disorder (FASD) and intellectual disabilities. Through this analysis, we aimed to identify key factors either supporting or hindering progress towards more neuro-affirming approaches. By exploring these factors, the study sought to enhance understanding of how to improve support, and the practical challenges and opportunities involved. The findings are intended to inform the development of policies and strategies that could address barriers and foster more inclusive support systems, contributing to the global movement towards neuro-affirming practices for neurodivergent adults.
Community involvement
This study was conducted by a mixed-neurotype practitioner–researcher partnership, which leads initiatives to bridge the evidence-to-practice gap, and drive whole-systems change in neurodevelopmental practice in Scotland. The partnership aims to support implementation of evidence-informed practice across the lifespan within a neurodiversity paradigm, by improving health and education provision for Autistic and other neurodivergent individuals. The team includes research professionals from Education, Speech and Language Therapy, Occupational Therapy and Psychiatry with direct experience of working in health, social care and education.
This study was co-designed across our authorship team from initial project development, data collection and analysis to interpretation of the findings and manuscript preparation. It incorporates insights about health care priorities gained from the team’s neurodivergent partner network, as well as those identified in recent research literature. Autistic members of the research group were included at every stage of the study design. Participants included individuals who shared a neurodivergent identity with us (n = 3). This information was not requested.
The study will be used to produce guidelines for practice, to be co-produced and disseminated in conjunction with National Autism Implementation Team (NAIT) divergent partners.
Setting
The study was undertaken in Scotland, the second largest country in the United Kingdom, with a population estimated at greater than 5 million. Health provision is state-funded by the National Health Service (NHS), with services delivered through 14 regional Health Boards. Legislation passed in 2014 (Public Bodies (Joint Working) (Scotland) Act 2014) aimed to integrate delivery of services between Health and Local Authority areas by introducing 31 NHS ‘Health and Social Care Partnerships’ (HSCPs). The first point of contact for adults, including those with an intellectual disability, and individuals with complex mental health needs, is usually the General Practitioner (GP), referred to as a Primary Care service. The GP may then refer on to Secondary Care services, primarily Community Mental Health Teams (CMHTs), with input from nurses and Allied Health Professionals (AHPs) such as Occupational Therapists, if a support need is identified (Maciver et al., 2025; Rutherford et al., 2023). The non-NHS element of HSCPs is primarily led by social care professionals, who are responsible for commissioning third-sector postdiagnostic support, including employment supports along with additional healthcare support, if a need is identified.
Theoretical approach: realist evaluation
A qualitative approach using a Realist Evaluation framework (Pawson & Tilley, 1997) was adopted for this study. Adult health and social care services are complex structures, with a range of support pathways that are often contingent upon local organisation and culture. Realist evaluation is of particular utility in exploring complex, multilayered systems (Jagosh et al., 2022; Nielsen et al., 2022; Skivington et al., 2021) by exploring ‘what works for whom in what circumstances . . . and why’ (Pawson, 2013). This approach identifies the multiple interacting processes, or ‘mechanisms’, through which a programme or intervention operates, and the extent to which different contexts can interact with mechanisms to facilitate or hinder successful programme implementation or ‘outcomes’ (Herens et al., 2017; Greenhalgh & Manzano, 2022). For this study, we reported against the identified contexts using four levels identified by Pawson and Tilley: (1) individual level: the skills and capacity of key individuals to deliver a programme or intervention; (2) interpersonal level: interpersonal relationships supporting effective programme delivery; (3) institutional level: the culture and organisation of the institution where the intervention is delivered; and (4) infrastructural level: the overarching infrastructural system, including political landscape, priorities and practice (Pawson et al., 2004).
Methods
Preliminary programme theory
Developing a ‘preliminary programme theory’ (PPT) is important in realist-style analysis. This involves formulating a hypothesis about how and why a programme is expected to achieve desired outcomes (Pawson & Tilley, 1997). For this study, we developed a PPT of what constitutes neuro-affirming support, against which the contextual factors could be analysed. The PPT was based on nine mechanisms identified in recent research (Cage et al., 2024; Crane et al., 2021; Crowson et al., 2023; Curnow, Utley, et al., 2023; Royal College of Psychiatrists, 2023), alongside a feasibility study, which evaluated potential adult ADHD pathways and gathered perspectives on broader neurodevelopmental needs (Scottish Government, 2021), and research into existing neurodevelopmental pathways in Scotland (Rutherford et al., 2023) which tasked four large diagnostic teams across Scottish regions, chosen as ‘pathfinder’ sites, with developing local autism and ADHD action plans. This work included insights from staff and neurodivergent individuals who were part of a neurodivergent partner network, supporting stakeholder involvement in the development of the PPT.
The purpose of the current research was not to explore or expand on the mechanisms of the PPT, but rather to develop hypotheses about the factors which may facilitate or prohibit their delivery (Table 1).
Preliminary programme theory – mechanisms for neuro-affirming support for adults.
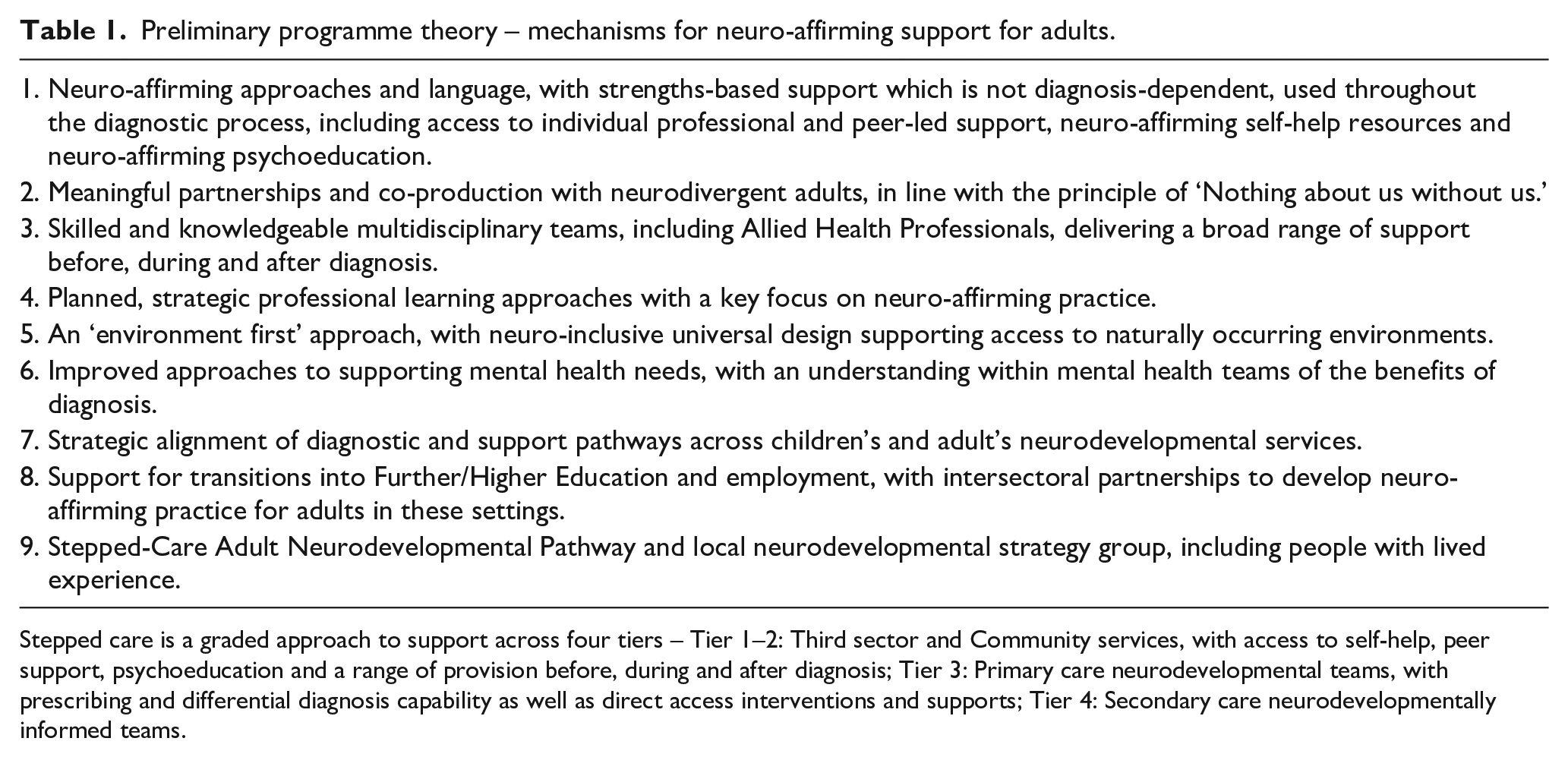
Stepped care is a graded approach to support across four tiers – Tier 1–2: Third sector and Community services, with access to self-help, peer support, psychoeducation and a range of provision before, during and after diagnosis; Tier 3: Primary care neurodevelopmental teams, with prescribing and differential diagnosis capability as well as direct access interventions and supports; Tier 4: Secondary care neurodevelopmentally informed teams.
Participants and recruitment
We aimed to include at least one participant from each of Scotland’s 31 HSCP areas. We sent invitations, study information and consent to participate confirmation to key operational and leadership staff from services supporting neurodivergent adults within each area. These were distributed via established networks, with additional participants recruited through snowball and word-of-mouth sampling. Participants were aged 18 or above, employed in an HSCP supporting neurodivergent adults, with at least 2 years of relevant experience in a paid role within health or social care. They had strategic or practitioner leadership roles and were able to provide a comprehensive overview of facilitating and challenging contexts to effective neurodevelopmental support within their respective settings.
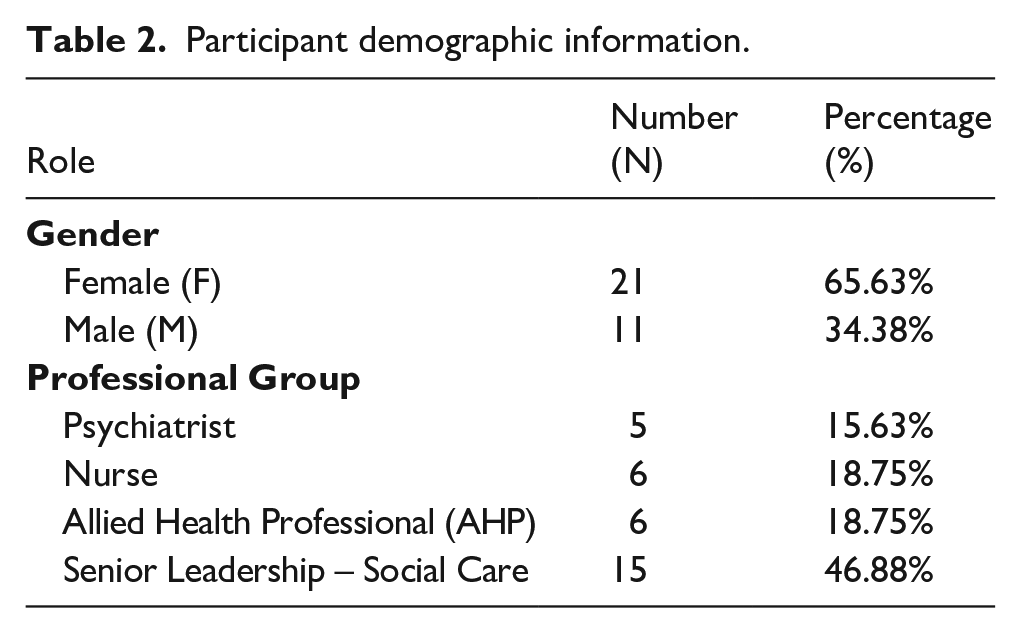
In total, 32 people, representing 27 HSCPs, participated in an interview or provided written information. Two areas responded on behalf of the entire health board rather than for individual HSCPs, and the individual HSCPs in each Board have been included accordingly. Demographic information regarding gender and role was collected (Table 2).
Participant demographic information.
Data collection procedure
Data were gathered through structured interviews exploring participants’ views on current supports for neurodivergent adults, key challenges, and potential improvements (Supplementary Materials 1 – Interview Schedule). A pilot interview was undertaken by the lead researcher and a research colleague. Each member of the research team took 60- to 90-min online interviews, with the majority being undertaken by the lead researcher. Before the interview, all participants were asked to complete a brief online survey using JISC, to capture data on support services in their area (completion n = 10). Survey data were used to support and enhance information obtained through interviews (available on request). The concept of neuro-affirming practice was discussed as part of the research interviews (Supplementary Materials 1 – Interview Schedule, Question 9). This question explored the concept of ‘neuro-affirming’ through the lens of the neurodiversity paradigm, including service alignment with the neurodiversity paradigm, conceptions of the value of neurodivergent preferences and the acceptability of practice to the neurodivergent community. This enabled discussion of different conceptualisations of neuro-affirming practice to ensure a shared understanding with participants.
Data analysis
Interviews were professionally transcribed. The lead researcher led the analysis. The research team is positioned as a mixed-neurotype group. The lead researcher maintained a reflective diary and had regular supervision with experienced research colleagues to ensure reflexivity in data analysis. The involvement of the wider team in undertaking some of the interviews allowed different perspectives, and all data were discussed and reviewed as a research team to ensure any points of contention or disagreement in the analysis could be explored and reconciled. The key analytic focus was on identifying the contexts favouring or disfavouring the actual or potential activation of mechanisms identified in our preliminary programme theory, and the reasoning for this. We undertook thematic analysis, involving familiarisation, coding the data, charting themes, and interpreting the data (Braun & Clarke, 2013, 2021; Ritchie & Spencer, 2002; Seale, 1999). For example, aspects relating to the ways in which areas organised diagnostic and support services were first grouped into a broad ‘service structures’ code, and items related to staff knowledge and expertise were grouped into the ‘engagement with and access to relevant professional learning opportunities’ code. Data were further classified using Pawson and Tilley’s ‘Four I’s’. All data were then coded until no new codes were identified, aiming for increased levels of abstraction. As analysis progressed, further codes were created, refined and grouped to identify mutually exclusive categories of coherent contexts which could be designated single unifying labels. Final labels were then assigned to each area. Finally, mechanisms were grouped according to each of the contexts, as identified by participants (Supplementary Materials 2). Data were reviewed and agreed by the research team, and the narrative summary was written.
Results
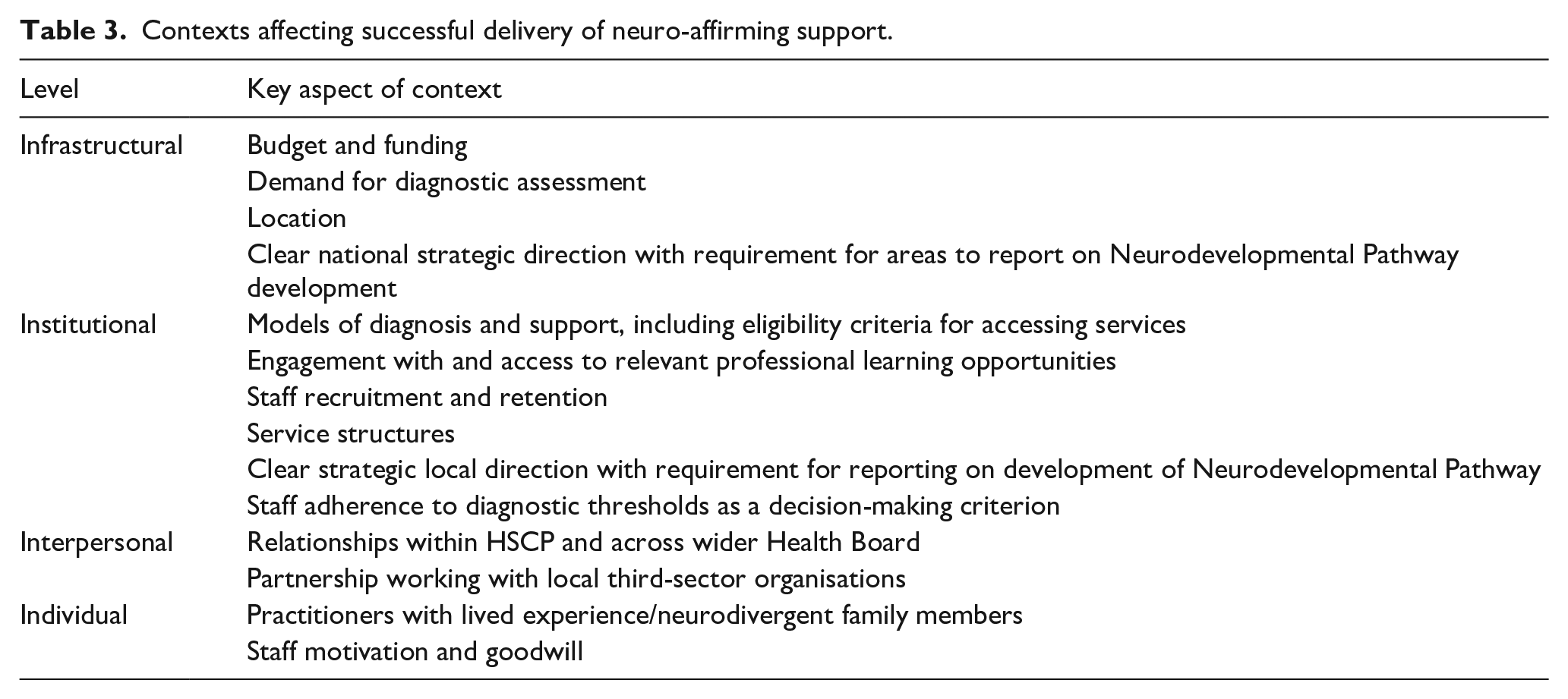
Support for neurodivergent adults before, during and after diagnosis showed significant variation across and within areas. Fourteen contexts affecting successful implementation of the mechanisms in the PPT were identified (Table 3), all of which interacted with one another as well as operating across mechanisms (Supplementary Materials 2).
Contexts affecting successful delivery of neuro-affirming support.
Identified contexts
Infrastructural level
Budget and funding
Budget was a significant factor for almost all participants. Allocation of funding within a sustainable model to develop new, established (i.e. not time-limited) cross-service roles was a favouring context. Budget to develop multidisciplinary approaches was also important, with funding across teams necessary to provide effective support pathways. However, most participants perceived budget as a restrictive factor, with competing local and national demands leading to challenges in prioritisation. Budget also affected staffing levels, affecting capacity for strategic development of new neuro-affirming approaches, particularly in the context of greatly increased demand. Smaller areas were limited by their ability to achieve staffing benefits of scale seen in larger areas, which also hindered the implementation of multidisciplinary teams.
Demand for diagnostic assessment
Increased demand for diagnostic assessments, especially for ADHD, was a significant context. Demand was largely seen as restrictive, with a perception of the need to focus on operational diagnostic work reducing staff availability, affecting capacity to engage in professional learning, and hindering the development of new support pathways. There was significant reliance on third-sector organisations to provide support for newly diagnosed individuals and in areas with stable support, this was a facilitating factor. However, in other regions, instability, short-term funding or geographical challenges made the third sector’s support unreliable, leading to fluctuating outcomes that could be either supportive or restrictive. In some areas, high demand and low capacity issues were seen as leading to an increased number of individuals seeking private assessment, and participants described challenges including integrating privately obtained diagnoses into public services, with the limitations of private provision leaving public sector services managing increased numbers requiring postdiagnostic support, along with an increase in health inequalities for some under-represented groups. Limited capacity for ADHD support led to a focus on pharmacological approaches, with prioritisation of diagnosis for those most likely to benefit from medication. All participants acknowledged the potential efficiencies that transdiagnostic approaches could provide, particularly through the integration of autism and ADHD teams. However, while there was a clear desire for change, given perceived staffing capacity issues, this was largely viewed as aspirational.
Location
Location was an important context, particularly affecting remote, rural and island communities. This could be an enabling factor, driving development of connections and joint working. Location in smaller and less densely populated areas could also facilitate support for neurodivergent individuals by virtue of them being better known within communities, in turn increasing community knowledge and understanding. However, relative remoteness was more commonly viewed as restrictive, particularly affecting recruitment and retention, causing increased reliance on locum staff which affected strategic planning and delivery of support. Reduced availability of third-sector or peer support could also lead to an increased sense of isolation for newly diagnosed adults. The impact of rurality on digital connectivity and hidden poverty in rural areas were highlighted as prohibiting factors in some areas.
A clear national strategic direction with requirement for each area to report on development of neurodevelopmental pathways
A national government-led direction, with the requirement for each area to report on their development of new approaches to neurodevelopmental pathways, was identified as a strong enabling factor in ensuring prioritisation of neuro-affirming work. Nationally agreed and implemented values and standards for neuro-affirming practice was noted as a potential supportive factor, by providing a framework within which areas could develop strategic approaches.
Institutional level
Models of diagnosis and support, including eligibility criteria for accessing services
Models of diagnosis and support was a highly influential context. Support pathways for adults with intellectual disability and/or mental health needs were generally well established, which could be facilitative in delivering person-centred, strengths-based approaches. While well-embedded approaches have their benefits, they can also create a prohibitive context if pathways are inflexible and resistant to changes, such as neuro-affirming practice.
Support often had a single condition focus contingent on high thresholds for access, and in general was less available for Autistic adults and those with ADHD, especially after diagnosis or when no formal diagnosis was made but support requirements existed. There were no discrete pathways for adults with FASD. Very few areas provided AHP support in Primary Care teams for this population, and in the significant majority of areas multidisciplinary team input was not routinely available unless assessed as being required due to significant mental illness or other risk. In some HSCPs, support was based solely on eligibility for Self-Directed Support (a statutory government benefit), making it inaccessible to many. This particularly affected individuals with ADHD, with support restricted to those benefitting from medication and/or being assessed as having a serious co-occurring mental illness or substance misuse need. Executive functioning difficulties for some adults with ADHD were a compounding factor in creating barriers to accessing support within existing pathways.
Engagement with and access to relevant professional learning
Professional learning was a crucial enabling context. Higher levels of staff skill and expertise within and across neurotypes led to confidence, effective multidisciplinary working and flexible approaches to support. Availability of professional learning for nonclinical staff was associated with improved support across employment, education and independent living. Professional learning opportunities were variable locally and nationally, making this a restrictive context for some. While specific groups of professionals, including GPs and Community Mental Health Teams, were particularly likely to benefit from increased access to higher level professional learning, a lack of access to relevant opportunities and capacity to participate in professional learning was a restrictive factor. In some areas, training was offered on an ‘ad hoc’ basis, with attendance based on staff willingness to engage rather than being strategically planned. The lack of staff with sufficient skills and knowledge to meet an increased complexity of need in Autistic and ADHD adults, and gaps in clinician expertise in diagnosis and support for people with FASD inhibited delivery of neuro-affirming support. The potential of Communities of Practice to support intersectoral professional learning was noted by several areas.
Staff recruitment and retention
Staff recruitment and retention were critical factors, with ongoing challenges, particularly for AHPs and Psychiatrists, being a severely prohibitive context for most areas. High staff turnover and/or gaps in staffing was a restrictive factor where this affected communication, consistency of support and multidisciplinary working across services, which could also limit the application of neuro-inclusive practice in the community and third sector. While this issue affected all areas, remote and rural locations faced the greatest challenges. Stable staffing models, however, facilitated strong relationships, communication and effective multidisciplinary neuro-affirming support while also improving staff morale, skills and confidence.
Service structures
Service structures, defined as the ways in which different services for neurodivergent people operate within the same HSCP, was an important context. Alignment of service structures could be a facilitating factor in developing effective support, and was particularly key during transition from paediatric to adult services. Conversely, a lack of alignment was a prohibitive context. The majority of areas identified inconsistent approaches and persistence of ‘silo’ working across services, affecting communication and establishment of multidisciplinary pathways. As was the case for ‘Models of diagnosis and support’, this could have a particular impact on individuals not meeting a specific service’s eligibility criteria, who would then be referred to another service, thereby increasing diagnostic waiting-times and delaying support.
Clear local strategic direction with requirement for reporting on development of neurodevelopmental pathways
A clear local strategic direction, aligned with a national Neurodevelopmental Pathway strategy and mandatory reporting to strategic governance committees, was identified as a facilitating factor; in contrast, a focus on competing health priorities was seen as restrictive. This context was not only vital for effective support but also influenced the development of other critical contexts, making it essential for the evolution of neuro-affirming practice.
Staff adherence to diagnostic thresholds as a decision-making criterion
Staff adherence to diagnostic thresholds as a decision-making criterion for accessing support, interlinked closely with ‘Models of diagnosis and support’. Rigid adherence to thresholds was a restrictive factor where these were conceptualised within a medical model, focusing on the presence of individual diagnoses and overlooking co-occurring differences, leaving some needs unaddressed or some groups unsupported. Movement away from thresholds was an enabling context, and was facilitated by staff skill, expertise and confidence.
Interpersonal level
Relationships between services and staff
The strength of relationships between professionals across services was a fundamental factor in enabling effective multidisciplinary, neuro-affirming practice. This was strongly influenced by institutional contexts, particularly ‘Service structures’ and ‘Recruitment and retention’. Relationships were also important for professionals seeking advice and support from other services, both for their own professional learning and to increase the effectiveness of support.
Partnerships with local third-sector organisations
Effective partnership working with local third-sector organisations particularly affected support after diagnosis. Few areas formally commissioned or supported third-sector organisations; however, many relied on these to provide support, information and advocacy after diagnosis. Relationships with staff in local third-sector organisations were impacted by recruitment and retention in both sectors. The short-term nature of funding in the third sector led to a perceived lack of stability, and challenges related to the availability of services locally and nationally were highlighted, particularly in rural and remote areas. Views across different third-sector organisations about what constitutes effective support was also an important factor for effective partnership working, and was a restrictive context for some areas.
Individual level
Practitioners with lived experience/neurodivergent family members
The involvement of practitioners with lived experience of neurodivergence and/or neurodivergent family members was identified by relatively few participants; however, where this was highlighted, it was a significant facilitating context for delivering support, and was associated with improved engagement with professional learning, and increased staff confidence and expertise. A potential lack of awareness of reporting of this as an enabling factor could be driven by current low numbers of staff with lived experience, or perceived stigma leading to a reluctance among medical professionals to disclose their neurodivergent status.
Staff motivation and goodwill
Staff motivation and goodwill was an important context, in the absence of more planned and strategic approaches. Connections between lived experience of neurodivergence and practitioners’ goodwill and motivation suggested a positive correlation between these contexts as a further enabling factor.
Discussion
This research employed Realist Evaluation techniques to investigate the contexts that could promote or hinder neuro-affirming support pathways for adults. By analysing these practices through the lens of practical implementation, the study provides information on how local contexts can be harnessed and adapted to deliver neuro-affirming practice. The findings revealed that many supportive factors were present, indicating considerable opportunity for change and implementation. The study demonstrated a strong consensus among participants regarding the necessity for change. Nevertheless, participants also identified many obstacles.
A key finding at the institutional level is the impact of rising demand for diagnostic assessment, particularly for ADHD. Some areas had developed a new single-condition ADHD pathway to address increased demand; however, this was perceived as affecting capacity to offer support for Autistic adults. Demand could be a facilitating factor, driving development of more holistic, flexible pathways, but many areas were focused on the operational impact of increased numbers, which was consistently identified as a disfavouring factor, affecting capacity to implement new pathways and supports. Capacity to meet demand was also seen as contributing to an increase in private assessment, potentially contributing to health inequalities across marginalised groups (Devaja, 2023; Hendrickx & Hendrickx, 2024; Lethbridge, 2016). Models of assessment have previously assumed lower prevalence and although co-occurrence of neurodevelopmental conditions is highly likely, many services retain single condition, rather than transdiagnostic approaches (Rutherford & Johnston, 2022). In planning future services, recent research suggests a requirement for models which can meet the needs of 10% to 15% of people (Rutherford et al., 2023), rather than existing clinical models aimed at 1% to 5% (Radley et al., 2024). This ‘either/or’ approach relates to the broader context of budget and economics; however, viewed through the lens of neuro-affirming practice, these challenges reinforce the argument for transdiagnostic or multicondition approaches (Maciver et al., 2025).
Service structures and eligibility criteria for accessing support were also critical contexts, with particular importance for adult mental health support. While there are benefits to well-embedded approaches, this could be a prohibitive context where support pathways were inflexible and less likely to evolve in response to new ideas, in this case neuro-affirming practice. Barriers arise from the delivery of support through secondary care services, with high thresholds and stringent criteria for access within a medical model of reacting to crisis, potentially exacerbating mental health issues and contributing to poorer long-term outcomes. Different models of service provision across paediatric and adult services could also create barriers. There was a general lack of involvement of Higher and Further Education institutions and employers in strategic planning of support pathways during transition and there was a clear need for improved alignment and joint working across services to help embed neuro-affirming practice and facilitate more consistent and equitable supports. High thresholds for support could also affect newly diagnosed neurodivergent adults’ understanding of their diagnosis, perpetuating a sense of stigma, and a feasible hypothesis is that less rigid service structures and more flexible approaches to diagnostic pathways, including embedded transdiagnostic approaches with established multidisciplinary diagnostic teams, and access to support which is not diagnosis-dependent (Rutherford & Johnston, 2022) could facilitate better access to, and experiences of, support.
Planned, strategic professional learning, including third-sector colleagues, was an important enabling factor. Participants highlighted gaps in professional skill, expertise and confidence across services and particularly among some professional groups, aligning with recent commentary (Shaw et al., 2023). Lack of professional expertise can contribute to underdiagnosis, long waiting-times, and affect mental health, and while some resource is focussed on mental health consequences this can miss the key context of the person being neurodivergent (Curnow, Rutherford, et al., 2023; Evans et al., 2022; Kiehl et al., 2024). There was a clear need for ongoing professional learning, guidance and resources to be developed and disseminated widely to support neuro-affirming practice.
At infrastructural level, several contexts were highlighted by a majority of participants. Principal among these was budget, primarily a restrictive factor affecting operational staffing and capacity for strategic development, particularly in the context of increased demand. Allocation of funding within a fiscally sustainable model to develop new cross-service roles was a favouring context, supporting the argument that targeting budget to develop multidisciplinary approaches can facilitate neuro-affirming pathways (Maciver et al., 2022). Location was also an important context, most commonly affecting remote, rural and island communities as a disfavouring factor. For these areas, location impacted significantly on other contexts, particularly recruitment and retention, and availability of peer networks and third-sector support. Participants highlighted the need to address these barriers and there are potential benefits in these areas collaborating at national level to develop context-specific supports.
While a relatively small number of contexts operated at the interpersonal level, these were key in delivering change within overarching institutional and infrastructural contexts. Third-sector agencies were an enabling factor in providing support, aligning with recent research findings (Featherstone et al., 2024; Wigham et al., 2023). However, variable availability and short-term funding could be prohibitive. Co-production with neurodivergent partners was also an important context; however, this could be restrictive where challenges existed in relation to governance, lack of consensus across partners of what constituted effective support and accessibility of meetings. Innovative approaches to facilitate engagement included use of technology, and specific professional engagement and support roles.
At the individual level, professionals with lived experience of neurodivergence and/or neurodivergent family members was the most significant enabling context, aligning with recent research (Curnow et al., 2025). This could facilitate an increased understanding of, and confidence in delivering, neuro-affirming approaches as well as mitigating the double-empathy and triple-empathy problem (Milton, 2012; Shaw et al., 2023).
Recommendations
In seeking to implement neuro-affirming pathways, those aiming to improve practice must be prepared to navigate and, at times, counteract restrictive, context-driven responses that could undermine effectiveness and sustainability, such as service eligibility, capacity and budgets. Professional mindsets can also be a disfavouring factor. Resistance does not always stem from opposition to neuro-affirming ideas, but from responses to resource constraints and perceived complexities of delivery. For instance, a response to rising demand might involve restricting assessments to the most visibly affected, which contradicts neuro-affirming goals by prioritising reduction of service demand over addressing needs in a timely manner. Implementing neuro-affirming approaches in such settings will require engaging with and, where possible, adapting or shifting these contexts. Encouragingly, participants in this study expressed a commitment to neuro-affirming approaches, recognising both the potential for improvements and work needed to overcome barriers.
Considering the findings, several further practical recommendations emerge. It is crucial to build a comprehensive understanding of what constitutes neuro-affirming pathways for diagnostic assessment and support. Current deficit-focused models, centred on reacting when individuals experience high levels of distress with interventions which place the need for change in the person, must be replaced with strategic, whole-system lifespan support built on universal design approaches across the community, society and all services. Transdiagnostic models (e.g. which include co-occurrence, such as autism and ADHD) along with more proactive, flexible approaches to support could enhance access for individuals who might fall outside or between current thresholds. It is also important to recognise the effects of intersectionality and potentially increased difficulty accessing healthcare for individuals with multiple marginalised identities. By eliminating the need for multiple consultations and assessments, this would enable streamlined and earlier support, which would in turn decrease the likelihood of individuals reaching crisis-point and requiring intensive mental health interventions, thereby helping to manage demand and capacity issues. This is particularly pertinent in settings where neurodevelopmental assessment services are currently embedded within broader mental health services. In implementing such changes, named multidisciplinary teams are integral to the model, to build sustainable, locally funded services, rather than relying on short-term projects and precarious funding.
While the contextual barriers to implementing effective neuro-affirming practices can appear formidable, overcoming one barrier can trigger a series of positive changes across the system. For example, strategically planned and tailored cross-service professional learning, focused on neuro-affirming approaches and the essential contexts for their delivery, alongside local and national networking opportunities such as Communities of Practice, could create a virtuous cycle where enhanced staff expertise and confidence lead to greater engagement in further learning and more holistic roles. In delivering these changes, it is important to recognise that many contexts are historically entrenched and a paradigm shift requires significant effort to address barriers. While there was a strong commitment to this change expressed by participants in our study, ongoing support to deliver this was essential.
Limitations
We may have overlooked insights from some professionals, due to the difficulties identifying individuals with comprehensive knowledge of service structures across various areas of neurodivergence. Data on participants’ age, ethnicity, socioeconomic status and educational attainment levels were not collected; however, this may have been useful in exploring conceptions of neuro-affirming practice through the lens of different cultural backgrounds. Although the focus was on staff perspectives and professional practices, and the study design built on insights obtained from neurodivergent adults, incorporating further feedback from neurodivergent individuals in future research would enhance our understanding. While this work is limited to practice in Scotland, the importance of improving neuro-affirming support for adults is recognised across many countries, and the use of a realist-style analysis enables the development of a programme theory that identifies contextual factors and mechanisms which may resonate with other regions worldwide, offering broader application of these findings in different locations.
Conclusion
This study identified key contexts influencing the implementation of neuro-affirming support for adults, highlighting opportunities and obstacles. The findings reveal strong professional support for adapting pathways, although barriers such as resources, eligibility criteria and service structures persist. While increased demand is often seen as burdensome, it also presents an opportunity to reconsider traditional, single-condition models and embrace approaches that reflect the needs of individuals. Our analysis suggests that neuro-affirming practice is achievable with a deeper understanding of contextual factors. The insights gained may be applicable across different regions and countries with similar features or challenges. Implementing neuro-affirming practice is undoubtedly challenging, but it is also a moral and ethical imperative. This study provides part of the picture towards meaningful change.
Supplemental Material
sj-docx-3-aut-10.1177_13623613251360275 – Supplemental material for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care
Supplemental material, sj-docx-3-aut-10.1177_13623613251360275 for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care by Anna Gray, Donald Maciver, Eleanor Curnow, Lorna Johnston and Marion Rutherford in Autism
Supplemental Material
sj-pdf-1-aut-10.1177_13623613251360275 – Supplemental material for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care
Supplemental material, sj-pdf-1-aut-10.1177_13623613251360275 for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care by Anna Gray, Donald Maciver, Eleanor Curnow, Lorna Johnston and Marion Rutherford in Autism
Supplemental Material
sj-pdf-2-aut-10.1177_13623613251360275 – Supplemental material for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care
Supplemental material, sj-pdf-2-aut-10.1177_13623613251360275 for Contextual factors influencing neuro-affirming practice: Identifying what helps or hinders implementation in health and social care by Anna Gray, Donald Maciver, Eleanor Curnow, Lorna Johnston and Marion Rutherford in Autism
Footnotes
Acknowledgements
We wish to give thanks and acknowledge the contributions of stakeholders, the Scottish Government, people who are experts by experience of neurodevelopmental differences and families, health and education professionals who have supported this work.
Ethical considerations
The study received ethical approval from the Research Ethics Committee at Queen Margaret University (approval no. 2023/09) on 03/07/2024.
Consent to participate
Participants gave written consent to participate, and their signature, before completing the research surveys and interview.
Consent for publication
This paper does not include any data relating to an individual.
Author contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The National Autism Implementation Team completed this work and is funded by the Scottish Government.
Data availability statement
Supplemental data have been submitted. Supplemental data with examples of emerging practice and anonymised direct quotations from participants are available upon request from the corresponding author.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.