
Abstract
Autistic adults face various psychological and physical health conditions which often require ongoing medical attention. Despite a greater likelihood of health conditions, autistic adults face many systemic barriers in accessing healthcare services. It is important to identify facilitators to healthcare access and recognize the impact of self-advocacy on these experiences. In this qualitative study, we interviewed 15 autistic participants to understand their experienced and desired facilitators when accessing healthcare services, as well as the role of self-advocacy in accessing these services. Overall, participants agreed that formal and informal supports, provider knowledge about autism, and provider openness to providing accommodations served as facilitators. Participants also shared about their experiences related to self-advocacy and accessing healthcare services such as examples of self-advocacy in healthcare, learning to be a self-advocate, and facilitators of self-advocacy. Implications for research and practice are discussed.
Lay abstract
Autistic adults often have both mental and physical health needs that require ongoing care. However, they often face obstacles when trying to get healthcare. This study aimed to find out what helps autistic adults get the healthcare they need and how self-advocacy, or speaking up for themselves, plays a role. We talked to 15 autistic individuals about their experiences and what they wished for when accessing healthcare. Participants mentioned that support from others, doctors’ knowledge about autism, and doctors being willing to make changes as needed per patient need were helpful. They also shared how self-advocacy impacted their healthcare experiences, including examples of how they advocated for themselves and what helped them do so. The study offers insights that could inform future research and healthcare practices.
Autistic adults face various psychological and physical health conditions (Mason et al., 2021) which often require ongoing medical attention. Regarding physical health conditions, compared to the general population, autistic adults are at 1.5 times increased risk for heart disease, 1.6 times increased risk for diabetes, and 1.7 times increased risk for dyslipidemia (Dhanasekara et al., 2023). In addition, autistic adults (versus individuals without autism) are significantly more likely to have sleep disorders, epilepsy, and sensory impairments (Micai et al., 2024). Mental health conditions include anxiety and depression (Linden et al., 2023) which may reduce life expectancy (Doherty et al., 2022). As a result of the greater likelihood of health needs, autistic adults may need healthcare services. Indeed, compared to the general population, autistic adults use more healthcare services including emergency department visits, hospitalizations, outpatient mental health services, preventive appointments, and primary care (Gilmore et al., 2022). Notably, even though autistic adults are at increased risk for poor physical and mental health, there is very little research about health issues for autistic adults over the age of 35 (Weir, 2023).
Despite a greater likelihood of health conditions, autistic adults face many systemic barriers in accessing healthcare services. Mason and colleagues (2019) identified several challenges including: communication barriers, sensory sensitivities, and lack of healthcare providers for autism. Systemic barriers such as the location of services, limited healthcare resources, and financial barriers also may preclude healthcare services (Walsh et al., 2020). Perhaps because of the frequent barriers to accessing healthcare services, autistic adults report unmet needs and poor communication with healthcare providers. In alignment with Bronfenbrenner’s (1993) ecological systems theory, it is likely that barriers reflect multiple sources. Specifically, sources may include the autistic adult (i.e. microsystem), the provider (i.e. the mesosystem), and the service delivery system (i.e. the mesosystem). Indeed, in an interview study with 39 autistic adults, Nicolaidis and colleagues (2015) identified system (availability of formal or informal supports), provider (knowledge about autism in adults), and patient barriers (sensory sensitivities) to accessing healthcare services. While several studies have explored the barriers to accessing healthcare services (e.g. Dern & Sappok, 2016; McLean et al., 2024; Wooldridge et al., 2017), few studies have identified facilitators to access. By identifying facilitators, a solutions-based approach can be developed to improve access to healthcare services. For example, a facilitator may be self-advocacy. While studies have increasingly centered the voices of autistic adults (e.g. Doherty et al., 2022; Mazurek et al., 2023; Nicolaidis et al., 2016), few studies have examined the role of self-advocacy in accessing healthcare services. Self-advocacy is critical in the neurodiversity movement (Botha et al., 2024) in alignment with the “nothing about us, without us” mantra (Charlton, 1998). The purpose of this study was to explore the facilitators and self-advocacy of autistic adults when accessing healthcare services.
It is important to identify facilitators to healthcare service access. In one of the few studies which explored the barriers and facilitators to accessing inclusive healthcare for autistic adults, facilitators included informal and formal supports (e.g. partner, parent, sibling, and care professionals), positive patient-provider rapport, and the ability to schedule appointments online (McLean et al., 2024). While McLean and colleagues (2024) identified several systemic barriers to accessing inclusive healthcare, their study did not explore the role of self-advocacy which is key among autistic adults (Botha et al., 2024). In addition, more research is needed that identifies facilitators to accessing healthcare services; by identifying facilitators, targeted interventions can be developed to improve access. While the extant research has minimally explored facilitators to access healthcare services for autistic adults, there may be some lessons learned from the research about barriers. For example, Nicolaidis and colleagues (2015) suggested that provider training about autism could facilitate access to healthcare services. Altogether, more research is needed to identify facilitators, including the role of self-advocacy, in accessing healthcare services.
Self-advocacy is a critical component of accessing healthcare for autistic adults. While there are many definitions of self-advocacy, to be more encompassing, one may consider a broad definition of self-advocacy: effectively communicating one’s wants and needs (Test et al., 2005). In contrast, “advocacy” refers to speaking and acting on behalf of another person or cause (Wolfensberger, 1977). For decades, the autistic self-advocacy movement has been gaining momentum. In the 1990s, autistic social groups emerged into autistic culture leading to the proclamation that autism is a valid way of being (Singer, 1998). In the early 2000s, the neurodiversity movement was born in response to the advocacy of the autistic community (Kras, 2010; Leadbitter et al., 2021). The autistic community has continued to advocate for their rights, wants, and needs across many domains, including accessible healthcare. In the context of healthcare services, some autistic adults report that accessing healthcare can enhance self-advocacy, while other autistic adults have reported it can be difficult to speak up for themselves (Mason et al., 2021). By exploring the ways in which autistic adults use advocacy to access services, we can ensure that self-advocacy is effective.
Given the increased healthcare needs of autistic adults and the plethora of barriers in accessing healthcare services, it is critical to explore facilitators and self-advocacy in healthcare service access. While barriers to healthcare services have been explored (e.g. McLean et al., 2024; Nicolaidis et al., 2015), it is possible that facilitators are not the inverse of barriers. Thus, this study extends the literature by exploring facilitators to healthcare. Our research questions were as follows: According to autistic adults, (1) What are the experienced and desired facilitators of healthcare services?; and (2) How does self-advocacy impact accessing healthcare services?
Method
Researcher identity and reflexivity
Our team included two university researchers, two graduate students, and two self-advocates with disabilities, one of whom has autism. Two team members reported having autistic family members. Altogether, our team had experience working alongside autistic adults as family members, advocates, and service providers; we each value self-determination among autistic individuals. To address our experiences, we conducted whole and small group discussions throughout data analysis. Detailed field notes and meeting notes were taken and revisited alongside interview transcripts to aid group discussions. Each team member engaged in peer debriefing and group conversations to identify and mitigate biases, as well as to challenge instances of ableism throughout data collection and data analysis.
Research design
We used social constructivism as the epistemological perspective because our purpose was to explore the lived experiences of autistic adults with their access to healthcare. This study is part of a larger study to adapt a healthcare services app for autistic adults. We conducted individual interviews (versus focus groups) to maintain the privacy and confidentiality with each participant as healthcare can be a sensitive topic.
Participants
Altogether, 15 autistic adults participated in this study. To be included, participants had to have a professional or self-diagnosis of autism and be at least 18 years of age. Most participants had a professional diagnosis of autism (n = 14; 93.33%). Most participants were White (n = 11; 73.33%). On average, participants were 37.93 years of age (SD = 10.00; range from 20 to 51). Participants resided in 11 states across the United States. Slightly more than half of participants had graduate degrees (n = 8; 53.33%). Fewer than half of the participants identified as female (n = 7; 46.67%). See Table 1.
Participant demographics and characteristics.
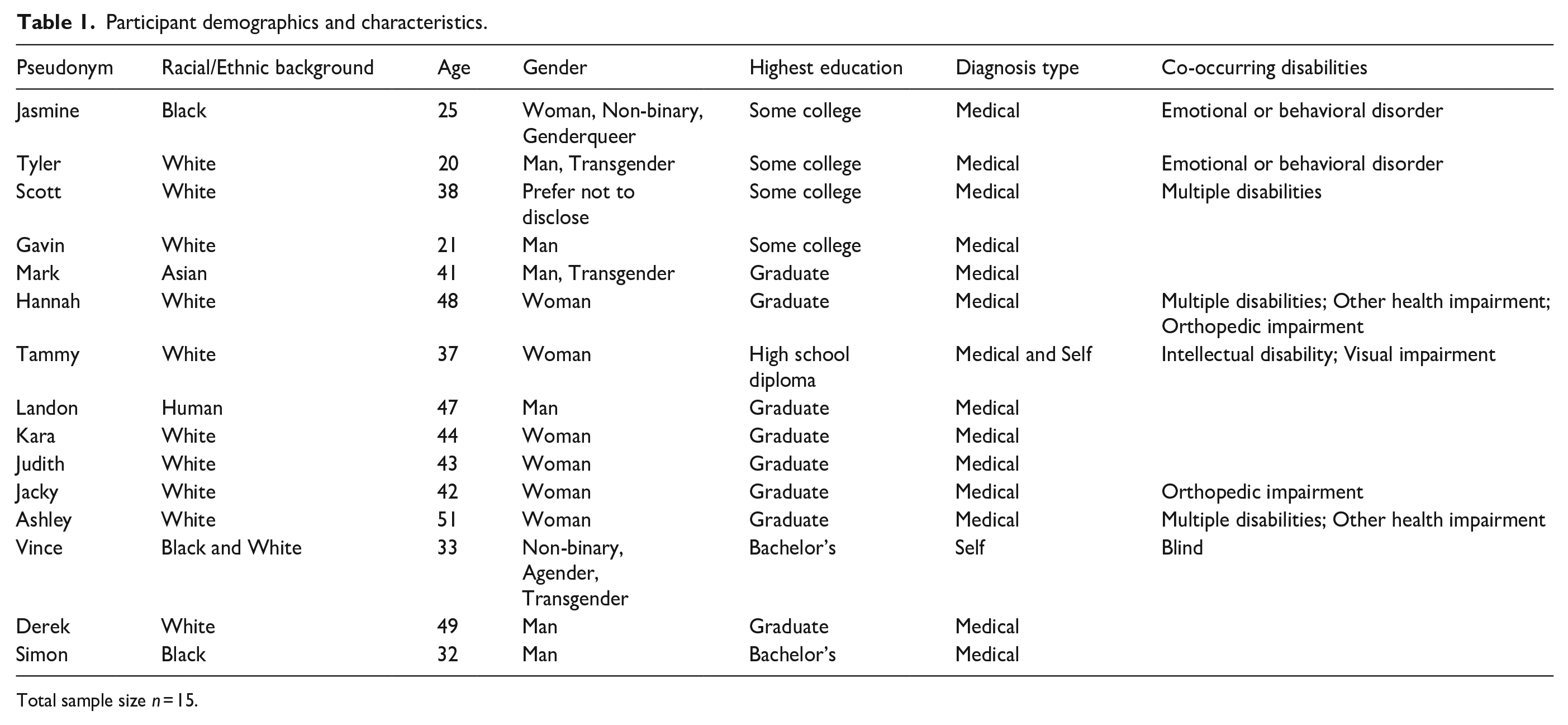
Total sample size n = 15.
Recruitment
Participants were recruited in multiple ways. Recruitment methods included word-of mouth as well as sharing information about the study via social media, flyers, and websites specific to autism and self-advocacy. Recruitment finished once data saturation was reached due to redundancy of themes and both the richness and thickness of data had been achieved (Burmeister & Aitken, 2012; Dibley, 2011). Participants were compensated a total of US$75, or US$25 per interview, in the form of an electronic gift card.
Procedures
This study received University Institutional Review Board approval (Reference Number 24214). Each individual who was interested in participating in this study completed an interest form via REDCap. The research team conducted an eligibility screener to ensure they met the inclusionary criteria. If the individual met the inclusionary criteria, the individual was asked to complete the consent form. Once consent was provided, a demographic questionnaire was sent to the participant. Then, each participant completed three interviews with the research team (Seidman, 2006). Each interview was scheduled at the preferred date and time of the participant. Although all participants were given the option of conducting the interview over Zoom or phone, all participants elected to complete their interviews over Zoom.
The majority (n = 37; 82.22%) of interviews were co-conducted by two researchers, including a co-researcher with a disability. The remaining interviews were conducted by one researcher due to limited research team availability. Two of the three interviewers had prior experience with conducting individual interviews; the first author trained the second author to conduct interviews. At the beginning of the first interview, the research team member(s) introduced themselves and their connection to autism. At the start of the second and third interviews, the research team member(s) asked rapport building statements (e.g. “How is your week going?”). During each interview, the research team members took detailed field notes. After each co-conducted interview, the interviewers debriefed together. In addition, all interviews were debriefed during a weekly meeting by the research team. On average, the first interview lasted 41.60 minutes (range 18–82 minutes), the second interview lasted 47.20 minutes (range 28–76 minutes), and the third interview lasted 54.80 minutes (range 28–94 minutes).
Instrumentation
Questionnaire
All participants completed a brief questionnaire. The questionnaire was developed by the research team and included questions related to their characteristics (e.g. gender, co-occurring disabilities). Participants were also asked to indicate if they needed any accommodations during the interview(s) (e.g. receive interview questions in advance, enlarged text). The questionnaire took 5–10 minutes to complete.
Interview protocol
The three interview protocols were developed based on extant literature about healthcare access and experiences for autistic adults (Calleja et al., 2020; Nicolaidis et al., 2016). The protocols were co-developed by researchers with and without disabilities, including autism. The first interview protocol included questions about healthcare and self-advocacy experiences. During the second and third interviews, participants were asked specific questions related to adapting a healthcare services app for autistic adults. The protocols were reviewed by faculty with expertise in autism. Each protocol was piloted with an autistic adult. As a result of the pilot, small changes were made to the protocols (e.g. minor wording changes to increase clarity, format, or arrangement of interview protocol questions). See Supplementary Materials for the protocols.
Data analysis
We elected to analyze all three interview transcripts for each participant across interview protocols. While we originally considered only coding Interview One to answer these research questions for this study, we found that participants shared information related to facilitators, barriers, and self-advocacy during the second and third interviews. For example, when giving input on specific healthcare services, filter options, or software features of the app, participants often chose to disclose a story or example of why that would be important to them. Participants reported instances of advocacy, specific accommodations they desired or would want to request, and who was helpful to them in healthcare process. Thus, we coded Interviews 2 and 3 during data analysis for these research questions. Notably, we consider it a strength to have coded multiple interviews from each participant as, with each interview, we developed greater rapport with the participant and were able to probe deeper.
All interviews were transcribed verbatim. To familiarize themselves with the data, all six research team members reviewed each transcript multiple times (Tesch, 1990). An initial codebook was developed based on a review of the literature (Nicolaidis et al., 2015) and through constant comparative analysis (Glaser et al., 1968). We employed thematic analysis to code our data, generate themes, and define and name themes (Braun & Clarke, 2006). Initially, each team member independently coded the same nine interviews from three participants (i.e. three interviews per participant). A line-by-line approach was used to individually code all data. Each piece of data was compared with other data, highlighted, and annotated with a specific phrase (Creswell et al., 2003). Each new piece of data was then compared with previously coded data to check if the new data was considered a new code or an existing code. For example, a line of data pertaining to challenges in self-advocacy may be identified as, “Advocacy,” “Self-advocacy,” “Facilitators in self-advocacy.” The research team met weekly to compare codes and resolve differences. Once the nine transcripts were coded, the research team finalized a draft of the codebook. The remaining 36 transcripts were coded in pairs by five research team members. Each team member, in the pair, independently coded the transcript(s). Then, the pair met to compare codes and resolve differences. All research team members met weekly to discuss and reconcile codes.
Once all data were coded, the codes were grouped into categories and organized into themes grounded in the data. For example, the theme of “learning self-advocacy” was derived from the following categories: past experiences advocating, parent support when learning about self-advocacy, and knowledge of one’s self prompting advocacy. If there were any disagreements when coding, team members met to discuss the codes until consensus was reached.
Community involvement statement
One autistic adult participated in this study in various ways, including the design of this research study and related materials, co-facilitation of interviews, data analysis, interpretation of findings, and write up of the present manuscript. One member of our research team is a family member of an autistic individual. This research team member was also involved in the design of this research study and related materials, co-facilitation of interviews, data analysis, interpretation of findings, and write up of the present manuscript.
Trustworthiness
The research team made several efforts to ensure the trustworthiness and credibility of this study. We conducted first-level member checks, maintained an audit trail, reviewed our initial themes for disconfirming evidence, and sought to provide rich detail and participant quotes that captured their experiences (Brantlinger et al., 2005). Regarding the member checks, we created a written, two-to-three-page summary of each interview for each participant to review. Altogether, 11 participants responded to the member check; only two had feedback which included minor changes. We engaged in data triangulation by using different data sources within the study (Trainor & Graue, 2014) and purposive sampling and reflexivity to ensure the experiences and voices of the participants were captured and centered (QR Collective et al., 2023).
Findings
Experienced and desired facilitators to accessing healthcare services for autistic adults
System-level factors
System-level factors are healthcare interactions that are a part of a larger context than the autistic adult and/or the provider (Nicolaidis et al., 2015). Factors included formal and informal supports and accessibility of healthcare facilities. See Table 2.
Overview of findings.
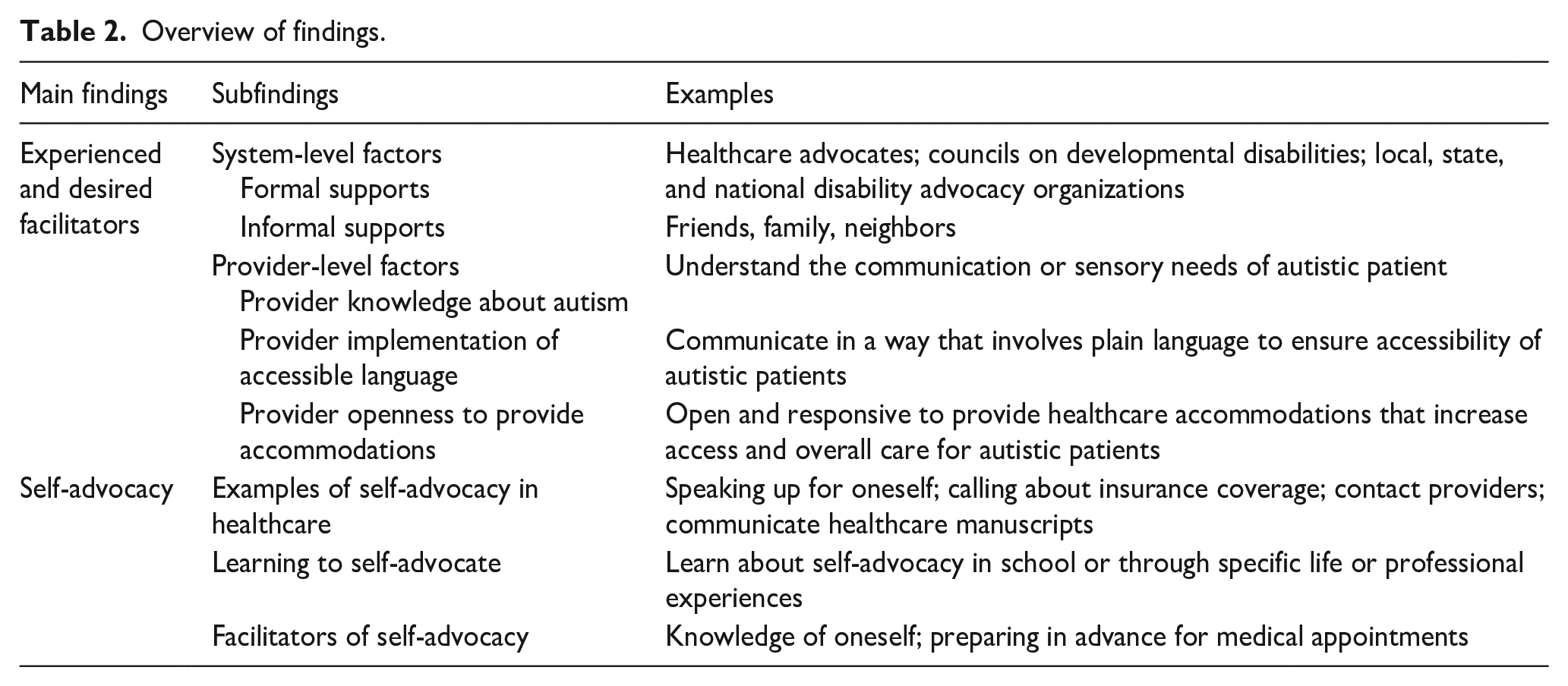
Multiple participants reported desiring formal supports (e.g. healthcare advocates, Councils on Developmental Disabilities, local, state, and national autistic and disability advocacy agencies) and utilizing informal supports (e.g. friendships). Mark, a 41-year-old Asian transgender man, was an active advocate in the autistic community. He shared about the positive impact of a healthcare advocate on his healthcare experiences. Mark reported that his friend referred him to a healthcare advocate. The advocate supported him to fill out paperwork and provide support during medical appointments. Since he met his healthcare advocate, Mark shared “I don’t have any problems with [healthcare center]. She [healthcare advocate] is awesome . . . when there are questions, I don’t really know how to answer, she is going to help me.” When considering informal supports, Tammy, a 37-year-old woman with multiple disabilities, shared that a friend provided transportation when she had a dental procedure. Tammy shared, “I was very happy that my friend gave me a ride, because that meant I didn’t have to fuss with the bus on my way back because I was put to sleep. I was knocked out for that procedure.” Participants reported wanting more formal and informal supports.
Participants shared desired facilitators such as staff support to locate offices, clear language from providers on the care they are providing, and sensory considerations to increase accessibility in healthcare facilities. Vince, who is also blind, shared that it would be helpful if office staff were willing to meet patients in the parking lot as it can be difficult to find an office in a larger building. Vince explained, “One thing that would really help is just someone to be able to meet me in the lobby or something and walk with me to the appointment. That would be super helpful.” In addition, Vince shared about a desire for healthcare services to extend into the home to ensure everything was safe, given their blindness, stating, “It would be really helpful if there was someone who could help us out to make sure certain things are safe. That is another part of health.” Landon, a 47-year-old man, suggested that providers support autistic individuals by communicating what they are doing. Landon shared, “Let us know what you’re doing and why you’re doing it and be clear and calm. So that we have a measured understanding of what’s going on. So that we can digest and processes everything and not get overwhelmed.” Tyler, a 20-year-old White transgender man also shared that “lowering the lights” or having an option to have them off can be helpful. He also explained that telehealth can often help in accessing healthcare stating, “If you have access to telehealth, that would make things much easier, because you could just use zoom or something.”
Provider-level factors
Provider-level factors are defined as factors related to healthcare providers themselves and how these factors interplay with patient factors (Nicolaidis et al., 2015). Such factors included provider having knowledge about autism in adults, providers’ use of accessible language, and providers’ openness to providing other accommodations.
Nearly all participants reported that they desired healthcare providers to have more knowledge about autism in adults. Derek, a 49-year-old White man, detailed how it can be difficult to identify providers as they often change:
There seems to be constant personnel turnover. And that’s particularly challenging for us. Because when I find any sort of professional that I need help with, that professional can’t just be a professional. That person also has to be knowledgeable about autism. So, there’s an extra layer of expertise. So, it’s not that hard to find a doctor, but to find a doctor who has some understanding and compassion when it comes to autism, and it’s hard to find.
Jasmine, a 25-year-old Black individual shared about the stigma she had experienced from her medical professionals and her desire for providers to be more knowledgeable about autism. When asked about a recent healthcare experience and if the provider was knowledgeable about autism, Jasmine responded, “I would definitely say no. The first time I saw that provider, he told me that I’m pretty smart, which is of course, the usual . . . you know, you get the ‘your extremely smart, I can’t tell that you’re autistic.’” Jasmine went on to share, “I would really love for doctors to work with affirming autistic organizations.” Ashley, a 51-year-old White woman with a graduate degree, shared how impactful it would be to have a list of neurodivergent physicians and therapists. Ashley reported that a neurodivergent provider would make her feel more comfortable at healthcare appointments: “We [neurodivergent individuals] wouldn’t want to overwhelm the neurodivergent providers, but I think it would be really nice to have that information available when seeking a provider.” By increasing the knowledge healthcare providers have of autism, it may improve the healthcare access and experiences of autistic adults.
Many participants reported a desire for healthcare providers to use accessible language. Kara shared, “I want providers to explain what is going on using their own words and not the systems words.” Jasmine expressed how frustrating it has been in the past to see a provider who did not use accessible language. In response, she suggested, “It would be better to maybe provide some kind of plain language summary.” Tammy, a 37-year-old White woman who also identifies as having an intellectual disability and visual impairment, recounted previous experiences she had when seeing a provider. Tammy recalled how much of the communication with the provider was verbal and that sometimes she will remember to ask for a pamphlet or something stating, “Or I’ll get really lucky and they’ll give me a pamphlet and some information about what’s going on, what to do afterwards, all the good stuff.” Judith, a 43-year-old White woman shared how it has been helpful to her when providers are open to providing accommodations. Judith shared, “[It is helpful] when doctors begin to understand the sensitivities and accommodating to the needs of the individual patient, rather than trying to follow the medical textbook word for word and in the name of equality, forcing everything on everyone.” Scott, a 38-year-old individual, shared that navigating different providers can be difficult and prefers when their providers can communicate directly with them. Scott shared, “I like how they communicate with me because some [providers] do and some do not.” When providers use accessible language and materials, it allows for deeper understanding and access to important medical information needed to make informed decisions.
Participants shared a plethora of accommodations that providers could proactively provide that would be of benefit to them when accessing healthcare services. Tyler shared about how there should be specific waiting room accommodations, such as “having an option to wait in the car rather than the waiting room.” Jasmine shared, “I would have liked social or sensory stories when going to the doctor so that way I would know about the expectations on the ‘what’ and ‘why’ I’ll be going to the doctors.” Jasmine further shared that it would be helpful if doctors would be willing to talk slower given her auditory processing issues. Mark shared many accommodations such as providers offering translation services or visual supports. Put simply, Derek stated, “I think all of us. Every human being on the planet, if we had the right accommodations and supports for what we need to thrive and be successful . . . we would do amazing work.”
Self-advocacy and healthcare services for autistic adults: examples of self-advocacy in healthcare
Participants reported many ways in which they advocated for themselves when accessing healthcare services. Participants reported speaking up for themselves, calling about insurance coverage, contacting providers, and communicating their preferences during medical appointments. When asked about how they access healthcare services, Vince discussed how they and their fiancé, who is also legally blind, work together to schedule joint doctor’s appointments as it makes transportation easier stating, “We basically just speak up for ourselves.” Another example of self-advocacy included calling to get a list of providers who accepted a specific health insurance. While transitioning from his parents’ insurance to his own insurance, Tyler shared:
So, I was calling [organization] to get a list of providers, but I still, when I was calling providers, wanted to double check that they took my insurance just in case there was problems, which there were fun and exciting differences . . .and when I say fun and exciting, that’s sarcastic or facetious.
Participants also shared about asking questions and expressing their medical needs with providers. Mark reported advocating in multiple mediums (e.g. the online portal, leaving messages): “I just went to the patient portal, sending them emails, leaving them messages, like a couple of emails.” Mark had to remain persistent in his self-advocacy to ensure his questions were answered and his medical needs were met. Participants also shared about their self-advocacy during medical appointments. Judith shared an experience where her self-advocacy ensured that no unnecessary procedures were done:
They asked me if I would be comfortable having one of those [gynecological] exams, and I actually said “no,” because part of the Asperger’s is I’m hypersensitive, and so I can’t tolerate those exams. I tried to have one once and it set off a panic attack.
Overall, participants reported advocating for themselves in many ways for healthcare.
Learning to self-advocate
Many participants reflected on their journey with self-advocacy. Participants considered not only how they self-advocate when accessing healthcare services, but how they learned to self-advocate and what circumstances brought them to advocate for their care needs. Participants reported learning about self-advocacy in specific places, such as at school, or learning about self-advocacy through specific life experiences. Kara shared about her journey as a self-advocate. She discussed how her experience in the Peace Corps and traveling to almost 20 countries helped her to learn how to self-advocate. When asked how self-advocacy had impacted her experiences in accessing healthcare services Kara responded, “It’s been everything . . . I didn’t believe I had the right to [ask for medical services]. I had to push through that and accept that I do have the right to speak up and that changed the whole thing for me.” While Kara referenced learning how to self-advocate to access healthcare, Jasmine identified that going to her doctor’s appointments prompted her self-advocacy. When asked when she started advocating for healthcare services, Jasmine shared, “It wasn’t really until maybe a few years ago once I started doing, going to my own doctor’s appointments. That’s kind of when I started to kind of advocate for myself.” Meanwhile, other participants specifically reported learning about self-advocacy through classes or school. Gavin, a 21-year-old college student, recalled back to middle school when he was first introduced to the topic of self-advocacy. Gavin shared, “Originally, I had done some stuff [learning about advocacy] in middle school at this place [local agency] by where I live.” The spaces and ways in which participants learned to self-advocate were individualized, but all participants referenced the impact of self-advocacy on accessing healthcare services.
In addition, many participants reported specifically about the timing or urgency of learning to self-advocate to access healthcare services. Jacky stressed how overwhelming it was to have to learn to advocate for healthcare services due to not receiving an autism diagnosis until she was an adult. Jacky shared, “I just started doing the whole self-advocacy thing, so it’s kind of fresh. I’m in uncharted waters here.” Tyler spoke at length about the transition from seeing a pediatrician to seeing a primary care physician: “I’ve had to learn how to self-advocate very quickly, which I don’t like, and then the other thing, it’s hard for me to know when something [medical need] is a big enough concern to go to a doctor.” Many participants shared about how the stages of life, including when they received an autism diagnosis, influenced the necessity to learn and grow in their self-advocacy to ensure access to healthcare services.
Facilitators of self-advocacy
A key facilitator was knowledge of oneself. Kara identified the need to accept oneself first before you can advocate for your own wants and needs explaining:
I don’t see the stigma and discrimination as much now that I am comfortable with who I am. I approach people without the [camouflage] mask. I am my authentic self. They see that I’m comfortable with who I am. I like who I am.
Simon, a 32-year-old Black man, further touched on the need to know oneself, stating, “I know that I need support . . . I know that if I don’t speak, then nobody’s gonna speak for me. With this knowledge, I tend to put my [medical] sheets together to express myself so my condition can be understood.” Derek, who regularly participates in self-advocacy and supporting autistic adults in advocating shared similarly, “I’ve gotten pretty good at explaining things to doctors in a way that they at least have some understanding so they can not only serve me better, but other autistic adults.” When participants had knowledge of themselves and their medical needs, they were able to better advocate for healthcare services which facilitated greater access to medical care.
Another facilitator to self-advocacy was preparing questions in advance for a healthcare appointment or interaction with a healthcare provider. As Gavin reflected on the courage it takes to advocate, he also shared about how he prepares questions in advance for healthcare appointments sharing, “[You need] to make sure you ask all your questions that you need to ask.” Tyler shared about his current endeavors to find a new primary healthcare provider and how he had been compiling questions to be able to ask in the upcoming weeks. Tyler shared, “It is really helpful to be able to prepare and like ask questions and get them answered.” By preparing questions in advance, participants were able to advocate for services.
Discussion
While autistic adults often have greater need for healthcare services, they also face greater and/or unique barriers to accessing services. To extend prior research, which mostly identified barriers to accessing healthcare services and provides limited findings related to self-advocacy and healthcare, our study explored facilitators to accessing such services and the role of self-advocacy. We had three main findings. First, self-advocacy occurs in healthcare access. This finding underscores the importance of self-advocacy as aligned with the neurodiversity movement (Kras, 2010; Leadbitter et al., 2021). Indeed, this finding not only conforms with the tenet of the importance of self-advocacy, but also suggests empirical evidence that self-advocacy can impact service access. More research is needed to parcel out the types of advocacy that may lead to improved access to healthcare services. For example, in special education, Trainor (2010) characterized advocacy as four strategies: disability expert, intuitive advocacy, agent of systems change, and strategic advocate. Research in the context of advocating for healthcare services, may consider whether similar advocacy strategies exist and, if so, their degree of effectiveness in improving service access. Research is also needed about self-advocacy. Specifically, research is needed to understand how practitioners (e.g. school professionals) and families may support or hinder self-advocacy among autistic individuals. On the one hand, it may be that families support self-advocacy and self-determination (Moser et al., 2025). Conversely, it may be that parent advocacy may occlude the autistic adult from their own advocacy. More research is needed to target supporters of self-advocacy while mitigating barriers to self-advocacy.
Second, autistic adults valued both formal supports and natural supports as facilitators to service access. This finding underscores the importance of the balance of both types of supports for autistic adults. To date, more research about supports examines formal supports to the exclusion of natural supports (Nuri et al., 2024). The limited research about the balance of supports is problematic, as autistic adults value both types of supports. The limited extant research is also problematic given that, in the United States, only 25% of adults with disabilities (including autism) receive formal supports (Rehabilitation and Research Training Center at the University of Minnesota, 2022). This finding suggests that more research is needed to explore the balance of formal and natural supports in improving access to healthcare services.
In the context of self-advocacy, the roles of natural and formal supports are also important. Participants reported relying on friends (natural supports) and healthcare advocates (formal supports) to access healthcare services. While such supports were characterized as “facilitators,” it is possible that natural and formal supports could negatively impact self-advocacy. Some research suggests that supporters (e.g. parents, siblings) could be overprotective of autistic adults and reduce their ability to self-advocate (Thompson-Hodgetts et al., 2023). Future research may consider interviewing autistic adults and their supporters (both natural and formal) to explore how self-advocacy can be promoted (not inhibited) by supporters.
Third, facilitators were identified related to system issues, providers, and autistic adults themselves. This finding aligns with prior research (Nicolaidis et al., 2015) about barriers to healthcare services underscoring that there are multiple issues which impact access. Further, the barriers map onto an ecological approach to understanding access to healthcare services (Bronfenbrenner, 1993). This finding suggests that targeting an intervention at only one of these ecological systems (i.e. micro, meso, or macro) would be insufficient to completely mitigate barriers to service access. Instead, a holistic approach is needed to reduce barriers and increase facilitators within each system.
While this study had several important findings, there were also some limitations. The sample was nearly entirely comprised of autistic adults without an intellectual disability and held limited racial and ethnic diversity; thus, the findings may have limited transferability. Future research should include a more representative sample. Relatedly, research may consider whether there are unique facilitators in relation to one’s support needs or other aspects of their background (e.g. race, ethnicity). Also, this study was based on cross-sectional data of three interviews within a six-month time span. It is unclear how facilitators and self-advocacy may change over time.
Directions for future research
An important next step for research is to explore intersectionality in the context of healthcare service access. As demonstrated from this study, some participants who had co-occurring disabilities (e.g. blindness) reported some unique accommodations and facilitators. Given that autistic adults are more likely to have co-occurring disabilities (e.g. anxiety, Linden et al., 2023), it is important to consider the intersectionality of multiple disabilities in the context of healthcare service access. Relatedly, other aspects of intersectionality should also be explored including race, ethnicity, and gender. Regarding race and ethnicity, prior research has suggested, for example, compared to White autistic adults, that Black autistic adults have different life experiences, including stigma and discrimination (Malone et al., 2022). Autistic females (versus male) report unique experiences in relation to camouflaging their autism (Goscicki, 2023). Future research should explore intersectional traits among autistic adults to understand their nuances in accessing healthcare services.
Future research should also consider longitudinal research. In this study, participants reflected on their beginning attempts at self-advocacy, suggesting that the evolution of their self-advocacy may impact service access. Yet, little research has explored the beginnings of self-advocacy among young autistic children. In the general disability population, though, it has been documented that self-advocacy and self-determination can and should begin at young ages (Palmer et al., 2013). By collecting longitudinal data about the nature of self-advocacy over time, we can identify points wherein self-advocacy needs to be strengthened and ways in which practitioners can best support autistic adults to be self-advocates.
Implications for practice
In alignment with prior research about healthcare service access for autistic adults (e.g. Dern & Sappok, 2016; McLean et al., 2024; Nicolaidis et al., 2015; Wooldridge et al., 2017), more training is needed for healthcare providers to learn about autism and offer accommodations. Based on this study, healthcare providers may need training about how to work with advocates to ensure that all medical care is person-centered. Relatedly, it is important to train providers who are neurodiverse themselves to increase the representation of autistic adults within the healthcare workforce. To these ends, training programs may consider embedded content about autism, focusing on sharing the lived experiences of autistic adults themselves.
While several implications for practice relate to large and perhaps expensive systemic changes (e.g. revising the messaging portals between providers and patients, training the workforce about autism), some implications may be simple and low-cost. For example, providers may offer plain language, accessible summaries of appointment visits to patients, or classes or resources on how to advocate in healthcare spaces. Providers may also offer accommodations (e.g. lowering the light in the room; offering to walk someone from the parking lot to the office). Such accommodations may be easy to provide and increase access to services.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251343350 – Supplemental material for From awareness to action: Facilitators and advocacy in healthcare by autistic adults
Supplemental material, sj-docx-1-aut-10.1177_13623613251343350 for From awareness to action: Facilitators and advocacy in healthcare by autistic adults by Megan Best, RaeAnne Lindsay, Sarah Demissie, Isabelle Burakov, Saury Ramos-Torres and Meghan Burke in Autism
Footnotes
Acknowledgements
The authors gratefully acknowledge the contributions of the participants in this study.
Author contributions
Data availability statement
The authorship team has elected not to publicize data due to concerns around anonymity. The authorship team may be contacted for specific questions or further inquiry.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: We confirm that all the authors have had material input into the submission. We confirm that, to our knowledge, all the claims, statements and conclusions are true and are our jointly held opinions. We confirm that we all accept the terms of publication of the publisher.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under the Autism Intervention Research Network on Physical Health (AIR-P) grant, UT2MC39440. The information, content and/or conclusions are those of the authors and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
Compliance with ethical standards
Institutional Review Board approval was received for this study. All participants consented to participating in this study by reviewing and signing a statement of informed consent.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.