
Abstract
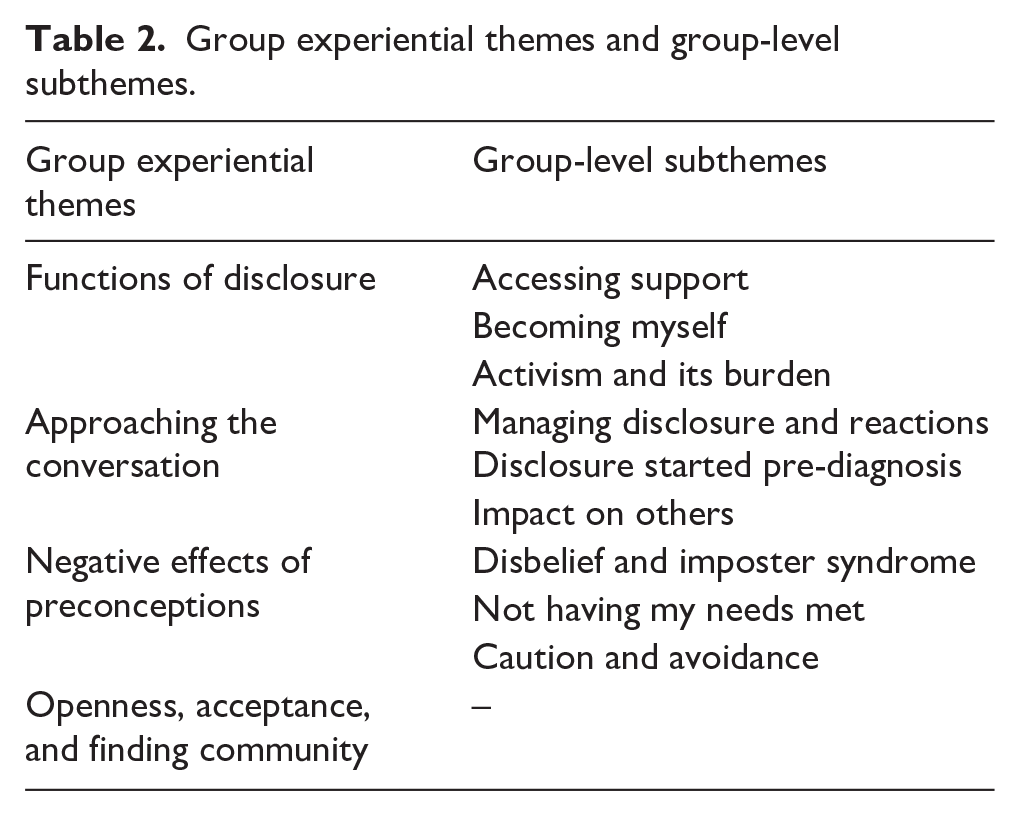
An increasing number of people receive autism diagnoses in adulthood, and there are few studies investigating autistic adults’ experiences of disclosing their diagnosis. This study sought to understand autistic adults’ experiences of diagnostic disclosure using interpretative phenomenological analysis. Twelve autistic adults, who received their diagnosis in adulthood, participated in one-to-one semi-structured interviews exploring their experiences of diagnostic disclosure. Quality control and reflexivity procedures were used to ensure rigour. Four group experiential themes and nine subthemes emerged: (1) ‘Functions of Disclosure’ (subthemes: i. Accessing Support; ii. Becoming Myself; iii. Activism and its Burden); (2) ‘Approaching the Conversation’ (Subthemes: i. Managing Disclosure and Reactions; ii. Disclosure Started Pre-Diagnosis; iii. Impact on Others); (3) ‘Negative Effects of Preconceptions’ (Subthemes: i. Disbelief and Imposter Syndrome; ii. Not Having My Needs Met; iii. Caution and Avoidance), and (4) ‘Acceptance, Openness and Finding Community’. Disclosure served multiple functions for the autistic participants. There was variability in the support that autistic participants received in preparation for disclosing the diagnosis. More consistent post-diagnostic support is required to engage newly diagnosed autistic adults in considering the practicalities and potential consequences of disclosure, its benefits and challenges.
Lay Summary
An increasing number of people are receiving diagnoses of autism in adulthood. However, there are few studies investigating autistic adults’ experiences of ‘disclosure’, that is, telling others about their autism diagnosis. The aim of this study is to understand autistic adults’ experiences of telling other people that they are autistic after receiving a diagnosis during adulthood. Twelve autistic adults were interviewed about their experiences of disclosure. The interviews showed that autistic people disclose to access support, be themselves and to help others. To disclose, autistic people had to make decisions about what information to share and how to handle people’s reactions. Some people started telling others about their potential diagnosis before being formally diagnosed. Disclosure has an impact on people receiving the news of disclosure. Many autistic people experienced not being believed, resulting in unmet needs. This led them to be more careful about future disclosure. However, disclosure also led to some positive experiences, where autistic people felt listened to and accepted by those they disclosed to. This led to receiving support and feeling part of a community. It is recommended that clinicians and autism service providers include discussions about disclosure as part of routine post-diagnostic support.
Introduction
After going through a diagnostic process and receiving an autism diagnosis, autistic people may choose to share their diagnosis with others. Currently, there is a lack of clear and detailed guidance on what post-diagnostic care should look like for autistic adults. While clinicians are recommended to talk to the newly diagnosed person about the implications and concerns about the diagnosis and any future support needs, there is no advice about how clinicians should go about this (Beresford et al., 2020; National Institute for Health and Care Excellence [NICE], 2012). Accessing support post-diagnosis, such as reasonable adjustments under the Equality Act, UK (2010), often requires an individual to disclose their diagnosis, and it is therefore not only important that autistic people are receiving timely diagnosis (Rutherford et al., 2016) but also to be engaged in preparation to effectively communicate their diagnosis. A recent evaluation of an autism-led programme supporting newly diagnosed and self-identified autistic individuals (Crane et al., 2021) found that exploration of issues around disclosure was valued by participants and helped them develop a positive outlook on being autistic. Similarly, a recent Delphi study (Crowson et al., 2024) demonstrated that autistic adults would like practical support with disclosure.
Research on autistic people’s experiences of disclosure has often focussed on the workplace context. A systematic review by Lindsay et al. (2021) explored disclosure and workplace accommodations for autistic people and noted that there were both pros and cons of disclosure in the workplace. Benefits included achieving a greater sense of acceptance and receipt of support during the recruitment process. Furthermore, the review identified that disclosure facilitated adaptations in working patterns, support and increased autism awareness. Negative outcomes of disclosure included experiences of stigma and discrimination. A qualitative study cited with Lindsay et al.’s review found that autistic participants diagnosed at a younger age perceived less discrimination disclosing their disability compared to those who were diagnosed later in life (Johnson & Joshi, 2016), highlighting age of diagnosis as an important factor influencing the disclosure experience.
Up until now, no studies have directly investigated autistic people’s experiences of disclosure within the United Kingdom. Disclosure experiences are likely to vary across cultures and influenced by stigma within a particular system context (McDonald et al., 2020). Within Lindsay et al.’s (2021) review, only one UK study was found, though this study did not examine disclosure directly (Richards, 2012), rather, it explored reasons why autistic employees were excluded from the workplace using secondary qualitative datasets. The study found that disclosure of a diagnosis on job applications had led to autistic jobseekers being excluded during the selection stage and these were perceived to be due to employers not being willing to make reasonable adjustments for those who declare a disability. In recent years, there has been implementation of a national strategy (UK Government, 2021) to improve public understanding and acceptance of autism within the United Kingdom as well as improving support for autistic people across different areas, including employment, healthcare, education and the justice system. It is therefore important to understand whether these changes have influenced autistic people experiences of disclosure within the context of the United Kingdom.
One important factor that could influence disclosure experience is age at diagnosis, as people diagnosed in childhood are likely to have less autonomy over whether a diagnosis was sought out (Huws & Jones, 2008) and therefore this could potentially influence whether a person chooses to disclose or not. Hence, there is a need to consider similarities and differences of disclosure experiences of autistic people diagnosed in childhood and those diagnosed in adulthood. One Australian study (Huang et al., 2022) reported a mixed method survey investigating autistic adults’ decision-making for disclosure and nondisclosure across different contexts. Using content analysis, they found reasons to disclose included wanting to help others gain understanding; raising public awareness; and to express autistic identity. Reasons for nondisclosure included avoiding anticipated misunderstandings and prejudice, lack of relevance and not wanting to be labelled. In line with Lindsay et al.’s (2021) review, Huang et al. (2022) also found that there were both positive and negative consequences of disclosure. Negative experiences of disclosure may not only create unnecessary stress for autistic people but could also subsequently affect future decisions to disclose, leading to withdrawing from or losing out on important support that they need (Dugdale et al., 2021). While the study by Huang et al. provided some direct insight into experience of autism disclosure, the study sample included autistic people who received their diagnosis across both childhood and adulthood; therefore, it was not possible to identify the specific challenges experienced by those diagnosed in adulthood. Therefore, a study to specifically investigate the experiences of autistic people diagnosed in adulthood is required.
This study explores how autistic adults in the United Kingdom experience the process of disclosing their autism diagnosis to others. The study seeks to understand idiosyncratic contexts associated with decisions to disclosure or not to disclose. It is interested in understanding where, why and how autistic people make sense of their experiences of disclosure following diagnosis in adulthood. Second, given the limited guidance within the United Kingdom as to what post-diagnostic support should look like, and the growing interest in improving post-diagnostic support, a study to specify recommendations in this area based on actual experience is required. The clinical implications of the findings will therefore be discussed.
Methods
Design
Interpretative phenomenological analysis (IPA, Smith et al., 2021) was used to explore autistic adults’ experiences of disclosure and semi-structured interviews were conducted individually with autistic people who received their diagnosis in adulthood. This provided in-depth first-person accounts of autistic people’s experiences. The IPA approach allows open-ended responses from participants to be analysed in a way that allows researchers to engage in a double hermeneutic process to make sense of participants’ making sense of their own experiences. It also allows the identification of similarities and nuances in a particular phenomenon (diagnostic disclosure) experienced by a specific group (autistic people diagnosed in adulthood) within a given context (diagnosed in the United Kingdom in the last 10 years). The IPA approach has been gaining prominence within autism research in recent years and is a valued approach by both the autistic community and researchers (Dugdale et al., 2021; Howard et al., 2019; Smethurst et al., 2024).
Community involvement
Two autistic adults were consulted regarding the development of the interview questions (see Supplemental Materials S1), and all participant facing documents. Consultations were conducted over email communications or during an online meeting based on the autistic adults’ preferences. Changes were made to the materials based on these consultations.
Participants
Participants were 12 autistic adults (aged 18 years or over) who received a clinical diagnosis in adulthood within the last 10 years and living in the United Kingdom. Purposive recruitment of people meeting these inclusion criteria was performed via information being shared with autistic people who have signed up to the Sheffield Autism Research Lab database and via social media advertisements. Participants’ characteristics are summarised in Table 1. Pseudonyms are used throughout the article when referring to participants, and these were chosen to be in line with the traditional assumed gender of the names participants would like to be known by.
Participant characteristics.
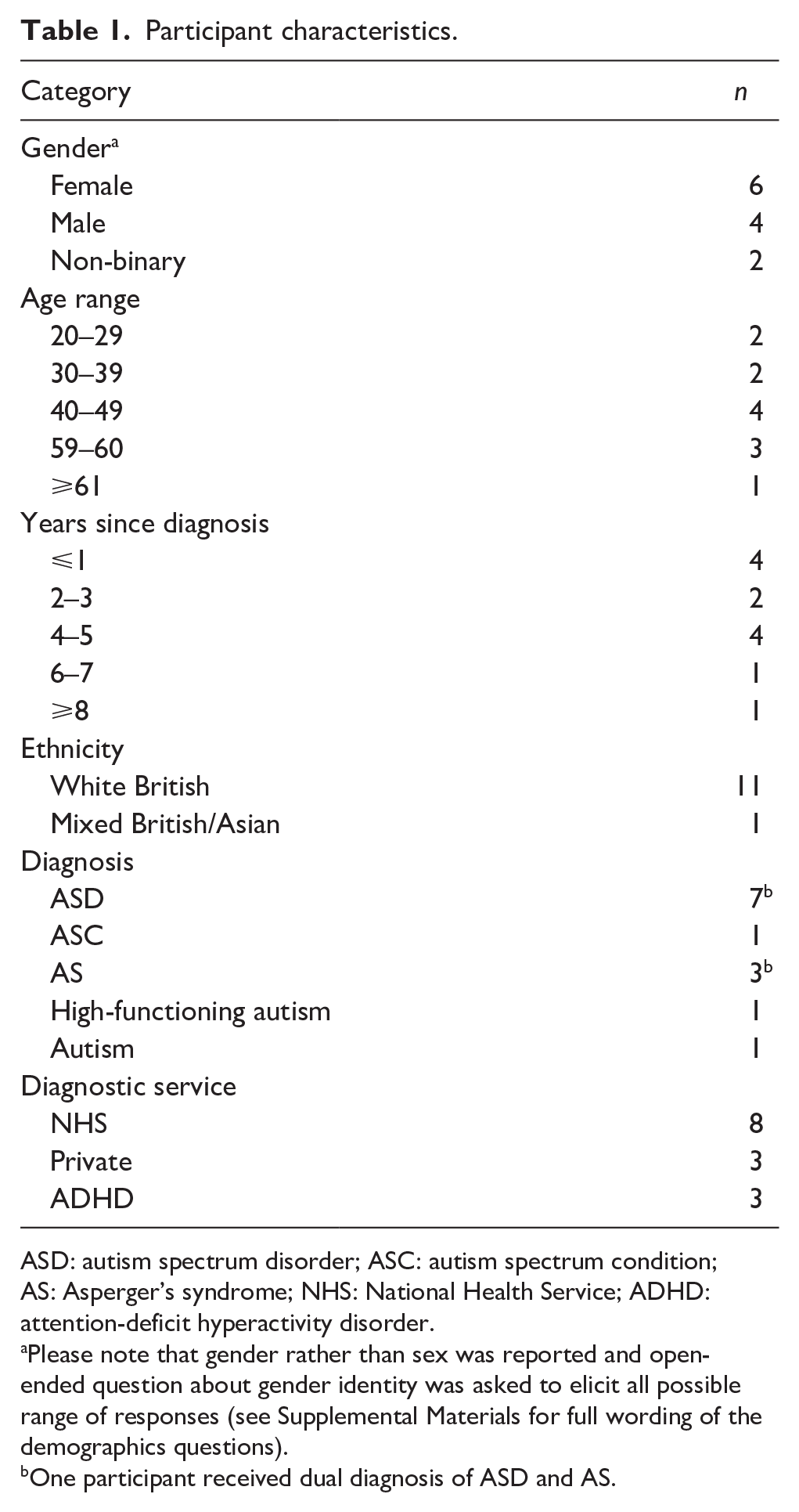
ASD: autism spectrum disorder; ASC: autism spectrum condition; AS: Asperger’s syndrome; NHS: National Health Service; ADHD: attention-deficit hyperactivity disorder.
Please note that gender rather than sex was reported and open-ended question about gender identity was asked to elicit all possible range of responses (see Supplemental Materials for full wording of the demographics questions).
One participant received dual diagnosis of ASD and AS.
Procedures
Ethical approval was received from University of Sheffield Department of Psychology Ethics Committee (ID: 051331). Participants provided written informed consent form prior to participation. Interviews took place at the university or online via Googlemeet and lasted approximately 1 hour. Recording was made using a dictaphone or the Googlemeet recording function. The interviews started off with demographics questions on gender, age, age at diagnosis, ethnicity, type of autism diagnosis, service at which diagnosis was received and other co-occurring neuro-developmental conditions (see Table 1; Interview Schedule in Supplemental Materials S1) which were then followed by open-ended questions on diagnostic disclosure. The interview questions on diagnostic disclosure acted as a guide to the interviewer to ensure that all key topics were covered rather than being followed verbatim. Participants were debriefed after the interview and received a £10 shopping voucher.
Analysis
The interviews were transcribed verbatim and non-verbal utterances were noted in brackets. The transcripts were checked against the recordings to ensure accuracy and identifiable information was redacted.
Data analyses were completed using Nvivo 10 for Windows (n.d.). The first author read and re-read each transcript to gain an initial impression of the data. Initial notes were made to systemically capture observations, which included descriptive, linguistic and conceptual comments (see Supplemental Materials S2). Personal Experiential Statements that reflected the understandings gained from the initial notes were then identified. Connections identified across the Personal Experiential Statements were used to support the creation of Personal Experiential Themes (PETs). Once this process was completed for every participant, PETs from all participants were exported into Microsoft Powerpoint to facilitate examination of patterns across different participants’ accounts and create a set of evidenced Group Experiential Themes. A sample of the data throughout the analysis process was audited by the second and third authors to ensure the IPA process were completed thoroughly. The principles recommended by Yardley (2017) for qualitative research were applied to ensure quality and rigour of the study (see Supplemental Materials S3).
Positionality and reflexivity
The first author identifies as a person from an ethnically minoritised background in the United Kingdom and had experience working within autism research and mental health settings. The first author kept a reflexive log which included notes of observations and reflections of interview and analysis processes, which enabled them to consider the impact of their personal and professional identities, experiences, knowledge and preconceptions on their interpretation of the data. The IPA approach acknowledges that the researcher’s characteristics and pre-existing personal and professional experiences will influence the interpretation of the data. Careful recognition and use of such a ‘lens’ is seen as essential to the interpretation and development of the data obtained (Shaw, 2010; Smith et al., 2021).
Results
The analysis identified four group experiential themes and eight subthemes (Table 2). Additional supporting quotes can be found in Supplemental Materials S4.
Group experiential themes and group-level subthemes.
Functions of disclosure
Accessing support
Participants disclosed their diagnosis for practical reasons in various settings, including employment and health and social care, to access adjustments and legal protection. Past experiences of being marginalised meant that autistic people felt a need to defend themselves via disclosure of a formal diagnosis:
Without the diagnosis, you don’t get things like social service support and all the kind of benefits that you need because you tell them your symptoms, but they don’t believe you. (Tina)
Awareness of situations where they felt likely to be misunderstood also meant that they disclosed in daily life to manage social interactions and stressful situations in the hope that others would be more understanding towards them:
um, I thought it was useful to have that, to disclose, to have that level of protection. So that if anything I guess if anything went wrong, or I was, I got into a a difficult position of there was some misunderstanding and I felt, you know, what was which was, which put me in a vulnerable position or I felt very uncomfortable about that I would have some extra protection there to to to use. (Eric)
Becoming myself
Sharing one’s diagnosis with others also served a psychological function, allowing participants authentically ‘be yourself’ (Rachel) after years of masking. This was important within personal life with loved ones, as well as with their working life. For participants, like Michael, disclosure at his workplace represented an act of self-acceptance of his differences and meant that he felt more able to resist the pressure to conform to neurotypical social norms and be less critical of himself:
but I think that feeling of missing out is shorter than the negative feeling I’d have if I went along and was exhausted and really struggling with it . . . and thinking ‘oh but I could have joined in, I could have done this, I could have done that, why didn’t I do that when I was there’, well if I’m not there in the first place then I don’t need to be thinking about it, I’m just, you know, just accept. (Michael)
Activism and its burden
For many participants, disclosure also had an altruistic function. Participants talked about the desire to use their disclosure for ‘helping the autistic community’ (Rachel), to ‘raise awareness’ (Edward) and ‘pushing back’ (Eric) against unhelpful narratives about autism, or to hold organisations accountable for inclusive practices:
I’ve felt empowered now to push them to say a) we should be looking, not necessarily to fill a quota but we should be looking in places where neurodivergent people are because they fill, they fill a lot of the skill sets that we don’t have because it’s a different way of thinking and b), what allowances can we make as an organisation for people that probably have a lot more struggles than I do. (Josh)
Participants talked about enjoying and feeling empowered to do this type of work. However, the sense of moral responsibility can often feel burdensome. This was particularly challenging for someone newly diagnosed if they didn’t yet feel ready to disclose publicly but felt that it is ‘incumbent’ (Rachel) for them to disclose if they want to be involved in activism. Often participants had to consider self-protection and maintaining boundaries, for example, Brandon talked about the challenges and discomfort he faced having ‘different compartments coming together’ between his professional and private life when using his lived experience occupationally. Furthermore, the pressure on autistic people to take responsibility in educating others ‘over and over’ (Liza) again was experienced as exhausting by some.
Approaching the conversation
Managing disclosure and reactions
Some participants felt anxious as they were unsure how people were going to react to their disclosure. Jane described ruminating over whether she was ‘gonna say the right thing, do it in the right way, if it’s going to be appropriate’. These worries appeared to have impact on how participants disclose. Liza chose to ‘drip feed’ information about her diagnosis to others and had to carefully work out which person she felt ‘comfortable telling’ and who were ‘safe’. For Helen, being autistic further complicated the situation as she found it ‘hard to tell’ who may be interested or how they may react.
Participants varied on how comfortable they were regarding being open about their diagnosis. Some chose to share their diagnosis publicly, such as over social media platforms or to colleagues at work. However, even when they become more open about their autism over time, some still ruminated about potential negative consequences, such as thinking ‘am I gonna regret this?’ or ‘is this gonna affect me negatively?’ (Liza).
A minority of participants were able to access advocacy services to support disclosure or private therapy to talk about disclosure. Some accessed post-diagnostic support from their diagnostic service or through community groups. Participants found space to think about disclosure helpful, whether these were one-to-one or in groups, or from professionals or other autistic people. Participants valued hearing others’ experiences of disclosing and talking through different elements of disclosure, including who to disclose to and how, as well as handling people’s reactions:
what if you know, somebody discloses and the reaction they get from family members or colleagues at work, if they’re in work, is almost negative and it’s not what they were expecting, how does somebody deal with that and if there isn’t that support there, you know, somebody that you can go to and say ‘I need a bit of help here’. (Michael)
Impact on others
Participants found that disclosure could be a tricky process in which they had to balance openness and considering the impact it has on others and their relationships. For Eric, he felt hesitant about disclosing as he was aware of the potential impact disclosure could have on his relationships:
. . . maybe slightly awkward . . . I didn’t want anything to escalate into a falling out. So yeah, it was definitely kind of a tentative or wanting to be open and honest and talk about it but not wanting to almost talk about. (Eric)
Furthermore, people’s reactions varied greatly depending on existing relationship dynamics and people’s life circumstances. Participants found that their disclosure often led others to reflect on their neurodiversity. This could be positive as Helen has experienced:
. . . and they’re great about it and I often get emails saying ‘I’ve often thought about myself’. (Helen)
whereas for others, the thought being potentially autistic themselves could be unsettling:
My dad like really reacted badly to it but my dad is actually the person in my family who has the most traits and characteristics erm so I always wonder whether that he saw a lot of himself in me and is now slightly perturbed potentially (LAUGH) by the fact that maybe he fits the criteria. He will never admit that . . . (Jess)
For some parents receiving the news of disclosure, and triggered feelings of guilt:
she felt very like stuck that it was a bad thing like a really negative thing and also maybe erm, was a sign that she haven’t parented me well, or something like it was something that was her fault and was also really I guess might mean that, I was just going to have a really unhappy life. (Olivia)
Some participants found that time and further conversations was required for loved ones to process and adjust to the diagnosis:
you know, cos my family for the most part have just gotten over it, its taken them a long time don’t get me wrong, like it’s taken them years to be able to have a discussion with me about the nature of autism and about autistic culture and rights and stuff. (Jess)
and that they had to learn to tolerate some uncertainties during the process:
. . . it’s an autistic thing to want to control an environment, to want to control a response, to control the conversation, because you feel safer. And I think what I’ve learned is that you just got to trust people, you know, if they’re a good friend, and they care then that’s all that matters really, and they’ll go away and they’ll deal with it in whatever way they think best. (Rachel)
Disclosure started pre-diagnosis
Many participants began the process of disclosure before receiving their formal diagnosis. Some sought out a diagnosis after discussing the possibility of autism with their loved ones:
I watched that documentary with my wife . . . watching that and then doing the AQ test online straight afterwards [giggle] um, and getting quite a high score. um you know, I was immediate – well yeah, you know, that that’s it, whereas my wife was was like, no way, no way you can be autistic, surely not, and and then um the more we talked about it and wow, ‘maybe maybe’. (Brandon)
For Olivia, involving a trusted loved one in conversations about a potential diagnosis and the diagnostic process had allowed their loved one to ‘adjust’, ‘accept’ and be more ‘supportive’ towards them and meant that disclosure of the formal diagnosis felt less of a shock.
Negative effects of preconceptions
Disbelief and imposter syndrome
Not being believed was a common experience and participants felt that this is likely fuelled by the perceived mismatch between other people’s expectation of what an autistic person is like and the how the participants present:
. . . the response is often ‘you don’t look autistic’, and its well what does looking autistic look like, or, you know, ‘you seem really well put together’, or people just disbelieving that I’m autistic because I’m fairly high functioning in my career . . . (Josh)
Participants found that people often associated autism to ‘bad news’ (Helen), whereas their strengths were not recognised. Olivia also experienced this in her workplace:
the implication for me from that, was that she (manager) saw autism as something that basically was a negative thing and it should be impacting my job, rather than thinking actually, it might be helping me to do the job I’m doing. (Olivia)
Participants attributed these assumptions to be influenced by popular media portrayals, myths and stereotypes of autistic people (e.g. ‘Rainman’ (Josh), ‘little boys who liked trains’ (Jess)) as well as overgeneralisation that autism is associated with being ‘low functioning’ (Jane) or involving ‘meltdowns’ (Olivia) with this knowledge being based on limited encounters with autistic people. Participants also thought that a lack of knowledge and education around autism contributed to people’s scepticism about their diagnosis. Some participants noticed that there was a generational divide in knowledge and education around autism, such that some people from the older generation tended to not know ‘what it is’ or ‘what to say’ (Helen). One participant, Josh, even had his disclosure viewed as making ‘excuses’ and that ‘everybody wants a label these days’. He felt that people’s lack of compassion towards him is influenced by the increasing incidence of self-identification and people’s perception that there is an element of social contagion to autism. Jane also had similar experiences with relatives who thought that she had received a diagnosis by reading up about autism and knowing what to say in front of assessors. In addition, she thought that her years of masking may have exacerbated scepticism from others:
she said, ‘if you feel that helps you then I’m happy for you, but I don’t think you’re autistic’ It was devalidating . . . I think what I’ve learned is, it’s not so much about me erm cause could be because being a woman, you mask a lot as well. (Jane)
For others, autistic traits have been so normalised within their family that their signs of autism had been overlooked, and this further contributed to discomfort around disclosure:
They didn’t really think that at seven years old wanting to watch [programme relating to special interest] was anything atypical particularly because I come from quite an academic family . . . (Jess)
Not being believed had a negative emotional impact on participants and triggered unhelpful thought processes in which some participants questioned the legitimacy of their diagnosis. This was particularly difficult at a time when they were newly diagnosed:
. . . and so at that time my conviction felt really fragile anyway, so other people questioning, it really didn’t help. It made me feel quite easily shaken and made me question like have I just gone down the wrong path, have I somehow like subliminally convinced the assessor that I am when I’m not. (Olivia)
These feelings of self-doubt had been described as ‘Imposter Syndrome’ (Liza) and the severity appeared to be affected by the timing of the disclosure and whether participants have come to terms with the idea of being autistic. Experiences prior to receiving a diagnosis also contributed to ‘Imposter Syndrome’. Helen talked about her experience of emotional abuse in childhood meant that she tends to question herself even though ‘autism makes sense’ logically. For Liza, the uncertainty around her diagnosis during the assessment process further played a role in her ‘Imposter Syndrome’:
. . . I think I was kind of like borderline . . . so the fact that she (psychologist) had to go and double-check, made me feel like, well it’s not clear, and I’m not like I’m not autistic enough . . . (Liza)
Not having my needs met
Participants felt that people’s assumptions and lack of understanding about autism meant that not only did disclosure not lead to the desired effect of having their needs met, but they were also either dismissed or discriminated against. For example, when Jess requested reasonable adjustments at university, she was told that
well everybody else manages so why do you need adjustment, if you need adjustment maybe you shouldn’t be here.
Other participants had similar experiences across a range of contexts including employment, healthcare and statutory services which were frustrating for them. Participants found that organisations often either had rigid rules around who to give support to or what type of support to give, and these were not set up to accommodate individual needs of autistic people across the spectrum. Tina found that social services did not seem to understand ‘neurodiversity can also be debilitating’ and were not able to offer her appropriate support due to autism not being a ‘physical disability’.
Even when adjustments were offered, participants felt that these were not always timely or did not fully meet their needs, or not managed appropriately due to the lack of knowledge and confidence. In Brandon’s case, he found that his manager was
‘sympathetic’ towards his disclosure, though ‘was worried about doing the wrong thing’ and even though adjustments were made, Brandon felt that it was a ‘knee-jerk response rather than a careful weighing’.
Furthermore, the constant need to remind others about their autism and adjustment needs could be exhausting as it served a constant reminder of their limitations:
I think cos it’s, because it’s relatively hidden . . . but I think people quickly forget that that’s the case and so its felt sometimes that I just needed to keep reminding people . . . it reminds me of the things that I, that I struggle with, that I’m aware that I’m, it’s just really difficult for me to do, erm and I think that’s what stirs up the negative feelings sometimes around it. (Michael)
Caution and avoidance
Negative experiences of disclosure impacted on participants’ subsequent engagement with services and disclosure behaviours. For example, Edward felt ‘reluctant to go back to the clinic again’ after getting ‘dysregulated’ by healthcare professionals not understanding his needs. Participants talked about weighing up the risks and benefits and choosing nondisclosure when perceived risks outweighed the benefits, or if change is not expected:
if I can’t see that there’s a difference, a change as a result of it then I suppose that’s the reason why I wouldn’t necessarily tell people. (Michael)
For some participants, nondisclosure became the default and many became more cautious about who they disclose to and what information, especially when negative reactions, discrimination and negative change in attitude were anticipated:
I think I’m to a degree guarded upon who I decide to disclose to . . . erm, especially in a, in a professional setting . . . I don’t want disclosure to hinder my progress or how people treat me at work . . . (Josh)
Some chose to use partial disclosure strategies as a form of self-protection, for example, only talking about the strengths that autism brings them in a job interview situation (Brandon), or only sharing what is required to get their needs met, rather than sharing full details of their autism diagnosis:
. . . I won’t say to them, ‘Oh yeah, I’m autistic’. I will say . . . I struggle sleeping . . . that sort of thing . . . especially when you think it might change people’s attitude or behaviour towards you. (Tina)
Openness, acceptance, and finding community
Participants often associated positive experiences with people who responded in a way that was open, curious, willing to listen or prepared to drop any preconceptions they have:
I remember her just being very much wanting to know how I was feeling rather than her jumping in and being like, ‘Oh that’s great’ or ‘Oh it’s terrible’. I think that was again maybe why it was such a positive experience because I felt like she was waiting to hear how I felt, and then was going to kind of take my lead on that erm rather than jumping to her own conclusions. Erm, so whether she had negative views about it or not, I never really knew because she just went with what I said if that makes sense. (Olivia)
In general, participants found that those who responded with a positive attitude to their disclosure tended to have progressive views, lived experiences or well-informed knowledge of neurodiversity or disabilities. This tended to be the norm within certain communities, such as neurodiverse families or workplaces that value neurodiversity and inclusivity. Many participants found that disclosure opened opportunities for them to connect with others, including autistic and non-autistic allies, as well as those considering their own neurodiversity, and felt celebrated:
I got another friend who’s brother and sister are autistic and he also looks and supports somebody else who’s autistic, and they’re both around. And I said, ‘Look, I’m autistic’ and the one that was autistic was like, ‘well, you know, you’ve just joined the most interesting club in the world. You’re gonna meet some amazing people. . . . So erm that that was really heartwarming erm to hear that. (Jane)
Some were able to find employment where their experiences of being autistic was valued, while others found opportunities to take part in community groups and events (e.g. autism dialogue sessions (Brandon)), where they were able talk openly about autism and share experiences with both autistic and neurotypical people. These experiences had a normalising effect on the autistic experience and brought participants sense of relief, belongingness, optimism and hope:
. . . knowing other people in real life that are all like, doing okay, they’ve got jobs that they are really happy with, that they’ve got partners that they are really happy with, and, I know them personally and they just seem like, nice decent, people like that stuff It’s really reassuring, and that’s the stuff that feels like kind of, destroys the stereotype the most for me. (Olivia)
Practically, others’ acceptance and openness not only meant that participants could work together with those they disclose to consider how they could be best supported:
So, yeah, my brother is really read up about it a lot and investigated, how he can support me and he’s discussed with me things like, say, he’s taking me to an event or a medical appointment or something, erm how best he can support me. So things like finding the quiet quiet place to be possible and probably sitting down and, and perhaps, erm I carry a [item associated with special interest] around with me now . . . that calmed me down greatly . . . And and it’s really greatly appreciated. (Tina)
Discussion
This study aimed to explore autistic adults’ experiences of diagnostic disclosure and non-disclosure. Disclosure served three particularly important functions for autistic people, including accessing support, to be more authentically themselves, and as a form of activism. Disclosing a diagnosis could be an anxiety-provoking experience and participants varied greatly in the support they received on disclosure. For many, the disclosure often began before a formal diagnosis was received. The decision regarding whether to disclose was experienced as a balancing act between honesty and considering the saving the feelings of those involved. Disclosure was reported as impacting those receiving the disclosure and had consequences. On occasion, participants experienced not being believed due to mismatches between themselves and people’s preconceptions of autism. This left participants on occasion feeling like ‘imposters’ and prevented them from having their needs met. Furthermore, these negative experiences led participants to become more cautious and avoidant on future disclosures and interactions. On the other hand, participants also described positive experiences when disclosure was met with openness, which led to a sense of acceptance and community.
We found that autistic people’s decisions to disclose were influenced by the hope of accessing support which is commensurate with previous research within the employment context and largely conducted outside of the United Kingdom (Huang et al., 2022; Lindsay et al., 2021). In addition, for the autistic adults in our study who received a diagnosis in adulthood and generally had low support needs, disclosure served an emotionally restorative function of allowing them to be more authentically themselves. Being their authentic self meant resisting the need to mask (Bradley et al., 2021) and in the long term this may be more beneficial for autistic people’s mental health and reduce burnout (Raymaker et al., 2020).
Activism is an additional function of disclosure that this study has identified. Analyses of autobiographies of autistic people have drawn parallels between autism disclosure and disclosure in other minoritised groups, which act as a form of resistance against oppression (Davidson & Henderson, 2010) and challenges the power imbalance in institutions maintained by discriminatory policies and processes that encourages ‘collective closeting’, the act of concealing differences by a group of people who shares particular social characteristics (McDonald et al., 2020). However, we also found that the moral obligation to undertake such work can be exhausting for autistic people due to the need to repeatedly disclose. Furthermore, it could feel like autistic people are taking disproportionate amount of the burden for this work, much like people from ethnic minoritised groups, who are often expected to take on responsibility for equality, diversity and inclusion work (Van Laer & Janssens, 2011).
Our study found that support for disclosure varied widely across participants. This disparity is not surprising considering the lack of detailed guidance for post-diagnostic support in the United Kingdom (Beresford et al., 2020; NICE, 2012). Our findings are consistent with a recent systematic review with mapping of UK services, which showed while post-diagnostic is available in most localities, the extent of support can be minimal and difficult to access due to underfunding and pressures on services, which aligns with provisions internationally (Norris et al., 2024). Within our study, there was a consensus of being able to hear about others’ experiences of disclosure or having the space to talk through their own decisions and reactions in relation to disclosure were helpful. Recent qualitative research using autistic-led post-diagnostic psychoeducation programme (Crane et al., 2021) had also found preliminary support these interventions.
While this study was designed to understand disclosure after receiving an autism diagnosis, many autistic people said that they had discussed a potential diagnosis with loved before their official diagnosis was received. Involving trusted loved ones in discussions about a possible diagnosis meant that loved ones were able to support autistic people throughout the diagnostic process and may allow loved ones to begin to come to terms with the diagnosis at an earlier stage. For loved ones on the receiving end of disclosure, unexpectedness of the news could be challenging emotionally and may trigger a range of feelings associated with adjustment to grief and loss (Kubler-Ross, 1969). Feelings such as shock, denial and guilt had been documented in the parents’ accounts of receiving the news of their children’s autism diagnosis (Fernańdez-Alcántara et al., 2016). However, resolution through acceptance, positive changes in family dynamics and effort were also evident in parents’ account. Likewise, loved ones’ ability to adapt to disclosure of an adult autism diagnosis through time and ongoing conversations were also featured in autistic adults’ accounts in this study.
Intersectionality refers to how the positioning in different social divisions, such as age, gender, disability and race, interacts to affect people’s lives (Harris & White, 2018). Intersectional theory of ‘Closeting’ (McDonald et al., 2020) stipulates that revealing a difference in social identity can have both negative and positive impacts. Our study found that misconceptions of autism contributed to negative experiences of disclosure. These preconceptions may have been formed due to exposure to the media portrayal of autism, limited interactions with autistic people, as well as a lack of understanding about autism. In line with previous research (Huang et al., 2022), mismatch between people’s expectations of what autism should look like and how the autistic person presents meant that not being believed was a common experience.
Experiences of not being believed may be particularly disrupting for newly diagnosed autistic people who are going through their own process of adjustment, contributing to a sense of ‘Imposter Syndrome’. A recent study by Harmens et al. (2022) also documented ‘Imposter Syndrome’ in blog posts written by autistic women. Having to explain to others why they do not fit stereotypes can be exhausting for autistic people. ‘Imposter Syndrome’ might be more common in females and those with late diagnosis given male bias in autism diagnosis and the use of camouflaging strategies (Bradley et al., 2021; Cruz et al., 2025). Our findings contribute to existing intersectional theory that discrimination could occur when multiple forms of differences intersect with each other and autism can be considered as one of these differences. In the case of autism disclosure, being female and appearing ‘able’ seemed to exacerbate negative responses to disclosure.
An objective of this study is also to understand the context around nondisclosure. Intersectionality theory suggests a link between closeting of ‘invisible, non-normative, and stigmatised’ (p. 87) differences and oppression, and indeed, this study found that many autistic participants chose not to disclose because they wanted to avoid negative reactions and discrimination, which they were able to predict based on experience. Not having a disclosure taken seriously could become a barrier to autistic people getting their needs met. We found that negative experiences of disclosure deterred autistic people from making further disclosures or from engaging with services, concurring with previous findings on nondisclosure (Dugdale et al., 2021; Huang et al., 2022). Expectation of potential discrimination also meant that autistic people take caution in disclosing and may use alternative strategies, such as only discussing strengths of autism or only sharing information about difficulties rather than the full diagnosis.
Promisingly, positive experiences of acceptance and understanding from others featured in participant’s accounts in this study, and for some, these were the norm rather than the exception. This might be a result of the increasing public awareness of autism (Dillenburger et al., 2013) and increasing number of people diagnosed in adulthood (Lai & Baron-Cohen, 2015). Within the UK context, this is also likely to be influenced, at least to a certain extent, by the instatement of the Autism Act, UK (2009) and the national strategy to increase public awareness of autism (UK Government, 2021). This study also found that disclosure is experienced as bringing opportunity to build connections. Community connectedness and perceived positivity of autism identity had previously been suggested to be linked to increased self-esteem and improved mental health in autistic people (Botha et al., 2022; Cooper et al., 2017).
Strengths and limitations
This study benefitted from consultation with autistic adults, reflexivity, audit and adherence to good practice recommendations for qualitative research. However, while an effort was made to select a homogeneous sample, there were some factors that could have contributed to heterogeneity, including gender, time elapsed since receiving the diagnosis, service type at which diagnosis was received and co-occurring neuro-developmental conditions. Socio-economic status information was not collected. The ethic group of the sample was predominantly White British, and for all these reasons the findings may not be generalisable. It is unclear how the intersection of different characteristics, other than gender and ability, influenced disclosure. Future studies could more explicitly investigate other characteristics, such as ethnicity and dual diagnosis in relation to diagnostic disclosure. It is also acknowledged that our interview methodology may have excluded those who exclusively use alternative forms of communications.
Clinical implications
On a service level, discussions around disclosure should be incorporated into routine follow-up appointments for newly diagnosed autistic adults. Services should consider providing different format of post-diagnostic support, for example, either in groups or one-to-one to suit individual needs. Given the benefits of connecting with other autistic people and sharing of lived experiences disclosure could bring for newly diagnosed autistic people, services should consider developing roles for autistic people to lead and deliver post-diagnostic intervention, in the form of one-to-one peer support and support groups. At the same time, it will be important for service managers and supervisors to consider the impact of partaking in the delivery of these interventions for autistic employees, and to discuss these within line management and supervision, to ensure that autistic people’s privacy and work–life balance is protected.
Ongoing support sessions over a period post-diagnosis could be helpful for autistic people to start considering disclosure within different context, such as within personal relationships (family, friends, romantic relationships, etc.), work or education settings, health and social care, or other daily encounters. It may be helpful for clinicians and autistic people to discuss who they feel safe to disclose to, the depth of information required to be shared (e.g. a full disclosure of the diagnosis and its impact, or a partial disclosure) and different methods of disclosing, either verbally or through written communication. It would also be important for clinicians to consider how other differences and intersections of identity that an autistic person possesses, as well as the extent of stigma within autistic person’s systems, could impact on the disclosure experiences and the autistic person’s mental health, given that external source of autism acceptance had been negatively predicted mental health outcomes, including depression and stress (Cage et al., 2018). It is important to be aware that disclosure could trigger different reactions and emotional experiences for the autistic person and those around them; therefore, clinicians may wish to consider with autistic people how to manage these situations.
Conclusion
Whether autistic adults disclose their diagnosis is a context-dependent decision and is complex and challenging for autistic people to navigate. Disclosure can bring a sense of connection and being understood for autistic people. For some it may also represent an important act of self-acceptance and activism, though this can present a personal burden. Diagnostic disclosure may also open opportunities for autistic people to access much needed support. However, other people’s preconceptions of autism can lead to negative consequences, such as discrimination, that create barriers for autistic people to have their needs met and discourages further disclosure. Given the potential risks and benefit of disclosure, it is important that clinicians incorporate discussions about disclosure, including insights from experiences of others and consideration of potential consequences, as part of post-diagnostic support for autistic people.
Supplemental Material
sj-docx-1-aut-10.1177_13623613251337504 – Supplemental material for ‘Am I gonna regret this?’: The experiences of diagnostic disclosure in autistic adults
Supplemental material, sj-docx-1-aut-10.1177_13623613251337504 for ‘Am I gonna regret this?’: The experiences of diagnostic disclosure in autistic adults by Sheena K Au-Yeung, Megan Freeth and Andrew R Thompson in Autism
Footnotes
Author contributions
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.