
Abstract
Difficulties regulating emotions have been coined as inherent to autism, possibly even presenting a core difficulty of autism. While several models of emotion regulation have been proposed in the past, in this targeted review article, we aim to map emotion regulation difficulties in autistic individuals within the framework of the extended process model of emotion regulation. This model can be considered the most comprehensive one currently incorporating not only different emotion regulation strategy groups but also different stages and processes involved in successful self-focused emotion regulation. Within this model, we will identify areas and domains as specifically impacted by autistic individuals. We will also outline gaps in the literature and provide suggestions for future research that can help deepen our understanding of the emotion regulation processes of autistic individuals. The ultimate goal is to develop specific support programs that address specific emotion regulation mechanisms, providing a much more individualized support approach.
Lay abstract
We know that many autistic children, youth, and adults experience difficulties regulating emotions. Existing research has focused mainly on the differences in emotion regulation capabilities between autistic and non-autistic individuals, the relationships between autistic traits and emotion regulation, and how emotion regulation relates to other outcomes, such as social skills and mental health.
We want to take a new approach to review the existing emotion regulation research through the lens of a specific theoretical model: the extended process model of emotion regulation. Professor James Gross developed this model. It consists of four emotion regulation phases: identification, selection, implementation, and monitoring.
Our review revealed specific areas within these emotion regulation phases that could significantly impact the emotion regulation experiences of autistic individuals. We also outline the gaps in the research and propose avenues for future investigation.
By deepening our understanding of emotion regulation in autistic individuals through the proposed future research, researchers and clinicians can pave the way for the development of tailored support programs. These programs will directly target specific emotion regulation mechanisms, offering a much-needed individualized support approach.
Recent estimates suggest that approximately 15-20% of people worldwide are neurodivergent (Doyle, 2020). Autism is a neurodivergence characterized by differences across various domains, including communication, routine needs, repetitive behaviors, sensory processing, interests, and sociality. Although these are the core characterizations of autism, everyone on the spectrum is unique and different. Apart from the heterogeneity in these core characterizations, autistic individuals experience high variability in cognitive and emotion processing, everyday functioning, academic and employment outcomes, and support requirements (Hedley et al., 2017; Keen et al., 2016; Norbury & Nation, 2011; Tillmann et al., 2019). In addition, research has consistently found that a considerable proportion of autistic individuals experience significant mental health symptoms (Lai et al., 2019; Vasa et al., 2020), and more autistic individuals are diagnosed with anxiety and depression than non-autistic people (Hollocks et al., 2019). This increased occurrence of mental health issues in autistic children and adults has been attributed to difficulties with emotion regulation (ER) that are frequently observed in autistic individuals (Cai et al., 2018; Weiss et al., 2014; White et al., 2014).
According to the extended process model of ER, self-focused ER is a complex, cyclic process that includes identifying one’s own emotions, selecting and implementing strategies to regulate emotions, and monitoring the outcomes of this regulation process (Gross, 2015, 2023; Petrova & Gross, 2024). It allows us to change the intensity, duration, and types of emotions experienced (Thompson, 1991) and modify one or multiple components of emotions, such as emotional experience, psychophysiological constituents, bodily and outward expressions, and thoughts (appraisals) associated with an emotion. For instance, when we notice the physical sensations (heat rising in our bodies) and thoughts associated with anger in ourselves (blaming thoughts), we may first acknowledge that we feel anger and then try to reduce the intensity of this emotion by focusing on our breaths and practicing deep breathing. The outcome of the regulation process may be reductions in the intensity and duration of the anger. ER processes can occur either deliberately through conscious effort (previous example) or automatically without conscious awareness of one’s emotions or goal to regulate emotions (Gyurak et al., 2011). In infancy, we depend on caregivers to help us regulate emotions (see Riediger & Bellingtier, 2022), also coined as other-focused ER (see Petrova & Gross, 2024). As we grow and enter preschool, we rely less on caregivers and more on ourselves (Grolnick et al., 1996). Although the development of the regulatory systems increases and our ability to regulate emotions improves throughout childhood, a maladaptive shift may occur during adolescence (Cracco et al., 2017).
While the occurrence of mental health conditions in autistic people is often associated with ER difficulties, it is inappropriate to generalize these findings to all autistic individuals. Indeed, there is evidence indicating that a minority of autistic individuals exhibit adaptive ER capabilities (e.g., Cai et al., 2019). Nevertheless, we can conclude that as a group, autistic children and adults regulate their emotions less frequently and tend to use more maladaptive regulation strategies and less adaptive strategies than non-autistic people (e.g., Bruggink et al., 2016; Cibralic et al., 2019; Samson, Hardan, et al., 2015). Differences in neurobiology may explain the high frequency of ER difficulties often observed in and reported by autistic individuals. For example, there is lower structural connectivity between frontal regions and the lower limbic brain in autistic individuals (Samson et al., 2016), and when asked to down-regulation negative emotions, autistic individuals show a decreased engagement of prefrontal regions and less amygdala down-regulation (Pitskel et al., 2014; Richey et al., 2015).
Existing research on ER in autism has focused primarily on the differences in ER capabilities between autistic and non-autistic individuals (e.g., Mazefsky & White, 2014; Nuske et al., 2017; Rieffe et al., 2014; Samson, Wells, et al., 2015), the relationships between autistic traits and ER (e.g., Berkovits et al., 2017; Samson et al., 2014), the associations of ER with other outcomes such as social skills, mental health outcomes, and challenging behaviors (e.g., Berkovits et al., 2017; Cai et al., 2019; Conner et al., 2020; Goldsmith & Kelley, 2018; Jahromi et al., 2012), and more recently, factors that impact ER (e.g., Fenning et al., 2018; Greenlee et al., 2021). These empirical studies predominantly addressed two of the three theoretical models of ER (see an overview of models in Naragon-Gainey et al., 2017): ability-based and strategy-based models. Ability-based models focus on the dispositional factors that facilitate ER, while strategy-based models concentrate on specific ER strategies. Most of the existing studies have not explicitly examined autistic people’s ER through the lens of the temporal process models, which focus on the temporal unfolding of emotion and ER across various stages (for instance, a research question may be how do autistic adults identify the ER strategy most suitable for a stressful situation?). One of the most referenced models of ER in the Introduction sections of empirical papers is the extended process model (Gross, 2015, 2024; Petrova & Gross, 2024), which also happens to be a temporal process model.
We suggest it would be timely now to present the ER in autism literature through the lens of the extended process model, as initially and partly presented in the book chapter by Cai and Samson (2024). We anticipate that this novel approach to reviewing the literature will allow us to characterize ER in autism further and discover unique gaps in existing research. This not only helps researchers but also clinicians motivated to support ER in autistic individuals. Therefore, the current article aims to (1) connect existing autism literature to the extended model of ER (Gross, 2015, 2023), which postulates four ER phases (identification, selection, implementation, and monitoring), and (2) identify specific points in the ER process where issues may arise for those on the spectrum. As part of this review, we will discuss several factors that may contribute to the ER difficulties observed in autistic individuals, such as alexithymia, alterations in executive functioning, insistence on sameness, and cognitive inflexibility, which may differentially impact different phases and processes related to ER.
The process model of ER
In the extended model of ER, Gross (2015) described several stages and processes involved in ER. The identification phase first involves the perception of one’s own current or anticipated emotional state. This current state may not correspond to a desired state. It may, therefore, lead to a cascade of processes involved in ER, such as setting an ER goal and selecting and implementing one or more ER strategies combined or in sequence. Each stage can be broken down into cyclic subprocesses of perception, valuation, and action, which will be discussed in more detail below. Once a strategy has been implemented, it is followed by a monitoring stage, which allows one to observe the efficacy of a strategy—one may decide to stop using a strategy, continue implementing it, or switch to other strategies. To provide examples that may occur typically in autistic individuals: Noticing that one feels irritated about unprecedented changes and going to unfamiliar places may lead to setting an ER goal to feel less negative. To feel less irritated, one may decide not to go to an unfamiliar place (avoidance). Monitoring the efficacy of this strategy may reveal its success since negative emotions may have decreased due to the use of the avoidance strategy. In this case, there is no need to switch to other strategies (while this strategy may seem successful in the moment, there is evidence that avoidance strategy use may lead to increased anxiety or maintaining specific anxieties due to non-exposure; Ball & Gunaydin, 2022).
One can think of a myriad of ER strategies to change or maintain emotional states or their expressions, which can be categorized into five families of strategies in relation to different stages of how an emotion evolves (i.e. strategies tapping into situation selection, situation modification, attentional deployment, cognitive change, and response modulation) but can also be characterized based on their longer-term consequences on mental health (i.e. on a continuum from adaptive to maladaptive strategies). Cognitive reappraisal, a strategy that involves reframing an emotional situation’s meaning, is a particularly adaptive strategy. In contrast, expressive suppression, which involves suppressing the outward expression of emotions, is an example of a maladaptive strategy in the long term when used on a habitual basis (Gross, 2015).
Self-focused ER in autistic individuals via the process model
Identification stage
Breakdowns in the identification stage of the ER cycle may contribute to the challenges autistic individuals face in managing their emotions. Becoming aware of or identifying one’s emotions is the initial step in this stage. Researchers have utilized alexithymia to examine autistic people’s capacity to recognize, differentiate, and articulate their emotions. A systematic review and meta-analysis found that a higher proportion of autistic people have alexithymia than non-autistic people (50% vs. 5%; Kinnaird et al., 2019). It has been proposed that alexithymia plays a role in the emotional impairments observed in autism and hampers individuals’ ability to effectively regulate difficult emotions (Bird & Cook, 2013). Supporting this notion, a recent empirical study discovered a moderate association between alexithymia and emotion dysregulation in autistic youths (Gormley et al., 2022). One of the early studies on ER in autistic adults was able to show that autistic individuals still had more ER difficulties than non-autistic individuals, even if alexithymia was controlled for (Samson et al., 2012). Since around half of autistic people do not have alexithymia, we conclude that alexithymia is not universally present in all autistic people. Therefore, alexithymia may not be the only candidate to explain ER difficulties in autism, but other impairments exist that contribute to the difficulties in ER processes.
The identification process not only includes detecting or identifying a current emotional state but also involves appraising emotion. Specific appraisals of an emotion may influence how and if we attempt to regulate an emotion. Autistic individuals seem to appraise fear and anxiety, for example, differently than non-autistic children (Sharma et al., 2014). Fear and anxiety were rated higher by autistic children on self-accountability, lower on coping potential, and lower on future expectancy, which corresponded to a pattern of elevated experience of fear and anxiety. Such early misattribution patterns can likely lead to later maladaptive ER (see also Walle & Özden, 2024).
In addition to breakdowns in the initial step of detecting one’s own emotions, ER difficulties can also emerge during later processes of the identification stage. These later processes involve our beliefs about emotions. Ford and Gross (2019) suggest that individuals’ perceptions and beliefs about emotions, specifically whether emotions are perceived as good or bad (goodness of emotions) and controllable or uncontrollable, play a significant role in ER. They hypothesized that believing an emotion to be “bad” increases the likelihood that the emotion is identified as needing regulation. For many people, our natural inclination is to seek positive emotions and avoid negative emotions (Barrett, 1996; Larsen, 2000; Rusting & Larsen, 1995), therefore identifying positive emotions as good and negative ones as bad. This intrinsic motivation leads us to approach stimuli that make us feel good and avoid those that make us feel bad. As a result, we engage in the down-regulation of negative emotions to reduce the intensity or frequency, and we readily accept and embrace our positive emotions, as highlighted by Gross et al. (2006). However, it has been found that a higher proportion of autistic adults actively down-regulate positive emotions in everyday life than non-autistic adults (Cai et al., 2020). One possible explanation for this observation is that some autistic people may find any emotion, including positive ones, too overwhelming and unpleasant, leading them to label all emotions as bad. In the general population, believing that emotions are bad predicts lower well-being and greater depressive and anxiety symptoms (Ford et al., 2018; Karnaze & Levine, 2018).
Finally, Gross (2015) suggested another way that ER difficulties could occur at the identification stage is via psychological inertia—the tendency to continue acting as one has previously. Emotional inertia, defined as resistance to change emotionally (Kuppens et al., 2010), could be even more relevant. People with high emotional inertia have emotional states likely to persist from one moment to the next. High emotional inertia in both positive and negative emotions has been shown to predict internalizing symptoms in adolescents and adults (Koval & Kuppens, 2024; Kuppens et al., 2010). Recently, autistic individuals have begun to use the term autistic inertia to describe their difficulty in acting on their intentions, with potential causes being motor difficulties, poor mental health, and executive functioning impairments (Buckle et al., 2021). Although no research has been conducted on emotional inertia in autism, some autistic people likely experience high emotional inertia. We know that, as a group, autistic individuals experience more executive functioning impairments and higher levels of insistence on sameness than non-autistic people (Demetriou et al., 2018; Eisenberg et al., 2015). We suggest that these executive functioning impairments, coupled with high levels of insistence on sameness and specific beliefs about emotions (uncontrollability, for example), are likely to lead autistic people to be stuck in psychological inertia and not activate goals to regulate emotions.
To summarize, problems in the identification stage of the ER process may result in the regulation difficulties observed in some autistic people. There is mounting evidence for alexithymia in autism and alexithymia impacting effective ER. Other aspects within the identification stage need further exploration, such as autistic people’s beliefs about the goodness of emotions (devaluing positive emotions), the controllability of emotions, and the role of psychological inertia.
Selection stage
After setting a goal to attenuate, increase, or maintain one’s emotional state, one needs to access mental representations of ER strategies to select one or multiple. This mental representation can vary in breadth and depth, influenced by factors such as developmental stage and past experiences. Studies have indicated that the repertoire of ER strategies expands as individuals transition from childhood to adolescence and adulthood, progressing from primarily behavioral strategies to more cognitive strategies (Riediger & Bellingtier, 2022). However, research has also shown that autistic children tend to employ less sophisticated ER strategies compared to their typically developing peers, indicating a delay in ER development (Nuske et al., 2017). In addition, a systematic review suggests that autistic individuals may possess a different repertoire of ER strategies, including more maladaptive ones (Cibralic et al., 2019). Preliminary evidence suggests that there may not be a difference between autistic and non-autistic individuals in terms of the number of strategies employed for each regulation moment (Cai et al., 2020). Therefore, the issue may lie not in the quantity of strategies utilized but rather in the types of strategies selected. In line with this hypothesis, multiple studies have demonstrated that autistic children and adults utilize cognitive reappraisal less frequently compared to non-autistic individuals (Samson, Hardan, et al., 2015; Samson, Wells, et al., 2015).
One reason that many autistic people tend to utilize less cognitively taxing strategies, such as cognitive reappraisal, may be due to the combination of anxiety and executive function difficulties often observed in this population. South and Rodgers (2017) proposed in their anxiety model that alexithymia and differences in sensory processing, along with other co-occurring factors related to autism, such as rigidity of thought and intolerance of uncertainty, may result in increased arousal and anxiety in autistic individuals. Research in non-autistic samples indicates that cognitive reappraisal is less effective at modifying the experiences of negative emotions in intensely emotional situations (Sheppes & Meiran, 2007; Sheppes, 2023), and people are less likely to select reappraisal in these types of situations (Sheppes et al., 2014). For many autistic children and adults, these highly intense emotional situations occur quite frequently in daily life due to the reasons proposed by South and Rodgers (2017). Similar to the findings of the general population by Sheppes and colleagues, it may not be adaptive to choose cognitive taxing strategies like cognitive reappraisal. In addition, problems with executive function in autistic people may also lead them to use less cognitively taxing strategies. A meta-analysis of executive function found that autistic people performed, on average, significantly worse on executive function than non-autistic ones. Executive function subdomains (working memory, response inhibition, planning, fluency, mental flexibility, and concept formation) were not differentially impaired in autism—they were all impaired with moderate effect sizes (Demetriou et al., 2018). Cognitive reappraisal is associated with better working memory and attention shifting in the general population (McRae et al., 2012). The mixture of higher arousal and lower executive function may together contribute to autistic people’s tendency to prefer less cognitively demanding ER strategies, such as avoidance or distraction, which historically is deemed maladaptive in the general population. Finally, it is also possible that some autistic individuals may have difficulties changing their perspectives (needed for cognitive reappraisal), which often involves reinterpreting a situation in a different light (Samson et al., 2012).
The adaptiveness of specific strategies is often defined based on their long-term mental health effects. However, whether the appropriateness and efficacy of strategies are the same for people with and without autism is still an open question. While avoidance is generally considered a maladaptive strategy, initial evidence suggests that it may be adaptive for autistic children (Rieffe et al., 2014). ER strategies categorized under situation selection, such as avoidance, can be particularly effective for individuals who struggle with utilizing other types of strategies (Webb et al., 2018). Another example is the presence of restrictive and repetitive behaviors, specifically insistence on sameness, which are diagnostic criteria for autism. However, it is worth noting that such behaviors are also commonly observed in typically developing young children, and these behaviors serve as strategies to manage fears and anxiety (Evans et al., 1997). Interestingly, autistic adolescents and adults also appear to utilize repetitive behaviors as a means to regulate their emotions (Samson et al., 2022; Samson, Wells, et al., 2015). This may suggest that these strategies may be essential and potentially adaptive for autistic individuals, particularly when other, more cognitively demanding strategies are less accessible due to the factors associated with autism (as described above). These examples highlight the importance of considering individual differences when evaluating the effectiveness and adaptiveness of ER strategies in autistic individuals. While certain strategies may be considered maladaptive, they may serve a beneficial purpose for individuals with specific cognitive, sensory, and emotional profiles. Recognizing the potential adaptive functions of these strategies can inform interventions and support approaches that acknowledge and leverage the unique ER needs of autistic people. However, since a recent article showed that a tendency toward behavioral repetition could contribute to repetitive negative thinking, which was linked to mental health problems (Cooper & Russell, 2024), we think that more research is needed to fully understand the links between repetitive behaviors, ER, and mental health outcomes.
To summarize, there is increasing evidence that autistic people use less cognitively taxing strategies and tend to use more behavioral approaches, including avoidance or repetitive behaviors that are typically considered more maladaptive in the long run—however, more research is needed to determine to which extent autistic people may benefit from such strategies in the short and long run. Differences in the ER repertoire might also be linked to less efficacy of cognitive ER strategies due to elevated arousal in autism.
Implementation stage
In the previous section, we discussed the possible reasons for selecting fewer cognitively taxing strategies by autistic people. Another possible reason is difficulties with implementing strategies, i.e. translating strategies into tactics—however, due to the limited research on ER tactics in both autistic and other populations (see also Petrova & Gross, 2024), it is currently difficult to ascertain whether autistic individuals face challenges in the implementation stage of ER. Although autistic people tend to utilize cognitive reappraisal less frequently spontaneously, even a brief introduction with practice opportunities has shown significant improvements in the use of reappraisal in the laboratory setting (Samson, Hardan, et al., 2015), indicating that intervention programs focusing on the selection and implementation of adaptive strategies could be advantageous for autistic people (see, e.g., Zaharia et al., 2021).
Certain studies indicate that autistic individuals may employ cognitive reappraisal differently, potentially utilizing alternative tactics associated with different neural pathways. Richey et al. (2015) examined the neural correlates of instructed cognitive reappraisal, and no differences in subjective ratings of reappraisal efficacy were found between the autistic and non-autistic groups. However, distinct variations were observed in the brain activation patterns during regulation, including reduced activation in the dorsolateral prefrontal cortex among the autistic group. These findings suggest that autistic individuals may achieve effective ER despite employing alternative functional brain mechanisms. It is important to note that in research settings, the use of instructed reappraisal may be more effective than when used in real-life settings during high arousal moments. In addition to Richey et al.’s work on differing neural correlates in autistic people during reappraisal, Pitskel et al. (2014) demonstrated weaker functional connectivity between the prefrontal cortex and the amygdala, which aligns with previous findings of compromised structural prefrontal-amygdala connectivity associated with ER difficulties in autistic individuals (Samson et al., 2016).
In summary, autistic individuals can employ advanced strategies like instructed cognitive reappraisal in laboratory settings, albeit through alternative functional brain mechanisms. However, as discussed earlier, they tend to utilize these cognitively demanding strategies less frequently in spontaneous situations. Therefore, further exploration is warranted to understand how to effectively assist autistic people in utilizing strategies during stressful moments or, in other words, how to translate ER strategies into tactics. For instance, exploring alternative approaches such as other-focused ER or intervention programs targeting factors that support ER, such as self-compassion (see Cai et al., 2024), may prove beneficial in supporting autistic people in regulating their emotions.
Monitoring stage
Finally, after going through the earlier stages of the ER process, we need to monitor ER efficacy to maintain, change, or stop regulation efforts (Gross, 2015). Like the implementation phase, there is a scarcity of research examining the monitoring phase of ER. We propose that autistic individuals may encounter challenges in the monitoring stage of ER due to at least two potential mechanisms: alexithymia and psychological inflexibility/rigidity. To successfully monitor one’s emotions, we need to be able to assess the efficacy of our chosen ER strategies by detecting changes in our emotions. For those autistic individuals who experience difficulties with emotional awareness, it becomes challenging to identify subtle shifts in their emotional states. Reduced interoceptive ability, which involves being aware of the body’s perception of its internal states, has been hypothesized to serve as a pathophysiologic basis of alexithymia by non-autism-researchers (Brewer et al., 2016; Murphy, Brewer, et al., 2018; Murphy, Catmur, & Bird, 2018; Trevisan et al., 2019). This same pattern of relationship has been identified in autistic individuals (Butera et al., 2023; Ben Hassen et al., 2023; Mul et al., 2018). There is also preliminary evidence that alexithymia mediates the relationship between interoceptive sensitivity and ER abilities in autistic adults (Zdankiewicz-Ścigała et al., 2021). It would be challenging to empirically study the mechanism of alexithymia in the monitoring phase of ER via self-reported surveys and in naturalistic settings (using experience sampling methodology) because it may be difficult to untangle the role of alexithymia in the monitoring phase from its role on the identification phase. A more realistic approach to study this mechanism may be to conduct an experiment where after an unpleasant emotion is elicited from participants, they asked to report their bodily and emotional states, and are taught to emotionally regulate using an effective strategy. Then, participants are asked to report changes in their bodily sensations and emotional states. Individuals who did not notice alternations in bodily sensation or emotional states are likely to be less emotionally aware than individuals who noticed reduced emotional intensity and bodily discomfort.
The executive function issues we have previously discussed may also lead to psychological rigidity/inflexibility and insistence on sameness in autistic people, which potentially impacts the monitoring stage. An illustration of a situation would be when an individual has a behavioral habit that usually elicits an unwanted, unpleasant emotion and is able to successfully regulate their emotion (and acknowledge their regulation successes). However, due to their insistence on behaving in the same manner, they are unable to break their habit and repeatedly feel unpleasant emotions. Therefore, although the single instances of ER were successful, over time across multiple instances, regulation efforts were not successful. Similar to alexithymia, empirically studying the mechanisms of psychological rigidity/inflexibility and insistence on sameness on the monitoring phase is a challenging task. One idea would be to explore the behavioral addiction literature to see if research methodologies could be creatively adapted to be used in this context.
We hypothesize that the combination of alexithymia and psychological rigidity would strongly influence the monitoring stage of ER in autistic people; however, more research is needed in this area. By gaining a deeper understanding of the mechanisms that impact the monitoring stage, we can enhance our knowledge of the specific challenges faced by autistic people.
Discussion
In this article, we provided an overview of the current knowledge on ER in autism and mapped it onto the extended process model of ER (Gross, 2015). This framework enabled us to highlight potential challenges in emotional regulation across the stages of identification, selection, implementation, and monitoring (see Figure 1).
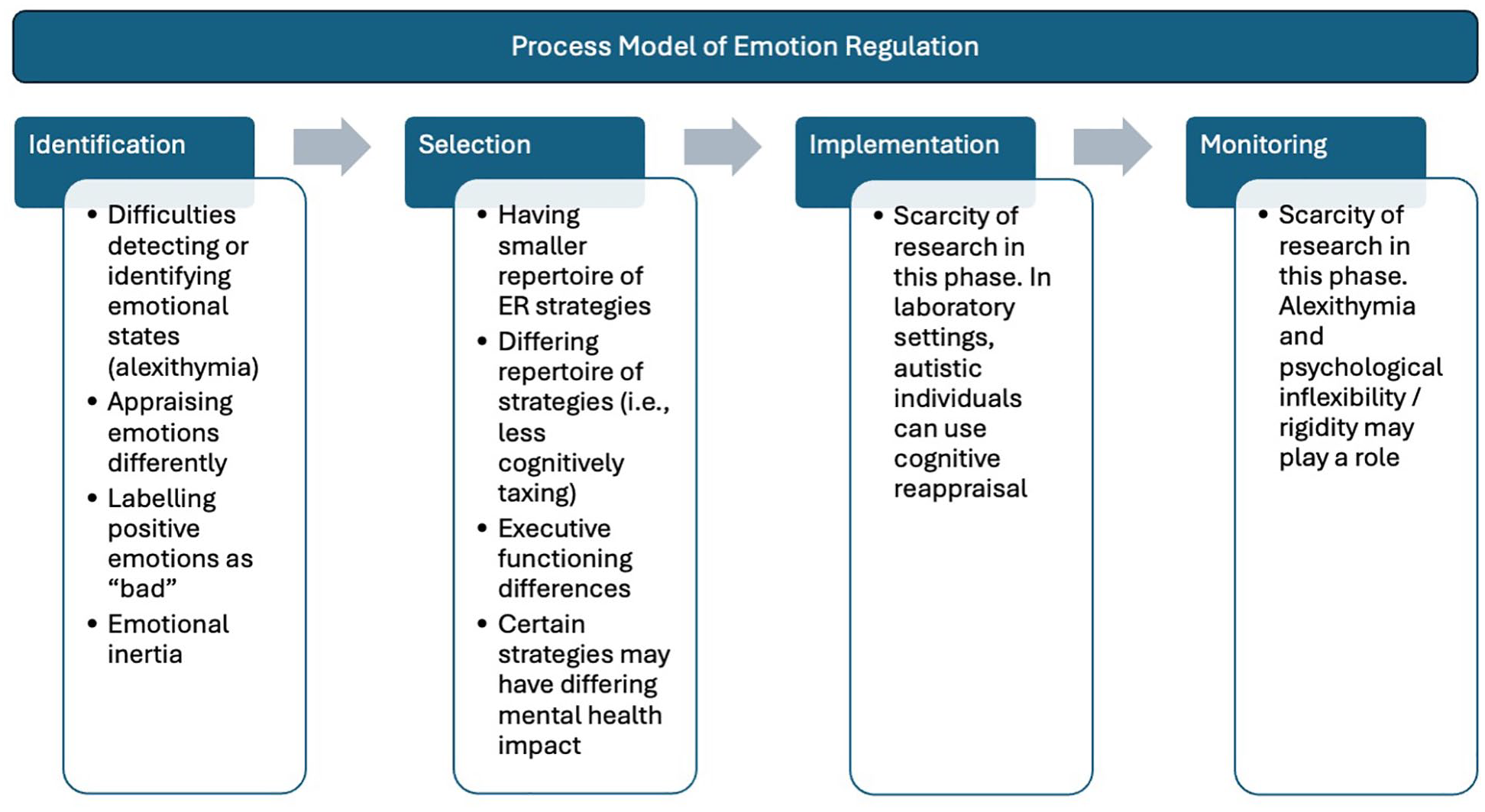
Possible ER challenges within the process model experienced by autistic individuals.
While we possess a more solid understanding of difficulties in the identification stage and some understanding of the selection phase, there remains a gap in our knowledge regarding the latter two phases. Drawing from the growing body of literature, it appears that autistic individuals show a different pattern of ER strategy use. However, it seems less clear at which stage of the ER process differences emerge. Linked to lower emotional awareness, it may be that ER strategies are less clearly mentally represented or that less knowledge and understanding about emotions exist, causing some autistic individuals to experience difficulties selecting suitable ER strategies. It may also be the case that despite knowledge and understanding of ER strategies, some autistic individuals may have difficulties predominately in the implementation phase. We have attempted to hypothesize points in the ER process where challenges may occur for autistic individuals based on existing studies; however, some of the challenges may relate to more than one stage of the ER process (e.g., both identification and selection).
We make a call to action—it is crucial and timely to implement paradigms in future research that discern the challenges that may occur at specific stages of the ER process in autism. One way to study temporal-based models is to adopt naturalistic paradigms, such as ecological momentary assessment studies, which have been coined as suitable for studying the different phases of ER (see Bettis et al., 2022). This will allow us to unravel the challenges that may be encountered by autistic individuals in the ER cycle, distinguishing between those occurring in the initial ER phases versus later stages. Having this understanding may help us identify the mechanisms that could influence various stages of the ER process and comprehend how issues in the early stages can affect the subsequent ones. Another way to examine the different stages of the ER process is by running experiments in laboratory settings to study individual phases of the ER process, such as the ER choice and implementation paradigms (see examples Milyavsky et al., 2019; Sheppes et al., 2011). A potential reason why the ER in autism literature has predominantly relied on ability- and strategy-based models is that these models are more straightforward to study. In contrast, methods used to examine the temporal-based models (such as experimental paradigms) are much more time-consuming and complex. Further, given earlier phases influence later phases, it is much more difficult to identify later phase issues and correctly attribute them, given the possibility of earlier phase breakdowns.
More advanced paradigms implemented in real-world contexts may be required to achieve this goal. For example, incorporating wearable sensing technology to monitor ER success or even acoustic and language analysis (see Bettis et al., 2022). Recent developments in software algorithms and computational methods for capturing and analyzing acoustic data could significantly contribute to our understanding and evaluation of ER processes. For example, Shih et al. (2016) showed that acoustic analysis can identify diaphragmatic breathing patterns as an index of deep breathing as an ER strategy. Moreover, acoustic analysis may also detect other commonly employed ER strategies with specific acoustic features (e.g., exercise, playing, or listening to music). Insights from such research may help to improve interventions for autistic individuals. Ideally, such interventions are individualized to consider the range of abilities and differences in sensory, cognitive, social, and emotional domains.
Given the far-reaching impact of ER, including mental health outcomes, effective interventions and supports can ultimately improve the quality of life of autistic people across the lifespan. Nevertheless, given that a mechanistic understanding of ER is critical for developing effective and individually tailored treatment options, it is important to continue to study ER to transition from group-based support to providing more optimized individual interventions. More specifically, it is essential to determine which phases of self-focused ER should be focused on by considering individual differences and the high variability in autistic symptoms, cognitive functioning, emotional awareness, reactivity, and regulation.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.