
Abstract
The COVID-19 pandemic required in-person interventions to be adapted for remote delivery all over the globe. In South Africa, an in-person cascaded task-sharing naturalistic developmental behavioural intervention was adapted for telehealth delivery in a low-resource context. Here we describe the adaptations made (the ‘what’) and reasons for adaptations (the ‘why’). The Framework for Modification and Adaptations (FRAME) was used to document the ‘what’, and the Exploration, Preparation, Implementation, Sustainment (EPIS) framework to describe the ‘why’. Systematic member-checking ensured robustness of results. The ‘what’ included 10 adaptations: selecting WhatsApp as delivery platform, developing images with simple text to communicate intervention concepts, modifying session structure for hybrid delivery, including a caregiver self-reflection checklist, utilizing online practitioner training, supervision, assessment and consent procedures, developing session recording procedures, distributing session materials electronically, and developing caregiver–child interaction recording and uploading protocols. The ‘why’ included three outer contextual factors (the digital divide, WhatsApp security/privacy policy, and COVID-19 restrictions), three inner contextual factors (characteristics of caregivers and practitioners, ethics board guidance, and school leadership and organizational characteristics) and one innovation factor (support from intervention co-developers). Adaptations were made in response to unchangeable outer contextual factors and through identification of malleable inner contextual factors.
Lay abstract
We were busy with an early autism caregiver-coaching programme in South Africa, when COVID-19 stopped all in-person work. We changed the programme so it could be done using computers and/or phones. Here, we describe programme changes (which we call the ‘what’) and the reasons for those changes (which we call the ‘why’). We used a tool called the Framework for Modification and Adaptations (FRAME) to describe the ‘what’, and the Exploration, Preparation, Implementation, Sustainment (EPIS) framework to describe the ‘why’ of our programme changes. The team members who helped make these changes checked that the changes described were correct. We made 10 changes in total: we used WhatsApp to deliver the programme, made simple pictures with words as visual tools for the programme, changed some session activities, changed a self-reflection checklist, provided all activities online, changed the way assessment and consent was done, made a session recording guide, sent things needed for sessions by email and WhatsApp, and made a caregiver–child play recording guide. The reasons for changes (the ‘why’) were about factors outside schools (the types of phones and data people had, WhatsApp security rules, COVID-19 rules), things inside schools/workplace (about the caregivers and nonspecialists themselves, ethics boards, things about the school itself), and support from people who developed the programme. Changes were made by working with things inside schools/workplace that could change. Identifying what could change helped focus and guide which changes were made to a programme.
Keywords
Early intervention for autism is a public health priority (Lord et al., 2022; World Health Organization [WHO], 2013). In recent years Naturalistic Developmental Behavioural Interventions (NDBI) have emerged as a class of evidence-based early autism intervention approaches. NDBI were designed to take place in naturalistic settings using behavioural strategies to teach developmentally informed child skills (Schreibman et al., 2015). Globally, researchers have been adapting and implementing early intervention in various contexts, more recently even in low- and middle-income countries (LMIC) where resources are typically limited (Divan et al., 2019; Franz et al., 2024; Naithani et al., 2022; Pierucci et al., 2023; Rahman et al., 2016; Rieder et al., 2023; Zhou et al., 2018). Early autism interventions adapted for implementation in LMIC (India, Pakistan, South Africa, Zambia and China) have typically utilized a caregiver-mediated approach, where caregivers were coached in strategies (either developmental or NDBI) to use with their autistic children (Divan et al., 2019; Franz et al., 2024; Naithani et al., 2022; Rahman et al., 2016; Rieder et al., 2023; Zhou et al., 2018). In many of the studies, the caregiver-mediated intervention was delivered by nonspecialists via a task-sharing approach where intervention tasks that would typically be the responsibility of highly qualified interventionists are shared between providers with different levels of training (Orkin et al., 2021). High quality research evaluating child, caregiver and implementation outcomes in response to adapted early interventions is limited globally, and virtually absent in LMIC (Crank et al., 2021; Sandbank, 2020).
The use of technology in autism interventions has been gaining interest in recent years (Amaral & de Vries, 2020; Kumm et al., 2022; Lord et al., 2022) and the COVID-19 pandemic accelerated this shift towards technology and telehealth due to restrictions on in-person interactions. Apart from the enforced shift caused by the pandemic, telehealth could be particularly promising in LMIC where services and expertise are scarce and difficult to access (Acharibasam & Wynn, 2018; Ellison et al., 2021; Franz et al., 2022; Heng et al., 2021; Stuckey & Domingues-Montanari, 2017).
A systematic review conducted by De Nocker and Toolan (2023) identified 16 peer reviewed studies published before January 2021 on telehealth intervention studies for children with autism. Most studies (14 of 16) provided coaching to caregivers, teachers or therapists via video conferencing, either through synchronous or a combination synchronous and asynchronous delivery. Two studies provided caregivers with asynchronous-delivered didactic training (no coaching component). Telehealth-delivered approaches were found to be feasible, satisfactory, and resulted in positive child outcomes such as increased social communication and language skills. In line with previous reviews (Boisvert et al., 2010; Ellison et al., 2021), telehealth services were found to be equivalent to in-person services or at least superior to control groups. No difference was found between outcomes from in-person and telehealth delivery, suggesting that participants benefit from telehealth as much as they do from in-person coaching. It is important to note that all studies considered participant access to technology, Internet and equipment in their study design. However, none of the 16 studies were conducted in LMIC (de Nocker & Toolan, 2023). Furthermore, several of the tele-delivered interventions included in these reviews (Boisvert et al., 2010; de Nocker & Toolan, 2023; Ellison et al., 2021) were adapted from in-person interventions, but to our knowledge no study systematically described and documented the adaptations.
Telehealth has the potential to provide a cost-effective manner of increasing the reach of service providers globally and could be a particularly promising solution to challenges in LMIC. In comparison to more traditional services, telehealth requires relatively little infrastructure and could therefore be cost-effective and scalable. It can put families in direct contact with services and service providers that are far away, expensive to get to, and thus not regularly accessible, if they are accessible at all. This could have a significant impact on young autistic children and their families in LMIC.
LMIC, however, have unique contextual factors (including socio-economic, linguistic and cultural) that may influence adaptations for telehealth delivery. A particularly important contextual consideration is the gap in access to digital technologies between different socio-economic groups, commonly referred to as the ‘digital divide’ (World Bank, 2016).
A systematic description of parts of an intervention adapted for telehealth delivery (referred to as the ‘what’) and reasons for the adaptation (referred to as the ‘why’) may serve as a model demonstration to inform clinical and research teams who wish to make similar intervention adaptations. No publication to date has documented the ‘what’ and the ‘why’ of an intervention adapted for telehealth delivery in any LMIC or low-resource context.
A framework for documenting telehealth adaptations
Systematic documentation of adaptations facilitates better understanding of factors leading to successful implementation as well as replication of adaptations. The Framework for Modification and Adaptations (FRAME) (Stirman et al., 2013; Wiltsey Stirman et al., 2019) guides documentation of adaptations through eight aspects of the adaptation process: (1) when and how in the implementation process the modification was made, (2) whether the modification was planned/proactive or unplanned/reactive, (3) who determined that the modification should be made, (4) what was modified, (5) at what level of delivery was the modification made, (6) the nature of content-level modifications, (7) the relationship to fidelity, and (8) reasons for the modification. The FRAME has been used to document adaptations to a variety of interventions, including evidence-based autism interventions (Chlebowski et al., 2020; Dickson et al., 2020; Lange et al., 2022). A codebook and coding sheet (or FRAME matrix) can be used to guide the documentation process (Stanford Medicine, 2023).
An implementation framework for telehealth adaptation
Optimal contextual fit has been shown to increase the likelihood of producing desired clinical outcomes and integration into everyday practice (Aarons et al., 2011; Fixsen et al., 2009; Pyne et al., 2005). Intervention adaptation therefore requires careful consideration both of the intervention and the implementation context to ensure a good contextual fit. (Bauer et al., 2015; Moullin et al., 2019; Vivanti et al., 2018). Many implementation factors, including affordability (cost of implementation), accessibility (ease of intervention access), appropriateness (perceived compatibility of intervention and context) and sustainability (extent to which intervention delivery can be maintained) influence intervention fit with the implementation context (Dawson-Squibb & de Vries, 2019; Kumm et al., 2022; Lord et al., 2022; Schlebusch et al., 2020).
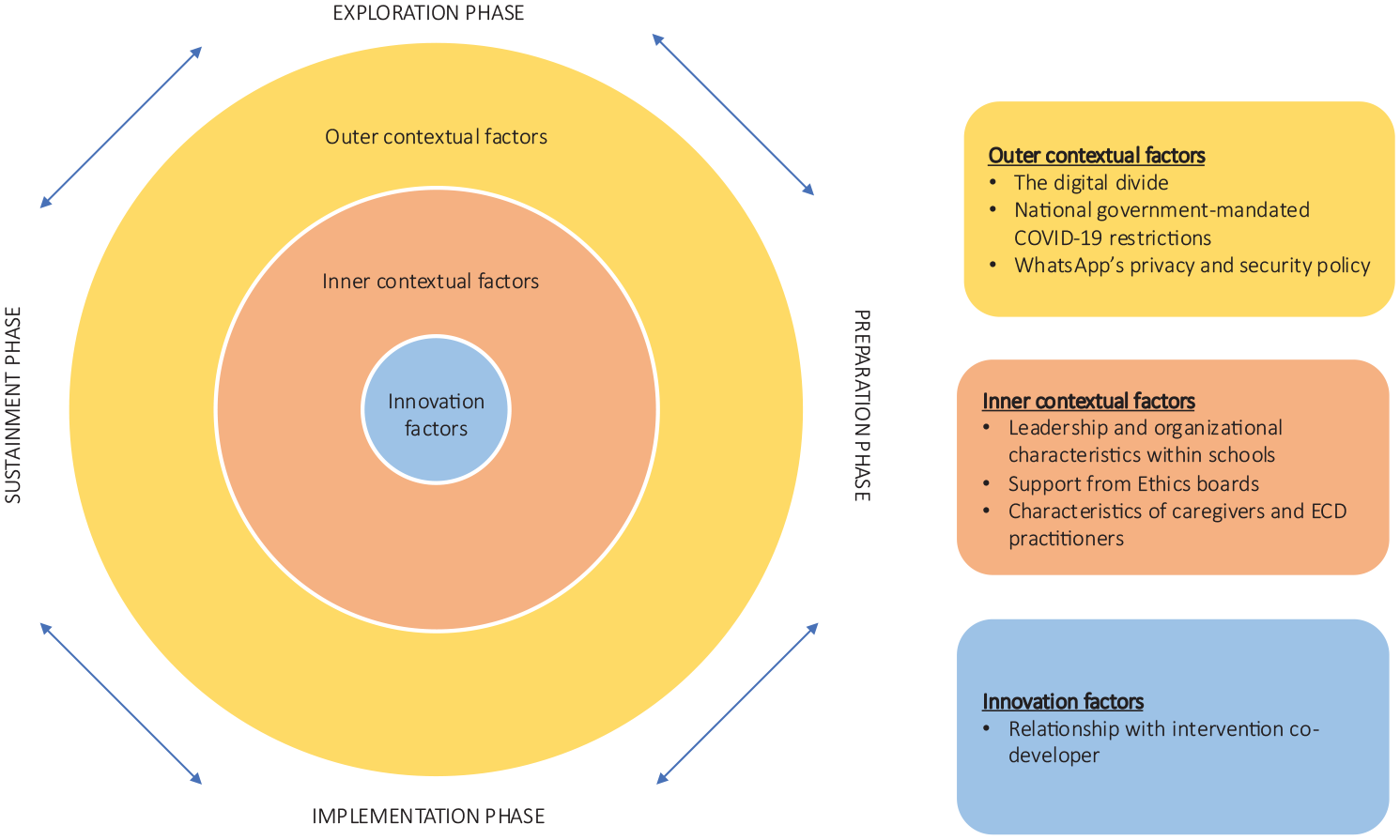
Various implementation frameworks have been developed to guide contextual considerations (Becan et al., 2018; Moullin et al., 2019; Proctor et al., 2009). The Exploration, Preparation, Implementation, Sustainment (EPIS) framework is one the most widely used implementation frameworks in the public service sector (Aarons et al., 2011; Moullin et al., 2019). The EPIS framework describes outer contextual, inner contextual, innovation and bridging factors that may influence implementation (see Figure 1) during the four implementation phases (exploration, preparation, implementation and sustainment). Inner context refers to characteristics within the organization where implementation is taking place, for example organizational leadership. Outer context refers to characteristics of the system outside the organization, for example national policies. Innovation factors are characteristics of the intervention, for example, characteristics of the intervention developers. Inner and outer contextual factors affect how much support and resources are available for implementation and how easily an intervention can be implemented in a specific context. Bridging factors connect inner and outer contexts and facilitates communication and collaboration between stakeholders. Innovation factors determine intervention fit and how much an intervention can be adapted to improve fit. This study describes adaptations made during the preparation phase. The main purpose/goal of the preparation phase is to identify implementation barriers and facilitators in the inner and outer contexts and plan around these so that implementation is supported during the implementation and sustainment phases (EPIS Framework, n.d.; Moullin et al., 2019; Stirman et al., 2013; Wiltsey Stirman et al., 2019).
The exploration, preparation, implementation and sustainment framework.
Adaptation is an integral part of implementation because it allows interventions to be tailored to fit diverse contexts, populations, and needs while maintaining core intervention components (Aarons et al., 2011; Becan et al., 2018; Wiltsey Stirman et al., 2019). The EPIS framework has therefore been used to inform and guide adaptation during the implementation process across all implementation phases in several studies (Aarons et al., 2011; Becan et al., 2018; Chambers, 2023). In this study, we describe EPIS inner contextual, outer contextual and innovation factors that guided adaptation during the Preparation phase of the EPIS.
While the adaptation of in-person sessions to telehealth delivery originated out of necessity in response to COVID-19 restrictions, it provided a naturalistic opportunity to ask key research questions about adaptation of telehealth interventions for autism in low-resource contexts.
In this article, we set out (1) to document the intervention adaptations made to switch our NDBI-informed caregiver coaching from in-person to telehealth-delivery (referred to as the ‘what’ of adaptations), and (2) to describe factors that informed adaptation (the ‘why’ of adaptations).
The starting place: an in-person cascaded task-sharing NDBI
The in-person cascaded task-sharing NDBI caregiver coaching intervention (Rieder et al., 2023) was based on the Community Early Start Denver Model (C-ESDM) approach, an open access, web-based distance-learning intervention designed to help community providers and caregivers of children at high likelihood of having autism in low-resource contexts learn NDBI strategies (Rogers et al., 2022, 2024). Early Childhood Development (ECD) practitioners employed by the Western Cape Education Department (WCED) delivered the NDBI-informed caregiver coaching session (Franz et al., 2018; Rieder et al., 2023; Guler et al., 2018; Makombe et al., 2019; Ramseur et al., 2019). ECD practitioners have a 10-month diploma in ECD which involves training on the basic principles of early child development and facilitating learning programmes for groups of children (e.g. in a preschool setting). They typically have no coaching experience or autism-specific training but may work with autistic children when teaching.
Session structure
The 12, 1-h, in-person cascaded task-sharing NDBI caregiver coaching sessions, delivered by ECD practitioners, followed a predetermined session structure consisting of five parts (Rieder et al., 2023). Sessions started with greeting and check-in, followed by a warm-up activity (to gauge the caregiver’s integration of skills coached on during the previous session) and caregiver reflection. Review of session content (the ‘topic of the day’) through review of C-ESDM video material was then followed by two in-session caregiver coaching activities during which caregivers were supported in implementation of the session skill. This was followed by a post-activity reflection, and a generalization/closing discussion on application of the session skill across daily activities.
Session content
Session content from C-ESDM video material included strategies to increase child attention to people through use of positioning and following the child’s lead, increasing child communication using gestures, sounds and speech, setting up joint activity routines, and strategies to help caregivers teach new behaviours by improving understanding of antecedents, behaviours and consequences (Rieder et al., 2023).
ECD practitioner training and supervision
Prior to delivering caregiver coaching sessions, the ECD practitioners and their direct supervisor (head of departments in the schools) attended a 4-day in-person training led by ESDM-certified South African therapists. The purpose of the training was to introduce intervention concepts, session structure and basic caregiver coaching principles through didactic instruction, role-play and practice sessions with a caregiver–child dyad. Following the 4-day training, ECD practitioners were supervised by ESDM-certified therapists during intervention sessions in the schools (Rieder et al., 2023).
Methods
The study was a collaboration between the University of Cape Town and Duke University. All research activities occurred at the Centre for Autism Research in Africa (CARA), based in the Division of Child and Adolescent Psychiatry at the University of Cape Town. Intervention sessions took place in autism-specific public schools in Cape Town. Public schools in the Western Cape are governed by the Western Cape Educational Department (WCED) who report to the National Department of Basic Education (DBE).
Ethics, protocol registration and funding
University of Cape Town and Duke University ethics review boards approved study procedures (UCT HREC 468/2019, Duke IRB Pr00103045). The study protocol was registered on Clinical Trials.gov (NCT04068688).
Study design
We conducted a qualitative description of adaptations made to the cascaded task-sharing NDBI when the intervention transitioned from in-person to telehealth delivery, and of EPIS factors that informed adaptations.
Data sources and adaptation process
The intervention was adapted through an iterative process while considering relevant EPIS factors. Weekly team meetings were held to discuss and plan the tele-adaptation. Adaptation plans and reasons for adaptations (informed by EPIS factors) were recorded in weekly meeting notes by the study team. Entries included the date of the meeting, the part of the intervention being adapted (e.g. ECD practitioner training), summary of the discussion or description of adaptation (e.g. a description of the online ECD practitioner training) and person/s responsible for action items (e.g. name of team member responsible for specific tasks in preparation for ECD practitioner training).
Some adaptation activities, such as the development of session materials, involved intensive planning that took place outside weekly team meetings. Planning steps and progress summaries were outlined for each of these adaptation activities in separate team summary documents. Entries included dated iterations of each version of the adapted session materials showing progress over time. ECD practitioners and a C-ESDM co-developer reviewed and provided feedback on adaptations to session materials. Summary documents and meeting notes were used as data sources to identify the ‘what’ and ‘why’ of adaptations.
Data analysis
The Framework for Modification and Adaptations (FRAME) (Stirman et al., 2013, 2019) was used to document adaptations (the ‘what’) and the EPIS was used to describe reasons for adaptation (the ‘why’). The FRAME provides an approach to systematically describe and categorize modifications to interventions. Analysis of the ‘what’ and ‘why’ of adaptations followed four predetermined steps as demonstrated in Figure 2. Steps 1 and 2 were informed by guidelines in the FRAME coding manual (Stanford Medicine, 2023) as well as Mui et al. (2024) application of FRAME coding guidelines. Steps 3 and 4 expanded on results from steps 1 and 2.
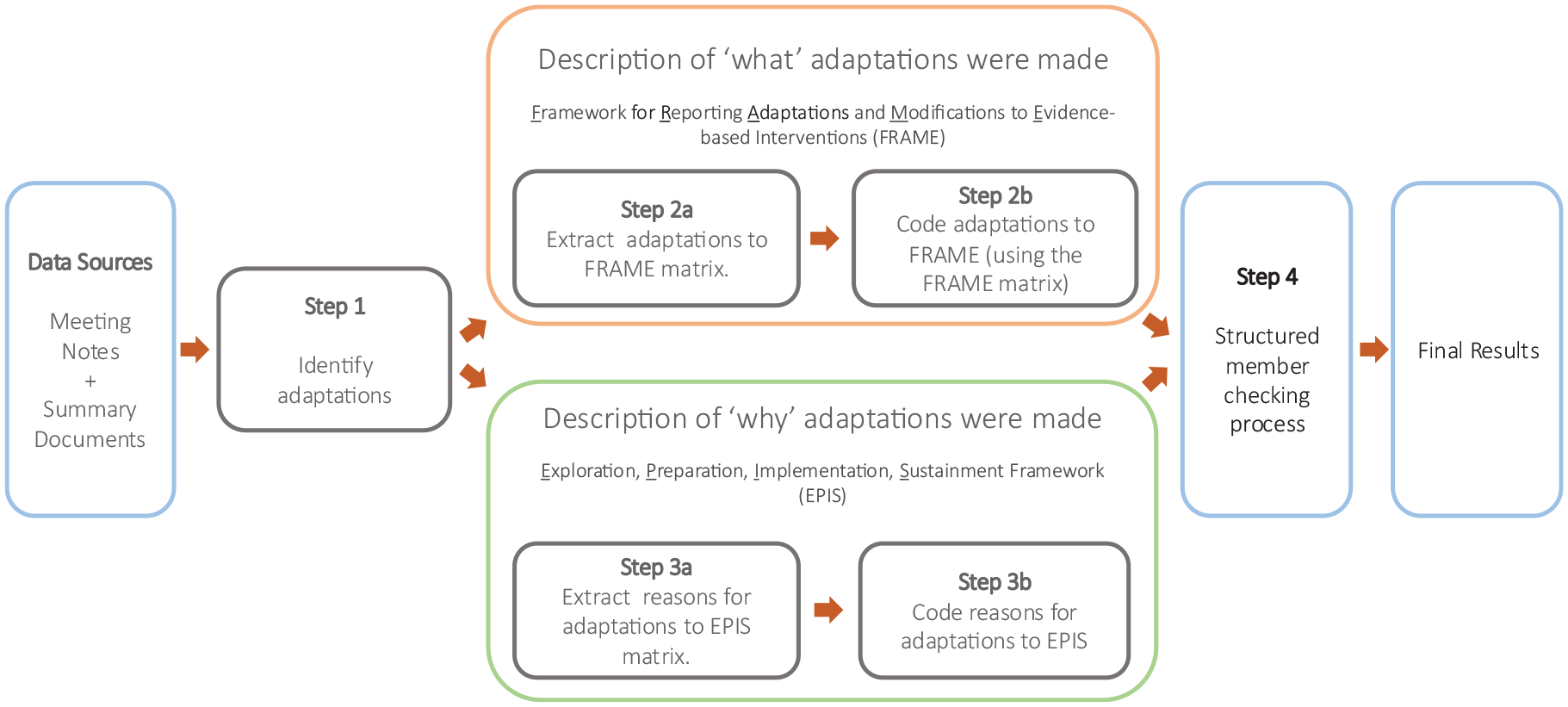
The data analysis process.
Analysis of adaptations made (the ‘what’)
The first step was to identify adaptations in data sources (meeting notes and summary documents) according to guidelines in the FRAME coding Manual (Wiltsey Stirman et al., 2019). The first author (M.V.) read through all data sources and identified entries that met criteria for Stirman’s definition of an adaptation (Stirman et al., 2013, p. 2). The first author was a certified South African ESDM therapist and study Project Coordinator who was familiar with the intervention prior to adaptation and could therefore recognize changes made.
The second step was to describe adaptations identified in step 1. This step consisted of two parts. The first part of step 2 (see step 2a in Figure 2) was to extract adaptations to the FRAME matrix. Following a similar approach to Mui et al. (2024), all adaptations identified in step 1 were summarized and extracted into Excel. Each row in the matrix represented one adaptation, and each column heading represented a FRAME construct (i.e. when the adaptation was made, whether the adaptation was planned or unplanned, who decided that the adaptation should be made, what was adapted, for whom was the adaptation made, if intervention content was modified – what part was modified, and the whether the core parts needed to make the intervention efficient was adapted). As per Mui et al. (2024), a column describing the original intervention component (prior to adaptation) was included to facilitate better interpretation of each adaptation. The second part of step 2 (see step 2b in Figure 2) was to code adaptations to FRAME using the Excel matrix created in step 2a. This was done by the first author (M.V.) by following the steps outlined in the FRAME coding manual (Wiltsey Stirman et al., 2019).
Analysis of the reasons for adaptations (the ‘why’)
Step 3, an analysis of why adaptations were made, consisted of two parts. In the first part of step 3 (step 3a), reasons for each adaptation were identified from data sources and extracted into an Excel matrix and coded to EPIS constructs (see step 3a in Figure 2). We used descriptions of EPIS factors as defined by Aarons and colleagues (Aarons et al., 2011). Each row in the matrix represented one adaptation, and each column heading represented an EPIS factor (i.e. six inner contextual factors, six outer contextual factors, five innovation factors). In the second part of step 3 (step 3b), adaptations were coded to the EPIS matrix. A single adaptation could have several reasons for adaptation and therefore could be coded to several EPIS factors.
Systematic member-checking process
In the final step (step 4, see Figure 2), a systematic member-checking approach as suggested by McKim (2023) was followed to allow for feedback on the accuracy of results (Candela, 2019; McKim, 2023; Motulsky, 2021; Thomas, 2017; Varpio et al., 2017).
A thorough understanding of the in-person intervention, telehealth intervention and other project details (e.g. names and roles of team members, details of schools and school staff) were necessary to interpret information in data sources (meeting notes and summary documents). Complete objectivity was therefore not a desirable expectation of a person interpreting the data as some degree of familiarity with the source documents and data was necessary to discern the meaning. Incorporating a member-checking process allowed us to explore the credibility of results from the perspective of all team members involved.
To facilitate reflection prior to the member-checking meeting a summary of adaptation descriptions according to FRAME and reasons for adaptation along with questions that would facilitate the meeting was sent to the study team who took part in the adaptations ahead of time. At the member-checking meeting, the first author presented findings and the following four questions asked: (1) After reviewing the findings, what are your general thoughts? (2) How accurately do you feel the findings capture the adaptations and reasons for adaptations? (3) What could be added to the findings to better capture adaptations and reasons for adaptations? (4) Are there adaptations and reasons for adaptations you would like to remove, and why? Feedback was integrated into results.
Community involvement
Discussions and feedback with community stakeholders (e.g. caregivers of young autistic children, early childhood development practitioners delivering the sessions, principals of schools) informed adaptations as described in this article. Community stakeholders and autistic individuals were however not directly involved in the design of the telehealth adapted caregiver coaching sessions.
Results
Description of adaptations – the ‘what’
Adaptation planning took place over 8 months and a total of 10 adaptations were identified (see Table 1). In the telehealth intervention, caregivers attended 12, 1-h telehealth sessions facilitated by ECD practitioners over WhatsApp voice or video call (adaptation 1). All sessions followed a predetermined session structure (adaptation 3) that included greeting and check-in, review of a home-recorded caregiver–child interaction video (adaptation 10) using a caregiver self-reflection checklist (adaptation 4), review of session content (the ‘topic of the day’) using images and accompanying scripts (adaptation 2) that were sent to caregivers over WhatsApp before sessions (adaptation 9), and finally discussion about generalization of session skills outside of sessions. Consent and assessment of intervention outcomes were either done telephonically or via online RedCap surveys (adaptation 7). Sessions were audio recorded to monitor ECD practitioner coaching fidelity (adaptation 8). Before sessions commenced ECD practitioners attended training over Zoom (adaptation 5) followed by weekly supervision over WhatsApp voice or video call (adaptation 6).
Summary of the ten adaptations made in this study (the ‘what’).
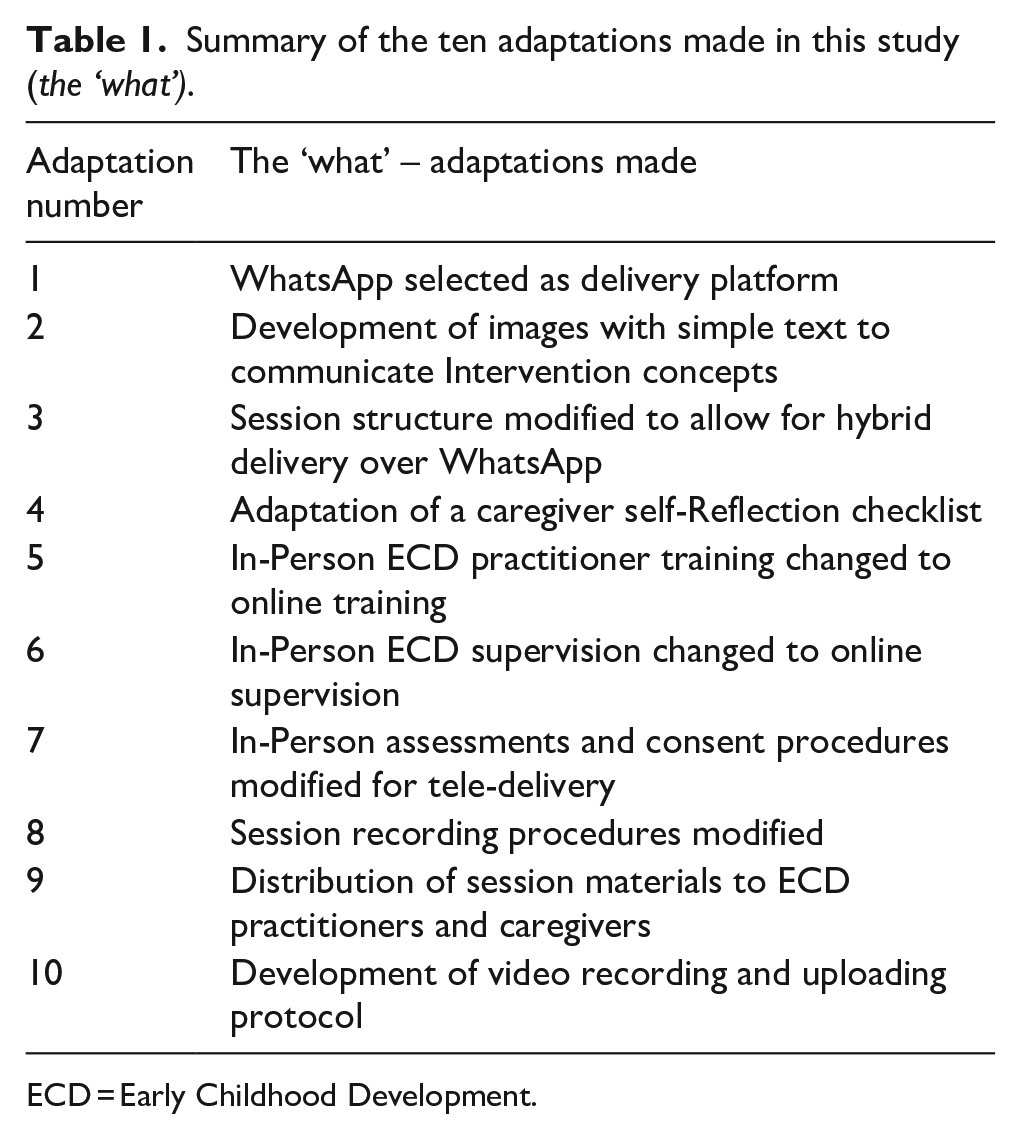
ECD = Early Childhood Development.
Consistent with components of the FRAME all adaptations were planned adaptations made during the preparation phase of the EPIS. The purpose of all adaptations was to develop contextually appropriate telehealth sessions that were accessible to participants and could be delivered by ECD practitioners. In addition, the purpose of adaptation 8 (session recording procedures modified) was ensuring session recordings were available to rate coach fidelity. Adaptations therefore targeted the intervention group, namely, caregivers of young autistic children and ECD practitioners responsible for delivering the coaching sessions. The entire research team participated in adaptation decisions and processes. Various stakeholders and experts were consulted on specific topics such as development of images to communicate intervention concepts, the online consent process and video recording and uploading (see supplementary material – FRAME coding matrix). By consulting an intervention developer, we took care to ensure that modifications to intervention content were fidelity consistent. Fidelity-consistency was however not evaluated at this stage of the study.
Adaptations were made to several levels of delivery. Adaptations to the context included WhatsApp selected as delivery platform (adaptation 1), and development of video recording and uploading protocol (adaptation 10). Adaptations to the content included development of images with simple text to communicate intervention concepts (adaptation 2), modification of session structure to allow for hybrid delivery (synchronous and asynchronous delivery) over WhatsApp (adaptation 3) and adaptation of a caregiver self-reflection checklist (adaptation 4). Changing in-person ECD practitioner training to online training (adaptation 5) and changing in-person ECD supervision to online supervision (adaptation 6) were both training adaptations. Modification of in-person assessments and consent procedures for tele-delivery (adaptation 7) and modification of session recording procedures (adaptation 8) were evaluation modifications. The only implementation activity modification was distribution of session materials to ECD practitioners and caregivers (adaptation 9).
Adaptation 1: WhatsApp selected as delivery platform
WhatsApp was identified as the online session delivery platform to replace in-person session delivery. WhatsApp is a widely used instant messaging platform. Voice and video calls and messages are end-to-end encrypted meaning data are not accessible by third parties while being transferred between devices. Study participants indicated that they had access to WhatsApp using entry-level Android smartphones and either mobile data or WiFi. Once WhatsApp was identified as a suitable delivery platform option, we identified activities that could be performed over WhatsApp while maintaining participant privacy and confidentiality as approved by University of Cape Town and Duke University ethics boards (see inner contextual EPIS factors). Approved actions and activities included WhatsApp voice calls, WhatsApp video calls and distribution of session materials to communicate intervention concepts (WhatsApp images).
Adaptation 2: development of images with simple text to communicate intervention concepts
Images and accompanying simple text were created to communicate core intervention concepts. They served as a substitute for C-ESDM video material, which our study population could not access due to the high data costs and need for high-end devices (phones or computers) capable of streaming online videos. To ensure fidelity to core intervention concepts the development of intervention material was led by the study PI (an ESDM trainer) and 3 culturally diverse South African ESDM-certified therapists who had experience supervising in-person coaching sessions in schools. A C-ESDM co-developer provided feedback on various draft of the intervention materials.
The WhatsApp image development process consisted of several steps that were guided by the eight dimensions of the Ecological Validity Framework (including language, persons, metaphors, content, concepts, goals, methods and context) (Bernal et al., 1995) to ensure development of materials that were culturally sensitive. The team first identified core concepts from each in-person intervention session as outlined on session ‘Refrigerator Lists’. Next images with simple text and accompanying ECD scripts that captured session-specific core concepts were developed in collaboration with a South African graphic designer through four rounds of iterative feedback and edits. A co-developer of C-ESDM video material who is also an implementation science expert, provided feedback and recommendations on the WhatsApp images and accompanying simple text. Recommendations were incorporated into the final version of the images, which consisted of twelve session-specific visuals with simple text. The images were shared over WhatsApp messages and therefore referred to as ‘WhatsApp images’ by the team and participants.
Adaptation 3: session structure modified to allow for hybrid delivery over WhatsApp
Telehealth sessions used elements from both synchronous (real-time interactions between caregivers and providers) and asynchronous (sharing of videos by caregivers for review by providers at a time convenient to them, and without face-to-face interaction between caregiver and provider) delivery approaches, referred to as a hybrid approach (Simacek et al., 2021). Intervention concepts were introduced during sessions, but caregivers practised implementation of skills outside of sessions and no in-session coaching took place. Caregivers used their smartphones to record and upload videos of them practicing the skills during caregiver–child interactions at home for reflection and discussion during sessions. As shown in Figure 3, the in-person session structure and plans were adapted for telehealth delivery with the goal of retaining all core intervention concepts and as many parts of the session structure (the sequence of activities that took place during each session) as possible. Four of the five parts from in-person session were adapted by tailoring, removal or substitution (Figure 3). No changes were made to the greeting and check-in. The in-person warm-up activity (a caregiver–child play activity observed by the ECD practitioner to gauge the caregiver’s integration of skills coached on during previous sessions) was substituted with the review of a home-recorded caregiver–child interaction using a caregiver self-reflection checklist (list of target caregiver and child behaviours). Review of C-ESDM video content (the ‘topic of the day’) was substituted with WhatsApp images with simple text and accompanying ECD scripts (description of images and skills illustrated in caregiver-facing materials). In-session coaching was removed entirely. The final part of each session was tailored to a more detailed discussion of generalization of the session skills across six everyday activities (mealtimes, self-care activities, toy play, chores, books and social play).
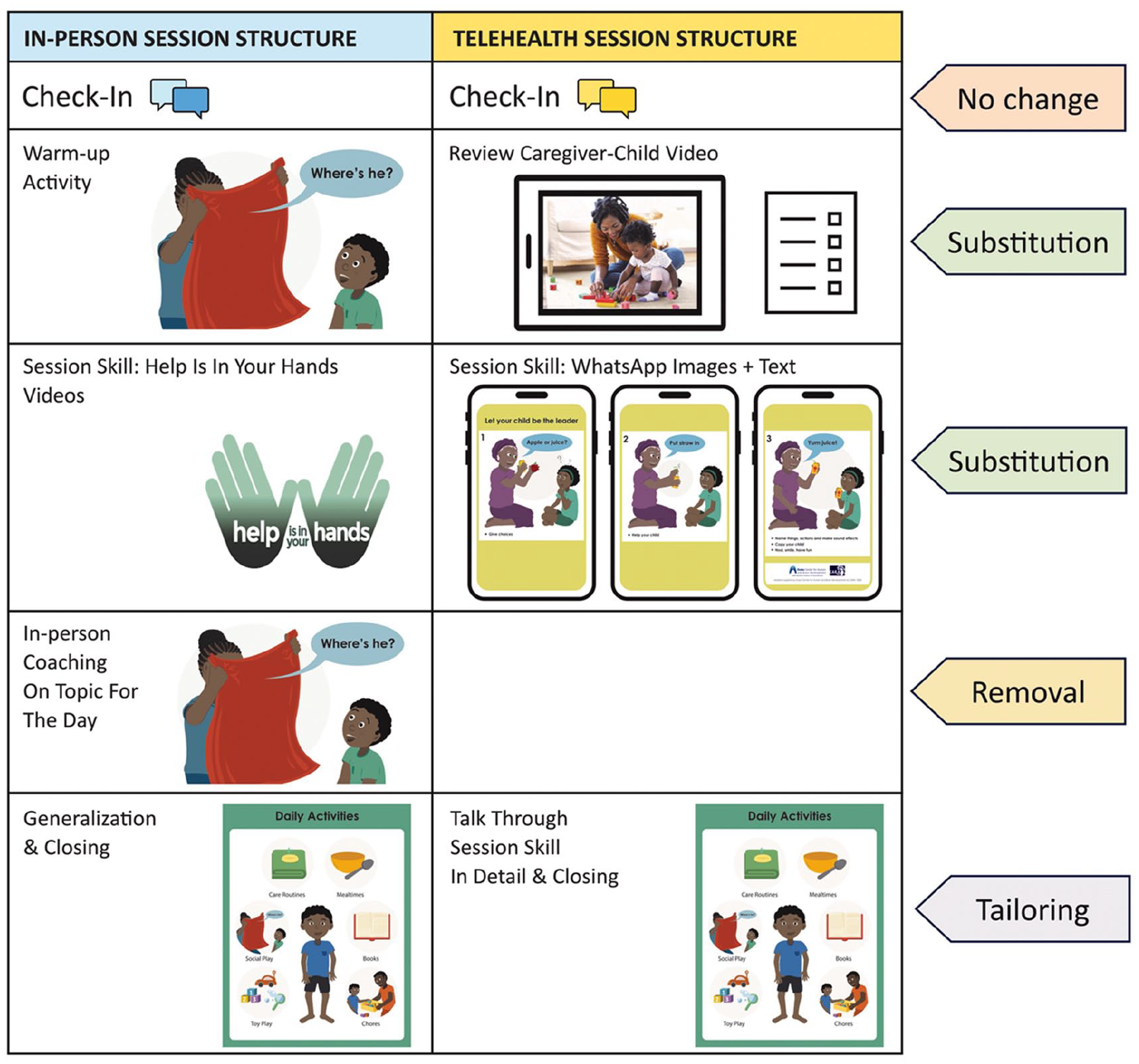
Session structure adaptations made by tailoring, removal, and substitution of session activities.
Adaptation 4: adaptation of a caregiver self-reflection checklist
The caregiver self-reflection checklist was used to facilitate structured reflection of caregiver–child video recordings during sessions. It was adapted from the ESDM caregiver self-reflection checklist (Rogers et al., 2021), keeping all the original items but simplifying the language to ensure clarity. Culturally diverse South African team members and the US PI revised the wording and decided on a final version during team meetings. The structure of the checklist was also adapted to make it easier for caregivers to understand. Changes involved grouping child behaviours and caregiver behaviours together and adding a sentence before questions referring to child behaviour (‘first, we are going to talk about things you saw your child do in the video’) and before questions referring to caregiver behaviour (‘now we are going to talk about some things you did in the video’).
Adaptation 5: in-person ECD practitioner training changed to online training
The 4 day in-person ECD practitioner training (8 h per day) was converted to a 4-day Zoom training (2 h per day). Two ECD practitioners and their school supervisors attended from their respective schools where they had laptop and Internet access. Since both ECD practitioners had prior experience with in-person sessions, they were already familiar with intervention concepts and the in-person session structure. The training included an introduction to telehealth sessions, technical aspects of conducting a WhatsApp call and viewing home-recorded caregiver–child interaction videos, practice using the caregiver self-reflection checklist, overview of intervention concepts displayed in WhatsApp images, session structure and plans, and conducting two practice sessions with a caregiver. Technical aspects, such as video downloading and setting up a WhatsApp call, were also practised during the mock sessions.
Adaptation 6: in-person ECD practitioner supervision changed to online supervision
After the online training, ECD practitioners had weekly 1-h long supervision sessions for 6 weeks, during which telehealth sessions were role-played by the ECD practitioners and study team members (the ECD practitioners practised the sessions with a team member who played the role of a caregiver). Once sessions with caregivers started, supervision occurred 30 min before and after each session. Supervision focused on discussing the caregiver–child video, the session skill and its relevant application for each caregiver–child dyad. All supervision sessions were conducted remotely over WhatsApp video call and facilitated by ESDM supervisors.
Adaptation 7: in-person assessments and consent procedures modified for tele-delivery
An e-consent protocol and online assessment process were created in collaboration with regulatory staff at Duke University and University of Cape Town. Administration of assessments from the in-person sessions were adapted for telephonic or online survey administration where possible. Surveys were administered via RedCap, a secure online platform for managing online surveys and databases. The research team was available to assist telephonically if caregivers needed assistance to complete RedCap surveys. The Vineland-3 (Sparrow et al. 2016) were conducted telephonically. Caregiver-child interaction videos were recorded at home by caregivers using smartphones and uploaded to a secure platform (StrongBox hosted by Duke University). Home-recorded caregiver–child interaction videos were used to complete the caregiver self-checklist during sessions, code caregiver implementation fidelity and describe caregiver–child interactions using the Joint Engagement Rating Inventory (JERI) (Ndlovu, 2024). Since in-person contact was not possible certain assessments, like the Griffiths-III, a clinician-administered developmental assessment that evaluates child strengths and challenges across 5 developmental domains (Green et al., 2015), had to be omitted from telehealth assessments.
Adaptation 8: session recording procedures modified
Audio recordings of sessions were used to capture data needed for rating ESDM coaching fidelity items related to session structure (greeting & check-in, introduction of the session topic, and session closing) and coaching behaviours (collaborative approach, reflective approach, nonjudgmental approach, conversational and reciprocal approach, ethical conduct, organization and management of sessions, and managing caregiver implementation difficulties). Because telehealth sessions were comprised of phone conversations between ECD practitioners and caregivers, audio recordings can be used to code all original items included in the ESDM coaching fidelity checklist, except for coaching activities 1 and 2 (two items that rate the coach’s ability to support the caregiver in practicing the session skill during an in-session coaching activity). In-session coaching was not part of the telehealth approach (see adaptation 3), and coaching activities 1 and 2 can therefore not be rated. Home-recorded videos of caregiver–child interactions informed warm-up activity reflection and need to be viewed with the audio recording to rate coaching fidelity for the warm-up activity reflection.
The development of an audio telehealth session recording protocol was guided by Duke University and University of Cape Town regulatory boards. Session supervisors audio recorded sessions using study laptops. Recordings were uploaded to a Health Insurance Portability and Accountability Act (HIPAA) compliant platform and then deleted from laptop devices.
Adaptation 9: sending session materials to ECD practitioners and caregivers
The purpose of this adaptation was to ensure timely access to session materials (session plans and WhatsApp images) for ECD practitioners and caregivers. WhatsApp was used for distribution of session-specific WhatsApp images. Session plans were uploaded on compliant platform where ECD practitioners could access them. Materials shared over WhatsApp were generic and did not contain any confidential participant identifying data.
Adaptation 10: development of video recording and uploading protocol
As noted above the in-person warm-up activity (a caregiver–child play activity observed by the ECD practitioners to gauge the caregiver’s integration of skills coached on during previous sessions) was replaced with the review of home-recorded caregiver–child videos. Caregivers were asked to upload caregiver–child interaction videos to a HIPAA-compliant platform as part of the baseline and follow-up assessments. To ensure that video recordings were of reasonable quality, a video recording protocol provided caregivers with guidelines on room set-up, phone set-up and the type of materials/toys to use when recording caregiver–child interactions. The process and steps for video upload were also outlined. Instructions for video recording and upload were provided in simple language and included images to illustrate concepts where appropriate. Instructions for video recording and upload were sent to caregivers via WhatsApp, and team members offered telephonic support when caregivers had challenges or questions.
Reasons for adaptations – the ‘why’
The outer contextual, inner contextual and innovation factors from the EPIS framework that guided adaptation are presented here and in Table 2.
Summary of the reasons for adaptations made (the ‘why’ of adaptations).
ECD = Early Childhood Development.
Outer contextual factors
The digital divide
The digital divide was an essential consideration in South Africa – the country with the highest economic inequality (difference between rich and poor) as measured by the GINI coefficient globally (Sulla & Zikhali, 2018; World Bank, 2024). Ensuring that participants from all socio-economic backgrounds could access the telehealth sessions was essential. Most South Africans have access to entry-level Android smartphones and rely on mobile data (Statista, 2023). For this reason, a delivery platform (WhatsApp) that utilizes minimal data and can be accessed with entry-level smartphones was chosen (adaptation 1). Limited access to devices and reliable Internet connection needed for video streaming meant that the session structure was adapted to facilitate a hybrid delivery approach that did not involve video streaming (adaptation 3). Furthermore, caregiver and ECD practitioner data costs were reimbursed by the study.
WhatsApp network privacy policy
WhatsApp’s privacy policy determines who can see messages and hear calls made over WhatsApp. These policies were considered when choosing a delivery platform (adaptation 1) that aligns with University of Cape Town ethics guidelines (see inner contextual factors). University of Cape Town ethics guidelines (see inner contextual factors) required selecting a delivery platform (adaptation 1) that is private and secure (only accessible to those on the call). WhatsApp calls and messages met this requirement as they are end-to-end encrypted, ensuring only the sender and recipient can hear or see them.
National government-mandated COVID-19 restrictions
South Africa implemented some of the strictest government-mandated COVID-19 restrictions globally and as a result no in-person research participant contact was possible during 2020 and most of 2021. Adaptations made to caregiver coaching sessions (adaptation 3), ECD practitioner training (adaptation 5), ECD practitioner supervision (adaptation 6), and assessments (adaptation 7) therefore had to be fully online.
Inner contextual factors
Leadership and organizational characteristics within the schools
The leadership and organizational characteristics within the schools supported telehealth-delivered caregiver coaching sessions, ECD practitioner training (adaptation 5) and ECD practitioner supervision (adaptation 6). Both school principals supported adaptation of caregiver coaching sessions for telehealth delivery because that meant continued access to sessions for caregivers of young autistic children. School principals also indicated that they were willing to allocate resources in the form of space, WiFi (where possible) and ECD practitioner time for caregiver coaching sessions, ECD practitioner training and supervision.
Support from ethics boards
Our team consulted the University of Cape Town Human Research Ethics Committee (HREC), the UCT Research Integrity Office which provides guidance to UCT researchers on responsible research conduct and compliance with international ethical and legal standards, and the UCT eResearch Centre which provides support to researchers on the use of technology, big data and artificial intelligence. All entities confirmed that WhatsApp as delivery platform (adaptation 1); modified assessment and consent procedures (adaptation 7); and session recording procedures (adaptation 8) met required standards. Importantly, Duke University’s Internal Review Board (IRB) also provided guidance on identifying a HIPAA-compliant data storage platform hosted by Duke University, as a secure online platform that could be used for data transfer, video uploading and review (adaptation 10).
Individual characteristics of caregivers and ECD practitioners
Individual caregiver and ECD practitioner characteristics such as cultural background, socio-economic status, level of education, literacy and technical abilities were carefully considered during adaptation. The recruitment source and referral route for telehealth sessions was identical to the in-person intervention and population characteristic were therefore anticipated to be similar. Data from the in-person intervention that included 12 caregiver–child dyads indicated that most caregivers had attained grade 12 or less, were unemployed, and financially ‘struggling’ or ‘just getting by’. Most ECD practitioners attained post-grade 12 certificates. All caregivers and ECD practitioners could speak English (Rieder et al., 2023) .
Telehealth participants (caregivers of young autistic children) indicated that while they had access to entry-level smartphones and data, data costs were high and posed a potential obstacle. This feedback from caregivers guided the decision to use WhatsApp as delivery platform (adaptation 1) as well as the development of a session structure reliant on minimal data (adaptation 3). To address this, data costs were kept low by conducting hybrid sessions that did not require video streaming (adaptation 3) and reimbursing participants for data costs. Caregivers and ECD practitioners indicated they had technical abilities ranging from basic (able to send/receive WhatsApp messages and make calls using mobile phones) to good (regular use of computers and mobile phones to make video calls, send messages/emails or draft documents). Telehealth assessment procedures (adaptation 7), session recording procedures (adaptation 8), distribution of session materials procedures (adaptation 9) and the video recording and uploading protocol (adaptation 10) were designed to be simple to accommodate for all technical abilities, as well as applicable to entry-level smartphones.
Images that communicated intervention concepts (adaptation 2) were representative of different racial and cultural groups in the Western Cape Province, and objects and toys commonly found in South African homes. Caregivers had varying levels of literacy, so images were designed to be understandable even without accompanying simple text. All caregivers could speak English, but English was not everyone’s first language. Text accompanying WhatsApp images (adaptation 2) was therefore minimal, in plain conversational English and read aloud to caregivers after asking them to describe what they saw in images. Similarly, the caregiver self-reflection checklist (adaptation 4) did not contain technical language and was read aloud to caregivers by ECD practitioners during sessions.
ECD practitioners and school supervisors expressed a desire to be part of the adaptation and offered feedback and suggestions around what would work in their schools. One school supervisor suggested using WhatsApp as the delivery platform (adaptation 1) since the school found it the most practical way of communicating with caregivers. They also highlighted the preference for video over voice calls to support communication and rapport building. Furthermore, ECD practitioner familiarity with C-ESDM concepts and in-person session structure meant that the content of online ECD practitioner training and supervision (adaptations 5 and 6) only included a brief overview of both these components. ECD practitioner training was therefore significantly shorter than the in-person training.
Innovation factors
Relationship with intervention co-developer
The research team and PI had an existing relationship with a co-developer of C-ESDM who was also a consultant on the study. They supported using C-ESDM video material as the foundation for the development of images to communicate intervention concepts. The co-developers input and feedback on various iterations of images was incorporated when finalizing the WhatsApp materials (adaptation 2). Furthermore, the team had an ongoing relationship with the original ESDM developers who were supportive of the telehealth adaptations.
Discussion
In this article, we described the ‘what’ and ‘why’ of adaptations to change an in-person cascaded task-sharing NDBI-informed intervention to telehealth for a low-resource population in Cape Town, South Africa.
The ‘what’ consisted of 10 adaptations that included selecting WhatsApp as delivery platform, developing images to communicate intervention concepts, modifying session structure for hybrid delivery over WhatsApp, adapting a caregiver self-reflection checklist, developing online ECD practitioner training, supervision, assessment and consent procedures, session recording procedures, distribution of session materials, and video recording and uploading protocol. The ‘why’ (reasons for adaptations) comprised of three outer contextual factors (digital divide, WhatsApp security & privacy policy, COVID-19 restrictions), three inner contextual factors (characteristics of caregivers & ECD, support from ethics boards and leadership & organizational characteristics within the schools) and one innovation factor (our established relationship with the intervention co-developer).
Over the past decade and especially during the COVID-19 pandemic the use of technology for autism accelerated (Acharibasam & Wynn, 2018; Amaral & de Vries, 2020; de Nocker & Toolan, 2023; Ellison et al., 2021; Kumm et al., 2022; Lord et al., 2022). Many of the technological innovations inspired by COVID-19 continue to be used post-pandemic (Ameis et al., 2020; Dow et al., 2022; Eapen et al., 2021; Rehman et al., 2021). In light of the rapid technology acceleration several papers have emphasized the importance of developing interventions supported by technology that do not exacerbate existing socio-economic disparities, that promote equitable access to services, and ensuring a ‘fit’ with the intervention delivery context (Amaral & de Vries, 2020; Kumm et al., 2022; Lord et al., 2022). In most instances, the intervention itself, the delivery context or both context and intervention have to be adapted to ensure a good fit (Bauer et al., 2015; Moullin et al., 2019; Vivanti et al., 2018).
In this adaptation, outer contextual factors, including the digital divide, WhatsApp security and privacy policy, and COVID-19 restrictions were harder to influence as they were outside the direct control of the team. As a result, adaptations had to work around outer contextual factors that could not be changed. In contrast, inner contextual factors represented more malleable factors that could be engaged with and in some cases shaped. For example, as a result of COVID-19 restrictions (outer contextual factor), no in-person contact was possible and ECD practitioner training had to be done online. Leadership and organizational characteristics (inner contextual factor) within the schools allowed for discussions on giving ECD practitioners time off teaching duties, providing Internet access, computers and space. A systematic review of task-sharing mental health interventions in LMIC (Le et al., 2022) identified a similar pattern in the 28 studies they reviewed. Factors that could be changed (e.g. provider or intervention characteristics) were predominantly located in the context where interventions were implemented (inner contextual factors) and identified by researchers as implementation facilitators. Factors outside the intended intervention delivery context (outer contextual factors) were harder to influence (e.g. health systems) and researchers identified them as implementation barriers (Le et al., 2022).
Several studies have highlighted the importance of engaging with inner contextual factors (school leadership, ethics boards, participants) to ensure contextual fit (Aarons et al., 2011; Ansari & Weiss, 2006; Bernal et al., 1995; Brookman-Frazee et al., 2020; Hoekstra et al., 2018; Kreuter et al., 2000; Pellecchia et al., 2024). One example is the consideration of participant characteristics (such as participant literacy) when developing data collection methods. Through engagement with community stakeholders an Ethiopian study (Tilahun et al., 2019, 2017) identified that questionnaires and online surveys were not a good fit for their participants and subsequently collected data through face-to-face interviews by trained lay interviewers (Tilahun et al., 2017, 2019). In our adaptation, participants indicated that they could complete online surveys, but on entry-level smartphones. An important consideration in our adaptation was therefore ensuring that RedCap surveys were compatible with entry-level devices. These two studies both required questionnaires to be completed, but used different data collection methods (online surveys vs interviews) based on information gained through engagement with participants and community stakeholders (inner contextual factors). Both examples illustrate how engagement with inner contextual factors can guide adaptations to ensure contextual fit, in this case of data collection methods.
It was helpful to have identified the outer contextual factors that could not be changed and make adaptations around those, while also considering the malleable inner contextual factors and how they could be shaped as part of the adaptation process. Recognition of malleable factors as well as factors that cannot be changed can focus adaptation efforts and guide the adaptation process.
Relevance of adaptation work and implications for research and practice
The early autism intervention gap in LMIC is close to 100% (Naithani et al., 2022; Pervin et al., 2022; Rahman et al., 2016) and almost all autism intervention research to date comes from high income countries (Franz et al., 2017; Pervin et al., 2022). Similarly, knowledge about technology, including telehealth, in autism intervention also originates almost exclusively from HIC (de Nocker & Toolan, 2023; Ellison et al., 2021; Kumm et al., 2022). Considering that 95% of children with autism live in LMIC, the need to address this intervention gap is clear. Adaptation work presented in this article has broad relevance to LMIC and other resource-limited contexts where researchers and clinicians need to address the intervention gap by adapting existing evidence-based approaches for their specific context. Adaptation of evidence-based approaches for telehealth, as illustrated here, could be a scalable and sustainable option for low-resource settings where designing novel interventions is not viable.
There is currently a lack of publications providing examples of intervention adaptations for telehealth-delivery, especially in diverse low-resource contexts (de Nocker & Toolan, 2023; Ellison et al., 2021). Examples of contextually relevant adaptation approaches, as outlined in this article, can help researchers and clinicians identify and understand common factors that should be considered during adaptation for telehealth-delivery. We propose that these common factors will include a combination of malleable inner contextual factors (such as organization leadership) and outer contextual factors that cannot be easily influenced (such as the digital divide). Identifying and focusing on malleable factors early in the adaptation timeline can streamline the process, making it more efficient and cost-effective.
Study limitations
We acknowledge various limitations of the study. Data sources were study documents (meeting notes and summary documents) that were analysed retrospectively. We recognize that some aspects of the ‘what’ and ‘why’ might not have been captured in the available data. However, to ensure that our results were as accurate as possible, we presented preliminary findings to team members who were part of the adaptation process during a structured member-checking process. Team feedback was integrated in the final version of results. Furthermore, while the EPIS framework was found useful for the purpose of this study, we recognize that other frameworks might have been equally or more suited. However, the EPIS is one of the most widely used frameworks in the public sector, and one of the few frameworks that have evidence in low-resource settings (Moullin et al., 2019), hence our of choice here. Furthermore, we recognize that adaptations 5 and 6 (adaptation of ECD training and supervision for online delivery) were designed for ECD practitioners who had received prior training and supervision in the in-person intervention. However, the online training presented in this article is generalizable, but it will be necessary to include additional didactic sessions (from the in-person training) on topics such as a general introduction to caregiver coaching, C-ESDM concepts and sessions structure. As a result, the training with ECD practitioners will be longer than the training described in this article.
Finally, we recognize that adaptations were done under unusual circumstances (global pandemic) and time pressure that could have impacted both the ‘what’ and the ‘why’ of our adaptations. However, the unavoidable natural experiment of COVID-19 has inadvertently forced us (and many other research teams around the globe) to be responsive and innovative within our contextual restraints to deliver interventions to families. We therefore believe that some of the adaptations and their reasons may provide a useful guide for future technology-informed autism interventions.
Conclusion
In this article, we describe 10 adaptations (the ‘what’) and their reasons (the ‘why’) of a telehealth-delivered early autism intervention. We hope that these findings can serve as a model for documenting contextual adaptation of other technology-supported interventions. Given the growing interest in the use of technology to support autism service delivery, it will be important to understand the acceptability and feasibility of telehealth-delivered sessions from the perspective of caregivers who attended sessions and practitioners involved in delivery. An additional next step will be to determine coaching fidelity as an implementation outcome. It will also be important to establish whether these telehealth-delivered sessions result in change in caregiver and child behaviours of interest, and whether home-recorded caregiver–child interaction videos made on entry-level smartphones can be used to detect intervention impact (Ndlovu, 2024).
Supplemental Material
sj-xlsx-1-aut-10.1177_13623613241300774 – Supplemental material for Adapting an early autism caregiver coaching intervention for telehealth delivery in low-resource settings: A South African study of the ‘what’ and the ‘why’
Supplemental material, sj-xlsx-1-aut-10.1177_13623613241300774 for Adapting an early autism caregiver coaching intervention for telehealth delivery in low-resource settings: A South African study of the ‘what’ and the ‘why’ by Marisa Viljoen, Noleen Seris, Nokuthula Shabalala, Minkateko Ndlovu, Petrus J de Vries and Lauren Franz in Autism
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Institutes of Mental Health (K01 MH104370; R21 MH120696; R01 MH127573).
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.