
Abstract
In autistic adults, measurement tools may not adequately differentiate between autistic characteristics and features of anxiety. This may be particularly evident in the case of social anxiety disorder; however, few measures of social anxiety disorder have been validated for autistic adults. Instead, assessments are often made using measures designed and validated for non-autistic adults. To address this, we examined the suitability of the self-report Severity Measure for Social Anxiety Disorder in 284 autistic adults. We evaluated its psychometric properties, explored a rescored version that aimed to account for autistic differences in reporting and conducted content analysis on qualitative feedback from autistic participants. Confirmatory Factor Analysis did not confirm the unidimensional structure of the Severity Measure for Social Anxiety Disorder for autistic adults and over half attributed at least one response to a factor other than social anxiety (e.g. fatigue). Exploratory Factor Analysis of a rescored version of the Severity Measure for Social Anxiety Disorder based on autistic adults’ responses to reflect those just due to social anxiety, revealed that a two-factor solution was most appropriate, again suggesting social anxiety was not a solitary latent variable. Our findings recommend caution be applied when using the Severity Measure for Social Anxiety Disorder with autistic adults and our content analysis may inform more precise future measurement.
Lay abstract
Mental health measures used with autistic adults are often only evaluated for use with non-autistic adults, which may cause inaccurate measurement. This is important when measuring social anxiety disorder as some features overlap with social characteristics of autism. This study evaluated one self-report questionnaire measure of social anxiety disorder, the Severity Measure for Social Anxiety Disorder. The Severity Measure for Social Anxiety Disorder is based upon criteria for diagnosis of social anxiety disorder, and we aimed to understand its suitability for autistic adults. The Severity Measure for Social Anxiety Disorder was completed by 284 autistic adults and 80 non-autistic adults who were then asked five follow-up questions about ambiguous questions on the Severity Measure for Social Anxiety Disorder. We found that over half our sample of autistic adults, on at least one question, attributed their answer to something other than anxiety. Furthermore, in autistic adults, one underlying construct of social anxiety did not link their answers on the Severity Measure for Social Anxiety Disorder together, suggesting the Severity Measure for Social Anxiety Disorder might not be suited to capturing social anxiety disorder in autistic adults. To improve measurement, we rescored answers where participants said their response was due to something other than social anxiety, however, the rescored Severity Measure for Social Anxiety Disorder did not only capture social anxiety in autistic adults either. Finally, we analysed the reasons other than social anxiety autistic adults said influenced their answers. We grouped their responses into 10 categories, for example, ‘fatigue’, ‘sensory overwhelm’, and ‘masking’. Overall, our findings suggest caution when using the Severity Measure for Social Anxiety Disorder with autistic adults, and the categories identified may suggest how to measure social anxiety more accurately in autistic adults.
Compared to the non-autistic population, autistic 1 people are more likely to experience anxiety related to social situations (Hollocks et al., 2019; van Steensel et al., 2011), broadly termed social anxiety, with some estimates suggesting that over half experience elevated symptoms of social anxiety during adulthood (Bejerot et al., 2014; Maddox & White, 2015; Spain et al., 2016). However, the prevalence of social anxiety symptoms in autistic adults varies greatly between studies (Hollocks et al., 2019).
The variability in the detection of social anxiety disorder (SAD) among autistic adults is complicated by two main reasons. First, in the general population, key models implicate specific cognitive and behavioural processes that underpin the development and maintenance of SAD (see Clark & Wells, 1995; Heimberg et al., 2010 for additional detail). Whether these general models of SAD (e.g. Clark & Wells, 1995) adequately explain the autistic experience of SAD remains unknown, particularly when accounting for differences in information and sensory processing (Rodgers & Ofield, 2018; Stark et al., 2021). Second, there can be high degrees of overlap between autistic characteristics and features of social anxiety (see Spain et al., 2018 for review), and differentiating between those characteristics associated with autism and social anxiety can be difficult. For example, some behavioural expressions commonly interpreted as anxiety in non-autistic individuals may serve a qualitatively different purpose for an autistic person–an autistic adult might withdraw from a social situation not due to fear of negative evaluation, but instead due to being overwhelmed by the sensory demands of the social environment. If the individual’s autistic characteristics are not considered, such social avoidance may easily be misinterpreted as indicative of SAD.
Our focus herein is specifically on the latter; that current measurement tools may not adequately delineate between social anxiety or autistic-specific experiences in autistic adults. To our knowledge, few studies have tackled this issue and there exists only one autism-specific measure of anxiety for adults, the Anxiety Scale for Autism-Adults (ASA-A) (Rodgers et al., 2020), which – although it includes a social anxiety subscale – is designed to measure anxiety symptomatology broadly and therefore may not be sufficiently comprehensive for the assessment of SAD. Given the lack of appropriate assessment tools, clinicians and researchers to date have largely relied on psychometric instruments designed for the non-autistic population, which may not account for phenotypic similarities between some autistic features and behavioural characteristics of SAD (Brugha et al., 2015; South & Rodgers, 2017).
In recent work, there have been attempts to explicate these phenotypic similarities and more accurately differentiate autistic characteristics from social anxiety symptoms. Chew et al. (2021) sought to disentangle autistic adults’ symptoms of social anxiety, as measured by the Social Anxiety Questionnaire (SAQ; Caballo et al., 2010), from ‘autism-related experiences’. Four qualified and experienced autistic consultants identified 5 (out of 30) SAQ items as potentially ambiguous – that is, the items could be interpreted idiosyncratically to reflect autistic experiences, rather than the intended social anxiety-related interpretation. The consultants and study authors developed clarified alternatives for the five ambiguous items, with clarified items designed to assess either social anxiety or autism-related experiences. Participants completed the original SAQ, then the modified scale including clarified items. While no significant difference was found between original SAQ and clarified SAQ total scores, it is worth noting that item-level differences were identified for several of the clarified items. The study authors suggested that the original SAQ is sufficiently clear and valid for assessing social anxiety in autistic adults; however, participants were not directly asked about their interpretation of the questionnaire items, therefore ambiguities may remain. In addition, findings regarding the SAQ cannot be extrapolated to other measures, and it is possible that alternative screening measures for social anxiety may contain even greater ambiguity.
In a second relevant study, Boulton and Guastella (2021) examined the psychometric properties of four social anxiety questionairres in autistic adolescents and adults aged 15–46 years: the Liebowitz Social Anxiety Scale-Self-Report (LSAS; Heimberg et al., 1999); the Social Interaction Anxiety Scale; the Social Phobia Scale (SIAS and SPS; Mattick & Clarke, 1998); and the Brief Fear of Negative Evaluation Scale (Leary, 1983). Results demonstrated a strong correlation between all summary scores; however, the authors noted that their sample size of 102 autistic adults was not sufficient for factor analyses and therefore could not investigate whether factor structures were similar between non-autistic and autistic adults (Boulton & Guastella, 2021). Furthermore, no qualitative data were captured regarding the autistic participants’ interpretation of the items. Thus, the underlying construct identified of SAD may have been partly due to measuring autism-related experiences, rather than symptoms of SAD. Qualitative data may be particularly helpful in understanding measurement of social anxiety in autistic adults – with one study suggesting that social anxiety can develop in part due to environmental cues that are non-social (Spain et al., 2020).
To effectively understand and treat SAD in autistic adults, accurate assessment of anxiety symptomatology is crucial. As stated above, few studies have evaluated the use of SAD-specific measures with autistic adults. We selected the SAD-D as it is closely based upon DSM-5 (American Psychiatric Association, 2013) social anxiety criteria, aiming to evaluate its suitability for autistic adults in four steps. First, we evaluated the factor structure and internal consistency of the SAD-D (LeBeau et al., 2016) to determine whether this is a valid measure of autistic adults’ symptoms of social anxiety. Second, we examined whether autistic adults attributed their SAD-D responses to factors consistent with SAD or other, non-social anxiety-related factors. Third, we investigated whether rescoring the SAD-D to reflect only those responses that participants attributed to social-anxiety-relevant factors (Rescored SAD-D, R-SAD-D) would improve the measure’s psychometric properties. Finally, we sought to understand in greater detail the non-social anxiety-related reasons to which participants attributed SAD-D responses. We hypothesised that 1) using standard scoring, the SAD-D would not be a reliable and valid measure of autistic adults’ social anxiety; 2) at least some participants would attribute SAD-D responses to factors unrelated to social anxiety; and 3) rescoring the SAD-D to reflect only social-anxiety-relevant responses would result in improved psychometric performance. Our final aim was exploratory; we did not have a corresponding specific hypothesis.
Method
Participants
Participants were drawn from 404 autistic and non-autistic adults in the Australian Longitudinal Study of Autism in Adulthood (ALSAA, Arnold et al., 2019). The sample was drawn prior to the completion of wave two recruitment and data collection and thus does not represent the entire ALSAA cohort. Participants were recruited via a range of methods as described in Arnold et al. (2019) with the addition of social media-based snowball sampling in wave two. They self-reported their clinical diagnoses (e.g. ‘autism spectrum disorder’), corroborated through the Autism Quotient – Short (AQ-S; Hoekstra et al., 2011), and completed a range of questionnaire measures (see Arnold et al., 2019 for details). Here, we focus on 287 autistic adults (age range = 25 – 83 years; M age = 43.64 years, SD = 11.86) and 80 non-autistic adults (age range = 25–80 years; M age = 45.53 years, SD = 14.19) who responded specifically about their symptoms of SAD (see Table 1). Autistic participants were included if they self-reported either a formal (a formally recognised diagnosis from a health professional) or self-informed diagnosis (self-identifying as being autistic without a formal diagnosis) of autism. In both cases self-reports were corroborated through the Autism Quotient – Short (AQ-S; Hoekstra et al., 2011). We opted to include those with a self-informed diagnosis because they represented only a small subset of the total sample (12%), and because previous research has highlighted those with a self-informed diagnosis share similar experiences to those with a formal diagnosis (McDonald, 2020). Three autistic participants were excluded as they did not report a formal diagnosis of autism and scored ⩽ 65 on the AQ-S (Hoekstra et al., 2011). Thus, the final sample included 284 autistic adults (Table 1). The 80 non-autistic participants were drawn from a general community sample (Arnold et al., 2019) and self-reported no diagnosis of autism (Table 1).
Participant characteristics.

Data are mean (SD; range) or N (%).
Notes. NA = not applicable, AQ = Autism Quotient.
Participants could select all options that applied to them. Percentages therefore do not add to 100. b Questions about gender were developed based on the Williams Institute best practice guidelines (The GenIUSS Group, 2014). cResponses refer to self-reported current co-occurring diagnosed conditions; we acknowledge that these terms do not reflect current best practice. Gender response options have been updated for subsequent ALSAA data collection waves.
Measures
The 10-item severity measure for social anxiety disorder (social phobia) (SAD-D) —adult (LeBeau et al., 2012)
The SAD-D is a self-report scale measuring the severity of social anxiety symptoms in individuals aged 18 years and older (Craske et al., 2013). It comprises 10 items, with each item rated on a 5-point scale (0 = Never to 4 = All of the time). Higher scores indicate more severe anxiety symptoms, and total scores range from 0 to 40. Items ask about thoughts, feelings, and behaviours regarding social situations; for example, ‘avoided, or did not approach or enter, social situations’. The SAD-D is directly based on DSM-5 conceptualisations of SAD and has been validated in non-autistic samples (e.g. Binasis et al., 2022; DeSousa et al., 2017; Möller & Bögels, 2016). In a community sample of Australian adults, the SAD-D has been found to have excellent internal consistency (⍺ = .95) (Rice et al., 2021). In this study, the SAD-D showed excellent internal consistency among autistic (⍺ = .92) and non-autistic adults (⍺ = .94).
Mini-social phobia inventory (Mini-SPIN) (Connor et al., 2001)
This 3-item measure is adapted from the 17-item Social Phobia Inventory (Connor et al., 2000) and is used as a screening assessment for generalised SAD (Connor et al., 2001). Adults rate on a 5-point scale how much a statement applied to them over the past week (1 = not at all to 5 = extremely), with a maximum total score of 15. The Mini-SPIN has been found to have good internal consistency in a representative community sample of German adults (⍺ = .80) (Wiltink et al., 2017). In this study, the scale showed good internal consistency among autistic (⍺ = .81) and non-autistic adults (⍺ = .86). This measure was included in this study to measure convergent validity.
Follow-up 6-item disambiguation severity measure for social anxiety disorder (social phobia) – adult (FUD-SAD-D)
Research advisors were sent a copy of the ALSAA survey, which included the SAD-D, FUD-SAD-D, and Mini-SPIN, and were asked to provide feedback on interpretability and accessibility of all the items for autistic participants. All assessment tools and questions used in the ALSAA survey were reviewed by at least two autistic members of the ALSAA Research Advisory Network. Prior to the review by the Research Advisory Network, five items on the SAD-D (questions 6–10) and one on the Mini-SPIN (question 2) were selected for the follow-up questionnaire (FUD-SAD-D, see Supplementary information). These questions were chosen as they targeted behaviours that may not be specific to social anxiety, whereas the remaining Mini-SPIN and SAD-D questions focus on cognitive and physiological signs of social anxiety, which are less open to idiosyncratic interpretation. The FUD-SAD-D disambiguation questions asked participants to indicate whether their SAD-D and mini-SPIN responses were indicative of anxiety or better attributed to other factors. Each disambiguation question asked ‘In the past 7 days, if you did any of the following, was this due to fear or anxiety about the social situation or was there another reason? Did you. . .’, followed by each relevant SAD-D and mini-SPIN item (e.g. ‘distract yourself to avoid thinking about social situations?’). No changes were made to the wording of the items on the original SAD-D and mini-SPIN, but only to the response options. Three response options were provided: ‘No, I did not’; ‘Yes, due to fear or anxiety’; and ‘Yes, other reason’ (see Supplementary Material for a copy of the questionnaire). If participants selected the ‘Yes, other reason’ response option, they were prompted to provide a brief free-text description of the factor/s that influenced their response. Disambiguation questions were presented immediately after the Mini-SPIN and SAD-D.
The Warwick Edinburgh mental wellbeing scale (WEMWBS) (Tennant et al., 2007)
This 14-item scale was developed as a measure of mental wellbeing. Adults rate on a 5-point scale statements about their thoughts and feelings that best describe their experience over the past two weeks. Specifically, the frequency in which they have been experiencing these thoughts and feelings (e.g. ‘I’ve been feeling optimistic about the future’.) (1 = none of the time to 5 = all the time), with a maximum total score of 70, where higher scores indicate greater mental wellbeing. In a general population sample, it showed excellent internal consistency (⍺ = .91) (Tennant et al., 2007). In this study, the WEMWBS displayed excellent internal consistency in autistic (⍺ = .93) and non-autistic (⍺ = .95) adults. This measure was included in this study in order to measure divergent validity.
The autism spectrum quotient (AQ-short) (Hoekstra et al., 2011)
This is a 28-item measure of autistic traits adapted from the original 50-item Autism Spectrum Quotient (AQ) (Baron-Cohen et al., 2001). For each item, adults are asked to rate a descriptive statement assessing a personal preference or habit on a 4-point scale (1 = definitely agree, 2 = slightly agree, 3 = slightly disagree, 4 = definitely disagree; see Table 1 for summary). The AQ-Short has previously shown good internal consistency among autistic (⍺ = .86) and non-autistic adults (⍺ = .86) (Hoekstra et al., 2011). In this study, the AQ-Short was also found to have good internal consistency in autistic (⍺ = .83) and non-autistic adults (⍺ = .87).
Procedure
All data were collected between November 2017 and March 2020. The Human Research Ethics Committee at the University of New South Wales approved the study (approval number HC150001). Data were collected using Qualtrics online survey software, with a pen and paper option also available. All participants were required to provide informed consent via the survey platform prior to their participation; see Arnold et al. (2019) for more detail regarding ALSAA study procedures.
Community involvement
Autistic adults and family members contributed to the design of ALSAA determining priority content areas (Arnold et al., 2019). Autistic research advisors reviewed all assessment tools used in the ALSAA for accessibility for autistic respondents, including the social anxiety follow-up items. Non-autistic researchers (SA, MB, LL & SB) and an autistic researcher (JdH) were actively involved in the analysis, interpretation, and writeup of the results.
Data analyses
Development of the rescored SAD-D (R-SAD-D)
To create the R-SAD-D, we used each participant’s five FUD-SAD-D responses that corresponded to the 5 items on the SAD-D. Participants were prompted to provide free-text responses to the FUD-SAD-D only if they indicated that their SAD-D responses were attributable to factors other than social anxiety, however, preliminary screening revealed that some free-text responses described social-anxiety-related factors. To ensure accurate rescoring of SAD-D responses, all FUD-SAD-D free-text responses were analysed and coded to a binary: ‘social anxiety’ or ‘not social anxiety’. Coding was conducted independently by SB (non-autistic psychology PhD scholar) and JdH (registered psychologist and autistic academic), with analysis informed by their training in psychology and JdH’s relevant positioning as an autistic researcher. When participants provided a free-text response, they had explicitly ticked that the reason for their response was not related to social anxiety (see Supplementary Material), therefore, the coders adopted a restrained approach, with free-text responses only considered to describe social-anxiety-related factors when the response explicitly referred to social ‘anxiety’, ‘worries’, or similar constructs. Moreover, ambiguous free-text responses were coded as ‘not social anxiety’, deferring to participants’ original multiple-choice response. Coders achieved 90% agreement with consensus reached via discussion.
Next, we screened each participant’s responses to the relevant SAD-D items (questions 6–10). For each SAD-D item a participant endorsed (i.e. item-level scores > 0), we checked their corresponding FUD-SAD-D response. If the participant had selected ‘other reason’ on the FUD-SAD-D and their free-text response was coded as ‘not social anxiety’, their score for the relevant SAD-D item was rescored to zero. If the participant had selected any other response on the FUD-SAD-D, or if they had selected ‘other reason’ but their free-text response was coded as indicating social anxiety, their score for the relevant SAD-D item was left unchanged. Rescored SAD-D items 6–10 were then combined with original scores for items 1–5 to create the ‘R-SAD-D’, a 10-item measure of social anxiety symptoms designed to take into account differences in reporting of ambiguous ‘social anxiety related’ behaviours by autistic adults. For all quantitative analyses see https://osf.io/gpce7/?view_only=2fa8bfb20ba1400fa073eadd49c245b7 for analysis scripts.
Confirmatory factor analyses
We conducted confirmatory factor analyses (CFA) in ‘R’ version 4.1.1 using the lavaan package (Rosseel, 2012). In accordance with previous studies (Beesdo-Baum et al., 2012) and to allow for direct comparisons to be made, polychoric correlations and Weighted Least Square Means and Variance Adjustment estimation methods (WLSMV) were used to account for the ordinal structure of the Likert-type scale data. With a sample size of 5–10 participants per item considered appropriate (Floyd & Widaman, 1995), sample sizes in both the non-autistic and autistic groups were sufficient to conduct CFAs. Fit indices including Chi-square, root mean square error of approximation (RMSEA; < .08), Comparative Fit Index (CFI; > .90), Tucker–Lewis Index (TLI; > .90), standardised root mean square residual (SRMR; <.08) and Goodness of Fit Index (GFI; > .90) were used to estimate model fit.
To examine the structure of the SAD-D, all 10 items were entered into a CFA with one latent variable, defined as ‘Social Anxiety’. Missing data were removed by listwise deletion.
Exploratory factor analysis
To explore whether the R-SAD-D was a suitable measure of social anxiety for autistic adults, we conducted an Exploratory Factor Analysis (EFA) in ‘R’ using the packages psych (Revelle, 2022) and nFactors (Raiche, 2010). Kaiser–Meyer–Oklin (KMO) factor adequacy test and Bartlett’s test of sphericity were first conducted to confirm that the R-SAD-D in the autistic sample was suitable for an EFA. A KMO value of 0.6 or greater is recommended (Bartlett, 1954; Kaiser, 1970; Kaiser, 1974) and assumptions of multi-collinearity were confirmed via examination of the correlation matrix. The Eigenvalue method, scree plot and parallel analysis were used to determine the number of factors to be retained in the EFA.
Convergent and divergent validity
To explore convergent validity, we calculated Pearson-moment correlations between SAD-D/R-SAD-D and mini-SPIN total scores. For divergent validity, we calculated Pearson-moment correlations between SAD-D and WEMWBS total scores.
Content analysis
To explore in more depth the non-social-anxiety-related factors autistic participants described in FUD-SAD-D free-text responses, conventional quantitative content analysis (Hsieh & Shannon, 2005) following Bengtsson’s (2016) four-stage method was used to identify recurring factors. We analysed data at the manifest level, focusing on participants’ own words rather than seeking deeper interpretation of latent meaning. Our analysis was inductive, with meaning units and codes derived from the data rather than a pre-existing framework.
Researchers SB and JdH familiarised themselves with the data and developed meaning units and codes (decontextualization). They reviewed the meaning units and text in relation to the aim (recontextualization) through discussion with the wider research team (SA, MB, LL), then condensed meaning units into categories (categorisation) and compiled the results (compilation). SB coded all free-text responses against the final categories and SA independently coded a proportion of free-text responses against the final categories. Inter-rater reliability was good, with 93% agreement between the researchers.
Responses with insufficient detail for coding and those that did not fall within the coding structure are not reported here.
Results
Profile of scores
Scores for the SAD-D, Mini-SPIN, and WEMBS are shown in the descriptive statistics in Table 2.
Descriptive statistics.
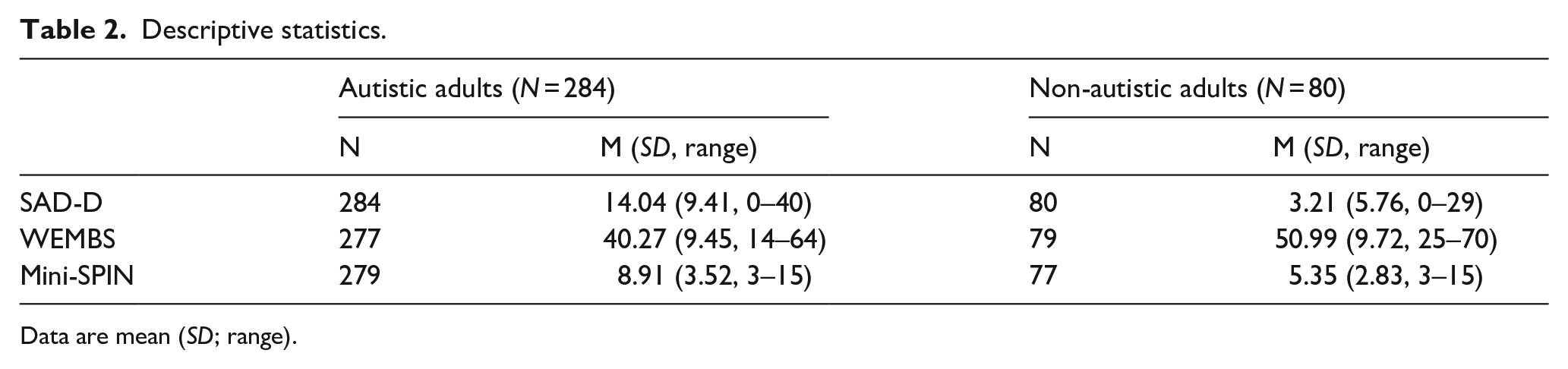
Data are mean (SD; range).
Of the 284 autistic adults who completed the SAD-D, 146 (51%) provided 417 free-text responses to the FUD-SAD-D. Of these, 376 (90%) responses were coded as unrelated to social anxiety, with corresponding SAD-D item scores recoded to zero forming the R-SAD-D. Sixteen free-text responses were coded as indicating both social-anxiety-related and unrelated factors, with an additional 25 responses coded as social anxiety related; corresponding SAD-D scores were left unchanged for these 41 items. Of the 80 non-autistic adults, 14 (17.5%) provided 45 free-text responses to the FUD-SAD-D; all 45 (100%) were coded as unrelated to social anxiety, thus corresponding SAD-D item scores were recoded to zero forming the R-SAD-D.
The SAD-D and R-SAD-D data distributions for both autistic and non-autistic adults were significantly non-normal (autistic SAD-D W = .96, p < .001; autistic R-SAD-D W = .94, p < .001; non-autistic SAD-D W = .60, p < .001; and non-autistic R-SAD-D W = .55, p < .001) according to Shapiro-Wilk tests. The median score on the SAD-D in the autistic adult group was 13 (interquartile range [IQR] = 12.2), whereas the median in the non-autistic group was 1 (IQR = 3). The median score on the R-SAD-D for autistic adults was 10 (IQR = 14), and for non-autistic adults was .5 (IQR = 3). Wilcoxon rank sum tests showed that scores in the autistic group were significantly higher than the non-autistic group on the SAD-D (W = 19766, p < .001, effect size r = .53) and R-SAD-D (W = 19156, p < .001, effect size r = .49). A Wilcoxon signed-rank test showed a significant difference between SAD-D and R-SAD-D scores in the autistic group, such that the recoded average total scores were significantly lower (W = 9453, p < .001, effect size r = .68). R-SAD-D scores for the non-autistic group were significantly lower than SAD-D scores, but with a very small effect size (W = 105, p < .001, effect size r = .06). See Table 3 for summary frequencies of the severity ratings for all participants on both the SAD-D and R-SAD-D.
Frequencies of severity rating on SAD-D and the R-SAD-D.
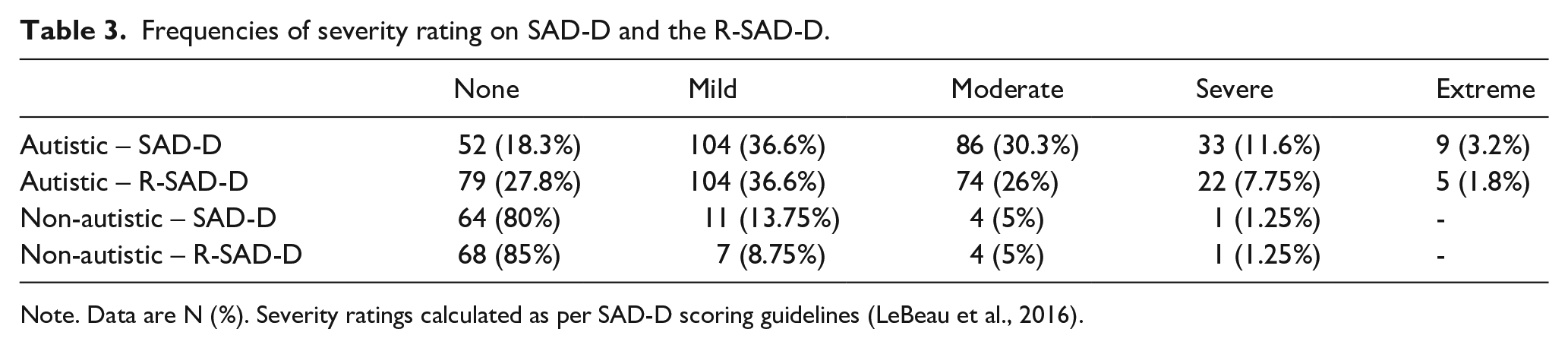
Note. Data are N (%). Severity ratings calculated as per SAD-D scoring guidelines (LeBeau et al., 2016).
Confirmatory factor analyses (SAD-D)
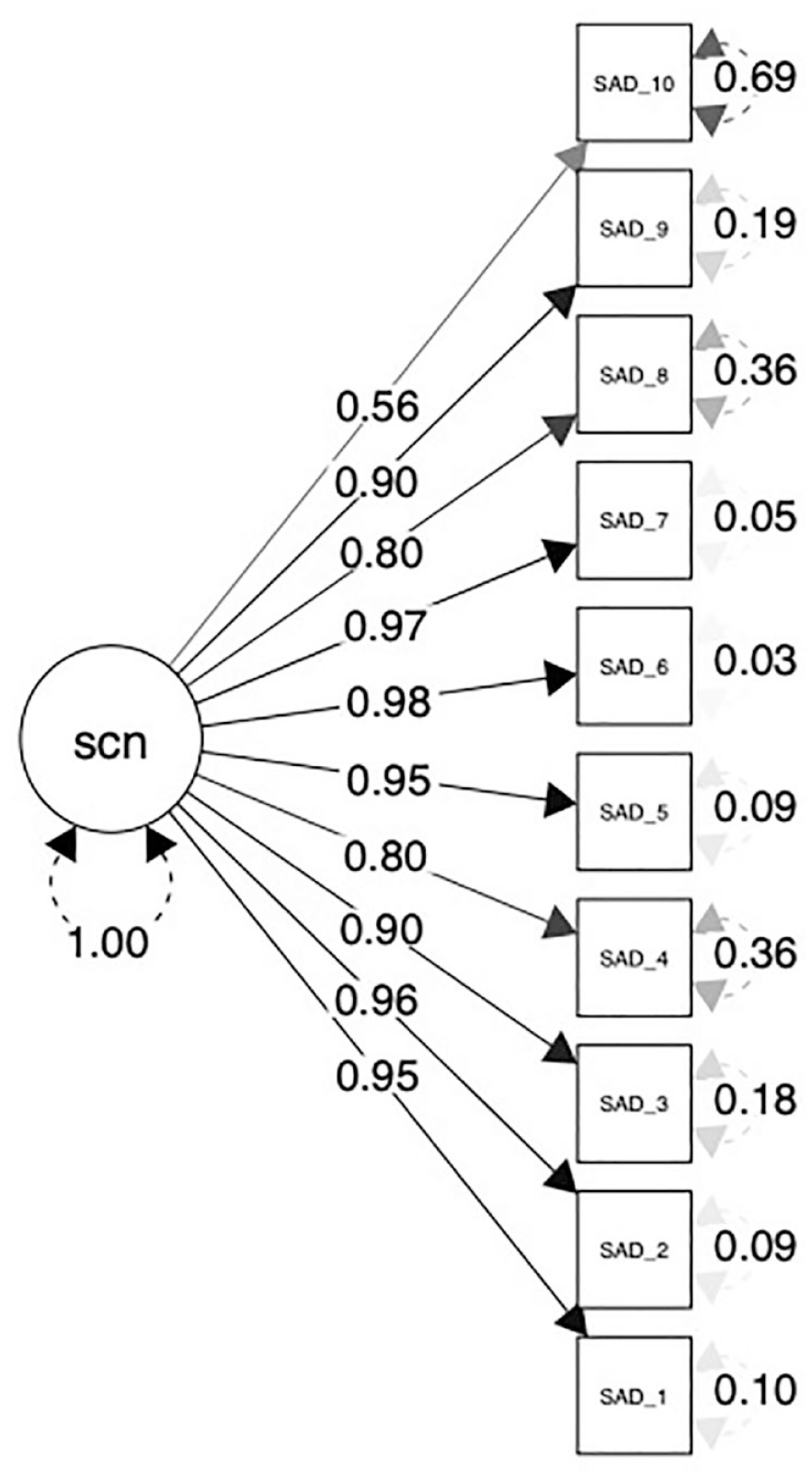
In the autistic sample, the one-factor solution only partially met guidelines for good fit (Figure 1 and Table 4), thereby failing to confirm the unidimensionality of the SAD-D for autistic adults. For the non-autistic sample, the one-factor solution met good fit guidelines (Figure 2 and Table 4) confirming the unidimensionality of the SAD-D for non-autistic adults.
Final model fit indices for autistic (n = 284) and non-autistic (n = 80) participants.
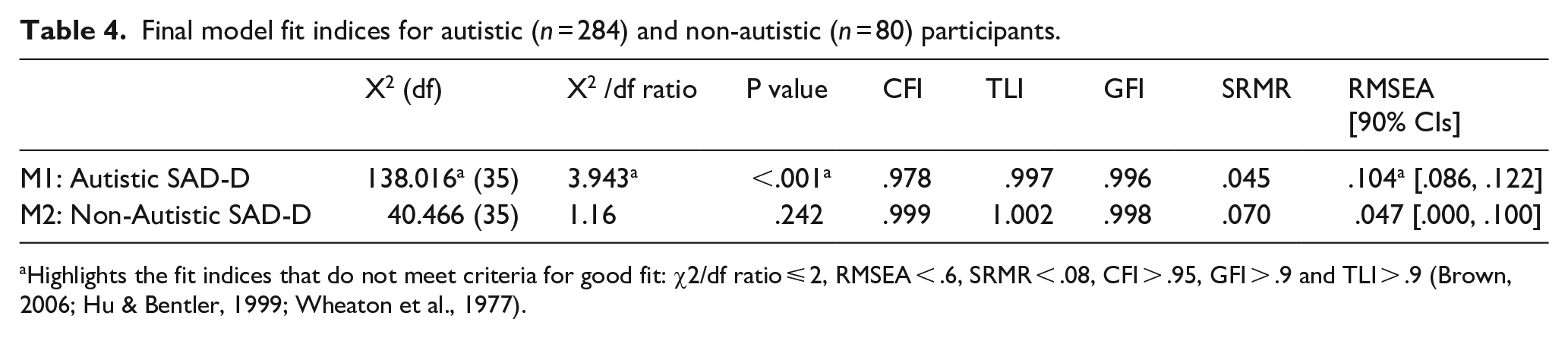
Highlights the fit indices that do not meet criteria for good fit: χ2/df ratio ⩽ 2, RMSEA < .6, SRMR < .08, CFI > .95, GFI > .9 and TLI > .9 (Brown, 2006; Hu & Bentler, 1999; Wheaton et al., 1977).
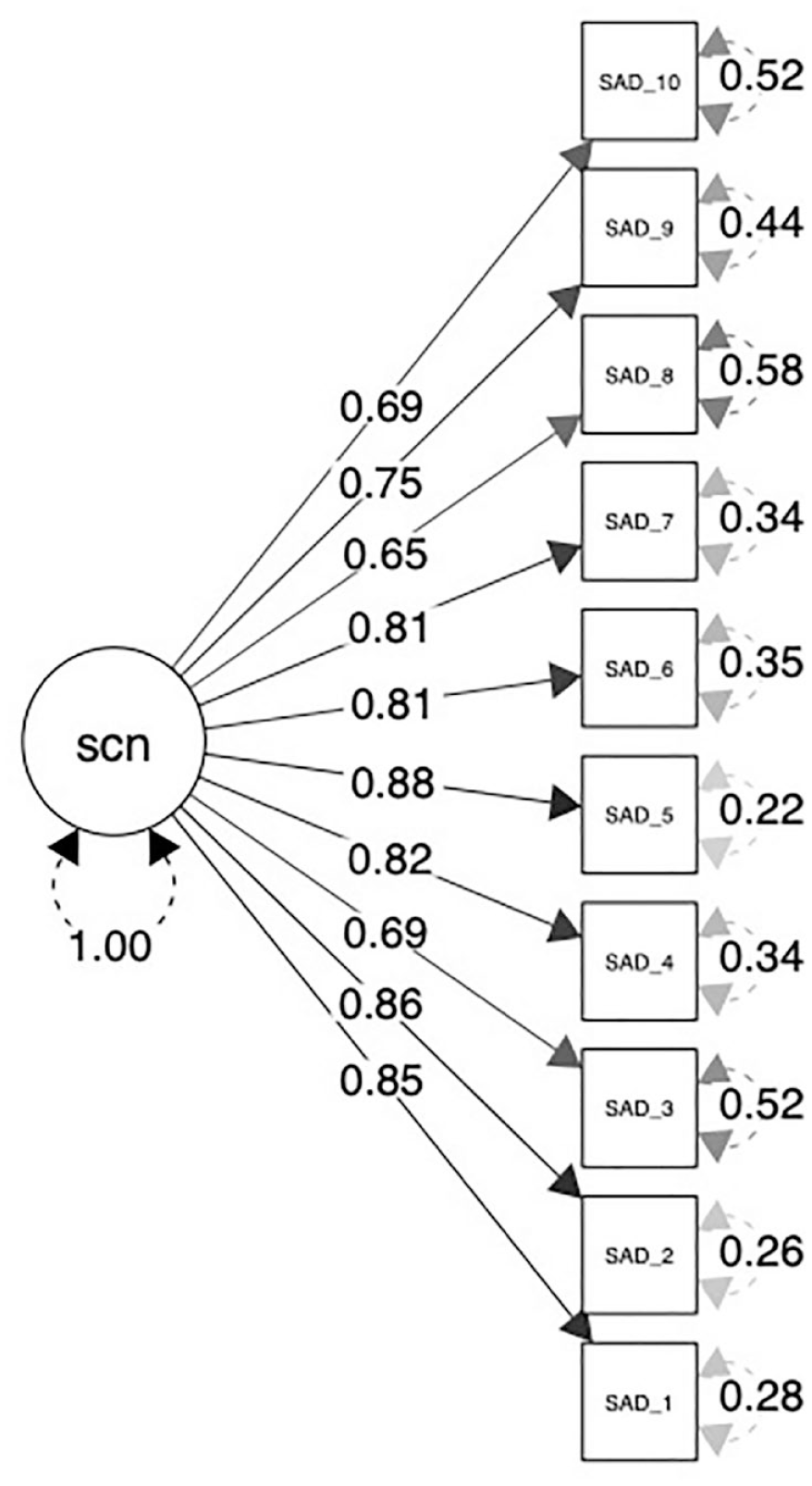
Model 1 (M1) the factor loadings for the autistic SAD-D data.
Model 2 (M2) the factor loadings for the non-autistic SAD-D data.
Exploratory factor analysis (R-SAD-D)
R-SAD-D scores for the non-autistic group were significantly lower than original scores, but with a small effect size; thus, EFA was conducted on R-SAD-D data for the autistic group only. The KMO factor adequacy test value (0.91) and Bartlett’s test (X2 (45) = 1455.40, p < .01) met criteria to indicate that the data were suitable for EFA and examination of the correlation matrix showed that all items were correlated with one another p < .001, r > .3, confirming assumptions of multi-collinearity. The EFA, estimated with Promax rotation due to the correlation between components, identified a two-factor solution in the autistic sample. A test of the hypothesis that two factors are sufficient also demonstrated significance (X2 (26) = 53.99, p < .01). Factor 1 explained 32% of the variance and factor 2 explained 23% of the variance (see factor loadings in Table 5). Internal consistency for both factors was good (Factor 1 = .89, Factor 2 = .82).
Factor loadings for R-SAD-D (autistic group).

Note. Bold indicates item included in factor.
Convergent and divergent validity
Mini-SPIN total scores and SAD-D total scores were positively correlated in both the autistic (r = .57, p < .01) and non-autistic (r = .64, p < .01) samples, suggesting convergent validity between these measures in both autistic and non-autistic adults. WEMWBS total scores and SAD-D total scores were negatively correlated in both autistic (r = –.49, p < .01) and non-autistic adults (r = –.59, p < .01), suggesting divergent validity between these measures in both groups. There was also a positive correlation between the Mini-SPIN total score and the R-SAD-D total scores for the autistic participants (r = .60, p < .01).
Content analysis
Through content analysis of autistic adults’ FUD-SAD-D responses, we generated 10 codes to describe factors influencing non-anxiety-related SAD-D and Mini-SPIN item endorsements (Table 6).
Content analysis of autistic adults’ 377 responses coded as ‘not social anxiety related’.
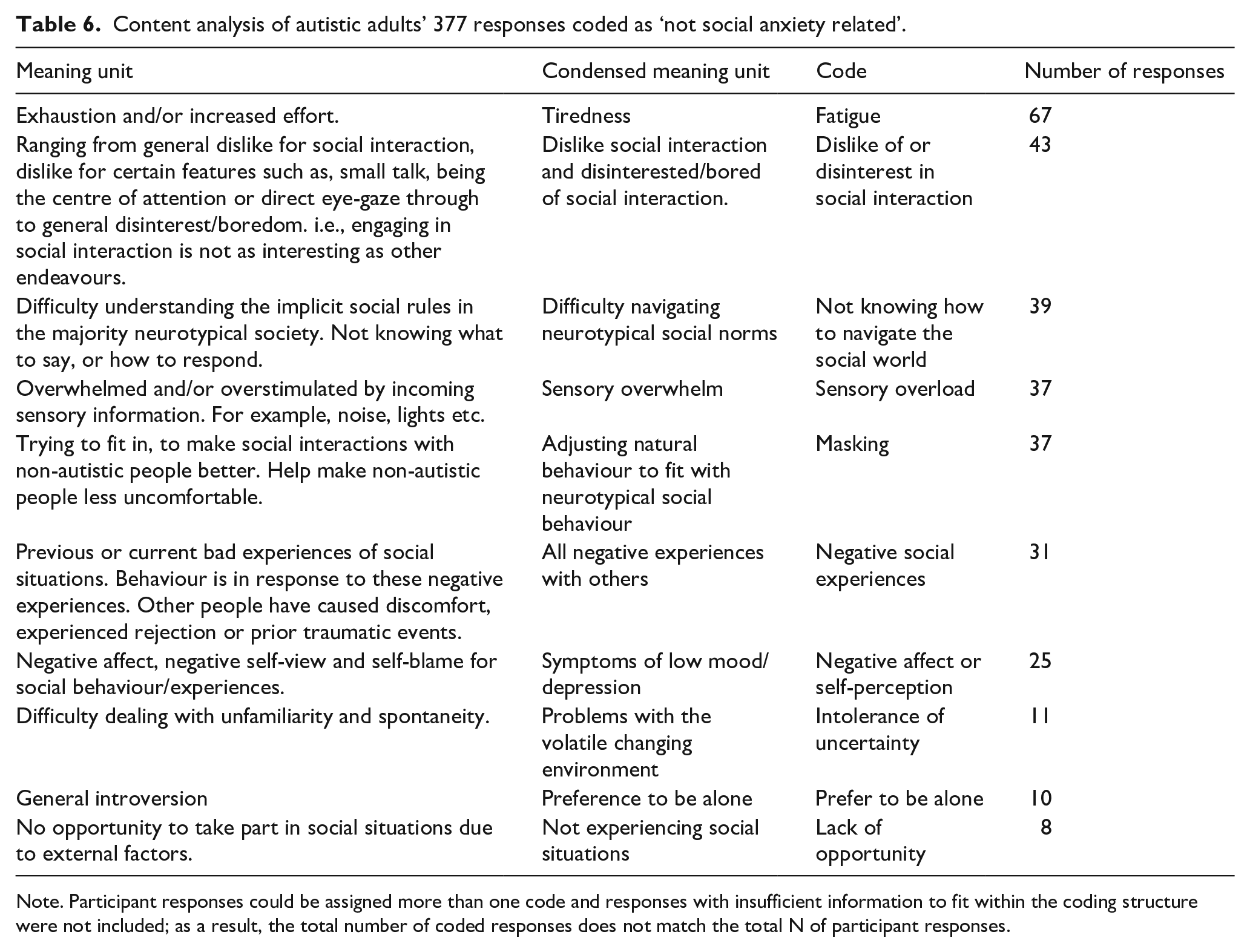
Note. Participant responses could be assigned more than one code and responses with insufficient information to fit within the coding structure were not included; as a result, the total number of coded responses does not match the total N of participant responses.
Fatigue was the most commonly occurring code, with 67 responses. Autistic adults reported feeling ‘exhausted’ (272-AUT) by social situations, stating that ‘dealing with people is hard work and tiring’ (45-AUT). One participant summarised ‘I find social situations extremely fatiguing, this is not strictly the same as having anxiety related to them. I have confidence that I can cope but to do so draws greatly on physical and emotional reserves’ (145-AUT). Of the 67 responses within this code, 24 related to FUD-SAD-D question two ‘avoid, or not approach or enter, social situations?’ and 21 to question three ‘leave social situations early or participate only minimally (e.g. said little, avoided eye contact)’, linking fatigue with avoidance behaviour.
Forty-three responses indicated that item endorsement was due to dislike of or disinterest in social interaction, with some participants stating generally ‘I don’t like socialising’ (60-AUT), and others identifying specific dislikes about aspects of social interaction, for example, ‘[ I ] dislike small talk’ (233-AUT). Participants also reported a more general lack of interest, ‘I don’t have an interest in pretending to be friends with people when I am not’ (55-AUT) and ‘it is just boring’ (93-AUT). ‘People do not like talking about the things I am interested in, but they do like talking about things I do not care about e.g. fashion and who said what about someone else’ (213-AUT).
Thirty-nine responses described not knowing how to navigate the social world. Some autistic adults described these difficulties in general terms, ‘I do not understand social situations; no idea of what others are doing or what I should be doing. Complete confusion’ (227-AUT), while others identified specific difficulties within social situations, ‘unsure how to end conversation or leave situation’ (80-AUT); ‘It is hard to join in fast conversation with several communication partners so I cannot say what I want without interrupting. I get fed up and leave if I can’ (213-AUT). Responses within this code primarily related to FUD-SAD-D question 3 (Responses = 12) and question 4 ‘spend a lot of time preparing what to say or how to act in social situations’ (Responses = 10).
Thirty-seven responses were coded as describing sensory overwhelm. Social situations were frequently described as being ‘overwhelming, [with] too much noise, lights, movements’ (90-AUT). This did not necessarily result in complete avoidance of social situations, but impacted participants when they did take part in social situations, ‘sometimes part way through I will start to experience sensory overload’ (216-AUT). Most commonly, sensory overwhelm was reported in relation to FUD-SAD-D question 2 (Responses = 9) and question 3 (Responses = 16).
The next most commonly occurring code was masking, with 37 participants describing efforts to camouflage autistic traits in social situations. Autistic participants reported needing ‘to wear a mask’ (114-AUT) and ‘attempting to improve social interactions’ (8-AUT) in order to ‘not be rejected’ (86-AUT). Twenty-seven responses within this code related to FUD-SAD-D question 4, with participants reporting that they prepare for social interactions because they ‘don’t want to appear odd’ (226-AUT), explaining that ‘to not stick out from others I have to watch how people do or say things and mimic it and memorize the things that work’ (133-AUT).
Thirty-one responses reported negative social experiences. For example, participants described ‘being judged or misunderstood’ (263-AUT) and wrote of having ‘had some repeated negative experiences’ (59-AUT). Twenty-five responses indicated negative affect or self-perception. Examples within this code included one autistic adult who stated, ‘I don’t feel enough’ (114-AUT), and another who reported that it ‘made me sad to think about the logistics of it and that it’s all hopeless’ (142-AUT).
Finally, 11 responses were coded as indicating intolerance of uncertainty, e.g. a desire ‘to maintain control’ (107-AUT); 10 responses stated a general preference for being alone, and eight responses highlighted a lack of opportunity for engaging in social situations.
Discussion
The measurement of co-occurring SAD in autism is complicated by the overlap of autistic characteristics and features of SAD. Our study is one of three that has examined self-report measures of SAD in autistic adults (Boulton & Guastella, 2021; Chew et al., 2021), and the only one to directly ask respondents about item interpretation. In our non-autistic adult sample, the SAD-D demonstrated a unidimensional structure, excellent reliability, and good convergent validity. In autistic participants, however, factor analysis did not confirm the unidimensional structure of the SAD-D, raising concerns as to the validity of this measure for use with autistic adults. Furthermore, FUD-SAD-D responses show that on at least one item, over half of our autistic participants reported on experiences unrelated to social anxiety when completing the SAD-D, compared to 17% of non-autistic participants.
We anticipated that adapting SAD-D scores to reflect only social-anxiety-related item endorsements may improve its unidimensional fit. Our hypothesis was not supported, with EFA of autistic participants’ R-SAD-D scores revealing a two-factor solution. This difference in factor structure may indicate that the R-SAD-D and the SAD-D capture a construct other than social anxiety when used with autistic adults, perhaps both social anxiety and autistic preferences or experiences in regard to social interaction. Alternatively, the structure of social anxiety in autistic adults may differ from that in non-autistic adults. Our findings indicate two distinct but related factors representing (1) emotional and (2) behavioural domains of social anxiety. Our results suggest that these domains should be considered separately, with the emotional domain perhaps providing a more accurate measurement of SAD symptoms in autistic adults. That being said, concurrent validity alongside clinical diagnosis is needed to determine whether asking follow-up disambiguation questions and rescoring the SAD-D (R-SAD-D) is valid to screen for social anxiety in autism.
It is important to note that factor 2 (behavioural domain) comprised all five R-SAD-D items that were rescored through our disambiguation process, whereas factor 1 (emotional domain) comprised items with scores unchanged from the SAD-D. It is, therefore, possible that our disambiguation and rescoring process influenced the resulting factor structure of the R-SAD-D. Even so, with our findings failing to confirm the unidimensionality of the SAD-D when following the conventional scoring protocol, the possibility that autistic social anxiety comprises two distinct factors, and the overlap of autistic social interaction preferences with what appear as socially anxious behaviours, warrants further investigation.
Our content analysis identified a range of factors unrelated to social anxiety that autistic adults reported as influencing their item endorsement on the SAD-D and Mini-SPIN. For example, participants described social interactions as a source of fatigue and sensory overload. Autistic adults show increased sensory sensitivity compared to non-autistic adults (Tavassoli et al., 2014), and our results highlight that these sensitivities contribute to behaviour in and/or avoidance of social interactions. Therefore, autistic adults may not be disproportionately fearful of overwhelming sensory stimuli in a social situation. Instead, many autistic adults experience a genuinely heightened sensory response to uncertain social situations. Thus, sensory overload and/or fatigue is a likely outcome, and a proportional response is to manage the amount, and quality of social interaction one engages in.
Cognitive models of SAD in non-autistic people suggest that when people with SAD fear being negatively perceived in a social interaction, they will engage in behavioural and cognitive strategies – known as safety behaviours (Salkovskis, 1991) – to prevent the feared outcome from occurring. Our results suggest that some autistic adults engage in similar behaviours (e.g. preparing a social script), which may not be due to preventing a feared outcome per se, but instead to mask or camouflage autistic traits. One autistic scholar described masking as adaptive morphing; that is, a self-protective strategy used to reduce the risk of exclusion from social groups (and thereby reduce risk of social, emotional, and physical harm; Lawson, 2020). However, emerging research also suggests that self-focused attention in the form of masking can play a role in reinforcing anxious thoughts (similarly to safety behaviours) (Black et al., 2023; Lei et al., 2024). Future research and clinical practice with autistic people should explore instances when self-reflection and forms of impression management may be beneficial, and when they may be unhelpful and negatively impact mental health (Black et al., 2023). Moreover, research and clinical practice should also focus on creating and understanding how to set up more enabling environments in which autistic people do not need to ‘adaptively morph’ in the first place.
Indeed, several of our participants attributed their SAD-D responses to prior negative social experiences. Previous research suggests that these negative social experiences may be exacerbated by the implicit negative attitudes that non-autistic adults often hold towards autistic people (Dickter et al., 2020). Thus, rather than disproportionately fearing negative evaluation (typical social anxiety), autistic adults may frequently experience actual negative evaluation by non-autistic individuals. In light of this, erroneously interpreting self-protective masking strategies as anxiety-driven safety behaviours is likely to prove unhelpful (Black et al., 2023). Clinicians working with autistic people must be aware of the broader social contexts in which autistic people are interacting within and assist in building positive autism identities, while helping non-autistic people in their social network improve their understanding and acceptance of autism, which may help to reduce non-autistic people’s explicit biases towards autism (Jones et al., 2021).
Combined, analyses presented in this study suggest the need for caution when using the SAD-D as a measure of social anxiety in autistic adults. Furthermore, although these results cannot be extrapolated to other measures of social anxiety, they are suggestive that further follow-up is needed to understand autistic adults’ interpretation of SAD questionnaire items developed originally for non-autistic people. Ideally, perhaps such a measure should be developed for autistic adults specifically, such as the Adult-Autism Anxiety Scale (Rodgers et al., 2020), but with a particular focus on SAD. The Response Process Evaluation Method (Wolf et al., 2023) might be a useful framework to help guide an inductive approach developed by and with autistic adults and draw on autistic adults’ lived experiences of social anxiety rather than applying conceptualisations developed on non-autistic samples.
The unique experiences reported by our autistic participants present the intriguing notion that we may need to look beyond measurement, to instead consider whether the neurotypical conceptualization of social anxiety itself is applicable to autistic individuals. If neurotypical conceptualizations of social anxiety inadequately capture the experiences of autistic individuals, future measurement based on this conceptualization is likely to continue to fail in capturing the nuance and complexity of social anxiety in autism.
This study should be interpreted with the following limitations in mind. First, though this study comprises a large sample, only two autistic participants reported co-occurring intellectual disability, thus limiting generalisability of results to the broader autistic population of individuals with differing support needs. Second, free-text responses to the FUD-SAD-D were typically brief, limiting the scope of our content analysis. Additional investigation using in-depth qualitative methods is needed to provide richer insight on this topic. Nevertheless, future studies–particularly those employing psychometric measures developed for non-autistic respondents–may benefit from providing opportunities for autistic participants to explain and contextualise their responses. Third, follow-up questions may also have been misunderstood by participants – it is possible that some participants responded ‘due to fear or anxiety’ even though it was not related to social anxiety per se, but more to do with anxiety in social situations related to an autistic trait (e.g. sensory differences). This might mean that our results are an under-estimate of the responses ‘not due to social anxiety’ (as it is conceptualised in non-autistic people) by autistic adults. Fourth, a subset of items on the SAD-D and Mini-SPIN were chosen for follow-up due to being related specifically to potentially ambiguous behaviours. This may limit the interpretation of the EFA as not all items were rescored; however, our CFA were unaffected by this decision. Finally, content analysis of responses deemed ‘non-social anxiety related’ resulted in categories that could be seen as related to social anxiety (such as masking and intolerance of uncertainty), which maybe is not surprising given the overlap between the social features of autism and characteristics of social anxiety (Spain et al., 2018). A conservative approach was taken in disagreeing with participants’ reasons given that they had explicitly selected ‘No, other reason’ when asked if their response was related to social anxiety. In performing the content analysis the two coders (both trained psychologists) made informed judgements based on whether they were more related to ‘social anxiety’ or ‘autism’. For instance, responses related to feelings of negative evaluation were coded as social anxiety, even though there is a probability that autistic people are genuinely being negatively evaluated by others as opposed to this being an inaccurately held perception. Participants could indicate ‘Both’ social anxiety and non-social anxiety related factors and in these cases item responses were not rescored. That said, given the inter-linked nature of the social features of autism and characteristics of social anxiety, it is difficult to completely delineate between the two. Fourth, we used a retrospective self-report measure, which may be influenced by post-rationalisation of behaviour. Future research using methods that capture in-the-moment-data (e.g. Experience Sampling Methodology; Myin-Germeys et al., 2018) would allow more precise investigation of the interaction between the immediate physical environment (e.g. sensory stimuli) and social anxiety symptoms.
In summary, our study indicates that autism-related experiences influenced autistic participants’ responses to several SAD-D items, likely contributing to its failure to confirm the unidimensional factor structure of the SAD-D. Moreover, after rescoring items using a disambiguation process to exclude responses unrelated to social anxiety (R-SAD-D), scale psychometrics were not improved, instead we found a two-factor solution to be more appropriate for autistic adults. Our findings highlight the importance of holistic, individualised approaches in the assessment of mental health symptomatology with autistic people, and the importance of clarifying items to aid interpretation. Our findings provide some indication that adapting existing psychometric measures for use with the autistic population may be of limited value; developing new, autism-specific measures in collaboration with the autistic community may facilitate more accurate quantification of social anxiety symptoms in autistic adults. The content analysis presented here provides several initial building blocks for consideration in any future efforts towards development of an autism-specific social anxiety measure.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241290547 – Supplemental material for Suitability of the DSM-5 social anxiety disorder severity scale for autistic adults
Supplemental material, sj-docx-1-aut-10.1177_13623613241290547 for Suitability of the DSM-5 social anxiety disorder severity scale for autistic adults by Simon G Brett, Jacquiline E den Houting, Melissa H Black, Lauren P Lawson, Julian Trollor and Samuel RC Arnold in Autism
Footnotes
Acknowledgements
The authors thank the ALSAA Research Advisory Network for their guidance and review of ALSAA study materials. They thank Professor Jennifer Hudson for her helpful comments on an early draft of this manuscript. Finally, they thank all the participants for taking part.
Data availability
Researchers can access the ALSAA databank through contacting the Autism CRC.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the financial support of the Cooperative Research Centre for Living with Autism (Autism CRC), established and supported under the Australian Government’s Cooperative Research Centres Programme. JT is supported by an NHMRC Leadership Fellowship GNT2009771. JdH was supported by a Macquarie University Research Fellowship award.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.