
Abstract
Autism diagnoses in adulthood have risen substantially over recent years. While providing potential benefits, many autistic adults struggle to navigate their new diagnosis. Our review aimed to synthesise the evidence for post-diagnostic support for autistic adults without intellectual disability diagnosed in adulthood in the UK: investigating availability, efficacy, and autistic adults’ experiences. A systematic search of four biomedical and three grey literature databases was conducted to identify UK-based studies published since 2012. A total of 27,581 records were screened in duplicate, with 19 studies regarding post-diagnostic support included. A narrative synthesis was undertaken due to anticipated heterogeneity. A service mapping exercise also provided a summary of post-diagnostic service provision currently available across the UK. Findings indicate that many services across the UK provide information and signposting as their primary form of post-diagnostic support, whereas autistic adults desire low-level support services, psychoeducation, and peer support. Evidence regarding the efficacy of post-diagnostic support was unavailable. This review highlights the need for adequate support to alleviate post-diagnostic challenges and improve autistic adults’ quality of life. Low-level support services, psychoeducation, and peer support appear acceptable and feasible, with a preference often indicated for autistic-led support. Future research should develop manualised post-diagnostic support programmes and assess their efficacy.
Lay abstract
More adults than ever before are seeking an autism diagnosis in adulthood. While receiving a diagnosis may be beneficial, many autistic people struggle to navigate their new diagnosis, and require support. This study conducted a systematic review of previous research on the support available after diagnosis (post-diagnostic support) for autistic adults without intellectual disability who were diagnosed in adulthood in the UK. A systematic review is a pre-planned method of searching for all relevant studies, before combining these to answer a larger question. The study aimed to investigate the availability of such support and its effectiveness, and to explore autistic adults’ experiences of accessing support. We also used publicly available information to create a map of the post-diagnostic support services currently available across the UK. A systematic search of seven databases was conducted, to identify UK-based studies published after 2012. Nineteen studies were eligible to be included in the study. Although some form of post-diagnostic support is available across most areas in the UK, this mostly consists of providing information and ‘signposting’ the person to other services. These options may not meet the needs of autistic people, who want services such as psychoeducation (therapy whereby an individual receives education about their diagnosis to improve understanding and self-management), and peer support. Findings highlight the need for adequate support to alleviate the post-diagnostic challenges autistic adults face. The study could not evaluate the effectiveness of support options in the UK due to a lack of information about this in published research. Research shows that autistic adults would like low-level support services, psychoeducation, and peer support, and may also prefer autistic-led support. Further research is required to develop and evaluate post-diagnostic support programmes which include these elements.
Autism spectrum disorder (ASD), while complex and heterogenous in presentation, is characterised by core difficulties in communication and social interaction, as well as restricted or repetitive behaviours, and presents with or without intellectual disability. 1 Although lifelong, and historically thought of as a diagnosis of childhood, it is increasingly acknowledged that autism may be unrecognised or misdiagnosed, resulting in presentation for diagnosis later in life (Au-Yeung et al., 2018; Punshon et al., 2009).
The prevalence of autism in the UK is relatively high (1.1%; National Institute for Health and Care Excellence, 2020). Diagnoses have risen exponentially by 787% from 1998 to 2018, with the greatest rise for any age group seen in adults (Russell et al., 2021). This increase is likely due to heightened awareness and improved diagnostic services following the introduction of the first disability-specific legislation in England; the Autism Act (2009), and the first Autism Strategy in 2010 (National Autistic Society, 2020).
Receiving a diagnosis has been credited with helping autistic adults to gain a better understanding of themselves, bringing a sense of relief (Powell & Acker, 2015; Stagg & Belcher, 2019), and may lead to improvements in mental health (Arnold et al., 2023). However, for some, it represents a shock, and can trigger negative emotions (Powell & Acker, 2015). Even when viewed positively, many autistic adults can struggle after their diagnosis. Difficulties include re-aligning their self-identity (revisiting potentially distressing past experiences during the diagnostic process), feelings of isolation, including the potential for discrimination and negative reactions from others, and impacts upon mental health (Leedham et al., 2020; Punshon et al., 2009; Stagg & Belcher, 2019). This is magnified by the fact that autistic individuals already face poorer health outcomes, with significantly higher rates of mental health disorders (Lai et al., 2019).
Given the substantial difficulties experienced by many autistic adults, support in this post-diagnostic period is vital. Post-diagnostic support can assume many different forms, including (but not limited to) the provision of information and signposting to other services; low-level support services to assist in the management of day-to-day life; peer support; and psychoeducation. Psychoeducation describes a structured therapeutic intervention involving education on a condition in order to improve understanding and self-management, delivered individually or in groups (Sarkhel et al., 2020). It has been more widely evaluated for other conditions, for example, for attention deficit hyperactivity disorder (ADHD), where psychoeducation has demonstrated efficacy in increasing knowledge of the condition and improving life satisfaction (Hirvikoski et al., 2017). The efficacy of psychoeducation or other support options for autistic adults is still unknown.
Many autistic adults have reported that support following their diagnosis is lacking or inaccessible, particularly for those without intellectual disabilities (Arnold et al., 2023; Powell & Acker, 2015; Public Health England, 2017; Stagg & Belcher, 2019). If no meaningful support is available following receipt of a diagnosis, the purpose of diagnostic services is limited. Within the UK, most post-diagnostic support is provided through the publicly-funded (i.e., free at the point of use) National Health Service (NHS), although this can include commissioning or paying for support offered by organisations and healthcare providers external to the NHS. Often due to long waiting times for such services, some adults may also choose to pay for private post-diagnostic support, although very little information is available on the prevalence or quality of such support.
The most recent UK Autism Strategy (2021) promises funding to improve post-diagnostic pathways (Department of Health and Social Care and Department for Education, 2021). However, there is a lack of evidence regarding current post-diagnostic support for autistic adults without intellectual disabilities diagnosed in adulthood. To address this gap, our review aims to investigate the current provision of post-diagnostic support for these adults in the UK, assess the efficacy of post-diagnostic support, and explore autistic adults’ experiences with post-diagnostic support. Through this, we aim to inform the design and commissioning of adult post-diagnostic services.
Methods
Overview
A protocol was registered with PROSPERO, the online International Prospective Register of Systematic Reviews (registration #CRD42022336677). The inclusion criteria were amended to incorporate studies with participants aged 16+ years with at least some diagnosed in adulthood, due to a paucity of studies identified in the initial search; otherwise, the review proceeded as intended. The review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines for conducting systematic reviews (Page et al., 2021; see Figure 1).
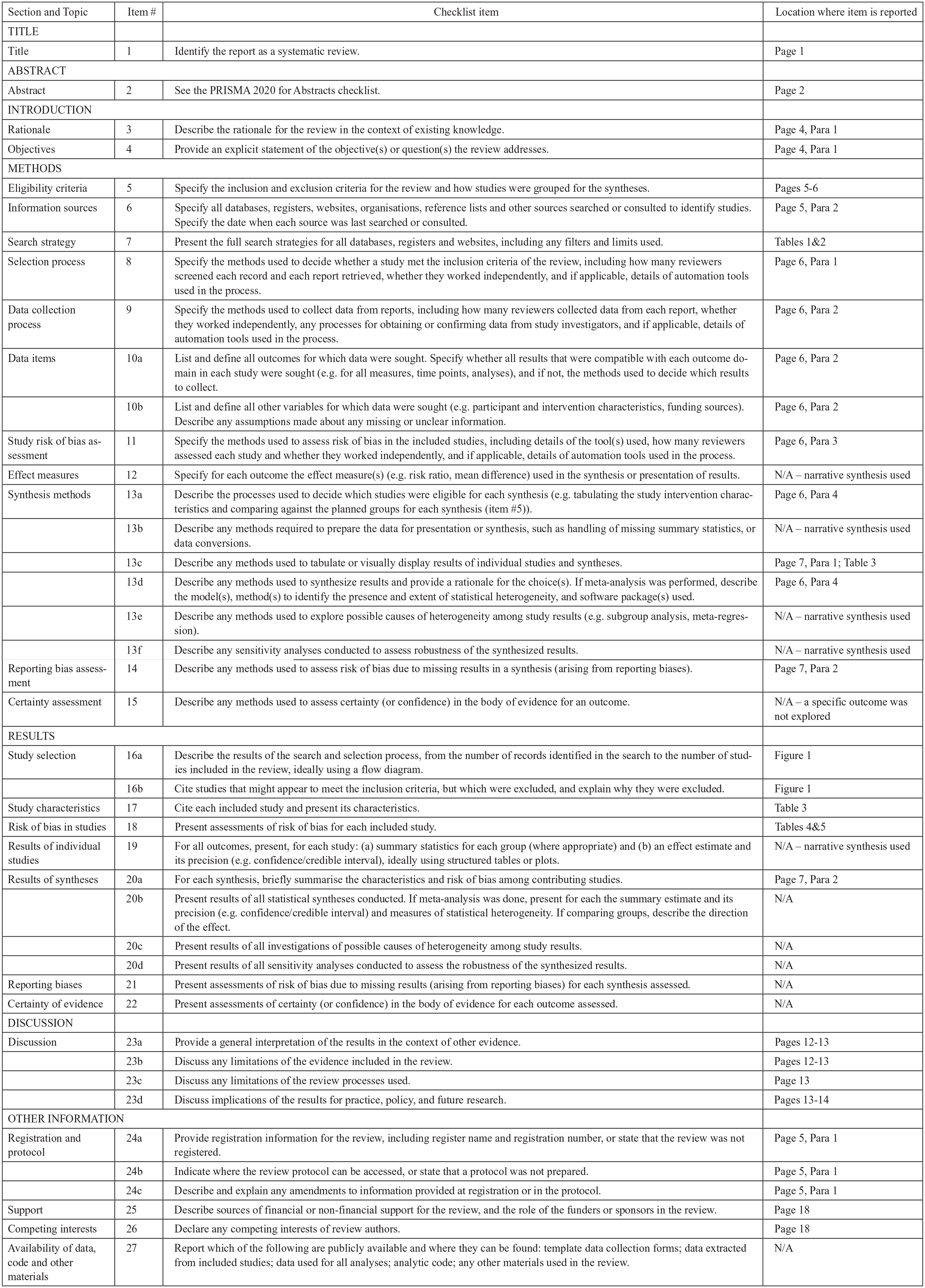
PRISMA checklist.
Search strategy
A systematic search of four biomedical databases was conducted on 16 June 2022: MEDLINE, PsycINFO, CINAHL and Web of Science. A comprehensive search strategy was developed by consulting topic literature (Supplemental Materials A and B). Due to varying methods of post-diagnostic support and an anticipated lack of studies, we aimed for a sensitive search and tolerated low specificity to ensure we captured all relevant studies. We restricted the search to English language studies published since 2012 to identify evidence relevant to current practice. Searches were re-run on 16 July 2022, and 10 April 2024 to locate any additional eligible studies. Citation searching (forwards and backwards) was also utilised.
Grey literature searches of Google Scholar, EThOS, and ProQuest were conducted for unpublished literature, allowing a richer evidence base. In addition, online searches were conducted on Government, NHS, Clinical Commissioning Group, Integrated Care System, and Council websites to identify other eligible studies.
Selection criteria
The inclusion criteria were:
Primary research studies of any design;
Involving adults diagnosed with autism, without intellectual disability, in adulthood (note that studies were eligible if they featured some adults diagnosed in childhood);
Regarding post-diagnostic support of any form;
and UK-based.
The exclusion criteria were:
Studies involving only children or only adults diagnosed in childhood, or adults diagnosed with autism and an intellectual disability;
Regarding interventions not utilised as, or available as, post-diagnostic support;
and non-UK based.
Screening and full-text review
Duplicate references were removed automatically using EndNote 20, and the remaining references were manually checked for missed duplicates and then exported into the screening software system Rayyan (Ouzzani et al., 2016). Titles and abstracts were independently double-screened, with any conflicts resolved by discussion. The second author then completed the full-text review for the first two searches, with the first and last author completing full-text review for the final search. The flow of studies is displayed in Figure 2.
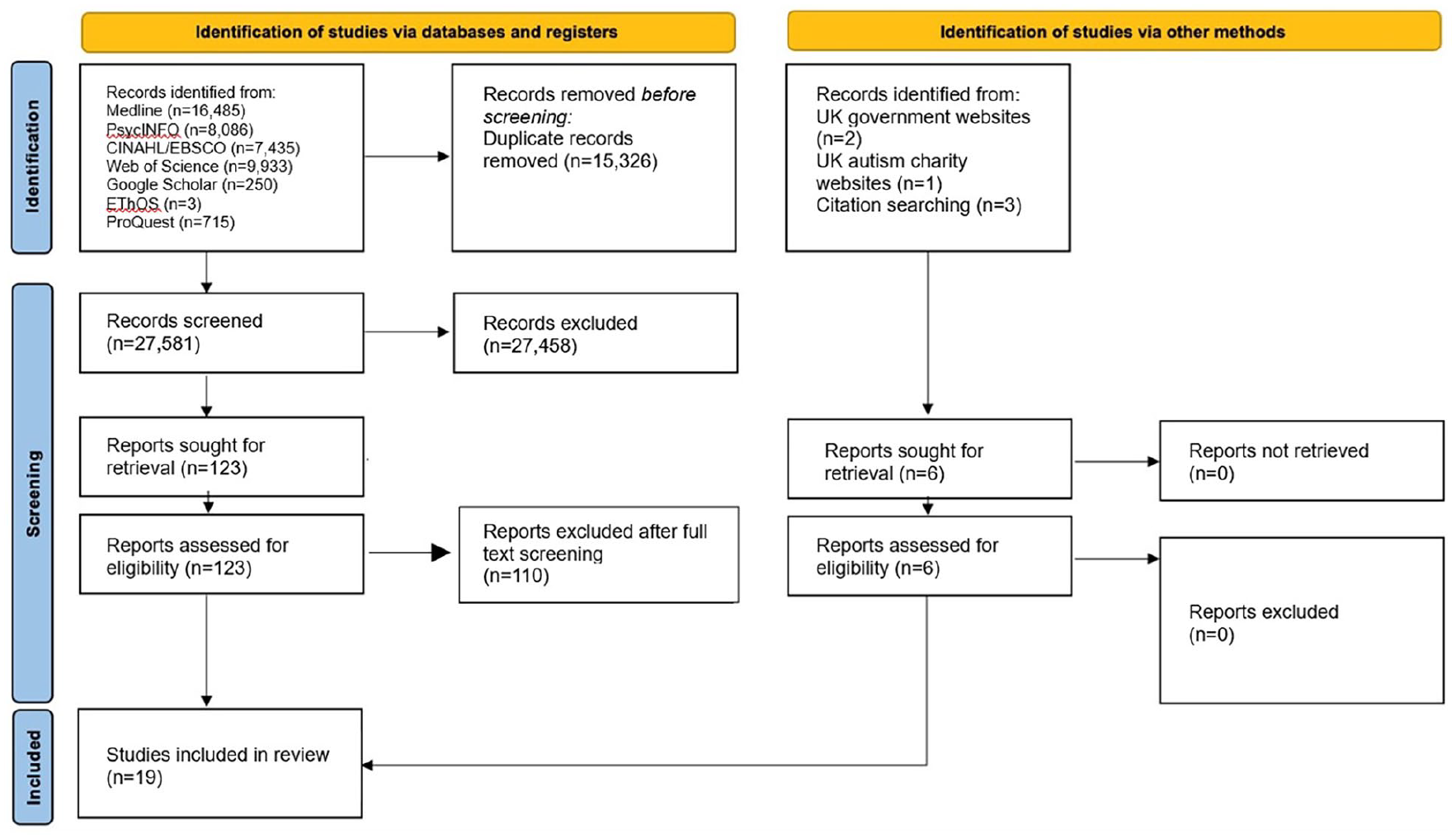
Flow of studies through the systematic review process.
Data extraction
Extracted data and quality assessment findings were imputed into Microsoft Excel (2022) by the second author, using a standardised form created for this review. Extracted information comprised the study aim; year; location; description of post-diagnostic support if applicable; study design; methodology; participants; inclusion/exclusion criteria; sampling; recruitment and retention; key findings; funding and conflict of interest; and strengths and limitations.
Quality assessment
The quality of journal articles was assessed using the Mixed Methods Appraisal Tool (MMAT), chosen for its application to diverse study designs (as anticipated with this review), and its domain-based (rather than score-based) approach (Hong et al., 2018; see Supplemental Material C). Grey literature quality was assessed using the Authority, Accuracy, Coverage, Objectivity, Date Significance (AACODS) checklist, selected for its comprehensive nature and domain-based approach (Tyndall, 2010; see Supplemental Material D).
Evidence synthesis
A narrative synthesis approach was chosen, due to the heterogeneity of study designs and aims which rendered meta-analysis unfeasible. Synthesis followed the framework provided by Popay et al. (2006) and the Synthesis Without Meta-analysis (SWiM) reporting guidelines (Campbell et al., 2020; Popay et al., 2006). Studies were grouped for synthesis according to the three components of our review aim, and sub-grouped by the post-diagnostic support method. We prioritised studies according to the volume of data regarding post-diagnostic support, and the quality assessment findings.
Service Mapping
A secondary aim of the study was to provide an overview of the currently available post-diagnostic support for autistic adults in the UK. All services identified through the systematic review were included in this mapping exercise, as well as services identified on Government, NHS, Clinical Commissioning Group, Integrated Care System, and Council websites which did not meet inclusion criteria for the systematic review; for instance, services which were described online only but were not referred to in any research studies.
Results
We included 19 studies in this review: 13 journal articles and 6 grey literature reports (summarised in Table 1). These were of varying study designs (8 qualitative, 4 quantitative and 7 mixed methods), represented all four UK countries and were published between 2014 and 2024. Below, we present summaries of the quality assessment, and characteristics of the participants to better describe the sample. We then present the findings related to (a) efficacy of post-diagnostic support options, (b) experiences of participants and (c) mapping the available services identified.
Summary of included studies.

SST: social skills training; NHS: National Health Service; SAT: Specialist Autism Team; ANCOVA: analysis of co-variance; ARGH: Autism Rights Group Highlands.
Studies may have included other participants. Only data related to adult participants are included here.
Studies may have reported other findings. Only findings related to post-diagnostic support are included here.
Quality assessment
Overall, the quality of journal articles was reasonable (see Supplemental Material C). Qualitative studies tended to be of higher quality. Issues within quantitative and mixed methods studies included the sample being unrepresentative of the autistic adult population (n = 4) and the risk of non-response bias (n = 4). Participants in the qualitative studies did not represent the entire autistic adult population, but qualitative findings are not intended to be generalisable. Grey literature study quality was mixed and generally lower (see Supplemental Material D); limitations included the absence of references (n = 2) or stated methodology (n = 1).
Participant demographic characteristics
In total, 1,607 autistic adults were represented across studies. The mean participant age was 42.68 years (range = 17–89 years), and 51.01% of participants identified as male. Participants were predominantly of White ethnicity (92.78%).
Efficacy of post-diagnostic support
Six studies evaluated two types of post-diagnostic support: low-level support services (McConkey et al., 2021; Southby & Robinson, 2018) and psychoeducation (Beresford et al., 2020; Crane et al., 2023; Crane et al., 2021; Hatton & Lee, 2022). However, none collected data for defined outcomes to enable assessment of the efficacy of such post-diagnostic support. As such, we cannot comment on the efficacy of any of the support options identified here.
Experiences of post-diagnostic support
General experiences
Adults’ experiences were often negative, with many reporting a lack of access to post-diagnostic support (Crowson et al., 2024). In a survey by Jones et al. (2014), 41.9% of the 128 respondents received no post-diagnostic support. When support was offered, it failed to correlate with what they desired (Jones et al., 2014). In another survey involving 343 autistic adults producing consensus statements on their experience and preferences of post-diagnostic support, most did not receive any ‘optimal’ support as defined by key stakeholders (Wigham et al., 2022; see Table 1 for more detail). This mirrored a large study by the Westminster Commission, with a misalignment between support available and desired; only 22.1% expressed satisfaction with the post-diagnostic phase (Centre for Applied Autism Research, 2021). Autistic adults in the study conducted by Hull et al. (2024) felt that the support they were offered was inflexible and needed greater personalisation, sometimes being inappropriate for certain individual’s needs.
A recent study by Crowson et al. (2024) used a modified Delphi method to generate a consensus from the autistic community on their post-diagnostic support priorities. Twenty-four key priorities were identified, which represented important elements that autistic adults wished to be offered in the context of post-diagnostic support. In particular, participants prioritised being able to access any support in their area in the first place, followed by feeling assured that professionals involved in offering services were adequately trained. Third, participants wanted to receive support with processing the impact of receiving an autism diagnosis in adulthood, followed by experiencing consistency in use of their preferred methods of contact, and being provided with an individualised support plan.
Adults did describe positive experiences and reported tangible benefits when appropriate post-diagnostic support was received (Crane et al., 2018, 2021, 2023). A recent Scottish evaluation of their national post-diagnostic support service, through which everyone can access support, sought the opinions of autistic adults via an online survey (Minister for Mental Wellbeing and Social Care, 2022). While it is unknown which specific support each received, impacts were largely positive: most commonly providing a better understanding of autism (90%) and themselves (87%), and in forming connections with autistic peers (67%). In addition, in an evaluation of the seven Welsh Integrated Autism Services, adults specifically praised services for their proactive offer of support (Holtom & Lloyd Jones, 2019).
Follow-up and signposting
Despite being the most common form of support provided, the sole provision of a follow-up appointment with signposting to other services appeared unfavourable. In a large evaluation, the SHAPE project (Supporting adults with High-functioning Autism and asPerger syndromE), participants either received post-diagnostic psychoeducation, or a diagnosis only; the diagnosis-only group received one follow-up session, leaflets, and signposting (Beresford et al., 2020). Many found the information inappropriate, and simple signposting was also deemed demoralising; none had contacted the recommended services, noting that being autistic made this challenging. One adult described the diagnostic process as ‘invasive’, and compared the subsequent lack of post-diagnostic support to a ‘hit and run accident’ (p. 83; Beresford et al., 2020).
Similarly, in a small grey literature evaluation of an NHS diagnostic service, participants desired more comprehensive signposting (Bracher, 2014). They were often able to identify a general problem, but were unsure of the necessary steps to manage such issues without the support of others (Bracher, 2014). Westminster Commission survey respondents likewise frequently received leaflets or signposting, but indicated that this afforded ‘no actual help’ (p. 52; Centre for Applied Autism Research, 2021).
Low-level support
Low-level support services take the provision of information and signposting further by allowing autistic individuals to utilise resources that are appropriate to them, with the support and advocacy of others, either on a 1:1 basis or as part of a larger service.
Two studies evaluated such services (described in Table 1). Southby and Robinson (2018) evaluated ‘Leeds AIM’, an autism hub, and McConkey et al. (2021) evaluated ‘RIGHT4U’, a 1:1 service. A significant outcome reported by Leeds AIM users was improved access to appropriate information and empowerment to act upon this, reporting positive impacts on access to education and employment. While both services facilitated access to opportunities (e.g., work experience), RIGHT4U users disclosed no changes to their employment or education status. This may be due to greater opportunities within Leeds AIM (e.g., through an employment peer-support group). Positive outcomes of service use identified by participants in both studies included reduced anxiety, improved confidence, increased social opportunities, development of coping strategies, and improved access to healthcare.
The ‘autism hub’ setup is seen within Scotland, with eight ‘One Stop Shops’ (integrated information hubs and advice services, offering information, guidance, access to other services, and training opportunities for autistic people and their families). In a small survey evaluating the Highland One Stop Shop, autistic adults rated the service highly, with positive results for peer support, socialising, and staff ratings (ARGH, 2018). Many felt it improved their mental health, including addressing their previously unsupported suicidal ideation (ARGH, 2018). One Leeds AIM user also stated the support prevented them from self-harming and attempting suicide (Southby & Robinson, 2018).
Psychoeducation
Five studies evaluated psychoeducation as post-diagnostic support (described in Table 1). Hatton and Lee (2022) qualitatively evaluated an NHS-delivered 7-week online group psychoeducation programme. Participants described an opportunity for knowledge sharing, consolidation, and self-reflection, subsequently allowing them to ‘manage rather than struggle’ (Hatton & Lee, 2022). Improved daily management was reflected in the evaluation by Crane et al. (2021) of an autistic-led 10-week group psychoeducation programme (‘Exploring Being Autistic’; see Table 1 for more details). The programme was described by one participant as enabling them to ‘see what’s happening and find a way out’ of problematic situations (p. 900).
Within the SHAPE study, autistic adults receiving psychoeducation recounted positive experiences (Beresford et al., 2020). A dominant theme was the impact on their self-perception; becoming more accepting and enhancing their self-esteem. Echoing Hatton and Lee (2022) and Crane et al. (2021), other significant benefits centred around developing coping strategies and learning from others. Participants of all three studies reported acquiring a sense of community, reduced isolation, and less need to mask (masking being the concealing of autistic traits or difficulties, which is often emotionally and physically taxing (Cook et al., 2021)).
In contrast, the subgroup of participants in the SHAPE study who did not receive psychoeducation reported unresolved difficulties post-diagnostically, particularly in accepting their diagnosis (Beresford et al., 2020). This negatively impacted the mental health of some, which they attributed to this lack of psychoeducation. From quantitative data, there was some evidence of deteriorating mental health immediately after diagnosis for this cohort, compared to a small but statistically significant improvement in mental health outcomes for those receiving psychoeducation (Beresford et al., 2020).
The autistic-led nature of the psychoeducation programme ‘Exploring Being Autistic’ was highlighted as a strength, in both the in-person and online versions of the programme (Crane et al., 2023; Crane et al., 2021). The autistic facilitator was deemed more understanding, and provided a positive role model for recently diagnosed participants. SHAPE study participants also appreciated hearing positive stories of autism, while participants in the study reported by Hatton and Lee (2022) felt the content should be more positive in their non-autistic-led programme (Beresford et al., 2020). In replicating their study of the Exploring Being Autistic programme when delivered online as opposed to in-person, Crane et al. (2023) noted some unique benefits of online delivery, including increased potential accessibility, reduced cognitive load/preservation of participants’ energy for focusing on the programme, and the opportunity to form meaningful social connections with other group members. However, participants also emphasised the importance of flexibility in delivery format, as technological issues had the potential to hinder access, and some group-based activities (e.g., the use of breakout rooms) were felt to be less effective online (Crane et al., 2023).
Hatton and Lee (2022) explored participants’ preferences for psychoeducation delivery. Some felt online delivery was practical and accessible, and lessened anxiety. Others, however, considered that it did not permit sufficient scope for interaction.
Peer support
No studies directly evaluated peer-support programmes. However, peer support was a theme common to most studies, with support groups being desired by autistic people, and with significant impacts arising from the support of like-minded individuals (Centre for Applied Autism Research, 2021; Jones et al., 2014).
For example, Crompton et al. (2022) explored post-diagnostic support in interviews with autistic adults. Many thought that peer support would lessen the difficulties of processing the diagnosis by validating their experiences (Crompton et al., 2022). Similarly, in the study by Hickey et al. (2018), a common thread in the experiences of older autistic adults (aged 50+) was the importance of universality; being ‘in the same boat’. In an exploration of the diagnostic experiences of autistic adults by Crane et al. (2018), the perceived invasive nature of the diagnostic process (‘dredging up old stuff’) was described as traumatic (p. 3768), and subsequent peer support found to be beneficial.
Within several studies, autistic people reported more comfortable relationships with other autistic individuals, with a lessened feeling of the need to mask, thereby improving self-perceived confidence and communication skills (Cook et al., 2021; Crane et al., 2021; Hatton & Lee, 2022). In addition, knowledge sharing helped to formulate coping strategies, with some considering sharing with peers to be more critical than the structured educational components of psychoeducation (Crane et al., 2021). Peer-led support was also seen as more authentic by participants in the study by Hull et al. (2024), resulting in a more positive experience of engaging with support overall.
As with psychoeducation, the preference was for autistic-led peer support (Crompton et al., 2022; Hull et al., 2024). However, individuals acknowledged that being autistic does not inherently provide the knowledge or skills necessary for the role, and that this requires training and/or experience. Limitations were likewise noted, particularly in peer-support not being used to replace specialist support, such as from mental health services (Crompton et al., 2022).
Service mapping
Systematic online searches identified 83 distinct services for autistic adults without intellectual disabilities. These included services offering diagnosis only (n = 6), diagnosis and support (n = 71), and support only (n = 6). Services covered all regions of the UK except two: County Down in Northern Ireland, and Leicestershire in England, where no information was found. The type and extent of post-diagnostic support varied geographically; this is visually represented in Figure 3.
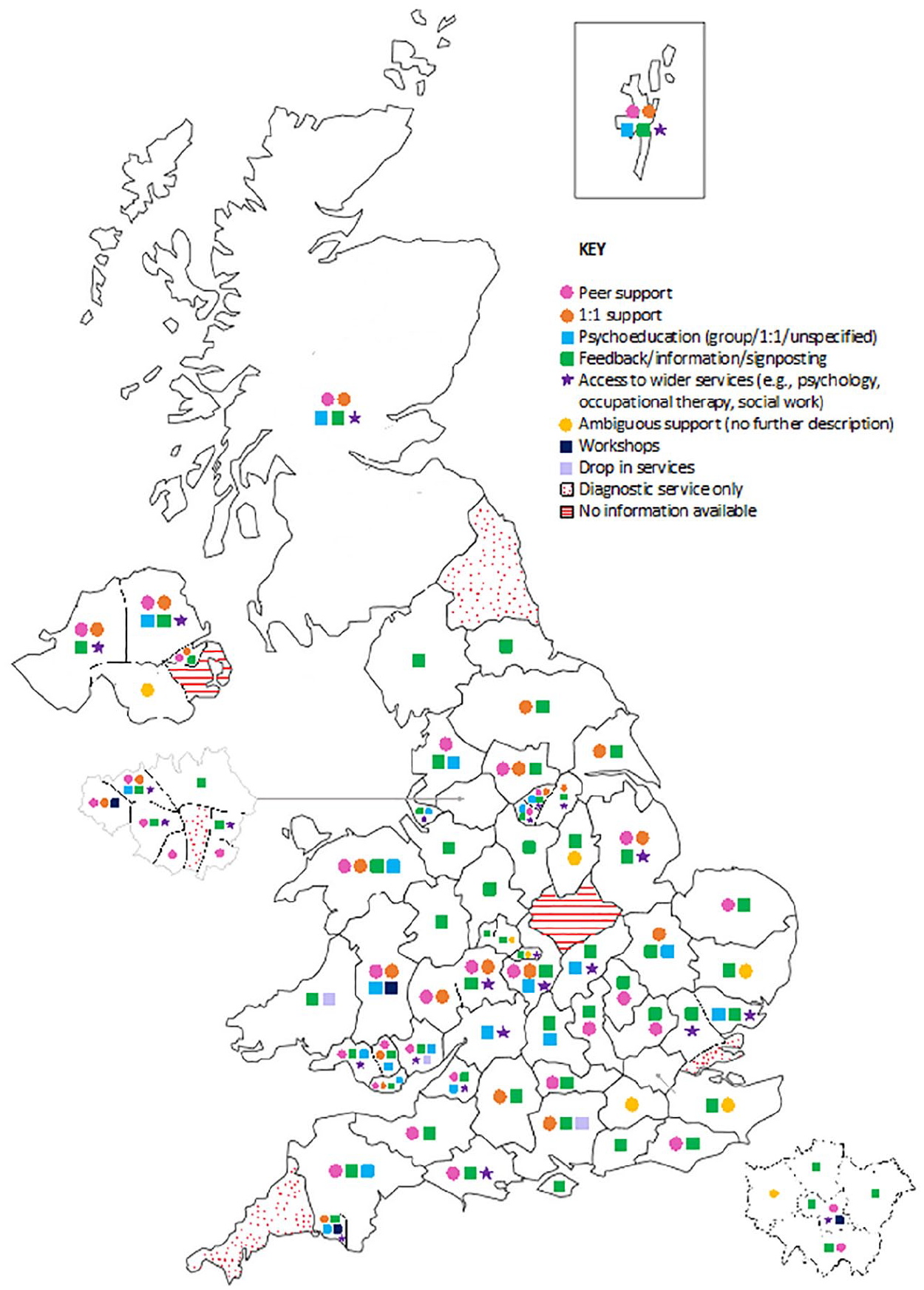
Map of the UK, with each symbol denoting the type of post-diagnostic support available in each region.
Of these 83 services, 93% reported providing post-diagnostic support. Most support concerned feedback, information or signposting (83%); some offered this exclusively (17%). Many provided either peer or 1:1 support (58%); most commonly peer-group support (49%). Some offered psychoeducation (31%), usually group psychoeducation (23%). One-third reported access to wider services, including psychology, occupational therapy, speech and language therapy, or social workers (34%). Few provided all of these forms of support (9%). Infrequently, drop-in services and workshops were also provided (9%).
Discussion
This study explored the content, provision, and evidence for post-diagnostic support for autistic adults receiving a diagnosis in adulthood in the UK, using a combination of systematic review of studies, and service mapping of available support.
Availability of support
Post-diagnostic support is available across most of the UK. However, the extent of support is variable, with some regions providing none or only a minimal amount (e.g., one post-diagnosis follow-up appointment to signpost to other services). Despite apparent provision, autistic adults frequently describe difficulties receiving support, indicating that availability does not necessarily translate to accessibility. UK healthcare professionals have previously highlighted that they are too overstretched and underfunded to provide adequate support, and that even when this is available, they are often pressured not to offer it (Crane et al., 2018; Rogers et al., 2016). This reflects findings internationally; in a recent European Union survey, most professionals reported the availability of post-diagnostic support, yet most autistic adults had received none (Scattoni et al., 2021).
Types of support
Follow-up and signposting represent the most common forms of post-diagnostic support. Although recommended by the National Institute for Health and Care Excellence (NICE), this alone appears insufficient and unacceptable to autistic people (National Institute for Health and Care Excellence, 2021). Autistic adults report difficulties reaching out to signposted services due to the very characteristics of autism; indeed, such help-seeking difficulties are likewise described as barriers to accessing mental health support (Camm-Crosbie et al., 2019).
Instead, autistic adults wish for a low-level support service, where they can access appropriate information and services accompanied by the advocacy of others. Low-level support from ‘autism hubs’ comprises the approach recommended in the previous Adult Autism Strategy (2014), and appears to improve multiple dimensions of autistic adults’ lives (Department of Health and Social Care et al., 2014). Indeed, where it is not accessed, low-level support is frequently desired (Centre for Applied Autism Research, 2021; Crane et al., 2018; Holtom & Lloyd Jones, 2019).
In addition, psychoeducation appears to have the potential to enhance self-esteem and self-acceptance, allowing adults to come to terms with their diagnosis, develop coping strategies, and improve the management of their day-to-day lives. Psychoeducation has been effective for other conditions, such as ADHD, schizophrenia, and bipolar disorders (Buizza et al., 2019; Hirvikoski et al., 2017; Xia et al., 2011). However, a manualised psychoeducation programme for autism requires development. Psychoeducation could also be integrated into other types of post-diagnostic support offered, for instance, mental health support. Up to 40% of autistic adults experience co-occurring mental health conditions (Lai et al., 2019), and may receive support through traditional mental health services. In addition to being aware of how autism may impact individuals’ experiences of mental health difficulties and potential treatment, ongoing mental health support may provide a practical context through which to provide post-diagnostic support. For instance, autistic adults interviewed about social skills training (although not necessarily in a post-diagnostic context) recommended that this type of support be integrated within mental and physical health support to meet needs in a holistic way (Hull et al., 2024). However, we note that mental health support for autistic adults also comes with limitations, including a lack of evidence, lack of provision, and long waiting times (Linden et al., 2023).
While not directly evaluated, peer support emerges as a critical aspect of other post-diagnostic support methods to autistic adults. Many desired such groups in order to build social connections and learn through the experiences of others (Crompton et al., 2022; Hickey et al., 2018).
Autistic-led support
Among the studies in this review, there was a call for autistic-led post-diagnostic support; to provide better understanding, highlight the strengths of being autistic, and to offer positive role models. A desire for this positive framing of autism in post-diagnostic support was reiterated throughout many studies (ARGH, 2018; Campbell et al., 2020; Cook et al., 2021; Crane et al., 2021, 2023; Hatton & Lee, 2022; Holtom & Lloyd Jones, 2019; McConkey et al., 2021). Notably, autistic adults consistently reported greater ease in communicating with other autistic peers. While communication difficulties define an autism diagnosis, recent evidence has shown that peer-to-peer information transfer among autistic people can be highly efficient, suggesting that post-diagnostic support co-produced and led by autistic people may provide benefits (Crompton et al., 2020; Hull et al., 2024).
Strengths and limitations
Strengths of this systematic review included the use of a comprehensive and sensitive search strategy in multiple databases and the inclusion of grey literature, which is commonly absent from reviews and can add valuable information. Furthermore, duplicate screening added rigour. In addition, the included studies were predominantly published within the last 7 years, providing up-to-date evidence. Finally, using a narrative synthesis allowed the integration of all available evidence when meta-analysis proved inappropriate.
However, limitations exist. Primarily, the lack of evaluations of post-diagnostic support is notable, although this also highlights its nature as an emerging research area. Existing evaluations are mostly small-scale and lack defined outcomes accompanied by efficacy data; as a result, this review was not able to evaluate the efficacy of post-diagnostic support. The variable quality of studies is also noteworthy; while the inclusion of grey literature is beneficial, the research being referred to was often of lower quality. In addition, several studies relied on self-selecting samples of autistic people to provide qualitative data on experiences of post-diagnostic support, which may impact upon study conclusions and recommendations. Moreover, despite the efforts made, the identification of support availability depended on services publishing such information and keeping this up-to-date, and therefore could be inaccurate. Finally, there is a notable underrepresentation of non-White ethnicities within the sample of participants, limiting the generalisability of findings to other ethnic groups (Hirvikoski et al., 2017).
Implications
Commissioning support and its development
Given the potential impact of not receiving post-diagnostic support, commissioning sufficient post-diagnostic support is essential. While requiring initial investment, the subsequent reduced demand for wider services (e.g., mental health) may balance this cost by preventing adults from reaching crisis point. However, a critical first step is funding the full evaluation of current support provisions and expanding or refining existing support as needed. The impact of the funding promised in the latest Autism Strategy will require investigation (Department of Health and Social Care and Department for Education, 2021).
Importantly, this review did not aim to identify the ‘best’ method of post-diagnostic support; those discussed should not be considered mutually exclusive. The post-diagnostic needs of autistic adults may evolve and depend on multiple factors (e.g., availability of family support, or the presence of co-occurring conditions), which may account for differing forms of post-diagnostic support desired by adults within this review. Thus, each may require something different from a post-diagnostic service; a spectrum of long-lasting support is required, rather than time-limited interventions.
Individual choice
Where explored, preferences varied for online versus face-to-face post-diagnostic support. Online support may improve accessibility and diminish anxiety, but could limit social interaction, and reliable internet access is also essential to consider (Baweja et al., 2022; Hatton & Lee, 2022). For group versus individual support, 11 consensus statements created by autistic adults and professionals recommend that post-diagnostic support be available in both formats, allowing for individual choice (Wigham et al., 2022).
Organisation
The provision of post-diagnostic support varies, creating a ‘postcode lottery’ in terms of access. Two UK countries currently have overarching, government-funded post-diagnostic support services: Scotland, with a national pilot service provided by third-sector organisations; and Wales, with seven regional services. While we cannot draw definite conclusions from these evaluations, a centrally-organised system could reduce inequality of access. Furthermore, many third-sector organisations are autistic-led or co-led, and commissioning such services nationwide could contribute to the creation of an expert post-diagnostic service.
Future research
Limitations of this review include the lack of efficacy evaluations and the absence of representative populations, predominantly of non-White ethnicities; the latter, unfortunately, has been the norm within autism research (Steinbrenner et al., 2022). High-quality evaluations with comparable outcomes are required to provide appropriate evidence for the efficacy of support currently offered, and to determine the impact for those not represented by current studies.
In addition, research should consider comparing post-diagnostic service provision across different countries. The present study focused on the UK due to its unique national healthcare system, and a limited capacity to conduct an international systematic review. Anecdotally, the majority of research in this area seems to be based in the UK. However, there are other locations where post-diagnostic support for adults has been evaluated, including across the European Union (e.g., Scattoni et al., 2021). Future research should expand comparisons beyond a single nation in order to synthesise the best evidence for post-diagnostic support for autistic adults.
Conclusions
This review is the first to appraise the evidence surrounding post-diagnostic support for autistic adults without intellectual disabilities diagnosed in adulthood in the UK. It highlights the need for adequate post-diagnostic support, and the positive impact this may have on the lives of autistic adults. Low-level support, psychoeducation, and peer-support methods appear acceptable and feasible; and when experienced, autistic adults appreciate these services. However, few post-diagnostic programme evaluations exist; thus, the ability to draw firm conclusions about their efficacy is limited. Nevertheless, our findings contribute to an emerging area of research. Further research is needed to develop manualised post-diagnostic support programmes and assess their efficacy. Such research should involve representative populations, to meet the needs of all autistic adults.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241273073 – Supplemental material for Post-diagnostic support for adults diagnosed with autism in adulthood in the UK: A systematic review with narrative synthesis
Supplemental material, sj-docx-1-aut-10.1177_13623613241273073 for Post-diagnostic support for adults diagnosed with autism in adulthood in the UK: A systematic review with narrative synthesis by Jade Eloise Norris, Rebecca Harvey and Laura Hull in Autism
Footnotes
Acknowledgements
The authors would like to thank Professor Dheeraj Rai for his guidance in designing this project.
Authorship contribution statement
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work received no formal funding. The third author is supported by the Elizabeth Blackwell Institute, University of Bristol, the Rosetrees Trust and the Prudence Trust.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.