
Abstract
Opportunities for adults to access support following a clinical diagnosis of autism are limited. This study investigated perspectives of autistic adults, relatives and clinicians regarding characteristics of optimal adult autism post-diagnosis support and services. In Stage 1, key stakeholders were surveyed about recent experiences of UK adult autism post-diagnostic services immediately following assessment/up to 12 months afterwards. Information gathered from Stage 1 was used to devise a set of statements describing optimal post-autism diagnostic support/service characteristics. In Stage 2 statements were presented to clinicians in a modified Delphi process. Data analyses were non-parametric and descriptive. Three hundred forty-three autistic adults and 45 relatives completed the Stage 1 surveys. Thirty-five clinicians completed a parallel survey. Just over half of adults and relatives reported receiving a follow-up appointment. Fewer than 40% of autistic people received support/services 12 months after diagnosis. Eleven statements describing optimal post-autism diagnostic support/service provision were developed and consensus among clinicians was reached on all. Autistic adults, relatives and clinicians described some aspects of post-autism diagnosis support and services positively; however, there were significant opportunities for improvement. The study findings can be used to develop current UK post-diagnosis support and services and may be relevant internationally.
Lay Abstract
Research has identified types of support helpful to autistic people, for example, physical and mental health interventions, psycho-education, peer support, developing positive identities and affiliation with social groups. However, accessing suitable post-autism diagnosis support and services is extremely difficult. We asked autistic adults, relatives and clinicians about their experiences of receiving and delivering post-autism diagnosis support/services. In Stage 1, 343 autistic adults and 45 relatives completed a survey. They answered questions about their experiences of UK autism post-diagnosis support/services for adults within 12 months after receiving a diagnosis. Thirty-five clinicians completed a similar survey. Just over half of adults and relatives said there was a follow-up appointment or discussion about support after diagnosis. Fewer than 40% received any support/services in 12 months after diagnosis. We used information from the surveys to create 11 statements describing characteristics of appropriate adult post-autism diagnosis support/services. In Stage 2, we asked clinicians for their views on the statements – they agreed with all of them. For example, those adults are offered an additional follow-up meeting after diagnosis and have access to mental and physical health services. We shared results with autistic adults, relatives and clinicians at two events. Some autistic adults, relatives and clinicians were positive about post-autism diagnosis support/services. However, they described many areas for improvement. The study findings can be used to define, develop and improve the types of adult post-diagnosis support services.
Introduction
Receiving a diagnosis of autism as an adult may facilitate self-understanding and acceptance but also emotional challenges and life re-adjustments (Arnold et al., 2020; Powell & Acker, 2016). Despite this several UK and international studies report support/services post-autism diagnosis for autistic adults are limited (Crane et al., 2018; Huang et al., 2020; Jones et al., 2014).
The type of support/services required by autistic adults crosses many diverse service sectors and differs depending on an individual’s profiles of skills, needs, preferences and circumstances (Scottish Intercollegiate Guidelines Network (SIGN), 2016). One significant area of unmet need identified in the United Kingdom and Canada is support/services for autistic adults with co-occurring mental health conditions (Crane et al., 2019; McMorris et al., 2019), including those at risk of self-harm and suicidality (Camm-Crosbie et al., 2019). Other areas of unmet need include lack of access to services for sleep problems and alcohol misuse (Bowri et al., 2021; Lawson et al., 2020) and autistic adults and professionals continue to identify the need to improve physical and mental healthcare access for autistic people (Mason et al., 2021). UK general practitioners (GPs) describe lacking confidence to support autistic adults (Unigwe et al., 2017), while autistic people described limited availability of reasonable adjustments as a further barrier to healthcare access (Brice et al., 2021). Other unmet support/service needs highlighted in a Canadian study, included limited access to appropriate housing, transportation and employment support (Tint & Weiss, 2018). Gaps in employment support for autistic adults are evident internationally with over-qualification and under-employment of autistic people described (e.g. in Germany) (Frank et al., 2018). The need to adapt job interview questions for autistic interviewees for recruitment process equity is described in the United Kingdom (Maras et al., 2021), and in Australia, appropriate workplace adjustments are required to improve employment outcomes for autistic people (Harvery et al., 2021).
Specific support/services found acceptable and effective for autistic adults include adapted low-intensity psychological interventions for anxiety and depression, for example, cognitive behavioural therapy (CBT) (Maskey et al., 2019; Russell et al., 2019). Other examples of support found helpful by autistic people include autistic-led peer-support groups for people recently diagnosed as autistic covering topics such as whether to disclose diagnosis (Crane et al., 2021; Leedham et al., 2020). A service user survey identified a frequently required type of support was access to support groups (Jones et al., 2014). Approaches to increase feelings of identification within social groups were associated with positive mental well-being and lower self-reported depression symptoms in autistic adults (Maitland et al., 2021). Social prescribing is an existing UK health-based initiative/recommendation to join community groups to improve mental well-being and reduce social isolation (Frostick & Bertotti, 2019; Royal College of General Practitioners, 2018); however, the efficacy for autistic people is yet to be established and adaptations may be required (Charlton et al., 2021; Maitland et al., 2021).
Clinical guidelines for post-autism diagnosis support/services for autistic adults
In the United Kingdom, the National Institute for Health and Care Excellence (NICE) clinical guidance (CG) documentation recommendations on post-autism diagnosis support include health passports, follow-up appointments, adapted interventions and employment support (NICE, 2012). NICE also published quality standards (QS) to facilitate improvement to current service provision, for example recommending adults have a documented discussion with a member of the autism team about opportunities for psychosocial interventions (NICE, 2014) (Table S1). In Scotland, a holistic life-course approach is recommended (The Scottish Government, 2011; SIGN, 2016), while in Australia, national guidelines recommend clients are put in contact with support/services based on need rather than diagnostic outcomes (Whitehouse et al., 2018). However, in a survey of autistic adults, carers and professionals across 11 European countries, fewer than 35% of adults and carers experienced each of the post-diagnostic support/services recommended in national guidance (Scattoni et al., 2021). Thus, despite international guidelines/recommendations (including NICE CG and QS) for provision of adult post-autism diagnostic pathways, there is evidence of a continuing lack of appropriate, personalised immediate and longer-term post-diagnostic support/services for autistic adults. This study set out to ascertain the views of key stakeholders who have (since publication of the NICE QS (NICE, 2014)) experience accessing and/or delivering current UK post-autism diagnosis pathways/service provision. We have used this contemporary information to define a set of agreed consensus statements describing the characteristics of optimum post-autism diagnostic support/services for adults that are relevant for service provision 10 years after publication of the NICE CG (NICE, 2012, 2014).
This study was successfully completed within a UK research programme focused on the diagnosis of autism in adulthood (Wigham et al., 2019, 2020, 2022).
This study aimed to: (1) explore the unique perspectives of key stakeholders (autistic adults, relatives and clinicians) regarding their experiences of recent UK adult post-autism diagnosis support/services provision; and (2) use this information to define and agree a current set of consensus statements describing the characteristics of optimal adult post-autism diagnosis support/services.
Methods
The study design was a two-stage process: in Stage 1, we surveyed three stakeholder groups (autistic people, relatives and clinicians); then using the information obtained, a modified Delphi process (Stage 2) was undertaken to achieve consensus among clinicians on statements regarding optimal adult post-autism diagnosis support/services (Figure 1: online Supplementary Materials). Stage 1 Methods and Results are presented, followed by Stage 2 Methods and Results. An abbreviated methods section is presented; more details can be found in a linked paper about diagnostic assessment (Wigham et al., 2022).
Wales Research Ethics Committee 5 gave the study a favourable opinion (Reference: 17/WA/0188).
Stage 1 Methods
Participants
Study inclusion criteria for autistic adults and relatives of autistic adults: aged 18 years and above; and receiving an autism diagnosis in adulthood during 5 years preceding the study. Autistic adults and relatives were recruited via the Adult Autism Spectrum Cohort-UK (ASC-UK), a cohort of autistic adults, and relatives of autistic adults recruited to longitudinal research (https://research.ncl.ac.uk/adultautismspectrum). Autistic adults and relatives were recruited as separate samples. To ensure confidentiality, we did not ask relatives for the name of their autistic relative and information from each cohort was not linked. We considered it important to capture the views of autistic people unable to consent to participate in the study, so invited a consultee/proxy to complete a self-report survey (not relative’s survey) on behalf of an autistic adult lacking capacity to consent. All recruited participants (autistic adults/consultee/proxies and relatives) gave informed consent to take part in either the autistic adult or relatives cohort. The ASC-UK team invited 667 autistic adults and 189 relatives of autistic adults to participate.
Inclusion criteria for clinicians: currently conducting UK adult autism diagnostic assessments. Clinicians were recruited from a number of sources: those supporting recruitment to the ASC-UK cohort, UK special interest groups and networks of professionals working in multi-disciplinary (MDT) autism assessment and diagnosis teams. One lead clinician from each service was invited to complete the survey on behalf of their MDT.
Measures
Demographic information about participants and Adult Social Responsiveness Scale (SRS-2) scores (Constantino & Gruber, 2012) were available from the ASC-UK cohort datasets.
In addition, a survey (‘Getting an Autism Spectrum Disorder Diagnosis in Adulthood, and Support or Services Received Afterwards’) was developed by the research team informed by international Clinical Guidelines including UK CG142 (NICE, 2012) and Quality Standards (QS51) (NICE, 2014) with parallel versions created for each stakeholder group (the adult and clinician surveys are shown in Supplementary Materials section 1–2). The survey for autistic adults (completed by adults able to give informed consent/or a consultee/proxy on behalf of an adult unable to give informed consent) and parallel survey for relatives both comprised 32 open/closed questions covering referral/pre-assessment, diagnostic assessment and post-diagnosis. A separate survey for clinicians comprised 31 open/closed questions regarding service setting, referral/pre-assessment, diagnostic assessment, post-diagnosis and training/consultancy. Questions in the surveys regarding post-diagnosis focused on the period immediately following and up to 12 months after the diagnostic assessment.
For all three surveys, there was a facility for respondents to add open-text comments to accompany some closed-response/multiple-choice questions.
Findings describing referral/pre-assessment, diagnostic assessment, training/consultancy and qualitative analyses of open-text responses will be reported separately. This article reports results from the closed and multiple-choice questions focused on the post-diagnosis period; we also report examples of comments added to the closed question items to give further context.
Procedures
Potential participants meeting inclusion criteria were sent paper or online (depending on their preference) versions of the information/consent forms and the survey. A link to the survey created using online survey software (Qualtrics, 2005) was sent to online participants via email. Non-responders were sent a reminder letter after 2 weeks. Following informed consent (online or on paper) participants completed the survey.
Data analysis
Assessment of skewness/kurtosis indicated Stage 1 quantitative data were non-normally distributed. Stage 1 analysis comprised descriptive statistics and non-parametric analyses to investigate between-group differences (Mann–Whitney and Chi-Square) (Field, 2009).
Generation of initial statements about optimal post-autism diagnostic services
The research team used the Stage 1 survey quantitative findings from all stakeholders (autistic adults, relatives and clinicians’ closed (yes/no) and open-text responses), and published literature including UK NICE CG documents to generate an initial set of statements describing characteristics of optimum post-autism diagnosis support/services. The first author reviewed the survey findings (through reading and familiarisation with the data) for aspects of services that were commonly considered sub-optimal. These areas were discussed within the research team (including an autistic co-investigator and clinicians experienced in UK NHS services for autistic people). The team generated statements via an iterative process of discussion, appraisal and refining wording during a series of meetings. The statements were used in the first stage of the Delphi process.
Community involvement statement
An autistic co-investigator was an integral member of the research team throughout the study. Prior to data collection, we held two focus groups attended by autistic adults and relatives and co-facilitated by a relative of an autistic person, during which draft documentation (information/consent forms and survey schedules) were reviewed and discussed. The documents were revised based on feedback and recommendations on content (number/wording of questions) and format (layout, font style/size and space for comments). Members of the autism community attending focus groups received vouchers to cover costs and thank them for their time.
During a stakeholder community dissemination event, we presented the study findings to autistic adults and relatives in the North-East UK region who had participated.
Stage 1 Results
Participant characteristics
Detailed information on the characteristics of participants is described in the main text and online Supplementary Materials of the related article (Wigham et al., 2022). A brief summary is presented here. Participants comprised 343 (51.4% response rate) autistic adults (four being consultees/proxies) including 194 females and 137 males (mean age = 43.2; SD = 13.0; range 19–89 years). The mean age of participants who received an autism diagnosis was 40.8 (SD = 12.8) years. Adults educated to post-graduate level comprised 19.8% of the sample; 13.1% were educated to school-leaving qualifications. One-third of adults (101, 29.4%) were unemployed, and 143 (41.7%) were in employment; the remainder of adults who responded to this question were volunteers (20, 5.8%), retired (19, 5.5%) or in supported-employment (9, 2.6%). Just under half (161; 46.9%) were not currently in a relationship. Mean SRS-2 total scores for the autistic adults were 114 (SD = 25); SRS-2 clinical cut-off score for autism is 65 (Constantino & Gruber, 2012). Adults reported co-occurring physical and mental health conditions. Thirty-nine (11.4%) self-reported obsessive-compulsive disorder (OCD), 196 (57.1%) depression and 11 (3.2%) reported problems with drugs/or alcohol. Regarding physical health conditions: 104 adults (30.3%) reported sleep problems, 83 (24.2%) gastro-intestinal problems, 63 (18.4%) asthma, 45 (13.1%) arthritis and 37 (10.8%) high cholesterol.
We compared key characteristics (including gender, age, autism traits (SRS-2 scores) and self-reported diagnoses of depression/anxiety) of autistic adult participants (responders) with those from the ASC-UK cohort who were invited to complete a survey but did not participate (non-responders). Responders were significantly older (median age 42 years) than non-responders (median age 37 years) (U = 61, 204; p = 0.001). There were no between-group differences in SRS-2 scores (U = 31,351; p = 0.56). Responders more frequently had a self-reported diagnosis of anxiety (199, 58.0%) (Χ2 (1) = 3.95; p < 0.05) and/or depression (196, 57.1%) (Χ2 (1) = 3.41; p < 0.05) than non-responders. The ratio of women to men was slightly higher among responders (56.5%) (Χ2 (2) = 7.83; p < 0.05).
Forty-five relatives completed a relatives’ survey about the autistic person they reported to ASC-UK about. The autistic people comprised 36 (80.0%) women, average age 58.3 years (range 25–79). Thirty-two relatives were parents (71%), 9 (20%) were partners. Relatives described the autistic adult they were reporting about as single (27, 60%), married (7, 15.6%), living with parents (20, 44.4%), unemployed (28, 62.2%), educated to school-leaving (24, 53.3%) and post-graduate qualifications (6, 13.3%).
Clinicians represented a range of services including specialist autism teams (16, 45.7%), community mental health (9, 25.7%), learning disability (4, 11.4%), neurodevelopmental (1, 2.9%), forensic (3, 8.6%) and private (2, 5.7%). Fourteen clinicians were psychiatrists (40.0%), 16 clinical psychologists (45.7%) and five (14.2%) were nurses, speech and language therapists or senior autism practitioners. Further details on the characteristics of participants can be found in the related article (Wigham et al., 2022).
Characteristics of support/services received after assessment: adults and relatives
A follow-up appointment is recommended (NICE, 2012; Table S1) and around half of the adults (182, 53.1%) and relatives (26, 57.8%) reported receiving a follow-up appointment with the diagnostic team to discuss implications of an autism spectrum diagnosis (Table S2). Regarding follow-up appointment timing, 40.5% of adults (139) and 46.7% relatives (21) had this less than 12 weeks after diagnosis. Around 60% of adults (195, 56.9%) and relatives (27, 60.0%) were able to discuss what support might be beneficial. Over half of adults (185, 53.9%) but fewer relatives (20, 44.4%) reported an opportunity to discuss the impact of diagnosis (e.g. strengths/difficulties, impact on work/career and relationships). However, a large minority of adults (148, 43.1%) and relatives (13, 28.9%) did not have a follow-up appointment.
The majority of adults (324, 94.4%) and relatives (38, 84.4%) reported that getting a diagnosis had made a difference. One-third of adults (108, 31.5%) and relatives (15, 33.3%) reported getting a diagnosis affected access to other services; just over half of adults (186, 54.3%) and relatives (28, 62.2%) said it had not. Example comments are shown in Table S3. Detailed analysis of qualitative findings regarding the impact of getting a diagnosis and access to other services are described separately (Wigham et al., in preparation).
Characteristics of support/services provided after assessment: clinicians
Twenty-two clinicians (62.9%) reported having resources to offer further support/advice after a follow-up session.
Support/services received within 12 months after diagnosis: autistic adults and relatives
At most around a third of adults and relatives reported receiving any of the types of support listed in the survey during 12 months after the autism spectrum diagnosis (Table 1). Mental health support (e.g. psychological therapies) was received by 117 adults (34.1%) and 12 relatives (26.7%), while the majority of adults (222, 64.7%) and relatives (26, 57.8%) reported receiving no support in this area.
Support/services received by autistic adults within 12 months after the autism spectrum diagnosis as reported by autistic adults and relatives.
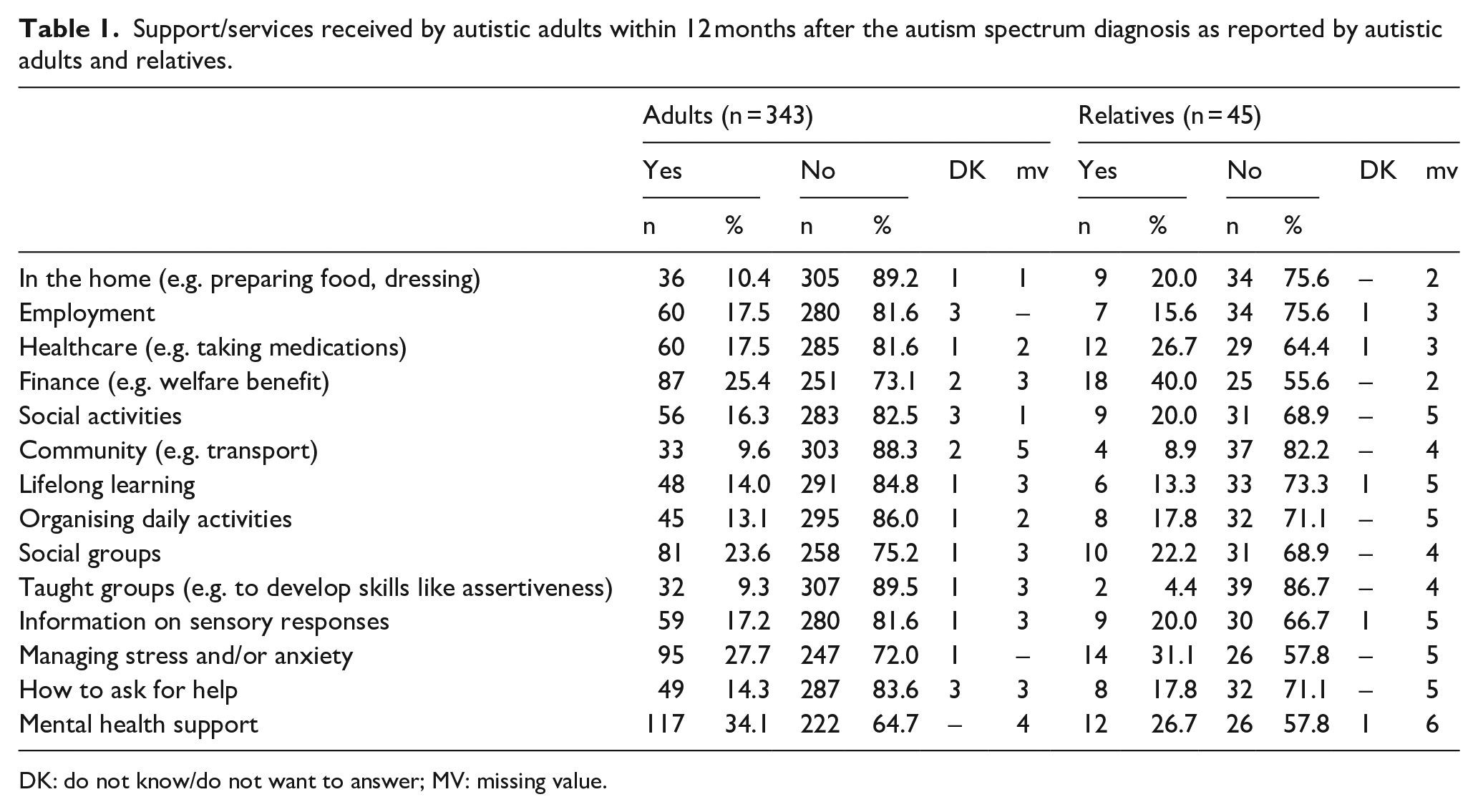
DK: do not know/do not want to answer; MV: missing value.
A minority of participants reported receiving support with employment (adults: 60, 17.5%; relatives: 7, 15.6%). Most adults (285, 81.6%) and relatives (29, 64.4%) were not receiving support with healthcare or how autism might impact physical health (adults: 313, 91.2%; relatives: 32, 71.1%).
Support/services provided within 12 months after diagnosis: clinicians
Despite the observation that just over 70% of clinicians were employed in Specialist Autism Teams and Adult Community Mental Health Services, and the majority of clinicians describing themselves as psychiatrists or clinical psychologists, fewer than half of clinicians (16, 45.7%) reported providing any preventive interventions to support the well-being of people with autism spectrum disorder not in crisis. Furthermore, fewer than half of clinicians (16, 45.7%) reported treating co-occurring health conditions identified during a diagnostic assessment. Many clinicians reported referring onwards including primary care (15, 42.9%), Improving Access to Psychological Therapies (IAPT) (16, 45.7%) and community mental health (19, 54.3%) regarding co-occurring conditions identified during a diagnostic assessment (Table S4).
Some respondents provided comments about lack of specific funding and clinical resources for post-autism assessment interventions (Table S3).
Stage 2 Methods
Modified Delphi Process Rounds 1 and 2
Participants
Clinicians participating in the Stage 1 survey (n = 35) were invited to participate in a modified Delphi process.
Measures
A total of 11 statements describing characteristics of optimum adult post-autism diagnosis support/services were developed (Table 2). The development of the statements was informed by published literature including UK NICE CG documents and aspects of services commonly considered sub-optimal in Stage 1 surveys. For example, gaps in professional members of the core MDT, lack of clear post-autism diagnosis pathways, limited strategic approach to post-autism diagnosis service provision, barriers to service access (e.g. secondary mental healthcare) and limited availability of adapted interventions. The 11 statements were circulated to participating clinicians in the Delphi round 1. Each statement was followed by a Likert-type-style response option from 1 (strongly disagree) to 9 (strongly agree). The response options (1–9) were informed by Delphi survey methodology, and methods of developing CGs/important outcome indicators (Alwin & Krosnick, 1991; Guyatt et al., 2011; Williamson et al., 2017). An open-text box allowed participants to make comments/suggestions for modifying statements.
Statements describing optimal post-diagnosis service characteristics in rounds 1 and 2 of the modified-Delphi process.
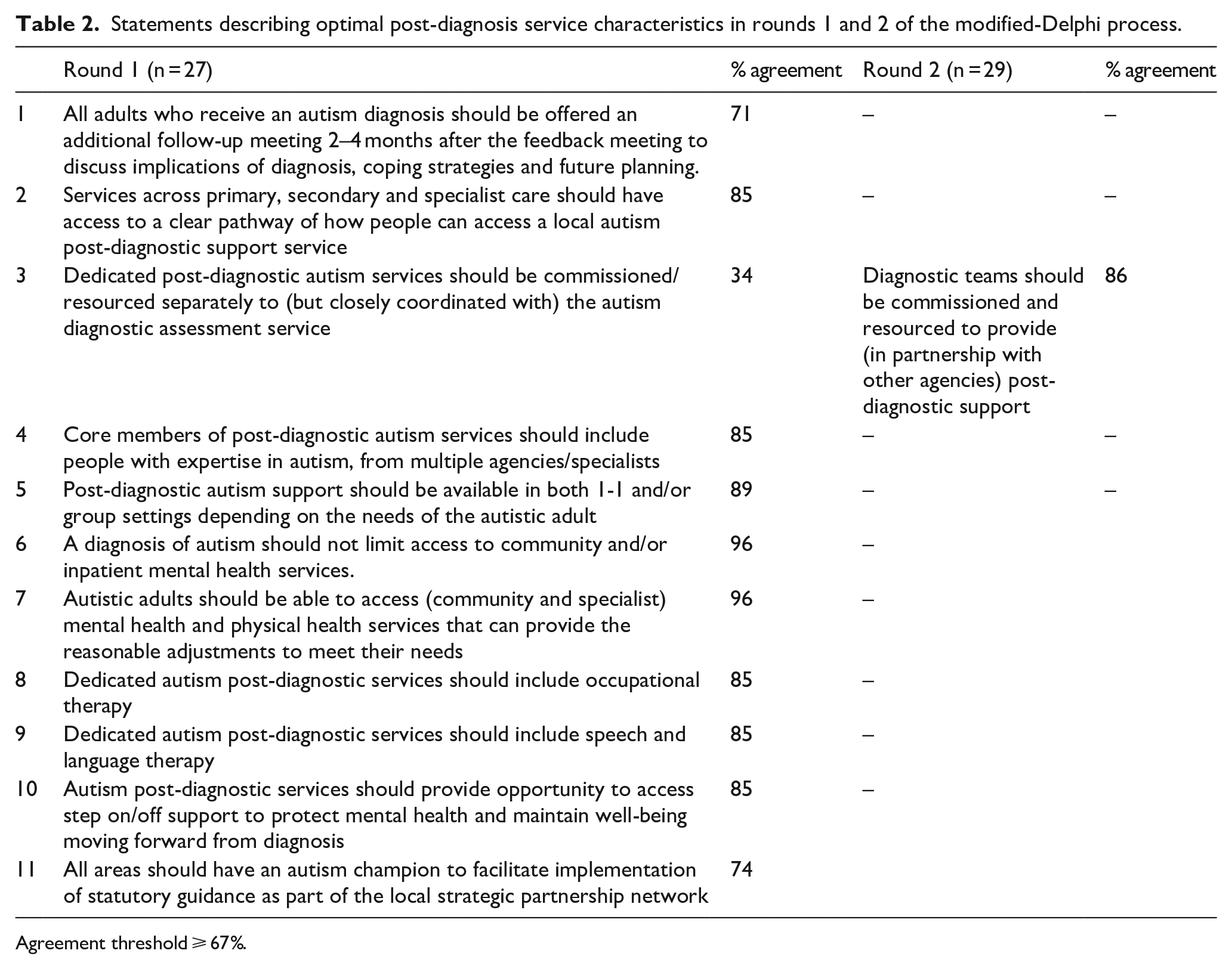
Agreement threshold ⩾ 67%.
Procedures
Qualtrics software was used for the online Delphi process. Statements were sent by email; participants were asked to respond within 2 weeks.
Following round 1, we retained statements on which there was agreement and revised the wording of statements falling below an agreement threshold using Delphi participants’ open-text comments. During round 2, participants were presented with and asked to re-rate revised statements using the same procedure as for round 1. The same 35 clinicians were invited to participate in Delphi round 2.
Data analysis
For both Delphi rounds, we used a pre-specified threshold to appraise agreement on statements (defined as ⩾67% of respondents scoring 7–9) (Sinha et al., 2011). This was based on recommended agreement levels (ranging from 50% to 80%) and published Delphi studies seeking consensus among NHS professionals (Hasson et al., 2000; Morris et al., 2014).
Stage 2 Round 1 and 2 Results
Twenty-seven clinicians completed Delphi round 1, and agreement was achieved on 10 of 11 statements with ⩾67% of respondents scoring 7–9 (Table 2). The research team modified the statement that fell below the agreement threshold taking into account participants’ open-text comments. The modified statement was included in round 2.
Twenty-nine clinicians participated in round 2 and agreement was reached on the modified statement (making a total of 11 agreed consensus statements) (Table 2).
Stakeholder workshops with professionals
Following the Delphi round 2, UK clinicians were invited to join a clinicians’ consultation event. This in-person stakeholder workshop was organised to disseminate the study findings and discuss the final statement set; presentations were made by the research team and an autistic co-investigator.
Discussion
Key findings
This study brought together the recent experiences of three key stakeholder groups (autistic adults, relatives and clinicians) about access to UK adult post-autism diagnosis support/services. Building on this information, we devised 11 statements describing aspects of optimum post-autism diagnosis support/services which were agreed upon by the participating UK clinicians. The stakeholder engagement/dissemination events undertaken with autistic adults, relatives and clinicians, elicited positive feedback regarding the survey findings and statements about optimal service provision and their potential utility for informing service developments and improvements.
While some aspects of the post-autism diagnosis support/services stakeholders had experienced receiving/delivering were viewed positively, in keeping with previous international research, there were significant gaps in service provision, and all stakeholders identified areas that could be improved.
A follow-up appointment with the diagnostic team to discuss implications of an autism spectrum diagnosis is recommended in national guidance (NICE, 2012; Table S1) and found helpful by autistic adults (Jones et al., 2014). However, only just over half of adults and relatives reported receiving a follow-up appointment, and clinicians reported not always being able to provide one. A person recently diagnosed as autistic may need time to consider implications for their life roles: recent studies describe aspects of the significant emotional impact of receiving an autism diagnosis (Huang et al., 2020; Leedham et al., 2020; Powell & Acker, 2016). Furthermore, questions a newly diagnosed autistic person may have for the diagnostic team may well arise later after reflection (Jones et al., 2014).
Many adults and relatives (just under half) in this study said there was no opportunity to discuss what support might be beneficial, for example where to access peer support, or reasonable adjustments when attending primary healthcare (Brice et al., 2021; Crane et al., 2021). The first consensus indicator of optimal services agreed by all stakeholders extended on NICE CG (NICE, 2012) (Table S1) by recommending that adults receiving an autism diagnosis be offered an additional follow-up meeting 2–4 months after the initial diagnostic feedback meeting, to discuss diagnosis implications, coping and future planning (Statement 1).
Research suggests key barriers to providing post-autism diagnostic support/services are both the lack of pathways (which require development) and limited availability of interventions (which require adaptation). One particular problem for clinicians is who/wherein primary and/or secondary care to sign-post autistic adults for co-occurring mental/physical health conditions (Crane et al., 2019; McMorris et al., 2019). In this study, although more than 50% of adults reported having co-occurring anxiety and/or depression, only 34% were receiving mental health support. However, all stakeholders agreed that an indicator of optimal service provision was a clear pathway to local post-diagnostic support across primary, secondary and specialist care (Statement 2).
A separately agreed indicator of optimal services provision was that diagnostic services be commissioned/resourced to provide post-autism diagnostic support in partnership with other agencies (Statement 3). This would likely require additional resources and evaluation of service provision, but given the lack of clear pathways identified might enable provision of continuity and flexible support/care, acknowledged in CG as important aspects of best practice (NICE, 2012; Table S1).
The employment rate of the sample (41.7%), although relatively encouraging compared to reported rates from the UK Office for National Statistics (ONS) rate of 22%, is low compared to overall UK national levels (75.3%) (ONS, 2021) and few adult participants (17.5%) reported receiving employment support. This accords with limited employment opportunities/gaps in employment support for autistic people identified internationally (Frank et al., 2018; Harvery et al., 2021; Maras et al., 2021). An indicator of optimal services extending on detail in CG (NICE, 2012) was that core members of post-autism diagnostic services include people with expertise in autism, from multiple agencies (Statement 4) which could include employment/human resources experts who could contribute to this aspect of service provision, for example, advising on adapting interview questions and workplace environments (Harvery et al., 2021; Maras et al., 2021).
Post-diagnostic support programmes (e.g. psychoeducation) for autistic people are currently being developed (Beresford & Mukherjee, 2021). Identification with social groups has been found to promote positive mental well-being for autistic people (Maitland et al., 2021) and providing post-autism diagnostic support in group settings (Statement 5) may facilitate this and is in accordance with CG (NICE, 2012; Table S1). Future research is needed to explore what types of groups would be most helpful and how these may be delivered, for example, autistic-led peer-support groups (Crane et al., 2021; Leedham et al., 2020) or adapted social prescribing (Charlton et al., 2021; Crompton, Hallett, et al., 2020; Crompton, Ropar et al., 2020; Maitland et al., 2021). Individual support may also be informed by recent developments in psychological therapies for autistic people experiencing anxiety/depression (National Autistic Society, 2021; Parr et al., 2020; Russell et al., 2019).
An indicator of optimal service provision was that a diagnosis of autism should not limit access to community and specialist mental and physical health services (Statements 6 and 7). This is a problem for some autistic people who experience gaps in service provision, for example, community mental health staff lacking confidence to adapt interventions for autistic people (Maddox et al., 2019) and reasonable adjustments may not be available (Brice et al., 2021).
The endorsement of Statements 8 and 9 (regarding inclusion of Occupational and Speech and Language Therapists in post-diagnostic teams) shows teams value MDT colleagues (responder teams most commonly included Psychiatrists and Clinical Psychologists). The expertise brought to services by members of the MDT is accepted, and specific expertise is needed to advise on/deliver some interventions. Guidance should be adapted to ensure MDT and multi-agency professionals, for example, social workers are available to provide appropriate advice/support.
Despite the potential advantages of early interventions (Baker-Ericzén et al., 2018), almost half of clinicians did not provide preventive support for autistic adults not in crisis or treat co-occurring mental health conditions. UK specialist autism teams recently reported needing resources to provide one-to-one support for co-occurring mental health conditions (Beresford et al., 2020); in this study, there was consensus that ‘step-on step-off’ services (so anyone with a known diagnosis does not need a new referral to access the service again) should be provided to protect mental health/well-being (Statement 10).
There is a discrepancy between what clinicians stated they were funded to provide and what they agreed with service users were characteristics of optimal post-diagnosis service provision. This may be contributing to the dissatisfaction described by UK clinicians (Crane et al., 2018) and provides new information regarding the reasons why aspects of NICE CG and QS are not fully implemented. A crucial component to expanding post-autism diagnostic support/services is training others, for example, in primary and secondary mental/physical healthcare, adult social care, IAPT and learning disability services. However, while recommended in national guidance (NICE, 2012; SIGN, 2016; Table S1), research has identified that UK specialist autism services lack resources for cascading expertise via training/consultancy (Beresford et al., 2020; Wigham et al., 2022) again highlighting barriers to implementation of NICE CG and QS.
Finally, European policy research findings and UK national guidance recommend a local lead professional facilitates access to adult autism care pathways and continuity/integration of care across multi-agency (e.g. employment, social care) support systems (http://asdeu.eu/) (NICE, 2012; Table S1). In this study, an indicator of optimal services was having a key person to facilitate the implementation of national guidance recommendations and advocate for autistic people and their access to support/services across different agencies/sectors (Statement 11) indicating the continued relevance of this recommendation.
Strengths and limitations
A definite strength of this study is combining recent experiences of three key stakeholders (autistic adults, relatives and clinicians) to better understand current practice. Our sample consisted of a large number of male and female autistic adults and relatives, across a wide age range together with clinicians from different UK adult autism diagnostic service settings. The study focused on adults receiving a diagnosis of autism in the last 5 years, and asked about the support received within 12 months immediately after diagnosis. The study contributes to the existing knowledge base by triangulating perspectives of key stakeholders recently accessing/providing adult autism pathways in the United Kingdom, facilitating a view of current issues/concerns regarding post-autism diagnostic support/services. Furthermore, by using these perspectives to inform consensus statements describing optimal post-autism diagnostic support/services, the study offers contemporaneous information captured since the publication of NICE CG/QS (NICE, 2012, 2014) relevant to those designing post-autism diagnostic service provision.
The statements describing the characteristics of optimal post-autism diagnosis support/services and evaluated during the Delphi process were derived from information gathered from each stakeholder group (autistic adults, relatives and clinicians). Introducing the statements into clinical practice would likely require a change in clinical practice; for this reason, clinicians were invited to take part in the Delphi process (Michie et al., 2005). While the absence of a consumer perspective during Stage 2 could be construed as a limitation, all statements had the endorsement of service users and the purpose of the Delphi was ascertaining whether clinicians could approve the statements as indicators of optimum services.
The clinicians who took part in this research were mainly psychiatrists and psychologists with only 14% described as ‘other disciplines’: indeed, many participants commented on the lack of other professional disciplines within their existing MDT. In line with published guidance emphasising a multi-disciplinary, life-course, holistic approach, clinicians endorsed Statements 8 and 9 recommending that post-autism diagnostic services include occupational and speech and language therapy alongside other professions that may more typically be associated with post-diagnostic services (NICE, 2012; Scottish Strategy for Autism, 2011; SIGN, 2016). UK and Australian clinical guidelines are prescriptive regarding team composition/professional roles within autism assessment and diagnosis while the composition/roles within post-autism diagnosis teams are less well defined (NICE, 2012, 2014; Whitehouse et al., 2018). In this study, many teams were resourced for assessment and diagnosis only. A strength is considering future post-autism diagnosis team composition, for example, speech and language therapists to provide support with communication difficulties and occupational therapists managing sensory sensitivities or engaging in activities of daily living; few adults in this study described receiving support in these areas (Cummins et al., 2020; Tavassoli et al., 2014; Tomchek et al., 2015).
While few adults and relatives reported they had received/were receiving any of the types of support listed in the survey during 12 months after the autism spectrum diagnosis, it was not ascertained via the closed/multiple-choice questions reported here whether respondents were offered/or interested in receiving these types of support. However, there was an opportunity to comment on this in the open-response questions. These verbatim comments are being explored separately (Wigham et al., in preparation). The ratio of women to men is slightly higher in this sample (56.5%); this differs from rates reported in prevalence studies, but recognising that autism diagnoses may be missed more frequently in women than in men (Brugha et al., 2016), the roughly equal number recruited in this sample facilitated a balanced representation of perspectives of both genders on adult post-autism diagnosis support/services. The majority of participants in this study self-reported as White-British. Future research should investigate how/whether different ethnic groups currently access services and the types of post-autism diagnostic support/services that would be helpful for other ethnic groups (NICE, 2012). Some autistic adults whose needs cross/intersect service boundaries and/or other minority community groups (e.g. gender identity, mental health and ethnicity) may experience marginalisation (Fletcher-Watson et al., 2021). There is emerging literature describing difficulties in accessing medical/healthcare benefits experienced by autistic people from minority ethnic groups (Benevides et al., 2021; Tromans et al., 2021).
Future research
Given the gaps in post-diagnosis support/service provision identified by the autism community, published research to date and stakeholders in this study, a key area for future research is understanding more about how/when post-diagnostic support could be provided. Given the relatively wide age range of adults at the time of receiving an autism diagnosis, it would be useful to explore in more detail the experiences and types of support across different age-groups and levels of ability. Investigation of whether help-seeking preferences differ depending on gender is also an area for future research. To progress this work, the priorities of autistic adults and the autism community should inform co-designed research processes (Fletcher-Watson et al., 2021). Research findings can then promote the development of new approaches to post-diagnostic support across statutory healthcare services and other agencies through personalised care. For example, psychological therapies adapted for autistic people experiencing mental health conditions (Parr et al., 2020) or social prescribing informed by research on peer-to-peer information transfer and rapport between autistic people (Crompton, Ropar et al., 2020; Maitland et al., 2021). Methods of effectively and sustainably integrating support/services appropriate for autistic people into existing broader complex care-system structures require investigation (SIGN, 2016). Implementation science and realist approaches could inform the development of support networks/pathways able to provide the necessary comprehensive and relevant multi-agency collaborations (Baker-Ericzén et al., 2018; Michie et al., 2014; Pawson et al., 2005; Snell-Rood et al., 2020). One example of support highlighted in this study with potential for development informed by implementation science methods is the provision of mental health services. In accordance with prior research (Beresford et al., 2020), there was agreement across all stakeholders that mechanisms to integrate step-on-step-off approaches involving specialists and other community services would benefit those autistic people with an already identified mental health condition. The development of support/service provision could also be informed by models of care for long-term health conditions, the key components being self-management, case-management and specialist stepped-care (Green, 2019).
Conclusion
A decade after the publication of NICE CGs, significant gaps in post-autism diagnosis service provision persist. We have compared current experiences and clinician perspectives with clinical guidance (NICE, 2012, 2014; Table S1); our consensus statements while in keeping with previously published literature add weight and provide new perspectives and insights. Bringing together key stakeholders and achieving agreement on what constitutes optimum provision is an important contribution, especially as the findings build on the existing UK and other available international clinical guidelines. The 11 statements provide pragmatic recommendations for improving existing community-based post-autism diagnosis provisions. The survey responses, and consensus statements endorsed by all stakeholders describing characteristics of optimal adult post-autism diagnosis support/services, are of immediate relevance to UK commissioners and may also be useful for international service providers to inform service developments and quality initiatives. The findings in turn may well contribute to improving experiences and outcomes for adults receiving an autism diagnosis in adulthood.
Supplemental Material
sj-docx-1-aut-10.1177_13623613221097502 – Supplemental material for Consensus statements on optimal adult post-autism diagnosis support and services: Delphi process following a UK survey of autistic adults, relatives and clinicians
Supplemental material, sj-docx-1-aut-10.1177_13623613221097502 for Consensus statements on optimal adult post-autism diagnosis support and services: Delphi process following a UK survey of autistic adults, relatives and clinicians by Sarah Wigham, Barry Ingham, Ann Le Couteur, Colin Wilson, Ian Ensum and Jeremy R Parr in Autism
Footnotes
Acknowledgements
The authors are grateful to the research participants, Dr Alex Petrou and Professor Helen McConachie for their work on the Adult Autism Spectrum Cohort-UK, to administrators Faye Wolstenhulme and Carla Black, and to Deborah Garland (National Autistic Society) for advice and support with the consultation groups.
Authors’ Note
We use the term autism throughout the article to describe the diagnoses such as autism spectrum disorder, autistic disorder, autism spectrum conditions, atypical autism, Asperger’s Syndrome and PDD-NOS. We use the term ‘autistic adults’ to describe adults with a range of autism spectrum diagnoses.
Author Contributions
JRP, ALC and BI were awarded funding. JRP was the chief investigator. JP, SW and ALC wrote the first draft of the article. All authors contributed during the editing and reviewing process and also approved the final article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The authors are grateful to the UK autism research charity Autistica, who funded the study as part of the Autism Life Course and Ageing research programme at Newcastle University, and to Cumbria, Northumberland Tyne and Wear NHS Foundation Trust for sponsoring the research, and providing funding through Research Capability Funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.