
Abstract
Emerging evidence suggests parenting supports implemented in the first 2 years of life may influence developmental outcomes for infants more likely to be Autistic. Yet questions remain about acceptability of these supports to the Autistic and autism communities. Through mixed-methods participatory research – co-designed and produced by Autistic and non-Autistic researchers – we sought diverse community perspectives on this topic, including to understand the relative acceptability of different support options. A total of 238 participants completed our online survey: 128 Autistic and 110 non-Autistic respondents, some of whom also self-identified as parents of Autistic, otherwise neurodivergent, and/or neurotypical children, and/or as health/education professionals and/or researchers. Most participants agreed that very-early-in-life approaches should help parents understand and support their children, and disagreed that these should seek to suppress autistic behaviour. Most agreed with the goal of respecting infant autonomy, and that parent education towards creating sensitive, accommodating environments could be appropriate, albeit with nuanced differences-of-opinion regarding the acceptability of specific therapeutic approaches. Participants generally endorsed the terms ‘support’ (vs ‘intervention’) and ‘early-in-life’ (vs ‘at-risk’/‘pre-emptive’). Engaging equal-power partnerships for the development, delivery of, and discourse around early-in-life autism supports will ensure end-user community values and needs are respected.
Lay abstract
Most support programmes for Autistic children are available only after they are diagnosed. Research suggests that parenting supports may be helpful for parents and their infants, when provided in the first 2 years of life – before a formal diagnosis is given, but when information suggests an infant is more likely to be Autistic. However, we do not know how acceptable these types of supports might be to the Autistic and autism communities. We asked 238 Autistic and non-autistic people – some of whom were parents, and some of whom were professionals working in research, health and education – about their perspectives on very-early supports. People generally agreed that it could be acceptable to work with parents to help them understand and support their child’s specific needs and unique ways of communicating. People suggested a variety of support strategies could be acceptable, including parent education, changing the environment to meet an infant’s needs, and creating opportunities for infants’ to make choices and exercise control. People preferred respectful and accurate language – including the term ‘support’ (rather than ‘intervention’) and ‘early-in-life’ (rather than ‘at-risk’ of autism, or ‘pre-emptive’ when describing developmental stage). Continuing to work with community members will help to make sure autism support programmes are relevant and helpful.
Introduction
Many Autistic children access early-in-life developmental supports, mostly post-diagnosis. However, with increasing knowledge of early autism behaviours there is growing interest in the potential of pre-diagnostic supports – services for infants more likely to be Autistic, whether they have an Autistic/neurodivergent family member or are showing emerging autism behaviours. While elsewhere variously referred to as ‘pre-emptive’ or ‘prodromal’ and ‘intervention’, here we use ‘very early’ or ‘early-in-life’ and ‘support’ when referring to services offered in the first 2 years of life.
Efficacy of very-early supports
Emerging research on the efficacy of very-early autism supports shows mixed findings across studies and support types. Three recent systematic reviews/meta-analyses have synthesised results from primary studies of early-in-life supports described as Developmental Interventions (DIs)/Naturalistic Developmental Behavioural Interventions (NDBIs; Hampton & Rodriguez, 2022; Law et al., 2022; McGlade et al., 2023). All sought to skill parents to respond supportively to their infant’s neurodivergent communication behaviours and/or building engagement through joint activities and play. Most were low-intensity (0.5–3 h/week) and primarily parent-delivered, although two studies described higher-intensity and primarily clinician-delivered programmes (15–20 h/week). Among these, two reviews examined parent-related outcomes (Hampton & Rodriguez, 2022; Law et al., 2022) finding significantly increased parental use of target strategies at immediate programme completion.
All three reviews also examined child-related outcomes, consistently reporting small, non-significant reduction in infants’ autism features, nor particular effects on other developmental outcomes (Hampton & Rodriguez, 2022; Law et al., 2022; McGlade et al., 2023). Developmental theorists suggest, however, that null short-term effects do not necessarily reflect programme inefficacy (Green, 2022, 2023; Whitehouse, 2023). Rather, cumulative benefits of small initial changes in parent–child interaction might only become evident with time. Indeed, long-term follow-up of two cohorts – both investigating the same approach – have suggested low-intensity (~10 h across 5 months) early-in-life support might have an initially small but cumulatively significant impact, reducing autism-related disability by early-childhood (Green et al., 2017; Whitehouse et al., 2021).
Acceptability of very-early supports
Successful programme implementation requires acceptability to community members, including programme deliverers and intended beneficiaries (Sekhon et al., 2017). Acceptable programmes will more likely be delivered as intended (i.e. with high fidelity), and sessions more likely attended and recommended strategies more likely adopted by end-users, thereby leading to improved outcomes (Proctor et al., 2009; Sekhon et al., 2017).
Rise of the neurodiversity movement has increased recognition of the value of involving Autistic people in research, and prompted reconsideration of how support effectiveness is determined and of whether current practices align with the priorities and needs of intended beneficiaries (here, the Autistic community; Leadbitter et al., 2021). The appropriateness of early-in-life autism supports is considered in several recent commentaries, addressing issues like the appropriateness of intended aims/outcomes (Dawson et al., 2021, 2022; Manzini et al., 2021), behavioural strategies/techniques (Anderson, 2023; McGill & Robinson, 2021; Mottron, 2017), and the population involved (MacDuffie et al., 2021). These highlight the ethical complexity and potential risk to community when well-intentioned programmes are misaligned with preferences and need.
There has been little direct community consultation on the acceptability – to Autistic (self-identified and diagnosed Autistic adults, including those who are parents/caregivers) and autism community (non-Autistic parents/caregivers, professionals, and researchers) members – of early-in-life autism support. The scant existing research focuses primarily on non-Autistic parent and/or service provider views (Pickard et al., 2016; Stone et al., 2021) and views from parents of older Autistic children (Jurek et al., 2023; Wei et al., 2023). Notable exceptions are studies on the general appropriateness of support goals for Autistic pre-schoolers (Baiden et al., 2024; Waddington et al., 2024) and a specific investigation of Autistic adults’ views on the acceptability of pivotal response treatment (PRT) as a particular early childhood support (Schuck et al., 2024).
Waddington et al. (2024) and Baiden et al. (2024) identified high-priority goals including promoting child safety, independence and quality of life, such as enabled child participation, compared to low-priority goals including specifically targeting play skills and autism characteristics (e.g. increasing eye contact, reducing intense interests, stimming, and so on). When reflecting on PRT session videos, Autistic adults engaged by Schuck et al. (2022) shared perspectives on the importance of following the child’s lead, personalising delivery, monitoring affect, and trying to understand the child’s perspective, but expressed concerns about the pursuit of specifically spoken (vs any functional) communication, including that child attempts to communicate differently were sometimes ignored.
This study
While recent articles document insights on the acceptability of early childhood supports, it is unclear how these findings might translate to the context of supports developed for and implemented with infants, pre-diagnostically. We sought perspectives on very-early-in-life supports for infants more likely to be Autistic, with a primary aim of understanding aspects potentially more/less acceptable to the Autistic and autism communities across therapeutic aims/outcomes, strategies/approaches, delivery methods, target populations and the language used to describe such programmes. As a secondary aim, we considered similarities and differences in the perspectives of Autistic and non-Autistic stakeholders.
Methodology
Community involvement and positionality
Autistic and non-Autistic researchers co-produced this research, collaboratively developing research questions, drafting and disseminating the survey, and interpreting results. A core project team of five Autistic and non-Autistic adults (with intersecting identities including, but not limited to, parents, clinical professionals, formally trained researchers) led the study through fortnightly meetings for ~12 months, while a larger international (Australia, United States, United Kingdom and India) working group of 24 Autistic and non-Autistic adults (with intersecting identities as above) also met three times (six paired meeting options) to discuss key issues (design, ethical considerations, survey content, findings). Members of the working group consented to have their input recognised via co-authorship and/or acknowledgement.
Design and participants
This mixed-methods, single time point survey study (approved by La Trobe University Human Ethics Committee; Ref HEC22081) was for participants identifying as any of Autistic, parent/carer of Autistic child or child more likely to be Autistic, professional/service provider working with Autistic children/families, and/or autism researcher. Participants indicated informed consent online ahead of the survey.
Measure and procedure
The purpose-developed survey (see Supplemental material) included items informed by group members’ knowledge of supports for Autistic children and items reflecting potentially topical/divisive issues. Participants first identified their perspective/s (e.g. as Autistic, a parent, and so on) and whether they had heard about supports/therapies for infants with social-communication differences or family autism history (i.e. infants aged 0–2 years more likely to be Autistic, but unlikely yet assessed/formally diagnosed). Thereafter, items were organised in five main sections – aims/outcomes, delivery, suitable populations, strategies/techniques and descriptive language. A final section captured further respondent demographic information. Each key section comprised optional fixed-response items (i.e. five-point Likert-type scale; strongly agree to strongly disagree) and free-text fields (i.e. prompting elaboration/additional considerations). The survey neither named nor described any specific support programme, seeking participants’ ratings of the acceptability of distinct programme features based on their own (and not our) perceptions of what these might involve.
The online survey was hosted on REDCap, open August 2022 to March 2023, and distributed via social media channels (and with snowball sampling to encourage broad dissemination) via the core project team and broader working group.
Data analysis
Quantitative analysis (using JASP 17.1) was conducted with data from participants who had completed at least one main survey section (range 20%–100% complete; M = 93%). Missing data were not imputed; item-level sample sizes are reported. Descriptive statistics were calculated for all variables of interest. To aid interpretability, Likert-type scores for each statement were dichotomised for ‘agreement’ (i.e. proportion of participants who agreed/strongly agreed) versus ‘did not agree’ (i.e. neutral/disagree/strongly disagree). Rates of ‘agreement’ by Autistic and non-Autistic participant subgroups were compared via chi-square test (with Mann–Whitney U-tests repeated on the original ordinal data to confirm the pattern of results; see Supplementary Tables S2 to S6). Bonferroni adjustment for multiple comparisons was applied, per section.
To contextualise the quantitative data, free-text responses were summarised inductively, with NVivo software used to assign codes and collate these into preliminary themes, which were further developed and refined through discussion with the project team.
Results
REDCap metadata indicated 402 instances of survey access, 313 (77%) Participant Information/Consent Form views, and 304 (76%) respondents commencing the main survey. Among these 304 participants, 66 (22%) completed only initial questions on role/identity and awareness of very-early-in-life supports (see Supplementary Figure 1), including approximately balanced numbers self-identifying as Autistic/non-Autistic. Compared to the 238 continuing to the main survey, those who ‘discontinued’ were less likely to report having heard about early-in-life autism supports (see Supplementary Table S1).
Participant characteristics
The final sample (n = 238; see Table 1) included approximately equal number of Autistic and non-Autistic respondents. Most Autistic participants indicated they were formally diagnosed. Most participants in each group self-identified as female, but more Autistic than non-Autistic participants identified as non-binary (20% vs 1%). Participants’ ages varied (22–74 years). Approximately half reported residing in Australia, followed by sizeable UK- and US-based subgroups (with no significant Autistic vs non-Autistic subgroup differences in age or country of residence). Most respondents reported University-level education. Respondents also self-identified intersecting identity subcategories – including as parents, researchers, and health/education professionals. Parent participants reported having 1–5 children (M = 1.93, SD = 0.89), including 20 (15%) who were infants (0–2 years) at the time of survey completion. A total of 107 (77%) parents reported having an Autistic child, 47 (34%) an otherwise neurodivergent child, 26 (19%) a child more likely (although not formally diagnosed) Autistic and 35 (25%) a neurotypical child (further to Autistic/neurodivergent child/ren).
Participant characteristics.
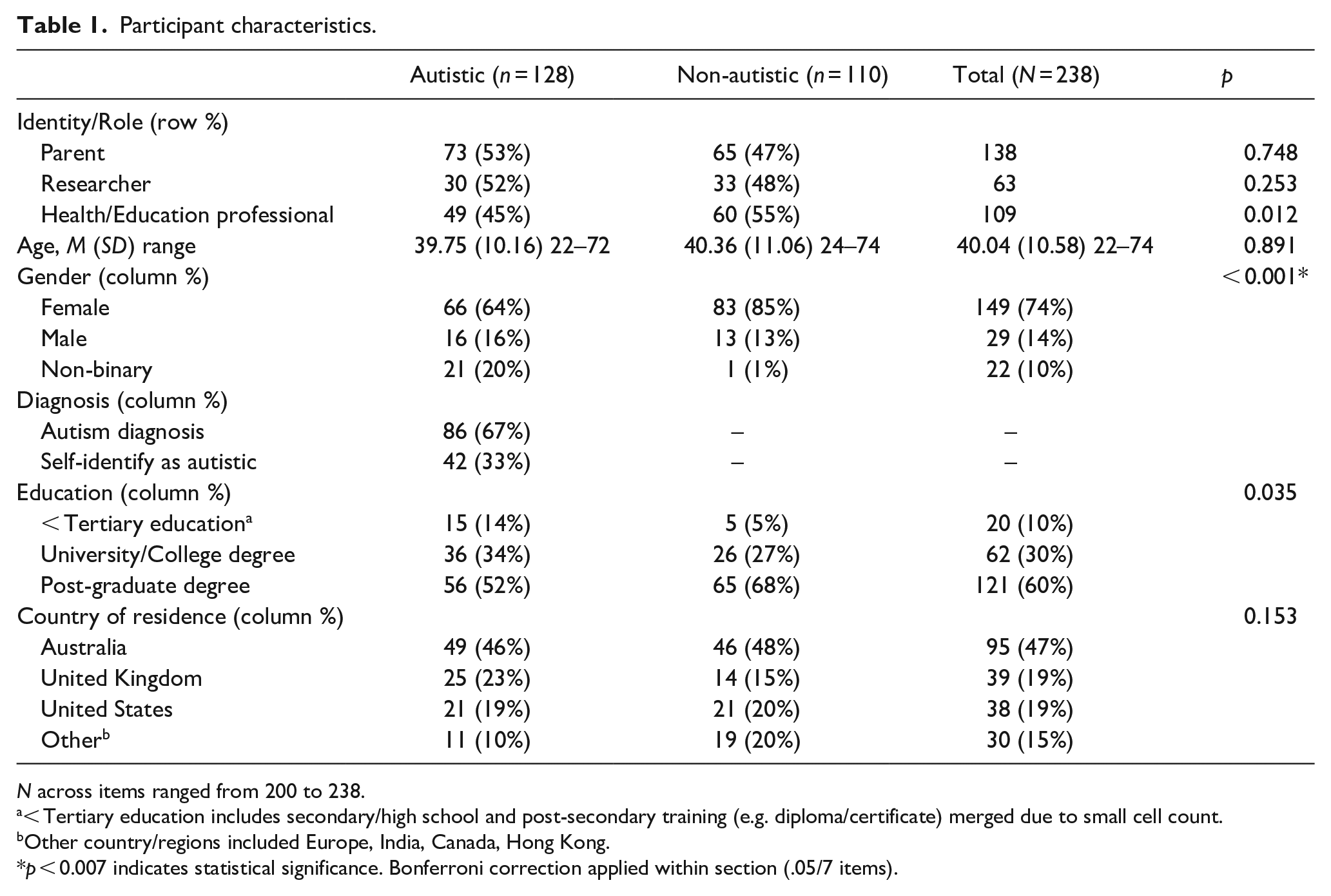
N across items ranged from 200 to 238.
< Tertiary education includes secondary/high school and post-secondary training (e.g. diploma/certificate) merged due to small cell count.
Other country/regions included Europe, India, Canada, Hong Kong.
p
Free-text input to open-ended questions was provided by 193 (81%) respondents. Here, we considered four participant groups – 48 Autistic non-parents [A], 58 Autistic parents [A-Par], 56 non-Autistic parents [NA-Par] and 31 non-Autistic professionals/researchers [NA-Prof]. Figure 1 summarises key themes within each topic area. Example quotes (assigned a random identifier) illustrate response breadth.
Summary of themes within each topic area.
Aims/outcome of very-early supports
Almost all participants ‘agreed’ that early-in-life autism supports should seek to help caregivers understand and/or respond supportively to their infant’s feelings, needs and behaviour, and to improve infants’ quality of life (see Figure 2; Supplementary Table S2). Autistic and non-Autistic participants responded similarly to these highly rated items. Items here with lowest ‘agreement’ were preventing an infant from developing autism, reducing repetitive or other early autism behaviours and encouraging eye contact. Consistently, Autistic participants were significantly less likely than non-Autistic participants to endorse these as ‘acceptable’, albeit with substantial variability within-groups across all items.
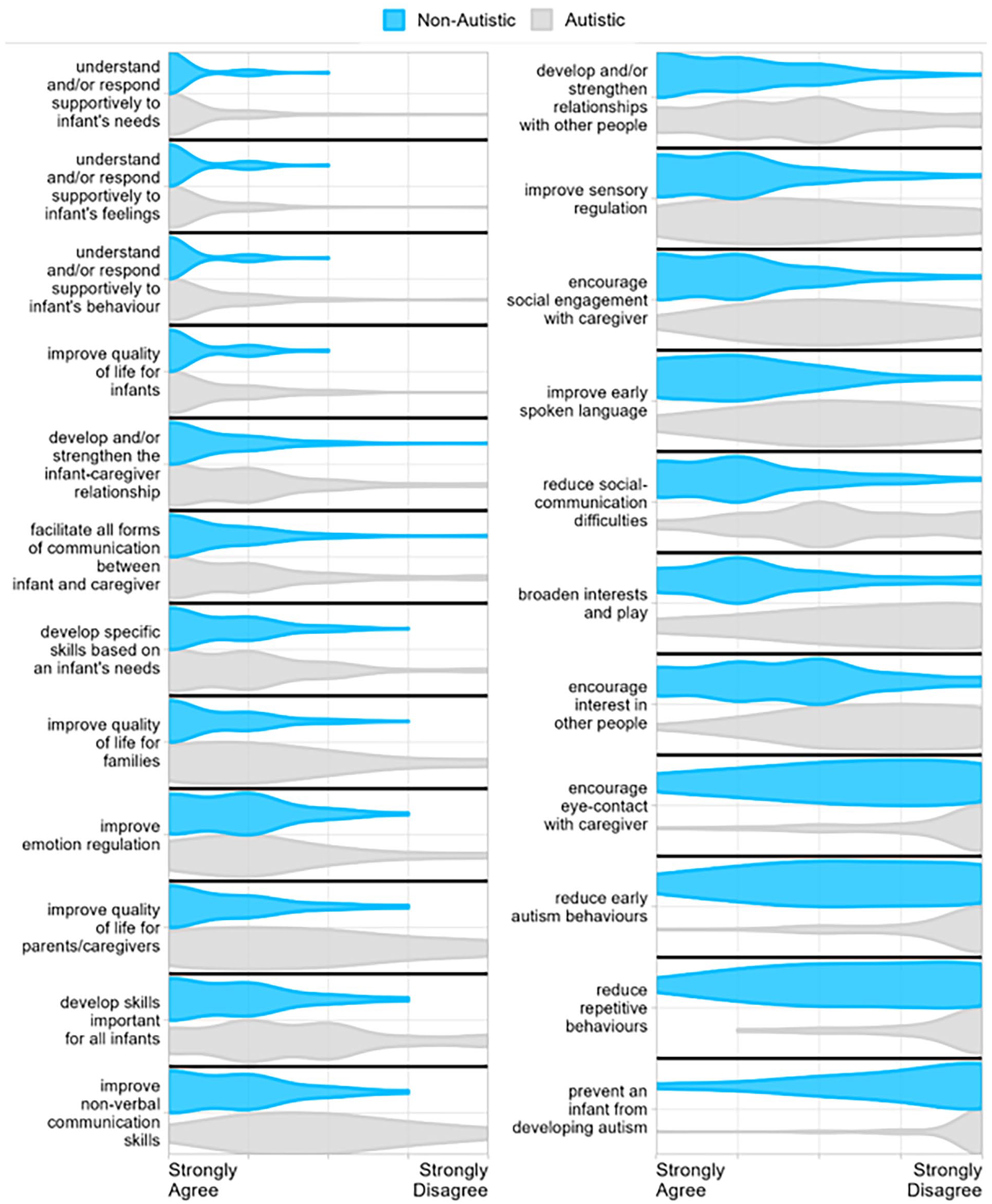
Responses to items regarding aim/outcome of very-early autism support, by descending order of mean ‘agreement’.
Theme 1.1: supporting families to understand and accept their neurodivergent infants
Participants’ free-text responses regarding early-in-life support aims/outcomes indicated ‘the primary goal should be helping caregivers understand and support their infant’s needs’[A175]. By ‘understand[ing] their child’s emotional, social and sensory needs’ families can ‘adjust the environment accordingly’[NA-Par136], ‘reduce stress for the infant’[A-Par154] and ‘create a space where the infant can be their authentic self’[A-Par123]. Participants felt ‘understand[ing] their Autistic babies’ cues . . . help[s] forge a bond where parent[s] communicate in a way baby can understand’[A-Par11] with ‘potential to be transformative for long term [parent-child] relationships . . . [and fostering] acceptance of the child’[NA-Par22]. Providing early support focused on ‘communication skills, parent-child relationship, and parents’ ability to respond to their child in supportive ways’ were also suggested ‘building blocks for supporting and teaching later skills across many domain[s]’[NA-Par147].
Theme 1.2: support for (neurodivergent) parents and families
Participants’ free-text responses also highlighted that early-in-life ‘supports [should be for] the child and their family’[A55], considering ‘the parent’s own neurodivergence, when applicable’[A-Par12]. Support for parents and families was suggested to include ‘ensuring [the] parent is supported to advocate for their child’[NA-Par136] as well as ‘caregiver adjustment to and acceptance of the child’s probable neurodiversity’[NA-Par136]. However, participants indicated efforts ‘should be about supporting the child, first and foremost’[A79] and ‘not focused on the caregiver’[A-Par165] as the needs of parent and family should not outweigh those of the infant: ‘There is nothing wrong with improving [quality of life] for parents . . . if addressed in ways that are supportive of everyone in the family’[A-Par124] and ‘while I am all for
Theme 1.3: supports should not aim to suppress autistic behaviour
Participants were also clear that ‘it is pointless at best – and extremely damaging at worst – to aim to reduce Autistic behaviours [and/or] prevent a child from developing Autism’[NA-Par99] as ‘you cannot make an Autistic child non-Autistic’[A-Par155]. Participants explained that ‘compliance with neurotypical standards should never be the aim or outcome’[A37] but that support for specific behaviours can be appropriate: ‘such as ones that can cause harm or anger but . . . not all Autistic behaviours are bad’[A168]. ‘Stimming might be considered weird by the majority (and therefore negative) but this is [an] important self-soothing behaviour for us’[A36]. Rather than ‘making the child appear less Autistic’[A-Par86] it was suggested ‘to teach Autistic people . . . to work with their Autistic behaviours’[A159]. Currently ‘most interventions use non-Autistic development as the reference . . . [while supports] should be geared toward supporting Autistic development, not “rerouting” the developmental pathway from Autistic to non-Autistic’[NA-Par28]. Indeed, participants expressed that neurodiversity-affirming programmes should ultimately ‘support Autistic ways of being, moving, playing, communicating, socialising’[A30].
Strategies and techniques involved in very-early supports
Most participants agreed that very-early-in-life autism supports should change the environment to meet infant needs, creating opportunity for choice and control, educating parents about autism and promoting positive, warm infant–caregiver interactions (see Figure 3; Supplementary Table S3). Again, Autistic and non-Autistic participants did not differ when strategies/techniques were generally strongly endorsed. Strategies/techniques with lowest overall ‘agreement’ – and where Autistic participants showed lesser endorsement – were around strategies to encourage infants’ communication and behaviours through tangible or social reinforcers, or intentional pauses during enjoyable games/activities. Again, however, substantial respondent variability was evident within both Autistic and non-Autistic groups.
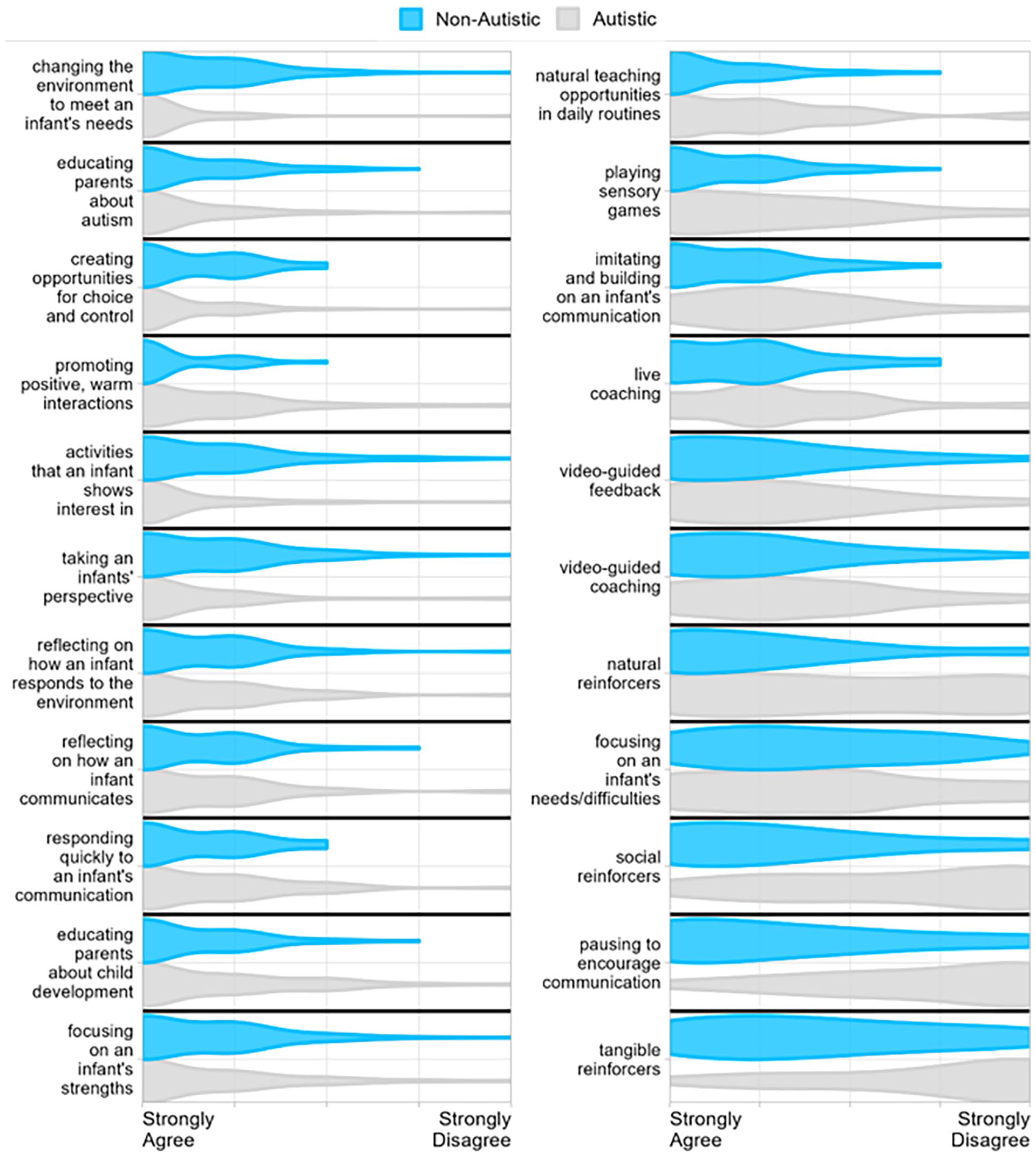
Responses to items regarding strategies/techniques involved in very-early autism supports, by descending order of mean ‘agreement’.
Theme 2.1: creating a supportive environment for the infant
Participants’ free-text responses suggested approaches to working appropriately with families of infants should ‘focus on making the best social/emotional/sensory/physical environment possible in which that child can thrive’[NA-Par136]. Support strategies could therefore ‘consider the environment, and peoples’ responses to the child’[A-Par82] and ‘educating parents; equipping them with the skills to support . . . [and] accommodate the child’s needs’[NA-Par81]. Specific support techniques could include ‘a mixture of watching and reflecting’[A158], ‘promoting mutually enjoyable [interactions] for infants and parents/caregivers’[A116] and ‘family strength-building’[NA-Prof19]. However, the appropriateness of support strategies ‘depends on how they are delivered’[A-Par56]. For example, ‘approaches that emphasise behaviour over relationships’ were considered inappropriate as ‘behaviour can come a little later, after baby and family have [a] good understanding of each other’[NA-Par22]. Similarly, ‘it depends on the type of education the parent is receiving . . .; insisting spoken communication is the only good outcome . . . would be harmful’[A40] while appropriate support could ‘recognise many attempts to communicate are non-verbal, and teach parents to look for their child’s non-verbal cues’[A-Par167].
Theme 2.2: reinforcement can be problematic
Many participants expressed concern that ‘reinforcement can be coercive and problematic . . . needs to be handled with a great deal of care’[A57] and that ‘any kind of ‘behaviour reinforcement’ – with natural rewards or otherwise – is not appropriate’[A-Par182]. Concerns included that ‘this reinforcement language kind of dehumanises children and their means of communication and choices of play’[A-Par86] rather than honouring ‘Autistic infants as young people . . . whose autonomy and authenticity should be respected’[A24]. Similarly, some participants viewed within-game/activity pausing, to encourage communication, as problematic; as ‘“withholding reward” until communication is satisfactory’[A-Par85], where ‘socializing, games, toys etc. should not be a reward contingent on communication . . . just part of healthy life and development for an infant’ and where ‘withholding them when the child does not communicate is actively harmful’[A175]. Others – primarily non-Autistic parents and researchers – viewed this strategy more favourably, framing pausing as a way to ‘allow the infant time and space to contribute to/play a role in the game/activities’[NA-Par136]. Furthermore, some participants suggested reinforcers could be appropriate if carefully applied. For example, ‘we should make experiences desirable and motivating rather than using extrinsic rewards. “Good things” should just happen’[NA-Prof155] and ‘if preferred toys are both rewards and available at other times, then this is okay’[A59].
Theme 2.3: individualised, child-led support
Respondents suggested strategies and techniques should be tailored to individual infant needs, as ‘every child has different needs – the supports need to be bespoke’[NA-Par93] and because ‘highly individualised support . . . [can be beneficial] in helping the parents see the child in front of them for who they are’[A36]. Similarly, ‘following [the] child’s lead and interest in a warm and supportive way’[NA-Par68] was suggested as important to ‘allow the therapy to be guided by the infant’[A79]. Respondents also suggested that working with an infant’s needs and preferences informed an individual’s readiness-to-learn, acknowledging that infants more likely to be Autistic may ‘need more downtime than average, more alone-time . . . more processing and consolidation time, more stimming time’[A-Par154].
Delivery of early supports
Almost all participants agreed very-early autism supports should primarily be delivered in family homes, involve parents supporting infants and be adapted to infants’ individual needs and family circumstances (see Figure 4; Supplementary Table S4). Again, groups did not differ in the proportion of participants endorsing these highly rated items. Autistic participants were less likely than non-Autistic participants to ‘strongly/agree’ that professionals should work directly with infants, and more frequently endorsed Autistic adults working with parents and infants. Supports provided at low intensity, over a longer time frame were endorsed more frequently than high intensity, shorter time frame options. Again, however, substantial within-group spread of responses here was evident.
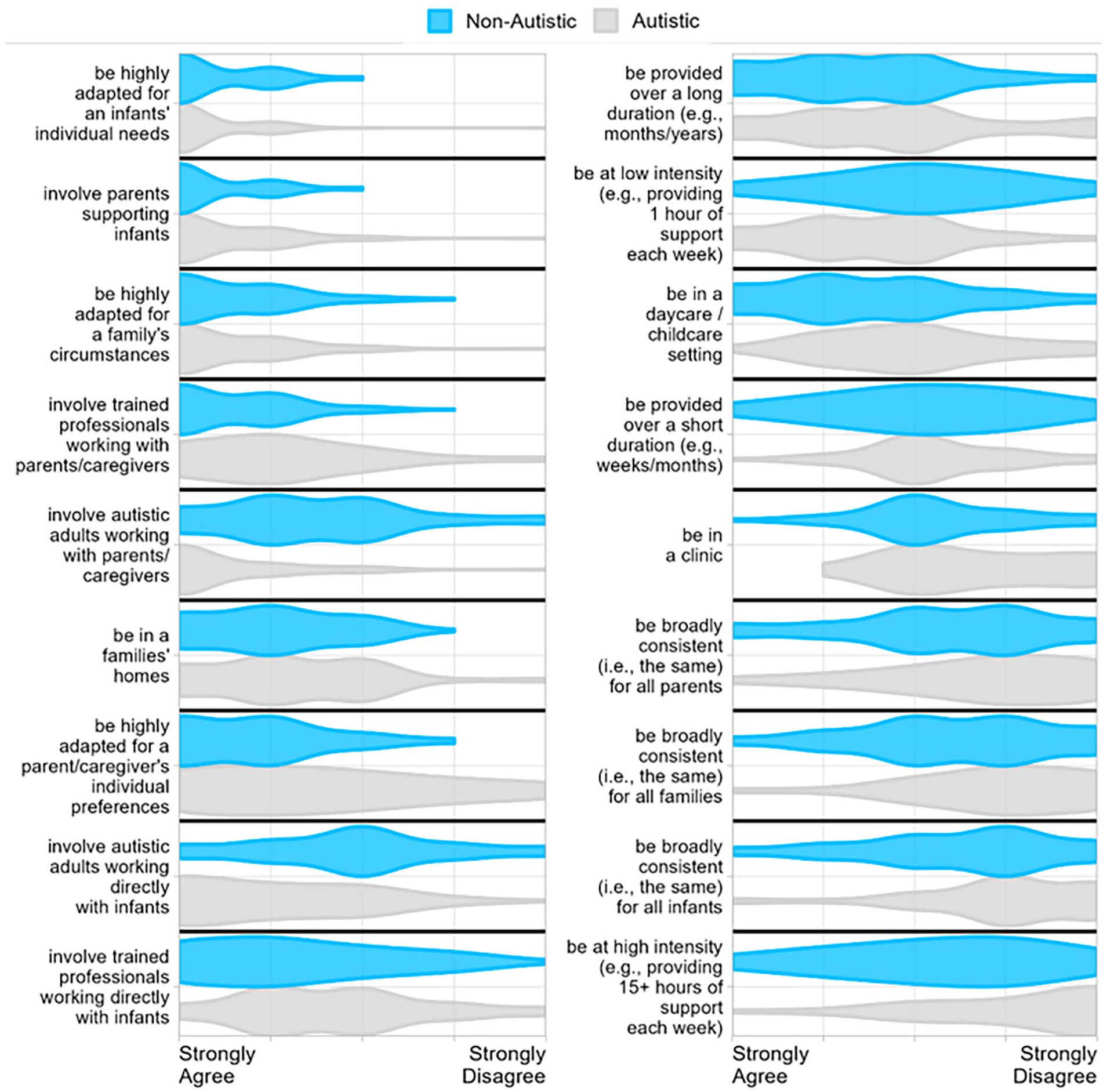
Responses to items regarding the delivery of very-early autism support, by descending order of mean agreement.
Theme 3.1: parent-mediated supports
While free-text responses emphasised that early-in-life supports should prioritise infant wellbeing, participants suggested delivery should harness the ‘team around the child’[A-Par154], involving ‘those most proximal to the infant’[NA-Prof155] including ‘family members like grandparents, older siblings’[NA-Par72]. Respondents explained ‘for children under [age] two, I believe it is often, if not always, appropriate to focus on the dyad’[NA-Par147] because ‘parents are the constant . . . and must be empowered’[A173].
Theme 3.2: ‘neuro-affirming’ approach
Participants emphasised that ‘practitioners delivering [supports] should . . . use a neuro-affirming approach’[A-Par96], ‘know about things like the double-empathy problem’[A166] and encourage families to ‘connect to the Autistic community [to] access peer support’[A36]. The ‘inclusion of Autistic adults in design and delivery of interventions’ was considered ‘very important’[A151] with ‘Autistic professionals . . . ideal, as they have theoretical knowledge [and] lived experience’[A-Par82], and further ‘bonus if they’re an Autistic parent of an Autistic kid’[A20]. Participants also acknowledged the value of Autistic and non-Autistic individuals collaborating: ‘neurotypical and neurodivergent brains have much to offer each other’[NA-Par189].
Theme 3.3: tailored to child and family
Respondents suggested the delivery of support programmes – including the setting and amount of support provided – should be ‘tailored to the child and . . . family’[A-Par75]. While several participants indicated ‘there should be a broad structure or framework . . . [this] should be adapted for individual child, parent and family needs’[NA-Par139] as ‘every infant with autism is different’[A-Par75]. Participants suggested ‘support delivery is best in a familiar and not overstimulating environment’[A175], which could include ‘a mix of online . . . and in-home’ or a ‘variety of settings – homes/clinic-/day-care based – depending upon the infants and their families’[NA-Par76]. Group-based education was also advocated for ‘the benefit of meeting other families’[NA-Prof32]. The amount of support provided ‘will depend on the family’[A-Par13] as some ‘require much more support than others’[NA-Prof32]. However, it was important to participants that ‘the child is not deprived of opportunities because of supports put in place’[NA-Par136]; ‘there needs to be balance’[A18] as ‘high-intensity programmes are very tiring for infants . . . [needing] plenty of time to rest and process’[A-Par21].
Infants/families suitable for very-early supports
Most participants agreed autism supports are suitable for infants and children of any age, with a confirmed diagnosis or showing early autistic behaviours, and for infants showing signs of broader neurodivergence such as attention deficit hyperactivity disorder (ADHD; see Figure 5; Supplementary Table S5). Items with the lowest ‘agreement’ were those suggesting autism supports be available exclusively for older children (i.e. not infants), or for any infant regardless of clinical need, or for those with a family history of autism/other neurodivergence.
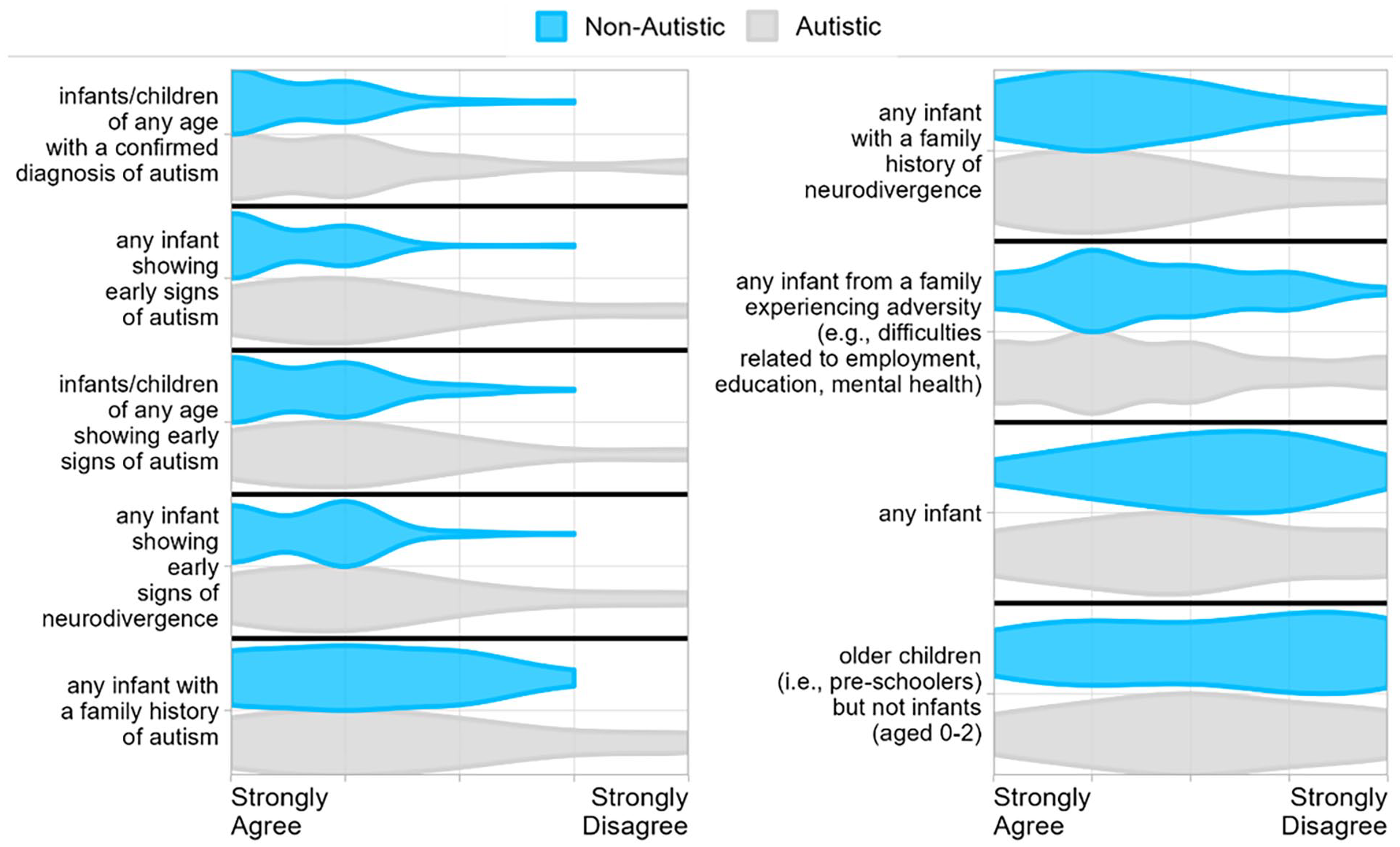
Responses to items regarding appropriate populations for very-early supports, by descending order of mean agreement.
Theme 4.1: broadly available according to need
Participants’ free-text responses suggested supports could be broadly available for ‘anyone who wants them’[A-Par9] as ‘the same types of training – helping the parent understand the child’s needs’[A-Par85] are ‘globally good for all infants’[NA-Par170]; ‘no-one needs to support autism like it is a separate thing’[A-Par124]. Others suggested that while ‘infants and preschoolers with family history . . . should all be provided assistance, priority should be for those needing more support’[A158]; ‘where there is identified need’[NA-Par136]. Some respondents emphasised the additional support needs of neurodivergent parents. For example: ‘Autistic mothers should be given support from the minute they get pregnant, on how to support their children developmentally’[A-Par15]. Others disagreed, explaining that ‘being Autistic . . . does not mean someone needs supports’[A-Par29].
Theme 4.2: reticence around starting supports too early
A minority of participants’ free-text responses did reflect concerns regarding the provision of supports during infancy. For example, one stated ‘I am extremely wary of any programs that would have singled her out earlier because of family history . . . she needed time to be a baby’[A-Par17]. Another explained ‘I don’t necessarily think there’s a rush to provide support if families don’t express a need’[NA-Par28]. The introduction of diagnostic labels was also concerning for some: ‘I do not see any value in focusing on “autism” for children of this age’[NA-Prof78], explaining that ‘it’s important not to artificially introduce autism as a concept without a degree of certainty’[A173].
Preferred language to describe very-early supports
Most participants agreed with the term ‘support’ over ‘therapy’ or ‘intervention’ (see Figure 6; Supplementary Table S6) and notwithstanding substantial response variability, use of ‘intervention’ was endorsed by fewer Autistic than non-Autistic respondents. Regarding language concerning the timing of such supports, most participants agreed with ‘early-in-life’ (but noting more Autistic than non-Autistic participants responded neutrally here), over alternatives such as ‘before/prior to diagnosis’, ‘pre-emptively’, ‘prodromally’ or ‘preventatively’. Autistic respondents preferred identity-first language (i.e. ‘Autistic child’) while non-Autistic participants more often agreed with ‘infants showing early signs of autism’. Smaller numbers agreed with ‘higher likelihood of autism’, ‘on the autism spectrum’ and ‘at-risk of autism’, with Autistic respondents indicating lower agreement here.
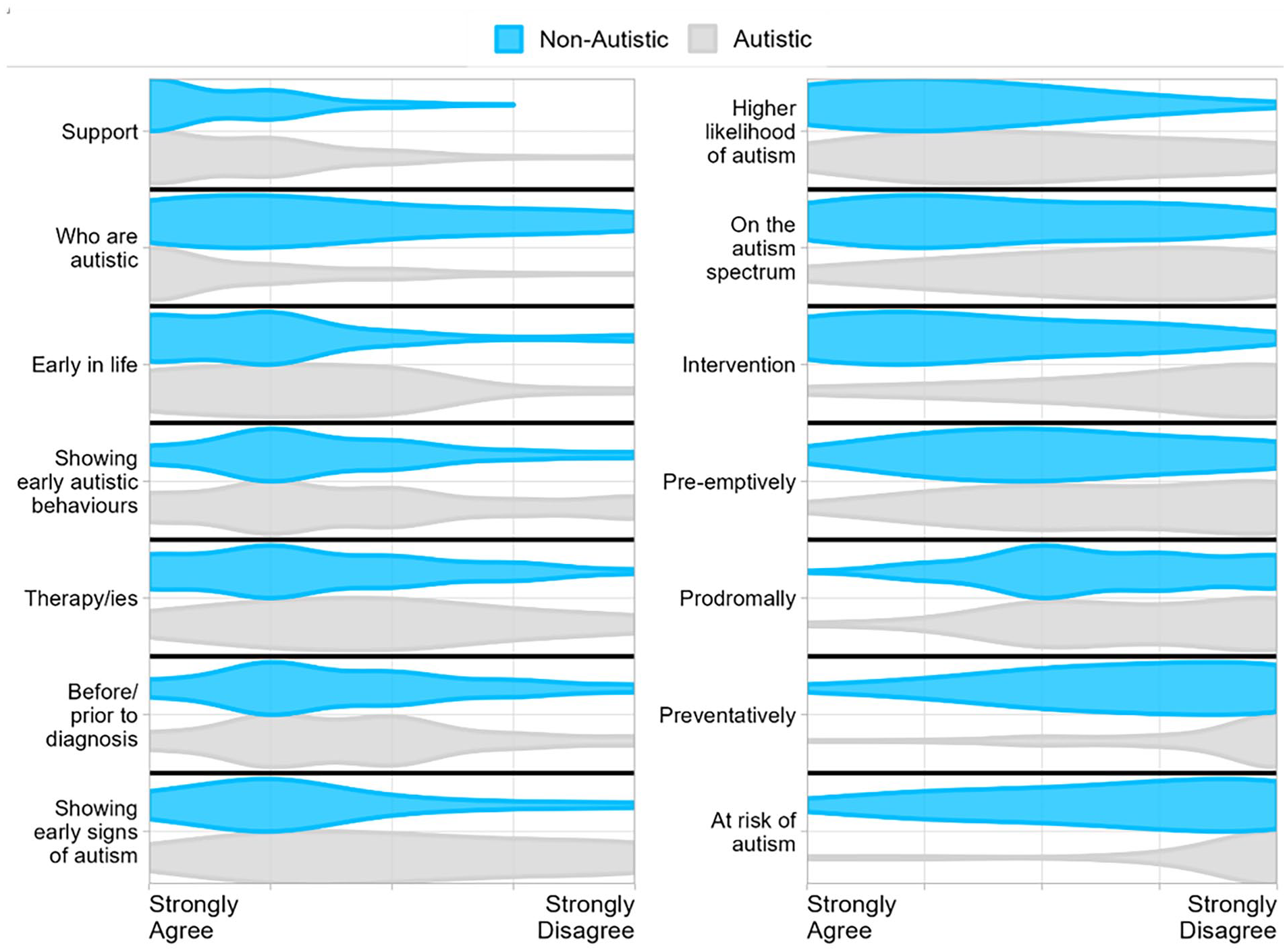
Responses to items regarding preferred language used to describe very-early autism support, by descending order of mean agreement.
Theme 5: respectful and accurate language
Many participants’ free-text responses indicated the language used to describe early-in-life supports should avoid terms that ‘make [autism] sound like a problem; something that can be fixed’[NA-Par93]. Many felt this included terms like ‘therapy’, ‘treatment’, ‘cure’, ‘intervention’, ‘pre-emptive’, ‘preventive’, ‘at-risk’ and ‘higher-likelihood’. As one explained: ‘You cannot prevent . . . [or] cure autism, [or] extinguish Autistic behaviours . . . terms like intervention, prevention, at risk, etc. are disrespectful . . . this should be about supporting children who may be . . . Autistic [or] born into neurodivergent families’[A73]. Similarly, ‘ableist’ terms implying comparison to neurotypical development were non-preferred, including ‘“delay” and “deficits” when talking about objectively neutral or even positive differences’[A166]. Several participants indicated preference for ‘more specific and direct terms’[A57] as respectful language should accurately describe the type of support offered and people involved, and ‘doesn’t mean everything should be oversimplified’[A158]. For example, one respondent explained ‘I would disagree with using the term Autistic or on the spectrum . . . as they may not be’[NA-Prof176], while others explained ‘I don’t care at this stage, it’s all a bit confusing focusing on terminology pre-diagnosis’[A-Par105] and suggested ‘maybe just say ‘We use the term . . . are you OK with that? Right let’s begin’’[A158].
Discussion
We sought diverse perspectives on supports offered within the first 2 years of life for infants who may be Autistic, including to understand more versus less acceptable aspects according to the Autistic and autism community members. Within both Autistic and non-Autistic respondent subgroups was apparent response variability, with some meaningful between-group perspective differences evident, particularly regarding the appropriateness of specific support strategies/techniques and use of the descriptive term ‘intervention’. Free-text responses offered insights into these nuanced differences of opinion.
‘Acceptable’ ways of supporting infants who may be Autistic
Almost all survey respondents agreed that early-in-life autism supports should aim to help caregivers understand and/or respond supportively to their infant’s feelings, needs and behaviour, with the ultimate goal of promoting infant quality of life. These findings converge with the priority-support goals for Autistic pre-schoolers aged 0–5 years recently identified by Baiden et al. (2024) and Waddington et al. (2024). Respondents also broadly agreed with educating parents towards adapting the environment to better meet their infant’s needs, understanding infants’ communication cues and enabling infant autonomy. These points are consistent with recent frameworks for neurodiversity-affirming supports, advocating for supportive environments that foster Autistic strengths (Lerner et al., 2023) and shared autonomy/control (Schuck et al., 2022). Most respondents agreed that early-in-life supports could be offered in the context of indicated clinical need (i.e. for infants presenting early Autistic/neurodivergent behaviours), more so than based on family autism history alone, reiterating perspectives recently raised by MacDuffie et al. (2021). Respondents also indicated broad agreement for approaches whereby parent/s directly support their infant (i.e. parent-mediated delivery), and where amount and type of support provided are individualised – consistent with calls to ensure autism services do not inadvertently negatively impact participation in other enriching life activities (Trembath et al., 2021).
When describing these types of supports, participants in both groups preferred the term ‘support’ over ‘intervention’, and ‘early-in-life’ over ‘at-risk’ or ‘pre-emptive’. Language plays a key role in facilitating shared understanding and shaping individual/societal views of autism, and these findings broadly converge with other adult-focused reports advocating neurodiversity-affirming language (Bottini et al., 2024; Bury et al., 2020). Here, however, were highly variable ‘agreement’ rates for specific terms, so we propose ‘respectful and accurate language’ as a guiding overarching principle, offered via free-text response.
Nuanced differences of opinion
Some meaningful if nuanced differences of opinion were also evident in Autistic and non-Autistic participants’ responses – often for items less frequently endorsed as ‘acceptable’ overall, where Autistic respondents in particular offered lower endorsement. For instance, the broad aim/outcome of reducing Autistic behaviours, the specific use of reinforcement strategies, a high-intensity delivery, and use of the term ‘intervention’ were all least frequently endorsed overall – mirroring a convergent shift in the field towards neurodiversity-affirming practices (Dawson et al., 2022) – but also particularly infrequently rated ‘acceptable’ by Autistic participants. This latter finding is consistent with accounts from the studies by Baiden et al. (2024) and Waddington et al. (2024), and may suggest stronger support for neurodiversity among Autistic than non-Autistic participants. Autistic respondents were also relatively more likely to endorse the involvement of Autistic adults in the development and delivery of early-in-life supports, suggesting an enduring hesitancy among non-Autistic stakeholders despite recent calls for co-production (Leadbitter et al., 2021). We note, however, that wording of this survey item did not include the potential for involvement of Autistic clinicians – as emphasised within free-text responses – which potentially influenced participants’ quantitative ratings.
Autistic participants were also less likely to endorse the use of intentional pausing to encourage infant communication/behaviour, consistent with findings from the study by Schuck et al. (2022). Free-text responses here suggest this strategy may be interpreted as either an environmental accommodation (i.e. allowing an infant additional time to contribute to a shared activity) or a behavioural management strategy (i.e. withholding reward until a desired communication behaviour is performed). Indeed, our specific wording of this item – phrased as ‘encouraging communication/behaviour’ – may have primed participants towards the latter. These nuanced response differences nevertheless emphasise the need to move towards reconciling differences of opinion.
Towards reconciliation of apparent contradictions
While a clear, positive shift is occurring towards shared understanding of acceptable ways to support infants who may be Autistic and their families, achieving effective early-in-life supports will require further collaborative effort to reconcile some apparently contradictory perspectives. One such point arising from this research concerns environmental adaptations to better suit an infant’s needs – a highly endorsed strategy viewed as neurodiversity-affirming – that may reduce the experience of clinical-need, indirectly leading to reduced expression of Autistic distress behaviours. For instance, prompt/sensitive responsiveness to infant communication cues may meet an immediate need and contribute to reduction in Autistic sensory/motor behaviours, which serve an adaptive coping function (Joyce et al., 2017; Kapp et al., 2019) – though deliberately aiming to reduce such behaviours would be contrary to neuro-affirming practice. Similarly, following an infants’ lead to engaging in activities of apparent interest, regardless of whether considered neurotypical – a highly endorsed strategy – may increase infant–caregiver social engagement – a less frequently endorsed outcome. This pattern of results highlights how implementing neurodiversity-affirming supports may indirectly impact outcomes viewed as incongruous with the neurodiversity movement (Lerner et al., 2023).
Green’s (2022, 2023) model of autism may provide middle ground towards reconciling these apparent contradictions. In this model, the behavioural presentation of autism is considered emergent over time, from transaction between the neurodivergent individual and their environment. Indeed, there is evidence to indicate some malleability in that emergence following on from particular supportive environmental changes. Hence, providing positive early environmental and interpersonal/relational support – generally valued by the current survey respondents – can indirectly result in reduction in autism-related clinical-need, without fundamentally altering underlying neurodivergent mechanisms, or impacting neurodiversity-affirming sense of identity (Green, 2023; Whitehouse, 2023; and see Dwyer et al., 2021).
Limitations
Notwithstanding novelty, topicality and good Autistic/non-Autistic respondent between-group matching we achieved here, non-representative sampling remains a potential limitation of this study. The sample included predominantly university-educated participants from Australia, United Kingdom and United States – with only small numbers from lower/middle income countries – so perspectives captured here may not generalise to stakeholders from other regions, cultural groups or socio-economic backgrounds. Indeed, other research shows that Autistic and non-Autistic individuals from diverse cultural backgrounds and resident in lower/middle income countries may have differing views of autism and related support needs/priorities (Divan et al., 2012; Smith et al., 2023) including that offered early in life which has, to our knowledge, yet to be considered beyond Western/high-resource settings. As in other online autism studies, respondents were also predominately female, and participation would have been difficult for non-speaking Autistic adults and Autistic children. Future research should target engagement efforts towards these subgroups to ensure their perspectives are also heard.
Conclusion
To our knowledge, this is the first study to have systematically engaged the Autistic and autism communities around perspectives on very-early-in-life autism supports. Many areas of common ground emerged, particularly around what is acceptable practice. Future efforts should carefully reconsider how existing programmes and outcome measures align with community priorities/preferences, and ensure that approach, delivery and specific strategies/techniques do not unduly burden or harm Autistic participants (Leadbitter et al., 2021). Co-developing, evaluating and delivering support programmes with Autistic people will ensure early-in-life autism supports respect and genuinely meet the needs of the community.
Supplemental Material
sj-docx-1-aut-10.1177_13623613241262077 – Supplemental material for Autistic and autism community perspectives on infant and family support in the first two years of life: Findings from a community consultation survey
Supplemental material, sj-docx-1-aut-10.1177_13623613241262077 for Autistic and autism community perspectives on infant and family support in the first two years of life: Findings from a community consultation survey by Catherine A Bent, Alexandra Aulich, Christos Constantine, Esther Fidock, Patrick Dwyer, Cherie Green, Jodie Smith, Ava N Gurba, Lucas T Harrington, Katherine E Gore, Aspasia Stacey Rabba, Lauren N Ayton, Kathryn Fordyce, Jonathan Green, Rachel Jellett, Lyndel J Kennedy, Katherine E MacDuffie, Shoba S Meera, Linda R Watson, Andrew JO Whitehouse and Kristelle Hudry in Autism
Footnotes
Acknowledgements
The authors gratefully acknowledge the Autistic and non-Autistic community members who completed the survey, as well as Sallie Nowell, Lael Ridgeway and Leonie Segal who advised on study design and conduct as members of a broader working group.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Several authors have been involved in the development (JG, LRW, SSM) and/or evaluation (AA, AJOW, CAB, CG, JG, JS, KH, LRW, SSM) of support programmes for young Autistic children. JG and LH receive royalties and/or other benefits from training related to a specific support model. AJOW, JG, JS, KF, LH, RJ and SSM are/have been employed by and/or have/have had roles with service providers that support young Autistic children. These potential conflicts of interest were managed within the research team by engaging Autistic and non-Autistic researchers and community members with no known conflicts of interest (ANG, ASR, CC, EF, KEG, KEM, LNA, LJK, PD).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was supported by funding via an International Society for Autism Research (INSAR) Topical Brief and a La Trobe University Early Career Researchers ‘ABC Award’ grant. JG is a UK NIHR Senior Investigator (NF-SI-0617-10168) and funded by the NIHR Manchester Biomedical Research Centre (NIHR203308). The views expressed are those of the authors and not necessarily those of the NIHR or the Department of Health and Social Care.
ORCID iDs
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.