
Abstract
Preschool teachers can play a critical role in early detection of autism. Equipping preschool teachers with prerequisite knowledge and skills would allow them to identify children with probable autism and referral to diagnostic services. This study aimed to investigate the impact of an educational module (EMiASD) that prepared preschool teachers to identify autism symptoms. The sample included 144 preschool teachers, of which 120 were stratified and randomly assigned to an intervention arm receiving training in EMiASD (n = 60) or a comparison arm receiving standard training (n = 60) using a parallel mixed-methods design. Responses to open-ended questions about video case studies revealed improvement in the identification of autism symptoms in preschool teachers in the intervention arm, in contrast to preschool teachers in the comparison arm. Moreover, significant changes in knowledge, belief, and self-efficacy about autism favoured EMiASD. Overall, these results demonstrate the influence of EMiASD in the Yemeni cultural context.
Lay Abstract
Preschool teachers can play a critical role in early detection of autism. Equipping preschool teachers with prerequisite knowledge and skills would allow them to identify children with probable autism and referral to diagnostic services. This study aimed to investigate the impact of an educational module (EMiASD) that prepared preschool teachers to identify autism symptoms. The sample included 144 preschool teachers, of which 120 were stratified and randomly assigned to an intervention arm receiving training in EMiASD (n = 60) or a comparison arm receiving standard training (n = 60) using a parallel mixed-methods design. Responses to open-ended questions about video case studies revealed improvement in the identification of autism symptoms in preschool teachers in the intervention arm, in contrast to preschool teachers in the comparison arm. Moreover, significant changes in knowledge, belief, and self-efficacy about autism favoured EMiASD. Overall, these results demonstrate the influence of EMiASD in the Yemeni cultural context.
Developmental disorders such as autism are at least as prevalent in low-income contexts as in high-income contexts (Olusanya et al., 2018). However, the prevalence of autism has not been systematically assessed in many low- and middle-income countries, such as Yemen (Bameer et al., 2016; Taresh et al., 2019). Studies of general mental health problems and intellectual disability issues in these countries indicate that these concerns are at least as prevalent as in high-income countries (Desta et al., 2017). In Yemen, autistic children are frequently diagnosed late and generally under-represented relative to their likely prevalence in the population (Al-Farsi et al., 2011; Taresh, Ahmad, Roslan, Ma’rof, & Zaid, 2020; Zaid et al., 2020). The reasons for this are multifaceted and include government policy, service provision, society, parents, and the educational system (Al-Eryani, 2021).
The governing body of Yemen has listed autism among the disabilities in the Handicapped Care and Rehabilitation Funds, established in 1999. This move has resulted in autism being categorized as a mentally disabled group, such that autistic children must enrol within centres in which specialized training is provided (Al-Eryani, 2021; Alyahri & Goodman, 2008). These centres are primarily located in the most populous cities of Yemen: namely, Sana’a, Aden, and Taiz. However, many families live in remote locations and thus cannot bear the expense of travelling, which limits the accessibility to critical services for almost 85% of these children (UNICEF, 2021).
According to the 2021 UNICEF report entitled Mapping Available Assistance to Children with Disabilities in Yemen, there are various reasons for the delayed autism diagnosis including insufficiencies in qualified teachers, specialized training, resources, and equipment to address the needs and integration of children with disabilities, including autism. This dearth of essential provisions and expertise is a key contributor to the lack of awareness about autism among the Yemeni community (UNICEF, 2021). Recently, the ongoing war in Yemen has negatively impacted diagnosis of psychological disorders, including developmental disorders. In addition, due to the nation’s economic crisis, few people can afford basic healthcare, let alone mental health services or behavioural interventions. Because mental illness and developmental disorders are often mistaken for a demonic condition, physical health is prioritized over mental health in Yemen (Taresh et al., 2020). People often turn to local sheikhs and traditional healers for mental health support as mental disorders are stigmatized and taboo. This is also true for developmental disorders such as autism, which are referred to as “crazy,“ “insane,” “possessed by Jinn,” or “far from Allah” by many Yemenis. Due to the stigma attached to psychological disorders, many Yemenis believe that individuals with them should be isolated from society (Taresh, Ahmad, Roslan, & Ma’rof, 2020; Zaid et al., 2022), negatively affecting autistic children and their families. Hence, certain families deliberately keep their autistic children secret from the community to prevent them from losing respect. In specific circumstances, some parents may engage in exploitative mistreatment of their autistic children. This mistreatment can involve involving the children in begging, child labour, and even exploiting their condition to receive money from charity or other sources (Al-Eryani, 2021). This predicament is exacerbated by the absence of social support, poor economic standards, inadequate access to essential services, and interrupted livelihoods (Zaid et al., 2022).
Research from other cultural contexts indicates that teachers of children at all ages, including preschool, can play a key role in the early identification and referral of children’s developmental, behavioural, and emotional problems. Notably, this work suggests that teachers can serve as a trusted source of information about autism after receiving training to identify its symptoms (Dominick et al., 2007; Latouche & Gascoigne, 2019; Talib & Paulson, 2015). Because teaching experience alone is inadequate to enhance preschool teachers’ knowledge of autism symptoms (Drusch, 2015), there is a need for the provision of formalized training in autism identification.
While preschool teachers may be well-positioned to identify early challenges faced by their students, they face numerous barriers in identifying autism symptoms and referring these children for further evaluation (Able, 2012; Biasotti, 2013; Rothì et al., 2008). These challenges include personal characteristics of the preschool teachers (e.g. their knowledge, attitudes, stigma, feelings, skills, and perceptions of autistic children; (Able, 2012; Biasotti, 2013), concerns about their ability to detect autism (Peterson et al., 2013), lack of motivation to identify and refer autistic children (Ensimau, 2019), low perception of self-efficacy to refer an autistic child to a specialist, and limitations in resources that may influence the cultural stigma surrounding an autism diagnosis (Reinke et al., 2011). Moreover, some preschool teachers do not want to overload school counsellors with their doubts about a child’s disorder (Ensimau, 2019). In view of these issues, preschool teachers’ knowledge about autistic children, identification skills, and misbeliefs about autistic children influence their susceptibility to cultural stigmas about autism in various cultural contexts (Obeid et al., 2015) as well as their eventual decision to identify and refer children suspected of having autism (Dunlap et al., 2006; Fantuzzo et al., 1999; Lee, 2014; Powell et al., 2007).
Evidence from diverse cultural contexts suggests that the understanding of early signs of autism may be deficient among preschool teachers (Al-Farsi et al., 2011; Anthony et al., 2005; Lian et al., 2008), suggesting a low level of overall knowledge of autism (Liu et al., 2016; Qi et al., 2016). Moreover, stigma is a well-documented obstacle to seeking a diagnostic and treatment services for autism, and this is particularly true in low- to middle-income countries such as Yemen. Thus, stigma likely has an impact on Yemeni preschool teachers’ emotional states and concerns about children’s behaviour, affecting their capacity to voice their concerns to parents and refer children to specialists. Research from the United States suggests that preschool teachers’ ability to identify and refer students with developmental impairments may be limited (Bradshaw et al., 2008; Splett et al., 2018). This may be due to a lack of understanding and ability in dealing with challenging behaviour in children as a result of limited training in this area (Alexander et al., 2015). Thus, increasing preschool teachers’ self-efficacy may increase the likelihood that autistic children will be referred to intervention services.
In summary, interventions focusing on early detection of autism spectrum disorder (ASD) are less common among preschool teachers in general and are absent among Yemeni schools in particular. Therefore, this study develops and evaluates an educational intervention to increase Yemeni preschool teachers’ knowledge, beliefs, and self-efficacy about autism and their ability to detect autism symptoms. In doing so, it aims to promote early referral and intervention of autistic children.
Method
Design
This study uses a parallel mixed-method design including both quantitative and qualitative measures. Participants were randomized to intervention and comparison arms. Group training sessions were held with the participants in the intervention arm with the purpose of improving the accuracy of autism identification among preschool teachers.
Preschool teachers assigned to the intervention arm received the educational module to identify autism spectrum disorder (EMiASD) intervention, described in the Intervention section below. Preschool teachers assigned to the comparison arm received the play learning strategy. Training in implementation of the play learning strategy is provided annually by the Ministry of Education to preschool teachers in Yemen. The play learning strategy provides preschool teachers with information and strategies concerning the use of toys and other materials in their teaching.
Participants assigned to both the intervention and comparison arms completed the Autism Knowledge (ASD-Q), Beliefs Towards Autism (BASD-Q), and Self-Efficacy to Refer Autistic Children questionnaires (see Measures section below) at three time points: before participating in the intervention (pre-test), immediately after the intervention (post-test), and 1 month after the intervention (follow-up test). At the same intervals, preschool teachers watched video case studies followed by open-ended questions to explore their ability to recognize symptoms of autism. Results were analysed separately and then combined in the interpretation stage.
This study followed the consolidated standards of reporting trials (CONSORT) guidelines for randomized trials (Campbell et al., 2012). Because this study was not registered and outcomes were not specified prior to data collection, however, it does not qualify as a randomized controlled trial. Therefore, its purpose is to provide a preliminary indication of the impact of the EMiASD.
Participants
Yemeni preschool teachers (n = 120) were recruited as per the following inclusion criteria: (1) Teaching at the kindergarten, preschool, or primary stage, (2) Aged between 20 and 40, (3) Having at least a high school level education, and (4) Giving consent to participate in the study. Exclusion criteria were as follows: (1) Quitting during the study period, (2) Teaching in elementary and high schools, and (3) Possessing lower than a high school education level.
According to the Lemeshow equation (Ary et al., 2018), this sample size is appropriate to achieve the study’s objectives and compatible with the recommendations for behavioural interventions in autism (Lwanga & Lemeshow, 1991). Of these preschool teachers, a total of 40 were randomly selected from those assigned to the intervention arm (n = 20) and comparison arm (n = 20) to participate in the qualitative phase.
Randomization and blinding
To ensure proper randomization and allocation to the intervention and comparison arms, a statistician produced the allocation sequence list using block randomization software (Hamamura et al., 2014) to allocate the 12 eligible clusters (schools) to the intervention and comparison arms with a 1:1 allocation using random block sizes of 2 and 4. Thus, six clusters were randomly allocated to the intervention arm (VX9, XP6, EP9, ZI8, FF5, and IQ3) and six clusters to the comparison arm (IO2, OM1, BM3, AT1, AA4, and KM3). Each cluster was given a unique code in a sealed opaque envelope. Following that, the research assistant opened the envelopes and assigned the clusters to the experimental or comparison arm based on the list of codes generated by the software. Moreover, to avoid bias at the individual level, the envelopes were opened only after the school coordinator obtained the required number of participants and after obtaining consent for treatment and collecting baseline data.
Intervention
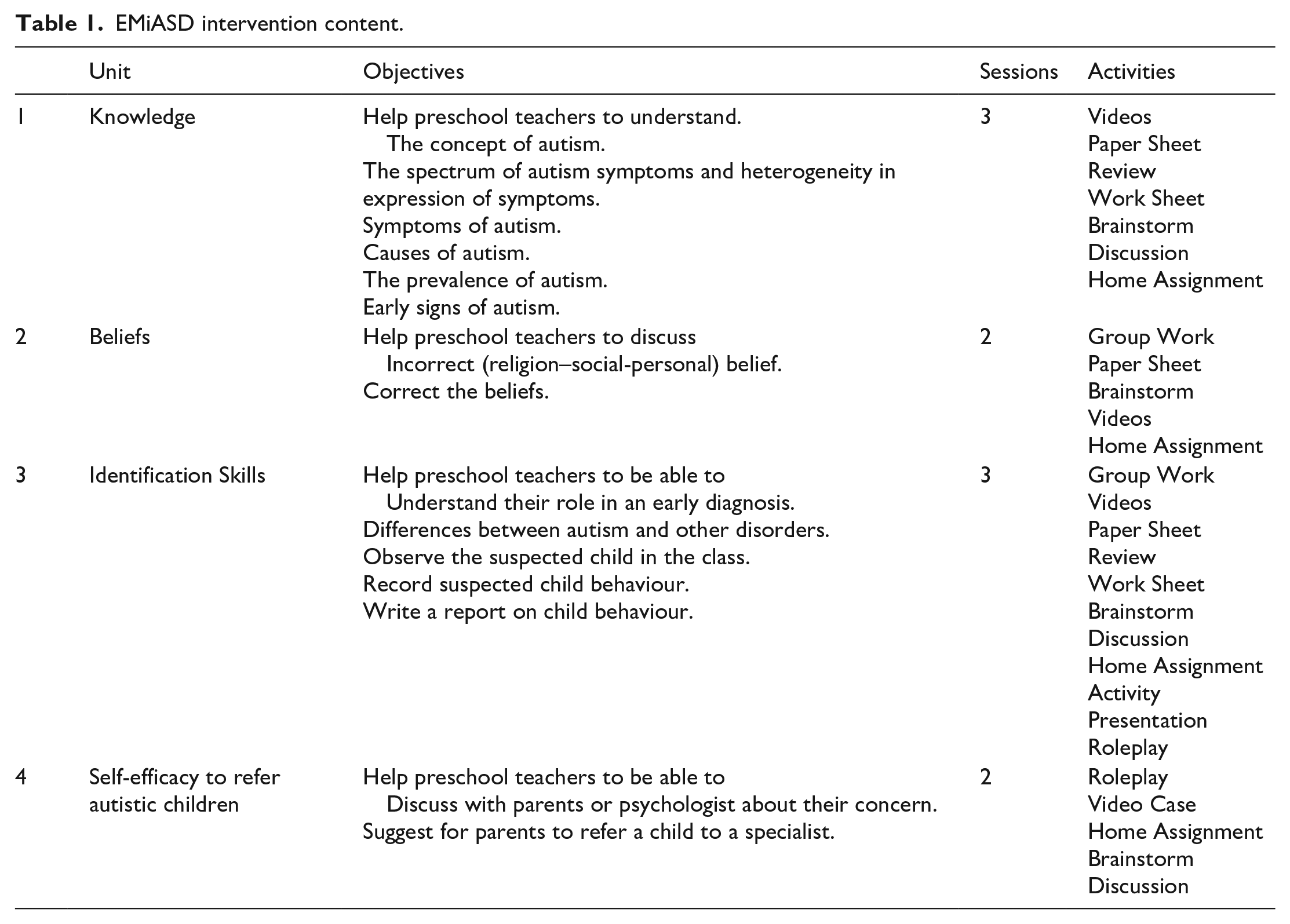
EMiASD was developed based on the ADDIE (analysis-design-development-implement-evaluation) model (Perels et al., 2009). Any instructional design requires the use of a system to analyse problems and identify learning objectives to establish a strategic plan to solve teaching problems, test solutions, evaluate the results and revise the programme. The EMiASD comprises four units: Unit 1 provides general information on ASD rate, causes of ASD, and symptoms of ASD based on the DSM-5 in order for the participants to have a clear understanding of the topic. Unit 2 discusses the misbeliefs and stigma associated with autism in order to enhance and correct them, which affects help seeking and early diagnosis. Unit Three offers an explanation of autism symptoms (e.g. an autistic child’s behaviour in class) in a bid to encourage participants to identify them via different steps, including understanding their role in an early diagnosis, identifying differences between autism and other disorders, observing the suspected child in the class, recording suspected child behaviour, and writing a report on child behaviour. Unit Four explains the referral procedure to raise participants’ awareness of the ASD specialist diagnostic team and raise their confidence to discuss a referral with parents. The selection of these units was based on the findings of previous studies indicating that knowledge, beliefs, and self-efficacy play a critical role in early identification of autism (Barrie, 2010; Drusch, 2015; Kingsley, 2012; Rosenberg et al., 2011). Therefore, this intervention was prepared and designed to address late referral and diagnosis of autism. The intervention has received copyright from MyIPO No. LY2023W00858. Table 1 provides an outline of the EMiASD along with the application of the strategies and materials used in the EMiASD.
EMiASD intervention content.
This intervention is grounded by the health belief model, which posits that perceived barriers affect beliefs about autism diagnosis. In particular, the intervention aims to reduce social stigma, which is considered one of these barriers. In addition, the intervention is grounded in social cognitive theory (Bandura, 2002), which hypothesizes that teachers who have confidence in their ability to handle developmental disabilities will make an effort to refer affected children to services (Liljequist & Renk, 2007).
Following the development of the EMiASD, face and content validity were checked and assessed by five professional expert panellists. The experts approved the educational material and indicated that these materials are sufficient and aligned with the study objectives. Their feedback focused on the understandability and simplicity of the content. They suggested that information about autism and any complex terms from the module ought to be removed to make it easier for participants to understand the content. They also suggested adding pictures to the module to make it clearer and more interesting. The researchers expanded the duration of the intervention to 10 sessions administered over 2 weeks to ensure that the participants become more interactive in them (see Table 1).
The EMiASD was implemented by the first author (S.M.T.), who was a lecturer in the faculty of education in a public university in Yemen at the time this research was conducted. She has experience in conducting workshops for pre- and in-service preschool teachers in Yemen. She also oversees evaluation of pre-service preschool teachers in their practicum. All training sessions were delivered in person to maximize accessibility.
Training sessions took 2 hours per day with a 15-minute refreshment break. They began with the implementer greeting the participants, who were then exposed to the topics of the day. Participants were given assignments at the end of every session to be submitted at the next session. In the next session, the implementer reviewed the topics introduced in the previous session and asked participants to present their assignments in front of their colleagues using working groups, slide decks, or individual presentations. After that, the implementer introduced the topic of the day by posting general questions for brainstorming or discussion. The participants presented their answers using roleplay, discussion, or working groups. The implementer then presented the correct answers via slides, video, or bringing guests to share their experiences with participants. The implementer presented two topics every day, one before the break and the second after the break. The implementer used the same teaching techniques (slide discussions, videos, roleplay, or workgroups) in all sessions.
At the end of the educational module, participants were offered a copy of the relevant booklet containing all information delivered to them in the educational module. They were given copies of the videos shown in sessions and an autism awareness logo sticker. These materials were intended to remind the participants of the importance of the early diagnosis of autism.
Implementation strategies to increase fidelity
To support the fidelity of the EMiASD, several strategies were used to preserve the consistency of intervention delivery and encourage and reinforce participants’ adherence to the intervention. First, detailed contact information was obtained so that the researchers could periodically call participants to assure that they understood and performed the required skills and support and encourage them to implement the programme as intended to ensure effective implementation of the intervention. Second, although no financial incentives were offered to participants, as was clearly indicated in the letter of invitation and meeting held prior to implementing the module, they were offered free transportation vouchers as a reward for their participation. Finally, a certificate of attendance was awarded to each participant who attended the module. The certificate encouraged attendance, active participation, and acquisition of new skills, demonstrating professional and personal accomplishment among teachers. In addition, the certification served as a formal acknowledgement by the state ministry of Yemeni education that an individual participant demonstrates skill and competence in identifying autism.
Materials
Each of these scales described below were administered using pen and paper as this method could be easily implemented in conjunction with the in-person training sessions. The questionnaire was administered by four undergraduate students at Taiz University. They volunteered to help the researcher after receiving all the information about the purpose of the study.
ASD Knowledge Questionnaire (ASD-Q)
The ASD Knowledge Questionnaire (ASD-Q) was created and used to measure preschool teachers’ general information related to autism symptoms, treatment, and causes. The items of this questionnaire were adapted from two questionnaires: the Autism Stigma and Knowledge Questionnaire developed by Harrison et al. (2017), which measures knowledge of ASD with respect to diagnosis and symptoms (17 items), treatment (14 items), and etiology (16 items) in college students and the general public in the United States; and a questionnaire about knowledge of autism developed by Al-Sharbati et al. (2015), which measures awareness of the etiology (5 items), signs and symptoms (10 items), and sociodemographic (and other) correlates of autism (15 items) in school teachers in Oman.
The ASD-Q consists of 27 items comprising four domains. Domain 1: Diagnosis and Symptoms includes nine items that assess preschool teachers’ knowledge of autism, including its diagnosis and symptoms. Domain 2: Treatment includes six items assessing preschool teachers’ knowledge about treatment or therapies that can be applied to an autistic child. Domain 3: Etiology includes four items assessing the causes of autism. Domain 4: General Information includes nine items assessing the general knowledge of preschool teachers about autistic children who do not fall into the other domains; for example, ‘the majority of children with autism suffer from mental retardation’, and ‘the child with autism suffers from social stigma’. All items were rated using a 5-point Likert-type scale ranging from strongly disagree (1 point) to strongly agree (5 points). The overall reliability for this scale with a pilot sample of 215 preschool teachers was α = 0.89, while the reliability of each domain was as follows: Diagnosis and Symptoms α = 0.78; Treatment α = 0.79; Etiology α = 0.68; General Information α = 0.8
Beliefs towards ASD Questionnaire (BASD-Q)
The BASD-Q was created and used to assess preschool teachers’ thoughts and perspectives towards autistic children and their families. The items of this questionnaire were adapted from two measures: a questionnaire about religious explanations for autism in Muslim parents (Gilligan, 2013), and the stigma subscale of the Autism Stigma and Knowledge Questionnaire for college students and the general public in the United States (Harrison et al., 2017). We adapted the items from these two questionnaires to create a more comprehensive questionnaire capturing Yemeni beliefs about ASD, the BASD-Q.
Reliability for the BASD-Q with a pilot sample of 215 preschool teachers was α = 0.87. This study used exploratory factor analysis to detect the underlying structure of the BASD-Q’s items. This analysis yielded three factors: namely, religious beliefs (six items), social beliefs (seven items), and personal beliefs (eight items), with a total explained variance of 55.01%, 47.69% and 52.63%, respectively. The Kaiser–Meyer–Olkin (KMO) index values of 0.64, 0.68, and 0.72, and the Bartlett’s Test of Sphericity (p = 0.0001) for religious beliefs and social beliefs, respectively, verified the normality of the distribution and the adequacy of the sample size for exploratory factor analysis (EFA). The items achieved adequate factor loadings ranging between 0.47 and 0.88, while the reliability of the subdomains was as follows: Religious Beliefs α = 071; Social Beliefs α = 0.62; Personal Beliefs α = 0.68.
The BASD-Q consists of three domains. Domain 1: Religious Beliefs assesses preschool teachers’ religious and spiritual beliefs associated with health practices; for example, ‘It is likely autism is a result of a curse or evil eye put upon/inflicted on the family’, and ‘I think an autistic child is a gift from God’, Domain 2: Social Beliefs assesses the individual’s common belief system and serves as an explanatory model for autism; for example, ‘In my community, children with autism suffer from social stigma’, and ‘People will be ashamed if a family member is diagnosed with autism’. Domain 3: Personal Beliefs assesses the preschool teachers’ perspectives that reflect their own thinking about autistic children; for example, ‘I think autism is caused by watching TV or a mobile phone for a long time’, and ‘I think traumatic experiences very early in life can cause autism’.
Self-Efficacy Questionnaire
This questionnaire assesses preschool teachers’ ability to discuss with parents and make referral recommendations for autistic children. Items of this questionnaire were adapted from Drusch (2015) and (Baker, 2012). This questionnaire contains two domains. Domain 1 measures preschool teachers’ ability to express their concerns about developmental delays with their parents or specialists. Example items include, ‘I feel confident in my ability to explain autism to parents and others’ and ‘When I share my concerns about a child’s growth with their parents, I am confident they will appreciate that’. Domain 2 measures preschool teachers’ ability to make a decision to refer autistic children to experts or intervention services. This domain contains seven items such as, ‘I am confident in my ability to recognize the (signs / symptoms) of autism in kindergarten children’ and ‘I am confident in my ability to ask specialists about taking appropriate action to get help for the needs of children’. All items were rated using a 5-point Likert-type scale ranging from strongly disagree (1) to strongly agree (5). Reliability for this scale with a pilot sample of 215 preschool teachers was α = 0.81, while the reliability of the domains was as follows: ability to express their concerns α = 0.78; ability to make a decision to refer autistic children α = 0.78.
Video case studies
Observing children’s behaviour in their natural setting is the most ecologically valid method for assessing them (Reinke et al., 2011; Tilahun et al., 2019). Therefore, the current study used video case studies because they provide an ecologically valid means of assessing preschool teachers’ skills and ability in identifying autism symptoms. Previous studies have used this technique to assess participants’ ability to identify autism symptoms in children (Ben et al., 2018; Chambers et al., 2017; Li et al., 2018).
Video case study assessments were conducted in one-on-one meetings with preschool teachers. In these assessments, the researchers gave the following instructions to the participants: ‘Two video cases of children will be displayed. Please watch the two videos carefully. You will be asked to answer a few questions related to the videos after watching them’. Video case studies consisted of two 5-minute videos of two 6- to 8-year-old children. Video 1 featured an autistic child with his mother in different settings while playing, eating, and teaching (taken from the Centres for Disease Control, USA). Video 2 featured a child with attention-deficit hyperactivity disorder (ADHD) in various settings including class activities, swimming, and lunch time (taken from the National Institute of Mental Health, USA).
After watching each video, the following four questions were presented to assess preschool teachers’ identification of autism symptoms and referral for diagnostic and support services. These questions were derived from Ben et al. (2018) and were utilized to assess preschool teachers’ skill in identifying autism symptoms based on the two video cases:
Is the child having any problems? [Yes/No];
Based on what you have seen in the videos, what kind of problem did the child have? [Open response];
What are the reasons for your answer? [Open response];
Based on what you’ve seen in the videos, would you recommend a referral service to the child’s parents? [Yes/No].
Prior to data collection, the researchers examined the validity and reliability of the questions related to the video case studies. This process encompassed submission to a skilled panel comprising four experts: paediatrician, developmental psychologist, and two developmental specialists. Each expert acquired at least 5 years’ experience in diagnosis and intervention for early childhood disorders, including autism. The panel’s ratings of the case study were used as a standard to determine the correct answers. Accordingly, a high degree of inter-reliability was found among the experts’ scoring (ICC = 0.79, 0.31–0.97 across DSM-5 criteria).
Procedures
Researchers assigned each participant a unique number (three digit-code) to identify their pre-test, post-test, and follow-up test questionnaires (e.g. I-4-15 stands for the intervention arm, school no. 4, and participant no. 15). These unique numbers were recorded in a separate list from identifiable information such as participant and school names. To ensure truthful responses, honesty was emphasized to preschool teachers, and they were informed that the questionnaires were anonymous.
Prior to the intervention, participants completed the pre-test, which consisted of the ASD-Q, BASD-Q, and self-efficacy measures as well as the video case studies described above. The intervention was then implemented, as described in the Intervention section above. Immediately and one month after the intervention, the same undergraduate students who administered the pre-test administered the post-test and follow-up test, respectively, which consisted of the same components as the pre-test.
Data analysis
All data from open-ended questions following video case studies were analysed using content analysis. Responses were first transcribed verbatim by the researchers. Coding began with a line-by-line analysis of each transcript to find words or phrases associated with participant responses. Themes were created using pattern coding, which uses ‘chunks’, or units, to create themes and subthemes. To ensure the credibility of the results and to reduce researcher bias, the researchers had two external readers (final year PhD students) review the analysis process as well as codes and themes (Creswell & Creswell, 2017).
Data from pre-test, post-test, and follow-up administrations of the ASD-Q, BASD-Q, and self-efficacy measures were analysed using analyses of covariance (ANCOVAs) with pre-test as a covariate, intervention arm as an independent variable, and post-test or follow-up test as the dependent variable. Prior to analysis, missing data on categorical variables was replaced by imputation using the regression technique. The data analyst (L.M.M.) was not blind to intervention arm assignment. The open-ended questions were administered by two undergraduate students at Taiz University. They volunteered to help the researcher after receiving all the information about the purpose of the study.
Results
Baseline characteristics
Pearson chi-square tests revealed that randomization was effective in assignment to treatment arms with no differences in age (χ² = 4.94, p = 0.08), educational level (χ² = 0.11, p = 0.95), or teaching experience (χ² = 3.36, p = 0.19; see Table 2).
Demographic variables of participants in the intervention and comparison arms.
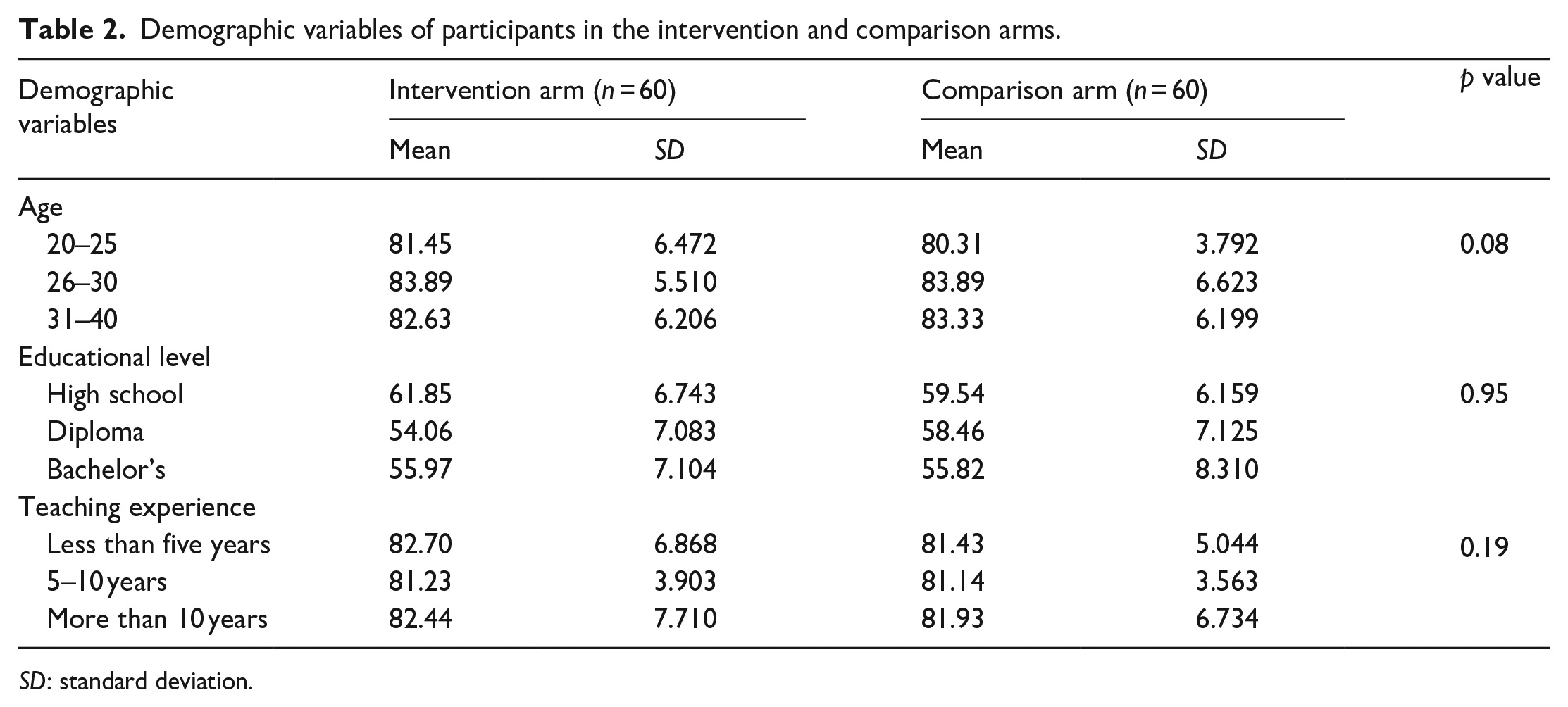
SD: standard deviation.
Feasibility and acceptability
We sought to recruit 200 preschool teachers from a total of 15 schools in Taiz. Our final sample consisted of 120 preschool teachers recruited from 12 schools. Figure 1 provides details concerning the number of teachers excluded at each stage of the study and the rationales for exclusion.
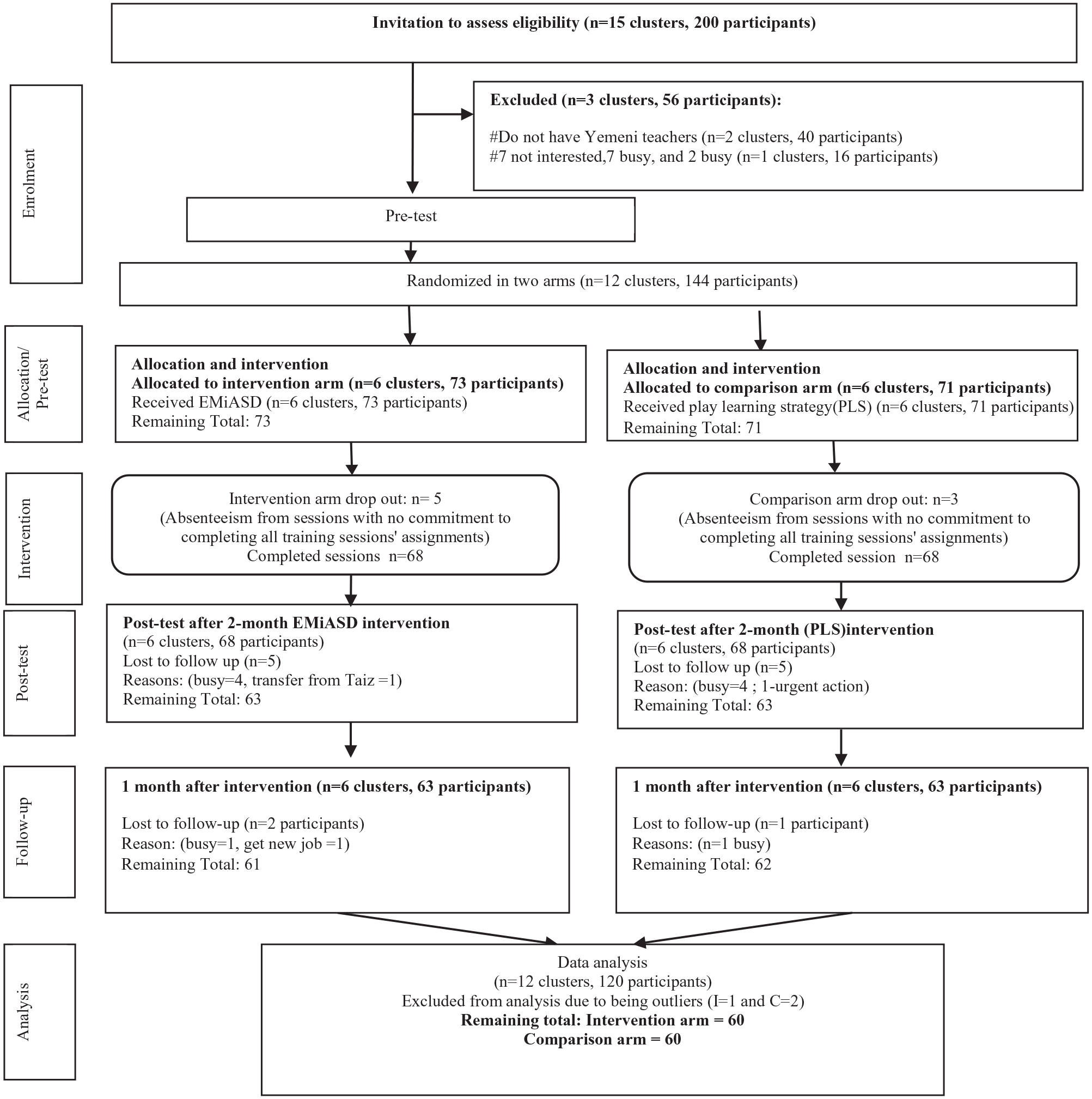
CONSORT flow diagram of the study.
The sample for open-ended responses to video case studies consisted of 44 participants selected from the original sample. Of this sample, 23 participants were selected from the intervention arm and 21 participants were selected for the comparison arm. Four participants dropped out of the video case studies for the following reasons: (1) one of the teachers had urgent travelling during the post-test; (2) two of the teachers were absent for the pre-test; and (3) one teacher was transferred from one school to another. Thus, the final sample for the video case study component of the study consisted of 40 participants.
Effects on content analysis of responses to open-ended questions about video case studies
Two major themes emerged from the analysis are elaborated below.
Theme 1: inaccuracy in identifying autism symptoms
Participants’ responses to video cases (Videos 1 and 2) in the pretest were largely inaccurate. Participants in both the intervention and comparison arms gave inaccurate labels for the child, such as hyperactive, spoiled, naughty, normal child, and problematic behaviour. Some preschool teachers stated that the child’s behaviour is normal and that all children exhibit similar behaviours. The following are quotes from preschool teachers’ responses:
[PST-I4] ‘The child in video 1 appears to be in perfect health. I have a lot of kids who act like him’.
[PST-C12] ‘I believe the child in Video 1 is simply spoiled. He has no issues with his behaviour’.
[PST-I14] ‘The child in Video 1 needs more schooling from his parents, and he will be fine’.
Although some preschool teachers were able to recognize the child had difficulties, they could only provide broad rather than specific descriptions of the kinds of difficulties the child had.
[PST-C8] ‘He has a psychological disorder’.
[PST-I6] ‘The child is abnormal’.
In contrast, in the post-test and follow up test, responses of participants in the intervention arm changed and became more accurate in comparison to responses of participants assigned to the comparison arm.
[PST-I20] ‘The child in Video 1 is an autistic child, whereas the child in Video 2 is ADHD’.
[PST-I19] ‘Previously, I thought that the child in Video 1 was naughty, but now I realize he is an autistic child’.
Theme 2: confusing autism symptoms with ADHD symptoms
In the pretest, participants in both the intervention and comparison arms confused the symptoms of autism with those of ADHD and other behavioural problems in their responses. As can be seen from participants’ responses in the pretest, some preschool teachers indicated that the child in Video 1 (autism case) lacks concentration and has a short attention span, which are symptoms of hyperactivity and ADHD. In addition, some preschool teachers in both arms stated that the child in Video 1 had a speech delay, was feeling bored, was not sleeping well, had behavioural problems, including inattention and introversion:
[PST-I8] ‘The child has delayed speech and ADHD because he can’t explain himself. He also throws stuff around’.
[PST-C9] ‘The child has ADHD – he was moving without purpose’.
Furthermore, some preschool teachers believed that the child in Video 1 was hyperactive. They explained their thoughts by saying:
[PST-I16] ‘He wants to explore the world around him. Furthermore, he shows aggression’.
[PST-C6] ‘He was jumping, moving his hands, and damaging stuff around him’.
[PST-C5] ‘He flung those objects around him and is enraged. He leaps on things, refuses to drink water, and refuses to do his homework because he wants to explore the world around him’.
[PST-C3] ‘He’s a hyperactive individual. He isn’t paying attention. He has a pattern of behavior. The child is unable to focus on what his mother said to him and has lost control of his movement. He also has trouble interacting with others and despises irritating sounds around him’.
With regard to Video 2 (ADHD case), some preschool teachers’ responses in the pretest indicated that they believed the boy was an autistic child, giving the following evidence to support their claim:
[PST-I2] ‘He doesn’t interact with his peers. He does not participate in sing-along activities with others. He imitates other buddies’ behavior. He is irritated by annoyances. He isn’t fond of his food’.
[PST-C5] ‘He prefers to play alone, away from his companions’.
[PST-I7] ‘He flaps his hands and lives in his own universe’.
[PST-C19] ‘He doesn’t listen to his teacher and wants to play by himself’.
Meanwhile, the preschool teachers who stated that the child in Video 2 was an introvert provided the following explanation:
[PST-C14] ‘He does not play with his peers. He doesn’t listen to directions and is irritated by high-pitched sounds’.
[PST-I15] ‘This child despises sharing with his classmates’.
Furthermore, some of the preschool teachers believed that the child in Video 2 was misbehaving:
[PST-I13] ‘The child is impolite, so his parents should control him’.
[PST-C16] ‘I believe he is spoiled’.
In contrast, in the post-test and follow up test, preschool teachers in the intervention arm were able to identify autism symptoms in Video 1:
[PST-I9] ‘I believe he is autistic since he is hyperactive and plays alone. Furthermore, he disobeys orders and throws stuff around. He can’t even play properly. He has trouble to look his mother and doctor in the eye’.
[PST-I10] ‘He doesn’t look people in the eye and repeats himself. I think he is an autistic child’.
[PST-I18] ‘He is an autistic child because he spends a lot of time staring at the ceiling fan and doesn’t listen to orders’.
Responses of preschool teachers assigned to the intervention arm showed a much further developing understanding of ADHD and autism:
[PST-I1] ‘The child is active. He is acting abnormally and is unable to concentrate until his father holds him. He does not follow orders, dislikes annoyances, and is disturbed by high-pitched noises’.
[PST-I3] ‘He has learning problems and repeats his behaviours’.
[PST-I6] ‘He is a very energetic student who despises class activities’.
[PST-I10] ‘He engages in self-directed activities and is unconcerned about his classmates’.
[PST-I18] ‘He is a very energetic person who spends most of his time playing’.
[PST-I5] ‘He repeats his behaviours, so he has learning problems’.
[PST-I9] ‘The toddler lacks focus. He has no concentration and plays by himself’.
However, in the post-test and follow-up test, the responses of participants assigned to the comparison arm remained similar to their pretest responses:
Video 1
[PST-C7] ‘The child is naughty and requires more education’.
[PST-C10] ‘The child is hyperactive and unable to concentrate’.
Video 2:
[PST-C1] ‘The child does not complete his studies and plays with whatever is around him’.
[PST-C13] ‘The child is autistic. He cannot control his movement, so he is continually moving and playing with whatever’.
To sum up, the responses from preschool teachers in both the intervention and comparison arms were inaccurate before the EMiASD session, as evidenced by inaccurate labelling of the autism case as well as confusion of autism symptoms with ADHD symptoms and vice versa. After EMiASD sessions, responses from participants in the intervention arm improved, such that they successfully identified autism symptoms in the child in Video 1 and distinguished them from ADHD symptoms. Meanwhile, responses from participants in the control arm remained inaccurate on all three measurements in the post-test and follow-up test.
Ability to recommend referral
Preschool teachers were asked whether they would recommend the children in Videos 1 and 2 for referral to a specialist. In the pre-test, only 22% of preschool teachers from the intervention arm and 19% of preschool teachers from the comparison arm expressed the need to refer the children in Video 1 (autistic child) and Video 2 (ADHD child) to a specialist. However, in the post-test, the referral recommendations of the intervention arm changed, with 95% of preschool teachers recommending referral of the child in Video 1 to a specialist and 92% recommending referral of the child in Video 2 to a specialist. Furthermore, in the follow-up test, approximately 98% of preschool teachers in the intervention arm recommended referral of the children from both videos to a specialist. In contrast, there was no change in the referral requests of preschool teachers in the comparison arm in the post-test, with only 18% and 19% of preschool teachers recommending referral to a specialist. These findings suggest that the changes in referral recommendation from the pre-test to the post-test and follow-up test observed in the intervention arm were due to participation in the EMiASD intervention.
Effects on knowledge, belief, and self-efficacy concerning autism
Table 2 displays descriptive and inferential statistics by arm and test. For analyses of both the post-test and follow-up test, the pre-test was included as a covariate; however, variation in pre-test scores failed to account significantly for variation in post-test and follow-up test scores in all cases. In terms of knowledge about autism, we observed main effects of arm for both the post-test and follow-up test (see Table 3). These findings indicate that participants assigned to the intervention arm demonstrated greater knowledge, beliefs, and self-efficacy concerning autism than participants assigned to the control arm on both the post-test and the follow-up test, and that this could not be attributed to differences in these factors between participants assigned to the intervention and control arms prior to training. Thus, these findings indicate that the EMiASD effectively increases preschool teachers’ knowledge, beliefs, and self-efficacy concerning autism.
Descriptive and inferential statistics for knowledge, beliefs, and self-efficacy concerning autism for post-test and follow-up test with pre-test as a covariate.
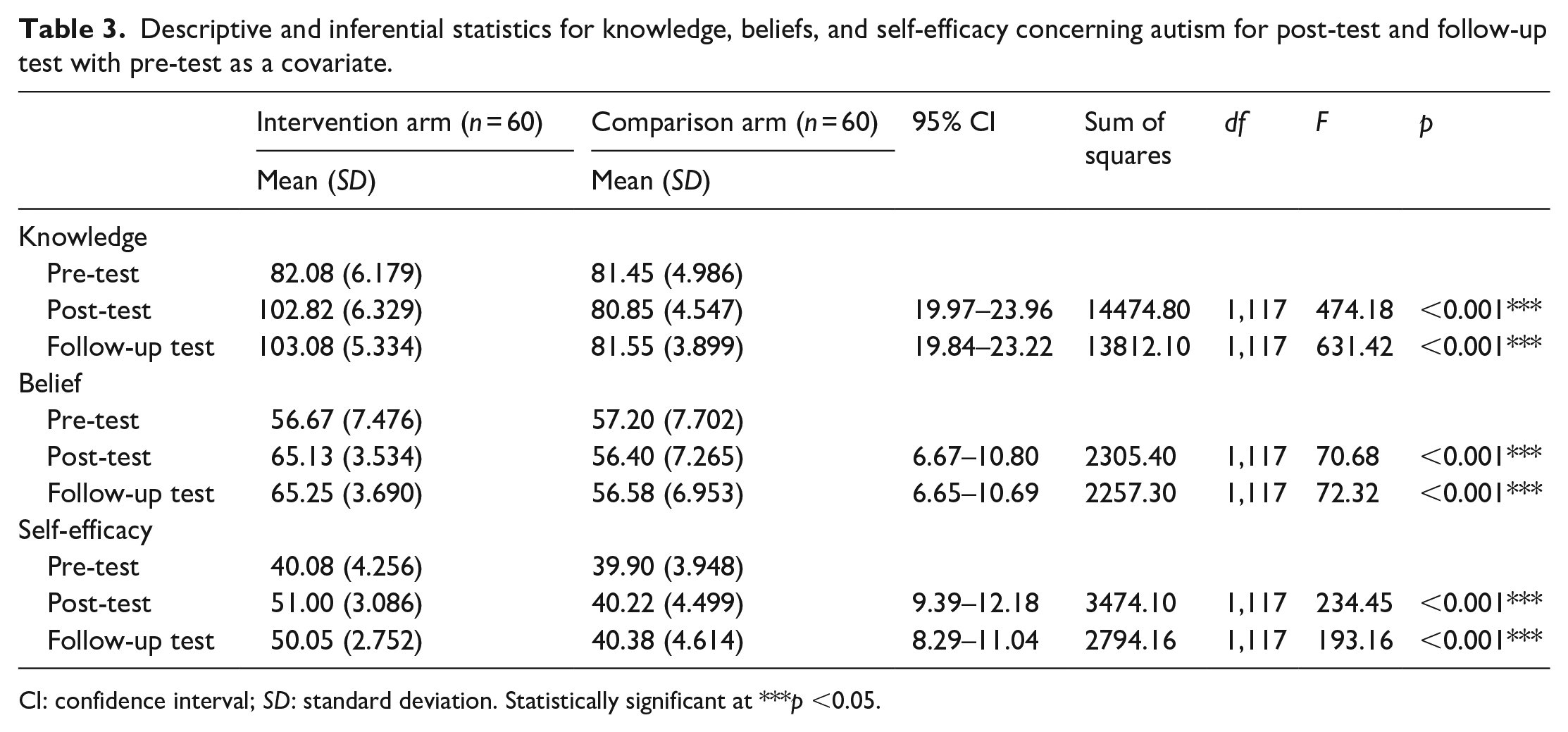
CI: confidence interval; SD: standard deviation. Statistically significant at ***p <0.05.
Discussion
To the best of our knowledge, this study is the first in Yemen to evaluate the efficacy of an educational module (EMiASD) preparing preschool teachers to identify autism and refer children exhibiting autism symptoms to a specialist. This study aimed to educate preschool teachers in Taiz City about children with autism. In addition, it sought to increase the rate of autistic detection in preschools serving the general population. This study evaluated the impact of educational module through two types of data: quantitative data from questionnaires of preschool teachers’ knowledge, belief, and self-efficacy; and open-ended responses to video case studies to comprehensively understand teachers’ ability to identify autism symptoms and recommend referral of children with them to a specialist. The results reveal that the EMiASD increased knowledge, reduced misconceptions, and enhanced self-efficacy among preschool teachers towards autistic children. Moreover, they demonstrate that it improved identification of autism symptoms and referral of children exhibiting these symptoms. The findings highlight the crucial role of preschool teachers in early autism detection and demonstrate the impact of EMiASD in the Yemeni cultural context. Moreover, this study adds further empirical evidence to the literature demonstrating that practical training can enhance the understanding of autism (Daniel et al., 2013; Latouche & Gascoigne, 2019; Samadi, 2020; Samadi et al., 2018).
Based on the study’s findings, preschool teachers’ understanding of autism significantly improved after participating in the EMiASD, whereas knowledge of autism among participants in the comparison arm remained the same. This could be attributed to the information provided by the EMiASD. Notably, the study revealed that preschool teachers were enthusiastic about understanding autism, which may have contributed to their active participation in the EMiASD sessions. The willingness of teachers to learn more about ASD is confirmed also in neighbouring Arab countries such as Oman, Saudi Arabia, and Egypt, where teachers have expressed the need for autism training (Al-Sharbati et al., 2015; Hussein et al., 2011; Obeid et al., 2015). Thus, preschool teachers have demonstrated a willingness to learn, discuss, and share information about autism with caregivers. Hence, this idea suggested that focused educational intervention programmes for preschool teachers may be able to improve low rates of autism identification.
Furthermore, the findings of this study indicate that beliefs concerning autism of preschool teachers in the intervention and comparison arms were inaccurate prior to training. Immediately and a month after training, by contrast, beliefs concerning autism were more accurate in preschool teachers in the intervention arm than the comparison arm, indicating that EMiASD improved them significantly. That is aligned with the previous studies, in which it was found that stigma and positive attitudes can be changed among teachers following an intervention (Sheehy et al., 2020). Other previous studies have found that enhancing knowledge leads to reduced stigma about autism (Al-Sharbati et al., 2015; Lodder et al., 2019; Stronach et al., 2019; van’t Hof et al., 2020). However, some other previous studies showed an increase in knowledge but no change in stigma (Green et al., 2018). Obeid et al. (2015) and van‘t Hof et al. (2020) confirmed the absence of a relationship between stigma and knowledge, suggesting that stigma and beliefs must be tackled directly, rather than being addressed by increasing knowledge. However, Green et al. (2022) highlighted that a single training approach might not be equally practical for different school and cultural contexts. For instance, in the United States, knowledge of autism is higher and stigma towards autism is lower than in Lebanon (Obeid et al., 2015). Accordingly, teachers must be supplied with more information relevant to their culture, as shown in this study through EMiASD.
In this study, the critical self-efficacy of preschool teachers concerning autistic children was low in the pre-test for participants in the intervention and control arms. In contrast, self-efficacy was greater in preschool teachers in the intervention arm than the comparison arm both immediately and 1 month after treatment. This difference may be attributable to commitment to the EMiASD session by the preschool teachers in the intervention arm, which comprised practical assignments to enhance the identification of autism symptoms. These teachers exhibited the motivation to work with autistic children but needed sufficient education to learn how to identify autism, which they received via the EMiASD. This study confirmed the importance of training preschool teachers to manage children with various disorders, including autism (Al-Eryani, 2021; Bameer et al., 2016; Taresh et al., 2019). It is consistent with previous research highlighting the significance of relevant training in increasing teachers’ confidence in discussing issues with parents (Drusch, 2015). Studies have shown that increased knowledge and self-efficacy positively affect teachers’ ability to handle specific disorders, such as ADHD (Able, 2012). Although teachers may be knowledgeable about ADHD, their confidence to identify those children is oftentimes lacking (Latouche & Gascoigne, 2019). Given these points, professional or personal experience is insufficient to increase self-efficacy among preschool teachers (Gillespie-Lynch et al., 2021). Thus, interventions are crucial not only for increasing preschool teachers’ knowledge but also for enhancing their confidence.
Furthermore, poor knowledge of autism negatively impacts preschool teachers’ ability to identify autism symptoms. A previous study in a different cultural context showed that teachers often confuse behaviours associated with autism and ADHD (Able, 2012). In this study, we showed that identification of autism symptoms improved from pre-test to post-test and follow-up test for preschool teachers receiving EMiASD, whereas no such improvement was observed for preschool teachers assigned to the comparison arm, who continued to confuse ASD and ADHD in the post-test and follow-up test. The results are consistent with Desta et al. (2017), who argued that training of teachers leads to increased accuracy in detecting mental health problems.
This study suggests that the EMiASD was highly feasible and acceptable to Yemeni preschool teachers. In particular, it is noteworthy that most teachers attended all sessions and followed through with the assignments and activities in this study. For teachers who dropped out at any point in the study, the most common reason was being busy, and one school did not participate due to a lack of time to implement the intervention, suggesting that time constraints may be a barrier to implementing the EMiASD and collecting the data needed to demonstrate its efficacy. Thus, in scaling up this intervention, it will be important to balance the amount of time needed to train preschool teachers to identify autistic children against the practical constraints of their availability. The school administration set the intervention period, in which the long duration was attributed to the examinations and school holidays. In order to overcome this issue, several module sessions were provided to ensure the information was remembered. Furthermore, this study was limited to only one city in Yemen due to the ongoing war, which meaningfully impacted the expansion of the scope of the study. However, the turnout on the training was high due to teachers’ need to return to normal life to rebuild the country from scratch.
Considering the ongoing conflict in Yemen, there is a limited number of dedicated private centres for autism, mainly located in large cities, making them expensive and inaccessible to many individuals. On the contrary, public centres are more accessible but lack specialized care for autism. The findings of this study highlight the effectiveness of the EMiASD in promoting a community case-finding approach. By training preschool teachers to identify autistic children within the community and refer them to specialized support services, the EMiASD can be a valuable tool in addressing this issue. Consequently, teachers hold the potential to significantly raise autism awareness among Yemeni society, especially among the illiterate population that constitutes 85% of the national total.
Conclusion
This study provides evidence of the impact of the EMiASD training in improving preschool teachers’ ability to identify autism symptoms and increasing the likelihood of referral for further assessment. Schools serve as the most convenient venue for children to be identified as having autism. It is important for global funding organizations to support studies of autism awareness in developing countries such as Yemen. Such support would encourage more research sensitive to these countries’ societal and cultural aspects, broadening our understanding of autistic children. Meanwhile, policymakers should consider using schools to assist poorly developed systems in terms of early detection, management, and societal education about autism. Future studies should explore the influence of comprehensive education for professionals to determine optimal strategies that improve knowledge, beliefs, and behaviours in detecting autism.
Footnotes
Data availability
The datasets analysed for the current study are available from the corresponding author on reasonable request.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.