
Abstract
Robust evidence supports the efficacy of early autism intervention. Despite broad consensus that earlier intervention leads to better outcomes, evidence for this has been limited to correlational studies. This study examined timing effects of the Early Social Interaction (ESI) model, a parent-implemented intervention, using a complete crossover randomized controlled trial (RCT). Effects of Individual-ESI were compared when initiated at 18 or 27 months of age, and also contrasted with effects of the less intensive Group-ESI as an active control condition. Participants included 82 autistic toddlers who received 9 months of Individual-ESI and 9 months of Group-ESI, with the timing/order randomized. Blinded clinicians completed assessments at baseline (18 months of age), end of Condition 1 (27 months), and end of Condition 2 (36 months). Toddlers randomized to Individual-ESI at 18 months showed greater gains during treatment than those starting Individual-ESI at 27 months in receptive/expressive language, social communication, and daily living skills. This pattern was not observed for Group-ESI, demonstrating that timing effects were specific to Individual-ESI and ruling out maturation effects. This RCT demonstrated that earlier intensive, individualized intervention led to greater improvements, and suggests that even a narrow window of 18 versus 27 months may impact child outcomes.
Lay abstract
Behavioral interventions that incorporate naturalistic, developmental strategies have been shown to improve outcomes for young children who receive an autism spectrum disorder (ASD) diagnosis. Although there is broad consensus that children on the spectrum should begin supports as soon as possible, the empirical evidence for this is relatively limited and little is known about the optimal age to start autism-specific interventions. Our team conducted a randomized controlled trial (RCT) to test the effects of starting intervention at different ages, using the Early Social Interaction (ESI) model, a parent-implemented intervention for toddlers on the spectrum. Participants included 82 autistic toddlers and their caregiver(s) who received 9 months of Individual-ESI and 9 months of Group-ESI, with the timing/order of these two treatment conditions randomized. Thus, families received the more intensive and individualized Individual-ESI at either 18 or 27 months of age. Results revealed that children who received Individual-ESI earlier showed greater treatment gains than those who received this intervention later. Gains were demonstrated in several areas, which included the use and understanding of language, social use of communication skills, and self-help skills. Importantly, these findings were specific to the intensive and individualized parent coaching model compared to group-based treatment, allowing us to rule out the possibility that these timing effects were due to children getting older rather than the treatment itself. Our results suggest that even a narrow window of 18 versus 27 months may have an impact on outcomes and underscore the importance of screening and evaluation as young as possible.
Early intervention can have long-term benefits for autistic children (Anderson et al., 2014; Estes et al., 2015; Pickles et al., 2016), as early differences in social attention associated with autism are hypothesized to lead to cascading effects on learning and developmental outcomes (Dawson et al., 2012; Klin et al., 2020).
A growing number of randomized controlled trials (RCTs) have demonstrated the efficacy of naturalistic, developmental behavioral interventions (NDBIs) in toddlers diagnosed with autism spectrum disorder (ASD; Tiede & Walton, 2019). Across studies, effects have differed somewhat across service delivery models (i.e. clinician- or parent-implemented) and specific domains targeted (see Landa, 2018 for review). For example, the landmark Early Start Denver Model trial (Dawson et al., 2010) compared clinician-implemented intervention and treatment as usual, and showed large effects on developmental and adaptive behavior measures, but not social skills.
Strong support for parent-implemented interventions is also emerging (Nevill et al., 2018), in part due to the feasible and cost-effective nature of this treatment modality. Within this mode of treatment delivery, effects on child outcomes are mediated by parents, who learn to implement evidence-based strategies into their child’s natural environment thereby promoting generalization. Effects on proximal outcomes such as parent responsivity and synchrony, parent stress, and specific child skills targeted by the interventions (e.g. imitation, joint attention, play) have been reported (Carter et al., 2011; Estes et al., 2014; Green et al., 2010; Kasari et al., 2010, 2015; Rogers et al., 2012; Siller et al., 2013). A small but growing number of RCTs have also demonstrated impacts on more distal outcomes (Hardan et al., 2015; Schertz et al., 2013; Wetherby et al., 2014), including one study demonstrating long-term effects on social skills into school age (Pickles et al., 2016). This follow-up of the Preschool Autism Communication Trial (PACT) trial revealed reductions in autism symptoms and greater initiation of social communication following a preschool parent-implemented intervention compared to treatment as usual, demonstrating the continuing impact of teaching parents to support their child’s social communication development (Pickles et al., 2016).
Despite substantial progress in treatments for toddlers on the autism spectrum, several important questions remain. There is strong consensus that earlier intervention is key—ideally under age three—but empirical support for this notion is mixed (see Towle et al., 2020 for review). Emphasis on early intervention is predicated upon the theory it capitalizes on early brain plasticity to achieve greater gains than would be possible later in childhood, potentially preventing the cascading effects of early social communication difficulties and repetitive behaviors on other domains of functioning (e.g. cognition and language). While earlier intervention has been associated with more positive outcomes in several prospective studies (Anderson et al., 2014; Rogers et al., 2012; Smith et al., 2015; Vivanti et al., 2019), others have failed to detect an effect of age (e.g. Tiura et al., 2017). The equivocal nature of the existing literature may be due to differences among studies in the intensity and duration of treatment, child ages at treatment initiation, and the domains of functioning considered (as different outcomes may have varying malleability at different ages). Further limiting the evidence for earlier intervention is the fact that the correlational methods used in these existing studies cannot determine causality, as none have randomized age at treatment initiation, leaving the possibility of selection bias driving the results. Experimental studies that specifically test timing effects are needed, in order to bolster evidence for earlier intervention and guide recommendations for the optimal age of intervention.
The current treatment literature in toddlers is also limited by the relative lack of community-screened samples, as most studies have used clinically referred samples (though there are notable exceptions; Baranek et al., 2015; Wetherby et al., 2014). In fact, this dearth of data on treatment outcomes for children identified by screening rather than parent/professional concern was cited by the United States Preventive Services Task Force (USPSTF) as one of several barriers to recommending universal screening for ASD under 30 months (Siu & U.S. Preventive Services Task Force (USPSTF), 2016).
Early Social Interaction (ESI) model
The Early Social Interaction (ESI) model (Wetherby et al., 2014, 2018; Wetherby & Woods, 2006) is a parent-implemented intervention for toddlers diagnosed with ASD that integrates evidence-based strategies blending behavioral and developmental techniques, and was included in the original description of NDBIs (Schreibman et al., 2015). ESI incorporates the SCERTS curriculum as the developmental framework to target and monitor child outcomes in social communication and emotional regulation (Prizant et al., 2006) and a coaching model based on principles of adult learning to teach parents to implement these evidence-based strategies in their everyday activities (Wetherby & Woods, 2006) in natural environments (see Supplemental online document for details on the evidence-based strategies used in ESI, the SCERTS framework, and the coaching model).
Our team completed a multi-site RCT of the ESI model, which compared two active treatment conditions: an intensive, individualized parent-coaching intervention (Individual-ESI) and a less-intensive parent-education group (Group-ESI; Wetherby et al., 2014). Both treatment conditions taught parents strategies to support their child’s social communication in everyday activities, but differed in format and intensity (see Methods for more detail). A complete crossover design was employed, such that the two ESI treatment conditions were implemented sequentially, with the order of the conditions randomized. Thus, children were randomized to receive either Individual-ESI or Group-ESI at ~18 months of age for 9 months of treatment, and then crossed over to receive the other treatment condition at ~27 months of age. Though many crossover studies consider timing/order effects to be a potential confound, we were particularly interested in this effect, so chose to specifically test, rather than control for, timing effects. Thus, the crossover design allowed us to empirically test two aspects of treatment: effects of treatment format/intensity and treatment timing.
Treatment format/intensity effects of the ESI model have been previously reported, in a paper that compared Individual-ESI and Group-ESI during the first condition (Wetherby et al., 2014). Results indicated that children randomized to receive the more intensive, individualized Individual-ESI at ~18 months of age made greater gains in a number of key developmental areas, as compared to children randomized to Group-ESI. Treatment effects were observed on distal outcomes including receptive language and social communication skills, two critical targets for early intervention for toddlers on the spectrum. Importantly, these effects were observed across parent-report and clinician-administered measures, making these findings particularly robust. Treatment effects were also observed on a parent-report measure of daily living skills, likely reflecting ESI’s emphasis on natural environments. In addition to these distal outcomes, treatment effects were demonstrated on child active engagement, a more proximal measure of targeted treatment outcomes than standardized assessments (Wetherby et al., 2018).
The objective of the present study was to test timing effects of ESI within this RCT design, using quasi-experimental comparisons of treatment timing. Specifically, we hypothesized that children randomized to receive Individual-ESI at ~18 months would show greater gains during Individual-ESI treatment than children randomized to receive Individual-ESI at ~27 months. Importantly, we also hypothesized that timing effects would be specific to Individual-ESI and not Group-ESI, such that the intensive, individualized treatment condition would show treatment timing effects, but the broader parent education group would not. Finally, we explored whether timing effects differed by recruitment method—community-screened or clinically referred.
Methods
Design and setting
This multisite, complete crossover RCT was conducted at Florida State University (FSU) and the University of Michigan (UM) and registered at clinicaltrials.gov (Identifier NCT00760812). Children entered the study at 18 (±2) months and were randomly assigned to receive either Individual-ESI or Group-ESI during Condition 1 (~18–27 months of age) and then crossed over to receive the other treatment during Condition 2 (~27–36 months of age). Thus, children received both treatment conditions, with the timing of Individual-ESI randomly assigned (starting at ~18 or 27 months). FSU and UM Institutional Review Boards approved this study and parents gave written informed consent for participation.
Recruitment and eligibility
Children were recruited between February 2007 and December 2011. At FSU, children were recruited through community screening through the FIRST WORDS® Project, in which children in pediatric primary care settings are screened with the Infant-Toddler Checklist (Wetherby & Prizant, 2002; see Wetherby et al., 2014 for more information on screening procedures). At UM, children were recruited through referrals based on parental/professional concern or elevated likelihood of ASD because of an older sibling on the autism spectrum.
Children were included if they were diagnosed with ASD at 18 (±2) months, lived within 50 miles of either site, and had no significant sensory or motor impairments. A best-estimate diagnosis of ASD was made by expert clinicians using multiple sources of information: the Autism Diagnostic Observation Schedule–Toddler Module (ADOS-T; Lord, Luyster, et al., 2012), symptom rating from a video-recorded home observation (Dow et al., 2020), parent report of autism symptoms (Wetherby et al., 2021), and standardized measures of development (Mullen, 1995) and adaptive behavior (Sparrow et al., 2005).
Randomization
Pairs of children were matched on baseline nonverbal developmental level using a computerized trickle-process for random assignment (Braucht & Reichardt, 1993; Shadish et al., 2002). A computer-generated list was used to randomly assign the first member of each pair to Individual-ESI or Group-ESI in Condition 1 and the second member assigned to receive the other treatment in Condition 1. The trickle process allowed children to be enrolled over time, as the matched pair was filled when the second member matching that developmental level was determined eligible. This allowed all children to be enrolled immediately, rather than waiting to enroll matched pairs at the same time, which would have delayed treatment for the first member of the pair.
Intervention procedures
Individual-ESI and Group-ESI each utilized the SCERTS curriculum (Prizant et al., 2006), a manualized curricular-based assessment to prioritize and monitor child intervention targets. SCERTS refers to Social Communication (SC), Emotional Regulation (ER), and Transactional Support (TS), which are three primary dimensions targeted to support the development of children with ASD and their families. The ESI model has a “layer cake” of 13 evidence-based strategies and supports, adapted from the SCERTS developmental framework and incorporating behavioral techniques that reflect the common features of NDBIs delineated by Schreibman et al. (2015). The “layer cake” metaphor provides an order for parents to learn the strategies, activity by activity, starting with Layer 1 and highlights the cumulative nature of the three layers of support to build a shared agenda in Layer 1, social reciprocity in Layer 2, and then better skills in Layer 3 (see Supplemental online document for details on the ESI model).
Individual-ESI
Individual-ESI was conducted in a 1:1 format designed to achieve treatment intensity, and included individualized treatment targets. This treatment condition included individual parent coaching sessions three times per week (2 home, 1 clinic) for 6 months, and 2 sessions per week (1 home, 1 community setting) for the last 3 months for maintenance and generalization. One or two primary parents/caregivers 1 were trained to implement these strategies by master’s-level interventionists.
Individual targets were identified and updated through collaborative consensus building between interventionists and parent(s). SC targets included expanding the spontaneous use of gestures, sounds, words, and joint attention, responding to social bids, understanding words, functional object use and pretend play, and extending reciprocity in interaction. ER targets included being available for learning and expressing emotion, expanding self-regulatory strategies to calm when dysregulated, communicating to regulate emotion when frustrated or help is needed, and using regulatory strategies to stay engaged in activities and handle new and changing situations. The TS domain included teaching parents the intervention strategies and learning supports that were selected to help the child meet individualized treatment targets.
During individual intervention sessions, a four-step collaborative coaching model was used. The interventionist and parent worked collaboratively to (1) identify what worked for each parent–child dyad with the interventionist using observation, direct teaching, and demonstration/modeling with explanation as needed to increase the parent’s understanding; (2) guide the parent’s practice embedding intervention, provide feedback, and engage the parent in problem solving about the practice; (3) repeat with parent-led practice and reflection on the child and parent’s participation; and (4) decide when the interventionist should back out for parent independence. The interventionist coached the parent in each new activity at the first level and moved to level four as quickly as possible to promote parent competence, confidence, and independence. Coaching in a variety of everyday activities promoted generalization of parent learning so the parent could support the child’s learning throughout the day as planned or as opportunities arose. Parents were asked to implement strategies with their child for 20 hours per week to achieve treatment intensity. Interventionists established ⩾ 80% fidelity on 3 of 4 sessions for 20 core features of the model using weekly videotaped sessions, prior to the start of the study. Fidelity was monitored for 20% of sessions, with an average of 81% fidelity.
Group-ESI
In contrast, the goal of Group-ESI was to provide a parent education group to serve as an active control condition to engage families when they were not receiving the more intensive Individual-ESI and minimize attrition. Group-ESI was designed to be low intensity and did not include specific, personalized parent coaching or individualized treatment targets. Instead, it offered information and education drawn from the SCERTS curriculum and peer support from other parents.
This treatment condition included one session per week in the clinic, attended by groups of four to five families and led by group interventionists. During the first week of every month, 1 of 9 topics from the SCERTS curriculum was presented in a parent educational meeting. The remaining three sessions per month were playgroups that provided parents with opportunities to discuss and practice intervention strategies and supports in a group setting. Parents were guided to practice interacting with their child on the topic of the day and were given general feedback. Group interventionists established ⩾ 80% fidelity on 10 core features of the model using videotaped sessions, prior to the start of the study. Fidelity was monitored for 20% of sessions with an average of 88%.
Outcome measures
Experienced clinicians, blind to treatment condition, conducted assessments at baseline (~18 months), end of Condition 1 (~27 months), and end of Condition 2 (~36 months). Families were provided a monetary incentive of $100 for each evaluation to offset participation costs and time.
Social communication skills
The Communication and Symbolic Behavior Scales (CSBS) Behavior Sample (Wetherby & Prizant, 2002) is a standardized assessment designed to elicit social communication behaviors during a face-to-face interaction in toddlers. It yields norm-referenced composite scores in three areas: Social (gaze shifts, shared positive affect, response to joint attention, and the form and function of social communication behaviors), Speech (use of sounds and words for communication), and Symbolic (representational skills demonstrated through understanding of words/gestures as symbols and symbolic play).
Modified raw scores were used, as they yield greater normality and sensitivity to change compared to raw or standard scores in children over 24 months. Raw scores were modified by rating the frequency of each item up to three times per activity (standard scoring allows for once per activity) within each of the 6 CSBS activities, thereby extending the maximum score for each composite (Social composite range = 0–136, Speech = 0–98, Symbolic = 0–106).
Developmental level
The Mullen Scales of Early Learning (MSEL; Mullen, 1995) is a standardized, norm-referenced measure of early development that yields T-scores for Visual Reception, Fine Motor, Receptive Language, and Expressive Language domains (M = 10, standard deviation [SD]= 10).
Adaptive behavior
The Vineland Adaptive Behavior Scales, Second Edition (VABS-II; Sparrow et al., 2005) is a parent-report interview that yields standard scores for Communication, Daily Living, Socialization, and Motor Skills domains (M = 100, SD = 15). Expressive and Receptive Language, and Fine and Gross Motor subdomains v-Scale scores (M = 15, SD= 3) were also examined.
Autism symptoms
The ADOS/ADOS-2 (Lord et al., 1999; Lord, Luyster, et al., 2012; Lord, Rutter, et al., 2012) is a standardized, semi-structured observation of autism symptoms. Comparison scores in two domains (Social Affect [SA] and Restricted, Repetitive Behavior [RRB]) were used (range = 1–10), as they reduce the influence of age, language, and module (Esler et al., 2015; Hus et al., 2014) compared to raw scores.
Demographic data
Parents self-reported child race, biological sex, and maternal age and education (used as a proxy for socioeconomic status).
Statistical analyses
Within this crossover RCT, quasi-experimental comparisons were made using analysis of variance (ANOVA)-based a priori contrasts (main effects: time and treatment condition timing). Using an intent-to-treat analysis, all available data from all participants were included in analyses regardless of treatment dropout status, with full information maximum likelihood employed for missing data. Only specific, planned comparisons that tested study hypotheses were conducted, rather than all possible comparisons. Comparisons tested the difference in change from pre- to post-Individual-ESI treatment between the group randomized to receive Individual-ESI in the first 9-month condition, which started at ~18 months (i.e. Condition 1; 18–27 months) and the group randomized to receive Individual-ESI in the second 9-month condition, which started at ~27 months (i.e. Condition 2; 27–36 months).
Crossover RCTs allow for these quasi-experimental tests of treatment timing effects, although they confer a possible confound of receiving two different treatments and resulting carryover effects. Indeed, children who received Individual-ESI starting at 27 months had just completed Group-ESI, and were compared to children starting Individual-ESI at 18 months without previous treatment. Medication trials often guard against potential carryover effects by including a washout period between treatments; however, this is not feasible when treatment effects are not intended to wash out when the treatment ends. Instead, potential carryover effects were carefully considered when interpreting results. Within this crossover design, a pattern of greater gains during Condition 1 (~18–27 months) than during Condition 2 (~27–36 months) can only be attributed to treatment timing, not carryover effects. Significant effects in favor of Condition 2 may be due to carryover effects given that the greater change could be the result of previous treatment during Condition 1. Thus, only effects in favor of Condition 1 were interpreted as treatment timing effects.
A second potential confound is maturation, given that this study did not include a no-treatment control group. Instead, Group-ESI served as the control or comparison group. RCTs with an active control condition define treatment effects as greater improvements in the experimental treatment condition (i.e. Individual-ESI) compared to the active control condition (Group-ESI), conferring the ability to rule out maturation effects. Similarly, this crossover RCT with an active control condition defined treatment timing effects as greater improvements during Condition 1 compared to Condition 2 in the experimental treatment condition (i.e. Individual-ESI) but not in the active control condition (i.e. Group-ESI). In other words, timing effects observed only in Individual-ESI were interpreted as due to the effect of the more intensive, individualized treatment (i.e. treatment timing effects). However, maturation and timing effects could not be disentangled when timing effects were significant for both treatments. In this case, the greater gains during Condition 1 for both treatments could be due to either timing effects observed for both treatments or due to maturation effects such that all children show greater change at earlier ages regardless of treatment, and this cannot be disentangled.
Thus, a significant treatment timing effect was defined as significantly greater change during Condition 1 than Condition 2 for Individual-ESI and no greater change during Condition 1 than Condition 2 for Group-ESI, because this pattern could be attributed to treatment timing but not to maturation effects. Significantly greater change during Condition 1 than Condition 2 for both Individual-ESI and Group-ESI was not considered a treatment timing effect, because maturation could not be ruled out.
Secondary analyses of the effect of recruitment method on timing effects were conducted using three-way ANOVAs (main effects: time, treatment condition timing, site) rather than planned comparisons, given the lack of a priori hypotheses about differential timing effects in community-screened and clinically referred samples. Significant interactions were followed up with contrasts comparing timing effects across FSU (community-screened) and UM (clinically referred) samples.
Community involvement
While the ESI and SCERTS models were developed using key stakeholder input, there was no formal community involvement in this study.
Results
Participants
Of 135 referred children, 53 were excluded for the following reasons: did not meet inclusion criteria (20), enrolled in another treatment study (28), or declined to enroll in this study (5). Of the 82 eligible children, 42 were randomized to receive Individual-ESI and 40 were randomized to Group-ESI in Condition 1 (see Figure 1). See Table 1 for participant demographics and Table 2 for outcome variable descriptive statistics at each time point.
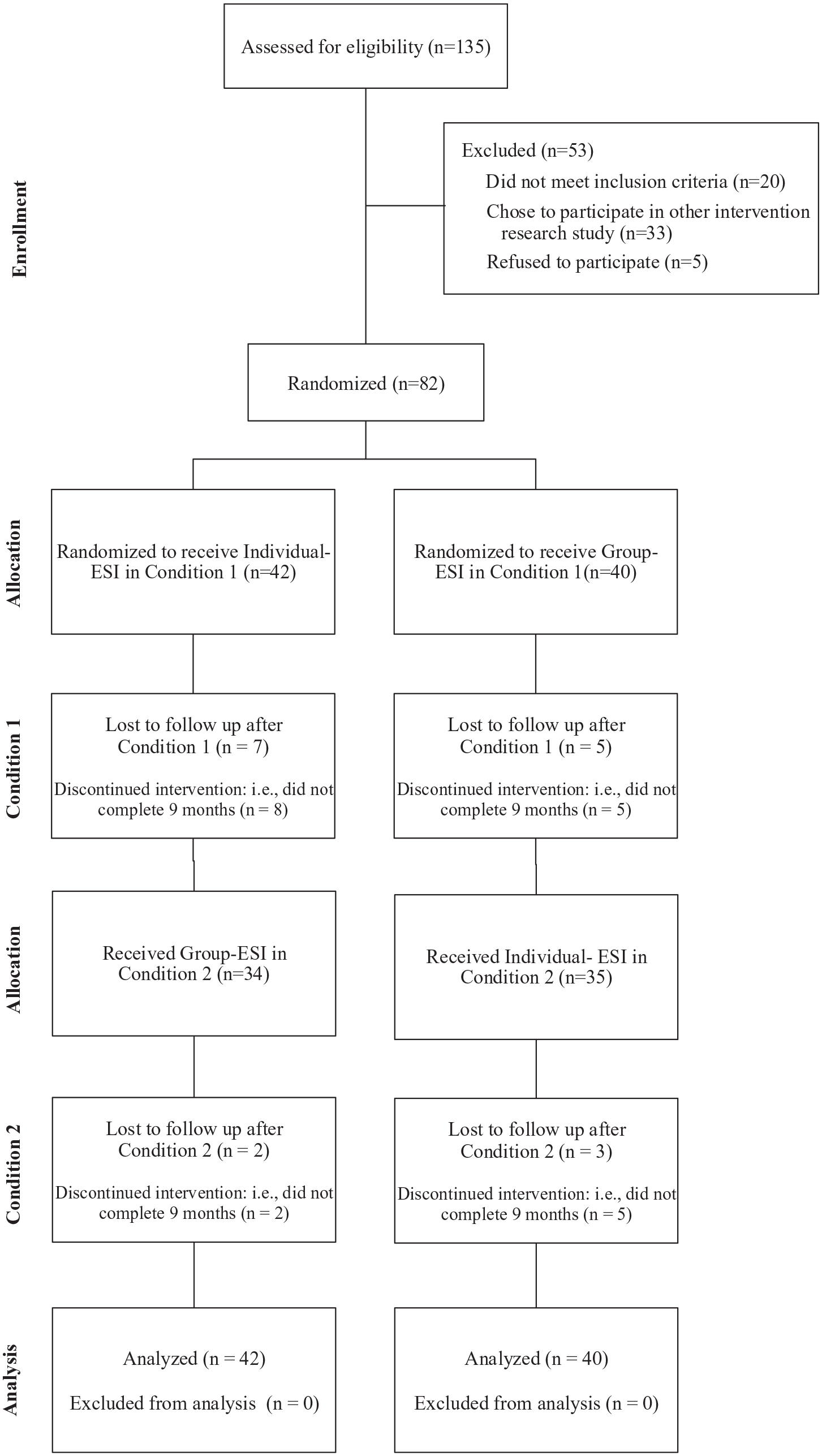
CONSORT diagram of participant flowchart.
Participant demographics by treatment timing group.
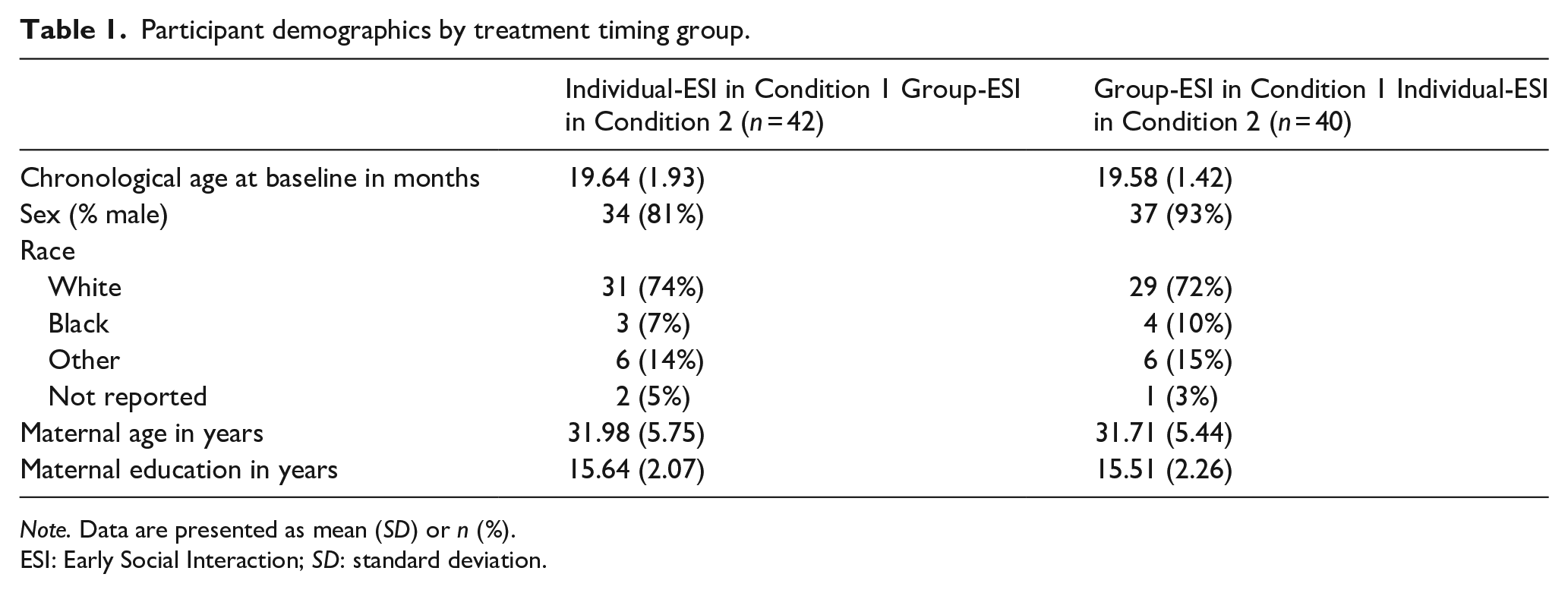
Note. Data are presented as mean (SD) or n (%).
ESI: Early Social Interaction; SD: standard deviation.
Child assessment measures at each time point by treatment timing group.
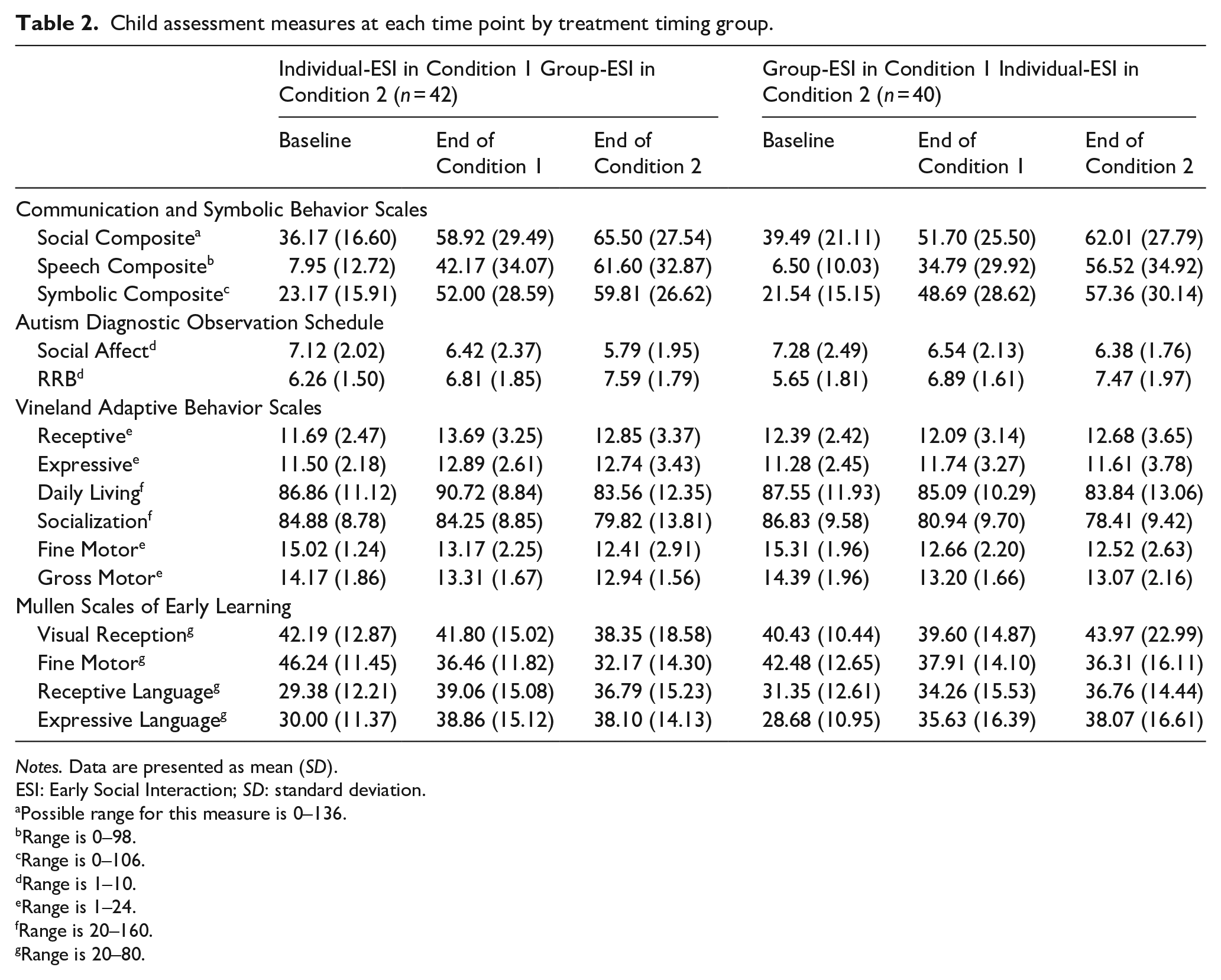
Notes. Data are presented as mean (SD).
ESI: Early Social Interaction; SD: standard deviation.
Possible range for this measure is 0–136.
Range is 0–98.
Range is 0–106.
Range is 1–10.
Range is 1–24.
Range is 20–160.
Range is 20–80.
As previously reported by Wetherby et al. (2014), the matching procedure yielded baseline equivalency between treatment timing groups (i.e. Individual-ESI in Condition 1 and Individual-ESI in Condition 2). Baseline differences between the community-screened and clinically referred samples were also not observed, with the exception of MSEL Visual Reception and Fine Motor scores (Wetherby et al., 2014). Treatment timing groups did not differ in total hours of other community interventions received during Condition 1 or 2.
Attrition, defined as failure to complete at least one follow-up assessment measure regardless of treatment completion, was low; 87% completed the assessment after Condition 1% and 82% completed the assessment after Condition 2. Attrition did not significantly differ by treatment timing group or site.
Outcomes showing significant treatment timing effects
Significant timing effects of Individual-ESI only
As noted above, significant treatment timing effects were defined as significantly greater change during Condition 1 than Condition 2 for Individual-ESI and no greater change during Condition 1 than Condition 2 for Group-ESI, because this pattern could be attributed to treatment timing but not to maturation effects.
Planned comparisons revealed that children who received Individual-ESI in Condition 1 at 18 months showed significantly greater gains during the 9-month treatment period, compared to children who received Individual-ESI during Condition 2 at 27 months across several domains (see Table 3). Planned comparisons were non-significant for Group-ESI for these outcome variables, suggesting that maturation effects cannot explain these differences and significant timing effects were specific to Individual-ESI.
Linear mixed model results with planned comparisons testing timing effects.
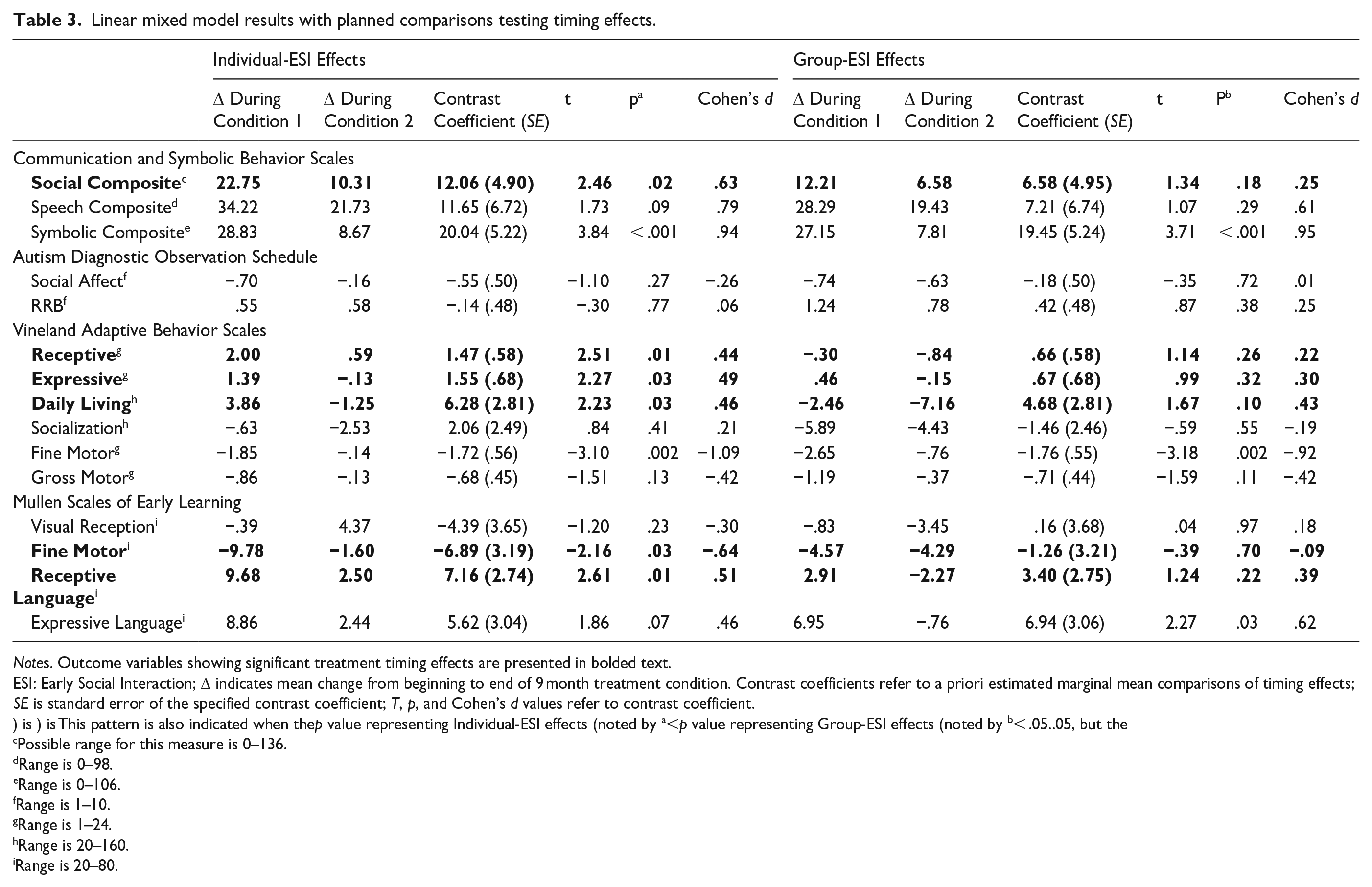
Notes. Outcome variables showing significant treatment timing effects are presented in bolded text.
ESI: Early Social Interaction; Δ indicates mean change from beginning to end of 9 month treatment condition. Contrast coefficients refer to a priori estimated marginal mean comparisons of timing effects; SE is standard error of the specified contrast coefficient; T, p, and Cohen’s d values refer to contrast coefficient.
) is ) is This pattern is also indicated when thep value representing Individual-ESI effects (noted by a<p value representing Group-ESI effects (noted by b< .05..05, but the
Possible range for this measure is 0–136.
Range is 0–98.
Range is 0–106.
Range is 1–10.
Range is 1–24.
Range is 20–160.
Range is 20–80.
Significant treatment timing effects were observed for both measures of receptive language; children who received Individual-ESI in Condition 1 showed an average increase of 9.68 T-score points on the MSEL and 2.00 v-scale points on the VABS-II, while children who received Individual-ESI in Condition 2 showed significantly smaller increases (MSEL: 2.51 T-score points; VABS-II: 0.59 v-scale points). Significant timing effects were also observed for expressive language (VABS-II) and social communication skills (CSBS Social), as children who received Individual-ESI in Condition 1 showed greater gains (1.30 v-scale points and 22.75 raw score points respectively), while children who received Individual-ESI in Condition 2 showed a decrease (-.13) and significantly smaller increase (10.31) in these domains respectively. Figure 2 depicts mean scores at baseline, end of Condition 1, and end of Condition 2 for both treatment timing groups for four outcome variables, which were selected to illustrate three different patterns of significant treatment timing effects and one pattern of no significant treatment timing effects.
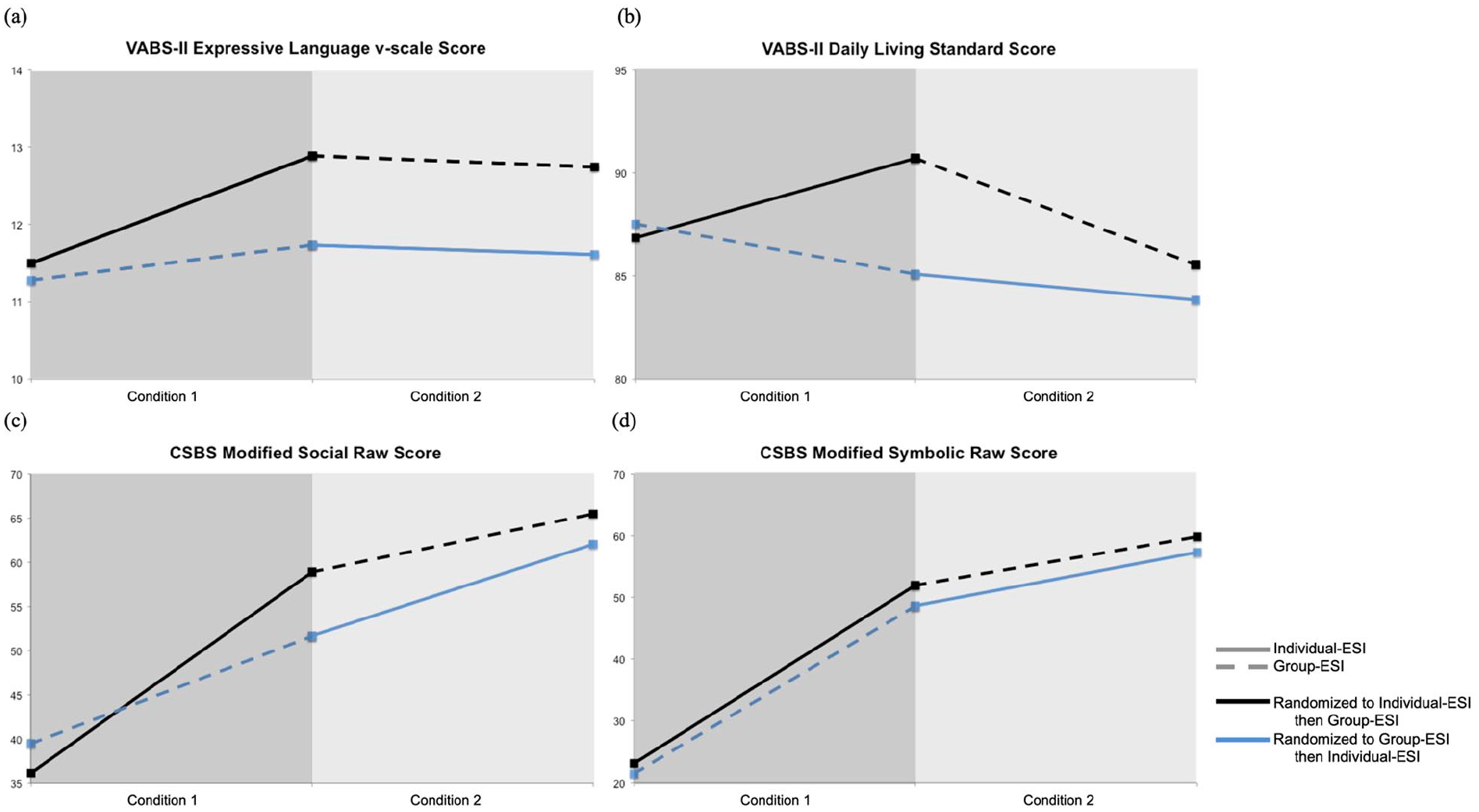
Mean scores for selected outcome variables at baseline, end of Condition 1, and end of Condition 2 by treatment timing group.
A significant timing effect was also observed for VABS-II Daily Living. Children who received Individual-ESI in Condition 1 showed an increase of 3.87 standard score points across the 9-month treatment period while children who received Individual-ESI in Condition 2 showed a decrease of 1.24 standard score points. Planned comparisons were not significant for Group-ESI, confirming the expected pattern associated with a significant effect of timing of intervention. Of note, the decreases in VABS-II standard scores observed in Individual-ESI during Condition 2 do not indicate a loss of skills for this group, because the corresponding age equivalent scores increased. Instead, this decreasing standard score indicates that children receiving Individual-ESI during Condition 2 failed to make age-appropriate progress during treatment.
Finally, significant timing effects of Individual-ESI were observed for MSEL Fine Motor scores, but in the opposite direction hypothesized. Greater growth was observed during Condition 2 than Condition 1 for Individual-ESI, as evidenced by smaller decreases in T scores (and larger increases in age equivalents) during Condition 2. As was the case for Daily Living Skills, the decreases in T scores did not reflect a loss of skills, but rather a failure to make age-appropriate gains. Planned comparisons were not significant for Group-ESI. As noted in the Methods section, this effect of Individual-ESI in favor of Condition 2 cannot be interpreted as a significant treatment timing effect, as carryover effects cannot be ruled out.
Outcomes not showing hypothesized treatment timing effects
Significant timing effects of Group-ESI only
A significant planned comparison was observed for Group-ESI on MSEL Expressive Language scores, as children showed greater growth during Condition 1 than Condition 2. The pattern and magnitude of results was similar for Individual-ESI, though the planned comparison between Condition 1 and Condition 2 within this condition did not reach statistical significance (p = 0.07, d = .42).
Significant effects of both Individual-ESI and Group-ESI
Planned comparisons for both Individual-ESI and Group-ESI were significant for CSBS Symbolic scores, indicating greater gains during Condition 1 than Condition 2 for both treatment conditions. This pattern of results cannot disentangle maturation and treatment timing effects for this variable.
Planned comparisons were also significant for both treatments on VABS-II Fine Motor scores, although in the opposite direction as hypothesized. Children in both treatments showed more growth during Condition 2 than Condition 1, as decreasing standard scores were observed during Condition 1 and stable scores were observed during Condition 2 (note that age equivalents increased in both groups during both treatment conditions, again not supporting a loss of skills). For this variable, neither carryover effects nor maturation can be ruled out.
No significant timing effects of Individual-ESI or Group-ESI
Planned comparisons were not significant for Individual-ESI or Group-ESI on VABS-II Social, ADOS-2 Social Affect, ADOS-2 RRB, CSBS Speech, MSEL Visual Reception, and VABS-II Gross Motor variables.
Effects of recruitment method
Three-way interactions that included site were nonsignificant for all outcome variables (interaction term p value > 0.05), demonstrating equivalent treatment effects across the community-screened and clinically referred samples, with one exception. Omnibus testing was significant for the interaction of treatment timing group, time, and site for ADOS RBB scores (p = 0.04), suggesting possible effects of recruitment method; however, follow-ups revealed that the specific treatment timing effects investigated in this study did not significantly differ between the community-screened and clinically referred samples (p = 0.71).
Discussion
This study demonstrated significant effects of the timing of the Individual-ESI treatment condition on child outcomes using an RCT design. These treatment timing effects were specific to Individual-ESI, which included individualized treatment targets developed collaboratively with parents and interventionists as well as specific parent coaching on implementation of the treatment strategies. This is in contrast to Group-ESI, which used the same SCERTS curriculum but offered parent education and playgroups without individualization or specific coaching. Interestingly, each of the domains that showed significant treatment timing effects was a skill set specifically targeted by the ESI model (see below).
Toddlers randomized to Individual-ESI at 18 months showed significantly greater gains in receptive and expressive language compared to toddlers randomized to Individual-ESI at 27 months. For example, children who received Individual-ESI earlier showed an improvement of almost one standard deviation on the MSEL Receptive and Expressive Language domains, compared to significantly smaller gains in children who received this treatment condition later. While all children began to catch up on language skills relative to same-aged peers, regardless of treatment timing, earlier Individual-ESI was associated with significantly greater improvement than later Individual-ESI. Timing effects for receptive language were particularly robust, as they were observed across the clinician-administered and parent-report tools (i.e. MSEL and VABS-II).
Toddlers who received Individual-ESI at 18 months also showed significantly greater gains in social communication skills on the CSBS. As was the case with language skills, these gains were substantial, as children receiving Individual-ESI earlier showed a 23 raw score point increase on the CSBS Social Composite, while those who received it later improved only 10 points (range on this measure is 0–136). Improvements on the CSBS Social Composite reflect gains in the frequency of specific social communication skills during the Behavior Sample, including gaze shifts, shared positive affect, and communication for the purpose of behavior regulation, joint attention, and social interaction. Other measures in the social domain (ADOS-2, VABS-II) did not reveal significant timing effects, though this may be due to differences in measurement modality or the specific constructs measured. For example, the CSBS measures specific social communication behaviors based on an observational sample rated by expert clinicians who were blind to treatment condition, while the VABS-II measures a broader range of social skills reported by parents, who could not be blinded to condition. In addition, CSBS items measure frequency of specific skills observed, while ADOS-2 items focus on the presence/absence (and clarity) of autism symptoms. As such, greater change might be expected on CSBS compared to the ADOS-2 items. In fact, very little change was observed for either treatment timing group in either condition on the ADOS-2 (i.e. improvements of < 1 point on the SA and RRB comparison scores), making it difficult to detect possible differences on this measure.
Finally, treatment timing effects were demonstrated on daily living skills, such that children receiving Individual-ESI earlier showed small increases in standard scores during treatment while those receiving it later showed small decreases (though raw and age-equivalent scores increased for both treatment timing groups). These findings likely reflect the importance placed on daily living skills within the ESI treatment model. Individual-ESI coaching sessions encouraged parents to embed treatment strategies into a wide variety of everyday activities, including caregiving (e.g. teeth brushing, bath time) and family chores (e.g. laundry). Earlier exposure to these daily living skills and increased expectations through individual coaching sessions at home may have provided a context for specific gains in this area.
In contrast to receptive/expressive language, social, and daily living skills, younger toddlers showed greater gains in symbolic skills than did older toddlers during both Individual-ESI and Group-ESI. However, neither timing effects nor maturation can be ruled out, given that this pattern was observed in children in both treatment timing groups, and the study design did not include a no-treatment control group.
A different pattern of results was observed for fine motor skills, as greater growth was observed in older toddlers (from 27–36 months) than younger toddlers (from 18–27 months). For the clinician-administered measure of fine motor skills, this effect was specific to Individual-ESI, suggesting that Individual-ESI may lead to greater growth in the fine motor domain for older rather than younger toddlers. However, carryover effects from the first condition (i.e. Group-ESI during Condition 1) on improvements in the second condition (i.e. Individual-ESI during Condition 2) cannot be ruled out. In contrast, this pattern of greater improvement from 27–36 months was observed for both treatments on parent-reported fine motor skills, suggesting that this may not be a result of treatment timing effects, but possible maturation effects. This finding may instead reflect the developmental trajectory of fine motor skills in this age range (Landa & Garrett-Mayer, 2006). Given that neither of the ESI treatments specifically targeted fine motor skills, additional research is needed to elucidate the relationship between early social communication treatment timing and fine motor skills.
A significant timing effect was observed for Group-ESI on MSEL expressive language skills, while the effect fell just short of statistical significance for Individual-ESI (p = 0.07, d = 0.42). Though it is possible that treatment timing only significantly impacted the less intensive Group-ESI treatment, the lack of significant effect for Individual-ESI may instead be due to limited power to detect effects of this magnitude. This explanation for these findings is further bolstered by the significant treatment timing effect found for expressive language on the VABS-II.
Timing effects were not found for the remaining outcomes (i.e. gross motor and visual reception), likely reflecting the fact that neither of the ESI treatment conditions specifically targeted these domains. Future research should examine timing effects of treatments that focus on these domains, in order to determine whether timing effects are present for these types of intervention (e.g. physical therapy).
The effect of treatment timing on child outcomes was not influenced by recruitment method, as timing effects were equivalent across the community-screened and clinically referred samples. Evidence from this study, one of the first-large scale RCTs to include community-screened children, addresses an important limitation pointed out by the USPSTF (Siu & USPSTF, 2016). However, future research that more directly tests the relationship between community screening and treatment outcomes is needed.
Overall, the use of RCT methods provides strong experimental evidence for the effects of earlier intensive, individualized treatment. This evidence is also consistent with previous correlational studies showing an effect of age of intervention initiation (Towle et al., 2020). Much of this previous work has shown effects in preschool-aged children, and the present findings suggest that this age effect extends even earlier into the toddler years (see also Itzchak & Zachor, 2011; Rogers et al., 2012; Vivanti et al., 2019). Previous work has been particularly equivocal with regard to specific domains affected by treatment timing, and this is among the first studies to show treatment timing effects across multiple domains of functioning (i.e. receptive and expressive language, social communication, and daily living skills). In addition, many of the studies showing age effects (including this one) have examined relatively high intensity treatments implemented with long durations (e.g. classroom-based interventions, early intensive behavioral intervention). As such, it is not clear that these effects would be observed for lower-intensity or briefer interventions.
Although the focus of this study was the effect of treatment timing on child outcomes, it is also critical to consider the role of parent/caregiver factors, especially for a parent-implemented intervention. Future research should investigate whether earlier intervention may also facilitate an increased capacity for parental learning and/or utilization of learned strategies. In addition to a child’s chronological age, parent factors may also be impacted by proximity to the child’s diagnosis, as some have suggested that this factor affects a family’s decision to enroll in intervention studies (Ingersoll et al., 2017), and once enrolled, this may affect a family’s engagement in intervention. Additional factors that may impact treatment timing effects and deserve additional attention are changes in parental stress, self-efficacy, motivation, and availability to devote time to intervention.
Results from this study underscore the importance of initiating treatment as early as possible, at least by 18 months. However, early intervention is contingent upon early identification of toddlers who require these autism-specific services. Unfortunately, the median age of diagnosis (50 months; Maenner et al., 2021) continues to be well above the age at which children can often be reliably diagnosed (Guthrie et al., 2013; Pierce et al., 2019). This gap coupled with the current findings highlights the need for accurate and efficient identification to facilitate autism-specific intervention by 18 months.
Study limitations and important future directions
A crossover RCT utilizing two active treatments confers both strengths and limitations. However, these limitations point to important next steps for treatment researchers. One benefit of a crossover design with an active control condition is the minimization of attrition, as all children received treatment almost immediately following diagnosis. However, without a no-treatment control group, we were unable to disentangle effects of timing and maturation for the small number of outcomes that showed significant effects for the treatment and active control conditions (i.e. symbolic skills and parent-reported fine motor skills). However, the majority of the significant results were not consistent with maturation effects, as greater gains were observed only in the more intensive treatment and not the active control condition.
Another potential limitation to the crossover component of the design is the possible confound of receiving two different treatments and resulting carryover effects of Condition 1 into progress made during Condition 2. However, the majority of significant results were not consistent with carryover effects, as greater gains were observed during Condition 1 as compared to Condition 2. Within a crossover design, this particular pattern of results can only be attributed to treatment timing. However, significant timing effects in favor of Condition 2 (i.e. fine motor skills) may be associated with carryover effects given that the greater change in these skills may be the result of carryover from the previous treatment. Given the complexity of interpreting results from crossover designs, future research focused on disentangling these effects would provide even stronger evidence for treatment timing effects.
There are a number of potentially important factors that were beyond the scope of this initial study but will be important for future research to consider. First, we compared only two ages of treatment initiation (18 and 27 months), so it remains unclear whether even earlier intervention would result in timing effects and whether timing effects persist at older ages. The first will be important as diagnostic methods allow clinicians to diagnose children at increasingly early ages, and the latter is also important question given the reality of delayed diagnosis and intervention for many children. In addition, future research should examine whether treatment timing effects vary by outcome domain, as there may be more sensitive periods of time for some areas of development compared to others. Future research should also explore the role of individual child, parent, and family characteristics on treatment timing effects to provide additional nuance to evidence behind the notion that earlier is better.
Finally, it is important to acknowledge that children and parents in this sample were predominantly White and the average parent had some college education, making this sample biased in important ways from the general population. Findings from this sample may not generalize to children from other community samples. For example, developmental priorities may differ across cultures, resulting in parents prioritizing some strategies over others when they implement intervention with their child. In addition, families from minoritized backgrounds may have high levels of mistrust of medical and research communities due to historical mistreatment, and therefore may prefer (and specifically benefit from) group-based interventions, which include greater contact with other families. It is critical for future research to include more racially, ethnically, and socio-demographically diverse samples, so these (and other) possible effects on response to treatment can be explored.
Conclusions
This RCT tested whether a relatively intensive and individualized parent-implemented intervention led to greater gains during the earlier treatment condition compared to the same treatment condition initiated 9 months later. Results support beginning treatment by 18 months and suggest that even a narrow window of 18 versus 27 months may impact outcomes in language, social, and daily living skills. Additional research is needed to determine whether initiating treatment younger than 18 months may be even more effective, and whether the specific effect of timing differs across individual children and outcome domains.
Supplemental Material
sj-doc-1-aut-10.1177_13623613231159153 – Supplemental material for The earlier the better: An RCT of treatment timing effects for toddlers on the autism spectrum
Supplemental material, sj-doc-1-aut-10.1177_13623613231159153 for The earlier the better: An RCT of treatment timing effects for toddlers on the autism spectrum by Whitney Guthrie, Amy M Wetherby, Juliann Woods, Christopher Schatschneider, Renee D Holland, Lindee Morgan and Catherine E Lord in Autism
Footnotes
Acknowledgements
We would like to thank the families that participated in this research. We would also like to thank the assessment clinicians, interventionists, and administrative team.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Amy M. Wetherby is author of the Communication and Symbolic Behavior Scales and the SCERTS Model and receives royalties but not from this study. Catherine Lord is author of the Autism Diagnostic Observation Schedule– Second Edition (ADOS-2). Catherine Lord and Whitney Guthrie are authors of the ADOS Toddler Module (ADOS-T). They receive royalties from use of the ADOS-2/ADOS-T, but not from this study. Amy M. Wetherby and Juliann Woods own Autism Navigator, LLC, which distributes Autism Navigator web-based courses and tools. The company is set up so that 100% of all profits are donated to a nonprofit organization. The remaining authors have no financial relationships relevant to this article to disclose.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Research for this article was supported by the National Institute of Mental Health under Awards R01MH077730 and R01MH078165 (Amy M. Wetherby, Catherine Lord) and the Eunice Kennedy Shriver National Institute of Child Health and Human Development under Award R01HD093055 (Amy M. Wetherby). This research was also supported in part by the funding from Autism Speaks (Grant 1791 awarded to Amy M. Wetherby and Catherine Lord; Grant 8551/Dennis Weatherstone Predoctoral Fellowship awarded to Whitney Guthrie) and the Simons Foundation (Catherine Lord).
Ethical approval
FSU and UM Institutional Review Boards approved this study and parents gave written informed consent for participation.
Trial registration
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.