
Abstract
Autistic children and adolescents are more likely than non-autistic youth to experience mental health problems, such as anxiety or depression, but less likely to receive psychotherapy to address these concerns. Recent research indicates that clinician factors, such as knowledge, attitudes, confidence and beliefs, can impact their decisions to provide care, though this work has primarily focused on adults or within the context of one kind of treatment (cognitive behaviour therapy). The current study examined psychological predictors (e.g. attitudes and confidence) of clinicians’ intention to deliver psychotherapy to autistic youth and those with attention-deficit hyperactivity disorder. Participants included 611 clinicians across publicly funded agencies in Ontario, Canada. Multiple mediation analyses revealed that clinician knowledge on mental health-related topics (e.g. core symptoms, developing treatment plans and identifying progress towards treatment goals) was associated with intention to treat autistic clients or clients with attention-deficit hyperactivity disorder, and normative pressures and attitudes partially mediated this association. Clinicians felt less likely to treat autistic clients than clients with attention-deficit hyperactivity disorder, partly because of differences in attitudes, normative pressures and knowledge. This research suggests that targeted training around autism and mental health care may be a useful initiative for agency staff.
Lay abstract
Autistic children and youth often experience mental health problems, such as anxiety, depression and behavioural challenges. Although there are therapy programmes that have been found helpful in reducing these issues, such as cognitive behaviour therapy, autistic children often struggle to receive adequate mental health care. Clinicians’ knowledge, attitudes, confidence and beliefs about treating mental health problems in autistic people may be related to their choices in providing psychotherapy. Across Ontario, Canada, 611 mental health clinicians, working in publicly funded agencies, completed an online survey about their experiences and opinions on delivering therapy for autistic clients compared to those with attention-deficit hyperactivity disorder. Clinician knowledge was associated with their intention to treat autistic clients or clients with attention-deficit hyperactivity disorder, partly because of their attitudes and the social pressures or values they felt. Clinicians reported feeling less intent on providing therapy to autistic youth compared to youth with attention-deficit hyperactivity disorder because of differences in their attitudes, social pressures and knowledge. This research can inform the training and educational initiatives for mental health practitioners.
Background
Autistic 1 children and adolescents often experience co-occurring mental health problems, such as anxiety, depression and conduct issues (Arim et al., 2015; Rydzewska et al., 2019; Strang et al., 2012). For example, a recent meta-analysis has indicated that compared to the general population, autistic people were significantly more likely to have attention-deficit hyperactivity disorder (ADHD, 28%), anxiety disorders (20%), depressive disorders (11%), bipolar and related disorders (5%), schizophrenia spectrum and psychotic disorders (4%) and obsessive compulsive and related disorders (9%) (Lai et al., 2019). Similarly, Totsika et al. (2011) found that the prevalence of parent-reported emotional and behavioural problems among autistic youth (with or without intellectual disability) was three to four times greater compared to the general population and youth with an intellectual disability only. There is a clear need for access to effective mental health care for autistic children and adolescents to address these emotional and behavioural challenges.
Psychotherapy is a common approach to addressing multiple kinds of mental health problems among children and adolescents (e.g. phobias, anxiety, depression and oppositionality) and has produced significant positive treatment effects (Kazdin et al., 1990; Weisz et al., 1995). Psychotherapies that are effective for youth in general can also target mental health problems in autistic youth. A variety of psychotherapeutic interventions have been found to be efficacious in reducing mental health problems in autistic individuals, including cognitive behaviour therapy (CBT) to improve anxiety or depression (Spain et al., 2015; Weiss et al., 2018; Weston et al., 2016), mindfulness-based therapy programmes to reduce aggression and anxiety (Cachia et al., 2016), acceptance and commitment therapy for minimizing distress and hyperactivity (Pahnke et al., 2014), exposure and response prevention therapy to treat obsessive-compulsive behaviours (Kose et al., 2018), and parent-training programmes to target child disruptive behaviours (Kasperzack et al., 2020; Postorino et al., 2017). Despite this evidence that many of the same kinds of interventions are effective, autistic youth often struggle to access evidence-based psychosocial interventions to treat these mental health difficulties (Adams & Young, 2020; Brookman-Frazee, Baker-Ericzén, et al., 2012; Vohra et al., 2014; Zablotsky et al., 2015).
Some studies suggest that autistic children and adolescents have trouble accessing quality mental health services because of long waitlists (Ning et al., 2019), inadequate insurance coverage (Vohra et al., 2014), not knowing where to access support (Vogan et al., 2017), limited workforce capacity or a disconnect between mental health and developmental disabilities systems (Maddox et al., 2021). Studying factors related to service providers, such as their intention to provide treatment, is an essential area to explore when investigating potential barriers to access to care, including psychotherapy. A clinician’s intention or motivation to provide treatment has been found to predict the implementation of evidence-based practices, such as for clinicians treating non-autistic children with mental health problems (e.g. CBT, exposure/systematic desensitization) (N. Williams, 2016), and teacher behaviour working with autistic children (e.g. pivotal response training, positive reinforcement) (Fishman et al., 2018, 2020).
The Theory of Planned Behavior (Ajzen, 1991) has been used as a framework to assess a person’s intention to engage in a specific behaviour and suggests that a person’s intention or motivation is a dominant predictor of behaviour under the appropriate conditions (Ajzen, 1991). This framework posits that the more favourable attitudes, more significant normative pressures felt from others, and greater self-efficacy or confidence towards a specific behaviour, the more likely the person is to engage in that behaviour (Ajzen, 1991). The theory has been used to understand therapists’ intention to provide CBT to autistic adults (Maddox et al., 2019). In Maddox et al. (2019), clinicians reported weaker intentions, less favourable attitudes and normative pressures, and lower self-efficacy in reference to starting CBT with autistic adults who have depression or anxiety disorders, compared to non-autistic adults who have depression or anxiety disorders. Clinician attitude, defined as the perceived advantages or disadvantages of starting CBT, was found to be a positive predictor of intention to deliver CBT. To our knowledge, no other studies have examined the psychological predictors (attitudes, normative pressures and confidence) of intention to provide psychotherapy to autistic people, including none for autistic children.
Clinician knowledge may also be a key consideration to influence a clinician’s intention to treat, as some research suggests that this factor may alter attitudes, normative pressures and confidence. Greater autism knowledge has been associated with more self-perceived confidence towards the treatment of autistic clients among psychiatrists (Crane et al., 2019; M. E. Williams & Haranin, 2016) and more positive attitudes towards working with autistic people among the public (Shand et al., 2020). Similarly, autism training, as a proxy for knowledge, has been linked to community providers’ experiences of normative pressures (e.g. social pressures from others) to deliver interventions for social communication development for autistic children in the United States (Ingersoll et al., 2018). In considering non-autistic clients, a recent meta-analysis found that clinician training on exposure therapy was associated with higher clinician knowledge of exposure therapy, more favourable attitudes towards using exposure therapy and confidence in delivering exposure-based interventions (Trivasse et al., 2020).
The existing work on psychological predictors of therapist intention towards treatment has often been looked at within the context of only one type of intervention (CBT), with less exploration of other forms of therapy, for example, dialectical behaviour therapy (DBT), solution-focused therapy, family therapy or psychotherapy more broadly. In clinical practice, service providers may treat clients using a variety of psychotherapeutic interventions; thus, it may be crucial to examine therapist intention across therapeutic modalities. In addition, it may be possible for clinicians in community-based settings to have limited training in evidence-based interventions, impacting their level of motivation or comfort to start treatment for specialized populations (Frank et al., 2020). Although clinician intention has been compared with autistic or non-autistic clients, few studies have reported on therapist experiences about delivering psychotherapy to children with a comparison chronic neurodevelopmental condition, such as attention-deficit hyperactivity disorder (ADHD). ADHD and autism are the two most common neurodevelopmental disabilities identified in childhood (Doernberg & Hollander, 2016), and researchers often use both in comparative studies examining child mental health care (Craig et al., 2015; Joshi et al., 2017). Comparing therapist ratings relating to clients with ADHD, not just non-autistic clients, can help delineate whether any therapist-reported differences are related to autism specifically or neurodevelopmental disability, more broadly. This is important to inform whether initiatives to support clinician-reported differences should be autism-specific or more about neurodevelopmental considerations, generally.
Current study
The current study aimed to understand the barriers in accessing mental health services in publicly funded agencies across Ontario, Canada, for autistic children and adolescents, by examining factors that influence clinicians’ intention to provide psychotherapy (i.e. attitudes, normative pressures, confidence and knowledge). Clinicians were asked to complete an online survey on their experiences related to delivering psychotherapy for autistic child and adolescent clients or clients with ADHD. The following research questions and hypotheses were addressed as follows:
Are there differences in clinician-reported intention to provide psychotherapy to autistic clients, and in the variables that may underlie this intention, compared to those with ADHD? It was hypothesized that clinicians would report weaker intentions, less favourable attitudes, less normative pressures, lower confidence and less knowledge about delivering psychotherapy to autistic children and adolescents with mental health problems compared to children and adolescents with ADHD.
Is clinician-reported knowledge associated with intention to treat autistic clients and those with ADHD, and are differences in intention mediated by the Theory of Planned Behaviour factors (i.e. attitudes, normative pressure and confidence)? It was expected that less knowledge would be associated with lower reports of confidence, attitudes and normative pressures, which in turn would be related to less intention.
Are differences in clinician-reported knowledge about mental health in autistic clients compared to clients with ADHD associated with differences in clinician intention, and are these differences mediated by differences in the Theory of Planned Behaviour factors? It was hypothesized that different rates of knowledge would be associated with different rates of intention, which would be mediated by clinician differences in psychological predictors of intention.
Methods
Participants
Mental health agency leads provided an estimate on the number of potential respondents that would be expected at each agency. Participants included 611 mental health care service providers, representing 35% of estimated available agency clinicians, in which 83% were women, between the ages of 20 and 75 years (M = 40.2 years, SD = 10.85). The majority of survey participants identified as White (79%), reported current employment status as full-time (92%) and had a post-secondary education (93%), such as a bachelor’s degree (32%) or a master’s degree (37%). Approximately 60% of participants had at least 10 years of clinical practice in the field.
To be included in this study, participants needed to have provided psychotherapy to children and adolescents at 1 of 66 publicly funded participating agencies. Participants included direct service providers (80%), supervisors/coordinators (11%) and some who noted being both direct service providers and supervisors/coordinators (8%). The surveys were completed by social workers (46%), child and youth workers (21%), registered psychotherapists (19%), clinical psychologists (5%) and those with other professional designations (9%).
All survey respondents reported treating mental health problems in children or adolescents in some capacity. Participants indicated that their primary theoretical orientation when treating clients was cognitive behavioural (42%), eclectic (35%), behavioural (12%) or other (11%; e.g. dynamic/analytic, integrative, collaborative problem-solving, attachment-based therapy). On average, participants reported having approximately 14 clients with mental health problems (SD = 11.1, Median = 12.0) on their current caseload. The majority of the sample reported treating at least one autistic client (90%) and one client with ADHD (98%) in the past. In fact, on average, respondents indicated 19% (SD = 19.5%, Median = 15%) of their caseload involved autistic clients and 47% (SD = 24.9%, Median = 50%) involved clients with ADHD. Furthermore, many respondents noted knowing an autistic person (60%) and someone with ADHD (88%) outside their work. However, the majority reported that the frequency of contact with autistic individuals (85%) was very rare or occasional, and nearly half of the respondents indicated the frequency of contact with individuals with ADHD (48%) was very rare or occasional.
Measures
Clinician attitudes
Clinicians’ attitudes were defined as the perceived advantages or disadvantages of delivering psychotherapy to treat mental health problems in autistic clients or clients with ADHD (Maddox et al., 2019).
2
Respondents’ attitudes were assessed using standard semantic differential scales (Fishbein & Ajzen, 2010) used in previous research by Maddox et al. (2019) on therapists’ attitudes towards starting CBT for autistic adults. Survey respondents reported how favourably or unfavourably they felt towards providing psychotherapy to autistic clients or clients with ADHD using opposite adjective pairs and a 10-point slider scale (10 to 0). The adjective pairs comprised good–bad, effective–useless, pleasant–unpleasant, hopeful–hopeless and manageable–burdensome. For instance, clinician attitudes were measured by asking participants the following statement:
Think about child/adolescent clients with mental health problems who present with [autism or ADHD]. If you were to provide psychotherapy with these clients, that would be . . . [e.g., manageable or burdensome]? For each pair of words below, select a number from 10–0 that reflects your opinion.
A total mean score of the clinician attitudes was computed by averaging across all five items, with higher scores indicating more favourable attitudes. The internal consistency for this scale in this study was excellent for all questions about autistic clients and clients with ADHD (α = 0.93 and 0.94, respectively).
Clinician normative pressures
Normative pressures, the social pressure felt from others, were defined in two ways: (1) the clinicians’ perceptions about what other people like them are doing (descriptive norms), and (2) the clinicians’ perceptions about expectations that other people important to them hold (injunctive norms) (Ajzen, 1991). Descriptive norms were measured by asking participants to identify the extent to which they agreed with the following statement: ‘Most clinicians like me, in my professional situation, would provide psychotherapy to these clients [clients with mental health problems who present with autism or ADHD]’, using a 5-point Likert-type scale (1 = strongly disagree; 5 = strongly agree). Injunctive norms were measured by asking participants to indicate their responses using a 5-point Likert-type scale (1 = strongly disapprove; 5 = strongly approve) for two items: ‘[Continue to think about providing psychotherapy to clients with mental health problems who present with autism or ADHD], how much would [other clinicians or your supervisor/manager] disapprove or approve if they knew you were providing psychotherapy to these clients’. The average score between the descriptive and injunctive items computed a total norm score. Higher total norm scores represented greater normative pressures felt by clinicians. This scale had adequate internal consistency across all three items for autistic clients (α = 0.77) and good internal consistency for clients with ADHD (α = 0.87).
Clinician confidence in delivering psychotherapy
Self-efficacy, or confidence, refers to a person’s sense of agency towards a specific behaviour (Ajzen, 1991). Survey respondents completed an adapted version of the Therapist Confidence Scale for Intellectual Disabilities (TCS-ID; Dagnan et al., 2015). The adaptations of the TCS-ASD (Cooper et al., 2018) included substituting the condition ‘learning disability’ to ‘autism/ADHD’ and including a statement at the beginning of the measure asking clinicians to rate their confidence in delivering treatment within the context of mental health care.
The adapted TCS-ASD (Cooper et al., 2018) assessed confidence across several therapeutic domains (e.g. assessment, building rapport, delivering interventions and ending therapy) with references to autistic clients or clients with ADHD. Respondents used a 5-point Likert-type scale (1 = not confident; 5 = highly confident). A mean score was calculated, with higher scores reflecting greater overall confidence. This 14-item measure exhibited excellent internal consistency in previous research (α = 0.92) (Cooper et al., 2018) and in our current study for all questions about autistic clients and clients with ADHD (α = 0.95 and 0.96, respectively). For example, respondents were asked,
Within the context of mental health care, how confident are you that you can . . . [e.g., develop a therapeutic relationship with a client with autism/ADHD, communicate with a client with autism/ADHD, explain results of an assessment process to a client with autism/ADHD]?
Clinician intention
Participants reported their level of intention, or motivation, in providing psychotherapy by answering a single-item question: ‘If it were up to you, how likely is it that you would provide psychotherapy to clients with mental health problems who present with [autism or ADHD]?’ Clinicians provided their responses using a 7-point Likert-type scale (1 = extremely unlikely; 7 = extremely likely). A mean score was calculated with higher ratings reflective of greater clinician intention to treat (Maddox et al., 2019).
Clinician knowledge on mental health topics for clients with autism/ADHD
A self-rated knowledge measure developed by Brookman-Frazee, Drahota, et al. (2012) and later adapted by Maddox et al. (2019) was used in this study. This 6-item tool captured how knowledgeable clinicians feel towards mental health-related topics for child and adolescent autistic clients or clients ADHD, using a 5-point Likert-type scale (1 = not at all knowledgeable; 5 = extremely knowledgeable). The items included core symptoms, co-occurring problems, the impact of autism or ADHD characteristics on behaviour, developing a treatment plan, delivering treatment and identifying progress towards treatment goals. An average score was calculated with higher scores reflecting greater self-reported knowledge for topics related to mental health issues in autistic clients or clients with ADHD. The measure showed excellent internal consistency across all items for autistic clients and those with ADHD (α = 0.95 and 0.96, respectively). For instance, respondents were asked: ‘Please rate how knowledgeable you feel about the following topics related to a child/adolescent client with mental health problems who present with [autism or ADHD] . . . [e.g. core symptoms of autism/ADHD, developing a treatment plan for a client with autism/ADHD]’.
Procedures
This survey was approved by the University’s Ethics Review Board (#e2020-253). The study collected information in a cross-sectional online survey. Survey questions about autism and ADHD were counterbalanced across participants, meaning that some respondents were first asked about these variables in relation to ADHD, while others were first asked about autism. Publicly funded mental health agency staff were asked by their clinical or administrative leads to share an anonymous survey link with all frontline staff who provide psychotherapy to children and adolescents with mental health problems. The survey was advertised as a project to help build capacity within the mental health and autism sectors and to identify providers’ targeted training needs. All eligible mental health clinicians were encouraged to participate regardless of whether they had previously or were currently serving autistic clients or clients with ADHD. This study was completed through convenience sampling, where clinical leads of interested agencies shared the survey with their mental health staff, who were then given the opportunity to participate. All participants provided informed consent before completing the survey. English and French versions of the survey were available. Clinicians did not receive compensation for participation in this research project.
Data collection for this project occurred at four time points. First, it was collected in December 2019 from eight core service providers in the Ottawa area affiliated with the Youth Services Bureau of Ottawa Lead Agency, where approximately 100 clinicians were estimated to be able to complete the survey. Second, it was collected in June–July 2020 from Woodview Mental Health and Autism Services (Hamilton, Brant and Halton regions of Ontario), with 65 potential clinicians. Third, it was collected in August–September 2020 from Kinark Child and Family Services (across the Durham, Halton, Northumberland, Peel, Peterborough, Simcoe and York regions of Ontario), with up to 388 potential clinicians. In partnership with Children’s Mental Health Ontario (CMHO), a webinar for publicly funded agencies was held in November 2020 about the survey to help build broader agency interest and provide information on how agency leads could involve their organization in this project. CMHO collected expressions of interest to identify the number of mental health agencies interested in participating. Finally, data were collected in April–May 2021 from member agencies across the province (excluding those who already completed the survey noted above). Ultimately, 66 agencies had some mental health providers who completed the survey, with approximately 1762 clinicians available to participate. Each agency decided on its own process for informing staff about the survey. In total, 627 clinicians completed the survey, but 16 were excluded for not meeting the criteria of providing psychotherapy to children and adolescents (e.g. administrative staff). Among those clinicians who started the survey, approximately 65% completed it entirely.
Community involvement
Autism agency leads, community mental health providers and researchers were involved in developing the research questions, study design, measures, implementation and dissemination of findings of this study. It was originally produced by researchers in consultation with Monica Armstrong, the Director of Mental Health Services for the Youth Services Bureau, and Cathy Lonergan, the Children and Youth Mental Health Lead Agency System Planner for the Youth Services Bureau who provided direction on the focus, language, length and design. There were no autistic people involved in the survey development or distribution. The survey was then shared and reviewed by three agency leads in child and adolescent mental health care settings. Prior to its distribution by CMHO, it was also shared with a Pan-agency Autism Working Group coordinated by CMHO, who reviewed and approved the survey before distribution across the province. Input on analysis and interpretation also occurred in consultation with these service providers.
Analysis plan
All analyses were performed using IBM SPSS version 26. No major violations in skewness and kurtosis were noted on visual inspection of histograms and normal Q-Q plots, and correlation and regression assumptions, including linearity, normality and homoscedasticity, were satisfied. Descriptive and correlational data were calculated to examine the associations between all variables of interest.
The first objective involved paired samples t-tests and Wilcoxon signed-rank tests to examine whether clinician factors were significantly lower for autistic mental health clients, in contrast with clients with ADHD, with Cohen’s d as a measure of effect size. The second and third objectives involved testing the possibility of multiple mediators using the PROCESS macro, embedded in SPSS (Hayes, 2012). Pearson’s product–moment correlation and Preacher and Hayes’s (2008) bootstrapping procedure (1000 samples) were used to analyse the data (Farmer, 2012; Preacher & Hayes, 2008). Mediations were significant if the intervals between the lower and upper limit of a 95% confidence interval (CI) did not contain zero (Preacher & Hayes, 2008). Clinician age was entered as a covariate across all mediation analyses. Two multiple mediation analyses were then calculated examining the knowledge–intention relationship regarding autism (Model 1) and ADHD (Model 2). The final multiple mediation analysis (Model 3) was calculated to investigate the relationship between differences in knowledge and intention for autistic clients compared to those with ADHD. R-squared was calculated as a measure of effect size for regression models in mediation analyses. Partial eta squared was calculated as a measure of effect size for significant independent variables.
Results
Objective 1: differences in clinician intention, attitudes, normative pressures, confidence and knowledge
As shown in Table 1, clinicians reported lower levels of intention to provide psychotherapy to autistic children and adolescents compared to clients with ADHD (with a small effect size, Cohen’s d = −0.36). Clinicians had less favourable attitudes (with a medium effect size, Cohen’s d = 0.70) and normative pressures (e.g. beliefs about attitudes that others hold, beliefs about what others like them do) (with a large effect size, Cohen’s d = 0.85) about delivering psychotherapy to autistic clients, compared to clients with ADHD. Clinicians also reported feeling significantly less confident and less knowledgeable about providing psychotherapy to autistic children and adolescents compared to youth with ADHD, with large effect sizes (Cohen’s d = 0.90 and 0.88, respectively).
Descriptive statistics for clinician attitudes, confidence, normative pressures, knowledge, and intention for autistic clients compared to clients with ADHD (n = 611).
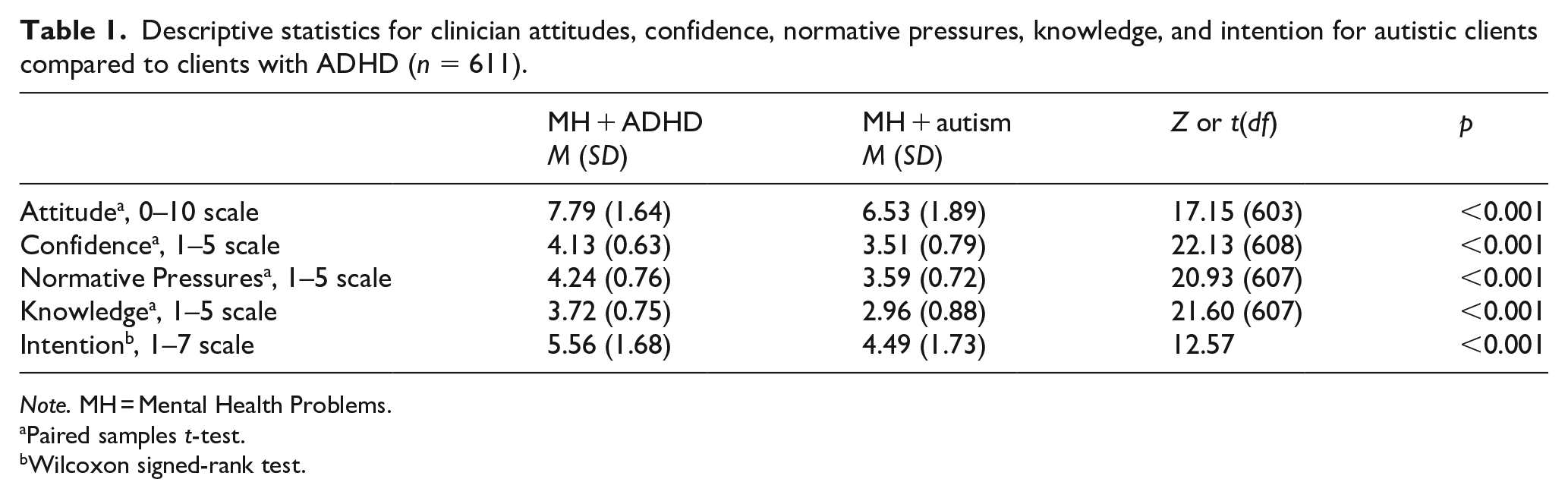
Note. MH = Mental Health Problems.
Paired samples t-test.
Wilcoxon signed-rank test.
As indicated in Table 2, most of the predictor variables were correlated with small to moderate size, and similar patterns of relations emerged with reference to autism and to ADHD. Knowledge and confidence had a strong positive correlation; however, standard regression collinearity (variance inflation factor (VIF) estimates) and multicollinearity diagnostics (condition index/variance proportions) revealed no evidence of collinearity. Furthermore, there was a significant positive association between clinician age and knowledge regarding clients with ADHD.
Correlations among independent variables, mediators, covariate and outcome variable for autistic clients and clients with ADHD.
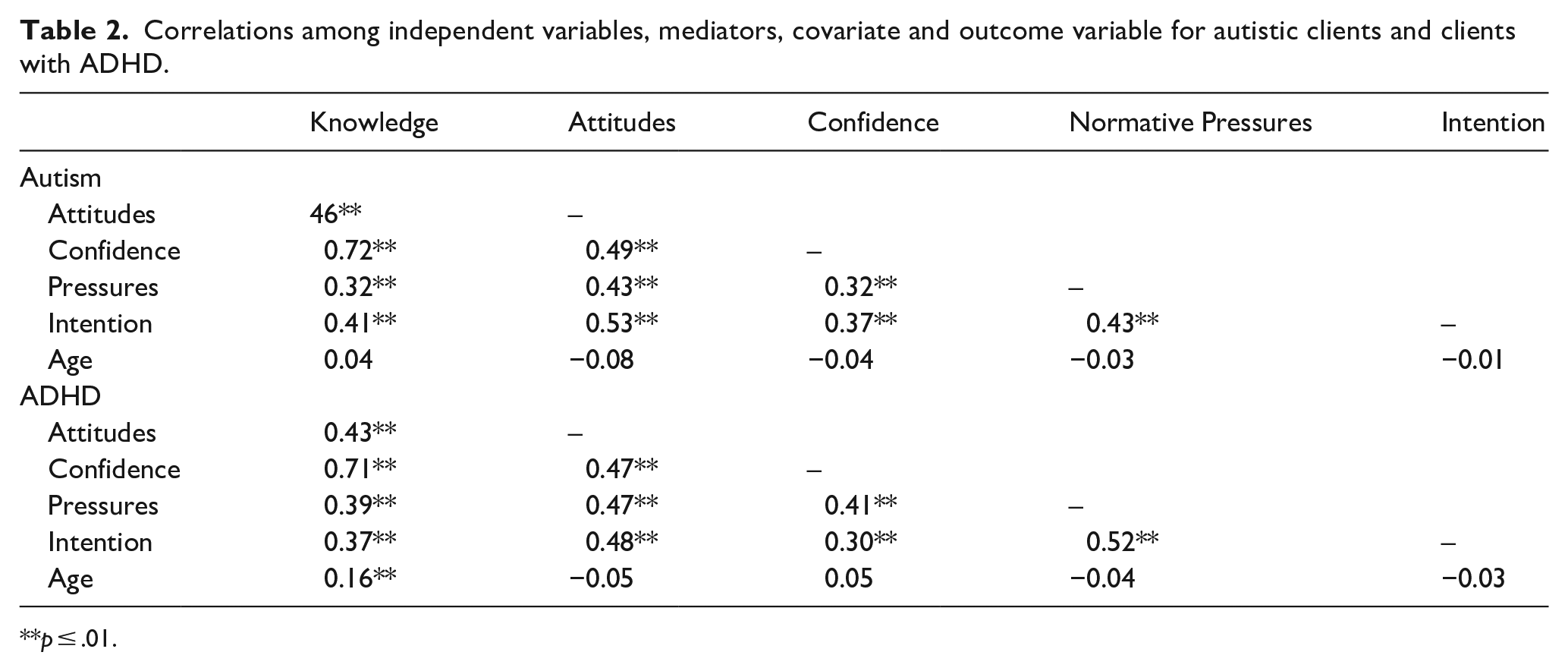
p ≤ .01.
Objective 2: mediators of the knowledge–intention relationship for autistic clients (Model 1) and clients with ADHD (Model 2)
As shown in Figures 1 and 2 (path c), the total direct effect of clinician knowledge was a predictor of intention to treat for autistic clients and clients with ADHD, prior to entering the mediator variables (tautism = 10.16, p < 0.001, 95% CI [0.61, 0.91]; tADHD = 7.47, p < 0.001, 95% CI [0.49, 0.84]), accounting for 16% and 9% of the variance, respectively. With the inclusion of the potential mediators, the overall Model 1 (Autism) and Model 2 (ADHD) accounted for 35% and 28% of the variance in intention, F(5, 556) = 60.23, p < 0.001 and F(5, 560) = 42.51, p < 0.001, respectively. As shown in Figures 1 and 2 (path b), for autistic clients or those with ADHD, attitude (tautism = 8.45, p < 0.001, η p 2 = 0.11; tADHD = 5.82, p < 0.001, η p 2 = 0.06), normative pressures (tautism = 5.74, p < 0.001, η p 2 = 0.06; tADHD = 7.14, p < 0.001, η p 2 = 0.08) and knowledge (tautism = 4.01, p < 0.001, η p 2 = 0.03; tADHD = 2.42, p < 0.05, η p 2 = 0.01) were all independent predictors, while clinician confidence (tautism = −0.96, p = 0.34; tADHD = −1.45, p = 0.16) was not. The multiple mediator results in both models indicated significant total indirect effects (point estimate autism = 0.36, 95% CI [0.18, 0.54]; point estimate ADHD = 0.38, 95% CI [0.17, 0.59]), accounted for by the indirect effect of attitude (point estimate autism = 0.30, 95% CI [0.21, 0.42]; point estimate ADHD = 0.26, 95% CI [0.15, 0.38]), and normative pressures (point estimate autism = 0.14, 95% CI [0.07, 0.20]; point estimate ADHD = 0.25, 95% CI [0.15, 0.36]). Having greater knowledge was related to more favourable attitudes and greater feelings of normative pressures (path a) for both clinical groups, which were related to greater clinician intention (path b). The continued significance of the direct association of knowledge and intention in both models suggests a partial mediation.
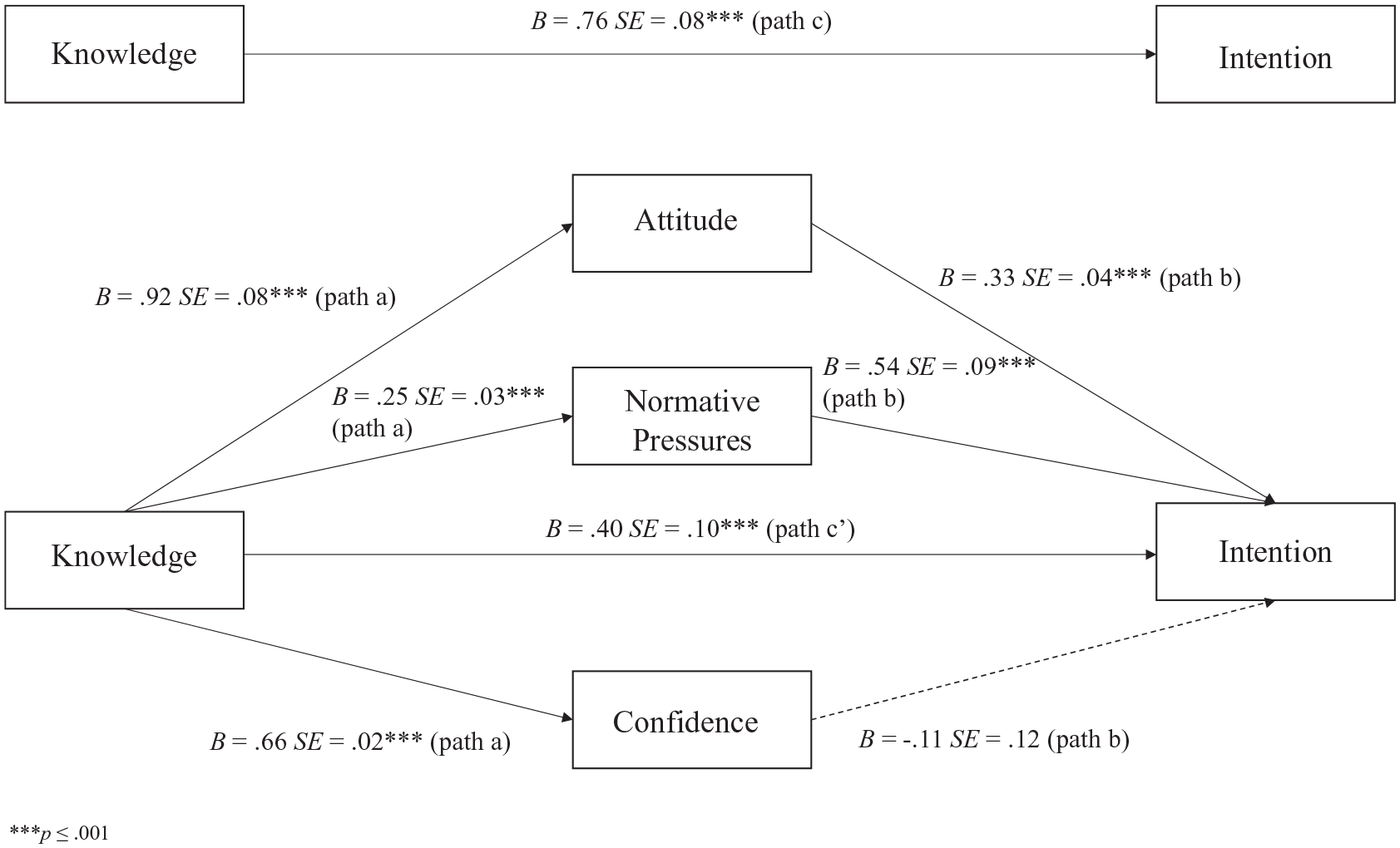
Multiple mediation analysis of attitude, normative pressures and confidence on the knowledge–intention relationship for autistic clients.
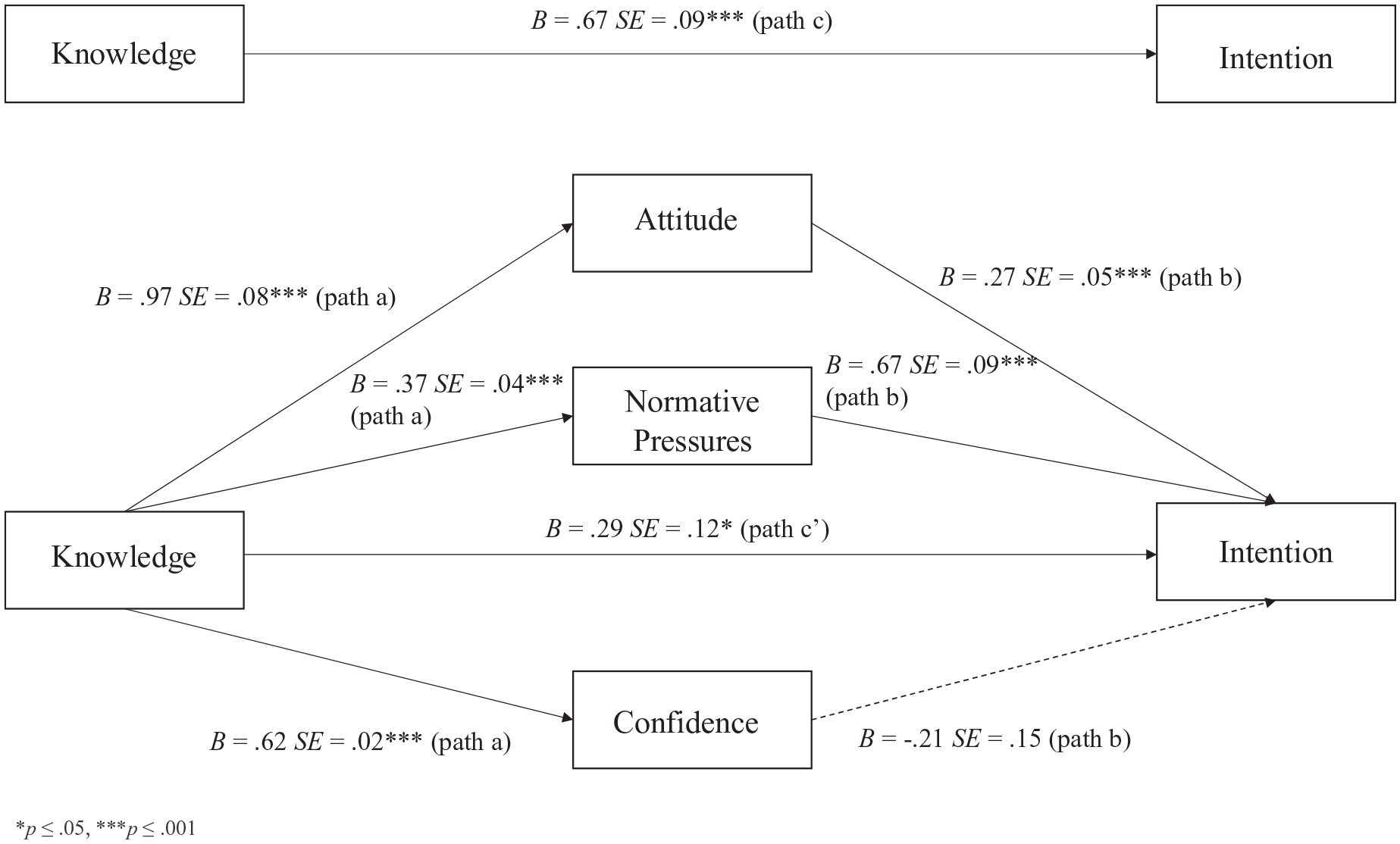
Multiple mediation analysis of attitude, normative pressures and confidence on the knowledge–intention relationship for clients with ADHD.
Objective 3: Model 3 – mediators of the knowledge–intention difference for autistic clients compared to clients with ADHD
Multiple mediation analysis was used to investigate different rates of clinician knowledge and differences in intention. As illustrated in Figure 3 (path c), the total direct effect of knowledge difference was a predictor of intention difference before entering the mediator variables, t = 7.28, p < 0.001, 95% CI [0.48, 0.83], accounting for 9% of the variance. The overall model accounted for approximately 19% of the variance in clinician intention after including the potential mediators, F (5, 555) = 26.00, p < 0.001. As demonstrated in Figure 3 (path b), once all the variables were entered, only differences in attitudes (t = 5.96, p < 0.001, η p 2 = 0.06), normative pressures (t = 3.20, p < 0.01, η p 2 = 0.02) and knowledge (t = 2.40, p < 0.05, η p 2 = 0.01) were independent predictors, while differences in clinician confidence (t = 0.15, p = 0.88) were not. Results indicated a significant total indirect effect for the set of mediators (point estimate = 0.37, 95% CI [0.18, 0.55]), and this mediation was accounted for by the indirect effect of attitude difference (point estimate = 0.23, 95% CI [0.14, 0.34]) and normative pressures difference (point estimate = 0.13, 95% CI [0.03, 0.23]). Differences in the knowledge of autism and ADHD led to the differences in clinician reports of their intention towards treatment, which was due to poorer attitudes and normative pressures. The relationship between knowledge difference and intention difference remained significant after entering the mediators and control variable, suggesting a partial mediation.
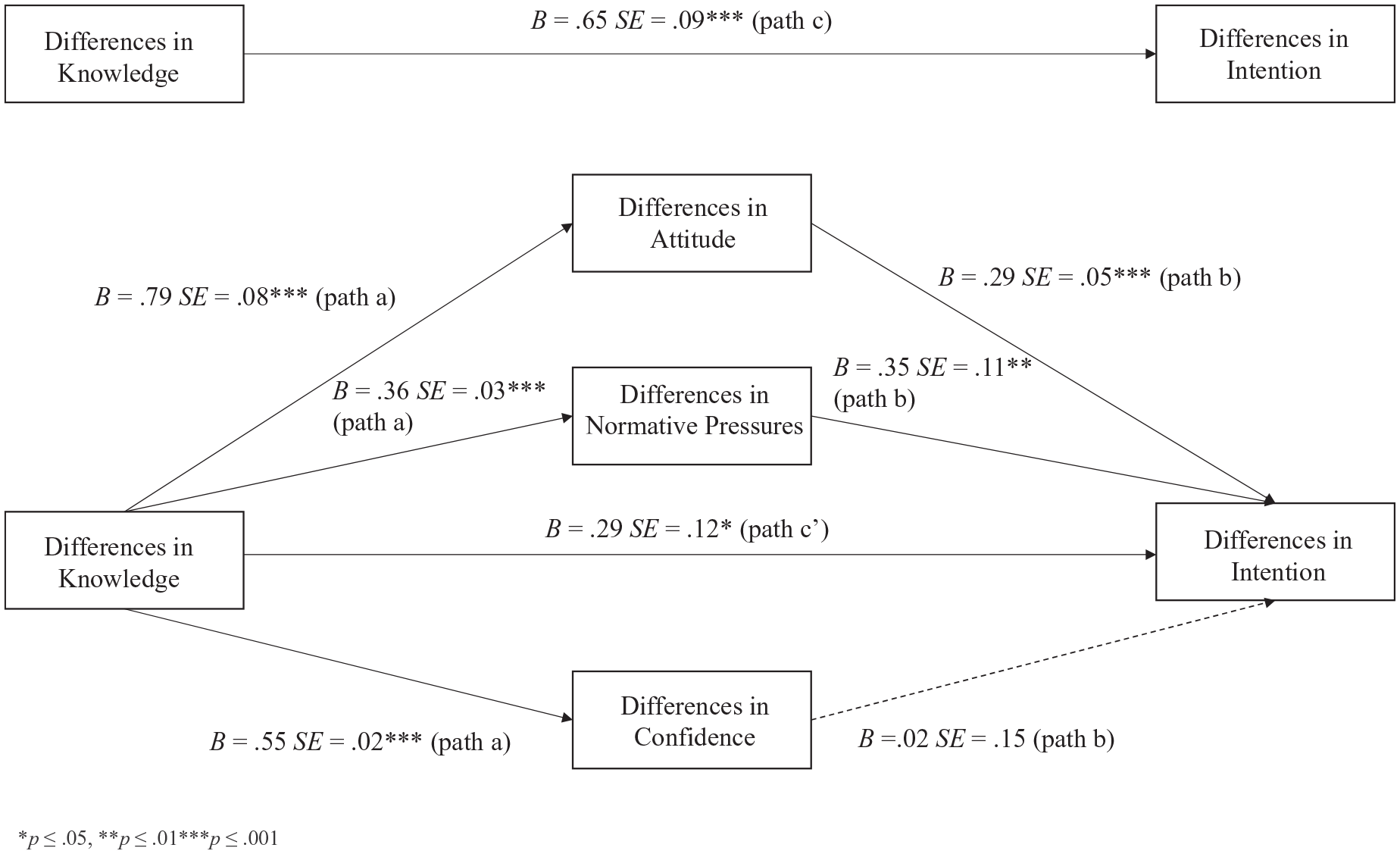
Multiple mediation analysis of differences in attitude, normative pressures and confidence on the knowledge–intention difference for autistic clients compared to those with ADHD.
Discussion
The current study examined clinician psychological predictors of intention towards delivering psychotherapy to autistic youth or youth with ADHD in publicly funded agencies in Ontario. In line with hypotheses, clinicians were less confident, felt less normative pressure, had less knowledge, demonstrated less favourable attitudes and had less intention to provide psychotherapy to autistic clients compared to those with ADHD. Clinicians reported moderate levels of ratings (i.e. feeling moderately knowledgeable or moderately confident) in many respects of their treatment delivery for both clinical groups, although compared to clients with ADHD, autistic clients appeared to be at a disadvantage. These results are not surprising, given past research demonstrating that most therapists do not report strong intentions to start CBT for autistic adult clients with co-occurring anxiety or depression (Maddox et al., 2019). Health care providers often report limited training and knowledge in working effectively with autistic individuals (Adams & Young, 2020; Heidgerken et al., 2005; Maddox et al., 2020; Maddox & Gaus, 2019; Zerbo et al., 2015), likely contributing to misconceptions or feelings of discomfort in treating this specialized population. Our results suggest that if it were up to them, service providers would be less likely to provide psychotherapy to autistic youth than those with ADHD, which may pose a barrier to mental health service access.
For both groups, clinician attitude and normative pressures were significantly related to their intention in the expected direction and functioned as partial mediators of the relation between knowledge and intention. This is partly consistent with Maddox et al. (2019), who found that clinician attitude, but not normative pressures, was a significant predictor of intention to treat autistic clients. However, that study focused on adult clients, and solely on CBT in the United States, and our children’s mental health focus in Ontario suggests that perceived pressures do matter in the current context.
Our results also suggest that the partial mediation of normative pressures and attitudes is not unique to autism. Increasing clinician knowledge about clients with neurodevelopmental disabilities may improve clinician motivation to provide care for both autistic clients and clients with ADHD (Ingersoll et al., 2018). Furthermore, there may be an overlap in autism and ADHD phenotypes. In the current study, we asked clinicians to consider autism versus ADHD as we were interested in their perspectives based on how they understood these descriptors; however, there may be clients who, of course, have both diagnoses and certainly demonstrate symptoms of both conditions. At the same time, when intake information specifies indicators of autism, the current study suggests that clinicians will be less motivated to provide psychotherapy based on this label alone. Thus, concerted efforts to address these differences are warranted, while also addressing overlapping symptomatology. Our findings linking the Theory of Planned Behaviour variables (i.e. attitudes and normative pressures) with intention is consistent with other studies on the intention of health care providers outside of the context of mental health (Kortteisto et al., 2010; Omura et al., 2018). Increasing knowledge, positive attitudes and the expectations clinicians perceive from colleagues or supervisors about delivering effective care may be particularly important for training, as it relates to clinician intention towards treatment for both populations. While we did not explicitly assess clinicians’ actual behaviour of delivering psychotherapy, our results suggest that higher clinician-reported knowledge, more favourable attitudes and social pressures felt from others in the work setting may be associated with greater clinician feelings of motivation to provide treatment. Surprisingly, we did not find that clinician confidence explained the variance in intention to deliver psychotherapy, despite it being correlated with intention. This finding is similar to Maddox et al. (2019), who found that self-efficacy was not a significant predictor of intention when considering autistic or non-autistic clients. We also found that knowledge and confidence were closely related; therefore, a possible explanation for this finding may be that when examining these constructs together, clinician knowledge may account for the variance in intention that may have otherwise been explained by confidence.
Differences in rates of knowledge found between autistic clients and clients with ADHD were associated with differences in intention, and these were again partially mediated by differences in attitudes and normative pressures, but not confidence. These results further test the hypothesis that the differences found in intention to treat different neurodevelopmental groups are linked to the differences found in knowledge, attitudes and normative pressures. Although training was not assessed in this study, it may have important implications in the theory of planned behaviour constructs and for improving knowledge. Training programmes have been linked with improved attitudes (Frank et al., 2020; Jones et al., 2021; Trivasse et al., 2020), normative pressures (Ingersoll et al., 2018) and knowledge (Frank et al., 2020; Gillespie-Lynch et al., 2015) and are an important consideration for future research into autism mental health care capacity building. This finding speaks to the importance of clinician training and educational programmes to address any potential negative beliefs or stigmatizing attitudes towards autistic individuals. For example, Jones et al. (2021) found that compared to a general mental health training module and a no-training control, non-autistic adults receiving a brief autism acceptance training programme reported more positive impressions of autistic individuals, fewer misconceptions and lower stigma about autism, and higher expectations of their functional abilities. Jones et al. (2021) demonstrated how training programmes designed to increase knowledge may be associated with more inclusive and accepting attitudes towards clients with neurodevelopmental conditions, such as autism. Autism training programmes designed with autistic involvement may be best to consider, as they are found to be more effective than non-autistic led training programmes (Gillespie-Lynch et al., 2021) and can provide meaningful perspectives on the types of mental health support best needed for autistic children and youth (Fletcher-Watson et al., 2019). Weaker clinician intention to deliver psychotherapy to autistic clients, even when compared to clients with ADHD, can reduce the number of skilled mental health service providers willing or available to work with autistic youth in need of support, serving as a potential barrier to access to services. It is crucial to shed light on barriers to accessing care for families seeking services to improve the provision of mental health care for those in need. The poor access to quality mental health care is further compounded in more rural or lower-income communities (Adams & Young, 2020; Cantor et al., 2020), highlighting the need for training and resources for wide-reaching publicly funded service provider networks.
Limitations and future directions
There are some limitations of this work. First, while the lead mental health agencies affiliated with CMHO were able to send the survey to all interested publicly funded service providers, there were variable levels of responses across agencies. While our sample represents approximately 35% of potential clinicians, it is possible that this sample does not represent the larger population of service providers who chose not to respond or those who work in private practice settings and are not affiliated with publicly funded agencies. Second, because the background information section appeared at the end of the survey, we could not compare the clinicians who fully completed the survey compared to those who started but did not finish on demographic variables. Third, although we had assessed for primary theoretical orientation, we did not examine the type or degree to which clinicians received evidence-based intervention training in the past. Fourth, clinician intention was measured by a single item, and although many research studies have successfully used this one-item to measure this construct (e.g. Fishman et al., 2018; Ingersoll et al., 2018), it may be useful to examine intention using a general measure with well-established psychometric properties. Fifth, while clinicians reported how likely they would be to provide psychotherapy to autistic clients and clients with ADHD if it were up to them, we did not collect data on their autonomy to select their cases, and it is possible that in reality, some clinicians may not have the opportunity to choose who they work with. At the same time, intention continues to be an important consideration because, based on the Theory of Planned Behaviour (Ajzen, 1991), it is a dominant predictor of behaviour (Fishbein & Ajzen, 2010) and can be used to understand efforts towards changing clinician behaviour and addressing barriers to treatment access (Maddox et al., 2019) and implementing evidence-based treatments (N. Williams, 2016). Finally, the data were cross-sectional and correlational in nature, limiting inferences on causality.
Future projects can expand on this work using similar online tools used in our study to measure training needs and the impact of training delivery for staff. More research is needed to determine how initiatives can improve autism knowledge, and most importantly, address clinician’s intention to treat by targeting normative pressures and attitudes. For instance, a community provider training initiative, the Extension for Community Healthcare Outcomes (Project ECHO; Arora et al., 2010) autism curriculum, was found to be successful in increasing US mental health providers’ self-efficacy, knowledge of autism and problem-solving skills for adapting evidence-based interventions for autistic clients with co-occurring mental health conditions (Dreiling et al., 2021). Programmes such as Project ECHO may be a feasible solution for improving clinicians’ training and the accessibility of mental health community services for families needing support. Longitudinal studies are needed to test whether intention predicts clinicians’ actual delivery of psychotherapy.
Conclusion
Our findings suggest the existence of potential barriers to treatment delivery for autistic child and adolescent clients experiencing mental health problems. Even when compared to other clients with ADHD, who may often present with chronic, pervasive behavioural challenges, autistic clients appear to be at a disadvantage. Overall, clinicians reported feeling less likely to deliver psychotherapy to autistic clients than those with ADHD, such as CBT, DBT and family therapy, partly because of differences in their attitudes and normative pressures, which related to their knowledge. Training initiatives addressing mental health service providers’ knowledge, attitudes and normative pressures towards autism or ADHD may improve their intention to treat and improve access to effective mental health care.
Footnotes
Acknowledgements
The authors thank the clinicians who participated in this research study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the York University Research Chair in Autism and Neurodevelopmental Disability Mental Health, the LaMarsh Centre for Child and Youth Research and by Children’s Mental Health Ontario.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.