
Abstract
Accessing adult autism diagnostic pathways can be difficult. This study explored perspectives of UK autistic adults, relatives and clinicians regarding the characteristics of optimal adult autism assessment and diagnostic services. In stage 1, three key stakeholder groups were surveyed about experiences of adult autism diagnostic services (pre-assessment/assessment): 343 autistic adults, 45 relatives and 35 clinicians completed parallel surveys. Information from stage 1 surveys was used to devise statements for a modified Delphi process in stage 2 seeking consensus among clinicians on optimal diagnostic service characteristics. Data analyses were non-parametric and descriptive. Over half of adults were in contact with mental health services prior to autism diagnosis. Clinicians reported that multidisciplinary diagnostic teams lacked key professionals. Thirteen statements describing optimal autism diagnostic service provision were developed. There was consensus from clinicians on 11 statements relating to clear assessment pathways, updates for people while waiting, pre-assessment information gathering/provision, co-occurring condition identification and training/networking. Some autistic adults, relatives and clinicians were positive about services, all stakeholders identified improvements were needed. The findings describing optimal service provision are relevant for UK clinicians, managers and commissioners to improve diagnostic assessments for autistic adults, and have international relevance for similar health systems.
Lay abstract
Living with undiagnosed autism can be distressing and may affect mental health. A diagnosis of autism can help self-awareness and self-understanding. However, it can be difficult for adults to access an autism assessment. Clinicians also sometimes find it hard to identify autism in adults. This may mean an autism diagnosis is delayed or missed. In this study, we asked autistic adults, relatives and clinicians how to improve this. The study was in two stages. In the first stage (stage 1), 343 autistic adults and 45 relatives completed a survey. In the survey, we asked questions about people’s experiences of UK autism assessment services for adults. Thirty-five clinicians completed a similar survey. Clinicians reported that some autism assessment teams lacked key professionals, for example, psychologists and occupational therapists. We used the information from the three separate surveys to create 13 statements describing best autism assessment services for adults. In stage 2, we asked clinicians for their views on the 13 statements. Clinicians agreed with 11 of the statements. Some autistic adults, relatives and clinicians were positive about autism assessment services, and many also described areas that could be improved. The study findings can be used to improve UK adult autism assessment services and may be helpful for service developments worldwide.
Introduction
Receiving an autism diagnosis can facilitate self-awareness/understanding and access to services and community support (Leedham et al., 2020; Powell & Acker, 2016; Stagg & Belcher, 2019). For some, it might also facilitate appropriately adapted support for co-occurring physical and mental health conditions (Hand et al., 2020; Lever & Geurts, 2016; Mason et al., 2021; Matson & Cervantes, 2014; Zerbo et al., 2019). Recognition and diagnosis of autism in adults can be challenging for professionals in primary and secondary care and other settings, especially in the presence of intellectual disability and/or co-occurring mental health conditions (Fusar-Poli et al., 2020; Luciano et al., 2014; Wigham et al., 2019, 2020). This may mean an autism diagnosis is delayed or missed (Au-Yeung et al., 2019; Fusar-Poli et al., 2020; Takara & Kondo, 2014). Living with undiagnosed autism can be distressing, have an impact on mental health and affect functioning in life-roles, for example, work/occupation and relationships (Stagg & Belcher, 2019; Zener, 2019).
In an international survey of 665 adults, 48% described how difficulties navigating local health systems, acted as a barrier to accessing an autism spectrum disorder (ASD) diagnosis (Lewis, 2017). Adults in the Netherlands and Australia (including those already known to social and mental health care providers), reported negotiating heterogeneous and confusing routes to diagnosis (Geurts & Jansen, 2012; Huang et al., 2021). Long waiting lists are a further challenge for service users trying to access adult autism assessment and diagnosis pathways and for service providers (Rutherford, McKenzie, Forsyth, et al., 2016; Rutherford et al., 2018). Any and all of these factors can affect quality, experience of and satisfaction with autism assessment and diagnosis provision for service users and clinicians.
In recent UK surveys, dissatisfaction with the assessment and diagnosis process was expressed by 40% of adults and 22% of professionals. Delays in accessing the clinical diagnostic pathway and lack of information received during the autism assessment/diagnostic process were identified as key factors (Jones et al., 2014; Rogers et al., 2016). A lack of training about autism, recognition of the presentation of autism in women and a lack of standardised assessments have also been identified as barriers to satisfactory pathway access and diagnostic assessment (Bargiela et al., 2016; Crane et al., 2018; Huang et al., 2021; Zener, 2019). Clear autism assessment/diagnosis pathways and fewer professional contacts were associated with client satisfaction in New Zealand (Evans et al., 2021).
A framework for reducing waiting lists in Scotland informed by implementation science including mechanisms for integrating solutions into practice and supporting staff to implement change, for example, via peer forums, has demonstrated some success. (Rutherford et al., 2018). In a separate evaluation of 18 UK Specialist Autism Teams, practitioners reported concerns about managing increasing numbers of referrals and upskilling others without equivalent expansion of resources, while providing consultation for mainstream services. The study identified that multi-disciplinary team (MDT) skill mix, and psychoeducation were key to optimal service user outcomes (Beresford et al., 2020).
Clinical guidelines for autism assessment and diagnosis
Adult autism assessment guidelines have been published in Australia, New Zealand and some European countries. However, variations in recommendations and some mismatch between best-practice guidance and what is experienced in adult autism assessment pathways has been identified (Hayes et al., 2018; Scattoni et al., 2021). In the United Kingdom, the National Institute for Health and Care Excellence (National Institute for Health and Care Excellence [NICE], 2012) has published clinical guidelines (CGs) and quality standards for assessment and diagnosis of autism in adults (Table S1; NICE, 2014). Guidelines for Scotland are informed by NICE guidance with MDT assessment recommended as the optimal approach (Scottish Intercollegiate Guidelines Network (SIGN), 2016). Australian national guidelines recommend a strength-focussed, holistic, neurodevelopmental approach to assessment and diagnosis considering adaptive functioning in life roles/contexts. Assessment comprises a comprehensive needs assessment (functioning/medical needs), if required progressing to a single practitioner diagnostic evaluation, in the absence of diagnostic confidence progressing to a consensus team evaluation (Whitehouse et al., 2018). A recommendation in New Zealand guidance is development of diagnostic assessments pathways; and that diagnostic assessments are most likely conducted by psychologists or psychiatrists (New Zealand Ministry of Health (Ministries of Health and Education, 2016)).
With an emerging literature on the discrepancies between existing CGs and the experiences of service users and clinicians providing services, it is timely to ascertain the views/experiences of stakeholders (those going through the autism diagnostic assessment pathway and those providing assessments) about what constitutes optimum autism assessment and diagnosis services for adults (NICE, 2012, 2014).
The aim of this study was to survey autistic adults, relatives and clinicians regarding recent experiences of adult autism assessment and diagnosis in the United Kingdom; and co-produce consensus statements on optimal adult autism assessment and diagnosis services.
Method
The study design was to survey three stakeholder groups (stage 1), followed by a modified Delphi process to achieve consensus among clinicians on statements regarding optimal adult autism assessment/diagnosis services derived from the collated Stage 1 survey findings from all stakeholders (autistic adults, relatives and clinicians; stage 2; Figure 1).
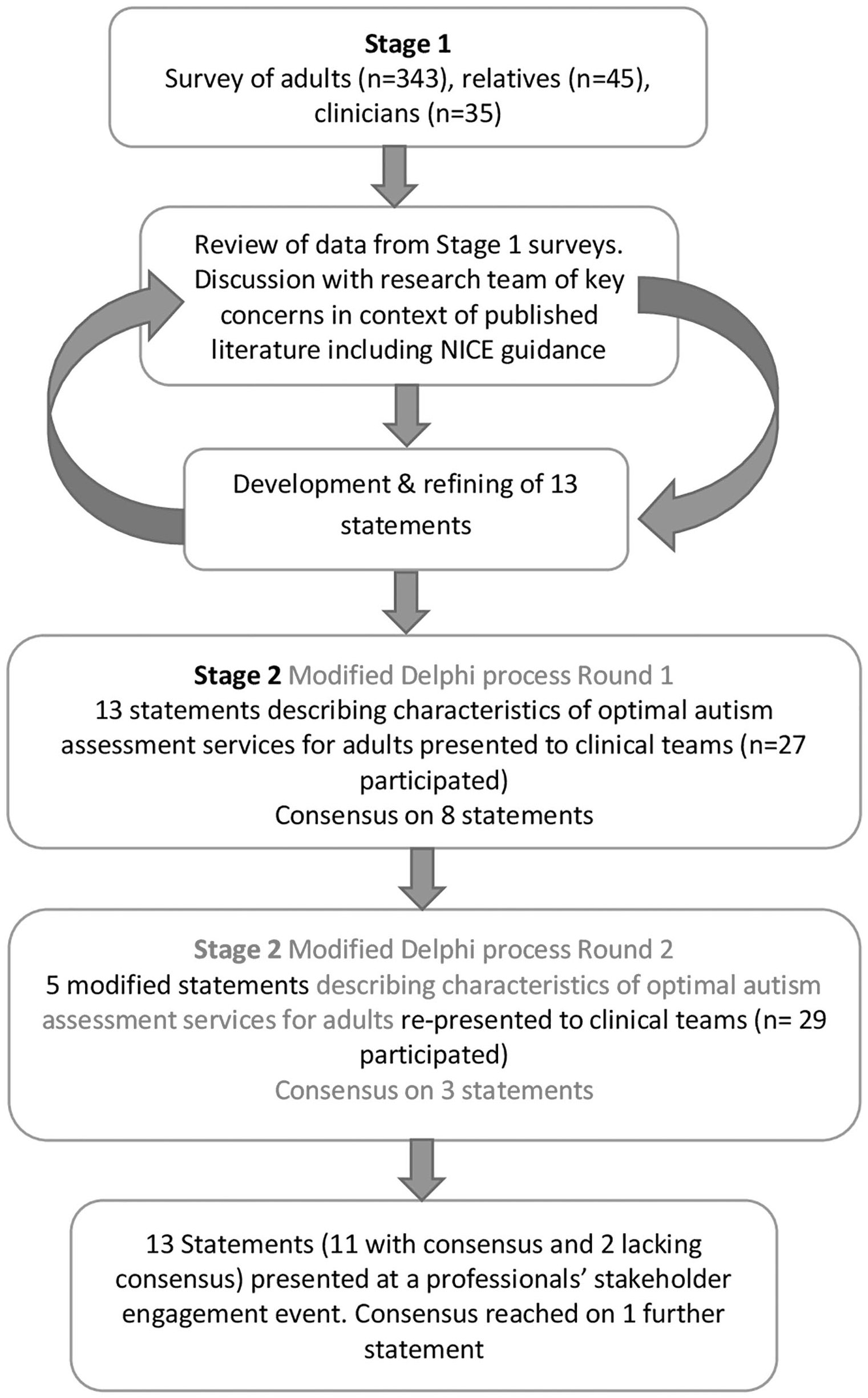
Study flowchart.
Wales Research Ethics Committee 5 gave the study a favourable opinion (Reference: 17/WA/0188).
Stage 1 methods
Participants
Autistic adults and relatives aged 18 years and above were recruited via the Adult Autism Spectrum Cohort-UK (ASC-UK), a cohort of autistic adults and relatives of autistic adults recruited to longitudinal research (https://research.ncl.ac.uk/adultautismspectrum). The ASC-UK team invited autistic adults and relatives to participate in this diagnosis study.
Regarding autistic adults who lack capacity to consent for themselves (e.g. some people with learning disability/intellectual disability), ASC-UK enables a consultee/proxy to join the cohort to represent them. Study inclusion criteria were autistic adults who had received an autism diagnosis during adulthood in the preceding 5 years, and relatives of adults diagnosed during adulthood within the past 5 years. Relatives of autistic adults were not required to be related to an adult participating in the study. Those invited to participate included 667 autistic adults and 198 relatives of autistic adults from ASC-UK.
Inclusion criterion for clinicians was conducting UK adult autism diagnostic assessments. We recruited clinicians from those supporting recruitment to the ASC-UK, national special interest groups and networks of multidisciplinary professionals working in autism assessment and diagnosis teams. The study team approached clinicians directly. We invited one lead clinician from a service to complete the survey on behalf of their team to capture MDT perspectives. During the consent process, clinicians participating in stage 1 survey were invited to participate in the follow-up stage 2 modified Delphi process.
Measures
Demographic data about participants were available from the ASC-UK cohort datasets. When consenting to join ASC-UK, adults and relatives are invited to complete a registration questionnaire (‘Learning about the Lives of Adults on the Autism Spectrum’). Questions include date of autism diagnosis, relationship and employment status, and any physical or mental health conditions. Adults consenting to join ASC-UK are also asked to complete the Adult Social Responsiveness Scale (SRS-2), 65-item measure of autism traits measured on a 4-point Likert-type scale, high scores corresponding to higher social and communication difficulties (Constantino & Gruber, 2012).
Participants completed one of three versions of a survey ‘Getting an Autism Spectrum Disorder Diagnosis in Adulthood, and Support or Services Received Afterwards’ (Online Supplementary Materials Sections 1 and 2). Survey content was informed by published international CGs including UK NICE CG142 (NICE, 2012) and Quality Standards (QS51; NICE, 2014). The survey for autistic adults (completed by adults able to give informed consent/or consultees/proxys on behalf of adults unable to give informed consent) and parallel survey for relatives each comprised 32 open, closed (yes/no) and multiple-choice questions across three sections: referral process/pre-assessment, diagnostic assessment and post-diagnosis. A separate survey for clinicians included 31 open and closed questions in five sections: service setting, referral process/pre-assessment, diagnostic assessment, post-diagnosis and training/consultancy. For all three surveys, there was facility for respondents to add comments if they wanted to for some closed-response/multiple-choice questions (e.g. in the ‘other please specify’ section).
The information, consent forms and survey schedules for service users were developed in consultation with autistic adults and relatives during two focus groups co-facilitated by a relative of an autistic person. Autistic adults and relatives interested in attending the focus groups were emailed study documentation prior to the group; during the group, their views on study documentation wording, layout, content and format were elicited.
Procedures
Autistic adults and relatives who met inclusion criteria were sent online or paper versions of the information sheet (including an ‘easy-read’ version), consent form and a survey depending on their preferred method of contact (information given when joining the ASC-UK).
Clinicians were sent paper or online versions of study documentation depending on their preference. Online participants were sent an email with a unique link to the survey created using online survey software (Qualtrics, 2005). Informed consent was provided by all participants and could be completed on paper or online. A reminder letter was sent to non-responders after 2 weeks. Following informed consent, participants completed the survey.
Data analysis
Stage 1 analysis comprised descriptive statistics. Assessment of skewness/kurtosis indicated quantitative data were non-normally distributed. Non-parametric analyses were used to investigate between-group differences (Mann–Whitney and chi-square; Field, 2013).
Using a combination of the three stakeholder groups stage 1 survey quantitative findings, open-text responses and taking published literature including the UK NICE clinical guidance documents into account, an initial set of statements describing characteristics of optimal autism diagnostic services were generated by the authors. The first author undertook a review (reading and familiarisation with the data) of closed/open-text responses and comments received in the stage 1 surveys from adults, relatives and clinicians to identify potential common topics of concern from which to develop Delphi statements. The research team (including an autistic co-investigator and clinicians experienced in diagnosing autism in adults) discussed topics identified over several meetings and defined the statements through an iterative process of discussion and refining wording.
This article reports results from the closed and multiple-choice questions; we also report examples of the comments added to the closed question items. The findings relating to post autism-diagnosis support and services (Wigham et al., submitted) and qualitative analysis of open-text responses are reported elsewhere.
Community involvement statement
An autistic co-investigator was part of the research team throughout the study; members of the autism community attending the focus groups as advisors on study documentation received vouchers to cover costs and thank them for their time. Autistic adults and relatives from the North East United Kingdom participating in the survey were sent an invitation to a community dissemination workshop where study findings were presented by the research team.
Stage 1 results
Participant characteristics
A total of 343 (51.4% response rate) autistic adults including 4 consultees/proxys (reporting on behalf of an autistic adult lacking capacity to consent themselves) consented and completed the survey. Participants included 194 women and 137 men (mean age 43.2 years, range 19–89 years): 148 (43.1%) participants were educated to University degree level or higher and 143 (41.7%) were in employment, 161 (46.9%) were in a relationship and 166 (48.3%) did not receive any support (Table S2a). The mean SRS-2 total score for autistic adults was 114 (SD = 25; clinical cut-off for autism 65; Constantino & Gruber, 2012). We compared gender, age, self-reported anxiety/depression diagnoses and autism traits (SRS-2 scores) of responders with participants from the ASC-UK cohort who did not participate (non-responders; Table S2a). The ratio of women to men was slightly higher in responders (56.5%) (χ2(2) = 7.83; p < 0.05). Responders were significantly older (median age 42 years) than non-responders (median age 37 years; U = 61,204; p = 0.001); and more frequently had a self-reported diagnosis of anxiety (χ2(1) = 3.95; p < 0.05) and/or depression (χ2(1) = 3.41; p < 0.05) than non-responders. There were no between-group differences in SRS-2 scores (U = 31,351; p = 0.56).
Of those relatives invited to complete a survey, 22.7% participated (n = 45) comprising 36, 80.0% women, 91.1% White British and average age 58.3 years (range 25–79). The characteristics of relatives and autistic adults they gave information about are shown in Table S2b.
Thirty-five UK clinicians completed the survey (see Supplementary Table S2c).
Referral process and pre-assessment: autistic adults and relatives
Perspectives of adults and relatives on the pre-assessment and referral process are shown in Table 1. Most adults (281, 81.9%) reported receiving help to make a referral (the majority from their primary care doctor: 204, 59.5%). Although most autistic adults reported no problems obtaining an autism assessment, 91 adults (26.5%) and 18 relatives (40.0%) reported difficulties. Few adults (89, 25.9%) and relatives (17, 37.8%) waited less than 12 weeks for their first assessment appointment; 224 adults (65.3%) waited more than 12 weeks. One-third of adults (113, 32.9%) completed a questionnaire about autism before their first appointment; 101 (29.4%) completed a questionnaire about their health. Some autistic adults (86, 25.1%) attended a pre-assessment appointment and a substantial minority (127, 37.0%) received information about what to expect during assessment. Some autistic adults (117, 34.1%) and relatives (27, 60.0%) received pre-assessment requests for information from a family member/friend.
Referral process/pre-assessment: autistic adults and relatives.
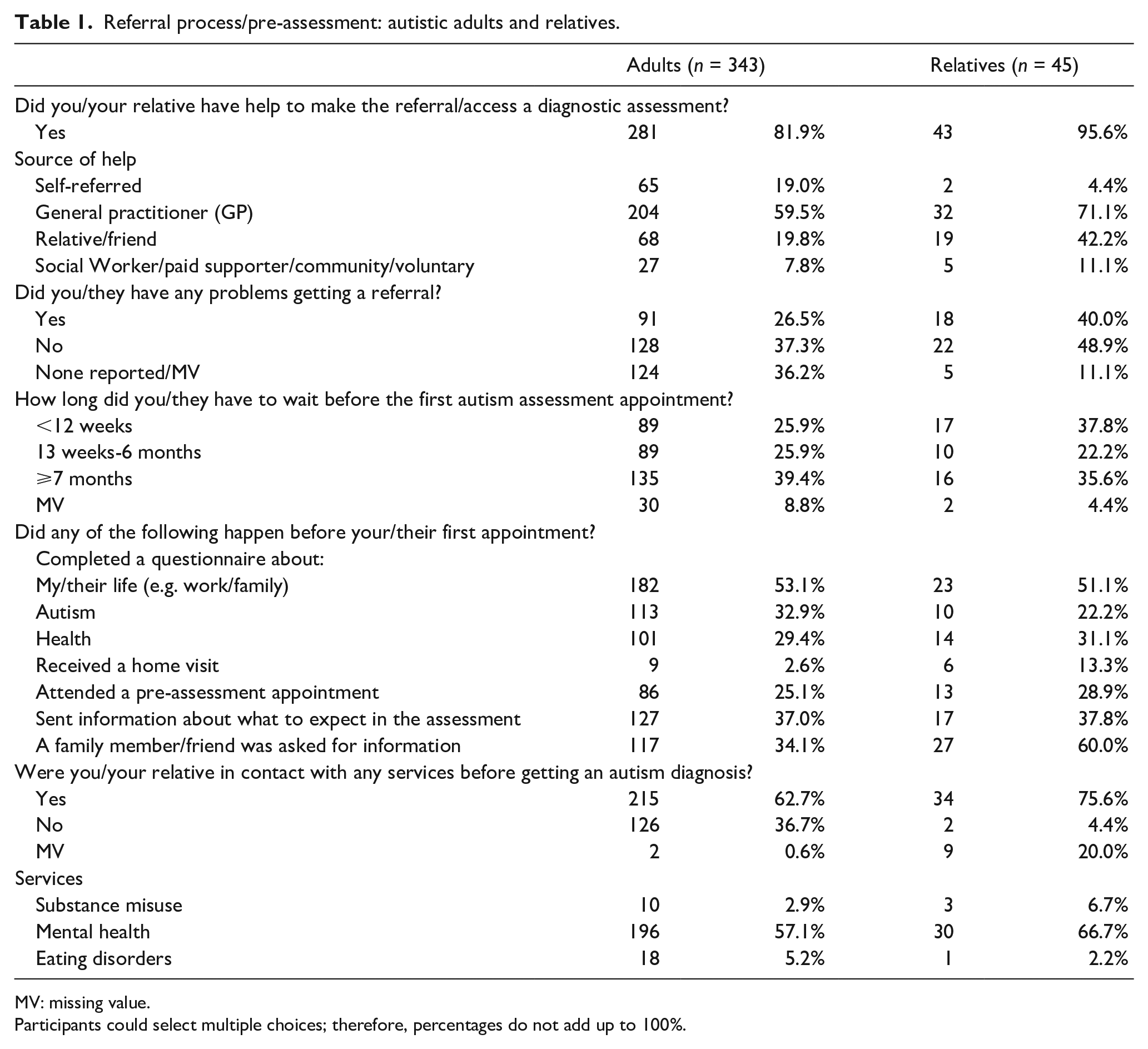
MV: missing value.
Participants could select multiple choices; therefore, percentages do not add up to 100%.
Many autistic adults (196, 57.1%) and relatives (30, 66.7%) reported contact with mental health services prior to their autism diagnosis.
Referral process and pre-assessment: clinicians
The majority of clinicians (30, 85.7%) conducted pre-assessment liaison or information gathering; 19 respondents (54.2%) obtained a report from referring clinicians. Some gathered pre-assessment self-report information including mental health questionnaires, for example, the Patient Health Questionnaire (PHQ-9; 5, 14.2%; Kroenke & Spitzer, 2002). Twenty-five (72.8%) used ASD-specific measures, for example, the Social Responsiveness Scale (SRS-2; Constantino & Gruber, 2012).
Most clinicians were able to report waiting times; 15 (42.8%) reported waiting times of less than 12 weeks, while 7 clinicians (20.0%) had a wait of more than 13 months. Thirteen clinicians (37.1%) described referring some people onward to another clinical team, for example, due to diagnostic uncertainty.
Diagnostic assessment: autistic adults and relatives
Perspectives of autistic adults and relatives on the characteristics of the diagnostic assessment procedure are shown in Table S3. Just under half of adults (164, 47.8%) and relatives (19, 42.2%) said the assessment was carried out in an autism clinic. Just over half of autistic adults (189, 55.1%) and relatives (24, 53.3%) reported a psychologist conducted the diagnostic assessment. A minority of adults (79, 23.0%) and relatives (8, 17.8%) reported being assessed by a psychiatrist. A few autistic adults reported being assessed by a speech and language therapist (33, 9.6%), an occupational therapist (24, 7.0%) or a nurse (42, 12.2%).
Most adults (273, 79.6%) and relatives (41, 91.1%) said their assessment was age-appropriate; though some adults (30, 8.7%) and relatives (1, 2.2%) were less positive. While the majority of adults (277, 80.7%) and relatives (41, 91.1%) reported their assessment was gender-appropriate, again some adults (16, 4.7%) and relatives (1, 2.2%) disagreed.
Regarding adjustments to make the assessment process acceptable for autistic adults, many adults (254, 74.1%) and relatives (27, 60.0%) were happy with the consideration given to sensory aspects. However, a substantial minority of adults (59, 17.2%) and relatives (10, 22.2%) were unhappy with this aspect of the assessment. Most adults (271, 79.0%) and relatives (33, 73.3%) were satisfied with availability of a quiet room/area during the assessment, or when waiting; and with the number of breaks during the assessment (adults: 272, 79.3%; relatives: 33, 73.4%).
While many adults (245, 71.5%) and relatives (31, 68.9%) were positive about information provided beforehand, a substantial minority (79 adults, 23.0%) and (6 relatives, 13.3%) were unhappy with this aspect of the assessment. Finally, most adults (307, 89.5%) and relatives (30, 66.6%) were satisfied with appointment length; however, some adults (24, 7%) and relatives (7, 15.6%) were less positive.
Most adults (322, 93.9%) and relatives (43, 95.6%) reported receiving feedback on assessment outcome. This was at a face-to-face appointment for just over half respondents (adults: 197, 57.1%; relatives 28, 62.2%). Most people reported receipt of a letter/formal diagnostic report (adults: 296, 86.3%; relatives: 40, 88.9%).
Diagnostic assessment: clinicians
At the assessment appointment, most clinicians (33, 94.2%) reported usually consulting a parent/family member to gather information about an individual’s current and past presentation. However, an informant was not always available – only three clinicians (8.6%) said all assessments included an informant-based developmental history (Table S4). Twelve clinicians (34.3%) reported that 50%–74% of assessments involved an informant. Seventeen clinicians (48.5%) reported they would consult a friend and 23 (65.7%) gathered school reports where relevant.
Clinicians regularly used a variety of standardised assessments. Sixteen used a standardised interview for history taking (45.7% using the Autism Diagnostic Interview-Revised: ADI-R; Rutter et al., 2003). Ten (28.5%) used the sensory profile to enquire about sensory aspects (Brown et al., 2001). Twenty-four clinicians (68.5%) used the Autism Diagnostic Observation Schedule-Generic (ADOS-G; Lord et al., 1999).
Regarding adjustments, most clinicians (29, 82.8%) accommodated people’s sensory needs. Twenty-five (71.4%) offered appointments in locations where light, noise and number of people were not overwhelming. Nineteen (54.2%) had received positive feedback on offering flexibility, for example, evening appointments.
Regarding professional disciplines of members of the autism assessment team, 24 clinicians (68.6%) had a psychologist while 18 (51.4%) had a psychiatrist available in the core team to complete diagnostic assessments. A minority reported having an occupational therapist (11, 31.4%) and/or a speech and language therapist (11, 31.4%) in their team. Clinicians reported assessments took a median of 6 h, followed by 3 h to prepare the diagnostic report and carry out liaison. One-third of clinicians shared the diagnostic outcome and formulation at the appointment where information regarding diagnosis was gathered; most teams (71.4%) reported sharing diagnostic outcome and formulation at a follow-up appointment.
Training and consultancy: clinicians
Many clinicians provided training, supervision or consultancy for other parties (Table S5) including potential referrers (23, 65.7%), adult mental health (17, 48.5%) and intellectual disability services (15, 42.8%). Twelve clinicians (34.2%) described providing training on use of diagnostic tools.
For all three surveys, some participants provided additional information for some closed-response questions (e.g. in the ‘other please specify’ section). Illustrative quotes representing the range of comments made have been included in Table S6.
Stage 2 methods
Modified Delphi process round 1
Participants
Clinicians participating in the stage 1 survey (n = 35) were invited to participate in a modified Delphi process.
Measures
Following stage 1, 13 statements were generated by the research team to describe what might constitute optimum adult autism diagnostic services (Table S7). The statements were included in round 1 of the modified Delphi process, grouped into the following categories: (1) referral process/pre-assessment, (2) diagnostic assessment, (3) post-diagnosis and (4) training/consultancy. Each statement was followed by a Likert-type-style response option from 1 (strongly disagree) to 9 (strongly agree). The range (1–9) informed by Delphi survey methodology and methods of developing CGs/outcome indicators (Alwin & Krosnick, 1991; Guyatt et al., 2011; Williamson et al., 2017). An open-text box allowed for comments including suggestions for wording modifications.
Procedures
The Delphi process was created using Qualtrics software and sent to participants by email. Participants were asked to complete the online Delphi process within 2 weeks.
Data analysis
We used a pre-specified threshold to appraise agreement on statements defined as ⩾ 67% of respondents scoring 7–9 (Sinha et al., 2011). This was based on agreement levels recommended in the literature (ranging from 50%–80%) and published Delphi studies seeking consensus among health professionals (Hasson et al., 2000; Morris et al., 2014). We retained statements on which there was agreement after Delphi round 1. Data collected on post-diagnosis are reported elsewhere (Wigham et al., submitted).
Modified Delphi process round 2
Participants
Clinicians participating in the stage 1 survey were also invited to participate in the modified Delphi process round 2.
Measures
The research team modified the wording of five statements that fell below the agreement threshold in round 1 taking into account Delphi participants’ open-text comments. The modified statements from round 1 were used for the Delphi round 2.
Procedures
Participants were only sent the modified statements in round 2 and asked to rate them using the same procedure as round 1 (by email/online with a response scale of 1 (strongly disagree) to 9 (strongly agree) and open-text box for comments). Participants were asked to complete their responses for the modified statements within 2 weeks.
Data analysis
The ratings for the modified statements were appraised against the agreement threshold used in round 1.
Stage 2 results
Modified Delphi process round 1
Twenty-seven clinicians completed Delphi round 1; scores ranged from 2 to 9 and agreement was achieved on 8 out of 13 statements with ⩾ 67% of respondents scoring 7–9 (Table S7).
Modified Delphi process round 2
Twenty-nine clinicians participated in round 2. Agreement was reached on three of the five modified statements (Table S7). Illustrative quotes from open-text comments regarding statements 1 and 10 for which consensus was not reached (i.e. did not reach ⩾ 67% agreement threshold) are shown in Table S8. These two statements were taken to a stakeholder workshop for discussion.
Stakeholder workshop with professionals
Following the Delphi round 2, an in-person stakeholder workshop with professionals was organised to disseminate survey findings and discuss the consensus statements. UK clinicians were sent an email invitation to join a clinicians’ workshop. Presentations of study findings were made by an autistic co-investigator and the research team.
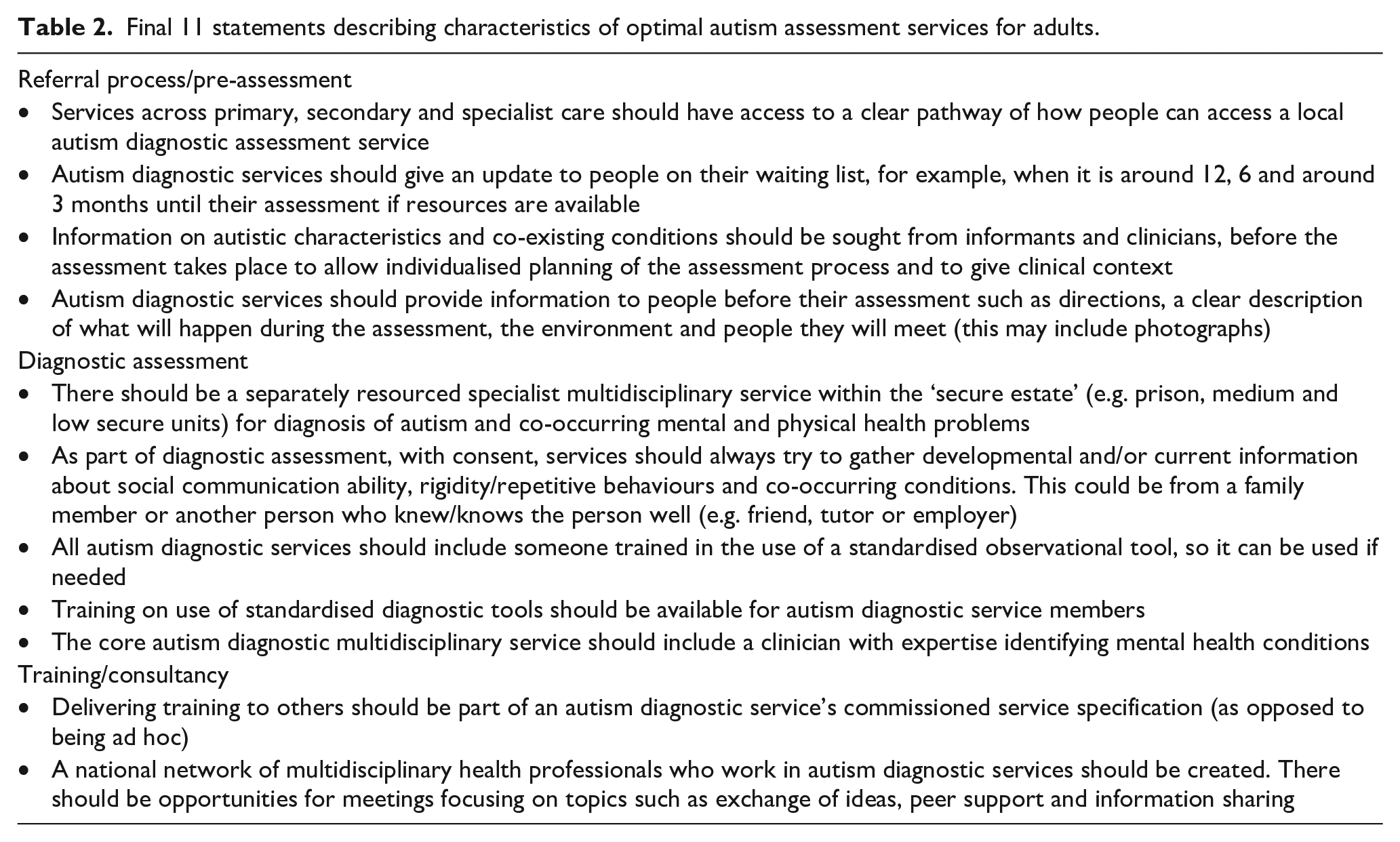
Round-table discussions at the clinician’s workshop facilitated consultation regarding the two outstanding statements, and there was agreement for statement 10 (‘there should be increased availability of free to use structured autism diagnostic interviews’) with caveats (Table S8). Workshop delegates were unable to reach consensus on statement 1 (‘autism diagnostic services should be commissioned, and resourced to accept self-referrals from adults who suspect they have an autism spectrum disorder’). The final set of statements are listed in Table 2.
Final 11 statements describing characteristics of optimal autism assessment services for adults.
Discussion
Key findings
This study is the largest, to date, to take account of the views from autistic adults, relatives and clinicians about UK adult autism assessment and diagnostic services, and how they could be improved. Autistic adults, relatives and clinicians reported some positive aspects and experiences; however, there were also examples of suboptimal service provision, and all stakeholders made suggestions about how autism diagnostic services might be improved. These responses, and the agreed statements describing the characteristics of optimal adult autism assessment and diagnostic services, are relevant for UK clinicians, managers and commissioners to improve diagnostic assessments for autistic adults, and relatives and have relevance internationally, especially in countries with similar health systems.
Dissemination events were undertaken and attendees were positive about the survey results, the statements about optimal clinical service provision and the potential for findings to be used in service improvements.
Referral process and pre-assessment
A high proportion of adults were in contact with mental health services before their diagnostic assessment reflecting possible difficulties in case-recognition of autism in the presence of mental health conditions (Fusar-Poli et al., 2020), missed opportunities for diagnosis and difficulties accessing the autism pathway. This is consistent with previous international research and is not unique to the United Kingdom (Crucitti et al., 2018; Huang et al., 2021; Lewis, 2017). While a clear diagnostic pathway is recommended in UK national guidance (NICE, 2012) and associated with service user satisfaction (Evans et al., 2021), international research identifies a heterogeneity of routes to diagnosis (Geurts & Jansen, 2012). An indicator of optimal services identified in this study was a clear pathway of how people can access a local autism assessment and diagnosis service (statement 2).
There were some positive comments from all stakeholder groups about self-referral to autism diagnostic services. However, consensus was not reached by clinicians regarding diagnostic assessment services accepting self-referrals. This may be because of concern about the number of self-referrals that could be received compared with assessment capacity and because clinicians wanted to highlight how important it is that individuals accessing diagnostic assessment services are linked with wider support (e.g. through primary/secondary care). Previous studies have also described concerns that if clinicians’ views on appropriateness of an autism diagnosis diverge from those of service users, insistence on self-referral to an autism assessment pathway may delay meeting a person’s needs appropriately (Crane et al., 2018). We recommend that for the United Kingdom, commissioners should work with diagnostic teams and the autistic community to identify whether acceptance of self-referrals should be part of service specification, and if so, the conditions and organisational arrangements required to support this.
NICE QS (2014) make recommendations regarding the length of waiting times (maximum 12 weeks), but as expected (Rutherford, McKenzie, Forsyth, et al., 2016) many adults and relatives waited considerably longer. Given the significant emotional impact of an autism diagnosis (Huang et al., 2020) the uncertainty of a lengthy wait for an assessment is bound to be an additional stress. Clinicians’ views about keeping people up to date with their position on the waiting list (statement 3) would involve extra work for services; additional resources would be required for implementation. Provision of information to people before their assessment (e.g. description of what will happen; statement 5) and gathering information before the assessment (e.g. from informants; statement 4) may also incur extra work and resources. These aspects could be incorporated into future service specifications and commissioned/funded.
Diagnostic assessment
Autistic adults in Australia described limited standardisation in the diagnostic assessment, similarly clinicians in Scotland had less likelihood of using standardised tools in adulthood versus childhood services (Huang et al., 2021; Rutherford, McKenzie, McClure, et al., 2016). This study identified three statements regarding standardised assessments (statements 8–10). We have created and undertaken an initial evaluation of the Autism Clinical Interview for Adults (ACIA; Wigham et al., 2020) that has both subject and informant versions to address the needs of clinical teams; training and the interviews are available on request from the corresponding author, and also see https://tinyurl.com/ACIAtraining.
In this study, indicators of optimal autism diagnostic services included gathering information on co-occurring conditions and having a core team member with expertise in identifying mental health conditions (statements 4 and 11). If implemented, both these indicators would help address the importance of identifying mental health conditions commonly co-occurring with autism, and contribute to better understanding of accurate differential diagnosis and reduce the risk of missed/misdiagnosis (Crucitti et al., 2018; Fusar-Poli et al., 2020; Hand et al., 2020; Lever & Geurts, 2016).
An interesting finding was statement 6, highlighting an important unmet need and gaps in specialist health provision for client groups with additional risks (e.g. people cared for within secure or forensic settings). This is in accordance with previous research (Kirby et al., 2015; McCarthy et al., 2019). For example, autism traits in male prisoners who later received an autism diagnosis were unrecognised by prison staff; the challenges of conducting autism diagnostic assessments in prisons have been identified (Underwood et al., 2016).
NICE (2012) recommend obtaining an early developmental history, and while most clinicians reported they would usually consult an informant, this was not always possible. Many clinicians highlighted the need for a flexible approach, for example, by consulting a friend or employer for current information in the absence of a developmental history (statement 7).
There were limitations in access to some professionals in the core diagnostic team, meaning provision of a MDT assessment as recommended was not always possible (NICE, 2012). This may impact the extent to which diagnoses and recommendations for co-occurring conditions could be made, and further development of MDTs is needed to ensure teams are able to complete assessments in line with NICE Clinical Guidance.
Training and consultancy
Several statements (8, 9 and 12) indicated the importance of access to high-quality training for clinicians (for example, to use an observational assessment) and the role of clinicians in providing training for other parties. This was aligned with legislation (Autism Act, 2009; NICE, 2012). For example, over 50% of adults were in contact with mental health services before receiving their autism diagnosis, which may mean a lack of understanding of autism in primary and secondary health care impacted their access to the diagnostic assessment service pathway. This is consistent with reports of autistic adults highlighting improved clinician understanding of autism as important for healthcare access (Brice et al., 2021; Mason et al., 2021). In the United States, gaps in knowledge and experience of clinicians in community mental health services, were identified as barriers to provision of mental health care for autistic adults, along with the need to improve training and consultancy to address this (Maddox & Gaus, 2019). Specialist skills are required to deliver high-quality mental health care for autistic adults, which some clinicians in secondary mental health care may lack confidence to implement (Maddox et al., 2020). For example, few autistic adults receive cognitive behavioural therapy (CBT) for anxiety and depression (Maddox et al., 2019) despite evidence of acceptability (Maskey et al., 2019) with specialist adaptations being required (Parr et al., 2020).
At the multidisciplinary professionals’ stakeholder meeting, clinicians let us know that was the first time they had ever met up with professionals from other UK autism diagnostic teams. They reported the need for a clinical network for adult autism assessment and diagnosis, which was developed subsequently.
Strengths and limitations
A strength of the study is the integration of the separate perspectives of key stakeholders (autistic adults, relatives and clinicians) including clinicians from different adult autism diagnostic service settings and achieving a consensus view across these different settings. A further strength is that roughly equal numbers of women and men were recruited facilitating a balanced representation of the perspectives of both genders on adult autism assessment and diagnosis services and processes.
The Delphi process consisted of two rounds only and consensus was not reached on all 13 statements. While two rounds are acceptable (Hasson et al., 2000), this is a potential limitation to the study. However, the clinicians provided detailed comments during round 2, which were considered during the clinicians’ stakeholder workshop round table discussions. This led to agreement about one further statement.
The statements presented during the Delphi process were derived from information gathered from all stakeholders (autistic adults, relatives and clinicians). Clinicians were then invited to take part in the Delphi process since implementation of the statements would likely require change in clinical practice (Michie et al., 2005). Although the absence of a consumer perspective during stage 2 could be considered a limitation, the statements all had the backing of service users and the purpose of the Delphi was to ascertain whether clinicians could endorse the statements as indicators of optimum services.
Although participating clinicians included intellectual disability services, the study findings may not reflect the experiences of individuals with intellectual disability who were under-represented in this sample of autistic adults and relatives. About 90% of participants in this study self-reported as White British. In light of evidence suggesting that access to autism assessment and diagnostic services is limited for individuals from indigenous and ethnic minority groups, this is a definite limitation and further research should be undertaken to capture the perspectives of a much broader range of ethnic groups (NICE, 2012; Roy & Balaratnasingam, 2010; Tromans et al., 2021).
Future research
This large study provides clear contemporaneous evidence about service improvements that should be undertaken; there was support from professionals that the findings should be implemented. There may also be other contexts where researchers could build on the findings from this study to see if they are applicable in their context.
A good evidence base for these indicators exists in the United Kingdom, hence priority should shift to focus on multi-level barriers/facilitators to improve integration of evidence-based service improvements into practice. Implementation science models could be used to understand the complex individual/organisational level factors (e.g. environmental resources/restrictions) required to support practical and sustainable implementation of the findings into clinical service provision (Michie et al., 2005, 2011; Proctor et al., 2009) Alongside investigating the effectiveness of improvements to facilitate pathways, timely and valid diagnoses, and patient and professional satisfaction, return on investment analyses would clarify the economic impact of making service improvements.
Conclusion
Autistic adults, relatives and clinicians reported some positive aspects and experiences; however, there were also examples of suboptimal service provision, and all stakeholders made suggestions about how autism diagnostic services might be improved. These responses, and the agreed statements describing the characteristics of optimal adult autism assessment and diagnostic services, have immediate relevance for UK service providers and commissioners to make service improvements that should increase quality and satisfaction for adults, relatives and clinicians going forward. Dissemination events were undertaken with autistic adults, relatives and clinicians; attendees were positive about the survey results, the statements about optimal clinical service provision and potential for the findings to be used in service improvements.
The areas of improvement identified for adult autism diagnostic and assessment services by autistics adults, relatives and clinicians and the 11 statements have relevance for international service developments. The study supplements NICE QS by presenting additional detail on the characteristics of optimal adult autism diagnostic and assessment services from the perspectives of autistics adults, relatives and clinicians gathered since publication of NICE guidance documentation. Some indicators could be implemented immediately and others will require protected funding to support sustainable implementation.
Supplemental Material
sj-docx-1-aut-10.1177_13623613211073020 – Supplemental material for A survey of autistic adults, relatives and clinical teams in the United Kingdom: And Delphi process consensus statements on optimal autism diagnostic assessment for adults
Supplemental material, sj-docx-1-aut-10.1177_13623613211073020 for A survey of autistic adults, relatives and clinical teams in the United Kingdom: And Delphi process consensus statements on optimal autism diagnostic assessment for adults by Sarah Wigham, Barry Ingham, Ann Le Couteur, Colin Wilson, Ian Ensum and Jeremy R Parr in Autism
Footnotes
Acknowledgements
The authors are grateful to the research participants, Dr Alex Petrou and Professor Helen McConachie for their work on the Adult Autism Spectrum Cohort-UK, to administrators Faye Wolstenhulme and Carla Black, and to Deborah Garland (National Autistic Society) for advice and support with the consultation groups.
Authors’ note
Note on terminology: We use the term autism throughout the article to describe the diagnoses such as autism spectrum disorder, autistic disorder, autism spectrum conditions, atypical autism, Asperger’s Syndrome and PDD-NOS. We use the term ‘autistic adults’ to describe adults with a range of autism spectrum diagnoses.
Author contributions
JRP, ALC and BI were awarded funding. JRP was the chief investigator. JP, SW and ALC wrote the first draft of the article. All authors contributed during the editing and reviewing process and also approved the final article.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors are grateful to the UK autism research charity Autistica, who funded the study as part of the Autism Life Course and Ageing research programme at Newcastle University, and to Cumbria, Northumberland Tyne and Wear NHS Foundation Trust for sponsoring the research, and providing funding through Research Capability Funding.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.