
Abstract
The Autism-Spectrum Quotient is a self-report scale, used to assess autistic traits. It was tested cross-culturally, and a short version was created to clinically refer adults for an autism assessment. This study aimed to examine the properties of the Hebrew version of the Autism-Spectrum Quotient and to create a short version suitable for Diagnostic and Statistical Manual of Mental Disorders (5th ed.). Ninety-three clinically diagnosed autistic adults (24 females) aged 18–53, and 147 comparable controls (34 females) completed the Hebrew version of the Autism-Spectrum Quotient. Ten clinicians specializing in diagnosing autism in adults classified the Autism-Spectrum Quotient’s items according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria. The Hebrew version of the Autism-Spectrum Quotient showed good internal consistency (Kuder-Richardson 20 = 0.90). Based on the prevalence of autism among clinically referred adults (70%), receiver operating characteristic analysis yielded area under the curve of 0.94. A cutoff of 21 demonstrated high sensitivity (0.90), specificity (0.76), positive predictive value (0.90), and negative predictive value (0.77). The short version of the Hebrew Autism-Spectrum Quotient included five social communication and five restricted, repetitive behavior items, which represented two social communication and two restricted, repetitive behavior criteria of Diagnostic and Statistical Manual of Mental Disorders (5th ed.). It showed good internal consistency (Kuder-Richardson 20 = 0.86), and receiver operating characteristic analysis yielded area under the curve of 0.95. An optimal clinical cutoff of five showed high sensitivity (0.90), specificity (0.82), positive predictive value (0.92), and negative predictive value (0.78). The Hebrew version of the Autism-Spectrum Quotient and the short version of the Hebrew Autism-Spectrum Quotient can be effectively used to help screen for autism in clinically referred adults.
Lay Abstract
Despite the attempt to diagnose autism at an early age, there are still many individuals who would only get an autism diagnosis in adulthood. For these adults, a questionnaire that could assist in highlighting their need to seek diagnostic assessment is needed. The Autism-Spectrum Quotient is a self-report scale used to assess autistic traits. It was tested cross-culturally, and a short version was recommended to help identify adults who should be referred for an autism assessment. However, its relevance for the up-to-date diagnostic criteria, according to the Diagnostic and Statistical Manual of Mental Disorders (5th ed.), has not been tested. This study aimed to examine the psychometric properties of the Hebrew version of the Autism-Spectrum Quotient and to create a short version of the Hebrew Autism-Spectrum Quotient, based on items which map on to Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria. Ninety-three autistic adults (24 females), aged 18–51, clinically diagnosed according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.), and 147 comparable controls (34 females) filled out the Hebrew version of the Autism-Spectrum Quotient. Ten clinicians who specialize in diagnosing autism in adults classified the Autism-Spectrum Quotient’s items according to Diagnostic and Statistical Manual of Mental Disorders (5th ed.) criteria. The short version of the Hebrew Autism-Spectrum Quotient comprised items that best differentiated between adults with and without autism, five items representing each of the Diagnostic and Statistical Manual of Mental Disorders (5th ed.) diagnostic domains. The overall probability for participants to be correctly classified as autistic or neurotypical was 86% for the Hebrew version of the Autism-Spectrum Quotient and 88% for the short version of the Hebrew Autism-Spectrum Quotient. We conclude that both versions are reliable and sensitive instruments that can help referring adults for autism assessment.
Autism spectrum disorder (henceforth autism) is a set of neurodevelopmental conditions characterized by differences in social communication (SC) alongside unusually repetitive behaviors and restricted interests, difficulties with unexpected change, and sensory hyper- or hypo-sensitivity, affecting 1.1% of the adult population (Brugha et al., 2016). According to the latest report from the U.S. Department of Health and Human Services, one in 44 eight-year-olds is diagnosed with autism (Maenner et al., 2021). The majority of autism research focuses on early childhood (Murphy et al., 2016), since outcomes may be optimal the earlier a diagnosis has been made (Fernell et al., 2013). However, despite comprehensive attempts to diagnose autism in childhood, many autistic individuals have been missed or misdiagnosed, even into adulthood (Lai & Baron-Cohen, 2015).
In Israel, autism prevalence is reported to be 0.49% among the total population of 8-year-olds (Raz et al., 2015). A recent governmental report showed that the number of adults diagnosed with autism (aged 21 and over) in 2018 was about a third of the number of registered children with autism (Ministry of Labor, Social Affairs and Social Services, 2019). This gap suggests under-diagnosis of autism in adults in Israel and highlights the need for good measures to identify those who require support and direct them to an appropriate diagnostic assessment.
A common adult measure of autistic traits is the Autism-Spectrum Quotient (AQ; Baron-Cohen et al., 2001). This self-report instrument comprises five theoretically driven subscales: social skills, communication, attention to detail, attention switching, and imagination. The AQ was originally designed to assess individual differences in autistic traits. It was also used as a screener, with a cutoff of 32 for probable autism in British adults (Baron-Cohen et al., 2001). A score of 26 and above has been suggested as an appropriate cutoff in a clinically referred population, in which a clinician has already raised the question of an autism diagnosis (Woodbury-Smith et al., 2005).
The AQ has been translated into 36 different languages and used extensively for research and clinical purposes. Various AQ cutoffs have been reported in cross-cultural studies, including 33 in Japan (Wakabayashi et al., 2006), 32 in the United States (Conner et al., 2019), 29 in Australia (Broadbent et al., 2013), 25 in Poland (Pisula et al., 2013), and 22 in French–Canada (Lepage et al., 2009). The cutoffs were defined based on various measures such as the instrument’s best correct classification (Woodbury-Smith et al., 2005), low false-positive rate (Broadbent et al., 2013), or the best differentiation between the percentage of participants with and without autism who passed the cutoff (Lepage et al., 2009). However, it has been suggested that positive predictive value (PPV) and negative predictive value (NPV) should be used to determine the appropriate levels of specificity and sensitivity, when defining the instrument’s cutoff (Bezemer et al., 2021; Parikh et al., 2008). These values can help define the cutoff in a given population, considering the chances that an individual who passed the cutoff actually has autism (PPV), as well as the chances that a person who does not have the condition scores below the questionnaire’s cutoff (NPV). PPV and NPV take into account the prevalence of the condition in the given population. Hence, different values and different cutoffs should be considered when screening in the general population, or when focusing on a clinically referred population, in which the condition’s prevalence may be significantly higher, thus requiring a more sensitive cutoff. A sensitive screening tool could be beneficial for the improvement of services in tertiary diagnostic centers. Contrarily, when screening in the general population, cutoffs with higher specificity and lower sensitivity may be valuable, to prevent flooding of the more limited autism diagnostic services for adults.
In a clinically referred population, there is a need for a short autism screening tool to help clinicians easily identify whether an individual should be referred for a comprehensive autism assessment. Toward this, the 10-item version of the AQ has been offerred by Allison et al. (2012). The AQ-10 is comprised of the two most discriminative items from each of the AQ’s five theoretical subscales. The National Institute for Health and Care Excellence (NICE; 2012) guideline #142 recommended administering the AQ-10 for individual adults who may be autistic. Some studies validating the AQ-10 against clinical diagnosis have suggested that it performs well in identifying autistic individuals (Allison et al., 2012; Booth et al., 2013), while others suggested it lacks specificity (Ashwood et al., 2016; see Wigham et al., 2019; Sizoo et al., 2015, for a review). However, these reports were based on Diagnostic and Statistical Manual of Mental Disorders (4th ed., text rev.; DSM-IV-TR) or ICD-10 diagnoses of autism conditions. It has also been suggested that the AQ lacks autistic nuance and that it is centered around one central theory (the extreme male brain) (Kapp et al., 2013).
Several differences were introduced in Diagnostic and Statistical Manual of Mental Disorders (5th ed.; DSM-5) diagnostic criteria for autism (APA, 2013), compared to those that characterized pervasive developmental disorders (PDD) in DSM-IV-TR (APA, 2000). Some of these include (1) merging the social and communication symptom domains in DSM-IV-TR into a SC domain in DSM-5; (2) requiring both SC deficits 1 and restricted, repetitive behavior (RRB) for an autism diagnosis; and (3) removal of diagnostic features such as delays in imaginative play or preoccupation with parts of objects, and the introduction of new features, such as sensory hyper-/hypo-sensitivity or sensory preoccupations. These changes may require corresponding adaptations in screening instruments. Some instruments have been revised to be adapted to DSM-5 criteria (Bruni, 2014), but to date, the AQ has not been adapted, either in its full form or in its short form.
This study aimed (1) to examine the psychometric properties of the Hebrew translation of the full AQ (henceforth AQ-50-Heb); (2) to create a short version of the Hebrew AQ (AQ-10-Heb), that fits with the up-to-date diagnostic criteria of the DSM-5; and (3) to examine the appropriate cutoff score of the AQ-50-Heb and AQ-10-Heb questionnaires for screening among clinically referred adults, and to estimate their cutoff in the general population.
Method
Measure
The AQ is a self-report instrument measuring autistic traits. It contains 50 descriptive statements, assessing five different theoretically driven subscales mentioned above. Participants rate their agreement with each statement on a 4-point Likert-type scale, ranging from “definitely agree” to “definitely disagree.” Participants’ ratings on each item are then collapsed to binary scores (agree/disagree) with the autistic trait response scoring 1. The total score range is therefore 0–50.
The AQ was translated and adapted to Hebrew (Milo & Golan, 2006) as part of Baron-Cohen’s book “The Essential Difference” (Baron-Cohen, 2004). The translation was made by a professional translator, assisted by a bilingual clinical psychologist specializing in autism diagnostic assessment, with close support of the original instrument’s author. This published translation has been used in various studies of Hebrew speakers with and without autism (e.g. Globerson et al., 2015; Haruvi-Lamdan et al., 2020; Milshtein et al., 2010; Zukerman et al., 2019). Clinically, the AQ has been used as a screening instrument for incoming clients by several clinical centers specializing in autism diagnostic assessment. Preliminary unpublished findings of its psychometric properties in Israel suggested a cutoff of 22, with sensitivity of 0.73, and specificity of 0.82 (Golan et al., 2009).
Participants and procedure
AQ and demographic data of the autism group were collected from records of adult clients who sought an autism diagnosis from two clinical centers operated by the Association for Children at Risk. These two tertiary centers provide diagnostic assessment services for children and adults with autism. A waiver of consent for this retrospective records review was given by the Ness-Ziona Beer-Yaacov Mental Health Center’s Helsinki Committee (#543). Ninety-three records of participants (24 females) aged 18–53 (M = 26.83 and SD = 8.31) were included in the study. To be included, participants had to have a clinical diagnosis of autism given by a psychiatrist or a clinical psychologist according to DSM-5 criteria, with no comorbid intellectual impairment.
The records showed that 53% of the participants had a previous neurodevelopmental diagnosis (most commonly, ADHD, learning difficulties, or tic disorders), and 41% of the participants had a previous psychiatric diagnosis (most commonly anxiety, depression, or OCD). About 29% of the participants had a previous PDD/autism diagnosis from childhood. Five percent had a sensory/genetic/other medical condition. In terms of education, 28% of the participants in the autism group attended special education settings (either special education schools or a special education class in a regular school) as children. Twelve percent of participants in the autism group had post-high school education.
Females in the autism group did not differ from males on age, birth country, residence type, education, or previous diagnosis, with the exception of a previous diagnosis of autism which was marginally significantly more prevalent in males (31.9%) than in females (12.5%; χ2(1) = 3.40, p = 0.065). The participants’ socio-economic status was medium-high (SES decile M = 7.33 and SD = 1.57).
The typically developing (TD) sample consisted of 147 participants (34 females), aged 17–50 (M = 26.03 and SD = 5.61). TD participants were recruited from the general community through their acquaintance with undergraduate research assistants. An exclusion criterion was having a diagnosis of either autism or a serious mental illness (e.g. schizophrenia). Ethical approval for the TD sample was given by the first author’s Department of Psychology ethics committee. All TD participants provided written informed consent. As shown in Table 1, groups were comparable on age, gender, country of birth, residence area, but differed on education.
Sample characteristics and group differences.
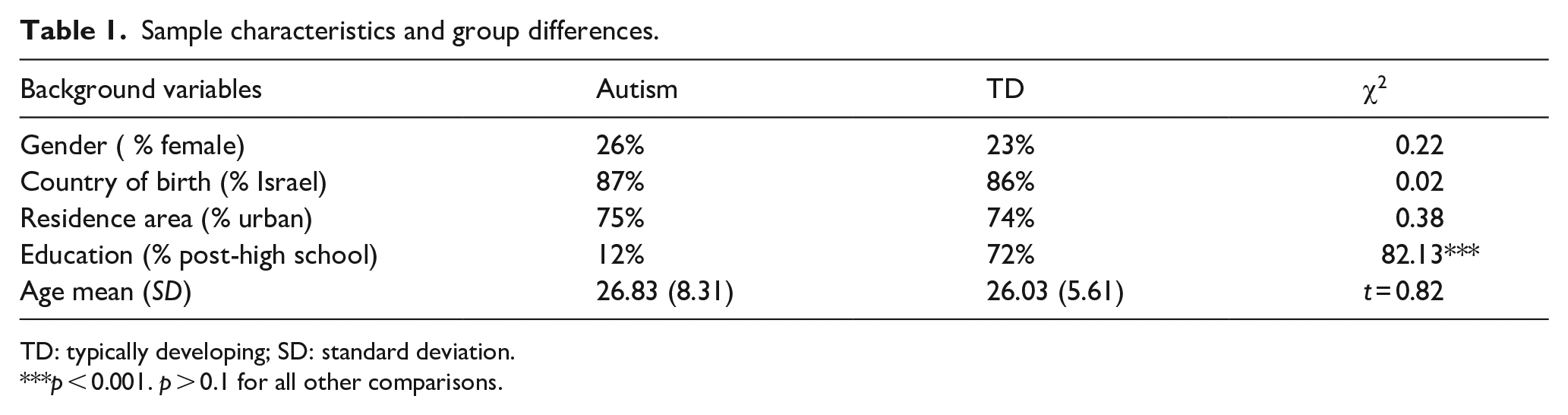
TD: typically developing; SD: standard deviation.
p < 0.001. p > 0.1 for all other comparisons.
Analysis
Power calculation was made with easy ROC software (Goksuluk et al., 2016) using the lowest area under the curve (AUC) of the AQ test (0.65) that was found in the literature (Baghdadli et al., 2017). The estimated sample size was at least 36 participants with autism and 54 with TD.
Receiver operating characteristic (ROC) curve analyses were conducted in SPSS, version 23. ROC analyses were computed separately for the full and the short versions of the AQ-Heb. MedCalc Software (MedCalc Software, Belgium) was used to determine the cutoff for each version, based on its sensitivity, specificity, PPV, NPV, and accuracy in a clinically referred population (i.e. with a prevalence of 70%, according to the clinical centers’ data), and to estimate these cutoffs in the general population (i.e. with a prevalence of 0.49%). Kuder-Richardson 20 (KR-20) was computed for each version to examine internal consistency. Two-way analyses of variance were computed to examine group and gender differences on total AQ scores. Finally, Pearson correlations between total AQ score and age were calculated for the entire sample and separately for each group.
Community involvement
There was no community involvement in this study.
Results
Discriminant power of the AQ-50-Heb
To test the diagnostic validity of the AQ-50-Heb with Israeli adults, a ROC curve analysis was performed (see Figure 1). The results showed that the AQ-50-Heb total score predicted diagnostic outcome, with an AUC of 0.94 (SE = 0.02, 95% CI = 0.91–0.97). As shown in Table 2, a cutoff of 21 seems optimal for clinically referred adults, as it offers high sensitivity (0.90), PPV (0.90), acceptable specificity (0.76), NPV (0.77), and good accuracy (0.86). For screening purposes in the general population a cutoff of 30 was estimated as optimal, with modest sensitivity (0.59), but high specificity (1.00), PPV (1.00), NPV (1.00), and accuracy (1.00). A separate analysis for males and females provided similar results and did not indicate that a gender-specific cutoff is required. An analysis of variance of the AQ-50-Heb total score with group and gender as between group factors yielded a group main effect (F(1,236) = 241.77, p < 0.001), with higher scores for the autism group (M = 31.39 and SD = 8.05), compared to the TD group (M = 16.23 and SD = 5.41), but no significant main effect for gender (males, M = 21.76 and SD = 9.63; females, M = 23.19, SD = 10.64; F(1,236) = 1.21, NS) or a group by gender interaction (F(1,236) = 1.12, NS). In addition, the AQ-50-Heb total score did not correlate with participants’ age either for the entire sample (r = 0.03, NS) or for each group separately (Autism: r = 0.03, NS; TD: r = –0.10, NS). The AQ-50-Heb’s internal consistency calculated using KR-20 was 0.90. The internal consistency of the subscales was estimated at 0.86 (social skill), 0.55 (attention to detail), 0.75 (attention switching), 0.82 (communication), and 0.61 (imagination).
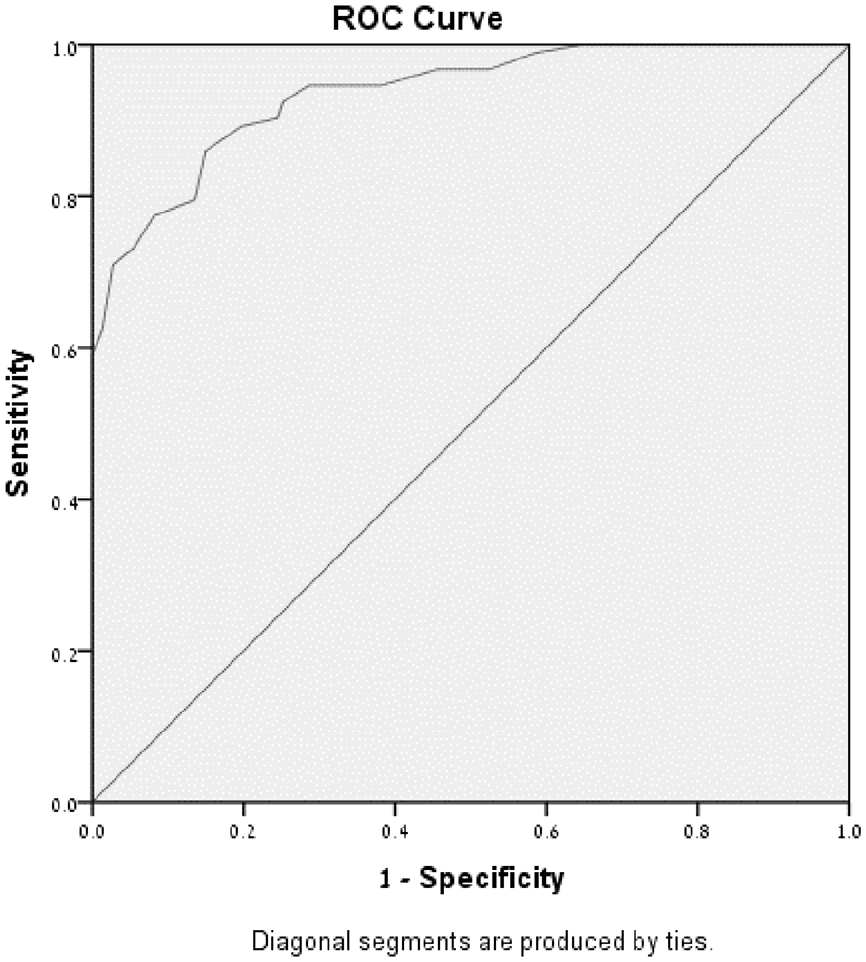
ROC curve of the AQ-50-Heb.
Sensitivity, specificity, PPV, NPV, and accuracy of the AQ-50-Heb.
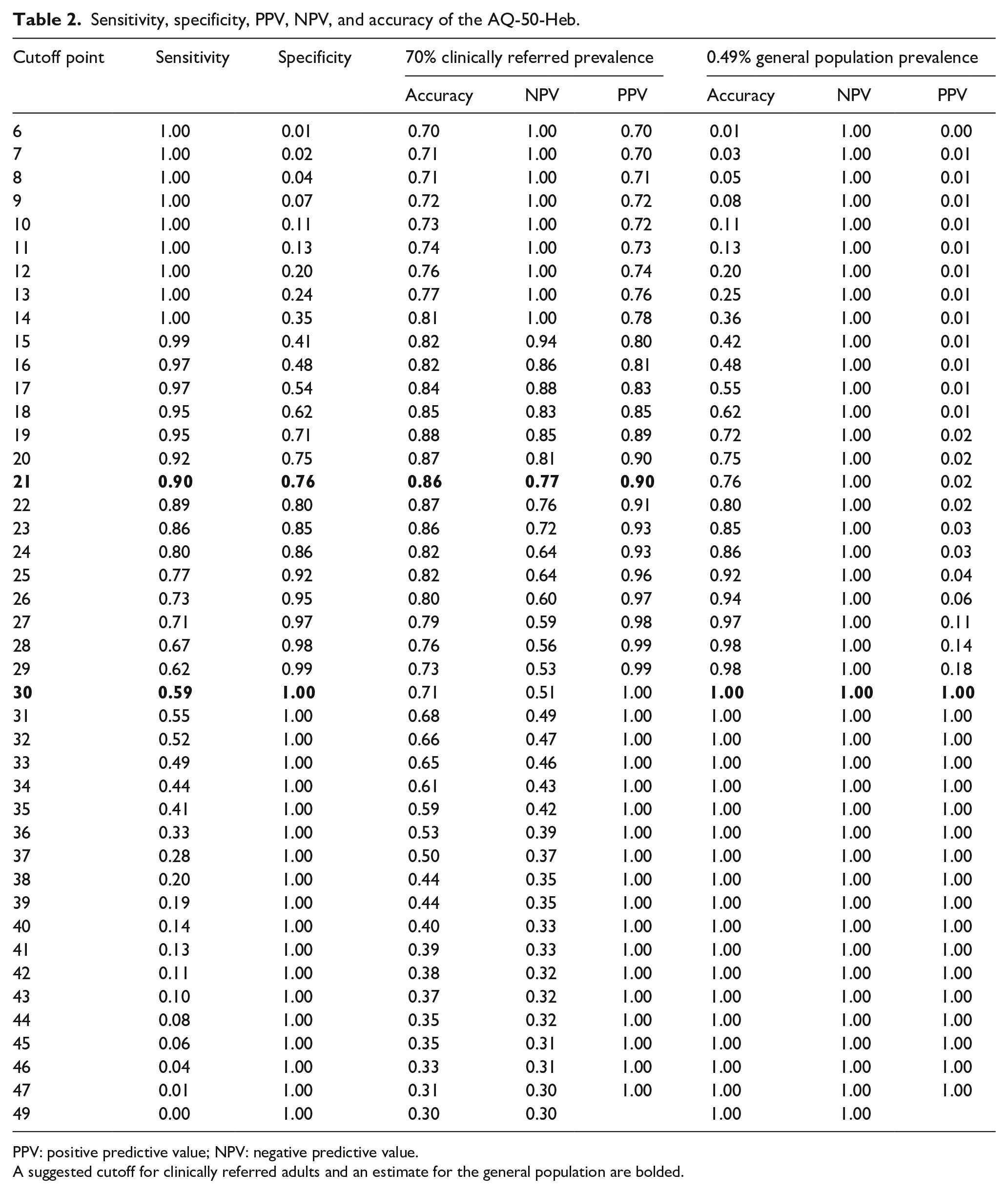
PPV: positive predictive value; NPV: negative predictive value.
A suggested cutoff for clinically referred adults and an estimate for the general population are bolded.
Development of the AQ-10-Heb according to DSM-5 criteria
A panel of 10 independent clinicians (3 psychiatrists and 7 psychologists), experienced in diagnosing autism in children and adults (years of experience: M = 9.55 and SD = 5.43), were asked to classify the 50 AQ items according to the seven diagnostic criteria of autism in DSM-5. For each item, experts were asked to choose the most suitable DSM-5 criterion, or to indicate whether the item could not be associated with any criterion.
A consensus of at least five experts on the classification of an item was required to associate it with the most suitable DSM-5 criterion (p < 0.01, binomial test). Based on these requirements, 10 AQ items were associated with criterion A1 (deficits in social-emotional reciprocity), two items were associated with criterion A2 (deficits in nonverbal communication), ten items were associated with criterion A3 (deficits in developing, maintaining, and understand relationships), nine items were associated with criterion B2 (insistence on sameness, inflexible adherence to routines, or ritualized patterns of verbal or nonverbal behavior), eight items were associated with criterion B3 (highly restricted, fixated interests), and one item was associated with criterion B4 (hyper- or hypo-reactivity to sensory input or unusual interest in sensory aspects). Five AQ items were classified as not relevant to any DSM-5 criterion, and five items did not reach a clear consensus between the experts. Clinician ratings for all AQ items are detailed in Table 3.
Experts’ classification of the AQ items to DSM-5 diagnostic criteria.
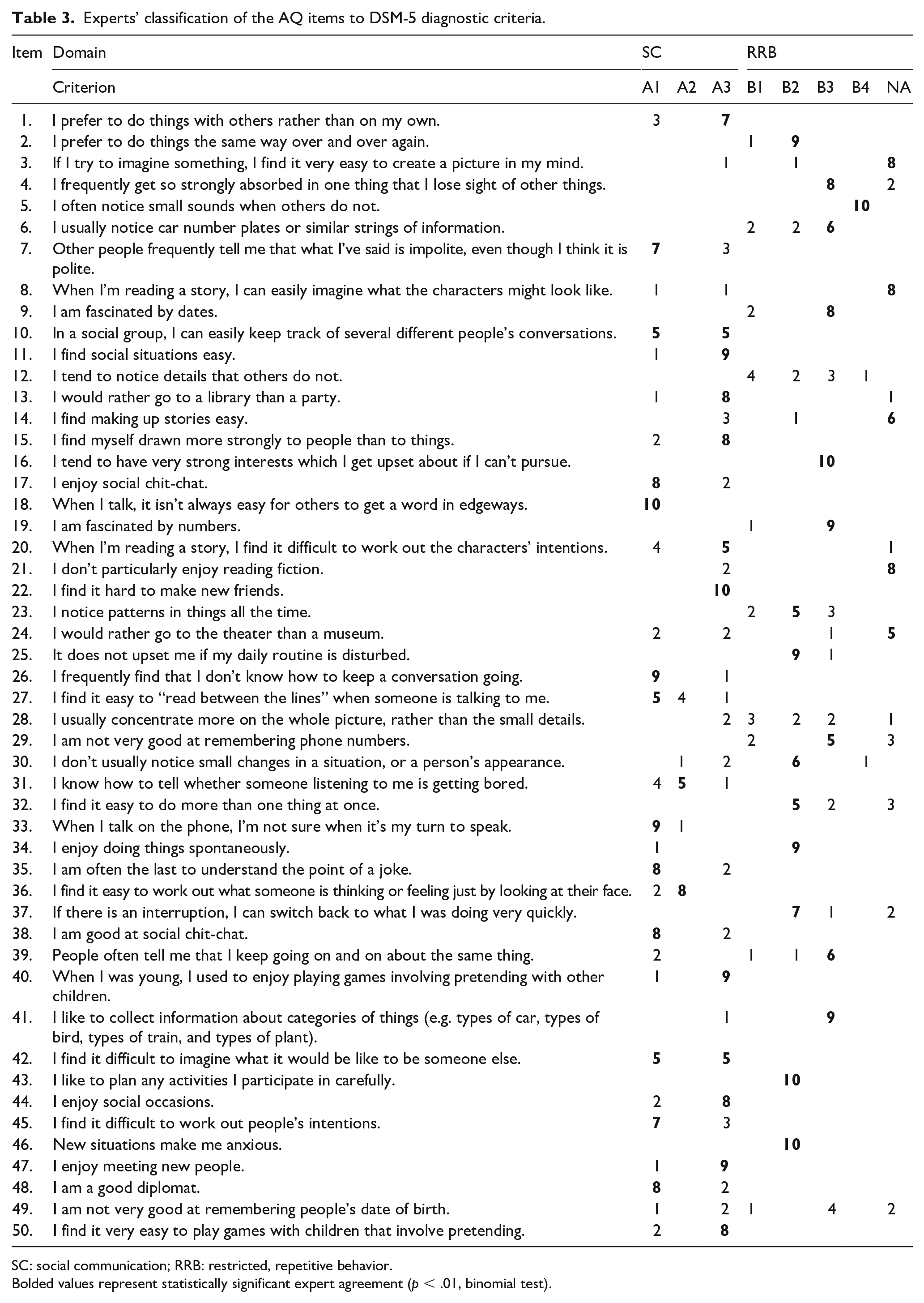
SC: social communication; RRB: restricted, repetitive behavior.
Bolded values represent statistically significant expert agreement (p < .01, binomial test).
In order to select the best items for the AQ-10-Heb, the procedure that Allison et al. used (Allison et al., 2012) was adopted. That is, for each item, the ratio between those with a positive score and the total group size was calculated for each group. Then, the TD group’s ratio was subtracted from the autism group’s ratio. The result was defined as the item’s discrimination index (DI). A DI ranging between 0.3 and 0.7 was deemed acceptable (Gillis et al., 2011). As shown in Table 4, the DI of 29 of the AQ items that were judged by the experts as relevant for DSM-5 fell within this range. Of these, 21 were classified by the experts as SC items and 8 as RRB items.
Selection of the AQ-10-Heb items by DSM-5 domain and DI.
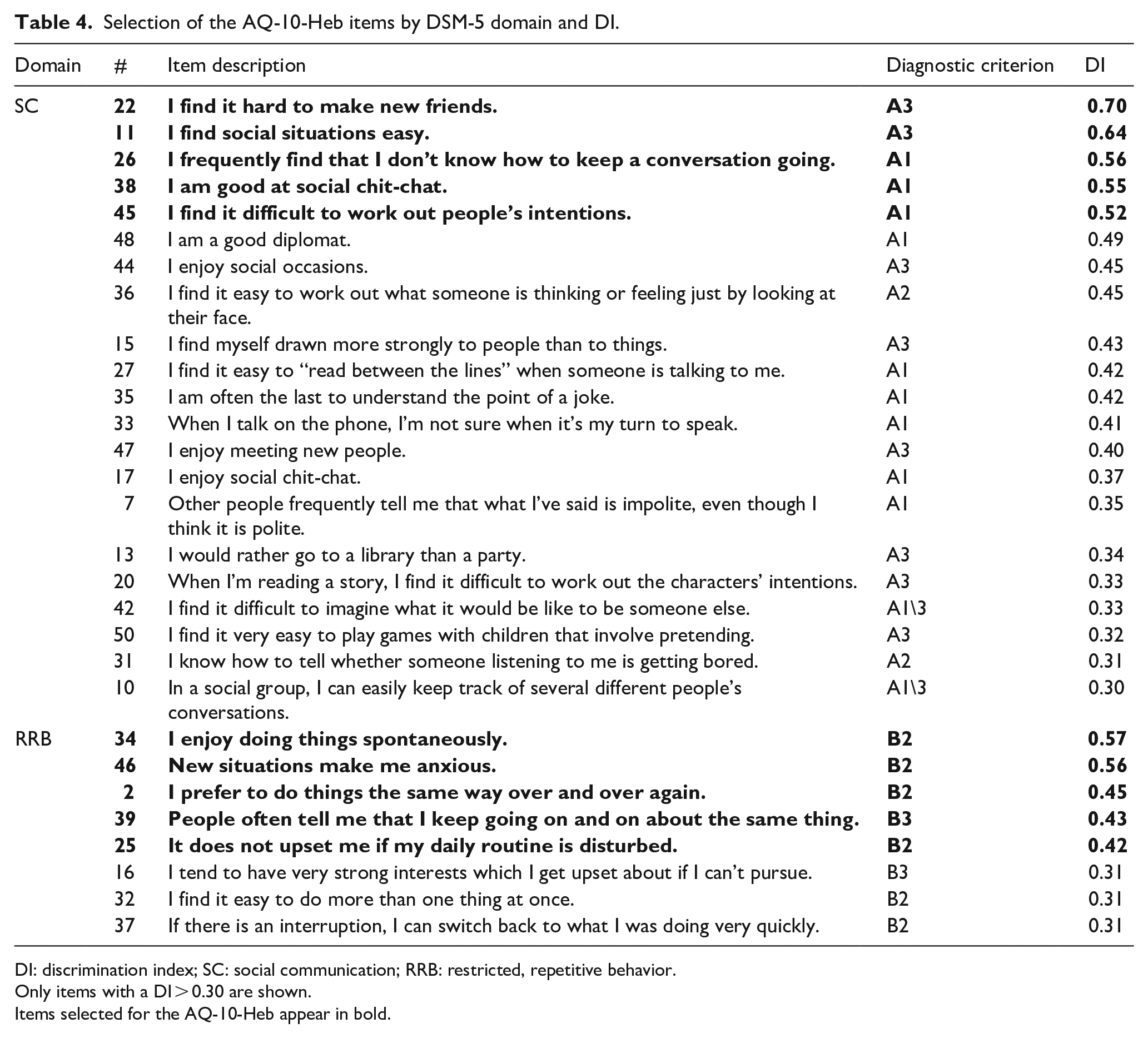
DI: discrimination index; SC: social communication; RRB: restricted, repetitive behavior.
Only items with a DI > 0.30 are shown.
Items selected for the AQ-10-Heb appear in bold.
Since a DSM-5 diagnosis of autism requires both SC difficulties and RRB, items were sorted by their DI in a descending order within the two DSM-5 domains, and the five items with the greatest DI from each domain were selected for the AQ-10-Heb. As shown in Table 4, these items represent DSM-5 criteria A1 (items 26, 38, and 45), A3 (items 11 and 22), B2 (items 2, 25, 34, and 46), and B3 (item 39). Next, AQ-10-Heb scores were computed for all the participants, and a ROC curve analysis was performed (see Figure 2). The results showed that the AQ-10-Heb predicted diagnostic outcome well, with an AUC of 0.95 (SE = 0.02, 95% CI = 0.92–0.98). According to the sensitivity and specificity data presented in Table 5 a cutoff of five may be optimal for clinically referred adults, with high sensitivity (0.90), specificity (0.82), PPV (0.92), NPV (0.78), and accuracy (0.88). An estimate of the cutoff for screening purposes in the general population suggested a cutoff of nine may be optimal, with modest sensitivity (0.53), and excellent specificity (1.00), PPV (1.00), NPV (1.00), and accuracy (1.00). KR-20 used to measure the AQ-10-Heb’s internal consistency was 0.86. Removing any of the items did not increase internal consistency. AQ-50-Heb and AQ-10-Heb scores were positively correlated (r = 0.80).
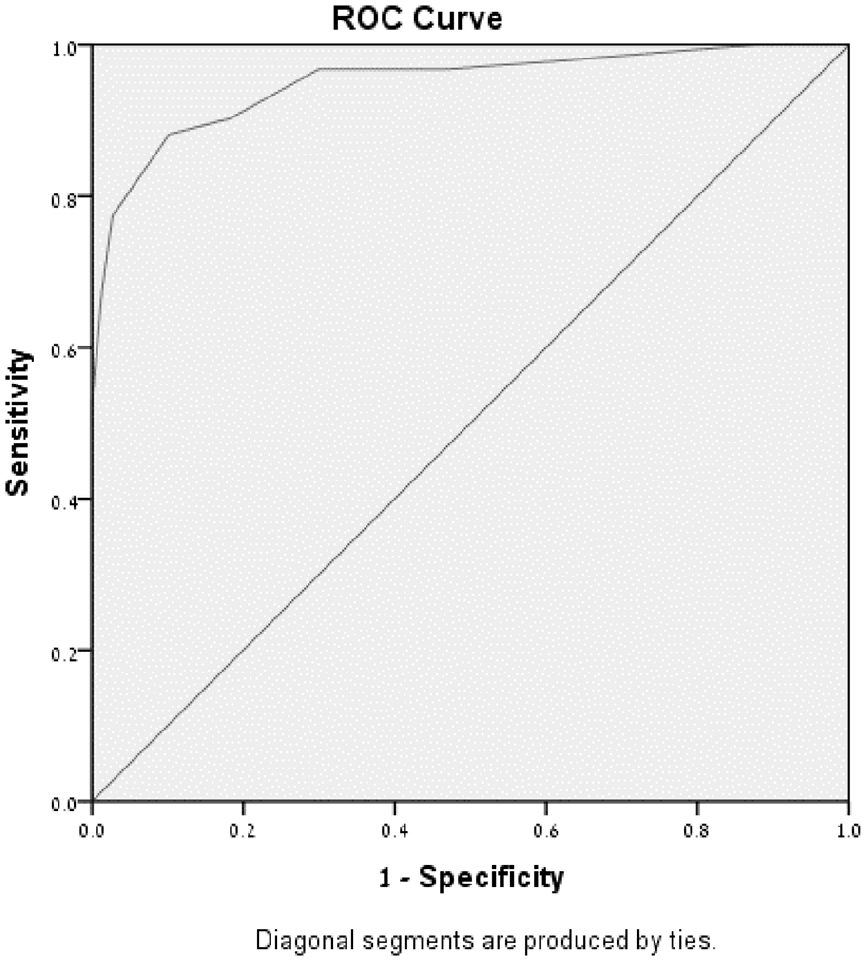
ROC curve of the AQ-10-Heb.
Sensitivity, specificity, PPV, NPV, and accuracy of the AQ-10-Heb.
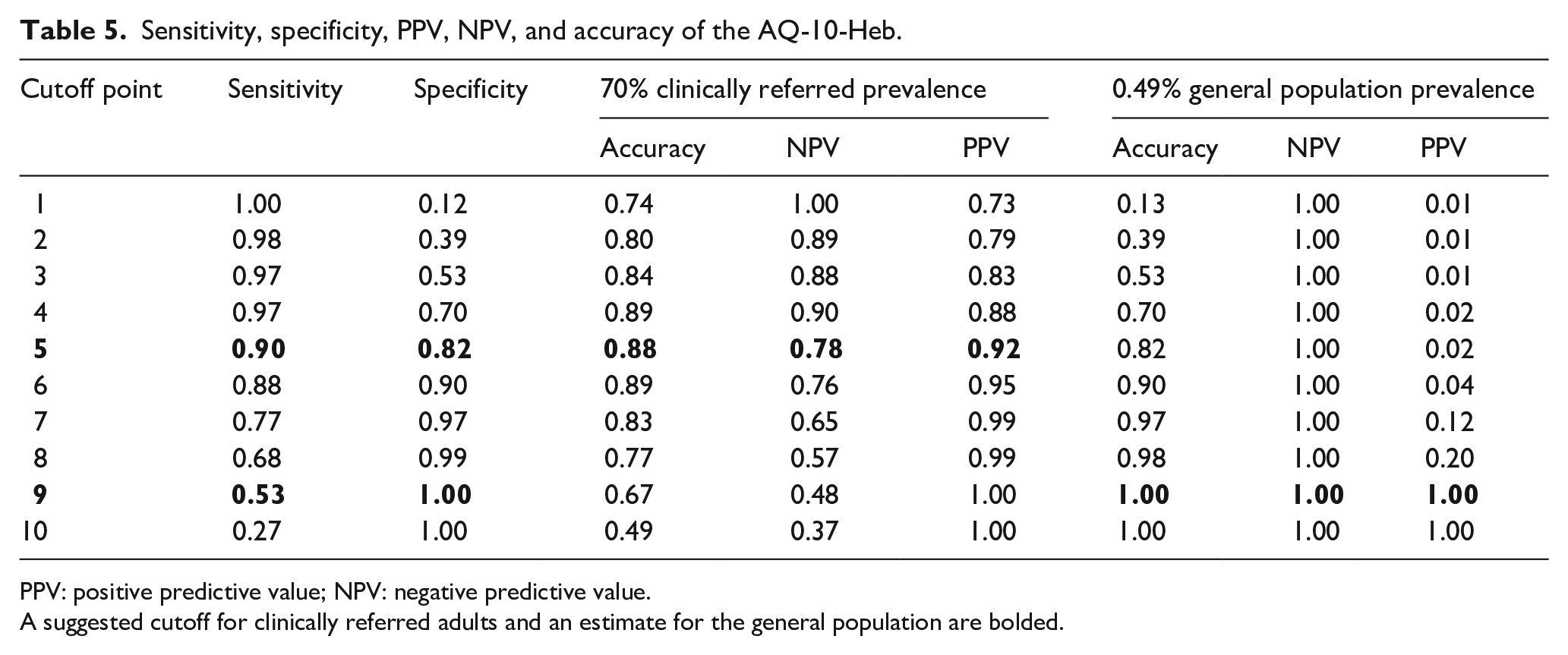
PPV: positive predictive value; NPV: negative predictive value.
A suggested cutoff for clinically referred adults and an estimate for the general population are bolded.
Discussion
This study aimed to examine the psychometric properties of the full AQ as a self-report screener for Hebrew-speaking adults (AQ-50-Heb). The AQ-50-Heb’s properties were examined as a screener for adults clinically referred for an autism diagnostic assessment and were also estimated in the general population. Since the AQ was originally created and validated in relation to the diagnostic criteria of DSM-IV-TR and ICD-10, we also aimed to create a short version of the AQ-50-Heb that fits the up-to-date diagnostic criteria of DSM-5. Toward that aim, a panel of independent clinicians classified the AQ items according to DSM-5 criteria and the most discriminating items from the SC and the RRB domains were selected to create the AQ-10-Heb. This short version was also tested as a screener among clinically referred adults and estimated for the general population.
When screening adults who have already been seen by an unspecialized clinician who wondered about a potential autism diagnosis, screening should consider a cutoff that is sensitive enough (i.e. sensitivity > 0.90) to detect most of the adults who will eventually be diagnosed with autism and to improve the efficiency of tertiary diagnostic centers. Therefore, we have established a cutoff of 21 for clinically referred adults on the AQ-50-Heb. This cutoff allowed for high sensitivity (0.90), PPV (0.90), and good accuracy (0.86), while somewhat compromising specificity (0.76) and NPV (0.77). This suggested cutoff was slightly lower than that of the preliminary Israeli report (Golan et al., 2009) but considerably improved its sensitivity; however, we used a larger sample; and all of our participants were diagnosed according to the DSM-5.
For the AQ-10-Heb, we have set the cutoff for clinically referred adults at five. This cutoff achieved somewhat better results than the full instrument, since alongside its high sensitivity (0.90) and PPV (0.92); it maintained good specificity (0.82) and accuracy (0.88), with lower NPV (0.78). It is important to note that in the clinically referred sample, unlike the general population, the proportion of adults receiving an autism diagnosis was 70% (according to the tertiary clinical centers’ statistics). Similar rates for clinical settings have been reported by Ashwood et al. (2016) and Woodbury-Smith et al. (2005). These rates highlight the importance of sensitivity on the account of specificity and the reasoning for a lower cutoff when using the AQ-10-Heb with clinically referred adults.
When screening in the general population, a cutoff that achieves both a high PPV and NPV as well as maximum accuracy is appropriate. In this manner, it can obtain certainty about the results of each individual’s condition, avoiding many false positives due to the reported prevalence of autism in Israel (0.49; Raz et al., 2015). The AQ-50-Heb general population cutoff was estimated to be 30. We compromised its sensitivity (0.59) to achieve full specificity (1.00), positive (1.00), and negative (1.00) predictive values, as well as accuracy (1.00). This estimated cutoff for the general population was slightly lower than that originally reported in the United Kingdom, with somewhat better PPV and NPV. For the AQ-10-Heb, a general population estimated cutoff of nine appeared to be optimal, with lower sensitivity (0.53), alongside full specificity (1.00), PPV (1.00), NPV (1.00), and accuracy (1.00). These estimated cutoffs require a proper examination in a large random Israeli sample. Following such an examination, the AQ could be used by general population establishments, such as the military system (which is mandatory in Israel) to detect undiagnosed individuals who may need additional attention or relevant accommodations. Notably, prioritizing high specificity in general population screening could help prevent flooding of the limited tertiary diagnostic services for autistic adults.
This study was the first to attempt to classify AQ items according to DSM-5 criteria. The ratings of our panel of experts indicated that 40 out of the 50 items of the AQ could be clearly mapped on to specific DSM-5 criteria: Twenty-two items were classified into the SC domain and 18 items into the RRB domain. The panel could not agree on the mapping of ten of the AQ items (3, 8, 10, 12, 14, 21, 24, 28, 42, and 49) to any of the DSM-5 criteria. Most of these items describe difficulties in imagination. Imagination differences have been historically perceived as an autistic trait (Craig & Baron-Cohen, 1999), while their representation in DSM-5 relates to the use of imagination in social interaction. Thus, AQ items that focus solely on imagination were not classified as relevant in the diagnostic criteria according to DSM-5. In addition, two of the excluded items relate to attention to detail which is described as a strength in autism (Baron-Cohen et al., 2009) but is not represented in DSM-5 criteria.
An examination of the 40 items that mapped clearly on to DSM-5 criteria indicated that the domains are not equally represented. In the SC domain, criterion A1—dealing with deficits in socio-emotional reciprocity and A3—dealing with the attainment, preservation, and understanding of social relationships were widely represented by the AQ. However, representation of criterion A2, which focuses on the expression and the understanding of nonverbal communication, was minimal; only two items were judged as representing this criterion (31 and 36), which relate to recognition and interpretation of nonverbal cues, rather than the ability to express oneself non-verbally. Therefore, evidence for the existence of nonverbal expression difficulties may need to be collected from third parties or from a direct diagnostic observation. In the RRB domain, criterion (B2), addressing inflexibility and need for a routine, and circumscribed interests (B3), are well represented in the AQ. However, according to our panel’s ratings, criterion B1 (relating to stereotypies and repetition) is not represented in the AQ, and criterion B4 (relating to sensory sensitivity and sensory interests) is represented by one item only. These findings suggest that the AQ offers a better representation of SC than of RRB, as previously suggested (Hoekstra et al., 2011). Measuring these traits may require the use of additional questionnaires, such as the sensory perception quotient (Tavassoli et al., 2014) or the repetitive behavior questionnaire (Barrett et al., 2015). Alternatively, a revision of the AQ may be required, to allow for better representation of the currently misrepresented DSM-5 criteria. Including autistic self-advocates as partners in such a revision process may allow for better representation of autistic adults’ experiences and interest in the screening process.
Despite its limited representation of RRB, in our selection of the items for the AQ-10-Heb, we aimed to balance between SC and RRB items, rather than to select the most discriminating items. This decision was made to ensure the AQ-10-Heb enquires about difficulties in both domains, as required by DSM-5. Our findings of an optimal clinically referred cutoff of five suggest this forced selection of items by domains did not reduce the instrument’s psychometric properties and even improved some of its psychometric qualities compared to the full AQ. Notably, for the clinically referred sample, our cutoff for the AQ-10-Heb is slightly lower than that of the original AQ-10 (Allison et al., 2012), which mirrors our findings for the full version of the AQ. It is important to remember that Allison et al. forced a classification that represented each of the five theoretical subsections of the original AQ (Allison et al., 2012), rather than on DSM-5 criteria. Moreover, our AQ-10-Heb findings differ from those of Allison et al. not only in our item selection rationale (AQ categories vs DSM-5 categories), but also culturally (British vs Israeli). Previous work examining cultural differences in personality traits has shown that, compared to British people, Israelis score higher on extraversion and lower on neuroticism (Eysenck & Yanai, 1985). Although these findings are not directly related to autism, they may suggest that in Israel it would take fewer autism traits for one to stand out as socially different. Future studies that examine short versions of the AQ cross-culturally according to DSM-5 criteria are needed.
Limitations and suggestions for future research
The examination of the AQ in Israel relied on its formal translation of 2006. As such, the acceptance and understanding of its items by autistic respondents were not obtained. Since the interpretation of items in a self-report instrument may affect its validity (Cassidy et al., 2018), information about the way items are understood by respondents is needed. Such an examination could also assist in confirming the instrument has been culturally adapted. This should be a focus of future studies examining the Autism-Spectrum Quotient–Hebrew version (AQ-Heb).
Moreover, as a self-report questionnaire, the AQ may miss adults who are unaware of their difficulties, or those who show camouflaging capabilities (Lai et al., 2017). Examining the associations of adults’ self-reports with the reflections of others (e.g., family members) and with clinicians’ ratings on standardized scales may provide further validation for adults’ self-reports. Our findings were limited to adults’ self-report on the AQ and clinicians’ DSM-5 diagnostic decision. Also, the clinicians who gave the diagnosis in the clinical centers were not blind to the AQ score at the time the diagnosis was made. Although their diagnostic assessment was not based on the AQ, it cannot be considered independent of clients’ AQ scores.
Data on participants with autism were collected from two clinics and located in two adjacent areas in the center of Israel. Although adults seeking a diagnosis have arrived from all around the country, a potential bias of the sample was the clients’ socio-economic status, which may have related to the costs of the assessment. Although clients who struggled financially have been offered a discounted assessment, lower SES participants were only partly represented, as were minority groups such as Israeli Arabs, Ultra-Orthodox Jews, or immigrants.
We did not find differences in AQ scores between men and women as has previously been demonstrated (Schuck et al., 2019). This may in part be due to a lack of power as a result of the small number of autistic women (n = 24) whose scores were analyzed. Future research should continue to examine gender differences on AQ scores, based on a larger sample. Noteworthy, in our autism group, fewer females than males had a previous autism diagnosis from childhood. This tendency highlights the importance of sensitive screening in adult females, who may have been missed or misdiagnosed along their childhood and adolescence (Rutherford et al., 2016). Another gender-related limitation lies in the inclusion of only cis-gender participants. Although unintentional, no transgender or gender-queer participants have appeared in our sample and their scoring on the AQ-Heb requires further studies.
Our sample was also limited in its focus mostly on newly diagnosed adults, that is, individuals who have not been diagnosed with autism as children. Future studies should examine differences in AQ and other parameters examined between adults diagnosed in childhood and adults diagnosed in adulthood (Marriage & Wolverton, 2009).
In the present study, clinical usage of the AQ questionnaire is discussed, and it is generally observed that the literature uses binary items for clinical purposes (e.g. Allison et al., 2012; Woodbury-Smith et al., 2005). The entire scale may be helpful in future studies examining the prevalence of autistic traits in the Israeli population.
In addition, the study is limited by the fact that most of the measures are based on sensitivity and specificity, so caution should be used when interpreting the results for applications other than screening.
The mapping of the AQ-50-Heb items onto DSM-5 SC and RRB domains for creation of the AQ-10-Heb was solely based on the ratings of our panel of clinicians. A future examination of the items autistic adults find most suitable may be beneficial. In addition, future studies employing a larger sample should examine the factor structure of both versions of the AQ-Heb. Finally, since the AQ-10-Heb was derived from the same sample in which the AQ-50-Heb was measured, a future study should examine these measures in separate, non-overlapping, independent samples, to avoid circularity.
Conclusion
We conclude that the AQ-50-Heb and its short DSM-5 adapted AQ-10-Heb version can be effectively used to help screen for autism in adults who were clinically referred for an autism diagnosis. Further testing in a large random sample is required to conclude about general population screening. Since the AQ-10-Heb represents four of the seven DSM-5 criteria for ASD, additional instruments may be needed to complement the clinical picture.
Supplemental Material
sj-pdf-1-aut-10.1177_13623613221117020 – Supplemental material for The Autism-Spectrum Quotient–Hebrew version: Psychometric properties of a full and a short form, adapted for DSM-5
Supplemental material, sj-pdf-1-aut-10.1177_13623613221117020 for The Autism-Spectrum Quotient–Hebrew version: Psychometric properties of a full and a short form, adapted for DSM-5 by Ofer Golan, Michael Terner, Sandra Israel-Yaacov, Carrie Allison and Simon Baron-Cohen in Autism
Footnotes
Acknowledgements
The authors wish to thank the Autism Research and Treatment Center, association for children at risk, for allowing access to their clinics’ records, and for their support throughout this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Michael Terner was supported by Bar-Ilan University president’s scholarship.
Ethical approval
A waiver of consent was granted by the Ness-Ziona Beer-Yaacov Mental Health Center’s Helsinki Committee (#543) for the retrospective review of records in the autism group. Ethical approval for the TD group was given by the last author’s Department of Psychology ethics committee. All TD participants provided written informed consent.
Supplemental material
Supplemental material for this article is available online.
Notes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.