
Abstract
The stressors autistic individuals encounter and experience as traumatic may vary from non-autistics. We conducted a qualitative study to identify potential sources of trauma for autistic individuals and evaluate correspondence with a standard measure. We enrolled autistic adults (N = 14) and caregivers (N= 15) with varied adversities, levels of functioning, and socio-demographics. Participants completed standard measures of autism, traumatic exposures and stress, and qualitative interviews, which were submitted to thematic analysis. A wide range of experiences were described as traumatic. Whereas some reflected traditional traumas (e.g. maltreatment) and forms of social marginalization, others reflected conflicts between autistic characteristics and the environment (e.g. sensory trauma). All adults and caregivers described sources of trauma in interviews not captured by standardized measures. Varied stressful experiences, many not detected by a standardized measure, may have a traumatic effect on autistic individuals. Whereas some reflect commonly recognized trauma sources, others may reflect particular vulnerabilities for autistic individuals. Results have implications for assessing traumatic events and understanding their contribution to mental health inequities in the autistic population.
Lay abstract
The stressors autistic individuals encounter and experience as traumatic may vary from those not on the spectrum and typically measured. We conducted in-depth interviews with autistic adults and caregivers of children and adults on the spectrum to identify potential sources of trauma for autistic individuals and evaluate the ability of a standard trauma measure to capture those experiences. Fourteen autistic adults and 15 caregivers with varied backgrounds, clinical profiles, and histories of adversity were interviewed. Participants also completed standard measures of autism, traumatic exposures, and stress. Interviews were analyzed to record both traditional sources of trauma, for comparison with the standard measure, and distinct sources, described as traumatic only in the narratives of participants. Participants described varied experiences as traumatic. Whereas some reflected traditional traumas (e.g. maltreatment) and forms of social marginalization, others reflected conflicts between autistic characteristics and the environment (e.g. sensory trauma). All adults and most caregivers described sources of trauma in interviews not reported on the standard measure. Results have implications for assessing traumatic events in autism and for understanding their contribution to the mental health of this group.
Trauma, though often a diagnostic term (i.e. an event designated to cause –stress disorder post-traumatic stress disorder (PTSD) in diagnostic manuals), can also be defined more broadly as an event or circumstance that is experienced as physically or emotionally harmful or life-threatening and has lasting adverse effects on functioning and well-being (Substance Abuse and Mental Health Services Administration (SAMHSA), 2014). This definition underscores that trauma often encompasses a wider range of outcomes than PTSD alone (Cohen et al., 2010) and results not only from an experience, but also from one’s appraisal of and ability to cope with that experience. There is thus strong rationale to examine individual narratives regarding trauma sources in an open-ended manner (i.e. qualitative inquiry) to inform the design and interpretation of more “top-down,” quantitative investigations. This may be particularly true for autistic individuals, whose experiences, appraisals, and coping may vary from non-autistics (Haruvi-Lamdan et al., 2018; Kerns et al., 2015).
Autistic characteristics may influence the experience of trauma at multiple levels, altering not only the rate of potentially traumatic events (PTEs) but also the range of experiences appraised as traumatic (Haruvi-Lamdan et al., 2018; Hoover, 2015; Kerns et al., 2015; Rumball et al., 2020). In support of these theories, studies suggest not only increased rates of PTE among autistic individuals but also enhanced vulnerability to PTSD (Berg et al., 2016; Golan et al., 2021; Haruvi-Lamdan et al., 2020; McDonnell et al., 2019; Rumball, Brook, et al., 2021). Various adversities are also implicated in the prevalent mental health concerns observed among autistic individuals (Dell’Osso et al., 2019; Kerns et al., 2017, 2021; Rumball, Antal, et al., 2021; Taylor & Gotham, 2016), and recent studies suggest PTSD may develop in this population in response to a broad range of experiences, including bullying, psychological “breakdowns,” unexpected sounds, misunderstandings, and life transitions (Kildahl et al., 2020; Rumball et al., 2020).
Nonetheless, research has relied upon measures developed for non-autistics (Rumball, 2019). Such measures may omit the adversities experienced as most traumatic by those on the spectrum and impinge our ability to identify the full breadth of experiences that contribute to poor health outcomes in autism, including but not limited to PTSD. As such, we conducted a qualitative study with autistic adults and caregivers to explore potential sources of trauma for autistic individuals. We also examined the congruence between qualitative findings and the frequency of PTE reported on a standard questionnaire. An ultimate goal was to develop an inclusive list of PTE, grounded in the personal accounts of autistic adults and caregivers, to ensure that hypotheses and measures utilized in future quantitative studies and ultimately clinical practice are appropriately tailored to the autistic population, informed by their priorities and equipped to evaluate the full range of events that may have a traumatic impact.
Method
Methods and findings are reported per the Consolidated Criteria for Reporting Qualitative Research (COREQ; Tong et al., 2007).
Participants
We used stratified purposeful sampling to enroll 14 autistic adults and 15 caregivers (Tables 1 and 2) with varied traumatic experiences, functional abilities, and socio-demographics. Thematic saturation (defined as the point at which no new themes emerged from two subsequent interviews) was achieved after 17 interviews (8 adults and 9 parents); however, 12 additional interviews were conducted to ensure diverse perspectives. No eligible participants withdrew or refused participation. Participants were required to be 18–70 years old, fluent in written or spoken English, and US residents. Autistic adults were required to have a self-reported, community diagnosis of autism and to have experienced a significant stressor that continued to consistently and negatively impact their health or well-being for a month or more after the stressor occurred (per self-report). Participating caregivers were required to be the adoptive or biological parent of a child or adult meeting these criteria (per caregiver report). Exclusionary criteria included (1) severe thought disturbance; (2) for autistic adults, scoring below the Ritvo Autism and Asperger Diagnostic Scale–Revised Screen (RAADS-14; Eriksson et al., 2013) clinical cut-off or, for caregivers, the identified child scoring below the Social Communication Questionnaire (SCQ; Rutter et al., 2003) clinical cut-off. We recruited participants via flyers to local and national autism-related organizations, professional contacts, and word of mouth. The interviewer had no prior relationships with all participants with the exception of one caregiver, who participated in a prior study. Selection of caregivers aimed to ensure experiences of young children and individuals with communication impairments were represented.
Characteristics of autistic adults (N = 14).
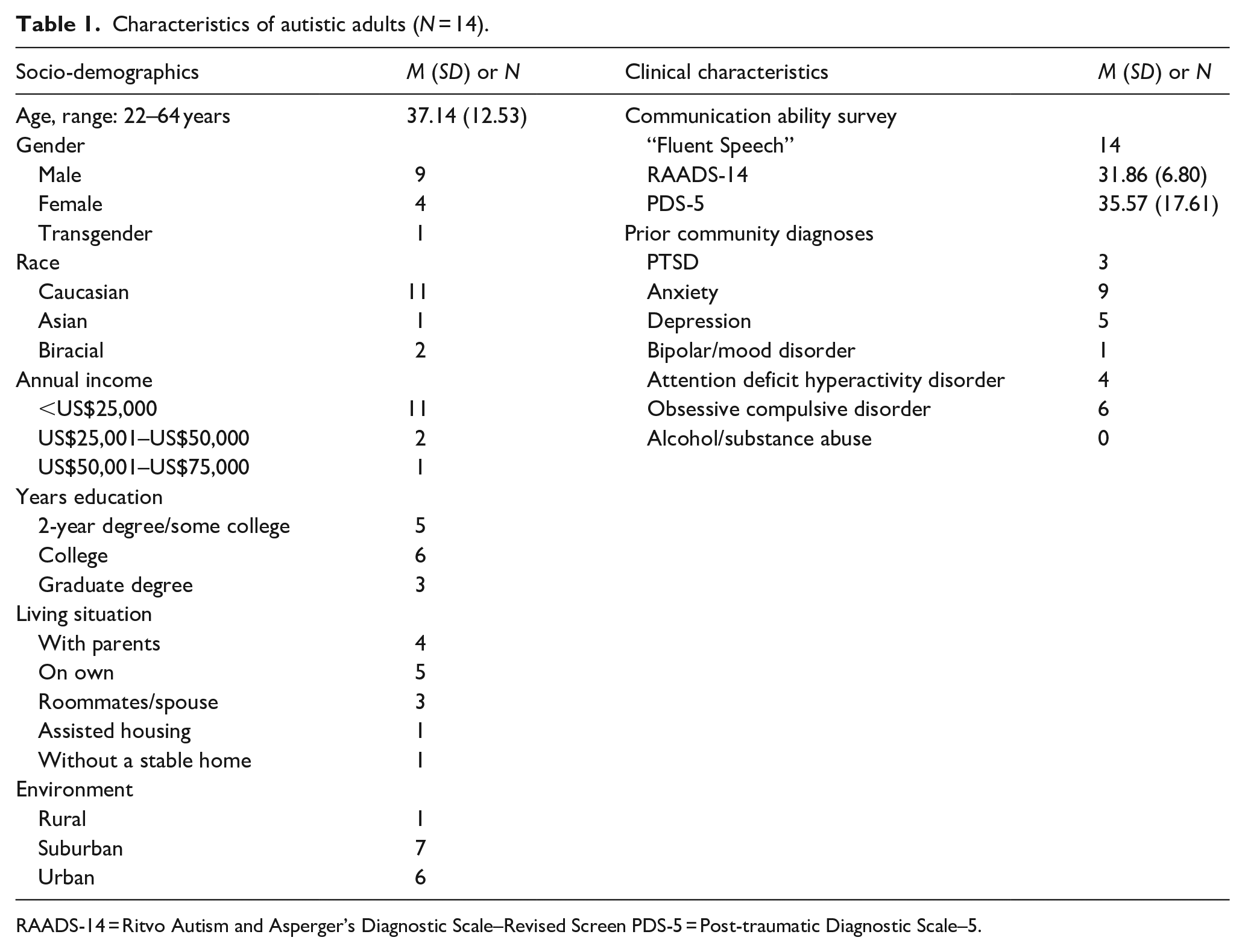
RAADS-14 = Ritvo Autism and Asperger’s Diagnostic Scale–Revised Screen PDS-5 = Post-traumatic Diagnostic Scale–5.
Characteristics of parent participants and their autistic children (N = 15).
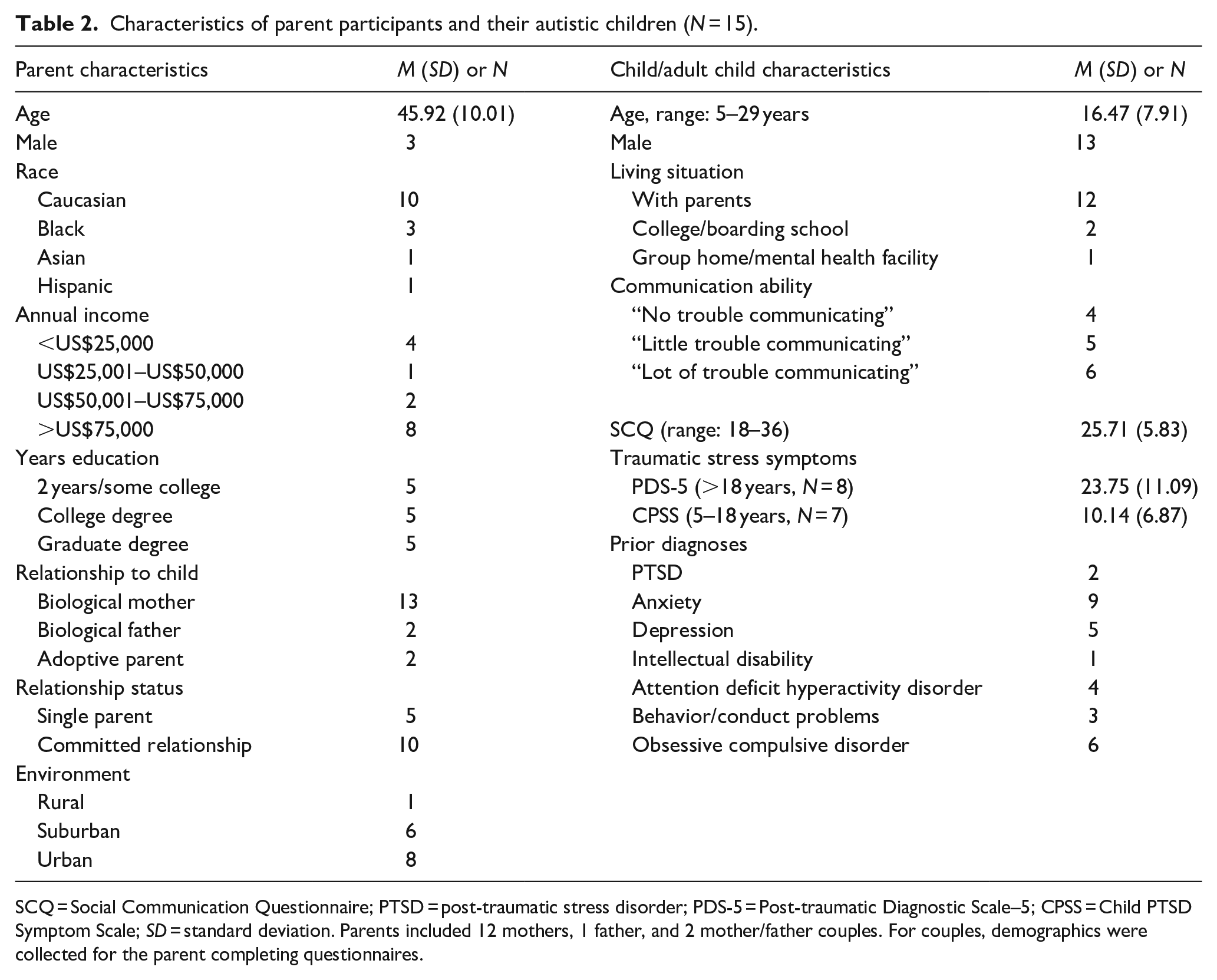
SCQ = Social Communication Questionnaire; PTSD = post-traumatic stress disorder; PDS-5 = Post-traumatic Diagnostic Scale–5; CPSS = Child PTSD Symptom Scale; SD = standard deviation. Parents included 12 mothers, 1 father, and 2 mother/father couples. For couples, demographics were collected for the parent completing questionnaires.
Procedures
This study was approved by the Drexel University Institutional Review Board. Participants provided informed consent, which included a description of study aims, planned questions, questionnaires, and the background and credentials of the principal investigator (PI), a Caucasian, female, and clinical psychologist with expertise in stress-related disorders in autism. Steps to recognize and offset researcher positionality and bias were taken throughout. The qualitative interview guide, though drafted by the PI, was piloted and revised with input from caregivers, autistic adults and researchers (study co-authors) with diverse expertise (autism, childhood trauma, and qualitative research), and training (social work, epidemiology, sociology, psychology, and psychiatry) to balance potential PI assumptions. All interviews were conducted and audio-recorded by the PI, but participation occurred, per participant preference, in-person at the research site (n = 13), by phone (n = 15), or by email (n = 1) to enhance participant comfort and empowerment. To enhance validity, field notes were recorded and interpretations shared with participants during interviews to clarify and confirm meaning.
To characterize the sample, participants completed several questionnaires prior to the interviews, including a survey of socio-demographics and communication ability and a traumatic events checklist, the Trauma History Questionnaire (THQ; Berkowitz et al., 2011; Stover et al., 2010). Participants also completed a standardized measure of traumatic stress symptoms, either the PTSD Diagnostic Scale (PDS-5) for adults or Child PTSD Symptom Scale (CPSS) for children. Both have demonstrated reliability and validity in individuals exposed to trauma, though not autistic samples specifically (Foa et al., 2001, 2016). Each interview was 60–90 min in length. Participants were given the SAMHSA (2014) trauma definition: “Psychologists define trauma as a response to an experience that overwhelms a person’s ability to cope and has a lasting, negative effect on his or her physical, social or emotional well-being.” They were asked to summarize this definition (to check comprehension) and describe events or circumstances they viewed as traumatic given this definition (“Are there any events or experiences in your childhood that may have been traumatic?” see Supplemental Appendix A). Participants received a gift card for their time and contributions.
Data analysis
Qualitative
Interviews were transcribed verbatim from audio-recordings and textually analyzed using NVivo 12. We conducted a six-step reflexive thematic analysis, using a realist framework and an integration of inductive and deductive approaches (Braun & Clarke, 2006, 2019): (1) data familiarization, (2) coding, (3) initial theme generation, (4) theme review, (5) theme definition/naming, and (6) writing of results. We identified semantic themes in the dataset and categorized them where appropriate into logical groupings related to known sources of trauma. These theory-based, deductive codes were based on the interview guide, THQ, and research literature. Inductive themes (e.g. novel trauma sources) were identified via “bottom up” coding (Lofland et al., 2006). To monitor and offset PI positionality, both the PI and two other analysts with different expertise (one masters and one doctoral student with basic autism training) were responsible for data familiarization and the generation of codes and initial themes. This began with line-by-line open coding and group discussion of four transcripts (two parent and two adult), followed by a review and revision of codes and themes via focused coding (e.g. applying formulated codes to transcripts) of original and four new transcripts (two parent and two adult). The coding scheme was documented in NVivo and applied to all remaining transcripts by two to three analysts, whom met regularly to ensure consistent code application and reconcile inconsistencies, review, and refine theme definitions and names. Finally, theme names, definitions, and a thematic map were presented to, reviewed, and refined with our multidisciplinary co-authors, consistent with a recursive, reflexive process.
Mixed-method analyses
We compared univariate frequencies for each THQ item, as reported within the THQ and qualitative interviews.
Community involvement
Community members provided letters of support to the grant agency and offered input on initial versions of the interview guide and study protocol.
Results
Participant characteristics
Autistic adults (Table 1) reported varied educational levels and living arrangements. They were predominantly Caucasian with annual incomes <US$25,000. The majority (n = 10; 71%) exceeded the clinical cut-off for PTSD on the PDS. Only three reported a prior PTSD diagnosis, a pattern also observed by Rumball, Antal, et al. (2021). Caregivers (Table 2) were more racially and socioeconomically diverse. Parents reported a prior diagnosis of PTSD in two children, although four exceeded the CPSS cut-off; six caregivers (40%) reported their child had “a lot of trouble communicating.”
Mixed-method analysis
Participants reported a range of 3–17 PTEs on the THQ (M = 9.08, SD = 4.15; Table 3). Bullying, physical abuse, emotional abuse, and “other traumas” were most frequently endorsed and described as trauma sources in qualitative interviews. Bullying and emotional abuse were the most frequently endorsed PTEs among children with communication challenges. Notably, 71% of adults and 47% of caregivers endorsed an “other trauma” on the THQ; 100% of adults and caregivers described sources of trauma in interviews not captured by the THQ.
Frequencies of PTEs (per THQ and qualitative interviews).
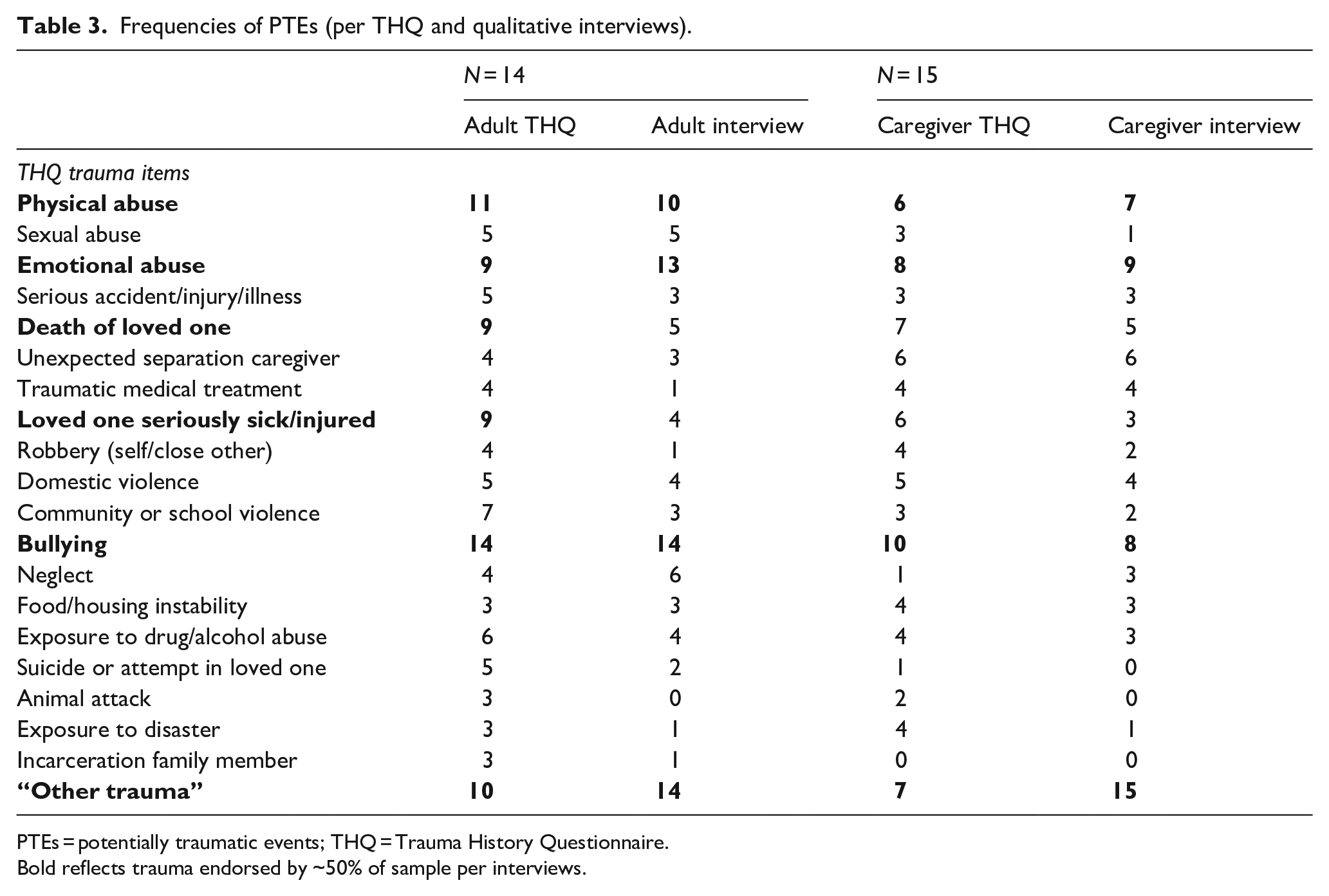
PTEs = potentially traumatic events; THQ = Trauma History Questionnaire.
Bold reflects trauma endorsed by ~50% of sample per interviews.
Qualitative analysis
Qualitative data provided insight into the sources of “other trauma” reported on the THQ (Table 4). Social exclusion and traumatic incongruities were the most common inductive themes, including among participants with communication challenges. Alternative names are used for quotes to maintain confidentiality.
Themes/subthemes with quotations and frequencies.
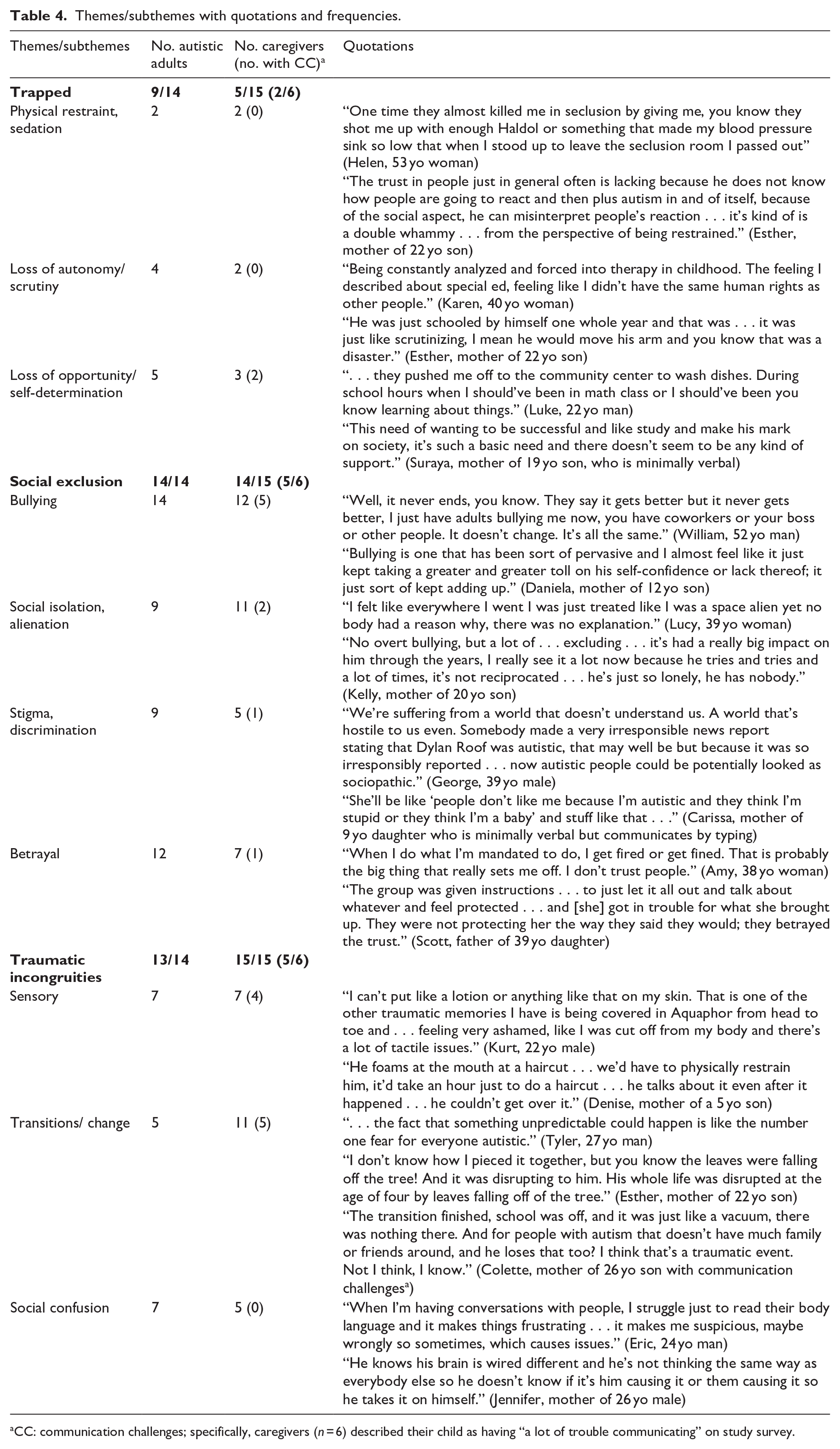
CC: communication challenges; specifically, caregivers (n = 6) described their child as having “a lot of trouble communicating” on study survey.
Trapped
Sources of trauma, described by both adults and caregivers, included being physically or psychologically trapped (theme). This theme comprised physical restraint and sedation (subtheme)—being physically (e.g. held down) or pharmacologically restrained via sedatives, mood stabilizers, or anti-psychotics. Participants noted that for autistic individuals these experiences may be particularly traumatic due to challenges predicting the behavior of others, such as when and why restraint/sedation would be used.
Psychological forms of entrapment were also described and included the loss of autonomy and constant scrutiny (subtheme)—for example, placement in institutions, where adults reported being “trapped” and “helpless,” or overly restrictive learning or therapeutic environments, in which they felt intensely monitored and controlled. Adults and caregivers described enhanced attention to and management of quotidian behaviors in autistic youth, for example, restricting the autistic child’s movements (e.g. ability to travel between classes independently, movement of body), basic decisions (e.g. when/where to eat), or ability to converse with others (e.g. forced seclusion). Traumatic restriction was also described as arising from diminished self-determination and opportunity (subtheme). Autistic adults described being blocked from opportunities for learning, development, and self-actualization in educational and therapeutic environments. This often occurred due to segregated schooling in which academic goals were inappropriately lowered or via prolonged institutionalization, during which necessary life and socialization skills were never mastered and opportunities for future autonomy and well-being derailed. Chronic, diminished expectations for the future and for an equal quality of life were also described and related to a dearth of employment opportunities, or appropriate education, vocational training, housing and other social services for autistic individuals, particularly those without intellectual disabilities.
In sum, a source of trauma, beginning in childhood, born out in varied scenarios and frequently reported by both adults and caregivers, related to feeling physically and psychologically restricted and, at a meta-level, socially stymied—prevented by society from being able to pursue a full life.
Social exclusion
Trauma was also attributed to different forms of social exclusion (theme), that is, being kept apart from others or thwarted social belonging. Though the THQ assesses bullying, we describe bullying here as well given its relevance to the social exclusion theme. Bullying (subtheme) was described as chronic, sometimes seemingly incessant and inescapable. This theme included emotional (e.g. teasing), physical and interpersonal (e.g. intimidation) aggression by peers. Parents noted social perception deficits could also lead their children to perceive bullying in nonaggressive encounters, compounding the issue. This ambiguity and heightened sensitivity to bullying was reported by autistic adults (e.g. “I always had the sneaking suspicion I was being bullied but I never knew who,” Jude, 27-year-old man), who also noted that the severity and impact of bullying was often underestimated by others due to a tendency for emotional difficulties to be viewed as innate in autism. Parents described feelings of powerlessness to end bullying or adequately protect their children; this feeling of powerlessness to escape bullying was echoed by autistic adults.
Participants also reported social isolation and alienation (subtheme). This theme, though often related to bullying encounters, transcended them, reflecting a prevailing feeling of social disconnectedness, difference, and isolation (e.g. “even if the bullying stopped I couldn’t be friends with these girls . . ..” Lucy, 39-year-old woman). Autistic adults and caregivers described subtle exclusions that cumulatively became traumatic (e.g. being treated like “a space alien” or as if “speaking a foreign language”). Exclusion was described as occurring in childhood, at work, and through social services, where individuals were periodically denied supports due to their autism diagnosis (“I keep falling through every single crack . . . I feel like the world doesn’t care about me.” George, 39-year-old man). George described the long-term impact of his alienation: “I’ve decided it’s easier to be a loner than it is to try and fit in where I don’t belong.”
Direct experiences of stigma and discrimination (subtheme) related to autism (e.g. discriminatory behavior from others following diagnosis disclosure) and, gender and sexuality (e.g. being intentionally misgendered), were also reported within this theme. Caregivers of Black children on the spectrum expressed concerns about their children being dually targeted by police for their race and autistic behavior, which could draw unwanted attention and prevent their children from understanding and safely navigating racially charged interactions.
Traumatic betrayal (subtheme) spanned not being believed or being blamed when reporting maltreatment (e.g. abuse, bullying), to a general perceived lack of support and protection from adults, peers and family. Several autistic adults reported traumatic betrayal within the context of romantic relationships, which they found particularly devastating given their difficulties connecting with others in general. Autistic adults also reported feeling betrayed by people due to a lack of directness and honesty. This form of betrayal often resulted from concrete interpretations by autistic individuals of others’ words. David (37-year-old man) described his mother’s failure to follow through on her word regarding his ability to quit an extracurricular activity as traumatic: “Right there, I lost my trust for what she would say.”
Traumatic incongruities
Per adult and caregiver report, trauma also arose in response to incongruities (theme) between the sensory, social and executive processing style of autistic individuals and the external environment. Participants described certain sensory experiences (subtheme; for example, haircuts, fire alarms, ointment) as causing intense distress, and, in some cases, physical pain and chronic anxiety. Traumas also appeared to stem from autistic children’s particular interpretations of certain phenomena (e.g. leaking roof perceived as preternatural and a drowning threat).
Participants described significant transitions and changes (subtheme) in daily life as trauma sources. Parents noted increases in depression, obsessive compulsive symptoms, aggression, hospitalizations and regressions in self-care coinciding with school transitions, high school graduation, and moves from specialized to mainstream learning. Autistic adults described these transitions as traumatic due to the mismatch of environmental demands with limited coping abilities (e.g. struggles to learn and adjust to new rules, people, social expectations) and resources (e.g. limited access to explicit training and supports to navigate a new environment). Adults and parents also described routine changes (e.g. falling autumn leaves) and unpredictability in day-to-day life as having a traumatic impact, again due to a dearth of both internal (e.g. cognitive flexibility) and external resources (e.g. clear communication, forewarning, social support) to support adaptation.
Finally, participants described trauma related to persistent social confusion (subtheme)—that is, chronic, damaging stress resulting from a reduced ability to understand and predict others’ intentions and actions. This subtheme reflected the confluence of difficulties interpreting social cues with inhospitable social environments, in which direct instructions and clarifications, better suited to autistic processing, were not provided. This confusion was linked to entrenched self-blame, self-doubt, anxiety, paranoia, and exhaustion related to having to communicate with others.
Autism and traditional sources of trauma
Rather than providing a description of all traditionally recognized sources of trauma reported, below we highlight how autism was described to shape these stressors.
Maltreatment
Physical abuse (subtheme) was described within the context of bullying and the use of physical restraints in therapeutic settings as well as in the home, when sensory resistance was brutally ignored (e.g. force feeding child who resists eating specific textures). Adults’ recollections of emotional abuse (subtheme) from caregivers and caretakers (e.g. therapeutic staff, teachers) were vivid and highly specific, consistent with a traumatic reaction. George (39-year-old male) described specific incidents of emotional abuse:
Those were so formative that I can’t wipe them out of my mind. I mean I could write a story about it. I could dictate to you the weather conditions of those days . . . It’s so burned into my memory.
The mother of a young boy who experienced sexual abuse (subtheme) noted another layer of trauma was added by her son’s struggle to communicate, which made interviews with child protective services extremely distressing and counter-productive. Participants also noted that difficulties communicating, a desire to be socially accepted and difficulties reading social cues make autistic children vulnerable to sexual abuse and assault.
Environmental instability
This theme covered instability other than maltreatment in formative relationships in the family and living environment. Housing instability (subtheme) was described by participants who spent time in shelters due to domestic violence and homelessness. Parents highlighted the struggle to establish routine and the sudden, enormous changes to their living situations as some of the more damaging aspects of this trauma. Other challenges noted were the lack of training in autism among shelter staff and limited space in shelters for their child’s self-regulatory behaviors (e.g. jumping), which escalated dramatically following relocation. A mother exposed to domestic violence also noted that she initially resisted moving out of danger due to concerns about losing her son’s intervention team. Another mother described that her son appeared most perturbed by the loss of his cat, his primary source of companionship, who could not accompany them to the shelter.
Autistic adults described trauma related to exposure to extreme mental illness (subtheme), including suicide attempts, violent outbursts, self-harm, delusional thinking, paranoia, stalking, and substance abuse within their families and the limited social networks they were able to establish, all of which added to their feelings of thwarted social connectedness (see social exclusion). Finally, when describing the loss of loved ones (subtheme), caregivers and adults included the traumatic loss of critical support staff due to the end of school, job turn-over, or lost funding.
Injury and illness
Another source of trauma described by adults and caregivers was related to injury/illness (subtheme) that required medical treatment. Even when not life-threatening, illness, injury, and subsequent medical care were described by some as traumatic because of a sensitivity to needles, other sensitivities (bright lights), as well as intolerance of uncertainty.
Discussion
We conducted interviews with autistic adults and caregivers of autistic people to identify potential sources of trauma and evaluate the ability of a standard questionnaire, the THQ, to assess these experiences. Consistent with the Kerns et al. (2015) model, findings suggest trauma may arise for autistic individuals from a combination of autism-specific and traditionally recognized stressors, some but not all of which were represented by the THQ. Consistent with the recommendations of Kildahl et al., (2020), Rumball (2019), Rumball et al., (2020), and Haruvi-Lamdan et al. (2018), these findings suggest a need to adapt current measures and diagnostic criteria to include a broader range of stressors in order to accurately assess, research, and treat traumatic reactions, including, but not limited to PTSD, in the autistic population.
Traditionally assessed sources of trauma, captured in both the THQ and qualitative interviews, included physical, sexual, and emotional abuse, neglect, severe injury and illness, and bullying. Findings are consistent with research suggesting autistic children experience these adversities at above-average rates (Hoover & Kaufman, 2018; McDonnell et al., 2019). Qualitative findings shed further light on how autism may shape a child’s vulnerability to these stressors via communication barriers (which may limit abuse allegations and convictions), social naivete, and a desire for social acceptance (which enhance a child’s vulnerability to manipulation) and sensitivities to sensory input and novel experiences (which can exacerbate the shock of injury, illness, and medical treatments), themes also reported by mental health clinicians supporting autistic adults with co-occurring autism and intellectual disability (Kildahl et al., 2020). Interviews also illuminated how autism may shape what aspects of a stressor are experienced as most traumatic; for example, a move away from one trauma (abuse) may yield another (change in routine, loss of pet) for someone on the spectrum. Understanding such nuances in how autistic children and adults experience commonly recognized stressors may be critical to ensure that the most seminal aspects of an autistic individual’s trauma are accurately identified and effectively targeted by clinicians (see Peterson et al., 2019).
Another key source of trauma was social exclusion and marginalization. Such experiences are associated with negative psychological and physical outcomes (Heinz et al., 2020; Leigh-Hunt et al., 2017; Williams, 2007), and social stressors have been linked to PTSD specifically in autism (Haruvi-Lamdan et al., 2020). Autistic adults and caregivers identified varied, often compounding forms of exclusion and being socially trapped—via physical restraint, sedation and institutionalization or via disenfranchisement—as sources of trauma that begin in childhood. The “trapped” theme reflected the experience of being limited and restricted by society, such that basic human drives—the drive to excel, prosper, contribute, become autonomous and for many, to connect with others—felt not only out of reach, but purposefully removed from range. Rather than isolated incidents, most participants described repeated experiences of restriction and removal of opportunities and rights that lastingly altered their coping resources and well-being overtime. Findings are consistent with research demonstrating autism is associated with bullying, poor social integration, and minority stress (Botha & Frost, 2020; Howlin, 2013; Roux et al., 2013; Sterzing et al., 2012). These varied, accumulating forms of exclusion and marginalization were among the most prominent themes identified, suggesting they may be key, but understudied contributors to mental health outcomes in autism.
Additional sources of trauma were incongruities between the sensory, executive function and social processing of autistic individuals and their surrounding environment. Haircuts, fire alarms, and dental work, managing changes—from the shifting seasons to moving homes to day-to-day stressors—and the chronic uncertainty and exclusion caused by missing or struggling to understand social cues were described as sources of long-lasting psychological injury. Prior research has identified these challenges as sources of stress and anxiety for autistic individuals with and without intellectual disabilities (Brewin et al., 2019; Groden et al., 2001; Kerns et al., 2021; Kildahl et al., 2020; Rodgers et al., 2016). Our results are consistent in suggesting a traumatic or long-lasting injurious effect of such stressors on the well-being of autistic individuals.
A secondary goal was to evaluate the correspondence between qualitative interviews and the THQ. Many, but not all experiences endorsed on the THQ were described as traumatic in qualitative interviews. Not all adversities are experienced as traumatic (Bonanno, 2005), and our results suggest such resilience or resistance to adversity is also observed in those on the spectrum. Nonetheless, some experiences (e.g. bullying, emotional abuse), when endorsed on the THQ, were universally described as traumatic by participants. Furthermore, most autistic adults and approximately half of caregivers endorsed “other trauma” on the THQ—indicating a trauma not covered by existing items. Moreover, all autistic adults and caregivers reported sources of trauma in interviews not represented by the THQ. Findings underscore the importance of developing tailored tools, better equipped to capture the diverse range of stressors experienced by this population.
Study limitations include reduced gender and racial diversity, which likely restricted our ability to examine the traumas of autistic women, non-binary individuals, and people of color. Our results were also focused on identifying potential sources of trauma for autistic individuals using retrospective reports, which may be subject to recall bias. Thus, the extent to which PTSD and other mental health concerns can be directly attributed to these stressors was not confirmed and should be investigated in future research, akin to Rumball et al. (2020). Finally, we used caregiver interviews to capture the experiences of individuals with communication impairments, an incomplete approach given that child and parent perspectives may be discrepant (Kalvin et al., 2020).
Conclusion
Physical and psychological comorbidities are disproportionately represented among autistic children and adults (Croen et al., 2015; Kerns, Rast, & Shattuck, 2020). There are growing calls for research to consider how adversities and social determinants, such as social status and integration, contribute to these outcomes (Kerns et al., 2015; Shattuck et al., 2020). To be most effective, such research must be informed by an understanding of the full range of stressors that impact the well-being of autistic individuals. The sources of trauma illuminated by this study may be transferable to other cases, but are unlikely to constitute an exhaustive or directly generalizable list since their representation and associated characteristics (i.e. communication ability, socioeconomic status) within the autistic population require quantitative evaluation (our sample was small and purposefully recruited for those with trauma histories). Nonetheless, our findings provide critical information regarding how adversity might be operationalized in future research and practice. Findings suggest that varied forms of exclusion and marginalization may be critical to assess and that facets of the autism phenotype may transform common life events into traumas and shape what aspects of traditionally recognized stressors are experienced as most traumatic. Awareness of these themes may help ensure that the traumatic experiences of autistic individuals are not underestimated in future research or inappropriately discounted in case formulations and the development and application of trauma-focused treatments.
Supplemental Material
sj-docx-1-aut-10.1177_13623613211070637 – Supplemental material for Exploring potential sources of childhood trauma: A qualitative study with autistic adults and caregivers
Supplemental material, sj-docx-1-aut-10.1177_13623613211070637 for Exploring potential sources of childhood trauma: A qualitative study with autistic adults and caregivers by Connor M Kerns, Stephen Lankenau, Paul T Shattuck, Diana L Robins, Craig J Newschaffer and Steven J Berkowitz in Autism
Footnotes
Acknowledgements
The authors would like to acknowledge Chandler Puhy and Chelsea Day for their work coding the data and caregivers of children and adults on the spectrum who shared their experiences and insights to make this research possible.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by the Eunice Kenney Shriver National Institute of Child Health and Human Development (K23HD07274) awarded to C. Kerns.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.