
Abstract
This article explores the motivational factors behind preferences for medical care in the country of residence or the country of origin among EU nationals living in the UK. Undertaking a thematic analysis on a large-N qualitative data set, the article aims to establish a data-driven typology of motivations inductively. This provides an intermediary analysis between qualitative depth and quantitative operationalisability, contributing to the existing literature on healthcare location preferences among transnationally connected social groups. This article finds that preferences for medical care in the country of origin are driven overwhelmingly by quality considerations, while preferences for the UK have more to do with convenience and financing. These perceptions result from negative personal experiences, lack of trust, and often concealed cultural differences, and the analysis identifies various nuances and connections between attitudes that previous in-depth qualitative studies could not systematise.
Introduction
Migration scholars have long been interested in how migrants access and utilise healthcare services (Nagi and Haavio-Mannila, 1980). It has been observed that difficulties in accessing healthcare in their countries of residence often lead migrants to ‘make trips to their homelands for the express purpose of receiving medical services’, what Horton and Cole (2011: 1846) refer to as ‘medical returns’. Recent research agendas have turned to documenting in greater detail the complexity of migrants’ healthcare-seeking behaviour within the broader ‘transnational social spaces’ they inhabit (Villa-Torres et al., 2017). From this socially situated perspective, motivations for ‘medical returns’ go beyond access difficulties and are deeply embedded ‘within individual biographies’ and familial relationships (Osipovič, 2013: 110), marking ‘a more complex cultural bond’ (Hanefeld et al., 2015: 357) and often also fulfilling various social functions not immediately related to healthcare (Horton, 2013).
Against the backdrop of this scholarship, this article examines the reasons why EU ‘migrants’ in the United Kingdom would choose to engage in ‘medical returns’ to their countries of origin. The case in question is a subset of intra-EU mobility, where the majority of those moving between EU member states enjoy widespread social citizenship rights in their countries of residence (Mainil et al., 2013). Despite a burgeoning literature contributing to our understanding of the motivations behind EU migrants’ transnational healthcare practices (Ehata and Seeleib-Kaiser, 2017; Goodwin et al., 2013; Guma, 2018; Legido-Quigleyet al., 2014; Migge and Gilmartin, 2011; Osipovič, 2013; Sime, 2014; Stan, 2015), these rich qualitative studies tend to focus on a relatively small number of cases, which does not allow a systematic overview leading to a more comprehensive typology of preferences and practices such as those identified in respect to broader phenomena of ‘cross-border patient mobility’ (Glinos et al., 2010). Addressing this gap, we aim to identify the factors motivating cross-border mobility or immobility among a relatively large pool of EU migrants and construct a qualitative typology that could be operationalised for quantitative analysis.
Our empirical data originate from an online survey conducted in 2016. The survey sample consisted of 1656 respondents from 10 countries of origin, the majority from Poland (60%), Hungary (8.6%), Portugal (8.5%), Romania (8.3%), and Germany (5.2%) (see Table 2 for details). We focus here particularly on the qualitative answers (N = 511) given to an open-ended survey question. The qualitative richness of the data highlights the distinctive and shared experiences of a wider population than that featured in previous research, thus providing a sense of scale, while the classification of motivations arrived at has already demonstrated its explanatory potential in subsequent statistical testing (Moreh et al., 2018). The main contribution of the article is thus to provide an intermediary analysis between qualitative depth and quantitative operationalisability. Before discussing our methodology and presenting our results in more detail, we briefly review the broader literature dealing with motivations for healthcare-related mobility in the EU, and the UK context in particular.
Intra-European mobility and motivational typologies of transnational healthcare
The EU provides a special institutional context for both transnational migration and what is commonly referred to as ‘medical tourism’ or ‘patient mobility’ (Glinos et al., 2010; Horsfall, 2020; Mainil et al., 2013). While in the wider purview of the latter long-term international migrants are assigned a secondary role as ‘diaspora patients’ (Hanefeld et al., 2015: 357), within the European context they take primacy. As Mainil et al. (2013: 132) point out, EU regulations facilitating access to healthcare across borders mostly target ‘those who become patients while abroad’. The lens of ‘medical tourism’ can also inadvertently mask more strictly migratory phenomena, and Horsfall (2020) shows how the overwhelming majority of medical exits from the UK registered in official statistics are undertaken by non-UK nationals travelling back to their countries of origin, while travel within the EU’s institutional arrangements for cross-border healthcare is rare.
Consequently, the various conceptual and empirical typologies designed to identify and categorise forms of patient mobility within the EU have combined the individual perspective of patients’ motivations with the regulatory frameworks and structural factors that stimulate or hinder such practices (Carrera and Lunt, 2010; Glinos et al., 2010; Hanefeld et al., 2015; Laugesen and Vargas-Bustamante, 2010). Glinos et al. (2010), for instance, have identified the availability (in terms of quantity and type) and affordability of services, patients’ familiarity with the healthcare system, and the latter’s perceived quality as the four main motivational factors and have coupled these with two forms of funding (with and without healthcare cover) to describe the reasons and financing of transnational healthcare choices. Mainil et al. (2013) add to these considerations the importance of distance – geographical, cultural, and even financial – and the level of searching effort required, which, they note, ties into aspects of familiarity and availability. Laugesen and Vargas-Bustamante (2010) have placed more emphasis on the type of medical service sought when distinguishing between ‘primary exits’ (i.e. exiting one’s country of residence because healthcare there is unaffordable), ‘complementary exits’ (seeking services that are not fully covered domestically), ‘duplicative exits’ (for faster or better quality treatment than the domestic offer), and ‘institutionalised exits’ taking place against the formal mobility policies devised primarily within the EU. Hanefeld et al. (2015) have focused on the type of treatment sought from a different angle when distinguishing between travel for ‘fertility’, ‘bariatric’, ‘dental’, ‘cosmetic’, and ‘other’ procedures.
The transnational healthcare practices of intra-EU migrants engaged in ‘medical returns’ sit somewhat uncomfortably within these schemata, although it is not hard to see how many of the motivational factors identified for ‘patient mobility’ in general also apply to migrants returning to their countries of origin for medical treatment. Migge and Gilmartin (2011) set out specifically to test the validity of Glinos et al.’s (2010) typology in respect to recent (mostly EU) migrants in Ireland and concluded that while the motivational framework is generally useful, issues of availability and familiarity require further elaboration to comprehend the complexities of migrants’ medical return practices. The authors argue that while actual barriers to accessing care might still exist for EU migrants, it is ‘perceptions of availability’ shaped by lacking or distorted information that affects migrants’ opinions and decision-making to a greater degree (Migge and Gilmartin, 2011: 1145).
Several studies have identified similar issues in the UK context (Ehata and Seeleib-Kaiser, 2017; Goodwin et al., 2013; Guma, 2018; Osipovič, 2013; Sime, 2014; Troccoli et al., 2021). Their findings show that knowledge gaps and language barriers hinder EU migrants’ access to medical services, leading to negative subjective perceptions and attitudes towards the quality of healthcare in the UK and therefore a preference for medical treatment in the countries of origin (Ehata and Seeleib-Kaiser, 2017; Goodwin et al., 2013; Sime, 2014). These preferences are shaped at the intersection of micro-level interpersonal experiences and macro-level structural factors relating to the institutional characteristics of the British and other European healthcare systems. In respect to the latter, the free movement of people across states with either universal residence-based healthcare systems – such as the UK, Ireland, Finland, Italy or Portugal – or reliant on insurance contributions – like Germany, the Netherlands, Poland, or Romania – further complicates the question of intra-EU migrants’ access, attitudes, and practices of transnational healthcare-seeking (Juravle et al., 2013). While the British National Health Service (NHS) provides free care at the point of use to resident EU nationals, this may not be commonly appreciated by migrants from countries with insurance-based healthcare systems. For instance, Ehata and Seeleib-Kaiser (2017) report how some ‘German participants . . . struggled to believe that they would be able to use the NHS ‘for free’, as they were required to enrol in statutory health insurance schemes in Germany’ (2017: 5). The role of NHS General Practitioners (GPs) as gatekeepers to secondary-care services is also a source of misunderstanding for many migrants who often feel that those services are in effect unavailable to them (Madden et al., 2017). In turn, as Madden et al. (2017: 2) have found, a ‘lack of understanding of the system can lead to dissatisfaction, frustration and distrust in the NHS, and the GP in particular’. On the contrary, intra-EU migrants’ access to social security benefits and free healthcare had become a politically salient topic in the years leading up to the 2016 EU Referendum, with various measures taken by the government to impose access restrictions (Harris, 2016). As part of these measures, healthcare professionals are increasingly tasked with policing the entitlement to free healthcare at the frontline of the system (Department of Health and Social Care, 2017). With the UK having left the EU, such checks are likely to present challenges in the years ahead for those resident EU nationals who obtained the so-called Settled Status in the country but do not possess physical evidence of their rights.
Unfamiliarity and mistrust of the system are often exacerbated by micro-level interactions with healthcare professionals due to language barriers that may result in miscommunications (Gorman and Porteous, 2018; Roberts et al., 2005; Sime, 2014). In a qualitative study of primary care consultations in multilingual settings, Roberts et al. (2005) have found that language and cultural differences caused misunderstandings in 20% of the consultations examined. Gorman and Porteous (2018) have further shown how women are at particular risk, as such misunderstandings may affect their participation in potentially life-changing preventive care initiatives such as cancer screening programmes. Pemberton and Doos (2017) have also noted how language issues have often led to perceptions of being discriminated against. EU migrants with limited English language proficiency are therefore more likely of being either cut out from healthcare or forced to seek care in their countries of origin.
The existing literature does not provide a clear sense of who is more likely to engage in transnational healthcare practices. There is evidence that more recent migrants, the middle-aged, those with limited language abilities, women, and those with lower incomes have reduced levels of trust in the NHS (Pemberton and Isakjee, 2017), which in turn can motivate ‘medical returns’. On the contrary, we know that transnational healthcare practices are often intertwined with social dynamics of ‘status’ positioning and thus tend to involve those with higher incomes (Sime, 2014). As Sime (2014: 91) described, ‘[t]he increased available financial capital of some migrants meant also that they would return to their homeland able to pay for private healthcare, seen as a marker of status, but also as a perceived guarantee of better care’. In any case, the existing qualitative literature agrees that transnational healthcare-seeking is rarely a zero-sum choice, with migrants often combining different treatment locations and services (Bilecen and Barglowski, 2015; Osipovič, 2013; Phillimore et al., 2018; Troccoli et al., 2021).
Building on these insights, this article aims to establish a typology of motivations inductively to draw a broad picture of the thematic complexity underlying healthcare location choices.
Data and methods
The data originate from an online survey conducted during March–June 2016, as part of a broader project examining attitudes towards mobility, citizenship, and transnational social rights among EU migrants in the UK in the run-up to the referendum on EU membership (‘EUinUK 2016’). Aiming to reach both recent and established migrants representing some of the largest EU nationality groups, the survey adopted an active targeting strategy by directly seeking out nationalities of interest in online social media communities (primarily Facebook groups; see Miller and Sønderlund, 2010). This method of participant recruitment was chosen for its proven efficiency in accessing hard-to-reach populations while reducing self-selectivity and increasing geographical representativeness (Sue and Ritter, 2012: 10–11). Targeted online surveys have also been shown to achieve better socio-demographic representativeness than traditional methods for subpopulations in certain contexts (Miller and Sønderlund, 2010: 1563).
To reduce selectivity bias based on linguistic competence, six nationality groups were targeted with translated questionnaires (in Hungarian, Italian, Polish, Portuguese, Romanian, and Spanish), while other nationality groups were approached with the English-language questionnaire in nationality-specific or general-interest online communities. The qualitative data were thus obtained in seven different languages and translated into English for the analysis.
This article focuses particularly on data from one survey question: If you ever needed medical treatment, where would you rather have it? The question had four answer options (‘In the UK’, ‘In my country of origin/citizenship’, ‘In another country’, and ‘Do not know’). It also provided an optional open-answer box to elaborate on the reasons behind the choice: Please explain why (optional). The richness of the answers provided to this open question has made the issue of transnational healthcare the main unanticipated emergent theme of the project.
In this article, we undertake an exploratory qualitative analysis of the reported motivations for transnational healthcare preferences. We include in the analysis respondents from the 11 nationality groups with at least 10 participants answering the target survey question. Our analytic sample therefore includes a total of 1,656 respondents from 11 countries of origin, of which 511 (31%) have provided additional qualitative explanations in the open-answer box. Table 1 summarises some basic socio-demographic characteristics of the sample, while Table 2 lists the included nationality groups alongside their response choices to the target survey question. As the largest EU migrant group in the UK, most of our respondents were Polish nationals (60%), and the majority were female (65%). Since our aim here is to draw a broad picture of the thematic complexity underlying healthcare location choices, these imbalances in our data should not have a negative impact on our thematic findings apart from overemphasising certain group-specific experiences. Nevertheless, we will reflect on the limitations this imposes on possible interpretations in the conclusion section.
Socio-demographic characteristics of the sample.
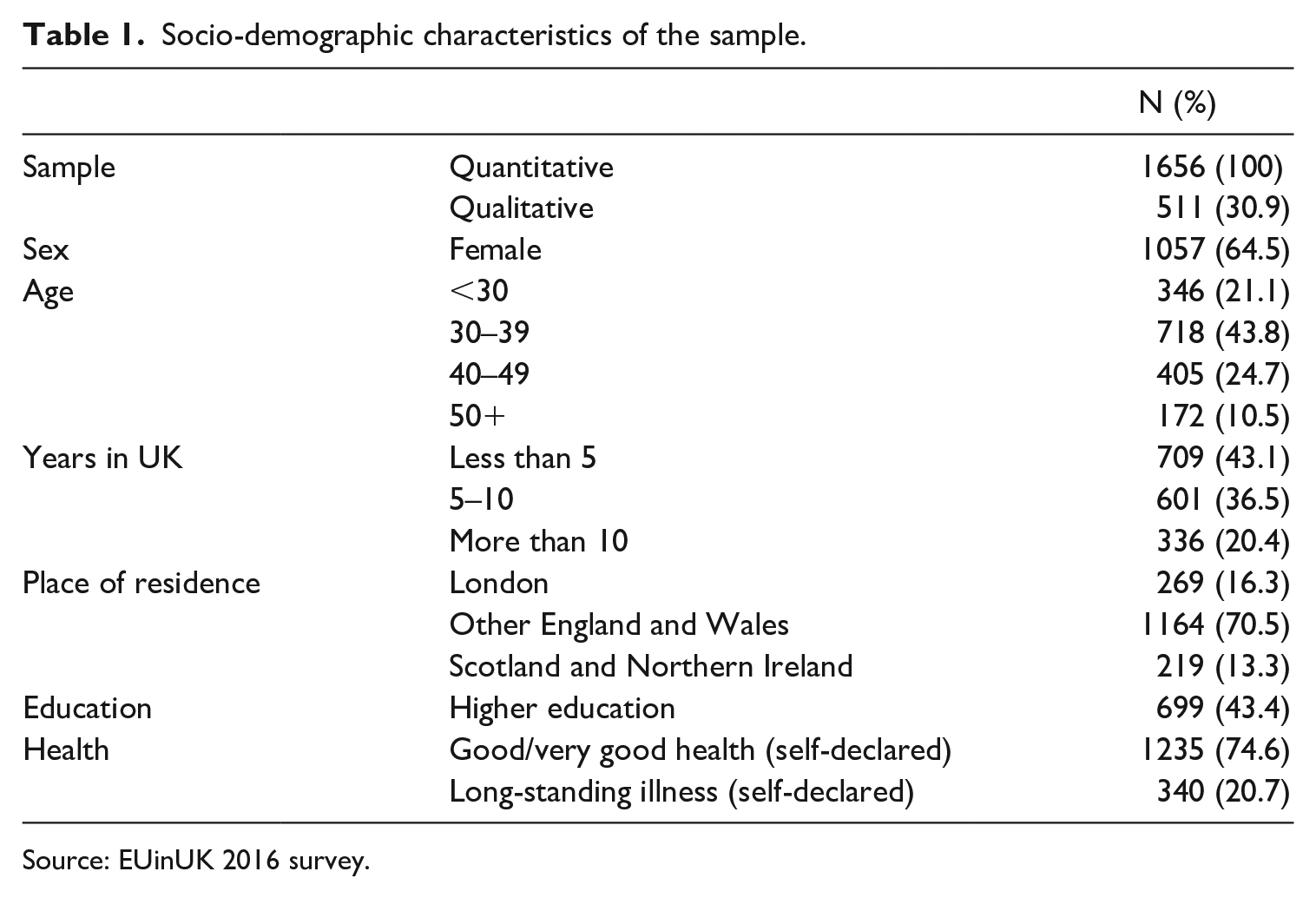
Source: EUinUK 2016 survey.
Treatment country preference by CoO.
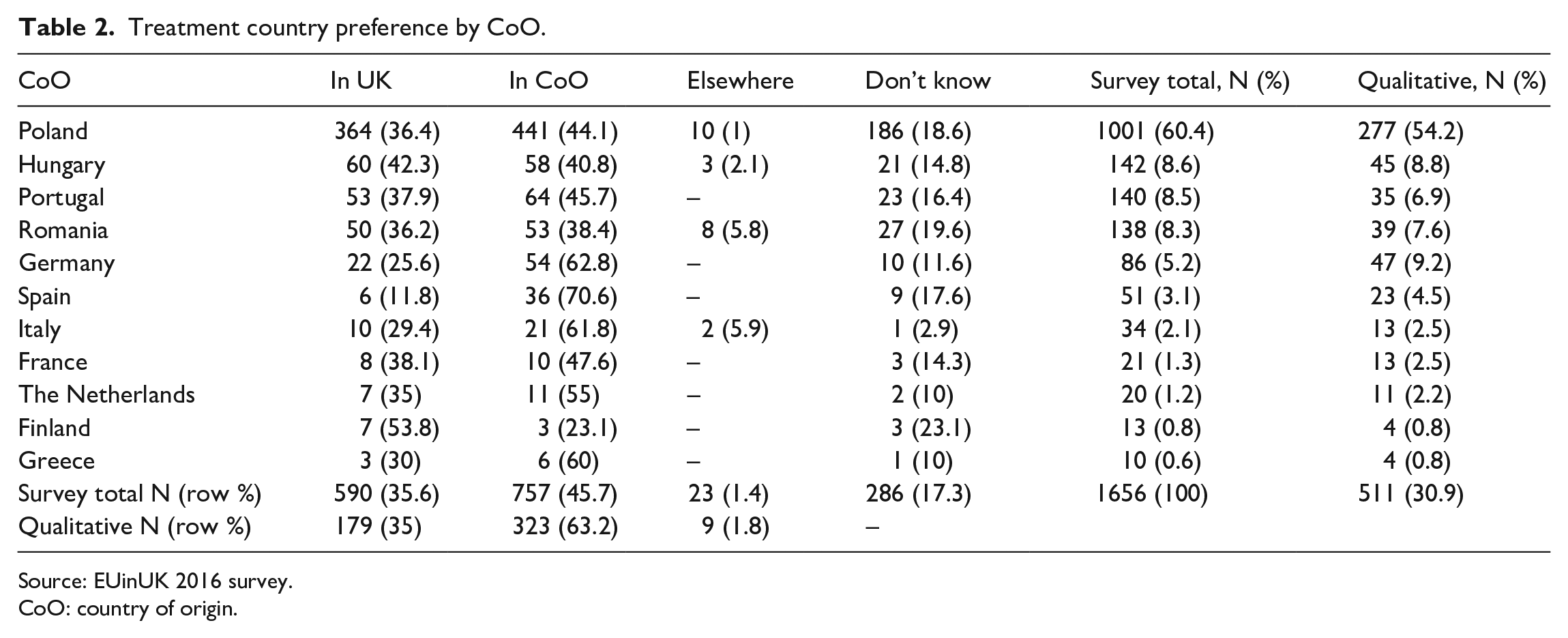
Source: EUinUK 2016 survey.
CoO: country of origin.
In this article, we focus primarily on the results from a thematic analysis of the qualitative sample (N = 511). The analysis generated a unified coding framework to allow a structured assessment of the reasons behind our respondents’ choices in respect to their preferred country for medical treatment (see Boyatzis, 1998). The thematic coding, performed using NVivo11, allowed the identification of multiple codes in each open-ended response and helped explore the interrelationships between the various reasons given by respondents regarding their preferred country of medical treatment. Following a brief overview of quantitative descriptive results, we turn to discuss the results from this thematic analysis and its relationship with the broader literature reviewed earlier.
Overview of descriptive results
We have found that fewer respondents preferred undertaking medical treatment in the UK (36%) than in their country of origin (CoO) (46%). A small number (1%) would prefer a third country, and a more significant share (17%) did not have a clear preference. Table 2 highlights that there are also noticeable nationality-based differences in these preferences. This distribution also hints to the fact that ‘medical tourism’ strictly conceived is a more limited phenomenon than mobility related to the ‘migrant’ condition (Horsfall, 2020; Mainil et al., 2013), and as the closer inspection of the qualitative comments of the nine respondents who explained their preference for a third country reveals, these are usually countries to which the respondent was connected through a previous migratory experience.
Our closer analysis will focus on the qualitative explanations concerning the reasons for preferring either the UK or the CoO for potential medical treatment. Overall, 179 participants preferring the UK and 323 favouring the CoO have provided qualitative responses. Following a thematic coding that identified one or more themes at different levels of coding detail in each of these open-ended explanations, we have identified five broad thematic groups containing a total of 598 lower level coded mentions (Table 3). The largest thematic group of mid-level themes relates to perceived differences in the quality of healthcare between the CoOs and the UK, with 67% of individual codes relating to various aspects of quality and 68% of participants in the qualitative sample mentioning quality aspects as a reason (not calculated in Table 2). However, perceived higher quality of healthcare was more widespread among those who would opt for treatment in their CoO on all the identified mid-level themes and particularly in respect to overall standards of care (31%), the professional expertise of doctors (19%), and timely access to treatments and specialists (9%). For those preferring the UK, convenience was an equally important factor (37%) followed by financial considerations (15%). Mix-matching services and procedures across the two locations, denoted as ‘bricolage’ following Phillimore et al. (2018), have emerged sporadically in the answers of both preference-based groups.
Reasons for treatment country preference (overview thematic groups).
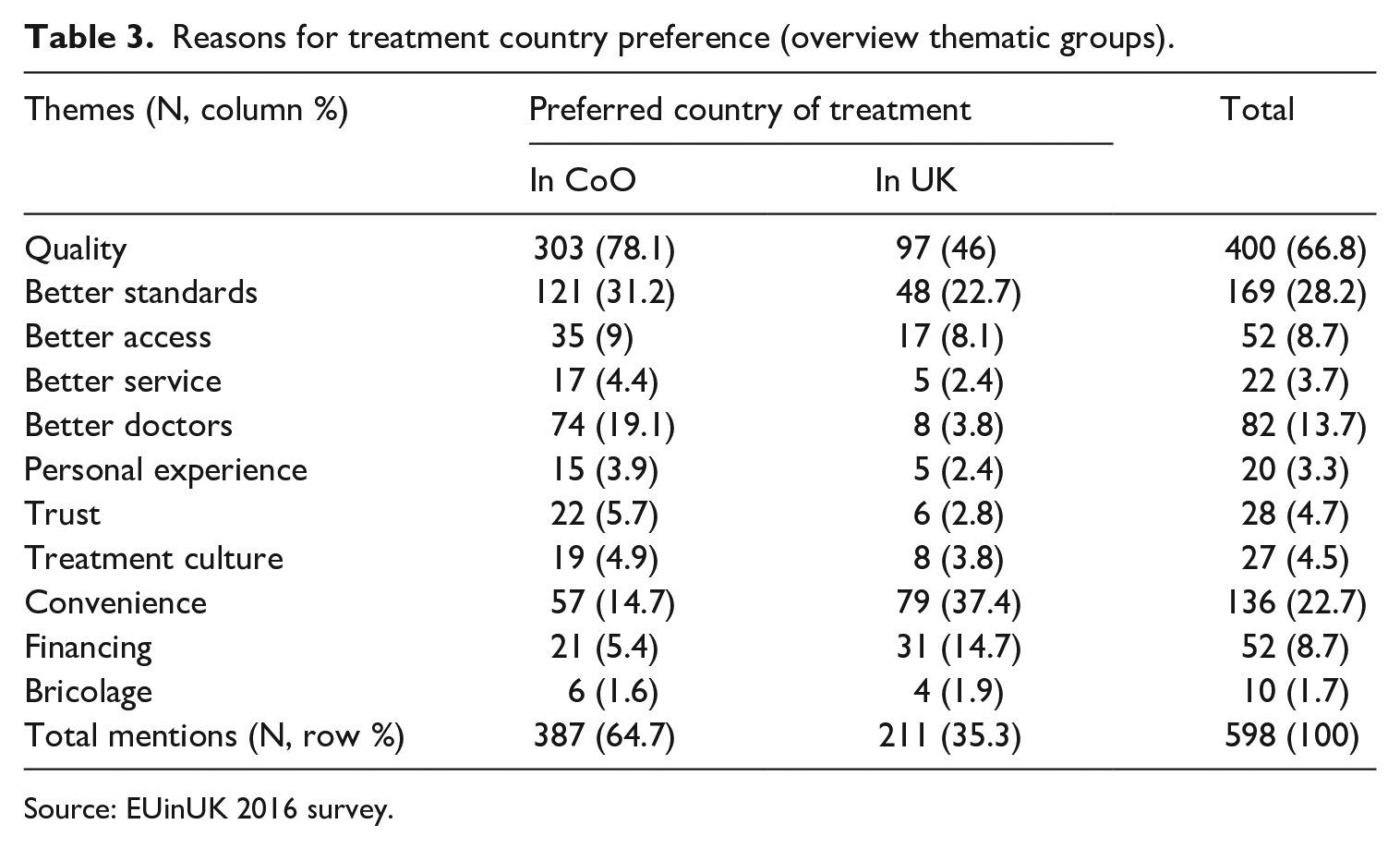
Source: EUinUK 2016 survey.
The thematic groups were designed to capture some shared aspects of the preferences for either location, which can also facilitate a statistical analysis of the effect of various socio-demographic factors on preferences and attitudes (see Moreh et al., 2018). Here, instead, we dwell on the qualitative depth behind this thematic classification to better understand the complexity of attitudes and the personal experiences underpinning them.
Results of thematic analysis
Table 4 presents a more detailed lower level coding. We find, for example, that expressions of opinion on healthcare standards could entail various subtleties allowing a more nuanced understanding of attitudes; it may not be irrelevant that a positive appreciation of standards in the UK is made in comparison with standards in the CoO or noncomparatively, as in the latter case its decision-influencing potential is likely to be mediated by the convenience of residence in the UK. The most common lower level theme associated with a preference for treatment in the CoO was the higher standards of care there compared to the UK (33% expressed this opinion), while preference for the UK was determined by the factual reality of residence for 29% of the respondents.
Reasons for treatment country preference (detailed coding, coded mentions).
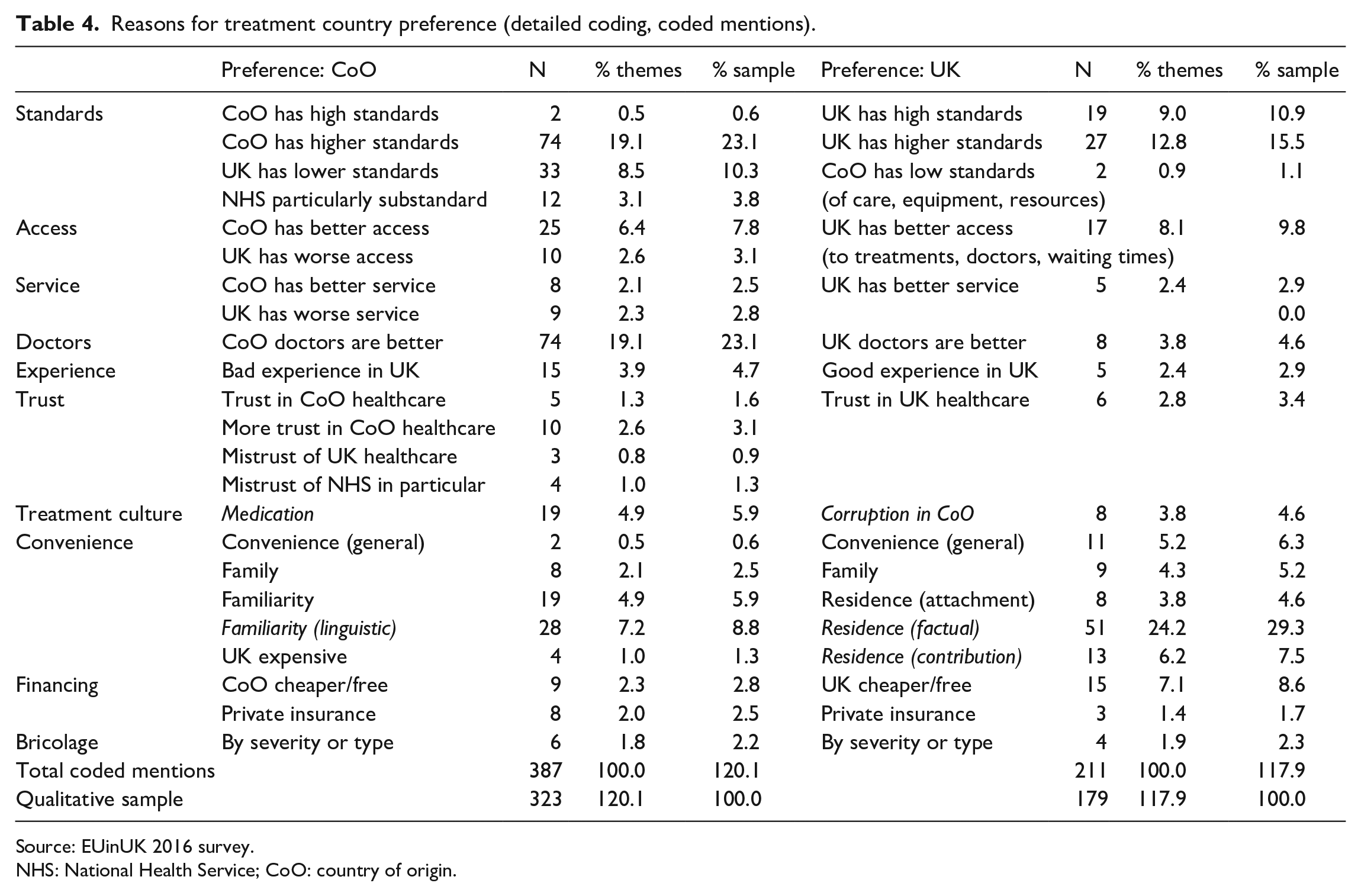
Source: EUinUK 2016 survey.
NHS: National Health Service; CoO: country of origin.
The following discussion of these results is organised into four subsections: the first three aim to better explain the dominance of quality-related motivations as they emerge from detailed descriptions of personal experiences, the social mechanism of trust, and cultural expectations; the fourth section aims to disentangle the complexity of factors making one treatment location more convenient or cheaper – overall or for specific purposes – than the other.
The depth of experience
The richness of detail provided by each response differed considerably with those describing actual experiences with healthcare services allowing for the most in-depth and personal understanding of reasons underlying treatment location preferences and opinions regarding the quality of healthcare provision. Such explicit accounts of personal experience help sensitise specific nuances often expressed through a set of interwoven issues, which in our analysis were assigned distinct lower level thematic codes. The following quote is an example of a detailed narrative account of multiple failings in the British healthcare system, whereby the respondent expresses a harsh but refined criticism of healthcare standards: It was here where I have been administered an overdose of penicillin for the first time. As doctors in Poland put it, it’s a miracle that I’m alive. The second time, they wouldn’t listen to me when I was telling them I was pregnant and told me to take antibiotics for an infection; when it turned out that I really was pregnant, I changed my GP. The third situation I had was when I started bleeding. They had me waiting for 48 hours in a situation where every minute was vital to save the pregnancy; they refused to give me medication to support the pregnancy; I was four months pregnant at that point; they told me to have natural birth which I couldn’t do, because I couldn’t determine the type of incision performed during my first C-section, as I was unconscious at the time. If the incision had been vertical, natural birth would carry a risk of rupture. In the end they told me to give birth one month prematurely, only to end up having to feed the little one with steroids due to the fact that he was smaller than their diagram had stipulated; and now, at the age of six months, he’s having to wear clothes for a twelve-month old because he’s so big . . . The health service in our area is horrible . . . (Polish, female, 30 years old, 8 years 8 months in UK)
This harrowing account is an implicit indictment of the medical aptitude of British doctors, service delivery, and quality standards at a local geographical level (‘in our area’). This perceptive observation on the part of our respondent reflects established knowledge about ‘unwarranted variation’ in healthcare provision across Britain caused by ‘idiosyncratic practices of clinicians and of healthcare organisations’ (Public Health England, 2015: 15).
Most explanations for preferring treatment in the CoO due to perceived lower quality healthcare in the UK were shorter statements – for example, ‘The British healthcare provision is not healthcare. Quality below all standards’ (Hungarian, f, 35, 4y2m); ‘English doctors lack medical knowledge!!’ (Polish, m, 57, 8y2m). These may well have similar underlying personal stories, but they may equally be based on second-hand opinion. In terms of thematic coding, what we have in such cases are explicit opinion statements relating to a single theme (standards and doctors, respectively). On the contrary, cases where negative experiences were made explicit as a single theme were rarer, although not absent (e.g. ‘I am not satisfied with NHS in the past’, Greek, f, 32, 5y7m). The same is true of comments describing UK healthcare as of higher quality, and of course, responses without an explicit reference to personal experience could also be rich in their thematic coverage: The level of healthcare on the British NHS is very advanced; the level of medical training is high, the doctors and nursing staff are very kind. Carers working with elderly people are required to have adequate training, and medications aren’t as expensive in relation to earnings, which is something you can’t say about Poland where medications are expensive and waiting time for specialists appointments is very long. (Polish, f, 58, 7y1m)
The mechanism of trust
The question of ‘trust’ has emerged from many explanatory comments as a more general theme and a social mechanism providing the emotional glue that connects experience to perceptions to preferences and eventual practices. The following quote provides a lively example of this process: I had a surgery in Poland. In my country I’m not treated as an intruder and have access to professional care in my own language (and don’t have to listen to stupid comments from an English doctor about the fact that my English isn’t sufficient enough to understand what the doctor from [X hospital] was telling me). Aside to this, there would be no one in the UK to look after me if I had an operation here, and I don’t trust the British health service. I was offered a surgery in the UK but was told it would take me two months to recover afterwards. I ended up being operated in Poland by more qualified doctors who carried out laparoscopy (British Indian doctors refused to operate on me in this way), which meant that recovery only took two weeks. It’s really pathetic. (Polish, f, 33, 9y2m)
Here, an experience of what Peled (2018) describes as ‘epistemic injustice’ led to a breach in trust, which, coupled with the lack of family support in the UK, induced the respondent to actually engage in ‘medical return’ to Poland.
The circulation of information distilled from negative personal experiences results in a generalised lack of trust in UK healthcare. As one Polish woman put it, ‘I don’t trust English doctors after what I’ve heard’ (28, 7y6m). ‘I don’t trust the NHS and the speed and level of care given in the UK’, wrote a 31-year-old German woman (6y). Or as a 64-year-old Portuguese woman who had been in the UK for almost 16 years succinctly explained her preference for healthcare treatment in Portugal: ‘More confidence’.
Such opinions echo those reported in other studies. According to Osipovič (2013: 106), ‘a dose of mistrust, unease and cultural unfamiliarity characterised [Polish] participants’ interactions with NHS professionals’. Sime (2014: 91) similarly concludes that limited intercultural contact ‘impacts on [migrants’] access to information and is likely to initially make them untrusting of services’. The mechanism that emerges from these observations is one through which cultural distance and unfamiliarity with the system translate into perceived discrimination and lack of trust that leads to negative opinions regarding healthcare standards and a preference for treatment in the CoO (see also Migge and Gilmartin, 2011).
While Sime’s quoted assessment implies that these attitudes and behaviours may change over time, Ehata and Seeleib-Kaiser (2017: 190) find that ‘even after living in the UK for a number of years, a relatively high degree of uncertainty with regard to social rights’ persists among EU migrants, and therefore mistrust of health professionals and the quality of service may extend beyond the initial phase of migration. Our parallel statistical analysis appears to provide more support to Sime’s integrationist expectations, finding a statistically significant effect of length of residency on location preferences although not on quality assessments (Moreh et al., 2018). Some of the qualitative responses can help illustrate this. While several respondents with shorter residence histories in the UK had made an explicit connection between familiarity and trust – ‘The doctors who treat me already know me well and I feel more confidence’ (Portuguese, m, 28, 7m); ‘I trust and know the system of my own country better than the British system’ (Spanish, f, 19, 9m) – many of the more established UK residents provided more carefully crafted explanations, like: ‘Medical care in my country of origin is better, but after all I’ve been here 20 years and therefore would probably trust the NHS’ (Finnish, f, 55, 21y1m). Similarly, a 30-year-old Polish woman (6y2m) would prefer treatment in the UK because ‘I live here and so I trust this country’s health service’. Trust, in their case, seems to relate to the factual reality or a rather more ambiguous moral imperative stemming from the residence in the UK.
The ambiguities of culture
The difficulties raised by ‘cultural unfamiliarity’ mentioned by Osipovič (2013) derive from a broader set of differences between what could be called ‘treatment cultures’. Two specific issues emerged from our data that can be related to such differences: one was the alleged practice by UK GPs to dispense ‘paracetamol’ for any medical condition while being overcautious about prescribing antibiotics; the other was perceived corruption in the healthcare systems of the countries of origin, specifically through the widespread expectation of ‘bribes’ and informal payments for various services. In our data, the two emerged as distinct influences on preferences for either CoO or UK treatment (Table 4).
‘The problem is’, explained one participant, that doctors in England prescribe paracetamol for everything. . . even when my son broke his thumb, they gave him paracetamol and nothing else; it’s a complete joke. I had to ask for an x-ray, beg even, because they wouldn’t do it. They did apologise later; it is horrific. (Polish, f, 37, 8y7m)
Compared to this, in Poland, there are ‘Definitely better doctors. No treating with paracetamol etc !!!’ (Polish, m, 34, 3y7m). According to a 34-year-old German woman (10y5m), ‘Most times one gets sent to the pharmacy to buy ibuprofen – seems to be the medication of choice for everything’.
Complaints along these lines are well documented in the qualitative literature (Ehata and Seeleib-Kaiser, 2017; Goodwin et al., 2013; Lindenmeyer et al., 2016; Madden et al., 2017), and beyond individual perceptions, they are likely to reflect broader differences between treatment cultures across Europe. An interesting case described by one respondent highlights this: Doctors here have a different approach; I often suffer with tonsillitis and I know that antibiotics have always been very helpful. When I asked for antibiotics, the lady asked me if I was from Poland, which made me feel very uncomfortable, and of course it wasn’t prescribed to me. When a week later I was no longer able to get out of the bed, my husband took me to another doctor who prescribed it to me. (Polish, f, 43, 11y)
In respect to the specific ailment mentioned in the quote, official NHS guidance advises patients that there are two types of tonsillitis – viral and bacterial – and while the former kind ‘has to run its course and antibiotics won’t help’, a GP ‘may prescribe antibiotics’ for the treatment of the latter type (NHS, 2017). More generally, the use of antibiotics is a particularly divisive practice across European countries, with Eurobarometer data showing a noticeable South-East/North-West divide in perceptions and knowledge (European Union, 2016). Cross-national differences often boil down to prejudice by both parties during patient–practitioner encounters, as evident in the quote above. Regardless of which party is correct in each individual case, such experiences are likely to enhance a more general sense of ‘not being taken seriously’, with direct consequences on trust and assessments of doctors’ competence and the quality of medical service (Feldmann et al., 2006; Lindenmeyer et al., 2016: 4; Phillimore, 2011).
On the contrary, the unchallenged expectation of ‘bribes’ or ‘gratuities’ by doctors in the CoO has been alluded to by several participants. In the UK, ‘you are treated as a person and not a source of bribe’, said a Romanian respondent (f, 49, 1y7m). You have ‘Easy access to specialist doctors; NO BRIBERY!’, explained a 35-year-old Polish man (10y2m). According to another participant, My family has experienced a more serious medical intervention, and although the NHS feels very slow, with long waiting lists, the care and attention is of high standards and there is no need for gratuity (Hungarian, m, 38, 7y4m)
According to Allin et al. (2006), this form of corruption is widespread in the healthcare sectors of post-communist Central and Eastern European countries and has both ‘economic’ and ‘sociocultural’ reasons. On the one hand, it ties into cultural practices of ‘gift giving as an expression of gratitude’ that are not dissimilar in countries with widely acknowledged unduly low remuneration of medical practitioners from classical sociological descriptions of reciprocity in social relationships (see Mauss, 2002). On the other hand, it risks undermining formally free-to-use public healthcare systems, transforming them into de facto fee-for-service systems in which the consequences of expected informal payments can range ‘from nuisance to obstacle to barrier and, ultimately, to self-exclusion’ (Allin et al., 2006: 63).
This dual economic-cultural nature of ‘gratuities’ also means that while in our data it emerged as solely reinforcing preferences for UK treatment, deeper ethnographic work confronts us with a more ambiguous picture in which emigrants’ engagement in informal payments in the country of origin is linked to processes of social distinction with the effect of reinforcing the system of gratuities and exacerbating local socioeconomic inequalities (Horton, 2013; Stan, 2015).
Assemblages of convenience and financing
Questions of ‘convenience’ are complex and relative, and while some of the explanatory comments invoked it in general terms, the majority framed it around aspects such as familiarity – ‘Being of similar quality, I’d choose my country of origin because I’m more used to the practices there’ (French, f, 30, 9m); feelings of belonging – ‘UK is where I live and work – it feels like home’ (Portuguese, m, 26, 2y6m); emotional attachment – ‘This is where I live and I love the NHS’ (Finnish, f, 32, 4y6m); the presence of family members – ‘My whole family lives in Poland, so I could rely on their help’ (Polish, f, 45, 10y), or ‘[In the UK] Because my husband is here’ (French, f, 58, 22y2m); language difficulties – ‘no language barriers for the medical terms, family nearby’ (German, m, 24, 4m); or the sheer fact of residence – ‘It’s where I live’ (Romanian, f, 39, 11y6m). Overall, the ‘convenience’ of treatment in the CoO relates to familiarity in a broad sense: the importance of ‘feeling at ease with a system, trusting its providers and being able to speak one’s language’ noted by Glinos et al. (2010).
Residence, expressed in purely factual terms, was overall the most common determining factor for preference of treatment in the UK (51 mentions, 29% of those opting for the UK). In several cases, residence was also related to financially contributing to the system and so fed into issues related to healthcare financing. A closer analysis of these comments reveals that ‘contribution’ is experienced and expressed broadly in three different ways: as an aspect of ‘convenience’ – ‘Due to the convenience of being where I pay my taxes and where I live’ (Portuguese, f, 34, 10y6m); as a sense of entitlement or ‘stakeholder’ justice (cf. McGhee et al., 2019) – ‘I live here and have been paying taxes for the past eleven years!!’ (Polish, f, 45, 11y1m); or as an ethical question of fairness – ‘I pay my taxes in the UK, so it would feel wrong to have treatment in a country where I do not contribute’ (German, f, 43, 9y7m). This last comment, of course, does not take into consideration, on the one hand, the possibility of resorting to private insurance schemes in the CoO or, on the other, the structural constraints on access to healthcare which another participant raised as almost in direct response: If you live in the UK, you cannot have medical treatment in Germany as only registered residents can have health insurance. I have private health insurance in the UK which I am quite happy with. (German, f, 28, 6y)
The topic of private insurance has emerged in several comments, although it is undoubtedly a much more common theme than our data allow to assess (Ehata and Seeleib-Kaiser, 2017; Horton, 2013; Sime, 2014; Stan, 2015). Some can afford to ‘have a private medical insurance in the UK so medical treatment is decent’ (French, m, 37, 10y9m). For others, it is not a question that in many countries of origin ‘Private treatments are of much higher quality and are much cheaper than in the UK’ (Romanian, f, 35, 1y11m). Yet, as Stan (2015) has also emphasised, the cost of private healthcare in the origin countries is not always affordable to migrants: I have already undergone four operations, but I’m still not well. In Poland, if I had the money, I would have had the right tests carried out by now and given a diagnosis (. . .) (Polish, f, 24, 4y6m)
Practices involving private healthcare-seeking can also take place in a transnational social space that supersedes geographical transnationalism. Several authors have remarked that many EU migrants in the UK also have access to local private clinics that cater exclusively to particular ethnic groups (Ehata and Seeleib-Kaiser, 2017; Osipovič, 2013). Although such opportunities may not necessarily affect treatment costs, they help remove the language barrier and reduce the trust deficit and the cultural distance we discussed earlier, while they can still be easily combined with state-funded services: When it comes to diagnosis and GP visits, I would ALWAYS choose private European doctors over British. They misdiagnosed me for 4 years . . . whereas I visited a Polish clinic in London and got diagnosed instantly and my problem sorted within 3 months! . . . But the hospital treatments I received was great. The nurses here are amazing, they go the extra mile to help you! (Poland, f, 30, 10y8m)
The sentiment encapsulated in the quote above is echoed in other research findings too, where Polish migrants expressed significantly higher levels of satisfaction with hospital treatments than with GPs or dentists (Goodwin et al., 2013: 162.)
Several other comments alluded to engagement with healthcare services in both the UK and the CoO, or to combining paid and free services as well as formal and informal treatments. Such practices of healthcare ‘bricolage’ (Phillimore et al., 2018), ‘assemblage’ (Bilecen and Barglowski, 2015), or ‘stitching’ across borders (Bilecen et al., 2015) are well documented. In most instances of referenced ‘bricolage’, the selected treatment location preference was qualified by the type or severity of the procedure required. Some preferred ‘Longer treatment in my country, basic treatment in the UK’ (Spain, m, 27, 1m), or ‘UK for minor things, my country of origin for serious medical issues (such as cancer)’ (German, f, 34, 2y2m). As another respondent explained, That depends on the treatment in question. For dental treatment I regularly go to Hungary only, but if I need to visit the general practitioner with some acute problem then I obviously do it in the United Kingdom. In the future, I think if I will want to give birth, then I will also do that in Hungary. (Hungarian, f, 37, 5y1m)
Dental care was the most mentioned ‘type’ of treatment to be sought in the CoO, mostly because it is not free to most patients on the NHS, but occasionally also for quality considerations. As one participant explained, Any dental work I had done in England had to be corrected in Poland in a very short space of time, due to the poor quality of work or the use of bad quality materials. (Polish, m, 50, 2y8m)
This experience gives a new meaning to the concept of ‘duplicative exits’ (cf. Laugesen and Vargas-Bustamante, 2010), and it may not reflect an isolated attitude; another participant had also chosen the UK ‘for convenience as I live in the UK but I might want to do further tests/get second opinion in Poland’ (Polish, f, 39, 9y11m).
Although the dichotomous choice imposed by the question design masked the true extent to which our respondents actually engaged in practices of ‘bricolage’, the abovementioned examples confirm that many EU migrants resort to different services and locations ‘concurrently, interchangeably or successively’ (Osipovič, 2013: 110), and that transnational healthcare is multidirectional and multilinear (Troccoli et al., 2021).
Conclusion
This article contributes to the literature on transnational healthcare among EU migrants by conceiving an inductive typology of preferences for medical treatment locations on a larger and more diverse sample than in previous studies. For this purpose, we used online survey data from 1,656 respondents, and we analysed 511 qualitative explanations.
A relative majority of our survey respondents disclosed a preference for medical treatment in their CoO rather than the UK. While this pattern of preference is in line with that suggested by the broader literature (Goodwin et al., 2013), we caution against giving it an inferential interpretation. Polish nationals and women are overrepresented in our survey, and both groups may have a higher propensity towards ‘medical returns’ (Horton, 2013). Polish migrants have been described as having a strong transnational connection with their CoO and therefore more likely to be aware of and engage with healthcare services there (Horsfall, 2020). Women, on the other hand, are known to face difficulties in accessing gender-specific healthcare treatments (Gorman and Porteous, 2018). Furthermore, the data were collected in the run-up to the EU Referendum, a period when the public discourse was dominated by debates on EU migrants’ alleged abuse of the UK’s free public services. It is possible that the context of this ‘hostile public discourse towards EU migrant citizens’ (Ehata and Seeleib-Kaiser, 2017: 9) has influenced both the overall response rate (positively) and the professed treatment location preferences, over-representing the voice of those whose experiences with the British healthcare system contrasted starkly with these political and media discourses (see also Ehata and Seeleib-Kaiser, 2017). Testing the possible effect of ‘hostile’ discursive environments on transnational healthcare attitudes and practices is beyond the scope of this article, but it is an important question to explore in future research.
Our thematic analysis has found that preferences for the CoO are driven overwhelmingly by perceptions of higher quality healthcare there, while preferences for the UK have more to do with convenience and financing considerations. Subjective perceptions regarding the quality standards of UK healthcare have thus been identified in both our data and the wider literature as an important reason for medical returns (Ehata and Seeleib-Kaiser, 2017; Goodwin et al., 2013; Madden et al., 2017; Osipovič, 2013; Sime, 2014). Our analysis has also revealed how these perceptions are created through an interaction between negative personal experiences, trust, and often concealed cultural differences, a process already alluded to by Migge and Gilmartin (2011). At the same time, the size and variety of the qualitative data at our disposal have allowed the identification of various nuances and connections between attitudes that previous studies could not systematise. Furthermore, another aim of the article was to achieve a thematic typology of motivations inductively, based on migrants’ answers and narratives, which then lends itself to further analysis of the socio-demographic and other factors that predict location preferences and quality perceptions (e.g. Moreh et al., 2018).
The chosen design of our main survey question, however, does not allow to fully explore several aspects of transnational healthcare among migrants that are undoubtedly of great significance, such as the multiplicity of ways in which treatment locations and procedures are combined in actual practice (Bilecen and Barglowski, 2015; Osipovič, 2013; Phillimore et al., 2018). In a follow-up research project, we have begun addressing these questions, describing how transnational healthcare should be understood as a multilinear process (Troccoli et al., 2021). Yet, more work is needed to fully understand the intricacies of transnational healthcare and to reach a holistic and dynamic picture of ‘medical returns’.
Footnotes
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Economic and Social Research Council. Grant: RES-625-25-0001.