
Abstract
Technological innovation is often positioned as a solution to the challenges of healthcare provision, yet the experience of bringing new technologies into practice has proven uneven and unpredictable. To realise the potential benefits of innovation, we need to understand the complex relations between contingencies and contexts that seem to be ubiquitous as new technologies are brought into play in healthcare settings. This article explores what the field of Science and Technology Studies (STS) can contribute to the understanding of implementation processes, arguing that combining Actor–Network Theory and Normalisation Process Theory provides a framework for prospective research. Drawing on examples from a prospective study of a new point-of-care test illustrates how the framework enabled an understanding of the processes likely to be involved in its implementation within three healthcare settings, with implications for the continued technical development. In combination, the theories enable different levels of analysis, but it is by keeping them in tension that this approach becomes practically applicable. If we are to rely on innovation to achieve improvements in healthcare provision, we need to find a way to intervene in the implementation process, and STS offer the resources to achieve this.
Keywords
Introduction
Although society is continually optimistic about technology, particularly within healthcare, even the most promising technologies can be difficult to incorporate into everyday use (for examples, see Bowns et al., 2006; Dent, 1990; Doolin, 2004; Halford et al., 2010; Heath et al., 2003; Heeks, 2006; Lehoux et al, 2002; May and Ellis, 2001; May et al., 2001; Timmons, 2003a, 2003b). If we are to rely on technology, especially within the complex environment of healthcare, then something in the process of technological development and organisational implementation needs to change – we need to intervene to enable the development of workable technologies. This means conceptualising the problem beyond the implementation of ‘finished’ innovations, towards an extended understanding of the process which draws together the early stages of scientific development and the practice required in end use. In contrast to the traditional linear approach, which sees scientific development as one end of the process that is discrete from implementation at the other end (Godin, 2006), developing workable technologies requires an iterative approach to bring them into dialogue.
The field of Science and Technology Studies (STS) has been immensely successful in demonstrating that the implementation of technologies is complex and cannot be reduced to purely technical factors (e.g. Akrich, 1992; De Laet and Mol, 2000; Jensen, 2004; Webster, 2007), providing methodological and theoretical tools to explore the social construction of technoscience. Yet the application of these resources in practice can be challenging. For example, previously in this journal Prell (2009) recounted her experience of using the STS theory ‘Social Construction Of Technology’ (Pinch and Bijker, 1984) as a framework to explore the construction of an information system. Finding the concept of ‘technological frames’ insufficient to explain and describe the impact of resource-access on the construction of the technology, Prell calls for more attention to structural influences on technological development. In this article, I argue that in addition to providing a detailed understanding of the construction of technologies, we need to push STS’ great resources further to intervene in technological development itself.
However, this endeavour is complicated by STS’ central focus on contingency and context. The preoccupation with context has inspired caution about acting on STS research – a source of frustration for some scholars who have called for more interventional approaches (Guggenheim and Nowotny, 2003; Law, 2008; Webster, 2007; Zuiderent-Jerak, 2015). The abundance of seemingly promising technologies that nevertheless fail to be successfully implemented should be seen as a call to action for STS. We must find a way to move beyond the focus on complexity and work to find similarities across settings, as it is in the similarities between cases that middle-range theory is generated (Geels, 2007). Only this kind of middle-range understanding can intervene in the development of appropriate technologies.
The aim here is not to remove complexity, but to seek to define a complexity that we can work with. I argue that combining two STS theories, Actor–Network Theory (ANT) and Normalisation Process Theory (NPT), provides a way to do this. In combination, the theories provide a framework that can navigate contingency to enable prospective research while maintaining empirical integrity. Feeding this information upstream to guide ongoing technical development offers the opportunity to develop a device that reflects the need for innovation within specific settings. Importantly, it is by keeping the theories in tension – using each to ask questions that the other on its own would not pose or could not answer– that the framework becomes empirically applicable. This is illustrated through examples from the empirical application of the framework to explore the potential implementation of an emerging point-of-care test (POCT). Although the POCT device was in very early stages of technical development, existing only within the boundaries of the laboratory, using an ANT/NPT theoretical framework enabled its potential implementation to be explored within three different healthcare settings: an acute medical unit (AMU), a genito-urinary medicine (GUM) clinic, and a respiratory centre (TRC). This generated information that could be moved upstream to inform the continued development of the technology.
A framework for intervention
ANT is the most widely accepted STS approach (Law, 2008) and, with its focus on the relations between heterogeneous actants, offers a valuable resource in understanding both the scientific development of a technology and the context of intended use. However, its epistemological focus on context and contingency is a double-edged sword for interventional research: while contingency is necessary in creating a space for research from the field to inform ongoing technical development, it simultaneously hinders the ability to generate such prospective data as it does not allow for prior assumptions about how a device might relate to future settings. Using an ANT approach alone, there is no mechanism to create a dialogue between these two fields to enable an iterative approach to technical development.
This is indicative of wider criticisms that ANT functions on two opposing levels: providing an ontological understanding of networks, while insisting that knowledge can only be acquired empirically and at the micro-level, hindering its wider application (Geels, 2007; Guggenheim and Nowotny, 2003; Webster, 2007). The focus on exploring theory through case studies has created a frustration that ANT unpicks black boxes but never compares them to others to formulate a normalised understanding of technical change (Bijker, 1993). Indeed, Geels (2007) calls for ANT to find a way to combine the similar yet separate concepts that have been developed through empirical research, to generate theory that can be applied beyond individual cases.
A normalised understanding of implementation, generated through the combination of multiple empirical case studies, would enable a prospective understanding of what would be required for a technology to come into use, in a way that cannot be extrapolated from single case studies. However, reducing multiple findings to generalisable laws sits at odds with ANT’s focus on context and contingency (Law, 2008). Yet, although a certain amount of reductionism is necessary to develop middle-range theory, it is possible to do this while recognising the complexity and messiness of local practices (Geels, 2007). In this case, I argue that NPT offers a way to navigate the problem of specificity in ANT analyses.
NPT is an STS theory that functions at the middle range to offer an understanding of the work that is done to integrate new practices and technologies within organisational settings (May, 2013a, 2013b; May et al., 2016; May and Finch, 2009). The central theme of NPT is that the establishment of innovations within organisational settings is not simply an indication that they met a need, but is an outcome of actors working to incorporate them into practice. It proposes that the work of normalisation is operationalised through four generative mechanisms – coherence, cognitive participation, collective action, and reflexive monitoring – illustrating that actors must continually invest in the required practices for it to become integrated within the setting. Table 1 provides more detail about the mechanisms of NPT.
NPT mechanisms.
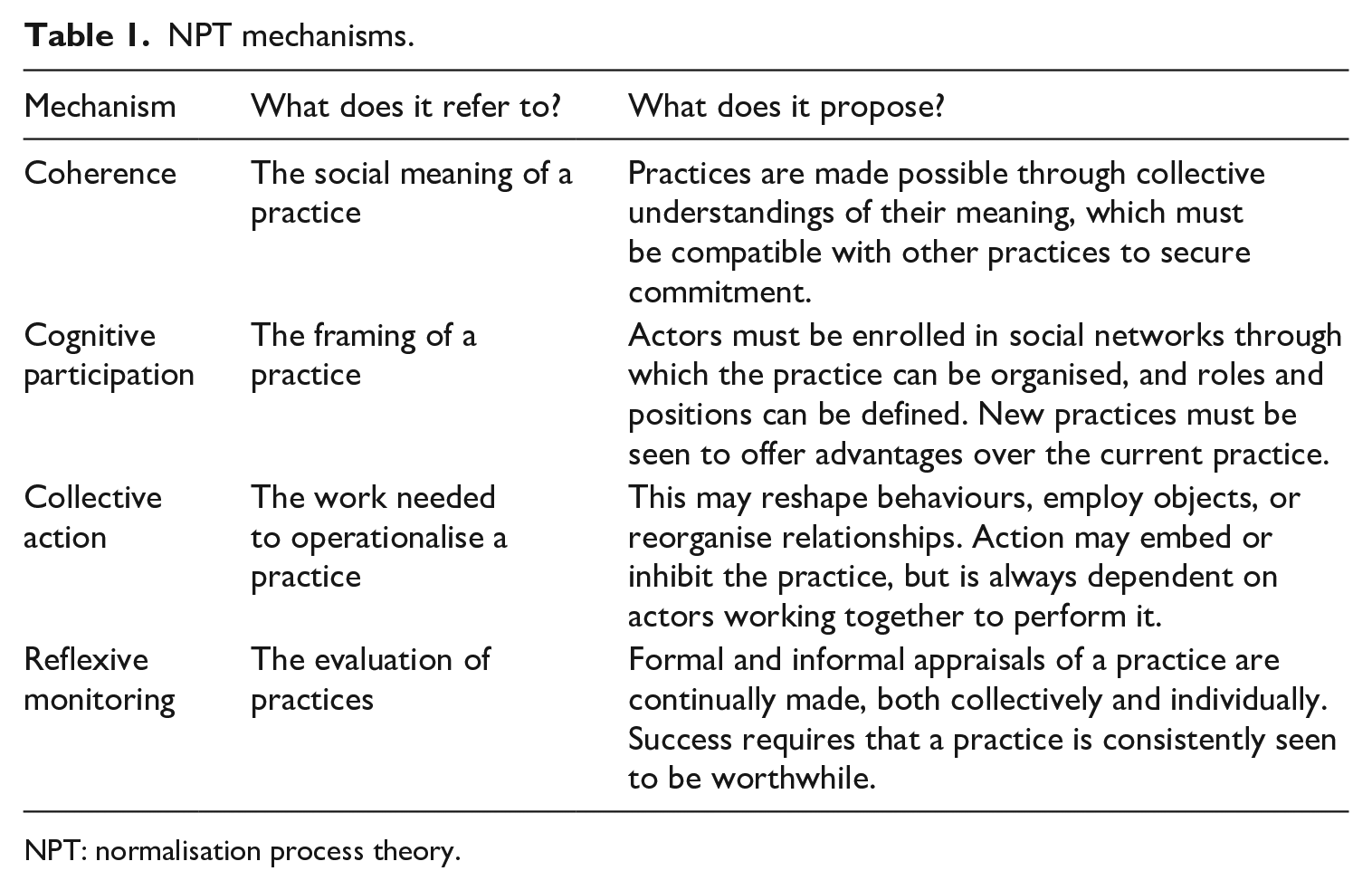
NPT: normalisation process theory.
Although NPT proposes the mechanisms through which implementation is likely to be achieved, it does not offer a methodological tool to explore how these mechanisms might be resourced within specific settings. Thus, in isolation, it cannot offer a comprehensive way of undertaking prospective research, at a time when a technology is in early development and its construction is fluid and adaptable. I argue that in combination, ANT and NPT offer a comprehensive analytical framework that exploits the advantages of each theory to enable prospective research into the potential implementation of a technology before it becomes black-boxed, allowing an iterative approach to developing workable technologies.
It is by facilitating analysis at an ontological, middle-range, and micro-level that ANT and NPT enable prospective research. NPT’s middle-range understanding of implementation provides an analytical framework through which to interrogate the empirical data derived through ANT-inspired fieldwork. Using NPT to analyse the data in this way acts to abstract it from its context, transforming it from a micro-level analysis that is intrinsically linked to an individual case study, to a middle-range analysis in which it can be understood as an empirical example of a category of action, allowing comparisons to be drawn across multiple case studies. It is this information that can be moved upstream to guide the development of a device that is appropriate to and workable within specific settings.
Essentially, NPT enables the prospective element of the research. ANT can be used to explore both the scientific development of the device and the context of its potential use, but NPT is the tool that enables a dialogue between the two. Keeping the theories in tension in this way, rather than attempting to amalgamate them, maintains the authenticity of each yet creates a research approach capable of moving beyond the relativity and contingency inherent in ANT case studies while leaving the integrity of the empirical data intact. This allows the researcher to work with the specificity and generalisability of knowledge simultaneously – to understand how a technology might fit into specific settings while also revealing the parts of implementation that are generalisable across multiple settings. This reflects what Heath et al. (2003) describe as location work, referring to the way that knowledge travels across sites yet is made specific and appropriate to the various places it connects. The discussion will now turn to explore the application of this framework in practice.
Methods
This research was undertaken as part of a wider interdisciplinary project focused on developing a POCT to detect viral infections. The project included a sociological component to explore the potential relevance of the device within specific settings and provides a case study against which to apply this framework for prospective research.
Research design
As the POCT was thought to have multiple applications, its development was not being targeted towards any particular setting. To reflect this flexibility, a comparative case study design was used to explore potential use within three medical settings thought to have a potential need for rapid test results: a genito-urinary medicine (GUM) clinic, an acute medical unit (AMU), and a respiratory centre TRC.
Using a comparative case study approach enabled exploration of the specific context of work in each setting. A technology that is successful in one context cannot necessarily be transferred to another user setting unproblematically. However, this does not mean that understandings of implementation should be bound by the contingencies and context of individual technologies, practices, and settings. As Jensen (2004) argues, in recognising the multiplicity of technologies, the focus should not be on exploring difference but on whether a coherent object emerges. Exploring the potential use of the POCT device in three settings generated a cross-case understanding of its potential use that recognises the contingencies of individual settings while highlighting common issues and themes that remain constant in others.
Data collection
Data collection within each case study focused on the actants that would potentially be involved in the implementation of the device. I conducted 30 qualitative interviews across the settings (see Table 2), with participants ranging from those involved in the assessment of technologies at a policy level, to managerial and front-line staff likely to be involved in the introduction and use of the device in the specific settings. Interviews explored participants’ views of the potential use of the technology, their understandings of the organisation of work in the department, whether there is a need for the technology, the changes that the introduction of the technology may bring, and the other actants involved in the production of work. Observational work was used to follow the ensembles of social practices through which work is produced, and I examined the relations between actants in policy and regulatory documentation. Using these qualitative methods enabled a detailed and empirically grounded understanding of if and how the POCT device might relate to each setting. Ethical approval was obtained from an NHS Research Ethics Committee prior to the study. Pseudonyms for participants have been used throughout this article and some details have been changed to protect participants’ identity.
Interviews with participants across the case studies.
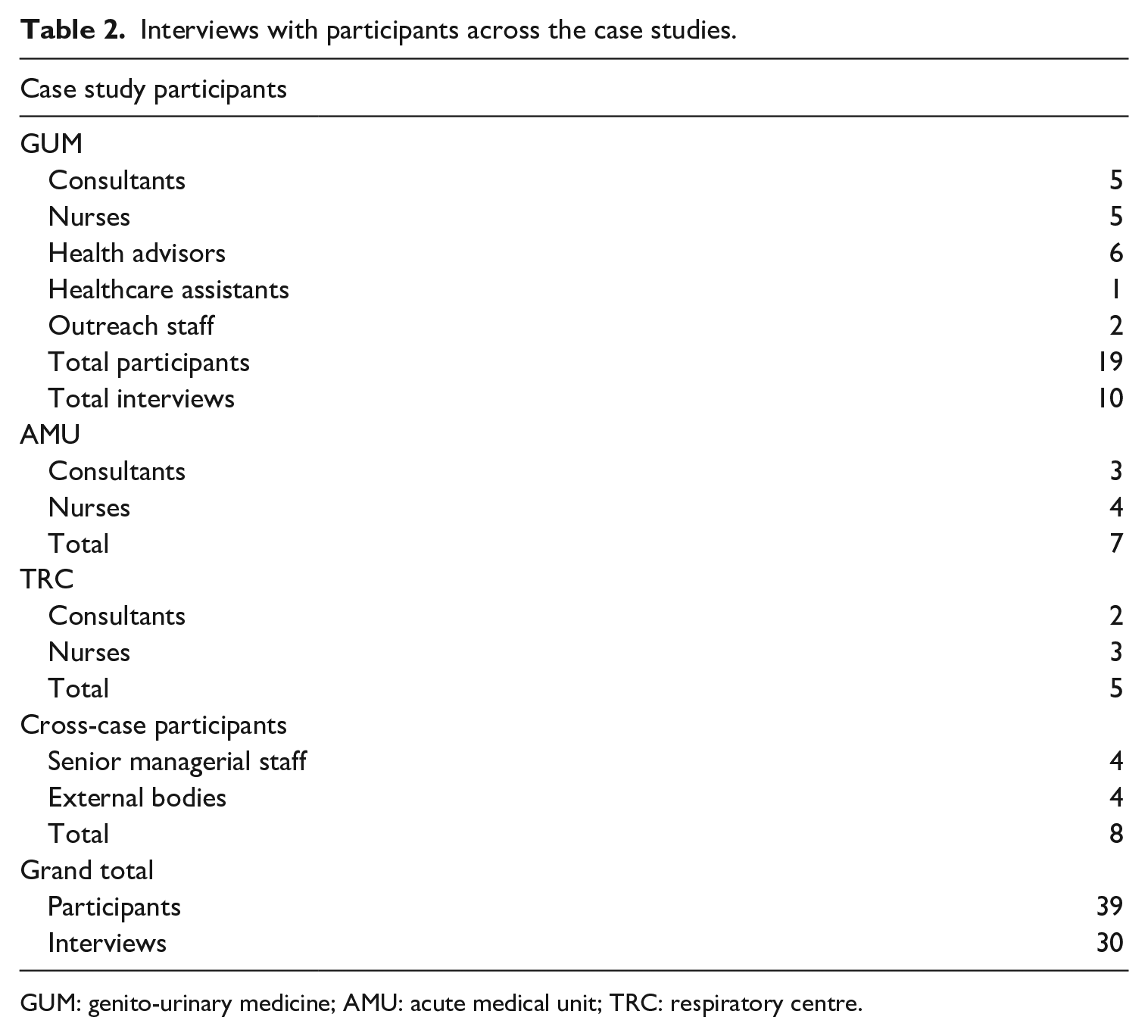
GUM: genito-urinary medicine; AMU: acute medical unit; TRC: respiratory centre.
Data analysis
Interviews were transcribed verbatim and analysed using NVivo data analysis software. Initially I coded all of the data using inductive and open coding, then refined the themes by combining similar codes into single categories. With the data consolidated into a manageable set, I introduced more deductive analytical processes to look for the themes promoted by ANT and NPT, grouping thematic codes according to the theoretical concepts. This enabled me to explore the relationship between ANT and NPT within the data, adding context and detail to the analysis that could not be offered using each theory individually.
In this way, data analysis was an iterative process of exploring the relationship between the deductive, thematic analysis emerging from my data, the categories promoted by ANT and NPT, and the insight this gives into the nature of the relationship between ANT and NPT themselves. The discussion now turns to the empirical analysis to illustrate how the theories function together in practice. To explore the potential implementation of the POCT, I utilised all four NPT mechanisms and explored how they relate to other ANT concepts. The following discussion focuses specifically on the relationship between the NPT mechanism of coherence and the ANT concept of problematisation as an example and provides a detailed account of how keeping the theories in tension enables a comprehensive understanding of how the POCT might relate to the different organisational settings.
Keeping theories in tension
Combining ANT and NPT provides a framework that functions across the analytical spectrum to enable a prospective understanding of implementation, but it is by keeping them in tension – that is, using each to ask different questions of the data – that the framework becomes empirically applicable. While ANT focuses on context and relational ontology to enable a detailed understanding of the network of actants in a setting, NPT asks which parts of this wide and complex network might be important to the implementation of the device? On the other hand, while an NPT analysis focuses on explaining implementation through generalisable mechanisms, ANT replies what about the complex relations already at work within the network? In this way, they provide a range of resources to enable prospective research capable of intervening in outcomes. Below I use empirical examples to demonstrate the tension in the relationship, focusing first on the use of NPT to move beyond the contingency inherent in ANT analyses, and moving on to show the importance of ANT in contextualising the generation of NPT mechanisms.
Problematising service provision
The ontological understanding of the relations between heterogeneous networks of actants provided by ANT is a valuable resource in exploring the context within the case study settings. ANT proposes that new actants are enrolled into the network of a technology through the process of problematisation; that is, convincing them that they have a problem to which the technology can be pitched as a solution (Callon, 1986). To be relevant in the case study settings, the POCT device must problematise service provision by demonstrating the advantages to be gained by delivering near-patient test results. However, a problem lies herein: the very features of a POCT that may hold advantages for practice bring inherent disadvantages. Moving testing procedures into the patient encounter distributes responsibilities for performing diagnostic procedures from the laboratory into clinical practice, often at the detriment of quality assurance and financial cost. To use diagnostic test results with confidence, it is important to ensure that the test has been performed correctly and without contamination. The laboratory provides a controllable environment in which external forces that might impact results can be quantified and excluded. The laboratory environment has been optimised to ensure the accuracy of test results, and within this setting it is possible to develop standardised procedures: You’ve got to make sure your laboratory has all the standard operating procedures . . . And [has] external quality assurance. So you have to be showing that your test in your lab is producing the same data to the same standards as other labs are. (Oliver, senior pathologist)
In contrast, POCTs are performed in clinical settings, which are comparatively unstable and difficult to control. The variability and inconsistency between clinical settings make the development of standardised procedures impossible. Often, procedures which are workable and stabilised within one setting become unworkable within another context: Because we see so many [patients], it’s not like in a GP surgery where it’s quite easy to calibrate. Where we were seeing maybe thousands of patients as a one off, then it’s hard to calibrate the machine to make sure that it’s reading. (Carolyn, AMU nurse)
In this example, the quality assurance procedures that were stabilised and controlled within the general practitioner (GP) surgery are destabilised by the volume of patient samples that it would need to process in the AMU.
Even when it is possible to stabilise quality assurance procedures within clinical settings, it is difficult to ensure that they are performed correctly. In the laboratory, trained technicians are responsible for performing and maintaining the equipment, whereas POCTs rely on a range of clinical staff. The redistribution of procedures integral to the accuracy of test results from trained technicians to potentially unreliable actors can reduce quality: You trade off some reliability with point of care, because you’re potentially missing out on some of the quality assurance things that happen when a machine is used in the laboratory, with trained technicians who regularly test the machine and look after it. Point of care can mean that you devolve some of the responsibility for using it to part-time practitioners, clinicians, doctors, nurses, whatever; and basically they have no interest in how the machine is set up, they don’t calibrate it, they just want to go in, switch it on, test out. (William, senior manager)
In addition to compromising quality, moving testing procedures away from the laboratory has financial disadvantages. The laboratory can accommodate large machines capable of processing high volumes of patient samples, which can process test results at such low costs it is unlikely that any POCT could compete with them on economic grounds alone: Disadvantages are that [point of care] is invariably more expensive . . . It’s about critical mass . . . because from the point of view of a lab, my guess is that 90 percent of the expense of putting a sample through a lab is consumed through the first test. (Chris, senior manager and pathologist)
An ANT analysis shows how severing relations with the stabilising actants present in the laboratory can bring compromises to the quality and financial performance of diagnostic procedures. Yet, this is not to suggest that POCTs are never valuable within clinical settings. Quite conversely, several examples of successful POCTs can be found in the case study settings. The important consideration is that the compromises inherent in their use are outweighed by their advantages. Yet, using ANT alone it is not possible to prospectively explore how this might be achieved by a new POCT. Employing NPT draws the analysis in a different direction and provides a mechanism to enable such prospective research. Using NPT it becomes possible to take the detailed ANT analysis and ask what do we know about how these actants are connected that can indicate how it might expand to include a new technology?
The NPT mechanism of coherence emphasises that the use of a technology needs to make sense within the aims of work, and it is only possible for the benefits of the POCT device to outweigh the compromises inherent in its use if it is considered to make a discernible and meaningful difference to patient care. To this end, problematisation occurs within the coherence of service provision: it is about convincing actors within the setting of a problem that is preventing them achieving the aims of the service provision that can be redressed with near-patient delivery of test results.
Using NPT to interrogate the ANT data lifts it from its context of production to enable comparison across case study settings. Metaphorically, NPT shines a spotlight on specific parts of the network that ANT reveals, to suggest where the device might come into use. As is explored below, this revealed very different aims for patient care that use of the POCT device would have to support to successfully problematise service provision within the three settings: encouraging, moderating, and preventing access to services.
Encouraging access to services
The role of the GUM clinic is to reduce the incidence of sexually transmitted infections (STIs) through prevention, diagnosis, and treatment and, as there are many barriers to utilising sexual health services, coherence in the work of the department can be seen in the focus on broadening access. The perceptions of sexual health issues within wider society and misrepresentations of testing act as a particular disincentive for patients to use services: It’s not just the infections that are stigmatised; it’s going for the test that can be stigmatised . . . The old Chlamydia tests were a swab in the urethra; these tests are really stigmatised by patients. Patients talk about . . . how they don’t want to be examined because they don’t want something horrible put inside their genitals. (Anthony, GUM consultant and manager)
Anthony continues to explain that barriers to access are exacerbated for the vulnerable patient groups who are in greatest need of sexual health services: And for sexual health you’re talking about young people, we’re talking about ethnic minorities, we’re talking about gay men . . . they’re all groups that struggle sometimes to access health care. And have the highest rates of medical problems. (Anthony, GUM consultant and manager)
The consequences of untreated STIs give significance to the difficulties patients face in accessing sexual health services; STIs pose increased risks to the infected body over time if they remain untreated and present a public health risk from onward transmission. These risks are exacerbated by the capacity of the infections to remain asymptomatic, allowing them to be passed on unknowingly. The corollary of this is that service provision within the department is directed towards encouraging greater access, not just for the health of individual patients but also for the health of the wider community. Part of the effort to encourage access is focused on ensuring that services are sensitive to patients’ needs: Our key goal a couple of years ago was to make sure that patients stayed in the department as little time as possible . . . they went into one room, they saw one person ideally, and that all their tests were done in that room if possible . . . What tended to happen previously . . . patients come in, they get seen by a doctor, they go and sit back in the waiting area, they get seen by a nurse, they go and sit back in the waiting area, they get seen by somebody else. And it’s very tortuous, and time consuming, and it’s not very patient friendly. (Anthony, GUM consultant and manager)
However, those who willingly access services are considered to be the ‘tip of the iceberg’, as rates of undiagnosed infection within the community are high. Therefore, efforts to improve access are also directed at providing services outside of clinical settings: The idea isn’t to target GUM clinics, because they are relying on people having symptoms, or having the ability to access the service; it’s about going out into the community and somehow rolling out testing in an accessible and easier way. (Anthony, GUM consultant and manager)
To problematise service provision within the GUM department, the POCT device must be positioned as a way to improve access to services. In contrast, to problematise service provision within the AMU, it would have to demonstrate its ability to moderate patient access to services.
Moderating access to services
The AMU is an integral part of the hospital where all medical admissions are assessed to determine whether they should be treated within the hospital or managed at home. To this end, coherence within the unit centres on its strategic role in moderating patient access to hospital services. Because of this, the AMU has come to be conceptualised as ‘the front door to the hospital’: The phrase is the ‘front door of the hospital’; we’re part of that with the emergency department. So, virtually all admissions to the medical wards will come in through us first. So . . . they’re seen and assessed, we’ll turn around and discharge about 40 to 50 percent of those admissions directly, rather than going downstream to the medical wards. (Matt, AMU consultant)
The work of the AMU is an essential part of rationing limited resources within the Trust. When viewed in these terms, the AMU could be seen to serve an economic agenda, yet good patient care is at the very heart of service delivery within the AMU. Indeed, the AMU itself was created as a way of providing a better system for dealing with hospital admissions: [AMUs] came about through the NHS plan back in 2000 or 2001 in response to a lot of bad media publicity with regards to the way patients were being treated through the emergency departments. And that’s when the four-hour target came in . . . As a result of that, AMUs sort of came in, because there was no way that that volume of patients were going to be able to just be brought in and put in medical wards. (Dave, AMU senior nurse)
Government intervention to reduce waiting times for hospital admissions effectively destabilised the emergency department as the gateway for patients to hospital services. Indeed, the 4-hour target could only be achieved through the instigation of a new hospital department: the AMU. Examining the background to AMU in this way reveals a commitment to patient-centred care that remains at the centre of service delivery. The coherence of work within the AMU focuses on reducing the duration of patient stays, and therefore, to demonstrate relevance, the POCT would have to problematise the efficiency with which patients are managed within the department. However, to be relevant to TRC, the POCT device must enable action that can prevent access to services.
Preventing access to services
TRC provides services for patients with a range of respiratory disorders. As most of these are chronic disorders, work focuses on management and control, rather than cure. The coherence of service provision within TRC is directed towards preventing hospital admissions by supporting patients to manage their conditions at home. In this context, hospital admissions represent a poorly controlled condition in need of further intervention as Sarah explains in relation to asthma: Any admission to hospital for asthma is considered to be a failure of treatment for whatever reason. (Sarah, TRC nurse)
A central component of care is the intervention that is initiated after a hospital admission. Different conditions are managed in different ways. Asthmatic patients are followed up for a period of weeks after a hospital admission in a nurse-led clinic to help them get their asthma back to a controllable level: The asthma nurses will see those admissions during the course of their stay, and they will make sure that follow up is put in place . . . the nurses will see them up to 3 times for follow-up in the nurse led centre, and usually they’ll sort them out and discharge them back to their GP, but if the patients are proving more complex, they will send them back to our complex disease clinic. (Seth, TRC consultant)
Follow-up care for patients with chronic obstructive pulmonary disorder (COPD) is predominantly provided by a community nursing team: [Patients] get discharged by the community team, which is part of the community centre, and looked after for at least a 21 day period, and then handed back to their GP. And during that 21 day period the community team can ask [consultants for] advice, we can bring them into the centre, just to try and make sure we keep them out of hospital. (Greg, TRC consultant and manager)
To be relevant to TRC, the POCT device would need to problematise care by demonstrating that its use would prevent hospital admissions for patients with respiratory disorders in a way that is not otherwise possible.
Keeping NPT in tension with ANT in this way draws attention away from the details of the interactions between actants within the network to show that they can be categorised at the middle range as relating to coherence within the setting, which is valuable in understanding how a new technology might fit within this network. Using the theories together, it becomes clear that the POCT would have to be seen as a route to achieving very different outcomes in order to problematise care in the different settings. But what is consistent across the settings is that the benefits it claims to hold for service provision must come from its ability to provide new information at the point of care. If the benefits are not related to the point in time at which the test was delivered, then performing it at the point of care is irrelevant; it could just as well be performed in the laboratory without compromise. Through the combination of ANT and NPT, problematisation comes to be seen as more than the demonstration of the value of test results per se; it is the perceived relevance of receiving results at a specific time, within a specific location, in relation to the coherence within the setting.
The advantages of using the theories together are not just about navigating the focus on contingency inherent in ANT, equally ANT can be used to question an NPT analysis, drawing attention to the context within which the NPT mechanisms must be resourced. This is demonstrated by exploring how the relational ontology of test results affects the ability of POCT tests to contribute to the coherence of a setting.
Relational ontology of test results
To problematise service provision in the specific ways detailed above, the POCT device must provide relevant information that can be acted in the near-patient context. However, information is fluid (Moser and Law, 2006) and needs change between contexts. Comparing the context of the case study settings illustrates the contingency of information – test results that are valuable in one setting may be irrelevant to another, even within the same department.
In the TRC, near-patient delivery of currently available blood tests would have little significance for patient care, as they do not have a prominent role in treatment decisions. Although blood tests are used in the diagnosis and treatment of respiratory conditions, they are only one element of a range of information that informs treatment decisions: Usually you’ll assess [new patients] on the first appointment with a very thorough history . . . [it] probably wouldn’t make a huge amount of difference [to have blood test results available], because you’ve already formed your clinical opinion and the blood tests very much confirm, or occasionally refute it, or occasionally add something else into the mix. But they don’t shape your major decisions very often . . . There are one or two minor situations where it’s helpful . . . but if that was the case, I might wait for the blood tests and write to their referring consultant and say . . . the blood tests confirmed this, can you start [treatment]. (Seth, TRC consultant)
Conversely, Seth was more enthusiastic about the value of a POCT if it could offer a mechanism for altering treatment, as currently there is no reliable measure of treatment response: A point of care test that could give you the reassurance about the level of airway inflammation, I think that would be the Holy Grail in many respects . . . So a point of care test that can tell you: well actually the levels of inflammation in your airways is fine, you don’t need to be on these steroids, let’s really push you to get these down, can be very helpful. (Seth, TRC consultant)
In this instance, the availability of current tests within a POCT device would be of little relevance to the coherence of work in the setting as they would neither affect treatment decisions nor avert hospital admissions. To be relevant here, the POCT would need to provide new information to the consultation to inform treatment decisions, which would require the discovery of reliable measures of treatment response.
In contrast, the need for information within the community service of TRC is comparatively simple. In this context, the results of blood tests are occasionally required to implement treatment, and the location of patients outside of the hospital can result in logistical difficulties in obtaining them. In this context, an appropriately targeted POCT could have value: If we had [a POCT] we could say yeah, they’ve got a bacterial infection, we need to start them on something straight away. Otherwise, if we had to do a blood test, we’d have to go back to the hospital, send the bloods off, go back out to the community to see other patients, then go back to that patient depending on how long the bloods take to come back from the lab, to start them on antibiotics. (Chloe, TRC community nurse)
The location of patients, the role of blood tests in instigating treatment regimes, and the absence of easy access to the hospital laboratory conspire to position a POCT that moves blood tests from the laboratory into the home as a valuable resource in the quest to prevent admissions by enabling interventions to be initiated more quickly.
Although both of these situations arise within the same department, the determinants of ‘useful’ information – something that contributes to the coherence of work in the setting – are very different. Similarly, the value of information also varies between case study settings. Comparing the information required of POCTs within the AMU and the GUM clinic demonstrates the impact of the relational ontology of test results, with very different implications.
As the AMU assesses all medical admissions, it deals with a variety of patients and conditions. Although a common set of tests is indicated in most new admissions, the results only become meaningful in relation to other tests, which are specific to individual cases. Here, a POCT can only be useful if it provides all the results needed to make treatment decisions, yet this is difficult to achieve due to the variety of conditions seen within the unit: If there are a common set of tests that you do, which there definitely are for our [patients], then the advantages of having point of care [tests] are less if there are bits of that that can’t be done at point of care. Because, say for example, you have point of care machines that would do you a full blood count, and they’ll do renal function and liver function, but won’t tell you sodium or potassium . . . and then you say ‘well actually I’m going to wait for the sodium and potassium until I make any decision’, in which case you could argue, what’s the point of the point of care machines? . . . So if you wanted to produce something that could be used on every admission then it is quite difficult. (Matt, AMU consultant)
Conversely, in the GUM department, collective test results take on a very different meaning. Although patients in this setting are at risk of several STIs, providing rapid testing for the spectrum of infections at a single point in time is considered to have the potential to cause anxiety in patients: The population that we’re targeting are people who don’t have a test regularly at the hospital . . . and in a way we’re separating it by saying ‘right, today we’re testing for the HIV, we’ll have that back in 20 minutes . . . [it] will take about two weeks for the other results to come back’ . . . So I’m thinking if you’ve got somebody presenting, really concerned about HIV and then you’re going to say ‘and we’re going to give you your hep C, syphilis, hepatitis A, B at the same time’ that might freak them out completely. (Graham, GUM nurse)
In contrast to the AMU, where the relational ontology of test results destabilises a POCT that does not provide a complete set, in the GUM department the relational ontology of test results destabilises a POCT that does provide a complete set. Yet what is similar across these settings is the need for the POCT device to provide a complete set of results for the particular condition being tested for. If the device does not provide all of the results needed to inform the diagnosis, it has little value as a POCT. This is well illustrated in the case of syphilis. Although there is a recognised clinical need for a syphilis outreach testing service, one of the reasons this is not currently provided by the department is the lack of POCTs that can diagnose the infection accurately: There are [point of care] syphilis tests . . . but they can’t distinguish between an old syphilis infection and a current one . . . [Syphilis] is one of those infections that kind of hangs around in the blood, even though you might have treated it successfully . . . So any syphilis test I’ve known to be used in an outreach capacity . . . if it did come up as syphilis positive then you’d have to . . . check ‘have you had an infection and have you had it treated before?’ (Rob, GUM health advisor)
Although the specific requirements of information vary greatly between contexts, for the information to be ‘useable’ it must provide a conclusive result that can be acted on at the point of care; this is what determines the value of POCTs. The examples here illustrate the importance of using ANT to interrogate NPT. ANT pulls the analysis back from the middle range – from understanding the coherence of work that draws the network together – to illustrate the importance of understanding the micro-level interactions within the network.
Keeping ANT and NPT in tension in this way provides a range of resources to explore both a generalised and specific understanding implementation, which is essential in pursuing interventionist research. Applying this framework to the developing POCT device enabled a detailed understanding of if and how it might come into use in the different case study settings, with practical implications for its continued construction. These findings were fed back to the technical team as they were constructing the POCT device and information from the continued technical development informed the ongoing fieldwork. Despite its important implications for the technical construction of the device, the process of feeding this information upstream was challenging and obstructed by the dynamics of interdisciplinary working across the social and physical sciences. A detailed ethnographic analysis of this process is reported elsewhere (Lyle, 2017).
Conclusion
This article has argued that ANT and NPT can be combined to enable prospective research, and it is by keeping the theories in tension that the framework becomes practically applicable. Keeping tension between the theories has methodological advantages for the researcher. By using each theory to interrogate the data derived through the other, the analyst is guided to focus data collection in specific places, helping to ensure sufficient depth of data while drawing important boundaries around that which is pertinent to implementation.
The framework can, to an extent, also be used to unpack innovations that have already been implemented and ‘normalised’, or failed to be normalised, within a setting. Indeed, an important component of prospective research is in unpacking the processes of implementation for existing technologies to allow this learning to be utilised in the development and implementation of new innovations.
However, to develop workable technologies, the story must not end here. Just as the development of the technology is flexible, with the potential to be influenced by information from the field of use (but also by other agendas), so too may the context of use alter – there is nothing static about networks of actants. To understand and influence how the two might relate to each other, prospective research must be able to stay abreast of changes in both the development of technology and its field of use. In this way, attempts to bring technological development into alignment with the context of use must continue throughout the complete process of scientific development, eventually seeing the device through to implementation. The combination of ANT and NPT provides a framework capable of enabling this iterative approach.
This theoretical framework offers a resource for other researchers concerned with exploring the potential fit of innovations within social settings. By using this approach to explore implementation at an early stage, when technologies are fluid and adaptable, we would be in a better position to show how STS can offer what Zuiderent-Jerak (2015) calls situated interventions. To this end, although the outcomes of implementation are contextual and contingent on a variety of influences, this need not hold us hostage. It is possible to find a way to work around the uncertainty and contingency of implementation without denying it and resorting to reductionism. The combination of ANT and NPT can marry attention to the contingency of relational ontologies with a sense of the sedimented contexts within which these operate, offering a comprehensive approach to better understand how innovation processes in healthcare reflect these two dynamics at work. If we are to continue to rely on technological innovation to make changes in healthcare provision, and indeed other aspects of society, then we need to change the way we construct innovation; arguably interventional STS is the route to achieve this.
Footnotes
Acknowledgements
I would like to thank the participants for their time and contribution, and the anonymous reviewers for their helpful advice and insights. I would like to give particular thanks to Professor Andrew Webster who has read countless drafts, and offered sage advice which has been so helpful in shaping and improving this paper.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research on which this article is based was undertaken as part of a PhD funded by the Engineering and Physical Sciences Research Council.