
Abstract
Introduction
This study aimed to analyze the risk factors for varicella encephalitis in children and establish a predictive model.
Methods
This retrospective cohort study included a varicella encephalitis group (n = 75) and a varicella-non-encephalitis group (n = 135). Logistic regression analysis was employed to find risk factors for varicella encephalitis and create a predictive model.
Results
Older age, vomiting, poor mental status, and prolonged rash duration were independent risk factors for varicella encephalitis (p < .05). The predictive model for varicella encephalitis combined above four factors. The ROC curve of the predictive model showed an area under the curve of 0.955 (95% CI 0.925–0.986) for varicella encephalitis in children with a sensitivity of 94.7%, and a specificity of 86.0%.
Conclusion
Children with varicella who are older, experience vomiting, exhibit poor mental status, or have a prolonged rash duration should be closely monitored clinically. The predictive model combining these four factors demonstrates good predictive efficiency.
Introduction
Chickenpox, or varicella, is an acute respiratory disease caused by the varicella-zoster virus (VZV). It is common in children and highly contagious, mainly transmitted through respiratory droplets and direct contact. 1 . Studies show that from 2016 to 2019, China reported 3,047,715 cases of chickenpox, with an average annual incidence rate of 55.05 per 100,000, showing an upward trend year by year. The average annual incidence rates (per 100,000) of chickenpox in the age groups of 0–4 years, 5–9 years, 10–14 years, 15–19 years, and ≥20 years were 61.77, 308.14, 228.31, 97.69, and 12.43, respectively. 2
Chickenpox presents a series of symptoms that typically occur in stages. The initial signs include fever, often the first indication of the infection, accompanied by feelings of tiredness and headaches. Loss of appetite may precede the appearance of a rash by 1–2 days. The hallmark symptom of chickenpox is the development of an itchy rash that transforms into fluid-filled blisters, eventually forming scabs. The rash initially appears on the chest, back, and face before spreading across the entire body, including inside the mouth, eyelids, or genital area. This process usually takes about a week, during which the herpes gradually become scabs. Additionally, some individuals may experience stomachaches, which typically persist for one or two days.3–5
Although the disease usually has a good prognosis, it can cause a variety of serious complications, including secondary bacterial infections, pneumonia, encephalitis, gastrointestinal disorders, and Reye’s syndrome. 6–8 Among them, chickenpox encephalitis is relatively rare, but if it is not treated in time in children with chickenpox encephalitis, it can lead to serious sequelae such as hearing and visual impairment, paralysis of limbs and varying degrees of intellectual retardation in children, or even death. 9 Therefore, early recognition of chickenpox encephalitis has important clinical significance to prevent the adverse effects caused by it. This study explores and summarizes the risk factors for encephalitis in children with chickenpox in order to provide a reference for clinical practice and early recognition and intervention of chickenpox encephalitis.
Materials and methods
General information
Seventy-five cases of children diagnosed with varicella encephalitis and hospitalized at hospital from January 2016 to September 2021 were selected as the study group. Inclusion criteria were as follows: (1) meeting the diagnostic criteria for varicella encephalitis, confirmed through clinical symptoms, laboratory, and pathogen examinations; (2) complete clinical records, and no prior treatment received before admission; and (3) under 14 years old. Exclusion criteria were as follows: (1) individuals with other varicella complications (non-varicella encephalitis); (2) patients who deceased during hospitalization due to non-varicella encephalitis; (3) individuals with other types of infections or critically ill patients; and (4) those with severe primary diseases. During the same period, a total of 135 cases of children diagnosed solely with varicella (ICD code: 1E90) and hospitalized were randomly selected as the control group. This retrospective cohort study received approval from the hospital ethics committee of Xi’an Children’s Hospital (20240036). Written informed consent was obtained from the parents/legal guardians of any minors included in the study.
Diagnostic criteria of varicella encephalitis
The criteria for diagnosing varicella encephalitis 10 typically include the following points: sustained alterations in mental status for more than 24 hours without any other known cause; meeting at least two of the following criteria: fever exceeding 38°C recorded within 72 hours before or after the onset of symptoms; new localized neurological symptoms; increased cell count in cerebrospinal fluid; new neuroimaging findings suggesting encephalitis; and epileptic seizures unrelated to previous epilepsy.
Clinical information collection
The general clinical data of two groups of patients were extracted from the medical records, including gender, age, body temperature, vomiting (yes/no), seizures (yes/no), mental status, state of consciousness, neurological reflexes, number of days with rash, and laboratory indicators (including white blood cell count, calcitonin, C-reactive protein, and creatinine kinase-myoglobin binding (CK-MB). Univariate and multivariate analyses were conducted to identify the risk factors for encephalitis in chickenpox patients. A prediction model for pediatric chickenpox encephalitis was established and its predictive value was evaluated.
Statistical analysis
Statistical analysis was conducted using SPSS 25.0 software. Count data were expressed as frequencies (%), and intergroup comparisons were conducted using the chi-square test or Fisher’s exact probability test. Normality tests were conducted for continuous data. For data following a normal distribution, mean ± standard deviation (SD) was used, and intergroup comparisons were carried out using independent t-tests. For non-normally distributed data, median (P25∼P75) was used, and intergroup differences were compared using the Mann–Whitney U test. Logistic regression analysis was employed to identify risk factors for varicella encephalitis in children, construct a predictive model, and perform Omnibus tests on the model coefficients. The model’s predictive value was evaluated using the Receiver Operating Characteristic (ROC) curve. A significance level of p < .05 was deemed statistically significant.
Results
Comparison of general clinical data between two groups of patients
Comparison of general clinical data of children in two groups.
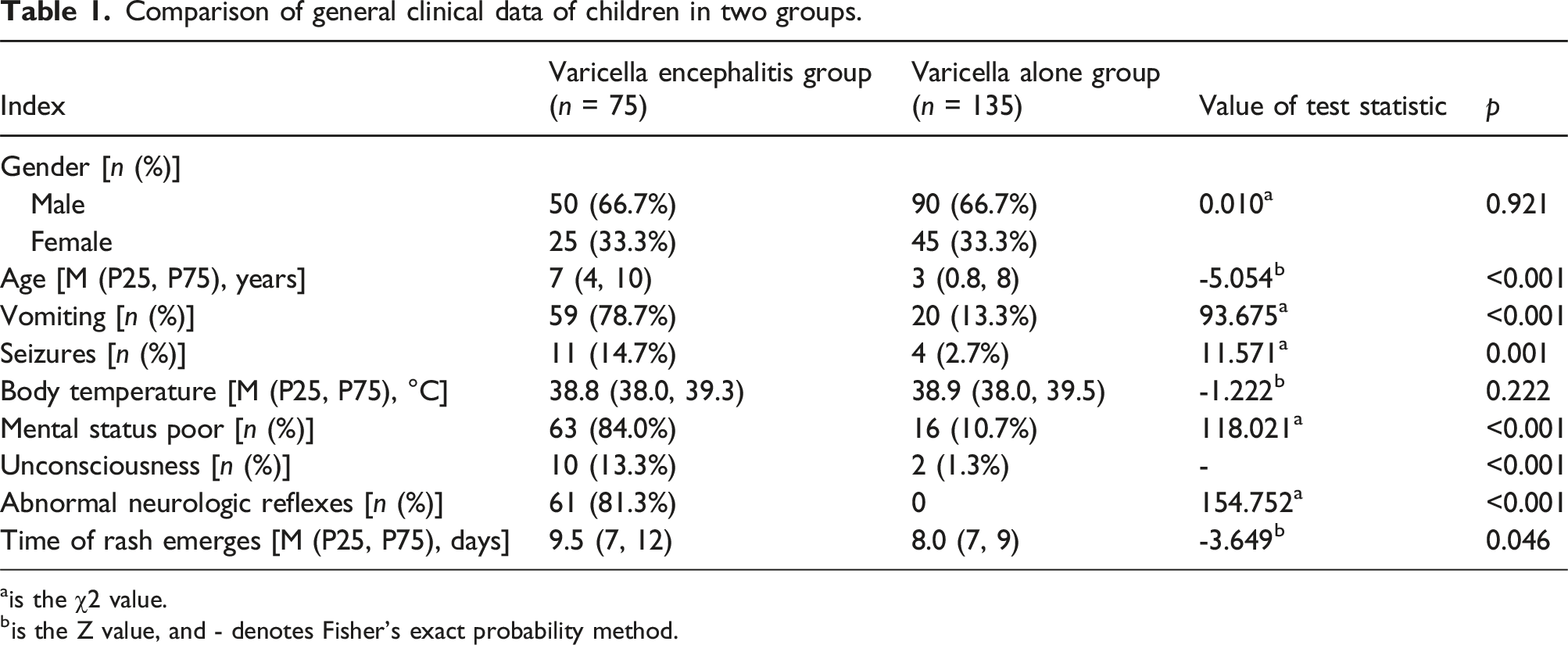
ais the χ2 value.
bis the Z value, and - denotes Fisher’s exact probability method.
Comparison of laboratory indicators between two groups of patients
Comparison of laboratory indices in two groups of children.

Note: WBC = white blood cell, CRP = C-reactive protein, PCT = procalcitonin, CK-MB = creatinine kinase-myoglobin binding (measured by enzyme rate method).
Multivariate analysis of varicella encephalitis in varicella patients
Risk factors for complication of varicella encephalitis in children with chickenpox.

a: CK-MB = creatinine kinase-myoglobin binding.
Establishment of the combined predictive model and its ROC curve
Predictive value of the joint prediction model for varicella encephalitis complicating children with chickenpox.

The Receiver Operating Characteristic (ROC) curve revealed an optimal threshold of 0.189, with a sensitivity of 96.0% and specificity of 85.3%. The area under the curve (AUC) was 0.955 (95% CI 0.925–0.986), indicating a high predictive value of the combined predictive model for varicella encephalitis (Figure 1). ROC curve of the joint prediction model.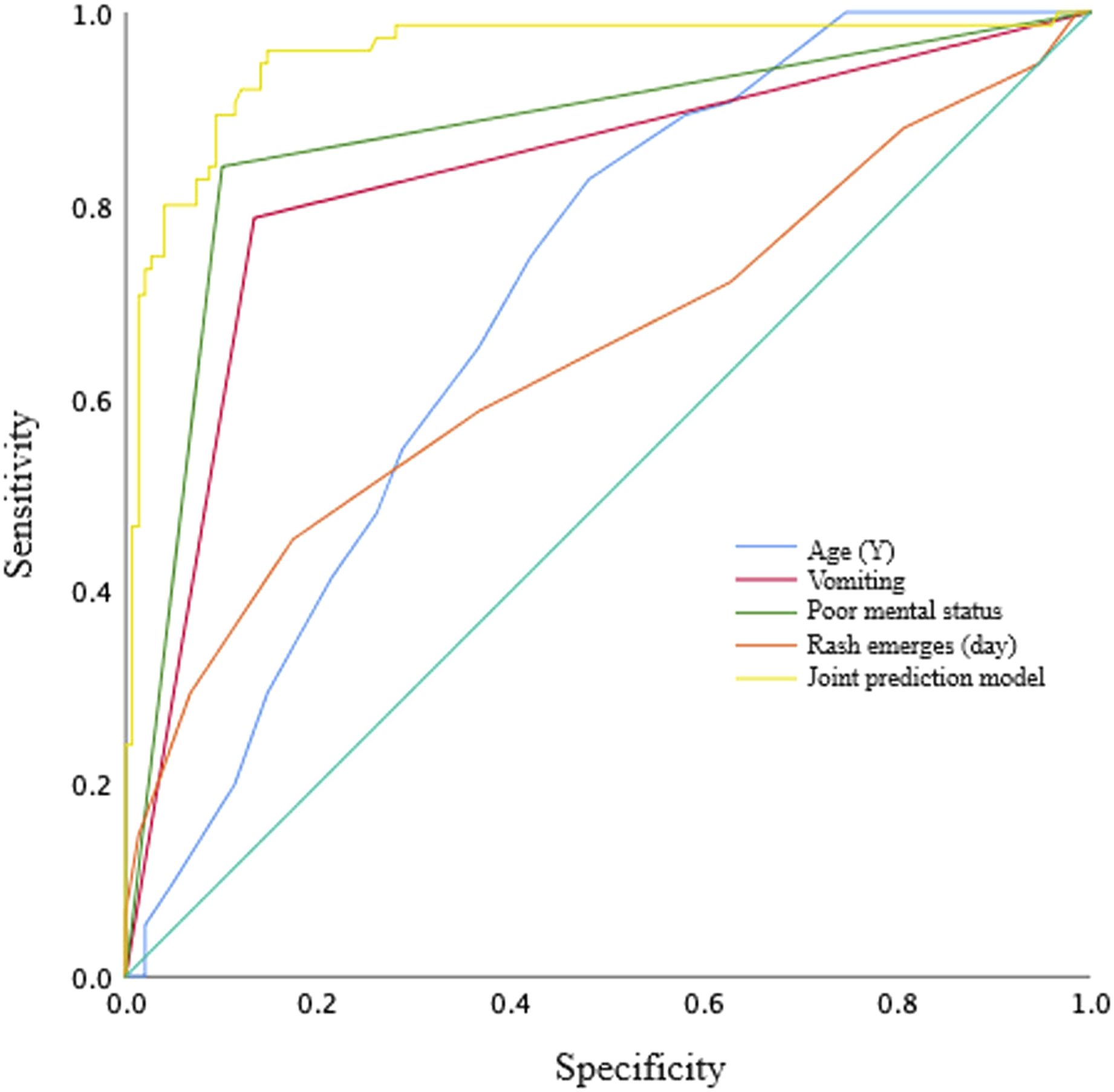
Discussion
This study employed a retrospective cohort design, starting with univariate analysis to identify statistically significant variables. Subsequently, logistic regression was utilized to analyze the risk factors for varicella encephalitis in varicella patients. The results revealed that compared to those without encephalitis, older age, vomiting, poor mental status, and prolonged duration of rash were all independent risk factors for varicella encephalitis. Vomiting, poor mental status, and extended rash duration often indicate a more severe condition in patients.
As an acute respiratory infectious disease, chickenpox has a higher incidence rate among children and is highly contagious. A small number of children with chickenpox may develop encephalitis, leading to pathological changes in brain tissue such as congestion, edema, necrosis, and permanent impairment of brain function, posing a serious threat to children’s life and health.11–16 This study showed a more serious symptoms in the patients with varicella encephalitis than those with only chickenpox.
Indeed, the study findings highlight a significant correlation between the onset of varicella encephalitis and various factors. The children of 1–8 years old are found to have a high likelihood of developing varicella encephalitis, as indicated by the pronounced negative correlation with age.17,18 Our study finds the age of varicella encephalitis group was median age of 10. Symptoms such as vomiting, seizures, poor mental status, unconsciousness, and abnormal neurological reflexes show a strong positive correlation with the disease, highlighting their clear association with varicella encephalitis.11–18 The appearance of rashes among patients occurs relatively quickly after the onset of the disease.11–18 Furthermore, elevated CK-MB levels (exceeding 18 U/L) are notably linked to the disease.11–18 These results underscore the pivotal roles these factors play in the diagnosis and prognosis of varicella encephalitis in children.17,18 In comparison to similar studies, our findings align with existing literature that emphasizes the importance of early recognition and prompt treatment in managing this serious condition.
The specific prediction models for varicella encephalitis are not commonly found in the literature. Most studies focus on understanding the epidemiology, clinical manifestations, and treatment outcomes of varicella encephalitis.19,20 However, the construction of a prediction model for varicella encephalitis in children would be a valuable tool for early identification and intervention. Such a model would likely incorporate various factors such as age, immunization status, presence of underlying health conditions, and severity of initial symptoms.19,20 The incidence of varicella encephalitis is relatively low and it is clinically rare. The symptoms at the onset may not be specific and can easily be overlooked by clinicians. In addition, there is a lack of consistent diagnostic criteria for varicella encephalitis, and it often needs to be confirmed by clinical symptoms, laboratory indicators, and imaging examinations, which can lead to delays in examination and treatment of the disease. If the condition of the child continues to develop, it can cause brain damage, disability, or even death.11–18 In clinical practice, patients with varicella presenting symptoms and/or signs suggestive of encephalitis (such as headache, seizure, and altered consciousness) should undergo additional tests (e.g., CSF analysis and brain MRI) to confirm or rule out the diagnosis of encephalitis. This predictive model could only be a reference tool for doctors to prevent the acute attack of varicella encephalitis. When the risk factors emerged, the doctors should proceed with additional tests as soon as possible to confirm the diagnosis of encephalitis.
Building upon the analysis of risk factors, this study established a predictive model for varicella encephalitis in varicella patients. This model aimed to predict the occurrence of varicella encephalitis by analyzing early disease risk factors. The area under the ROC curve for this predictive model was 0.955 (95% CI 0.925–0.986), exceeding 0.900, indicating excellent predictive performance. 21 The overall omnibus test for the model coefficients (χ2 = 178.085, p < .001) further affirmed the high predictive efficiency of this model.
However, it’s important to note that this predictive model was derived from retrospective analysis conducted at our center, which may have possible biases. While internal validation showed promising results, external validation was not performed. Therefore, future research necessitates collaborative efforts among multiple centers, incorporating additional variables, to enhance the clinical feasibility verification of the predictive model for varicella encephalitis in pediatric varicella patients.
Conclusion
Advanced age, prolonged rash duration, vomiting, and poor mental status have been identified as independent risk factors for varicella encephalitis in varicella patients. These factors should receive special attention in clinical practice. Furthermore, the predictive model based on these four factors demonstrates significant predictive value. It holds promise for application in clinical settings, aiding in the early identification and timely intervention of varicella encephalitis, thereby improving patient outcomes. This model possesses crucial clinical significance.
Footnotes
Author contributions
CW: conceptualization, methodology, validation, investigation, data curation, resources, writing original draft, review and editing, and project administration. LT: conceptualization, formal analysis, investigation, data curation, writing original draft, review and editing, and visualization. DG: conceptualization, formal analysis, investigation, data curation, writing original draft, review and editing, and resources.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
Data availability statement
The datasets are available from the corresponding author on reasonable request.