
Abstract
Bipolar disorders are among the most severe mental illnesses. The onset of the disorder is frequently preceded by phases with subsyndromal symptoms. In Germany, psychiatric early detection centres provide prevention services for help-seeking young people which focus on risk research. This article considers how music therapy contributes to the indicated prevention of bipolar disorders in preparation for a qualitative research study. The article presents a narrative literature review on research into early detection and prediction in bipolar disorders and approaches to prevention. The rationale for the use of music therapy in this context is discussed, with consideration of research questions leading to the next stage of the study.
Keywords
Introduction and methods
Mental health conditions that impair the quality of life may develop over a period of time until they are assessed as a disorder according to internationally recognized diagnostic category systems (Eaton et al., 1995; Klosterkötter, 2008). This is why the World Health Organization (WHO, 2004) has designated prevention as one of its main objectives. Depending on the target group and objective, prevention approaches can be classified as universal, selective or indicated prevention (Gordon, 1983). The present narrative literature review deals with indicated prevention, which has so far received less attention in music therapy. It examines the question of the contribution music therapy can make in the context of indicated prevention in order to support individuals at risk for bipolar disorders.
First, the findings of psychiatric risk and prediction research are outlined and available early intervention efforts described, based on a database search and expert consultations in the framework of a German early detection centre in 2018. A systematic database search supplemented by hand searches is then described to determine whether there are specific intervention concepts or prevention approaches to be found in music therapy literature in relation to the topic under question. The potential of music therapy within the framework of indicated prevention of bipolar disorder will be explored and discussed.
The theoretical orientation of the author is based on a psychodynamic music therapy approach (Metzner, 2016), which integrates developmental theories, attachment theory and theories of affect regulation and mentalization (Allen et al., 2008; Fonagy et al., 2015).
What does it mean to be ‘at risk’? Research on the early stages and predispositions of bipolar disorder
Bipolar disorders are among the most severe mental illnesses, and can place a huge strain on the individuals affected and those around them for long phases of their lives. They are often chronic, with a high number of relapses, an increased risk of suicide (the mortality rate from suicide is 15%), and severe impacts on the general state of health and functioning of those affected (Bingmann et al., 2016). The lifetime prevalence for all illnesses on the bipolar spectrum is about 3%, and the average age of onset is 19 (Pfennig et al., 2017a).
Bipolar disorder involves episodic shifts between depressive and manic phases or – in attenuated form – hypo-manic phases, which are characterized by swings in mood on one hand and in the level of drive and activity on the other (Angst, 2013). The bipolar spectrum encompasses not just bipolar I and II, but also other diagnostic criteria (Marneros, 2004: 26, 27). Because of this diversity, a correct diagnosis – and thus the beginning of the indicated therapeutic measures – is often only made long after the first symptoms, on average after 8 to 10 years (Seemüller et al., 2010). There are indications that the onset of full bipolar disorder is preceded, in most cases, by phases with less severe symptoms, which are the starting point for early detection and prediction research (Bingmann et al., 2016; Pfennig, 2012).
Strategies and findings of research on early detection and prediction
Psychiatric early detection and prediction research has particular challenges. For example, a high degree of diagnostic care is required to distinguish a subthreshold and symptomatic high or low mood from normal fluctuations in the context of adolescent development, or from the symptoms of attention-deficit hyperactivity disorder (ADHD) (Grimmer et al., 2010). In addition, the overlap between the early symptoms of this and other mental disorders (especially depression and psychoses) means that a transdiagnostic perspective is always needed in early detection and early intervention.
In over 50% of cases, bipolar disorders begin with a depressive episode (Bingmann et al., 2016), but the criteria justifying a bipolar disorder diagnosis are only fulfilled once a (hypo-)manic episode has been observed. As a consequence, there is discussion about whether an initial depressive episode should be classed as a risk factor for bipolar disorder or is already defined as part of bipolar disorder (determination of the point of conversion 1 ). More research is also indicated to ascertain whether signs predicting bipolar disorder can be identified within a depressive episode (Bingmann et al., 2016). In relation to the risk of psychosis, Pfennig notes that with regard to the precursors of bipolar disorders, ‘several symptoms with various qualities and dimensions must be observed simultaneously, which in some cases change episodically in the transition from precursors of the illness to its manifestation’ (Pfennig, 2012: 898). Thus, risk monitoring is characterized by a high degree of complexity.
Initially, early detection research used retrospective data collection methods based mainly on a survey of diagnostically confirmed patients with bipolar disorder and their family members. This made it possible to detect specific clusters of less severe symptoms and thus to investigate the occurrence of bipolar prodromes. 2 Since the validity of these results is limited due to memory bias in the context of the survey, prediction research is increasingly focusing on prospective methods. These use ‘real-time’ observation of subsyndromal phenomena to make nuanced statements about the nature and forms of progression of at-risk symptoms (Bingmann et al., 2016). Prediction research also examines biomarkers, with the aim to measure genetic predispositions and neurobiological changes which are, for example, associated with cognitive deficits or with changes in circadian rhythm. For an overview of this research, see Walker et al. (2014).
There is scientific consensus that the following factors increase the potential risk of suffering from bipolar disorder (Pfennig et al., 2017b: 214 onwards):
Biological risk factors: positive family history, 3 changes in sleep, changes in circadian rhythms
Environmental factors: stress, difficult family/educational environment, low socio-economic status, critical life events
Subclinical/clinical factors: manic symptoms, depressive episodes, atypical patterns of depression, (hypo)manic symptoms in connection with antidepressants.
Other factors contributing to a risk profile for bipolar disorders are drug abuse, a current or past diagnosis of ADHD, irritability, impaired psychosocial functioning, and particularly high levels of affective responsiveness and anxiety (Pfennig, 2012: 900). Both Pfennig (2012) and Leopold et al. (2013) mention the degree of creativity as a characteristic associated with risk. In a study by Burkhardt et al. (2019), creativity was measured among 38 persons at risk for bipolar disorder using the Barron–Welsh Art Scale (BWAS; Barron, 1963) and the Creative Achievement Questionnaire (CAQ; Carson et al., 2005). The findings show, that ‘there is evidence of increased creativity, but not of higher creative achievements, in persons at-risk of bipolar disorder. Mood swings are highly associated with creativity’ (Burkhardt et al., 2019: 1). These authors suggest that creativity should be further analysed regarding its predictive value and should ideally be addressed in the therapeutic process. The transferability of the methodology used by Burkhardt et al. and the results of the study to music therapy is questionable; however, it is beyond the scope of this article to consider this further.
As a result of these research efforts, structured, standardized early detection tools have been developed for people experiencing symptoms which measure the risk of developing a bipolar disorder in the future (Bechdolf et al., 2010; Correll et al., 2014; Leopold et al., 2012). These tools have not yet been used to assess resilience factors, as they have not yet been sufficiently studied in the context of research on bipolar disorder. In order to develop specific early intervention measures, it is important to understand the mechanisms behind both the protective aspects and any challenging development conditions in the etiopathology of bipolar disorders. Pfennig et al. (2017b) list characteristics which may have a potentially protective effect on mental health in general. These are functional emotional regulation, reliable social relations, awareness and management of stress, and lifestyle factors such as physical activity (p. 216).
Findings about premorbid personality and vulnerability connected to bipolar disorder
An understanding of the specific predispositions and conditions for the onset and persistence of bipolar disorder is essential for Music Therapists in considering the bio-psycho-social context of the client. Therefore, findings from neurobiology and cognitive and emotional psychology will now be presented and supported by psychodynamic perspectives on the development of bipolar disorder.
First, Böker et al. (2016) describe findings on the hyper-reactivity of the emotion-processing networks in the brain. Research on emotion regulation shows that a heightened emotional reactivity is connected with a limited cognitive control of emotions and consequently leads to dysfunctional regulation processes that can be observed both in the acute episode and in remission (Wolkenstein et al., 2017). This tallies with findings which have also shown evidence of structural and functional changes on a neurophysiological level in both the acute and remitted states, changes which are associated with the cognitive and psychosocial impairments of bipolar patients (Grimm, 2014). Comparable differences have been found between persons at risk of bipolar disorder and control groups in their responsiveness to positive and negative emotional stimuli (Heissler et al., 2014).
The findings of a controlled study by Choppin et al. (2016) provide useful insights for music therapy. The authors considered the emotional reactions of individuals with bipolar disorder in the euthymic phase, using pieces of music which trigger complex emotions. The study participants (experimental group n = 21; control group n = 21) were asked to indicate on a 9-point visual analogue scale (referring to the Geneva Emotional Music Scale by Zentner et al., 2008) what emotion they strongly perceived while listening. The results of this study confirm the model of emotional hyper-reactivity in bipolar disorder. However, it is striking that in the case of musical extracts where mood level was previously assessed as positive by the independent raters, the individuals with bipolar disorder generally described the affect they experienced as sadder than the control group. Choppin et al. (2016) surmise that patients had trouble processing or regulating the positive affect and therefore associated positive stimuli with distress, which was experienced as a negative (sad) affect. It is possible that the ambivalence in emotion regulation and the resulting distress also reveals a conflict regarding the evaluation of mood states, as Backenstrass et al. (2012: 198) observed. Gross (2014) refers to studies showing that bipolar disorder is associated with rumination on negative and positive affect, but criticizes the lack of longitudinal studies on the use of emotion regulation strategies that focus on the high-risk stage of the disorder. An important question is whether the use of maladaptive strategies precedes the onset of the disorder or whether it should be valued merely as a symptom or epiphenomenon of bipolar disorder (Gross, 2014: 413, 414).
There are also approaches which examine the connection between genetically determined temperament types and the occurrence of bipolar disorder (Akiskal, 1996; Kochman et al., 2005; Maute, 2002), but this link has not yet been sufficiently proven. Other authors argue that bipolar disorder is caused by a genetic vulnerability, which is responsible for the fact that ‘[neurobiological] mechanisms or rhythms easily become unbalanced and dysregulated’ (Hautzinger and Meyer, 2007: 1249). In contrast to previous writing on emotional regulation, dysregulation in this context does not refer to mood, but to the regulation of activity and drive. Any change (e.g. because of shift work or time difference) influences both motivational processes and the level of activity. In the case of insufficient regulation, this does not return to the initial level, but increasingly spirals ‘into mania or depression’ (Hautzinger and Meyer, 2007: 1249).
Böker et al. (2016), writing about the neuropsychodynamics of the manic syndromes, refer to studies on the premorbid personality of those affected by a manic syndrome. These are, however, somewhat ambiguous. Kraus (1991) considers that the premorbid personality of individuals with bipolar disorder includes characteristics like hypernomic behaviour and an intolerance of ambiguity associated with a longing for harmony and avoidance of conflicts in partnership. These characteristics maintain the regulation of self-esteem and the external identity (Kraus, 1991: 49f.). Mentzos (2006) understands mania not just as an ‘antidepressive mechanism’ but much more as an ‘alternative solution equivalent, but contrary, to depression’ which in situations of impeded life goals serves as ‘revocation of obedience’ (p. 134) to the strict super-ego. According to Schwarz (2014), individual ‘emancipatory themes’ are expressed in mania, which can also be understood as creative attempts to take developmental steps (e.g. low individuation or detachment from early relational dependency) that should be supported therapeutically.
Challenges emerge in three psychosocial areas when considering the causes of bipolar disorder: first, with regard to the regulation of emotions and mood, second, the regulation of activity and drive, and third, relationship processes and identity. These areas represent focal points for therapeutic and preventive intervention in bipolar disorder but are not specific to the condition. They illustrate a dimensional or continuum view of mental phenomena that makes it possible to maintain a necessary diagnostic uncertainty with regard to early subsyndromal processes. This view is also reflected in a transdiagnostic approach (Brown and Barlow, 2009; Sauer-Zavala et al., 2017), which refers to underlying mechanisms that are relevant across a class of disorders, thus offering benefits in the treatment of complex mental health conditions, especially considering the frequent comorbid relationships between mood and anxiety disorders (Ellard et al., 2017).
Early intervention: characteristics and objectives of indicated prevention for people at risk of bipolar disorder
Besides its focus on prediction, research on early detection is concerned with developing prevention measures. Indicated prevention is part of primary preventive approaches and is targeted at people with a high risk of illness, who may already be experiencing mental health challenges that range below the diagnostic threshold (see above; Klosterkötter and Maier, 2017: 22). Indicated prevention falls between the field of prevention and that of acute treatment (see Figure 1).
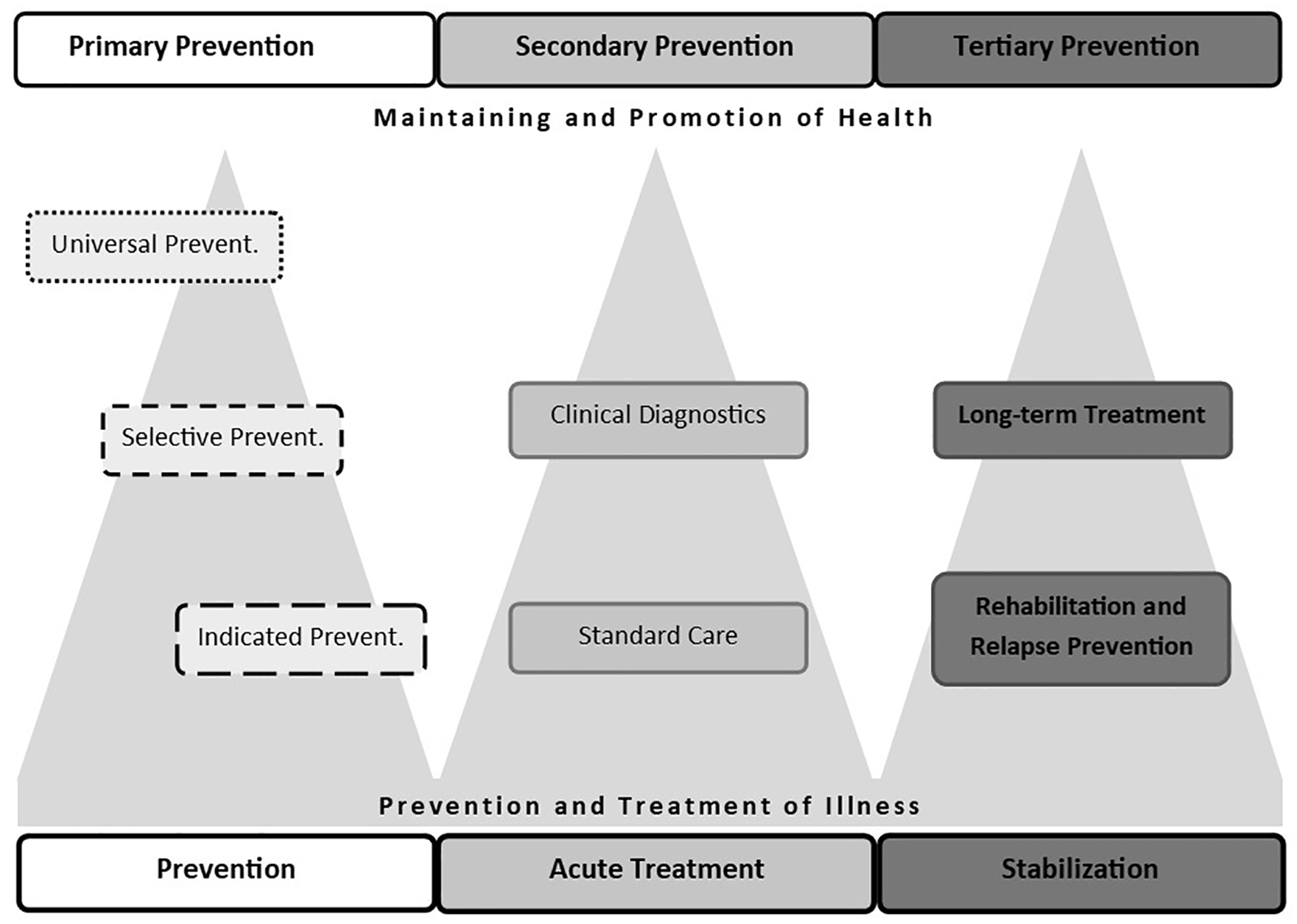
Integrative classification system for prevention objectives: the prevalent terms of the Public Health model from the 1950s on the top, compared to the terms following the Gordon model (1983) at the bottom.
The concept of indicated prevention, introduced in 1983 (Gordon, 1983), came from the need to examine more closely the border area between primary and secondary preventive objectives and thus creates a transition between these areas. Due to its focus on at-risk groups, the concept of indicated prevention makes it easier to develop specific preventive measures, to justify their use and to monitor their success (Klosterkötter, 2013: 1299). Besides the advantages of this shift for health policy, and the undisputed benefits – for the individual and for society – of being able to intervene as early as possible where there is a high risk of illness, prediction research and indicated prevention also present numerous ethical difficulties. Two problematic areas are discussed here as examples.
First, if the people concerned are informed about their increased risk of illness within the prediction process, this can lead to psychological stress. Here preventive measures should be deployed in such a way that they relieve stress and prevent stigmatization. It is important to ensure that individuals are not left in an uncertain state between sickness and health, and that the positive test result does not act as a self-fulfilling prophecy. Experiences from the early detection of psychosis show that it is sometimes a relief for those affected if their previously confusing complaints are given a name, and possible courses of action are suggested (Fangerau, 2017; Schultze-Lutter et al., 2017).
Second, individuals may be assigned to an at-risk group because of their combination of symptoms, but do not ultimately develop bipolar disorder. If this group of people is to be given treatment that may have side effects, this requires appropriate education and individual counselling (see below).
According to Pfennig (2012), the aims of indicated prevention strategies for people who are at risk of bipolar disorder are to reduce symptoms and stabilize the level of functioning, and to prevent or at least delay conversion to a full bipolar disorder diagnosis (p. 897). Other objectives are to shorten phases where the illness goes untreated and to have a generally positive impact on the course of the disorder.
In the framework of psychiatric care in Germany, indicated preventive work is carried out by early detection centres. Part of the focus here is wide-ranging publicity and education work as well as anti-stigma work. This significantly lowers the inhibition threshold for seeking or offering help (Pfennig et al., 2017b: 223), including anonymous access to initial support services, if required (Leopold et al., 2013).
The symptom-oriented measures of early intervention are subject to a careful risk-benefit analysis. Preference should be given to interventions with minimal side effects, which take a transdiagnostic approach and ‘can be assumed to have general benefits’ (Leopold et al., 2013: 1313). Information and education with regard to risk status and support available to individuals is seen as essential. Besides low-threshold psychotherapeutic approaches such as psychoeducation, sleep hygiene and mindfulness, there are now studies proving the effectiveness of cognitive-behavioural therapy (CBT), family-focused forms of therapy, and interpersonal and social rhythm therapy (IPSRT) (Goldstein et al., 2014; Schaub and Neubauer, 2013). No literature could be found on the use of creative therapeutic provision in the context of early intervention at bipolar disorder.
What do we know about music therapy in the treatment and prevention of bipolar disorder? The state of research
This section will first consider the knowledge available about music therapy treatment of bipolar disorder. Concepts of prevention in music therapy and their suitability for indicated prevention will then be examined.
Research on music therapy in psychiatry focusing bipolar disorder
Music therapy is a component of multi-disciplinary psychiatric treatment that has become established as a form of treatment for a variety of mental health conditions in both group and individual settings, particularly in the area of inpatient care (e.g. De Backer, 2008; Erkkilä et al., 2011; Metzner, 2014). Empirical research has shown the effectiveness of music therapy for severe mental health disorders, with at least three studies having inclusion criteria encompassing bipolar disorders (de l’Etoile, 2002; Gold et al., 2009, 2013). The described effects are mainly the reduction of negative symptoms and anxiety, and the improvement of general functional capacity and vitality. Systematic Cochrane Reviews including randomised controlled trials (RCT) and controlled clinical trials (CCT) have been undertaken for music therapy on schizophrenia (Geretsegger et al., 2017) and unipolar depression (Aalbers et al., 2017). Geretsegger et al. included 18 studies with a total of 1215 participants showing evidence of at least low to moderate quality over the short and medium term. Aalbers et al. included nine studies with a total of 421 participants indicating that music therapy provides short-term beneficial effects for people with depression. So far, there have been no specific effect studies for the spectrum of bipolar disorder.
A systematic database search in October 2018 of PSYNDEX, PubPsych, PubMed, Livivo and ScienceDirect, supplemented by manual searches in e-journals and library catalogues for the terms ‘music’, ‘music therapy’, ‘bipolar’, ‘bipolar disorder’, ‘mania’ and ‘hypomania’ (using wildcards or truncation) produced 11 subject-related hits.
There are four pieces of literature that consider the influence of music or music activity which are pertinent to the discussions about the connection between bipolarity and creativity noted above. Within theoretical discourses, Angeler (2018) addresses analogies between heavy metal music and bipolar disorder, and Schriewer and Bulaj (2016) discuss the use of music streaming services as adjunct therapies within bipolar disorder. The following authors provide empirical data: Lim et al. (2013) showed that during an interview, inpatients experiencing a manic episode were more willing to sing on demand than inpatients who had schizophrenia, and the study of Choppin et al. (2016) concerned emotional hyper-reactivity in bipolar disorder (see above). However, none of these articles make a link to music therapy as a form of treatment.
In addition to the three studies mentioned above, only four other articles address the use of music therapy interventions for bipolar disorder. Mastnak (1991) writes about group therapy with manic inpatients and his ‘polyesthetic approach’. The aim of the ‘percussion and movement improvisation’ was to improve the social interaction on the ward. His observations of patients’ expressive and interactive behaviour in relation to their mania are described in detail, but are not supported by empirical data. According to Mastnak, group therapy resulted in an ‘increasingly realistic self-assessment’, ‘socially more mature relationships’, a ‘decrease in dysphoric behaviour’ and a ‘desire to become more deeply involved with music and the instrument’ (p. 195). In a short report by Leonhardt-Günther (2008), group therapy for bipolar patients in a psychiatric outpatient clinic is described. Music therapy is mentioned as part of the overall concept, but neither the specific procedure nor its effects are described in detail. An explorative study of D’Abbadie de Nodrest et al. (2017) investigated the effects of a music therapy programme for individuals with long-term depressive and/or bipolar disorder on awareness, defence mechanisms, extent of depression, emotional capacity and body change. An improvement on all these levels is reported by the authors, which needs to be proven in a long-term study. Finally, an ongoing study by Lund et al. (2017) is investigating the extent to which the use of a ‘sound pillow’ with quiet music improves the quality of sleep and quality of life of people with bipolar and unipolar depression with sleep difficulties. The findings have not yet been published.
Therefore, although it can be seen that there is potential in music therapy to treat people experiencing bipolar disorder, there is a lack of literature and even less empirical data regarding appropriate interventions.
While the national guideline for the assessment and management of bipolar disorder in the United Kingdom (NICE, 2014) does not yet include arts therapies in the recommendations at all, the German equivalent (DGBS and DGPPN, 2019) rightly problematizes the lack of evidence of the effectiveness of music therapy, but assumes that it has the potential to boost ‘affect regulation, self-esteem, and social competence’ (p. 104). In the framework of a recommendation on good clinical practice, the use of music therapy is recommended, and is mainly mentioned in relation to maintenance of a balanced mood and the prophylaxis of severe phases of illness. 4 In the German treatment guideline for psychosocial therapies in cases of severe mental disorders (DGPPN, 2019), that include, among others, the treatment of bipolar disorders, the arts therapies have been given a mid-level recommendation due to inconsistent findings (p. 42).
It can be noted that there is a need to develop and evaluate concepts of music therapy intervention, in the context of both prevention and treatment of manic-depressive patients.
Research on music therapy and prevention
A further database search for the terms ‘music therapy AND prevention’ (November 2019) mainly generated models and studies relating to the area of child and youth care. Here, educational settings such as schools and special education schools constitute a growing field of prevention initiatives based on music therapy (Jordan et al., 2018). It is stressed that music therapy prevention work in these settings must be distinguished from educational support, in terms of both content and personnel (Heye, 2018). For example, music therapy is only used when it becomes necessary to alleviate or combat stresses, complaints or even symptoms. 5 These initiatives are classified as primary prevention. There are also publications that highlight the potential of music therapy in secondary prevention (e.g. as an anxiety-reducing supplement to treatment for somatic illnesses) and tertiary prevention (e.g. relapse prevention or long-term support in mental health). However, these will not be discussed further here.
In the following section, an attempt will be made to differentiate music therapy initiatives according to levels of ‘selective’ and ‘indicated’ prevention (Gordon, 1983).
A large proportion of music therapy offered outside hospital settings can be classified as selective prevention. Target groups are, for example, children and adolescents from migrant backgrounds or socially disadvantaged milieus (Lee and Chong, 2010; Weyand, 2012), who have experienced violence and (at least suspected) traumatization (McFerran and Wölfl, 2015); girls on the cusp of puberty (Prechtl, 2018); and children or adolescents whose parents or siblings have had cancer (Zimmer, 2012). They can be assumed to be vulnerable to psychosocial problems as a result of their experiences, but they do not necessarily show symptoms yet. Here music therapy has a stress-relieving, supporting and resilience-fostering function.
One area in which music therapy work can be regarded as indicated prevention in the narrower sense is neonatology, where music therapy acts as early intervention in order to mitigate the high risk of developmental and attachment deficits due to premature birth (Nöcker-Ribaupierre, 2007, 2012). In addition, approaches taken in response to specific cognitive difficulties can be found in the music therapy support programme for children with attention problems described in Rothmann and Hillmer (2015) and in the discussion of music therapy for children and adolescents with mental health challenges in Stegemann (2018). These approaches can be placed within the framework of indicated prevention, for the function of music therapy is to alleviate symptoms, strengthen resources and support regulation, and it is used in response to a heightened risk of illness.
Two recent investigations appear to be highly relevant to the focus of this article. First, a cluster-randomized trial of Gold et al. (2017) investigated the effects of group music therapy as a preventive intervention for young people at risk compared to self-directed music listening. Participants (children aged between 13 and 15) were recruited and treated in schools. The individual risk of developing mental health problems was assessed using primarily the ‘Healthy-Unhealthy Music Scale’ (HUMS, Saarikallio et al., 2015) supplemented by measurement of depressive symptoms, psychosocial well-being, the tendency of rumination or reflection, and personality traits. Both study groups showed improvements without significant differences in change. Second, Aalbers et al. (2019) recently published the development of a manualised short-time intervention called ‘Emotion-regulating Improvisational Music Therapy for Preventing Depressive Symptoms’ (EIMT-PD). The intervention addresses young adults (aged 16–40) with the aim of reducing depressive symptoms (assessed by using a self-report inventory) through the focus on emotion regulation. It is offered in an outpatient community setting. The results of an associated investigation are awaited. It therefore could be shown that indicated prevention in the sense of Gordon’s (1983) model is already applied in music therapy, although the term ‘indicated prevention’ is not used. The reasons for this will be examined in more detail below.
What considerations must be made regarding a music therapy approach in the indicated prevention of bipolar disorders?
When developing an intervention approach for indicated prevention, there should be a focus both on a so-called target condition (here: bipolar disorder) and take into account the diagnostic vagueness of the subsyndromal experiences. Music therapy must therefore find a balance between two seemingly contradictory perspectives: the categorical descriptions (on which risk assessment is based and which targets interventions) and other dimensions of mental health (such as relational and emotional processes that are not specific to a single diagnosis). The following four points show how music therapy can provide an intervention within indicated prevention of bipolar disorder. According to a psychodynamic music therapy approach (Metzner, 2016), the capacity for creative expression and dialogue is an individual resource that can be (re)activated in the co-creative processes of therapy (BCPSG, 2005), accompanied by verbal reflection within a therapeutic relationship. In improvisational music therapy, music serves as an interpersonal means for communication, but is also ‘considered to portray meaning and to give the individual the feeling of being mirrored, accompanied, and even personally understood’ (Metzner, 2016: 448). These authors consider that music therapy contributes to the development of an authentic and balanced self, enabling healthy relationships with oneself and others. Therefore, music therapy can be seen as a form of treatment that can be adapted flexibly and actively to the individual circumstances, and thus carries few side effects. This shows the potential of music therapy to the topic of this article.
Assessment
The term ‘indicated prevention’ defines an aim to prevent or at least delay crossing a diagnostic threshold, taking into account that prediction may be uncertain and with a careful assessment of risk. Specific early detection instruments for bipolar disorder already exist which assess current symptomatology and risk factors (see previous references). With the HUMS-Scale, Gold et al. (2017) are using an outcome measure developed for music therapy that measures the extent to which the use of music is experienced as helpful or not helpful, for example, with regard to emotion regulation. So far, there are no comparable instruments for assessing the risk symptoms of bipolar disorder in the context of music therapy, in which the three aforementioned psychosocial areas are brought together, which is certainly a relevant objective for further research. It would be a valuable contribution to prediction research if individual patient resources and protective characteristics could be assessed in the context of music therapy.
Target group
Early symptoms can be experienced with a latency ranging from a few months to several years before manifestation of a bipolar disorder (Bingmann et al., 2016: 144). As the average age of onset for bipolar disorder is 19 years, these symptoms potentially develop in both adolescence and young adulthood. Phases of life characterized by upheaval and change are associated with an especially high risk of illness. Pfennig et al. (2017b) identify the years from 15 to 30 as the vulnerable age for risk symptoms for bipolar disorder (p. 218). Within the music therapy literature on existing concepts of prevention (referred to above), there is some overlap in terms of the adolescent target group. Young adulthood (18+ years) is only considered in the recent intervention mapping study of Aalbers et al. (2019), and therefore still constitutes an under-served group in terms of preventive work using music therapy. One reason for the lack of knowledge about young adulthood which can be observed across disciplines may be that traditionally the transition between paediatric and adult services has not been paid enough attention. It is only in recent years that ‘transition psychiatry’ has begun to specifically highlight the challenges of patient-oriented continuity of care (Fegert et al., 2017), and this article argues that it is also of great importance for music therapy to develop protocols for this age transition.
Setting
The benefit of primary preventive offers established in educational contexts or community settings is that the approaches described are easily accessible and serve to prevent, as far as possible, stigmatization and premature pathologization (Stegemann, 2018: 52) by avoiding hospitalization. Individuals can access support within their familiar environment. However, preventive approaches that are integrated into hospital (primarily outpatient) settings seem to be less common in music therapy literature. As discussed above, the psychiatric early intervention context provides low-threshold medical and psychological help to individuals when they notice changes in themselves which have a negative impact on their everyday life. The advantage of these offers is that they are based on current scientific and interdisciplinary knowledge and incorporate specific predictive knowledge based on risk assessment and ethical considerations into intervention planning. It should be borne in mind that the outpatient music therapy setting may be challenging as individual appointments have to be made and the establishment of therapeutic continuity can be subject to external influences, for example, the diagnostic process, which may be ongoing, or other stress factors. For pragmatic reasons, individual therapy seems to be more feasible than group therapy, although a group may be more promising in terms of peer group experience. For treatment continuity, it can be advantageous to organize music therapy early intervention services under one umbrella with inpatient and outpatient mental health care, especially in the case of severe mental disorders with a high risk of chronification. However, the service concepts of prevention, acute treatment and aftercare should be carefully distinguished from each other. Overall, there is much to suggest that in music therapy, primary prevention in educational or community contexts and indicated prevention in the psychiatric context complement each other in the interest of individually tailored psychosocial care.
Intervention approach
The complex interplay between biological vulnerability and epigenetic and psychosocial influences means that the early diagnosis of bipolar disorder takes place in a multifaceted context. As outlined above, difficulties in regulation of emotions and mood, regulation of activity and drive, and shaping of identity and relationships are among the factors which influence the symptoms presented in the development of bipolar disorder. An early intervention approach should therefore primarily address the current symptoms and stress factors presented as well as personal needs, strengths and interests in order to activate individual resources and offer low-threshold access. Taking this as a basis, an early intervention approach should make it possible to ascertain the individual’s regulation capacities in order to improve them.
Improvisational music therapy facilitates self-expression through the use of music and creative interaction within a therapeutic relationship. The use of music is closely linked to emotional (Juslin and Sloboda, 2011) and social processes (DeNora, 1999) and research has examined the relevance of music for the constitution of identity and self-concept in adolescence (McFerran and Hense, 2017; North and Hargreaves, 1999; Saarikallio, 2017). Recent music therapy research is increasingly focusing on emotion regulation (Gebhardt et al., 2018; Marik and Stegemann, 2016; Saarikallio, 2011; Saarikallio and Erkkilä, 2007; van Goethem and Sloboda, 2011). According to Marik and Stegemann (2016), who are examining models of adaptivity and effectivity of emotion regulation in the context of music therapy, the creative processes of regulation take place within a safe therapeutic relationship and can be regarded as ‘interpersonal emotion regulation’ (Zaki and Williams, 2013). Further theoretical and clinical investigation is required to consider whether the regulation of activity and drive can be regarded as a consequence or result of emotion regulation, or rather as an independent process.
From the perspective of psychodynamic self-development and attachment theories (Fonagy et al., 2015), relational experiences and affect regulation processes are mutually dependent and contribute to self-regulation processes. Using this as a framework, the aims of the music therapy prevention approach described here are to improve self-awareness and self-efficacy in terms of emotional, motivational and social processes. Further clinical investigation is recommended into the application of music therapy methods and techniques in specific target groups and referral contexts.
Conclusion and research questions
The purpose of this article has been to discuss the potential of music therapy in developing an intervention framework for indicated prevention for individuals who have a higher risk of bipolar disorder and who use an early detection centre. This idea lies at the interface between prevention and acute treatment, which raises ethical and methodological questions due to the uncertainty of prediction of mental disorders. The article briefly summarizes the available knowledge on the characteristics of risk and vulnerability for bipolar disorder and the corresponding findings in music therapy, for example, on interpersonal emotion regulation, and existing good practice concerning treatment of the early stages of bipolar disorder. It is suggested that music therapy has the potential to successfully address subthreshold symptoms in adolescents and young adults as well as managing appropriately the ethical and strategic challenges of prediction and early intervention.
It is suggested that further research should address the details of intervention planning, such as the question of goals and methods of music therapy, but also the duration and frequency of preventive efforts. The question of what contribution music therapy can make to risk assessment as well as the qualitative analysis of specific change processes in the context of music therapy treatment are also topics for research. Finally, a scientific evaluation should be aimed at in order to measure the success of the intervention. However, the effectiveness of early intervention in music therapy with regard to the prevention of mental disorders can only be evaluated sufficiently by long-term monitoring of risk processes. This means that the results of a short-term investigation are not necessarily specific to the risk of bipolar disorder, but must rather be regarded as transdiagnostic.
It is hoped that this article will assist Music Therapists to address this under-resourced and under-researched clinical area. The specific demands that bipolar disorders place on therapy and the question of how to meet these demands through music therapy have not been sufficiently discussed in the music therapy literature. Music therapy potentials should be more courageously introduced into psychiatric outpatient care, for example, in the context of prevention but also maintenance and relapse prophylaxis of severe mental health conditions such as bipolar disorder, and thus make an important contribution to both early intervention and treatment continuity.
Footnotes
Acknowledgements
My thanks go to Professor Dr Susanne Metzner, head of the master’s programme in music therapy at Augsburg University, Germany, for her continuous advice and faithful support of my research. I also would like to thank Professor Dr Andrea Pfennig, head of the Early Detection Centre of the University Hospital in Dresden, Germany, who gave the initial idea to this topic and supported me with important comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.